We offered to take the patient to the county hospital to obtain the appropriate diagnostic procedure and to initiate inpatient care. He adamantly refused treatment in a hospital, stating he was “too busy” to go the hospital and he only wanted “some pills.”
What else could you now do to care for this patient?
The differential diagnosis includes septic arthritis (such as staphylococcal and gonococcal infections of the knee joint), inflammatory types of arthritis, septic bursitis, cellulitis, and impetigo. Joint aspiration was performed in the clinic because the patient refused to go to the emergency room for diagnosis and treatment.
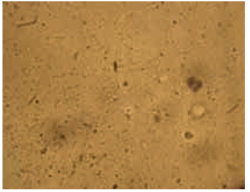
As seen in Figure 2, 10 mL of clear viscous yellow fluid was aspirated from the affected joint. Nine mL of aspirate was sent to a clinical laboratory for cell count, Gram stain, culture and sensitivity, crystal analysis, and microscopic examination. A drop of aspirate was placed on a wet mount and examined with plain light microscopy (Figure 3).
FIGURE 2
10 mL of clear viscous yellow fluid was aspirated from the joint.

Numerous refractile needle-shaped crystals were visualized.
Epidemiology of acute gout
Acute gout is predominantly a disease of the lower extremity, but any joint of any extremity may be involved. Ninety percent of patients experience acute attacks in the great toe at some time during the course of their disease. Next in order of frequency are the insteps, ankles, heels, knees, wrists, fingers, and elbows. The incidence of gout varies in populations from 0.20 to 0.35 per thousand per year, with an overall prevalence of 1.6 to 13.6 per thousand. The prevalence seems to increase substantially with age and increasing serum urate concentration.1 Prevalence is 3/100,000 for those 18 to 44 years of age; 21/100,000 for those 45 to 64, and 35/100,000 for those over 65. Men are 20 times more likely to have gout than women.2