Drs. Hashim and Goldenberg and Mr. Levy are from the Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, New York. Dr. Cohen is from AboutSkin Dermatology and DermSurgery, Greenwood Village, Colorado; the Department of Dermatology, University of Colorado Denver, Aurora; and the Department of Dermatology, University of California, Irvine.
Drs. Hashim and Goldenberg and Mr. Levy report no conflict of interest. Dr. Cohen is an advisory board member, clinical researcher, and consultant for Allergan, Inc, and Galderma Laboratories, LP; a consultant and speaker for Sciton, Inc; and a clinical researcher for CROMA-PHARMA GmbH and Suneva Medical, Inc.
Correspondence: Gary Goldenberg, MD, Department of Dermatology, Icahn School of Medicine at Mount Sinai, 5 E 98th St, New York, NY 10029 (garygoldenbergmd@gmail.com).
Microneedling therapy is an increasingly popular treatment of several dermatologic conditions. Platelet-rich plasma (PRP) may serve as a valuable adjunct to improve the regenerative effects of treatment. We review the evidence comparing the results of microneedling therapy with and without PRP. Based on the current preliminary literature, PRP appears to augment the cosmetic outcomes of microneedling without increasing the risk for adverse events.
Microneedling is an effective therapy for skin rejuvenation.
Preliminary evidence indicates that the addition of platelet-rich plasma to microneedling improves cosmetic outcomes.
References
Microneedling therapy, also known as collagen induction therapy or percutaneous collagen induction, is an increasingly popular treatment modality for skin rejuvenation. The approach employs small needles to puncture the skin and stimulate local collagen production in a minimally invasive manner. Recently, clinicians have incorporated the use of platelet-rich plasma (PRP) with the aim of augmenting cosmetic outcomes. In this article, we examine the utility of this approach by reviewing comparison studies of microneedling therapy with and without the application of PRP.
Dr. Gary Goldenberg demonstrates microneedling with platelet-rich plasma in a procedural video available here.
Microneedling Therapy
The use of microneedling first gained attention in the 1990s. Initially, Camirand and Doucet1 described tattooing without pigment for the treatment of achromatic and hypertrophic scars. Fernandes2 evolved this concept and developed a drum-shaped device with fine protruding needles to puncture the skin. Microneedling devices have expanded in recent years and now include both cord- and battery-powered pens and rollers, with needles ranging in length from 0.25 to 3.0 mm.
Treatment with microneedling promotes skin rejuvenation by creating small puncture wounds in the epidermis and dermis. This injury triggers the wound healing cascade and alters the modulation of growth factors to promote regenerative effects.3,4 Following microneedling therapy, increases occur in elastic fiber formation, collagen deposition, and dermal thickness (Figure).5 Of interesting histologic note, collagen is deposited in the normal lattice pattern following this treatment rather than in the parallel bundles typical of scars.6 Microneedling preserves the overall integrity of the epidermal layers and basement membrane, allowing the epidermis to heal without abnormality, verified on histology by a normal stratum corneum, enhanced stratum granulosum, and normal rete ridges.7
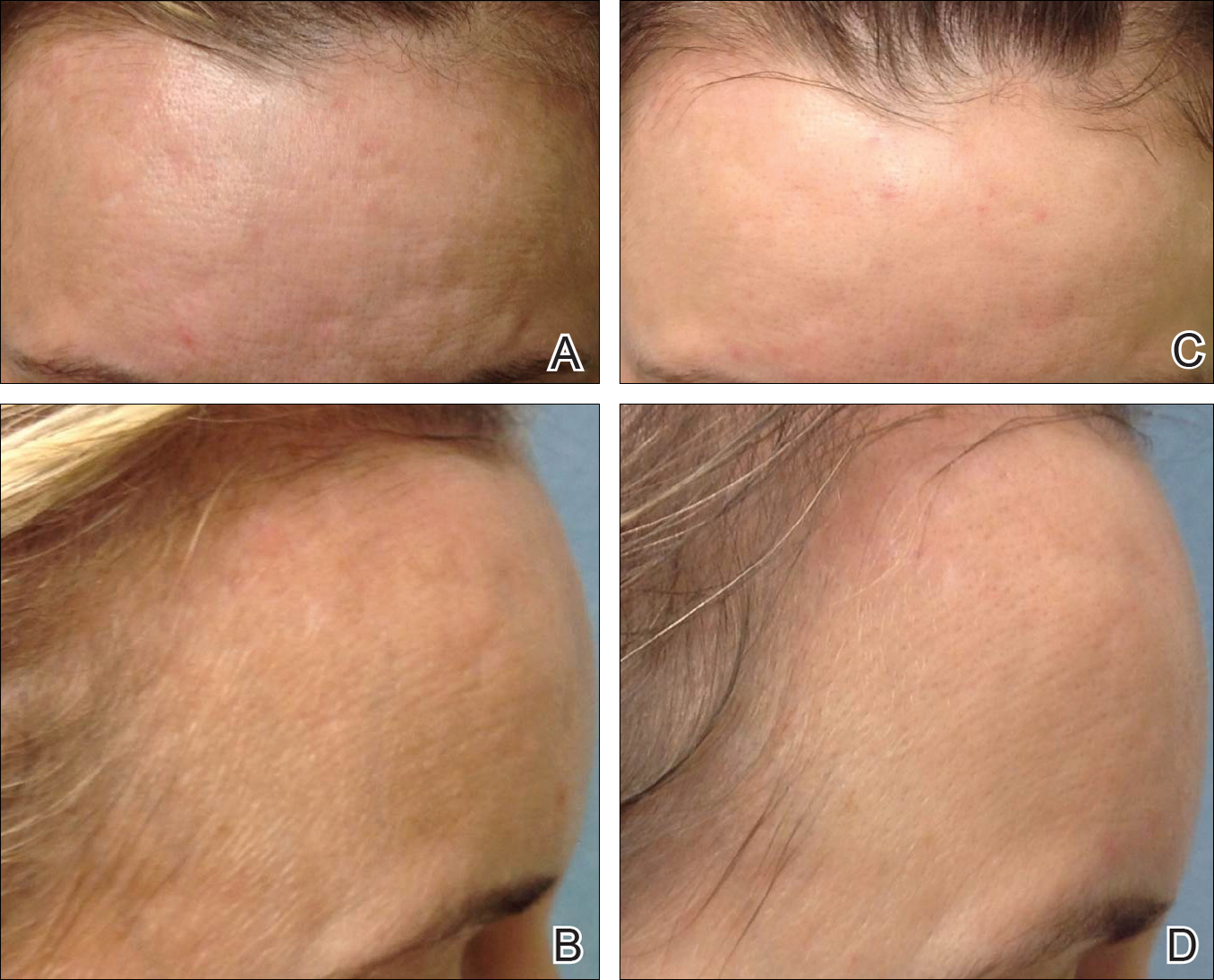
Photographs courtesy of Joel L. Cohen, MD (Colorado, USA).
Before (A and B) and after skin rejuvenation with 4 sessions of microneedling therapy (C and D).
Microneedling has demonstrated several uses beyond general skin rejuvenation. In patients with atrophic acne scars, therapy can lead to improved scar appearance, skin texture, and patient satisfaction.8,9 Hypertrophic and dyspigmented burn scars on the body, face, arms, and legs have shown to be receptive to repeated treatments.10 Microneedling also has shown promise in treating androgenic alopecia, increasing hair regrowth in patients who previously showed poor response to conventional therapy with minoxidil and finasteride.11,12
Platelet-Rich Plasma
Platelet-rich plasma is developed by enriching blood with an autologous concentration of platelets. The preparation of PRP begins with whole blood, commonly obtained peripherally by venipuncture. Samples undergo centrifugation to allow separation of the blood into 3 layers: platelet-poor plasma, PRP, and erythrocytes.13 The typical platelet count of whole blood is approximately 200,000/µL; PRP aims to prepare a platelet count of at least 1,000,000/µL in a 5-mL volume.14
An attractive component of PRP is its high concentration of growth factors, including platelet-derived growth factor, transforming growth factor, vascular endothelial growth factor, and epithelial growth factor.15 Because of the regenerative effects of these proteins, PRP has been investigated as a modality to augment wound healing in a variety of clinical areas, such as maxillofacial surgery, orthopedics, cardiovascular surgery, and treatment of soft tissue ulcers.16