Practice recommendations
For our purposes, the evidence ratings are based on literature quality, not expert opinion, and are updated to comply with the SORT taxonomy*
Grade A Recommendations
- Severity-of-illness scores can be used to identify patients with CAP who are candidates for outpatient treatment.
- Appropriate outpatient antibiotic treatment for a previously healthy person, with no risk factors for drug-resistant S. pneumonia (DRSP) is a macrolide (azithromycin, clarithromycin, or erythromycin).
- High risk patients: those with co-morbidities (chronic heart, lung, liver, or renal disease), diabetes mellitus, alcoholism, malignancies, asplenia, immunosuppression, or antibiotics within 3 months should be treated with a respiratory flouroquinolone—moxifloxacin, gemifloxacin, or levofloxacin (750 mg dose).
- A beta-lactam (high-dose amoxicillin, amoxicillin clavulanate, ceftriaxone, cefpodoxime, of cefuroxime), plus a macrolide is an option for high risk patients.
- Blood cultures and sputum cultures are optional prior to treatment of outpatients.
- In geographic areas where >25% of pneumococcal organisms are macrolide resistant, a beta-lactam, plus docxycycline should be considered.
- Treat with antibiotics at least 5 days.
- Health care workers in inpatient and outpatient settings and long-term facilities should receive annual influenza immunization.
Grade B Recommendations
- Severity of illness scores should be supplemented with physician subjective opinion about individual patients. the ability to safely and reliably take oral medications and the availability of outpatient resources should be considered.
- Patients with Cap should be investigated for specific pathogens that would significantly alter standard (empirical) management decisions, when suspected on the basis of clinical assessment.
- A beta-lactam, plus doxycycline is an alternative to the beta-lactam, plus macrolide combination for high risk patients.
- Pneumococcal polysaccharide vaccine is recommended for persons >65 years of age and for those with selected high-risk concurrent diseases.
Grade C Recommendations
- In addition to clinical features, an infiltrate by chest radiograph or other imaging technique is required for the diagnosis of pneumonia.
- An appropriate outpatient treatment for previously healthy individuals with no risk factors for DRSP infection is doxycycline.
- Use respiratory hygiene measures (hand hygiene, masks, tissues) for patients with cough in outpatient settings.
*Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. J Fam Pract 2004; 53:111–120.
When is outpatient treatment appropriate for community-acquired pneumonia (CAP)? Which antibiotics are recommended for outpatient therapy? What are the best prevention strategies? The answers are in the consensus guidelines published earlier this year by the Infectious Diseases Society of America and the American Thoracic Society (IDSA/ATS). The new guidelines update an IDSA guideline published in 2003.
Background. Management (and prevention) of CAP is inconsistent, and there is also emerging resistance of pneumococcus to macrolides.
These guidelines were developed to hasten consistency among caregivers and hospitals in the care of patients with pneumonia. Appropriateness of outpatient care, severity of illness assessment, hospital treatment decisions, ICU care, and choice of antibiotics for high-risk patients and for drug-resistant S pneumonia were reviewed. The joint committee recommended that hospitals standardize care and create policies to increase the vaccination rate.
Cases that test your skills

CASE 1
Your patient is a 45-year-old man with cough, fever, and chills. He has a history of metabolic syndrome, and a 40 pack-year smoking history. He was well until 1 week ago when he went camping in the rain. Over the last 2 days he has had shaking chills, cough productive of green phlegm, and he finds that he gets a bit short-winded when walking stairs. He wonders if he has pneumonia. He is overweight and in no acute distress.
T 101 • P 88 • RR 18 • WT 220 • HT 5 7
Exam Normal other than localized coarse rales in the left posterior lung field; spot O2 saturation is 96%
What is your diagnosis and initial management?
Which of the following statements are true regarding the outpatient management of pneumonia?
- If 2 or more CURB-65 criteria are present, the patient should be hospitalized
- A macrolide is an appropriate choice of treatment for a previously healthy person with no risk of drug resistance
- A positive chest x-ray or other imaging is required for the diagnosis
- Blood cultures and sputum cultures must be obtained
- Antibiotic treatment should be a minimum of 10 days
ANSWERS: A, B, AND C
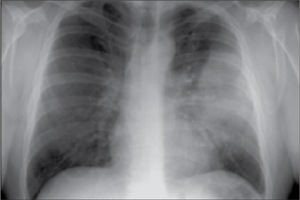
Diagnosis Community acquired pneumonia—left lobar.
Initial management This patient can be treated as an outpatient based on the severity-of-illness scores in this guideline. He should be treated with antibiotics a minimum of 5 days. With his comorbidities, antibiotic choices include 1) a fluoroquinolone, 2) a beta-lactam plus macrolide, or 3) (in areas with high prevalence of macrolide resistance) a beta-lactam plus doxycycline.
CASE 2
A 76-year-old man is brought into the office by his niece. “I just don’t feel well,” he says. The patient has been increasingly ill over the past week, and his niece is concerned that he seems to have trouble breathing. The patient minimizes his symptoms, but in relaying his history, he is obviously short of breath and cannot talk continuously. He needed a wheelchair to come in from the parking lot (and you know that he is usually spry and ambulatory). He has a history of congestive heart failure, hypertension, type 2 diabetes mellitus, depression, and osteoarthritis. He takes furosemide, potassium, enalapril, lantus insulin, sertraline, and PRN acetaminophen. He has never smoked. He denies PND and orthopnea. He is clearly short of breath and in some mild distress.
T 99 • P 102 • RR 36 • WT 260 • HT 5 9
Exam Remarkable for diffuse rhonchi and wheezing across all lung fields; spot O2 saturation is 89%
What is your diagnosis and initial management?
The differential diagnosis for this patient includes:
- Bacterial pneumonia
- Viral pneumonia
- Depression
- Congestive heart failure
- Pulmonary embolus
ANSWERS: A, B, D, E
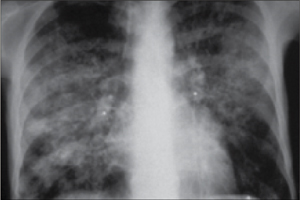
Diagnosis This interstitial pattern on the chest x-ray is associated with multiple etiologies, both infectious and non-infectious. Examples include viral pneumonia, opportunistic infections in HIV patients, atypical infections such as mycoplasm, congestive heart failure, and pulmonary embolus.
Initial management Based on severity-of-illness scores, this patient should be admitted to the hospital. He should have further evaluation to identify the etiology.