CHICAGO – Funding sources to cover care for undocumented immigrants have pulled back since 2008 and will continue to do so after the Patient Protection and Affordable Care Act takes full effect. Although the legislation strives to provide nearly universal health insurance coverage by 2014, undocumented immigrants are not included, and one hospital’s experience with dwindling reimbursement portends a cloudy future for paying for care in this patient population.
Even when the Affordable Care Act takes full effect, about 22 million people will still lack coverage – 10-15 million of whom will be undocumented immigrants, according to Dr. Michael S. Truitt of Methodist Dallas Medical Center. The Affordable Care Act will cut Medicare/Medicaid Disproportionate Share Hospital (DSH) funds by about 75% between 2014 and 2019.
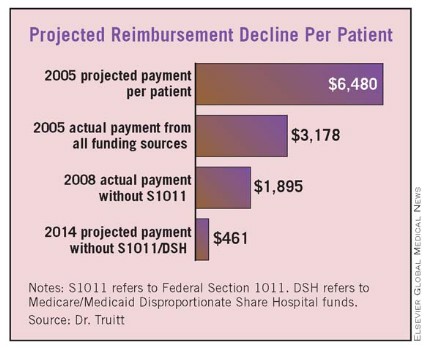
"We have serious and specific concerns about how the cut in DSH funding could affect trauma centers and safety net hospitals," Dr. Truitt said at the annual meeting of the American Association for the Surgery of Trauma. "On a per-patient basis at our institution, projected payments decrease from $6,480 in 2005 to $461 in 2014."
He presented a study that evaluated retrospectively 183,000 visits to his hospital’s emergency department from 2005 to 2008. Of those, 6,691 were undocumented immigrants, and about 20% of their visits were trauma related, he said.
The study focused on the four main funding mechanisms for the care of undocumented immigrants in Texas: self-payment; the Texas Driver Responsibility Program (DRP), which uses motor vehicle fines; federal Section 1011 funds; and DSH funds.
The state DRP program distributes $70 million to $90 million to Texas hospitals annually, Dr. Truitt said, but even that has been problematic. "Significantly more has been collected each year and earmarked for trauma, but disbursement from the state has not always been consistent," he said.
Section 1011 distributed about $1 billion from 2005 to 2008, one-third of which went to the eight states bordering Mexico, but that program has been unfunded since 2008, according to Dr. Truitt. Medicare/Medicaid DSH funds distributed $19.1 billion to U.S. hospitals in 2009, but these funds are used to subsidize numerous programs and are not specific to care of indigent trauma patients.

Dr. Michael S. Truitt
From May 2005 to May 2008, Methodist Dallas Medical Center actually collected about $4.2 million from these varied sources for uncompensated undocumented immigrant trauma care – about $4.9 million less than the hospital’s usual fees, Dr. Truitt said. These funds were shared by the hospital, ED physicians, and trauma surgeons, he noted.
"In the end, this may be just another call for fiscal responsibility on the part of trauma centers to reduce unnecessary charges and waste, such as robust use of CT scans, laboratory tests, etc. – not just for the undocumented immigrant trauma patients, but for all compensated and uncompensated patients," said Dr. Thomas Esposito of Loyola University, Chicago. He asked whether the authors had any suggestions for alternative funding sources, and whether states and trauma systems should take it upon themselves to establish or increase revenue from sources similar to the Texas Driver Responsibility Program.
Dr. Truitt called on policy makers to prioritize funding for trauma centers and safety net hospitals. "If it’s a federal responsibility, so be it, but it should be supported by a program that is not subject to the political winds. If it’s a state responsibility, the states should have the authority to collect these funds and ensure they are disbursed to the intended recipients expeditiously and consistently."
Dr. Truitt and his colleagues had no relevant financial disclosures.