A closed-loop feedback transcranial electrical stimulation system has proved its ability to detect and suppress spike-and-wave episodes from a rat model of generalized petit mal epilepsy, providing evidence that it may be possible to avoid the adverse effects of invasive deep brain stimulation while also reducing seizures.
It is the first study to report controlling seizures through the use of transcranial electrical stimulation (TES), a development made possible by reducing TES-induced artifacts via a closed-loop feedback system with recording of spike-and-wave discharges from a chronically implanted tripolar electrode. Spike-and-wave patterns are the hallmark of generalized petit mal epilepsy.

Dr. Paul R. Carney
The importance of the findings is that the researchers were "able to both record and stimulate simultaneously" and use TES as the form of electrical stimulation, Dr. Paul R. Carney said in an interview. Dr. Carney is chief of the division of pediatric neurology and director of the pediatric comprehensive epilepsy program at the University of Florida, Gainesville. He was not involved with the study.
In the study, led by György Buzsáki, Ph.D., of New York University, brain-activity timed feedback of TES at 1 Hz significantly shortened the spike-and-wave discharges of nine rats. In seven of the rats, the percentage of time spent having spike-and-wave episodes in a session also declined significantly. The device led to a greater than 60% decline in the duration and the fraction of session time spent in spike-and-wave episodes (Science 2012;337:735-7).
An investigational device currently in clinical trials, the NeuroPace Responsive Neurostimulation System, uses the same concept of closed-loop feedback stimulation but involves the placement of deep brain electrodes at the focal point of a patient’s complex partial seizures. When the NeuroPace device detects the onset of a seizure, it delivers a current through the same electrode that detected the onset, irrespective of the dynamics of the seizure.
The difference with the TES device is that it detects and responds to every single spike-and-wave episode, dampening the episode with every current discharge, not just a train of stimulation events, Dr. Buzsáki said in an interview. The high noise-to-signal ratio with devices that measure and deliver current through the same electrode, such as the NeuroPace Responsive Neurostimulation System, makes it difficult to detect ongoing seizure activity, he said.
 Courtesy György Buzsáki, Ph.D.
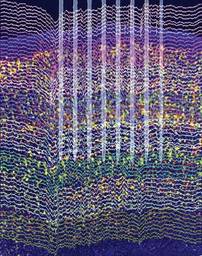
Courtesy György Buzsáki, Ph.D.
Large-scale silicon probe recordings from the rat neocortex allowed researchers to detect spike-and-wave episodes indicating generalized petit mal seizure activity.
To apply the study results of closed-loop TES successfully in a clinical situation without the use of a chronically implanted deep brain electrode, the investigators noted that they first would need to identify and record from the causal pathophysiological brain network activity. This could be accomplished in generalized spike-and-wave episodes and focal cortical epilepsies through the use of subdural or epidural electrodes, or electrodes inserted into the skull. However, for complex partial seizures, which make up the majority of drug-resistant epilepsies, the investigators wrote that "deep-electrode recordings are required for accurate detection of abnormal patterns."
Another requirement for clinical application will be the development of intra–skull plate electrodes, possibly in multiple locations, to provide closed-loop feedback TES of the target brain circuits. These implants would be much lighter and more cosmetically acceptable than what could be produced using the large and heavy coils needed for transcranial magnetic stimulation, according to the researchers.
The next step for the research group is to study patients who already have subdurally implanted titanium plates used to repair a skull defect following surgery for epilepsy. With a little modification of these plates, Dr. Buzsáki and his colleagues plan to stimulate the brain and see if they can get an adequate signal-to-noise ratio for detecting seizure activity.
The research was supported by grants from the National Institutes of Health, the Human Frontier Science Program, and the J.D. McDonnell Foundation. Neither the researchers nor Dr. Carney had relevant disclosures.