PRACTICE RECOMMENDATIONS
• Emollients should be used during acute flares as well as regularly for maintenance therapy in children with atopic dermatitis (AD). A
• Topical corticosteroids are the first-line therapy for acute AD flares. A
• There is no evidence to support the use of antihistamines for treatment of AD. A
• Exclusion of cow’s milk and eggs is not recommended except in proven cases of milk or egg allergy with sensitivity testing and food challenge. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Dylan, an 8-month-old boy whom you had seen for a routine check-up a little over a month ago, is in your office today because of a rash on his face and elbows. The rash began about 2 weeks ago, his mother reports—shortly after she had weaned him from the breast milk to formula. Certain that Dylan has a milk allergy, his mother tells you she plans to switch to a soy-based formula—and wants you to give her something to put on the rash to help clear it up.
CASE 2 Eighteen-month-old Angela had a mild case of atopic dermatitis when you saw her about 3 months ago. The reason for today’s visit is that “her eczema is getting worse,” according to her mother, and the moisturizing cream that you recommended at her last visit “stopped working.” The rash, which had been confined to the patient’s forearms and knees (FIGURE 1), now covers much of her face, forearms, knees, and trunk. Angela’s mother says that the rash appears to be very itchy and that her daughter has been crying and scratching at night.
If Dylan and Angela were your patients, what would you advise their parents to do, and how would you treat them?
FIGURE 1
An 18-month-old girl with an acute flare

This child has moderate atopic dermatitis, with erythema and localized thickened skin at the medial knee—a typical site for atopic dermatitis.
Atopic dermatitis (AD), or eczema, is a chronic inflammatory skin condition that affects up to 20% of children.1 The incidence of pediatric AD has increased 2- to 3-fold in the last 30 years (it’s not clear why), and the condition is a common reason for pediatric visits to family physicians.1,2
AD is marked by phases of pruritus and rash and, depending on the severity, can significantly affect the quality of life of young patients and their families.1-4 The pathophysiology involves structural abnormalities of the epidermis—leading to dry and sensitive skin—combined with immune dysregulation.

Topical corticosteroids to decrease the inflammation and emollients to repair and hydrate the skin are the mainstay of treatment.3,5,6 But numerous considerations, including what triggers patients should avoid; how potent a steroid to prescribe; how long to continue treatment; and when, or whether, to initiate systemic treatment, remain. The evidence-based review of traditional and alternative treatments (TABLE)1-3,7-19 and practical step-wise approach (FIGURE 2)1-3,5,6,9,19-22 that follow can help ensure that you give children with AD the best possible care.
FIGURE 2
A stepped approach to atopic dermatitis1-3,5,6,9,19-22
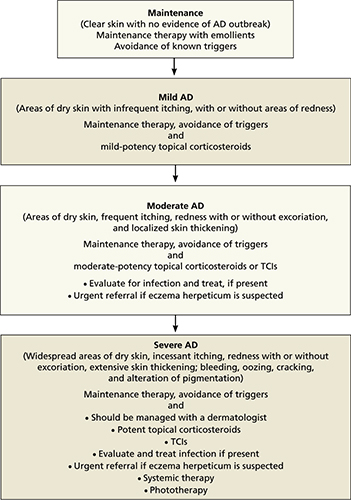
AD, atopic dermatitis; TCIs, topical calcineurin inhibitors.
TABLE
Treating atopic dermatitis: What the evidence shows
| Intervention (SOR) | Comments |
|---|---|
| Maintenance | |
| Emollients (A)1,2,7,8 | Mainstay of maintenance therapy |
| Treatment | |
| Corticosteroids9-15 – Topical (A) – Oral (B) | First-line treatment No proven benefit |
| TCIs:3,16,17 – Pimecrolimus (A) – Tacrolimus (A) | Second-line treatment |
| Symptom relief | |
| Antihistamines (A)11,14 | No proven benefit in the treatment of AD; sedating antihistamines may improve sleep |
| Tar (C)14 | |
| Wet wrap dressings (C )18 | |
| Infection1,11 | |
| Antibiotics – Topical (A) – Oral (A) | |
| Antifungals – Topical (A) – Oral (A) | |
| Alternative/preventive measures11,19 | |
| Breastfeeding (B) | May reduce risk of developing AD (poor quality study) |
| Essential fatty acids* | No proven benefit |
| Exclusion of eggs or cow’s milk (B) | Only in proven cases of allergy |
| Multivitamins, B6, zinc supplements (C) | No proven benefit |
| Probiotics (B) | No proven benefit |
| Vitamin D supplementation (C) | More studies needed |
| *Black currant seed oil, evening primrose oil, fish oil. AD, atopic dermatitis; TCIs, topical calcineurin inhibitors. | |
The patient has a rash, but what’s the trigger?
Epidemiologic studies have identified numerous AD triggers, including sweating, stress, dust, hard water, food allergies, and seasonality.23 Environmental or situational triggers should be avoided whenever possible,20 of course, but first, they must be identified—an often-difficult task. Establishing the role of any exacerbating factor in AD involves documentation of a temporal relationship between exposure and the development or worsening of symptoms; a dose-response effect; and remission after withdrawal of the trigger.
What’s more, avoidance does not always have the desired result. There is a well-demonstrated correlation between house dust mite sensitization and AD, especially in children of preschool age and older.7,21 Studies performed to determine whether decreasing house dust mite antigen would have a positive effect on disease severity, however, have had conflicting results.23