Choose carefully among the supplements
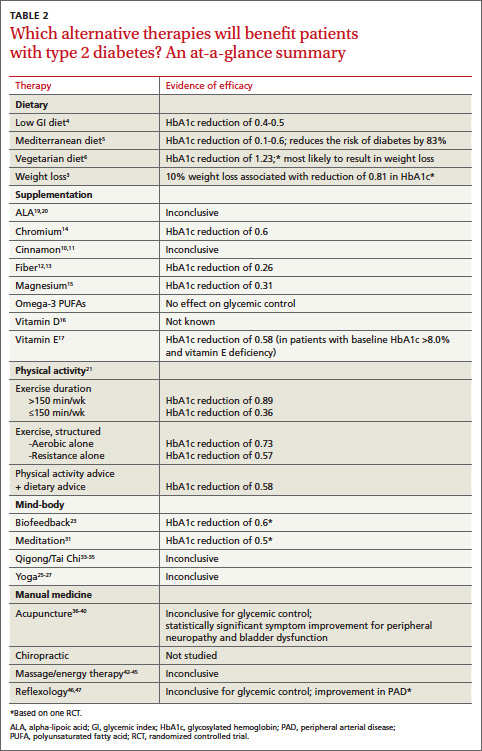
Metformin was derived from Galega officinalis—a plant (sometimes called goat’s rue, or French lilac) used by Europeans as a traditional treatment for diabetes since the Middle Ages.9 More than 400 dietary supplements have been reported to have beneficial effects for patients with diabetes, including plant-based products such as fenugreek, prickly pear, and ginseng; vitamins, and minerals. But in most cases, the evidence is of poor quality (TABLE 2). Only one—cinnamon—has Level I evidence (ie, evidence derived from at least one well-designed RCT).
Two recent meta-analyses of cinnamon supplementation for patients with diabetes—one from 2012 and the other from 2011— yielded different results. The 2012 evidence comes from a Cochrane review showing that 3 types of cinnamon—true cinnamon (Cinnamomum zeylanicum), Chinese cinnamon (C cassia), and Indonesian cinnamon (C burmanni)—had no effect on HbA1c in patients with type 1 or T2DM and a borderline effect on FBG.10 However, the 2011 meta-analysis found that cinnamon supplementation led to a significant improvement in FBG.11
The bottom line? The evidence is inconclusive.
Fiber and chromium stand out
Fiber. Whether taken as a supplement or in foods such as chickpeas, beans, peas, and lentils, fiber has been shown to improve glycemic control.12,13 The ADA recommends 25 to 35 g of dietary fiber daily.13 The American Diabetes Association recommends 25 to 35 g of dietary fiber daily.
Chromium, a trace mineral thought to be a necessary cofactor for insulin regulation and glucose metabolism, is present in many foods, especially brewer’s yeast, liver, carrots, potatoes, broccoli, and spinach. Notably, however, refining grains and processing foods removes most absorbable chromium. Patients with T2DM may therefore benefit from chromium supplementation: A 2007 systematic review found that it lowered their HbA1c by an average of 0.6.14
What about other supplements?
The ADA does not generally support the use of micronutrient supplements for patients with diabetes, but notes that individuals at increased risk for deficiencies (eg, those following very-low-calorie diets, the elderly, and strict vegetarians) may benefit from multivitamin supplements.
Magnesium. Dietary sources of magnesium, which is involved in insulin secretion, binding, and activity, include whole grains, leafy green vegetables, legumes, and nuts. A deficiency is associated with decreased absorption (in patients with diets high in processed food, for example) or increased elimination (in those who ingest large quantities of alcohol or caffeine or take diuretics or birth control pills). A 2006 meta-analysis found that magnesium supplements led to an improvement in FBG, but did not significantly lower HbA1c in patients with T2DM.15
Vitamin D. Although individuals with the highest vitamin D levels (>25 ng/mL) have a 43% lower risk of developing diabetes,16 it is not known whether vitamin D supplements are beneficial to patients with T2DM. (For more on vitamin D supplementation, see the Practice Alert in this issue.)
Vitamin E. A fat-soluble antioxidant found in vegetable oil, nuts, and green leafy vegetables, vitamin E’s best-studied component is alpha-tocopherol. A 2011 meta-analysis found vitamin E supplementation to have a beneficial effect in patients with T2DM—but only for the subset of patients who had both low serum vitamin E levels and an HbA1c >8.0%.17 Observational studies have raised questions about the safety of vitamin E supplements, and a 2005 meta-analysis concluded that high-dose vitamin E supplementation (≥400 IU/d) may increase all-cause mortality.18
Observational studies have raised questions about the safety of vitamin E supplements, and a 2005 meta-analysis concluded that high-dose vitamin E supplementation (≥400 IU/d) may increase all-cause mortality.18
What about omega-3 PUFAs?
The role of omega-3 polyunsaturated fatty acids (PUFAs) in the prevention and treatment of diseases related to inflammation has garnered much attention for years. But there is no evidence that taking omega-3 PUFAs lowers the risk of macrovascular outcomes or mortality for patients with T2DM.
Alpha lipoic acid (ALA), an antioxidant made by the body and found in very small amounts in foods, is widely used in Europe, and has shown promise in the treatment of diabetic neuropathy. Small studies have found that ALA may reduce oxidative stress and improve insulin sensitivity in patients with diabetes,19 and a recent small RCT showed a statistically significant decrease in FBG and postprandial glucose after 8 weeks of taking it.20
How to get patients moving
The ADA recommends that patients with T2DM get 150 minutes per week of moderate intensity aerobic activity (at 50%-70% of maximum heart rate), spread over at least 3 days a week and with no more than 2 consecutive days without activity. Resistance training provides additional benefit; the ADA recommends that patients engage in resistance training at least twice a week, using 5 major muscle groups.7 Regular exercise helps both weight reduction and glucose uptake, but simply pointing that out to patients with T2DM is not enough.