


Case Letter
Oral Fixed Drug Eruption Due to Tinidazole
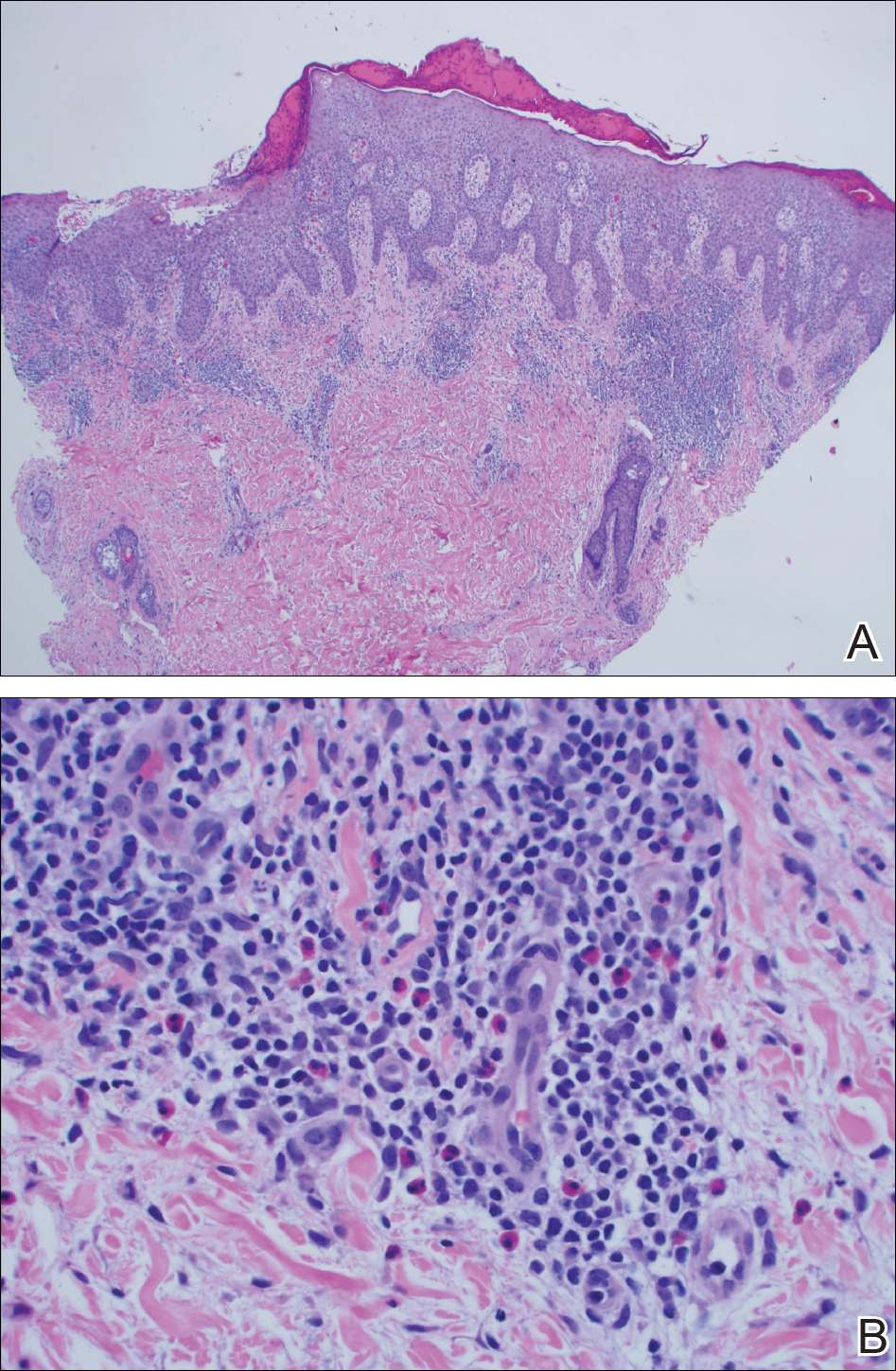
To the Editor:A 50-year-old man presented with a painful ulcer and a burning sensation on the tongue of 2 days’ duration (Figure, A). The ulcer...
Allergy as a cause of adverse outcomes in patients with implanted orthopedic hardware is controversial. Allergy to titanium-based implants has not been well researched, as titanium is traditionally thought to be inert. We highlight the case of a patient who developed systemic dermatitis and implant failure after surgical placement of a titanium alloy (Ti6Al4V) plate in the left foot. The hardware was removed and the eruption cleared in the following weeks. The plate and screws were submitted for metal analysis. The elemental composition of both the plate and screws included 3 major elements—titanium, aluminum, and vanadium—as well as trace elements. Metal analysis revealed that the plate and screws had different microstructures, and electrochemical studies demonstrated that galvanic corrosion could have occurred between the plate and screws due to their different microstructures, contributing to the release of vanadium in vivo. The patient was patch tested with several metals including components of the implant and had a positive patch test reaction only to vanadium trichloride. These findings support a diagnosis of vanadium allergy and suggests that clinicians should consider including vanadium when patch testing patients with a suspected allergic reaction to vanadium-containing implants.
Practice Points
To the Editor:A 50-year-old man presented with a painful ulcer and a burning sensation on the tongue of 2 days’ duration (Figure, A). The ulcer...

The reported sensitivity and specificity of enzyme-linked immunosorbent assay (ELISA) for bullous pemphigoid (BP) diagnosis is approximately 87%...

A 32-year-old woman presented with a recurrent painful eruption on the scalp of 1 year's duration. The lesion occurred on the left temporal region...