

A) Endometrial polyp INCORRECT
Endometrial polyps on ultrasonography appear as focal echogenic (hyperechoic) masses or as nonspecific endometrial thickening.1 Color Doppler often demonstrates a vascular stalk, which is a nonspecific finding that also can be seen in submucosal fibroids and endometrial cancer.2 On sonohysterography (SHG), endometrial polyps typically appear as well-defined echogenic/hyperechoic polypoid lesions (tissue appearance similar to that of normal endometrium) protruding into the endometrial canal but still preserving the endometrial−myometrial interface.2,3
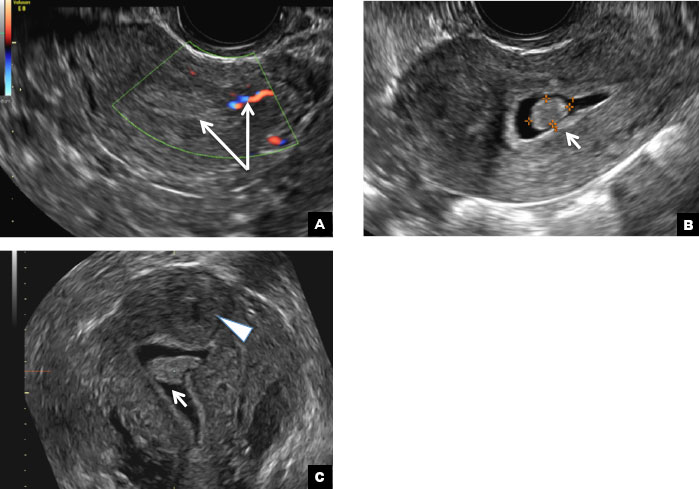
Endometrial polyp. (A) Transvaginal pelvic ultrasound of the uterus with color Doppler demonstrates a focal echogenic lesion with a vascular stalk (long arrows). (B) SHG shows a well-defined polypoid lesion, isoechoic to the endometrium, and protruding into the endometrial canal but still preserving the endometrial−myometrial interface (short arrow). (C) 3D SHG imaging shows the echogenic endometrial polyp (short arrow) and an incidental intramural fibroid in the fundus (arrowhead).
B) Submucosal fibroid CORRECT
Submucosal fibroids on ultrasonography appear as heterogeneous hypoechoic lesions distorting the endometrial cavity.1 In contrast to endometrial polyps, which involve the endometrium only, submucosal (intracavitary) fibroids originate in the myometrium, as clarified in Figures 3A & B. SHG demonstrates a broad-based mixed hypoechoic/isoechoic lesion protruding into the endometrial canal but preserving the echogenic endometrium, distinguishing myometrial from endometrial lesions. Submucosal fibroids often distort the endometrial myometrial interface and demonstrate acoustic shadowing.2,3
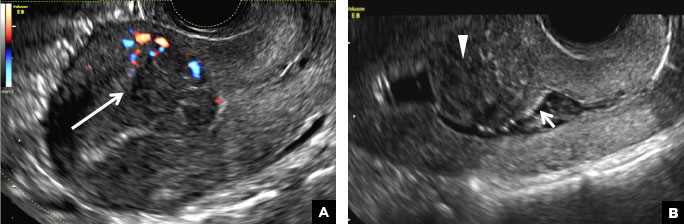
Submucosal fibroid. (A) Transvaginal pelvic ultrasound with color Doppler demonstrates a heterogeneous hypoechoic/isoechoic lesion arising from the myometrium (long arrow) and distorting the endometrial cavity. (B) SHG demonstrates a broad-based hypoechoic lesion protruding into the endometrial canal with areas of acoustic shadowing (arrowhead) but preserving the echogenic endometrium (short arrow).
C) Endometrial carcinoma INCORRECT
Endometrial carcinoma on SHG appears as an irregular inhomogeneous lobulated vascular mass distorting the endometrial−myometrial interface.3 Additionally, irregular frond-like projections can be seen extending from the mass into the endometrial cavity, which are distended with echogenic fluid.2
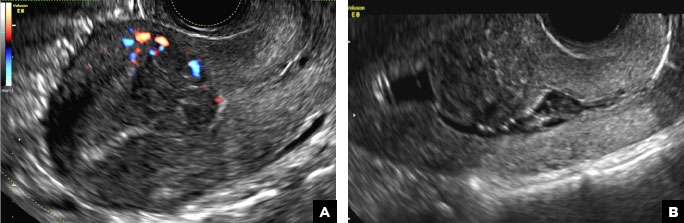
Endometrial carcinoma. (A) Transvaginal pelvic ultrasound demonstrates a retroverted uterus with the endometrial cavity distended by tissue and fluid. An irregular inhomogeneous lobulated mass with frond-like projections (long arrow) distorts the endometrial−myometrial interface (short arrow). (B) Color Doppler image shows marked vascularity within the mass and echogenic fluid in the endometrial canal (arrowhead).
D) Endometrial hyperplasia INCORRECT
On ultrasonography, endometrial hyperplasia has a nonspecific appearance, often presenting as diffuse smooth endometrial thickening.1 SHG typically demonstrates diffuse thickening of the echogenic endometrial stripe without a focal lesion and, when a focal lesion is present, can mimic a broad-based endometrial polyp.2,3

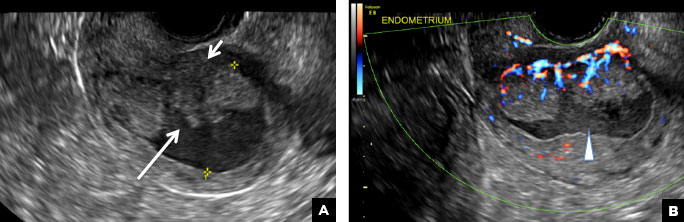
Endometrial hyperplasia. (A) Transvaginal pelvic ultrasound demonstrates diffuse endometrial thickening (long arrow). (B) SHG shows diffuse thickening of the echogenic endometrial stripe without a focal lesion (arrow heads).