This Photo Rounds aims to help you hone your visual diagnostic skills to recognize the 3 most common types of skin cancer (in order of prevalence): basal cell carcinoma, squamous cell carcinoma, and melanoma. (See also “Diagnosis of skin malignancy,”.)
Pattern recognition informs us about the initial differential diagnosis and the appropriate biopsy method.
Basal cell carcinoma
The most common basal cell carcinoma is nodular. Figure 1 shows nodular basal cell carcinoma with a raised pearly pink and white nodule with a smooth, shiny, translucent surface. The smooth surface reflects a loss of the normal pore pattern. Telangiectasias can be seen within the lesion, and the border may appear to be rolled.
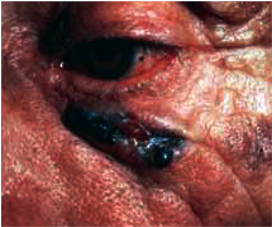
Figure 2 shows a nodular basal cell carcinoma that is both pigmented and has some central ulceration. This figure demonstrates how difficult it is to distinguish a melanoma from a pigmented basal cell carcinoma.
Figure 3 shows the next most frequently seen basal cell carcinoma, the superficial basal cell carcinoma. These lesions are found most often on the trunk and extremities rather than the face, and may appear as a pink scaling plaque. Sometimes shallow crusts or erosions may be seen within the lesion. Note the thready border present around this scaling plaque. This slightly elevated border is the best tip-off to recognizing this scaling plaque as a skin cancer rather than a plaque of psoriasis or nummular eczema.
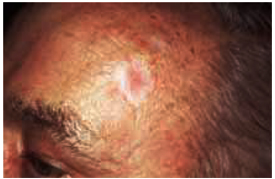
Figure 4 shows the least prevalent basal cell carcinoma, the sclerosing type. These lesions are often ivory-colored or colorless. The skin may be appear atrophic and feel indurated. A sclerosing basal cell carcinoma may resemble a scar and can be easily overlooked. These carcinomas are often called morpheaform because of the resemblance to localized scleroderma (morphea). They are also called infiltrating basal cell carcinoma because they infiltrate into the surrounding normal skin in a way not easily visible to the naked eye.
FIGURE 1