The second stage involves maturation of capsule scaring, resulting in decreased pain and increased restriction of movement.
The third stage is resolution of the condition, leading to a gradual increase in range of motion.
Full range of motion may or may not return, and the time to resolution is typically 1 to 2 years. Adhesive capsulitis is most common in older persons, especially women in the fourth and fifth decades.5
Comparing nonoperative treatments
Nonoperative treatment modalities include protection, relative rest, and ice (PRI); anti-inflammatory medications; physical therapy (supervised or home exercise program); acupuncture; and steroid injection.
Operative treatments, depending on the particular disorder, include rotator cuff repair, subacromial decompression, capsular tightening, or manipulation under anesthesia.
The efficacy of nonoperative treatments for shoulder pain is not well known. Studies of treatment modalities have been numerous but generally of poor quality due to a lack of uniformity in how shoulder disorders are defined and in the variability of outcome measures used. Several recent systematic reviews have tried to identify which interventions are efficacious ( Table 2 ).6-11
Overall, NSAIDs and subacromial steroid injections are effective in the short-term treatment of shoulder pain.26-28 However, only nonselective NSAIDs have been studied. Evidence is insufficient to recommend use of cyclooxygenase-2 (COX-2) medications for shoulder pain.
Steroid injections may not confer extra benefit when added to NSAIDs, but they appear superior to NSAIDs in improving shoulder abduction. This is particularly true for the painful stiff shoulder, as seen with impingement or rotator cuff disease.26,28
Two recent randomized control trials showed corticosteroid injections to be superior to physical therapy for treatment of shoulder complaints.12,13
Shoulder instability may be treated nonoperatively at first with PRI, NSAIDs, and strengthening and proprioceptive exercises for the rotator cuff. If 3 to 6 months of nonoperative treatment fails, the patient should be referred for surgical evaluation, especially in cases of full-thickness rotator cuff tears.14
TABLE 2
Nonoperative treatment options for shoulder pain
| Treatment | Comment | SOR |
|---|---|---|
| NSAIDs |
| C |
| Physical therapy |
| B |
| Ultrasound |
| A |
| Steroid injection |
| B |
| Acupuncture |
| C |
| SOR, strength of recommendation (SORT); NSAIDs, nonsteroidal anti-inflammatory drugs. | ||
Treatment of specific shoulder disorders
Subacromial impingement syndrome stage I
A recommendation (SOR: B) can be made for the use of NSAIDs in the treatment of stage I impingement ( Table 3 ). This is based on level 2 evidence that NSAIDs are beneficial for rotator cuff tendinopathy and bicipital tendinitis, compared with placebo in a 1 to 2 week follow-up.15,17 No specific NSAID has proved better than another.18,19
Steroid injection ( Figure 2 ) is beneficial for the acute treatment of SIS I reflected by improvement in pain (SOR: A).20-23 This is particularly evident during the first 1 to 2 weeks following injections.38 At 4 to 6 weeks, there appears to be no difference in the efficacy of steroid injection compared with NSAIDs,24,25 but they are both better than placebo.43
Physical therapy, specifically rotator cuff strengthening and range of motion, is as beneficial as surgery for SIS I at 6 month and 21/2-year follow-up, and both were better than placebo (SOR: B).26,27
TABLE 3
Treatments for SIS I impingement (rotator cuff tendinitis/tendinosis)
| Treatment | Comment | LOE |
|---|---|---|
| NSAIDs |
| 1c |
| NSAIDs vs steroid injection |
| 1a |
| Subacromial steroid injection |
| 1b |
| Surgery |
| 2a |
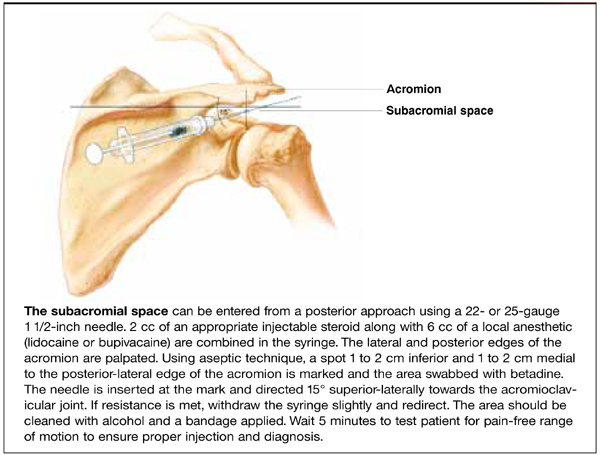
FIGURE 2
Steroid injection in the subacromial space
SIS stages II and III
There is very good evidence (SOR: B) regarding the efficacy of nonoperative treatment of SIS II and III, based on level 2 cohort studies that suggest nonoperative care leads to improvements in patient satisfaction, pain, and daily activities.28,29 Similar outcomes are reported for patients undergoing physical therapy alone.30,31 Weiss reported that corticosteroid injections for stage III/full-thickness rotator cuff tears resulted in an 86% improvement as measured by return to previous activities and less or no pain with motion ( Table 4 ).32
The most constant outcome measure was report of a reduction in pain. Younger patients or those with higher functional demands will likely consider surgical repair if nonoperative measures fail, particularly for full-thickness tears.