Shailendra Prasad, MBBS, MPH; Michael R. Wootten, MD Department of Family Medicine and Community Health, University of Minnesota, Minneapolis pras0054@umn.edu
Nichole Kulinski, PharmD; Scott A. Chapman, PharmD College of Pharmacy, University of Minnesota, Minneapolis
The authors reported no potential conflict of interest relevant to this article.
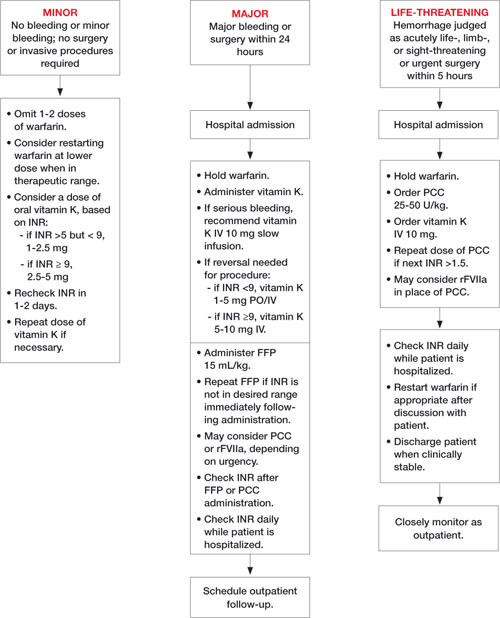
Here’s how to put this classification system—and the ACCP’s 2008 guidelines for managing patients with elevated INR16 (FIGURE)—into action:
In the case of minor bleeding and elevated INR, withhold the next 1 to 2 doses of warfarin.16 If the patient is considered high risk, give oral vitamin K in small amounts (1-2.5 mg). Keep in mind that excessive amounts of vitamin K will promote warfarin resistance.
FIGURE Reversal of warfarin-induced anticoagulation
FFP, fresh frozen plasma; INR, international normalized ratio; IV, intravenous; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII. Adapted from: Ansell J et al. Chest. 2008.16 Ask the patient to return to your office in 1 or 2 days for a recheck of INR. If it remains elevated, give another dose of vitamin K. Warfarin may need to be restarted at a lower dose depending on the clinical situation.17,32
FAST TRACK
A wide range of medications and herbal products can interfere with warfarin therapy, so it is essential to ask patients to tell you everything they’re taking.
In cases of major bleeding and elevated INR, stop the warfarin, give vitamin K (the administration route will be based on clinical presentation and the urgency of reversal), and arrange for factor replacement and hospital admission.16 Use FFP, if possible, because more is known about its safety than the safety of PCC or rFVIIa. That said, the choice of factor replacement should be based on the urgency of reversal and on clinical condition.16,33,34
INR should be rechecked immediately after factor replacement. Because coagulation factors have varied half-lives, INR should be checked daily for the next 4 days to confirm that it remains at a therapeutic level.16
In cases of life-threatening bleeding, stop the warfarin, give 10 mg vitamin K IV, and replace clotting factors.16 PCC should be considered because it will reverse the anticoagulation in the shortest amount of time, without limitations associated with fluid status, blood type-matching, or infusion reaction.35,36 While the risk of thrombosis needs to be evaluated in each high-risk circumstance, the use of either PCC or rFVIIa, depending on availability, is appropriate for a life-threatening bleed.29,37
FAST TRACK
While fresh frozen plasma can offset coagulopathy rapidly, the time needed for thawing and blood type-matching must be taken into account.
Classifying—and treating—our patient
Based on our classification system, we determined that Mary Jo had major bleeding: She needed inpatient monitoring, with the possibility of a blood transfusion, but her condition was not life-threatening. She was hospitalized immediately. Her warfarin was withheld and she was given vitamin K IV and FFP to reverse her hypocoagulable state.
Once Mary Jo’s hypocoagulable state was reversed, which took about 4 hours, she was evaluated and found to have a small bleeding ulcer. The ulcer was cauterized, and her condition remained stable. A detailed investigation of possible reasons for the patient’s elevated INR did not reveal any causes. Three days after the cauterization, Mary Jo was started back on a lower dosing schedule of warfarin. She was discharged after a 5-day stay, with instructions to return to the clinic in 5 days for continued monitoring.