Article
Reactive Benign Follicular Mucinosis: A Report of 2 Cases
We report 2 cases of adolescents who developed follicular mucinosis following cutaneous infections. A 17-year-old adolescent boy was evaluated for...
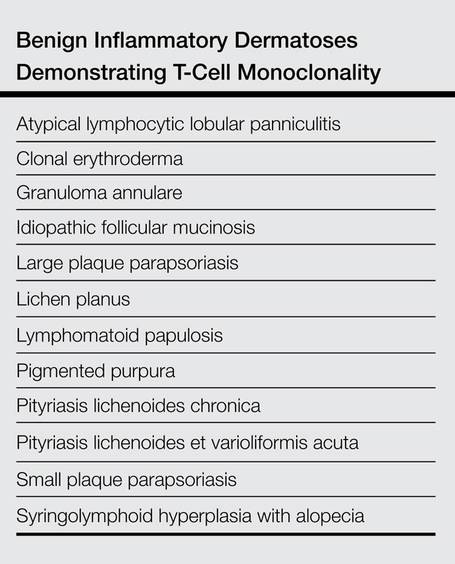
In recent years, the distinction between idiopathic follicular mucinosis (FM) and lymphoma-associated follicular mucinosis (LAFM) has been made through assessment of T-cell receptor gene rearrangement, flow cytometry, and immunohistochemistry. These methods, among others, have mostly identified monoclonality as a defining characteristic of LAFM; however, this finding cannot be considered conclusive, as monoclonality also has been described in benign inflammatory dermatoses such as lichen planus and idiopathic FM. Pure histologic diagnosis also is unreliable in many cases, as the histologic patterns of idiopathic FM and LAFM overlap. In this article, we discuss the importance of close clinical follow-up in patients with patch-stage mycosis fungoides (MF) or FM who have had a nondiagnostic histopathologic evaluation. We also highlight the value of ancillary testing, including T-cell receptor gene rearrangement, flow cytometry, and immunohistochemistry, as a component in the diagnostic process rather than the sole diagnostic moiety. Diagnosis and classification of idiopathic FM and LAFM continue to pose challenges for dermatologists, oncologists, and pathologists, and no single diagnostic tool is sufficient in providing diagnostic certainty; rather, a collective evaluation of pathologic, molecular, and clinical criteria is required. Currently, classification of idiopathic FM and LAFM incorporates clinical information and histologic assessment, but little consideration is given to the implications of the diagnosis from the patient’s perspective. Revisiting histologic classification of these entities while incorporating the patient’s perspective may prove beneficial to dermatologists as well as patients.
Practice Points
We report 2 cases of adolescents who developed follicular mucinosis following cutaneous infections. A 17-year-old adolescent boy was evaluated for...
Although rare, of all the cutaneous lymphoid malignancies, cutaneous T-cell lymphomas (CTCLs) constitute 65% of all lymphomas, of which 50% are...

We report the case of a healthy 17-year-old adolescent boy with an unremarkable medical history who presented with an asymptomatic fixed rash on...