Gary Rivard, DO Anthony Viera, MD Family Medicine Residency Program, Central Maine Medical Center, Lewiston (Dr. Rivard); Department of Family Medicine, University of North Carolina at Chapel Hill (Dr. Viera) rivardga@cmhc.org
The authors reported no potential conflict of interest relevant to this article.
Any patient who reports having a persistent cough should be considered for pertussis testing and treatment, and any clinician who triages such patients should ask detailed questions about the characteristics and duration of the patient’s symptoms. Antibiotics do not appear to shorten the duration of pertussis symptoms unless given in the catarrhal phase. However, while a prolonged cough is the hallmark of pertussis, there are many other potential causes of this symptom. Therefore, diagnosis of pertussis requires a combination of clinical and laboratory testing, because clinical parameters alone are neither sensitive nor specific enough for pertussis infection.
TABLE 216 outlines the clinical and laboratory diagnostic criteria for pertussis from the CDC and the World Health Organization. Suspect pertussis in a patient who’s had a cough for more than 14 days that includes an inspiratory “whoop.” In infants, pertussis should be suspected in those with symptoms that suggest cough and associated apnea.16 Order laboratory testing for any patients who have clinical signs or symptoms of pertussis.
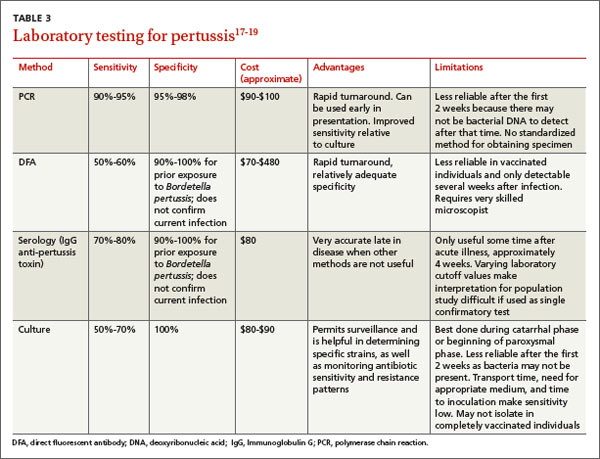
Four methods of lab testing for pertussis infection are polymerase chain reaction (PCR), direct fluorescent antibody (DFA) testing, serologic testing, and culture (TABLE 3).17-19 The sensitivity of these tests is as follows: PCR, 90% to 95%; DFA, 50% to 60%; serologic testing, 70% to 80%; and culture, 50% to 70%. The specificity is: PCR, 95% to 98%; DFA, 90% to 100%; serologic testing, 90% to 100%; and culture, 100%.
PCR is the preferred method because of its rapid turnaround and fairly high sensitivity. The reliability of PCR decreases, however, for a patient who’s had a cough for more than 2 weeks because the individual may have transitioned to the convalescent phase, when less bacterial DNA remain.
Results from DFA testing also are rapidly available, but the need for specialized equipment and a well-trained examiner of the specimen limits widespread use of this test. It also is not particularly sensitive for pertussis.
Serologic testing is less reliable in patients who have received an acellular pertussis vaccine and is not helpful in the first few weeks of infection.
The sensitivity of culture is best if the sample is collected appropriately (more on this in a bit) and within the first 2 weeks of symptoms (catarrhal stage). Culture is also very specific.
Given the strengths and weakness of the different tests, an acceptable method of laboratory confirmation is to obtain PCR and/or culture within the first 2 weeks of symptoms in all age groups.17-20 Testing after 2 weeks should include a combination of PCR and serology.17 It is essential that the clinical specimen used for PCR or culture testing for pertussis is properly collected. (See “Collecting a swab for pertussis testing” below.21)
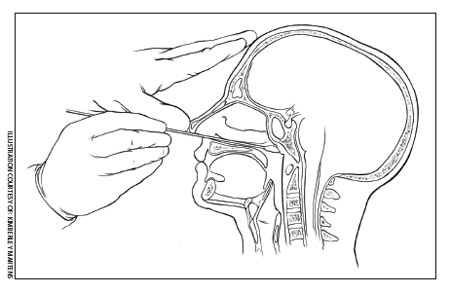
Collecting a swab for pertussis testing
The illustration below shows the correct swab and sampling method. Swab tips may be polyester (such as Dacron or rayon) or they may be nylon-flocked. Cotton-tipped or calcium alginate swabs are not acceptable because the residue will inhibit DNA assays.21 The specimen must be obtained from the posterior nasopharynx and not the nares or oropharynx. The Centers for Disease Control and Prevention offers a video that demonstrates how to properly collect a specimen for testing at http://www.cdc.gov/pertussis/clinical/diagnostic-testing/specimen-collection.html.
Tx is effective when started early
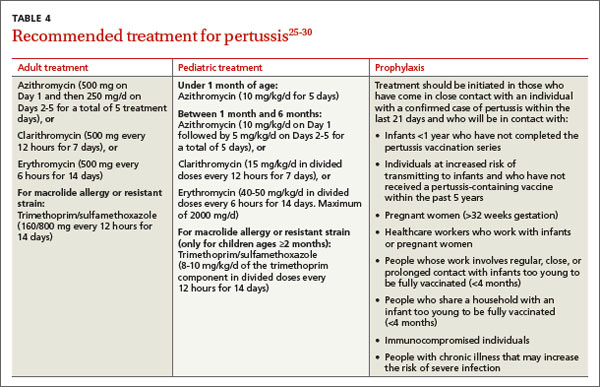
Antibiotics are an effective treatment for pertussis, but they need to be started within the first few weeks of developing symptoms. Studies have not found evidence that antibiotics shorten the duration of pertussis symptoms unless they are given in the catarrhal phase.22,23 It can be challenging to get treatment started during this window, however, because patients may put off seeking care for symptoms they perceive as only minor, such as a cough, until the disease progresses. In addition, physicians may not suspect pertussis in patients who present with a cough they have had for only a short time, and therefore may not test for it.
It may be necessary to rely on clinical suspicion when deciding whether to initiate treatment for pertussis before testing to confirm the diagnosis. For patients in whom clinical suspicion of pertussis is high and who may be in contact with high-risk individuals, it may be acceptable to begin treatment before receiving lab test results.24,25 A recent Cochrane meta-analysis26 recommended initiating treatment to render a patient who has pertussis “noninfectious” but without an expectation of diminishing symptoms.
Limited role for prophylaxis. There is little evidence that prophylactic treatment for pertussis can decrease the spread of the disease. Studies that investigated potential benefits of prophylactic treatment for pertussis have been inconclusive, except for individuals who are in close contact with an infant younger than 6 months of age who has not been fully immunized.27,28