7-Minute Neurocognitive Screen considers normal aging
This neurocognitive screen is highly sensitive and specific (mean, 92% and 96%, respectively) for the early stages of AD and can distinguish between cognitive changes due to normal aging and those due to dementia.29 The screen consists of 4 brief tests: orientation for date and time, a 5-word recall test to assess memory function, a clock-drawing test to evaluate visuospatial skills, and a semantic verbal fluency or output task. Examples of verbal fluency measures include category generation (eg, names of animals), letter (eg, number of words beginning with a particular letter), and first names.
Interpreting the 7-minute screen. This instrument was initially validated on 60 patients diagnosed as having probable AD and 60 community-dwelling volunteers of comparable age, sex distribution, and education. The neurocognitive screen has reasonable interrater and test-retest reliability and can be administered in a short time by an individual with little clinical judgment and minimal training. Unlike the MMSE, its outcome is not affected by age or education.29
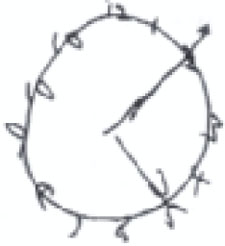
Clock-drawing: What to look for

The numbers on this clock are not proportionally distributed, and only 1 hand is correctly placed.
Total score: 2
The numbers are outside the circle, and there are 2 number 10s on this clock, but both hands are correctly placed.
Total score: 3
A reasonable circle with both hands correctly placed, but the numbers are disproportionately distributed.
Total score: 4
When clock drawing is used as an independent screen, it is generally graded 0 to 5, based on the shape of the circle, the distribution and inclusion of all the numbers, and the length and placement of the hands. A score of ≤3 is suggestive of dementia. All the patients here were asked to show the time as 10 minutes past 5.

The numbers on this clock are not proportionally distributed, and only 1 hand is correctly placed.
Total score: 2
The numbers are outside the circle, and there are 2 number 10s on this clock, but both hands are correctly placed.
Total score: 3

A reasonable circle with both hands correctly placed, but the numbers are disproportionately distributed.
Total score: 4
Could it be depression?
Patients with suspected dementia should also be screened for depression, because this psychiatric disorder can impersonate dementia, or exist concurrently. Depression occurs in 25% of dementia patients; it is an independent risk factor for institutionalization, and should be detected and treated.30 Subclinical depression in older women is a risk factor for cognitive decline, as well.31 Although patient presentation is not a substitute for a screening tool, the following can be helpful in distinguishing dementia and depression:
Memory. A patient suffering from depression alone is more likely to complain of memory problems than a patient with cognitive dysfunction.
Psychomotor. A depressed patient is also more likely to exhibit psychomotor retardation. Function is rarely, or only mildly, impaired in the early stages of dementia, and the movements and reactions of a patient with mild cognitive impairment often appear normal.
Concentration. Depression interferes with the ability to concentrate, and the patient may exhibit an obvious disturbance. Patients with dementia often appear to have a normal ability to concentrate, but demonstrate greater intellectual strain in attempting to answer test questions.
A 5-item geriatric screen for depression
One useful screen for depression is the 5-item version of the Geriatric Depression Scale, which has been validated in older adults.32,33 It asks the following questions:
Are you basically satisfied with your life? Do you often get bored? Do you often feel helpless? Do you prefer to stay at home rather than going out and doing new things? Do you feel pretty worthless the way you are now? This 5-item test is scored by awarding 1 point if the answer to the first question is No, and 1 additional point for each Yes answer to the remaining questions. A score of 2 or more is considered to be diagnostic for depression.
Did you suspect depression?
As you may have suspected, Fran B—the last of our 3 patients—was suffering from depression rather than dementia. Fran had a score of 4, and was referred to a psychotherapist.
Cognitive screening resources
Mini-Mental State Examination
http://www.nia.nih.gov/NR/rdonlyres/1C0BFA48-8280-422B-97E6-195BBFD84BA2/0/mmse.PDF
Montreal Cognitive Assessment
www.mocatest.org
AD 8 Dementia Screening Interview
http://alzheimer.wustl.edu/About_Us/PDFs/AD8form2005.pdf
7-Minute Neurocognitive Screen
http://memorydoc.org/7minutescreen
Keep these tools on hand
The assessment tools discussed in this review can help you identify mild cognitive impairment or early dementia, rule out depression, and—in many cases—reassure patients (or concerned family members) that their experiences are consistent with normal aging. All are easy to incorporate into a busy primary care practice without undue concern about the time they will take to administer.
Correspondence
Diana R. Kerwin, MD, Division of Geriatrics and Gerontology, Medical College of Wisconsin, 9200 West Wisconsin Avenue, Milwaukee, WI 53226; dkerwin@mcw.edu