PRACTICE RECOMMENDATIONS
› Schedule twice-monthly visits when prescribing a psychostimulant to assess symptom control, review adverse effects, and record blood pressure, pulse, height, and weight in determining the optimal dose. C
› Keep in mind that using a psychostimulant can put endurance athletes at risk for heat-related injury. C
› Advise college-bound athletes that the NCAA requires a therapeutic use exemption for those who take psychostimulant medications. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The symptoms typical of attention-deficit/hyperactivity disorder (ADHD)—inability to focus concentration and maintain attention span, and associated hyperactivity—impair normal daily functioning and cause distress for affected individuals.1 For the student athlete with ADHD, sports are a natural outlet, fulfilling the need to be active. In the case of a developing child with ADHD, involvement in sports often is a haven from negative feedback that can occur in the classroom and an environment in which to experience success.
Symptoms of ADHD also may offer an advantage in sports. Impulsivity, or the ability to act without reflection, enables quick decision-making and the spontaneity required of a quarterback or point guard.2 Well-known athletes with ADHD have said that while tasks requiring long stretches of concentration are difficult, aspects of their sport involving instantaneous reactions help them to succeed. Evidence also shows a statistically significant decrease in markers of anxiety and depression among ADHD subjects with higher levels of sports participation.3
Given the positive experience sports can provide, children and adolescents with ADHD are likely to continue participating and be as large a segment of youth athletes as they are of the general population.2,4 Primary care providers often treat student athletes, and in this article we discuss the need for accurate diagnosis through comprehensive clinical evaluation, proper use of psychostimulant medication and other available treatments, and special health concerns for athletes who have ADHD.
Diagnosis: The need for awareness and accurate evaluation
The worldwide prevalence of ADHD is 5.3%.5 In the United States, it is 8.7% among adolescents and 4.4% among adults.6,7 One study of NFL athletes found that 14 of 159 players studied had either ADHD or a learning disability for a combined prevalence of 8.8%.8 ADHD is diagnosed 3 times more often in males than females9; however, studies have shown no gender effect on ADHD, and referral patterns contribute to the higher prevalence pattern for males.10
ADHD usually is diagnosed in childhood, but increasingly, it is not established until adolescence or adulthood.2,9 Although there is no age limit for the diagnosis, the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) calls for the presence of some symptoms before age 12, and symptoms must cause impairment of functioning in multiple settings.1 While hyperactivity symptoms may decrease over time, a significant number of children and adolescents will experience inattention symptoms into adulthood.11 In fact, the disorder may not become evident until college entry, when academic demands overwhelm an individual’s usual coping strategies.2
Multiple reasons for an accurate diagnosis. Initiate evaluation for ADHD for any child 4 to 18 years of age who exhibits symptoms of inattention, hyperactivity, or impulsivity to such a degree that it causes distress or impairment at home, at school, or on the sports field.12 Making an accurate diagnosis of ADHD is vital in student athletes given that treatment, or lack thereof, may put their health at risk and adversely impact their academic and athletic performances. Diagnostic accuracy also aids in distinguishing the student athlete with a legitimate need for treatment from one who is fine and merely looking for a performance enhancer.9 Moreover, having a comprehensive assessment with diagnostic confirmation already in place when an individual enters college greatly facilitates completion of National Collegiate Athletic Association (NCAA) medical exemption documentation.
Essential diagnostic steps. The core clinical evaluation should cover the following:
• Ensure that DSM-5 criteria are met.
• Obtain objective reports to confirm the presence of symptoms in multiple settings. Commonly applied symptom assessment scales include the Brown, Vanderbilt, and Connors questionnaires administered to parents, teachers, and adolescent patients mature enough to complete a self-evaluation.
• Determine whether comorbid conditions are present.
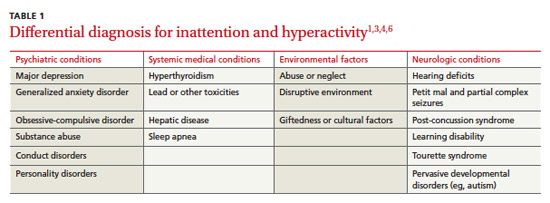
• Rule out medical conditions that can mimic ADHD (eg, lead toxicity or thyroid disorder).
No neurocognitive or laboratory test for ADHD has sufficient sensitivity and specificity to qualify as a standard diagnostic test.2,13 In the future, advanced neuroimaging may provide a means of diagnosing ADHD. Functional magnetic resonance imaging has shown characteristic patterns of reduced activation in the basal ganglia, frontal lobe, and parietal lobes in patients with ADHD.14