User login
Pharmacist-led clinic boosted hypertension control after discharge
SAN DIEGO – Pharmacist-physician collaboration on hypertension management was effective for controlling blood pressure in patients discharged from an urban ED, results from a pilot study showed.

“Hypertension is the leading risk factor for cardiovascular events and stroke in this country,” Brittany Stewart, RD, PharmD, said at the annual meeting of the American College of Emergency Physicians. “The good news is that we’re not trying to figure out how to treat this disease, but the bad news is that we have 50% of people with uncontrolled high blood pressure.”
“Pharmacists are highly accessible in the community in outpatient settings,” Dr. Stewart of the department of pharmacy practice at Wayne State University, Detroit, said. “This is where ED providers can really integrate and work on a team to refer patients for their chronic diseases on an outpatient basis.”
In a prospective pilot trial, Dr. Stewart and her colleagues recruited 89 patients with uncontrolled hypertension who presented to the ED at Wayne State during May 24, 2017–May 18, 2018. Their average age was 43 years, 51% were male, 94% were black, 51% were current smokers, the mean body mass index was 34.5 kg/m2, and 18% had no health insurance.
“In Detroit, we have significant health disparities with our patient population,” she said. “They are high utilizers of the emergency department, not only for their acute illness but for chronic illness as well. There are several studies showing that team-based care has improved hypertension and blood pressure control. However, the adoption and sustainability of these models haven’t really taken off in our health care landscape yet.”
Over a period of 1.5 years, Dr. Stewart and two physicians developed a transitional care clinic, based on a collaborative practice agreement with emergency physicians. Per protocol, five follow-up visits were planned in an outpatient pharmacy clinic, where Dr. Stewart initiated and titrated antihypertensive medications and handled refills.
“The physician does not have to physically be at the clinic,” she said. “We work closely over the phone to make the best decisions, but it’s not typical ambulatory care where the physician has to be sitting right next to the pharmacist to make the best decisions for the patients.” The primary outcome was the transitional care clinic’s impact on blood pressure.
Dr. Stewart reported results from 47 medication interventions that were provided over 97 follow-up visits. The researchers found that the median blood pressure dropped from an initial reading of 160/102 mm Hg to 130/93 mm Hg by the fifth transitional care clinic visit. Across all patients, systolic blood pressure decreased by an average of 48 mm Hg. “I don’t think we were surprised by these results; we are getting people very much in need down to their blood pressure goals,” she said. “By the end of the study, patients were on an average of three antihypertensive medications.”
She and her colleagues plan to conduct a larger randomized, clinical trial of this care model. The research was supported by a faculty award from the Eugene Applebaum College of Pharmacy and Health Sciences at Wayne State University and by the National Association of Chain Drug Stores Foundation.
Source: Brody A et al. Ann Emerg Med. 2018 Oct;72;4:S36-7. doi. 10.1016/j.annemergmed.2018.08.088.
SAN DIEGO – Pharmacist-physician collaboration on hypertension management was effective for controlling blood pressure in patients discharged from an urban ED, results from a pilot study showed.
“Hypertension is the leading risk factor for cardiovascular events and stroke in this country,” Brittany Stewart, RD, PharmD, said at the annual meeting of the American College of Emergency Physicians. “The good news is that we’re not trying to figure out how to treat this disease, but the bad news is that we have 50% of people with uncontrolled high blood pressure.”
“Pharmacists are highly accessible in the community in outpatient settings,” Dr. Stewart of the department of pharmacy practice at Wayne State University, Detroit, said. “This is where ED providers can really integrate and work on a team to refer patients for their chronic diseases on an outpatient basis.”
In a prospective pilot trial, Dr. Stewart and her colleagues recruited 89 patients with uncontrolled hypertension who presented to the ED at Wayne State during May 24, 2017–May 18, 2018. Their average age was 43 years, 51% were male, 94% were black, 51% were current smokers, the mean body mass index was 34.5 kg/m2, and 18% had no health insurance.
“In Detroit, we have significant health disparities with our patient population,” she said. “They are high utilizers of the emergency department, not only for their acute illness but for chronic illness as well. There are several studies showing that team-based care has improved hypertension and blood pressure control. However, the adoption and sustainability of these models haven’t really taken off in our health care landscape yet.”
Over a period of 1.5 years, Dr. Stewart and two physicians developed a transitional care clinic, based on a collaborative practice agreement with emergency physicians. Per protocol, five follow-up visits were planned in an outpatient pharmacy clinic, where Dr. Stewart initiated and titrated antihypertensive medications and handled refills.
“The physician does not have to physically be at the clinic,” she said. “We work closely over the phone to make the best decisions, but it’s not typical ambulatory care where the physician has to be sitting right next to the pharmacist to make the best decisions for the patients.” The primary outcome was the transitional care clinic’s impact on blood pressure.
Dr. Stewart reported results from 47 medication interventions that were provided over 97 follow-up visits. The researchers found that the median blood pressure dropped from an initial reading of 160/102 mm Hg to 130/93 mm Hg by the fifth transitional care clinic visit. Across all patients, systolic blood pressure decreased by an average of 48 mm Hg. “I don’t think we were surprised by these results; we are getting people very much in need down to their blood pressure goals,” she said. “By the end of the study, patients were on an average of three antihypertensive medications.”
She and her colleagues plan to conduct a larger randomized, clinical trial of this care model. The research was supported by a faculty award from the Eugene Applebaum College of Pharmacy and Health Sciences at Wayne State University and by the National Association of Chain Drug Stores Foundation.
Source: Brody A et al. Ann Emerg Med. 2018 Oct;72;4:S36-7. doi. 10.1016/j.annemergmed.2018.08.088.
SAN DIEGO – Pharmacist-physician collaboration on hypertension management was effective for controlling blood pressure in patients discharged from an urban ED, results from a pilot study showed.
“Hypertension is the leading risk factor for cardiovascular events and stroke in this country,” Brittany Stewart, RD, PharmD, said at the annual meeting of the American College of Emergency Physicians. “The good news is that we’re not trying to figure out how to treat this disease, but the bad news is that we have 50% of people with uncontrolled high blood pressure.”
“Pharmacists are highly accessible in the community in outpatient settings,” Dr. Stewart of the department of pharmacy practice at Wayne State University, Detroit, said. “This is where ED providers can really integrate and work on a team to refer patients for their chronic diseases on an outpatient basis.”
In a prospective pilot trial, Dr. Stewart and her colleagues recruited 89 patients with uncontrolled hypertension who presented to the ED at Wayne State during May 24, 2017–May 18, 2018. Their average age was 43 years, 51% were male, 94% were black, 51% were current smokers, the mean body mass index was 34.5 kg/m2, and 18% had no health insurance.
“In Detroit, we have significant health disparities with our patient population,” she said. “They are high utilizers of the emergency department, not only for their acute illness but for chronic illness as well. There are several studies showing that team-based care has improved hypertension and blood pressure control. However, the adoption and sustainability of these models haven’t really taken off in our health care landscape yet.”
Over a period of 1.5 years, Dr. Stewart and two physicians developed a transitional care clinic, based on a collaborative practice agreement with emergency physicians. Per protocol, five follow-up visits were planned in an outpatient pharmacy clinic, where Dr. Stewart initiated and titrated antihypertensive medications and handled refills.
“The physician does not have to physically be at the clinic,” she said. “We work closely over the phone to make the best decisions, but it’s not typical ambulatory care where the physician has to be sitting right next to the pharmacist to make the best decisions for the patients.” The primary outcome was the transitional care clinic’s impact on blood pressure.
Dr. Stewart reported results from 47 medication interventions that were provided over 97 follow-up visits. The researchers found that the median blood pressure dropped from an initial reading of 160/102 mm Hg to 130/93 mm Hg by the fifth transitional care clinic visit. Across all patients, systolic blood pressure decreased by an average of 48 mm Hg. “I don’t think we were surprised by these results; we are getting people very much in need down to their blood pressure goals,” she said. “By the end of the study, patients were on an average of three antihypertensive medications.”
She and her colleagues plan to conduct a larger randomized, clinical trial of this care model. The research was supported by a faculty award from the Eugene Applebaum College of Pharmacy and Health Sciences at Wayne State University and by the National Association of Chain Drug Stores Foundation.
Source: Brody A et al. Ann Emerg Med. 2018 Oct;72;4:S36-7. doi. 10.1016/j.annemergmed.2018.08.088.
REPORTING FROM ACEP18
Key clinical point: Hypertensive patients discharged from an urban ED benefited from a pharmacist-led clinic.
Major finding: By the last follow-up visit, patients’ mean systolic blood pressure had decreased by 48 mm Hg.
Study details: A pilot study of 89 patients with uncontrolled blood pressure.
Disclosures: The research was supported by a faculty award from the Eugene Applebaum College of Pharmacy and Health Sciences at Wayne State University and by the National Association of Chain Drug Stores Foundation.
Source: Brody A et al. Ann Emerg Med. 2018 Oct;72;4:S36-7. doi. 10.1016/j.annemergmed.2018.08.088.
Ultrasound can’t rule out pulmonary embolism in the ED
SAN DIEGO – In the ICU, ultrasound has been shown to reduce the need for CT to evaluate potential pulmonary embolism. But in the ED, this strategy hasn’t worked out so far, according to Joseph Brown, MD, of the department of emergency medicine at the University of California, San Francisco.

Based on the data so far, the ED patients were less likely than the ICU patients to have another etiology identified on ultrasound that explained their symptoms. Further, ultrasound alone missed small subsegmental pulmonary emboli that were detected on subsequent CT scans in 2 of 11 patients.
The study is continuing, and Dr. Brown explains in this interview how ultrasound might be combined with other risk stratification measures to safely achieve reductions in CT scans.
SAN DIEGO – In the ICU, ultrasound has been shown to reduce the need for CT to evaluate potential pulmonary embolism. But in the ED, this strategy hasn’t worked out so far, according to Joseph Brown, MD, of the department of emergency medicine at the University of California, San Francisco.
Based on the data so far, the ED patients were less likely than the ICU patients to have another etiology identified on ultrasound that explained their symptoms. Further, ultrasound alone missed small subsegmental pulmonary emboli that were detected on subsequent CT scans in 2 of 11 patients.
The study is continuing, and Dr. Brown explains in this interview how ultrasound might be combined with other risk stratification measures to safely achieve reductions in CT scans.
SAN DIEGO – In the ICU, ultrasound has been shown to reduce the need for CT to evaluate potential pulmonary embolism. But in the ED, this strategy hasn’t worked out so far, according to Joseph Brown, MD, of the department of emergency medicine at the University of California, San Francisco.
Based on the data so far, the ED patients were less likely than the ICU patients to have another etiology identified on ultrasound that explained their symptoms. Further, ultrasound alone missed small subsegmental pulmonary emboli that were detected on subsequent CT scans in 2 of 11 patients.
The study is continuing, and Dr. Brown explains in this interview how ultrasound might be combined with other risk stratification measures to safely achieve reductions in CT scans.
REPORTING FROM ACEP18

Syncope alone after age 60 does not require admission
SAN DIEGO – Unless the cause of syncope has been identified after a thorough workup in the emergency department, there is no advantage to admitting patients aged 60 years and older who complain of syncope, an ED-based study has found.
Almost 2,500 patients aged 60 or older with unexplained syncope after a thorough workup had similar 30-day outcomes whether they were admitted to the hospital or sent home from the ED, based on the results of a retrospective study presented at the annual meeting of the American College of Emergency Physicians.
Dr. Marc A. Probst of the Icahn School of Medicine at Mount Sinai, New York, who presented the data, reported that many centers admit older patients with syncope, although the benefit of this practice has not been well established.
In a video interview, Dr. Probst points out how the findings may be useful in guiding clinical decisions or counseling patients when admission is being considered.
SAN DIEGO – Unless the cause of syncope has been identified after a thorough workup in the emergency department, there is no advantage to admitting patients aged 60 years and older who complain of syncope, an ED-based study has found.
Almost 2,500 patients aged 60 or older with unexplained syncope after a thorough workup had similar 30-day outcomes whether they were admitted to the hospital or sent home from the ED, based on the results of a retrospective study presented at the annual meeting of the American College of Emergency Physicians.
Dr. Marc A. Probst of the Icahn School of Medicine at Mount Sinai, New York, who presented the data, reported that many centers admit older patients with syncope, although the benefit of this practice has not been well established.
In a video interview, Dr. Probst points out how the findings may be useful in guiding clinical decisions or counseling patients when admission is being considered.
SAN DIEGO – Unless the cause of syncope has been identified after a thorough workup in the emergency department, there is no advantage to admitting patients aged 60 years and older who complain of syncope, an ED-based study has found.
Almost 2,500 patients aged 60 or older with unexplained syncope after a thorough workup had similar 30-day outcomes whether they were admitted to the hospital or sent home from the ED, based on the results of a retrospective study presented at the annual meeting of the American College of Emergency Physicians.
Dr. Marc A. Probst of the Icahn School of Medicine at Mount Sinai, New York, who presented the data, reported that many centers admit older patients with syncope, although the benefit of this practice has not been well established.
In a video interview, Dr. Probst points out how the findings may be useful in guiding clinical decisions or counseling patients when admission is being considered.
REPORTING FROM ACEP18

Get ready for high-sensitivity troponin tests in the ED
SAN DIEGO – The rule-in cutoff level for high-sensitivity cardiac troponin measures in the diagnosis of acute MI have been established by the European Society of Cardiology, but the value might not be applicable to a U.S. population.
In a video interview at the annual scientific assembly of the American College of Emergency Physicians, Richard M. Nowak, MD, of the department of emergency medicine at Henry Ford Hospital, Detroit, explains why the rule-in cutoff is not likely to apply to American patients and may be associated with a higher risk of false positives.
Since high-sensitivity troponin measures will soon be coming to every ED, each institution may have to arrive at their own rule-in cutoff value in order to diagnose acute MI with an acceptable number of false positives, he said. Dr. Nowak explains how to begin addressing that process.
SAN DIEGO – The rule-in cutoff level for high-sensitivity cardiac troponin measures in the diagnosis of acute MI have been established by the European Society of Cardiology, but the value might not be applicable to a U.S. population.
In a video interview at the annual scientific assembly of the American College of Emergency Physicians, Richard M. Nowak, MD, of the department of emergency medicine at Henry Ford Hospital, Detroit, explains why the rule-in cutoff is not likely to apply to American patients and may be associated with a higher risk of false positives.
Since high-sensitivity troponin measures will soon be coming to every ED, each institution may have to arrive at their own rule-in cutoff value in order to diagnose acute MI with an acceptable number of false positives, he said. Dr. Nowak explains how to begin addressing that process.
SAN DIEGO – The rule-in cutoff level for high-sensitivity cardiac troponin measures in the diagnosis of acute MI have been established by the European Society of Cardiology, but the value might not be applicable to a U.S. population.
In a video interview at the annual scientific assembly of the American College of Emergency Physicians, Richard M. Nowak, MD, of the department of emergency medicine at Henry Ford Hospital, Detroit, explains why the rule-in cutoff is not likely to apply to American patients and may be associated with a higher risk of false positives.
Since high-sensitivity troponin measures will soon be coming to every ED, each institution may have to arrive at their own rule-in cutoff value in order to diagnose acute MI with an acceptable number of false positives, he said. Dr. Nowak explains how to begin addressing that process.
REPORTING FROM ACEP18
Ice pops improved parents’ ratings of ED quality
SAN DIEGO – Simply offering an ice pop to children who are receiving care in an ED boosts satisfaction scores and physician ratings by their children’s parents, according to data presented at the annual meeting of the American College of Emergency Physicians.

Patient experience and subsequently patient satisfaction scores “have become an increasingly important component of health care delivery. ... Does [the act of] administering Popsicles actually make us better clinicians?” asked Ryan Finn, MD, of the Mayo Clinic, Rochester, Minn., who presented these data.
Exploring low-cost ways to improve patient experience and, by extension, patient satisfaction led to this study of an ice pop intervention, Dr. Finn explained. The study design was simple. During a 3-month period, all children under the age of 14 years (mean age, 6 years) who visited the ED on an even numbered date were offered an ice pop. On odd numbered dates, no ice pop was given. There were no other differences in care.
Parent perceptions of care were assessed with the proprietary Press Ganey patient satisfaction survey. Although a completed survey was submitted for less than 5% of the more than 4,500 patients treated during the study period, differences between the groups still reached statistical significance.
When parents were asked to rate physicians on concern for their child’s comfort, 74% of the group given ice pops and 58% of the group given no ice pops gave favorable responses (P less than.05). The parents of children in the ice pop group also were significantly more likely to rate physicians favorably for their courtesy (77% vs. 62%; P less than .04) and for their willingness to take the time to listen (84% vs. 57%; P less than .03).
Overall rating of care (64% vs. 61%) and likelihood of recommending the ED to others (66% vs. 59%) did not approach statistical significance, according to Dr. Finn.
There are numerous potential advantages to improving the patient experience and boosting patient satisfaction in the ED, as is the case in other areas of the hospital. Even if medical care is of high quality, patient satisfaction does not necessarily follow. Although this single-center study had limitations, such as the low survey completion rate, the measurable effects of the ice pop intervention encourages this direction of research.
“Further studies should increase sample size, assess age group subsets, and assess return on investment for this and other low-cost interventions with the potential to alter patient perceptions,” Dr. Finn said. Because patient satisfaction can be reasonably expected to favorably affect quality of care assessments, he indicated that this is a reasonable target for quality improvement strategies.
SAN DIEGO – Simply offering an ice pop to children who are receiving care in an ED boosts satisfaction scores and physician ratings by their children’s parents, according to data presented at the annual meeting of the American College of Emergency Physicians.
Patient experience and subsequently patient satisfaction scores “have become an increasingly important component of health care delivery. ... Does [the act of] administering Popsicles actually make us better clinicians?” asked Ryan Finn, MD, of the Mayo Clinic, Rochester, Minn., who presented these data.
Exploring low-cost ways to improve patient experience and, by extension, patient satisfaction led to this study of an ice pop intervention, Dr. Finn explained. The study design was simple. During a 3-month period, all children under the age of 14 years (mean age, 6 years) who visited the ED on an even numbered date were offered an ice pop. On odd numbered dates, no ice pop was given. There were no other differences in care.
Parent perceptions of care were assessed with the proprietary Press Ganey patient satisfaction survey. Although a completed survey was submitted for less than 5% of the more than 4,500 patients treated during the study period, differences between the groups still reached statistical significance.
When parents were asked to rate physicians on concern for their child’s comfort, 74% of the group given ice pops and 58% of the group given no ice pops gave favorable responses (P less than.05). The parents of children in the ice pop group also were significantly more likely to rate physicians favorably for their courtesy (77% vs. 62%; P less than .04) and for their willingness to take the time to listen (84% vs. 57%; P less than .03).
Overall rating of care (64% vs. 61%) and likelihood of recommending the ED to others (66% vs. 59%) did not approach statistical significance, according to Dr. Finn.
There are numerous potential advantages to improving the patient experience and boosting patient satisfaction in the ED, as is the case in other areas of the hospital. Even if medical care is of high quality, patient satisfaction does not necessarily follow. Although this single-center study had limitations, such as the low survey completion rate, the measurable effects of the ice pop intervention encourages this direction of research.
“Further studies should increase sample size, assess age group subsets, and assess return on investment for this and other low-cost interventions with the potential to alter patient perceptions,” Dr. Finn said. Because patient satisfaction can be reasonably expected to favorably affect quality of care assessments, he indicated that this is a reasonable target for quality improvement strategies.
SAN DIEGO – Simply offering an ice pop to children who are receiving care in an ED boosts satisfaction scores and physician ratings by their children’s parents, according to data presented at the annual meeting of the American College of Emergency Physicians.
Patient experience and subsequently patient satisfaction scores “have become an increasingly important component of health care delivery. ... Does [the act of] administering Popsicles actually make us better clinicians?” asked Ryan Finn, MD, of the Mayo Clinic, Rochester, Minn., who presented these data.
Exploring low-cost ways to improve patient experience and, by extension, patient satisfaction led to this study of an ice pop intervention, Dr. Finn explained. The study design was simple. During a 3-month period, all children under the age of 14 years (mean age, 6 years) who visited the ED on an even numbered date were offered an ice pop. On odd numbered dates, no ice pop was given. There were no other differences in care.
Parent perceptions of care were assessed with the proprietary Press Ganey patient satisfaction survey. Although a completed survey was submitted for less than 5% of the more than 4,500 patients treated during the study period, differences between the groups still reached statistical significance.
When parents were asked to rate physicians on concern for their child’s comfort, 74% of the group given ice pops and 58% of the group given no ice pops gave favorable responses (P less than.05). The parents of children in the ice pop group also were significantly more likely to rate physicians favorably for their courtesy (77% vs. 62%; P less than .04) and for their willingness to take the time to listen (84% vs. 57%; P less than .03).
Overall rating of care (64% vs. 61%) and likelihood of recommending the ED to others (66% vs. 59%) did not approach statistical significance, according to Dr. Finn.
There are numerous potential advantages to improving the patient experience and boosting patient satisfaction in the ED, as is the case in other areas of the hospital. Even if medical care is of high quality, patient satisfaction does not necessarily follow. Although this single-center study had limitations, such as the low survey completion rate, the measurable effects of the ice pop intervention encourages this direction of research.
“Further studies should increase sample size, assess age group subsets, and assess return on investment for this and other low-cost interventions with the potential to alter patient perceptions,” Dr. Finn said. Because patient satisfaction can be reasonably expected to favorably affect quality of care assessments, he indicated that this is a reasonable target for quality improvement strategies.
FROM ACEP18
Key clinical point: Providing an ice pop to children in the ED boosted satisfaction scores.
Major finding: The parents of children given ice pops ranked physicians higher on measures of courtesy and concern.
Study details: Prospective, controlled study of survey results completed by 5% of more than 4,500 patients.
Disclosures: Dr. Finn reported no financial relationships relevant to this study.
How to manage difficult dislocations
SAN DIEGO – Being prepared to manage difficult dislocations is key to maintaining the flow of patient care in any emergency department.
In a video interview at the annual meeting of the American College of Emergency Physicians, Danielle D. Campagne, MD, FACEP, shared her clinical pearls for managing dislocations of the jaw, hip, ankle, and shoulder.
Dr. Campagne is an emergency medicine physician who practices at Community Regional Medical Center in Fresno, Calif. She is also vice chief of emergency medicine at University of California, San Francisco, Fresno. She reported having no financial disclosures.
SAN DIEGO – Being prepared to manage difficult dislocations is key to maintaining the flow of patient care in any emergency department.
In a video interview at the annual meeting of the American College of Emergency Physicians, Danielle D. Campagne, MD, FACEP, shared her clinical pearls for managing dislocations of the jaw, hip, ankle, and shoulder.
Dr. Campagne is an emergency medicine physician who practices at Community Regional Medical Center in Fresno, Calif. She is also vice chief of emergency medicine at University of California, San Francisco, Fresno. She reported having no financial disclosures.
SAN DIEGO – Being prepared to manage difficult dislocations is key to maintaining the flow of patient care in any emergency department.
In a video interview at the annual meeting of the American College of Emergency Physicians, Danielle D. Campagne, MD, FACEP, shared her clinical pearls for managing dislocations of the jaw, hip, ankle, and shoulder.
Dr. Campagne is an emergency medicine physician who practices at Community Regional Medical Center in Fresno, Calif. She is also vice chief of emergency medicine at University of California, San Francisco, Fresno. She reported having no financial disclosures.
REPORTING FROM ACEP18

Five “can’t miss” oncologic emergencies
SAN DIEGO – Acute promyelocytic leukemia is one of five “can’t miss” oncologic emergencies, Megan Boysen Osborn, MD, MHPE, told a standing-room-only crowd at the annual meeting of the American College of Emergency Physicians.
In our exclusive video interview, Dr. Osborn, vice chair of education and the residency program director in the department of emergency medicine at the University of California, Irvine, offered tips on how to recognize acute promyelocytic leukemia, leukostasis, neutropenic fever, tumor lysis syndrome, and disseminated intravascular coagulation.
“All patients with suspected leukemias should be admitted,” she said. “Time is of the essence.”
Dr. Osborn reported having no financial disclosures related to her presentation.
SAN DIEGO – Acute promyelocytic leukemia is one of five “can’t miss” oncologic emergencies, Megan Boysen Osborn, MD, MHPE, told a standing-room-only crowd at the annual meeting of the American College of Emergency Physicians.
In our exclusive video interview, Dr. Osborn, vice chair of education and the residency program director in the department of emergency medicine at the University of California, Irvine, offered tips on how to recognize acute promyelocytic leukemia, leukostasis, neutropenic fever, tumor lysis syndrome, and disseminated intravascular coagulation.
“All patients with suspected leukemias should be admitted,” she said. “Time is of the essence.”
Dr. Osborn reported having no financial disclosures related to her presentation.
SAN DIEGO – Acute promyelocytic leukemia is one of five “can’t miss” oncologic emergencies, Megan Boysen Osborn, MD, MHPE, told a standing-room-only crowd at the annual meeting of the American College of Emergency Physicians.
In our exclusive video interview, Dr. Osborn, vice chair of education and the residency program director in the department of emergency medicine at the University of California, Irvine, offered tips on how to recognize acute promyelocytic leukemia, leukostasis, neutropenic fever, tumor lysis syndrome, and disseminated intravascular coagulation.
“All patients with suspected leukemias should be admitted,” she said. “Time is of the essence.”
Dr. Osborn reported having no financial disclosures related to her presentation.
REPORTING FROM ACEP18

Physical assaults in the emergency department on the rise, survey finds

Those are key findings from an email-based survey administered to ACEP members in August of 2018.
“The results are quite troubling,” Vidor E. Friedman, MD, FACEP, president of ACEP, said during a press briefing at the group’s annual meeting. “Emergency physicians are reporting that violence in emergency departments is increasing and that it’s harming not only physicians and nurses, but also patients and the care that’s being provided to them.”
Dr. Friedman, who practices emergency medicine in Maitland, Fla., recalled one afternoon shift when police brought in a drunk man they had cited for vagrancy after finding him in a ditch by the roadside. It was the man’s first day out of jail in 10 years. “He was a pretty intimidating looking guy,” Dr. Friedman said. “He threatened me and he threatened the staff, so we appropriately restrained him, which only increased his agitation. The fourth time he said he was going to kill me, he told me he was going to put an ice pick in my heart. When his buddies came to pick him up, I had the police escort him to the city limits, and I didn’t sleep at home for a week. This is the kind of thing that health care workers are exposed to on a fairly regular basis.”
The ACEP survey found that emergency physicians across all demographics experience various forms of violence and are increasingly concerned about violence in the ED. “We know that there is gross underreporting of [violence in the ED],” said Terry Kowalenko, MD, FACEP, chair of emergency medicine at Oakland University William Beaumont School of Medicine, Rochester, Mich., and coauthor of a new study that assessed violence against emergency physicians in that state. “Some studies have shown it to be under 50%. The other thing is, it’s very difficult to predict who the perpetrator will be, or who the victim will be. We did find that the time you spend with the patient certainly increases your chances of violence perpetrated against you. Clearly, there are consequences to the victim, the perpetrator, the institution, and potentially, other patients.”
According to Dr. Kowalenko’s own research, 72% of emergency medicine physicians in Michigan reported experiencing violence in the past year. In 2018, an increasing proportion of that state’s emergency physicians reported feeling “constantly fearful” of becoming a victim of violence (8.1% vs. 1.2% in 2005), with 22% reporting feeling frequently fearful (up from 9.4% in 2005).
For the ACEP-sponsored survey, on Aug. 21, 2018, Alexandria, Va.–based Marketing General sent an email to 31,389 ACEP members, inviting them to answer 22 questions in an effort to understand emergency physicians’ views on the level, type, frequency, and impact of violence experienced in the ED. By the time polling closed 6 days later, 3,539 surveys were completed, for a response rate of about 11%. Clinicians in California led the way with 8% of total responses, followed by those in Texas (7%), New York (7%), Florida (5%), Pennsylvania (5%), and Ohio (5%). Nearly two-thirds of respondents (71%) were male, and 25% work for emergency departments with annual patient volumes between 50,001 and 75,000, while another 39% work for departments with even higher volumes.
Nearly half of respondents (47%) reported being physically assaulted while at work in the ED, while 71% have witnessed an assault. Only 10% have experienced neither. The majority of assaults were committed by patients (97%), but 28% involved a patient’s family member or friend. The most common form of assault was a hit or a slap (44%), while other frequent forms of violence included being spit on (30%), punched (28%), or kicked (27%).
Among those who have been physically assaulted, 48% reported that at least half of all assaults were committed by people believed to be seeking drugs or who were under the influence of drugs or alcohol, while 41% said that more than half of assaults were committed by psychiatric patients.
“Our emergency departments are kind of a microcosm of all the challenges that we face today in society: gang violence, gun violence, domestic violence, and psychiatric illnesses [for which] we have a shortage of beds,” said Leigh Vinocur, MD, FACEP, former chair of ACEP’s Emergency Department Violence Committee. “Then there is the opioid crisis.” She added that being in an emergency department can be “an emotionally volatile experience for people from all walks of life. People come in hurt. They’re at their worst; they’re frightened, they’re vulnerable and stressed.”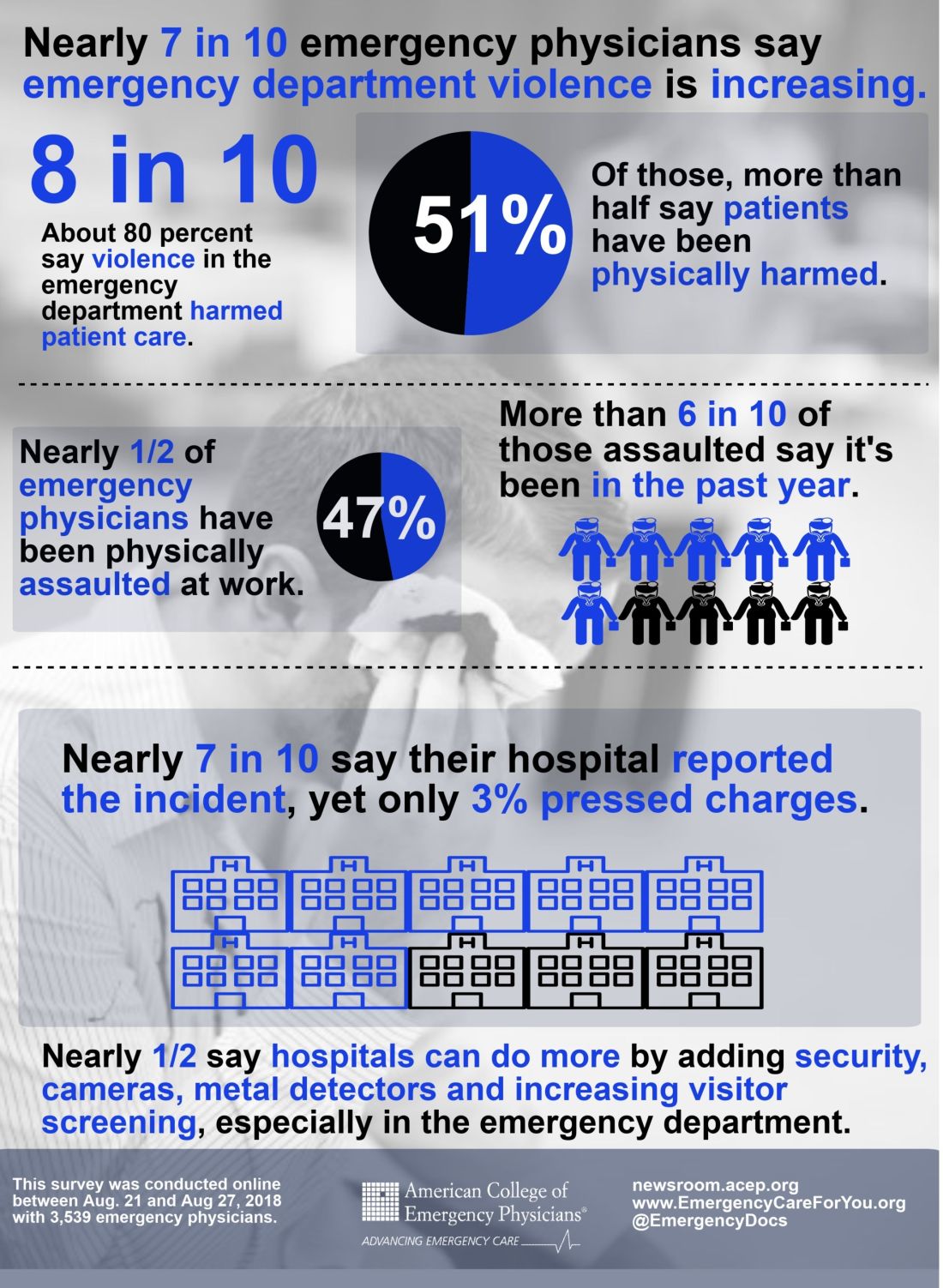
More than three-quarters of ACEP survey respondents (77%) believe that violence in the ED has harmed patient care, primarily by loss of productivity (81%), emotional trauma (81%), increased wait times (80%), and less focus from emergency staff or physicians (76%). In addition, 49% ranked “increase security” as the most important step hospitals can take to increase ED safety, while the top three contributing factors to violence in the ED were no adequate punitive consequence or response toward the attacker (34%), behavioral health patients (32%), and absence of adequate protective mechanisms for physicians/staff (15%).
When asked how the hospital administration or hospital security responded to the assault, 28% said that the hospital or nursing staff put a behavioral flag in the patient’s medical chart, while 21% said that hospital security arrested the patient for the assault or enlisted law enforcement to arrest the patient.
Finally, nearly half of respondents indicated that hospitals could do more by adding security cameras, metal detectors, and increasing visitor screening. “Obviously this is site-specific,” Dr. Friedman said. “We’re not saying that every emergency department in America needs to have a metal detector out front, but this needs to be something that institutions take seriously, to protect both patients and the providers that work there.”
dbrunk@mdedge.com
Those are key findings from an email-based survey administered to ACEP members in August of 2018.
“The results are quite troubling,” Vidor E. Friedman, MD, FACEP, president of ACEP, said during a press briefing at the group’s annual meeting. “Emergency physicians are reporting that violence in emergency departments is increasing and that it’s harming not only physicians and nurses, but also patients and the care that’s being provided to them.”
Dr. Friedman, who practices emergency medicine in Maitland, Fla., recalled one afternoon shift when police brought in a drunk man they had cited for vagrancy after finding him in a ditch by the roadside. It was the man’s first day out of jail in 10 years. “He was a pretty intimidating looking guy,” Dr. Friedman said. “He threatened me and he threatened the staff, so we appropriately restrained him, which only increased his agitation. The fourth time he said he was going to kill me, he told me he was going to put an ice pick in my heart. When his buddies came to pick him up, I had the police escort him to the city limits, and I didn’t sleep at home for a week. This is the kind of thing that health care workers are exposed to on a fairly regular basis.”
The ACEP survey found that emergency physicians across all demographics experience various forms of violence and are increasingly concerned about violence in the ED. “We know that there is gross underreporting of [violence in the ED],” said Terry Kowalenko, MD, FACEP, chair of emergency medicine at Oakland University William Beaumont School of Medicine, Rochester, Mich., and coauthor of a new study that assessed violence against emergency physicians in that state. “Some studies have shown it to be under 50%. The other thing is, it’s very difficult to predict who the perpetrator will be, or who the victim will be. We did find that the time you spend with the patient certainly increases your chances of violence perpetrated against you. Clearly, there are consequences to the victim, the perpetrator, the institution, and potentially, other patients.”
According to Dr. Kowalenko’s own research, 72% of emergency medicine physicians in Michigan reported experiencing violence in the past year. In 2018, an increasing proportion of that state’s emergency physicians reported feeling “constantly fearful” of becoming a victim of violence (8.1% vs. 1.2% in 2005), with 22% reporting feeling frequently fearful (up from 9.4% in 2005).
For the ACEP-sponsored survey, on Aug. 21, 2018, Alexandria, Va.–based Marketing General sent an email to 31,389 ACEP members, inviting them to answer 22 questions in an effort to understand emergency physicians’ views on the level, type, frequency, and impact of violence experienced in the ED. By the time polling closed 6 days later, 3,539 surveys were completed, for a response rate of about 11%. Clinicians in California led the way with 8% of total responses, followed by those in Texas (7%), New York (7%), Florida (5%), Pennsylvania (5%), and Ohio (5%). Nearly two-thirds of respondents (71%) were male, and 25% work for emergency departments with annual patient volumes between 50,001 and 75,000, while another 39% work for departments with even higher volumes.
Nearly half of respondents (47%) reported being physically assaulted while at work in the ED, while 71% have witnessed an assault. Only 10% have experienced neither. The majority of assaults were committed by patients (97%), but 28% involved a patient’s family member or friend. The most common form of assault was a hit or a slap (44%), while other frequent forms of violence included being spit on (30%), punched (28%), or kicked (27%).
Among those who have been physically assaulted, 48% reported that at least half of all assaults were committed by people believed to be seeking drugs or who were under the influence of drugs or alcohol, while 41% said that more than half of assaults were committed by psychiatric patients.
“Our emergency departments are kind of a microcosm of all the challenges that we face today in society: gang violence, gun violence, domestic violence, and psychiatric illnesses [for which] we have a shortage of beds,” said Leigh Vinocur, MD, FACEP, former chair of ACEP’s Emergency Department Violence Committee. “Then there is the opioid crisis.” She added that being in an emergency department can be “an emotionally volatile experience for people from all walks of life. People come in hurt. They’re at their worst; they’re frightened, they’re vulnerable and stressed.”
More than three-quarters of ACEP survey respondents (77%) believe that violence in the ED has harmed patient care, primarily by loss of productivity (81%), emotional trauma (81%), increased wait times (80%), and less focus from emergency staff or physicians (76%). In addition, 49% ranked “increase security” as the most important step hospitals can take to increase ED safety, while the top three contributing factors to violence in the ED were no adequate punitive consequence or response toward the attacker (34%), behavioral health patients (32%), and absence of adequate protective mechanisms for physicians/staff (15%).
When asked how the hospital administration or hospital security responded to the assault, 28% said that the hospital or nursing staff put a behavioral flag in the patient’s medical chart, while 21% said that hospital security arrested the patient for the assault or enlisted law enforcement to arrest the patient.
Finally, nearly half of respondents indicated that hospitals could do more by adding security cameras, metal detectors, and increasing visitor screening. “Obviously this is site-specific,” Dr. Friedman said. “We’re not saying that every emergency department in America needs to have a metal detector out front, but this needs to be something that institutions take seriously, to protect both patients and the providers that work there.”
dbrunk@mdedge.com
Those are key findings from an email-based survey administered to ACEP members in August of 2018.
“The results are quite troubling,” Vidor E. Friedman, MD, FACEP, president of ACEP, said during a press briefing at the group’s annual meeting. “Emergency physicians are reporting that violence in emergency departments is increasing and that it’s harming not only physicians and nurses, but also patients and the care that’s being provided to them.”
Dr. Friedman, who practices emergency medicine in Maitland, Fla., recalled one afternoon shift when police brought in a drunk man they had cited for vagrancy after finding him in a ditch by the roadside. It was the man’s first day out of jail in 10 years. “He was a pretty intimidating looking guy,” Dr. Friedman said. “He threatened me and he threatened the staff, so we appropriately restrained him, which only increased his agitation. The fourth time he said he was going to kill me, he told me he was going to put an ice pick in my heart. When his buddies came to pick him up, I had the police escort him to the city limits, and I didn’t sleep at home for a week. This is the kind of thing that health care workers are exposed to on a fairly regular basis.”
The ACEP survey found that emergency physicians across all demographics experience various forms of violence and are increasingly concerned about violence in the ED. “We know that there is gross underreporting of [violence in the ED],” said Terry Kowalenko, MD, FACEP, chair of emergency medicine at Oakland University William Beaumont School of Medicine, Rochester, Mich., and coauthor of a new study that assessed violence against emergency physicians in that state. “Some studies have shown it to be under 50%. The other thing is, it’s very difficult to predict who the perpetrator will be, or who the victim will be. We did find that the time you spend with the patient certainly increases your chances of violence perpetrated against you. Clearly, there are consequences to the victim, the perpetrator, the institution, and potentially, other patients.”
According to Dr. Kowalenko’s own research, 72% of emergency medicine physicians in Michigan reported experiencing violence in the past year. In 2018, an increasing proportion of that state’s emergency physicians reported feeling “constantly fearful” of becoming a victim of violence (8.1% vs. 1.2% in 2005), with 22% reporting feeling frequently fearful (up from 9.4% in 2005).
For the ACEP-sponsored survey, on Aug. 21, 2018, Alexandria, Va.–based Marketing General sent an email to 31,389 ACEP members, inviting them to answer 22 questions in an effort to understand emergency physicians’ views on the level, type, frequency, and impact of violence experienced in the ED. By the time polling closed 6 days later, 3,539 surveys were completed, for a response rate of about 11%. Clinicians in California led the way with 8% of total responses, followed by those in Texas (7%), New York (7%), Florida (5%), Pennsylvania (5%), and Ohio (5%). Nearly two-thirds of respondents (71%) were male, and 25% work for emergency departments with annual patient volumes between 50,001 and 75,000, while another 39% work for departments with even higher volumes.
Nearly half of respondents (47%) reported being physically assaulted while at work in the ED, while 71% have witnessed an assault. Only 10% have experienced neither. The majority of assaults were committed by patients (97%), but 28% involved a patient’s family member or friend. The most common form of assault was a hit or a slap (44%), while other frequent forms of violence included being spit on (30%), punched (28%), or kicked (27%).
Among those who have been physically assaulted, 48% reported that at least half of all assaults were committed by people believed to be seeking drugs or who were under the influence of drugs or alcohol, while 41% said that more than half of assaults were committed by psychiatric patients.
“Our emergency departments are kind of a microcosm of all the challenges that we face today in society: gang violence, gun violence, domestic violence, and psychiatric illnesses [for which] we have a shortage of beds,” said Leigh Vinocur, MD, FACEP, former chair of ACEP’s Emergency Department Violence Committee. “Then there is the opioid crisis.” She added that being in an emergency department can be “an emotionally volatile experience for people from all walks of life. People come in hurt. They’re at their worst; they’re frightened, they’re vulnerable and stressed.”
More than three-quarters of ACEP survey respondents (77%) believe that violence in the ED has harmed patient care, primarily by loss of productivity (81%), emotional trauma (81%), increased wait times (80%), and less focus from emergency staff or physicians (76%). In addition, 49% ranked “increase security” as the most important step hospitals can take to increase ED safety, while the top three contributing factors to violence in the ED were no adequate punitive consequence or response toward the attacker (34%), behavioral health patients (32%), and absence of adequate protective mechanisms for physicians/staff (15%).
When asked how the hospital administration or hospital security responded to the assault, 28% said that the hospital or nursing staff put a behavioral flag in the patient’s medical chart, while 21% said that hospital security arrested the patient for the assault or enlisted law enforcement to arrest the patient.
Finally, nearly half of respondents indicated that hospitals could do more by adding security cameras, metal detectors, and increasing visitor screening. “Obviously this is site-specific,” Dr. Friedman said. “We’re not saying that every emergency department in America needs to have a metal detector out front, but this needs to be something that institutions take seriously, to protect both patients and the providers that work there.”
dbrunk@mdedge.com
AT ACEP18
Ketamine beats midazolam for agitation control
SAN DIEGO – Following in the wake of a previous prospective comparison of ketamine and haloperidol for control of severe prehospital agitation, a new prospective study by the same group and presented at the annual meeting of the American College of Emergency Physicians found ketamine superior to midazolam for the same indication.
“The difference between the two drugs was larger when agitation was more profound,” reported Jon B. Cole, MD, an emergency medicine physician at Hennepin Healthcare and associate professor of emergency medicine at the University of Minnesota, Minneapolis.
Relative to ketamine (Ketalar), midazolam (Versed) was associated with fewer side effects, “so for less agitated patients, midazolam may still be the preferred therapy,” he added in his late-breaker presentation.
In recent years, ketamine has become a popular drug in emergency medical services for control of agitation, according to Dr. Cole, but he said that this approach has been adopted with relatively limited support from objective evidence. In his literature search, only 2 of 11 original studies that addressed ketamine for agitation involved prospective comparative studies.
One of those prior prospective studies was one Dr. Cole led and published 2 years ago (Clin Toxicol. 2016;54:556-62). In that study, comparing 5 mg/kg of intramuscular (IM) ketamine to 10 mg IM haloperidol, ketamine had a faster onset (median 5 vs. 17 minutes) but produced more side effects, including higher rates of intubation (39% vs. 4%).
In the new prospective study, ketamine and midazolam were compared over separate consecutive 6-month periods in which ketamine and then midazolam were employed as the dominant strategy for agitation control. This was the same open-label, nonrandomized design used for the comparison of ketamine and haloperidol, but with one difference. When the Altered Mental Status Score was +2 or +3, considered severe agitation, patients received 3 mg/kg of IM ketamine or 5 mg of IM midazolam. When the AMS score was +4, called profound agitation, the doses were 5 mg/kg and 15 mg, respectively.
The primary result was that adequate sedation overall was achieved in a median 4.3 minutes on ketamine but 8.8 minutes on midazolam, producing a more than 3-minute advantage for ketamine, which translated into an odds ratio (OR) of 1.8 for adequate agitation control favoring ketamine, according to Dr. Cole. In those with severe agitation, the median advantage was less than 2 minutes, but the OR of 1.6 remained significant. In those with profound agitation, the mean difference climbed above 5 minutes with an OR of 2.5.
but Dr. Cole did report that midazolam was better tolerated. On the lower doses of the two drugs, for example, adverse events that were more common on ketamine than midazolam included vomiting (7% vs. 1%) and hypersalivation (20% vs. 0%).
In addition to the nonrandomized design, one limitation was unequal numbers of patients in the comparative groups. Only 113 were treated with midazolam while 202 patients were treated with ketamine. The reason was that the study of these drugs, which had been in widespread use at Dr. Cole’s institution, was conducted without asking patients to agree to participate. When negative stories in local papers framed this as a study conducted without consent, the institution asked the investigators to halt the study, and they complied.
“Subsequently, we have been assured after multiple evaluations that the rights and safety of our patient population were never violated,” Dr. Cole said, but he acknowledged that closing the study was an appropriate step in order to preserve patient confidence. “What we learned from this experience is that we may need to reconsider how we do waive of consent research at our institution,” he added.
In the meantime, the comparisons of ketamine with haloperidol and midazolam have provided objective evidence of their relative efficacy and safety in the management of prehospital agitation.
Dr. Cole reported no conflicts of interest.
SOURCE: Ann Emerg Med. 2018 Oct. doi. org/10.1016/j.annemergmed.2018.08.007.
SAN DIEGO – Following in the wake of a previous prospective comparison of ketamine and haloperidol for control of severe prehospital agitation, a new prospective study by the same group and presented at the annual meeting of the American College of Emergency Physicians found ketamine superior to midazolam for the same indication.
“The difference between the two drugs was larger when agitation was more profound,” reported Jon B. Cole, MD, an emergency medicine physician at Hennepin Healthcare and associate professor of emergency medicine at the University of Minnesota, Minneapolis.
Relative to ketamine (Ketalar), midazolam (Versed) was associated with fewer side effects, “so for less agitated patients, midazolam may still be the preferred therapy,” he added in his late-breaker presentation.
In recent years, ketamine has become a popular drug in emergency medical services for control of agitation, according to Dr. Cole, but he said that this approach has been adopted with relatively limited support from objective evidence. In his literature search, only 2 of 11 original studies that addressed ketamine for agitation involved prospective comparative studies.
One of those prior prospective studies was one Dr. Cole led and published 2 years ago (Clin Toxicol. 2016;54:556-62). In that study, comparing 5 mg/kg of intramuscular (IM) ketamine to 10 mg IM haloperidol, ketamine had a faster onset (median 5 vs. 17 minutes) but produced more side effects, including higher rates of intubation (39% vs. 4%).
In the new prospective study, ketamine and midazolam were compared over separate consecutive 6-month periods in which ketamine and then midazolam were employed as the dominant strategy for agitation control. This was the same open-label, nonrandomized design used for the comparison of ketamine and haloperidol, but with one difference. When the Altered Mental Status Score was +2 or +3, considered severe agitation, patients received 3 mg/kg of IM ketamine or 5 mg of IM midazolam. When the AMS score was +4, called profound agitation, the doses were 5 mg/kg and 15 mg, respectively.
The primary result was that adequate sedation overall was achieved in a median 4.3 minutes on ketamine but 8.8 minutes on midazolam, producing a more than 3-minute advantage for ketamine, which translated into an odds ratio (OR) of 1.8 for adequate agitation control favoring ketamine, according to Dr. Cole. In those with severe agitation, the median advantage was less than 2 minutes, but the OR of 1.6 remained significant. In those with profound agitation, the mean difference climbed above 5 minutes with an OR of 2.5.
but Dr. Cole did report that midazolam was better tolerated. On the lower doses of the two drugs, for example, adverse events that were more common on ketamine than midazolam included vomiting (7% vs. 1%) and hypersalivation (20% vs. 0%).
In addition to the nonrandomized design, one limitation was unequal numbers of patients in the comparative groups. Only 113 were treated with midazolam while 202 patients were treated with ketamine. The reason was that the study of these drugs, which had been in widespread use at Dr. Cole’s institution, was conducted without asking patients to agree to participate. When negative stories in local papers framed this as a study conducted without consent, the institution asked the investigators to halt the study, and they complied.
“Subsequently, we have been assured after multiple evaluations that the rights and safety of our patient population were never violated,” Dr. Cole said, but he acknowledged that closing the study was an appropriate step in order to preserve patient confidence. “What we learned from this experience is that we may need to reconsider how we do waive of consent research at our institution,” he added.
In the meantime, the comparisons of ketamine with haloperidol and midazolam have provided objective evidence of their relative efficacy and safety in the management of prehospital agitation.
Dr. Cole reported no conflicts of interest.
SOURCE: Ann Emerg Med. 2018 Oct. doi. org/10.1016/j.annemergmed.2018.08.007.
SAN DIEGO – Following in the wake of a previous prospective comparison of ketamine and haloperidol for control of severe prehospital agitation, a new prospective study by the same group and presented at the annual meeting of the American College of Emergency Physicians found ketamine superior to midazolam for the same indication.
“The difference between the two drugs was larger when agitation was more profound,” reported Jon B. Cole, MD, an emergency medicine physician at Hennepin Healthcare and associate professor of emergency medicine at the University of Minnesota, Minneapolis.
Relative to ketamine (Ketalar), midazolam (Versed) was associated with fewer side effects, “so for less agitated patients, midazolam may still be the preferred therapy,” he added in his late-breaker presentation.
In recent years, ketamine has become a popular drug in emergency medical services for control of agitation, according to Dr. Cole, but he said that this approach has been adopted with relatively limited support from objective evidence. In his literature search, only 2 of 11 original studies that addressed ketamine for agitation involved prospective comparative studies.
One of those prior prospective studies was one Dr. Cole led and published 2 years ago (Clin Toxicol. 2016;54:556-62). In that study, comparing 5 mg/kg of intramuscular (IM) ketamine to 10 mg IM haloperidol, ketamine had a faster onset (median 5 vs. 17 minutes) but produced more side effects, including higher rates of intubation (39% vs. 4%).
In the new prospective study, ketamine and midazolam were compared over separate consecutive 6-month periods in which ketamine and then midazolam were employed as the dominant strategy for agitation control. This was the same open-label, nonrandomized design used for the comparison of ketamine and haloperidol, but with one difference. When the Altered Mental Status Score was +2 or +3, considered severe agitation, patients received 3 mg/kg of IM ketamine or 5 mg of IM midazolam. When the AMS score was +4, called profound agitation, the doses were 5 mg/kg and 15 mg, respectively.
The primary result was that adequate sedation overall was achieved in a median 4.3 minutes on ketamine but 8.8 minutes on midazolam, producing a more than 3-minute advantage for ketamine, which translated into an odds ratio (OR) of 1.8 for adequate agitation control favoring ketamine, according to Dr. Cole. In those with severe agitation, the median advantage was less than 2 minutes, but the OR of 1.6 remained significant. In those with profound agitation, the mean difference climbed above 5 minutes with an OR of 2.5.
but Dr. Cole did report that midazolam was better tolerated. On the lower doses of the two drugs, for example, adverse events that were more common on ketamine than midazolam included vomiting (7% vs. 1%) and hypersalivation (20% vs. 0%).
In addition to the nonrandomized design, one limitation was unequal numbers of patients in the comparative groups. Only 113 were treated with midazolam while 202 patients were treated with ketamine. The reason was that the study of these drugs, which had been in widespread use at Dr. Cole’s institution, was conducted without asking patients to agree to participate. When negative stories in local papers framed this as a study conducted without consent, the institution asked the investigators to halt the study, and they complied.
“Subsequently, we have been assured after multiple evaluations that the rights and safety of our patient population were never violated,” Dr. Cole said, but he acknowledged that closing the study was an appropriate step in order to preserve patient confidence. “What we learned from this experience is that we may need to reconsider how we do waive of consent research at our institution,” he added.
In the meantime, the comparisons of ketamine with haloperidol and midazolam have provided objective evidence of their relative efficacy and safety in the management of prehospital agitation.
Dr. Cole reported no conflicts of interest.
SOURCE: Ann Emerg Med. 2018 Oct. doi. org/10.1016/j.annemergmed.2018.08.007.
REPORTING FROM ACEP2018
Key clinical point: In severe agitation involving violent or threatening behavior, ketamine sedates patients more quickly than midazolam.
Major finding: Because of a 3-minute faster onset, ketamine was associated with a 1.8 greater odds ratio than midazolam for adequate sedation control.
Study details: Prospective open-label nonrandomized study.
Disclosures: Dr. Cole reported no conflicts of interest.
Source: Ann Emerg Med. 2018 Oct. doi. org/10.1016/j.annemergmed.2018.08.007.
Previous psychiatric admissions predict suicide attempts
SAN DIEGO – Among patients presenting to the emergency department with suicidal ideation, the number of previous psychiatric admissions is the most important predictor of a subsequent suicide attempt, results from a 2-year-long study showed.

Momentary measures – significant current difficulties with sleep, energy, or appetite, and anhedonia – “are important considerations during suicide risk assessment, regardless of whether the patient meets the threshold for major depressive disorder, lead study author Anne C. Knorr said in an interview in advance of the annual meeting of the American College of Emergency Physicians.
“Many traditionally studied psychiatric risk factors do not significantly differ between individuals who think about suicide and those who act on their suicidal thoughts, an important distinction as only one-third of those who think about suicide carry out a suicide attempt. While there is support for some psychiatric factors – for example, anxiety, substance use disorders, sleep disturbance – being useful in differentiating these groups, the current study is unique in its use of a longitudinal design to identify influential risk factors that predict future suicide attempt among those with suicidal ideation,” she said.
Ms. Knorr, a research project manager at Geisinger Medical Center, Danville, Pa., and her colleagues collected electronic medical record data from 908 patients who had received a psychiatric evaluation at an index emergency department visit for suicidal ideation over a 2-year period. The mean age of patients was 39 years. The target sample was 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
The researchers analyzed 32 predictor variables from patient charts, including demographics, psychiatric history, and current psychiatric presentation. The evaluation was done with “a machine learning statistical approach which is more capable than traditional statistical approaches in handling a large number of predictor variables,” Ms. Knorr said.
The number of previous psychiatric admissions was the most important predictor of a subsequent suicide attempt. The next nine most important variables were sleep disturbance, history of family suicide, low energy, patient age, psychiatrist determination of severe suicide risk, psychiatrist determination of moderate suicide risk, appetite issues, presence of a support system, and loss of interest/pleasure.
These symptoms may not typically be weighed heavily in risk assessments, Ms. Knorr said. “Additionally, given that research suggests that the clinical determination of suicide risk is historically poor, it was interesting that psychiatrist determination of moderate or high risk was influential in predicting a return visit for suicide attempt. Finally, we were surprised that a past history of suicide attempt, often viewed as the strongest predictor of a future suicide attempt, did not emerge as one of the top 10 influential predictors.
“Limitations of this study include the use of a return visit to a Geisinger emergency department as the only measure of a future suicide attempt and the utilization of data from only one health system,” she noted.
The study was funded by the Geisinger Clinic Research Fund. One of the coauthors, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
SOURCE: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23. doi. 10.1016/j.annemergmed.2018.08.055.
SAN DIEGO – Among patients presenting to the emergency department with suicidal ideation, the number of previous psychiatric admissions is the most important predictor of a subsequent suicide attempt, results from a 2-year-long study showed.
Momentary measures – significant current difficulties with sleep, energy, or appetite, and anhedonia – “are important considerations during suicide risk assessment, regardless of whether the patient meets the threshold for major depressive disorder, lead study author Anne C. Knorr said in an interview in advance of the annual meeting of the American College of Emergency Physicians.
“Many traditionally studied psychiatric risk factors do not significantly differ between individuals who think about suicide and those who act on their suicidal thoughts, an important distinction as only one-third of those who think about suicide carry out a suicide attempt. While there is support for some psychiatric factors – for example, anxiety, substance use disorders, sleep disturbance – being useful in differentiating these groups, the current study is unique in its use of a longitudinal design to identify influential risk factors that predict future suicide attempt among those with suicidal ideation,” she said.
Ms. Knorr, a research project manager at Geisinger Medical Center, Danville, Pa., and her colleagues collected electronic medical record data from 908 patients who had received a psychiatric evaluation at an index emergency department visit for suicidal ideation over a 2-year period. The mean age of patients was 39 years. The target sample was 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
The researchers analyzed 32 predictor variables from patient charts, including demographics, psychiatric history, and current psychiatric presentation. The evaluation was done with “a machine learning statistical approach which is more capable than traditional statistical approaches in handling a large number of predictor variables,” Ms. Knorr said.
The number of previous psychiatric admissions was the most important predictor of a subsequent suicide attempt. The next nine most important variables were sleep disturbance, history of family suicide, low energy, patient age, psychiatrist determination of severe suicide risk, psychiatrist determination of moderate suicide risk, appetite issues, presence of a support system, and loss of interest/pleasure.
These symptoms may not typically be weighed heavily in risk assessments, Ms. Knorr said. “Additionally, given that research suggests that the clinical determination of suicide risk is historically poor, it was interesting that psychiatrist determination of moderate or high risk was influential in predicting a return visit for suicide attempt. Finally, we were surprised that a past history of suicide attempt, often viewed as the strongest predictor of a future suicide attempt, did not emerge as one of the top 10 influential predictors.
“Limitations of this study include the use of a return visit to a Geisinger emergency department as the only measure of a future suicide attempt and the utilization of data from only one health system,” she noted.
The study was funded by the Geisinger Clinic Research Fund. One of the coauthors, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
SOURCE: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23. doi. 10.1016/j.annemergmed.2018.08.055.
SAN DIEGO – Among patients presenting to the emergency department with suicidal ideation, the number of previous psychiatric admissions is the most important predictor of a subsequent suicide attempt, results from a 2-year-long study showed.
Momentary measures – significant current difficulties with sleep, energy, or appetite, and anhedonia – “are important considerations during suicide risk assessment, regardless of whether the patient meets the threshold for major depressive disorder, lead study author Anne C. Knorr said in an interview in advance of the annual meeting of the American College of Emergency Physicians.
“Many traditionally studied psychiatric risk factors do not significantly differ between individuals who think about suicide and those who act on their suicidal thoughts, an important distinction as only one-third of those who think about suicide carry out a suicide attempt. While there is support for some psychiatric factors – for example, anxiety, substance use disorders, sleep disturbance – being useful in differentiating these groups, the current study is unique in its use of a longitudinal design to identify influential risk factors that predict future suicide attempt among those with suicidal ideation,” she said.
Ms. Knorr, a research project manager at Geisinger Medical Center, Danville, Pa., and her colleagues collected electronic medical record data from 908 patients who had received a psychiatric evaluation at an index emergency department visit for suicidal ideation over a 2-year period. The mean age of patients was 39 years. The target sample was 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
The researchers analyzed 32 predictor variables from patient charts, including demographics, psychiatric history, and current psychiatric presentation. The evaluation was done with “a machine learning statistical approach which is more capable than traditional statistical approaches in handling a large number of predictor variables,” Ms. Knorr said.
The number of previous psychiatric admissions was the most important predictor of a subsequent suicide attempt. The next nine most important variables were sleep disturbance, history of family suicide, low energy, patient age, psychiatrist determination of severe suicide risk, psychiatrist determination of moderate suicide risk, appetite issues, presence of a support system, and loss of interest/pleasure.
These symptoms may not typically be weighed heavily in risk assessments, Ms. Knorr said. “Additionally, given that research suggests that the clinical determination of suicide risk is historically poor, it was interesting that psychiatrist determination of moderate or high risk was influential in predicting a return visit for suicide attempt. Finally, we were surprised that a past history of suicide attempt, often viewed as the strongest predictor of a future suicide attempt, did not emerge as one of the top 10 influential predictors.
“Limitations of this study include the use of a return visit to a Geisinger emergency department as the only measure of a future suicide attempt and the utilization of data from only one health system,” she noted.
The study was funded by the Geisinger Clinic Research Fund. One of the coauthors, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
SOURCE: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23. doi. 10.1016/j.annemergmed.2018.08.055.
AT ACEP18
Key clinical point: A number of factors representing momentary experiences such as low energy emerged as predictors of suicide attempts among suicidal ideators following an ED visit.
Major finding: The number of past psychiatric admissions was the most influential predictor of a subsequent suicide attempt.
Study details: A study of 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
Disclosures: The Geisinger Clinic Research Fund supported the study. A coauthor, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
Source: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23.