Cryptococcosis is a granulomatous infection caused by Cryptococcus neoformans1,2 that usually develops in immunocompromised hosts, especially those with human immunodeficiency virus (HIV) infection. Cryptococcosis rarely has been described in patients with diabetes mellitus (DM).3 Patients with uncontrolled DM are prone to numerous infections, as glucose-rich blood serves as an excellent medium for growth of organisms and hyperglycemia has been shown to cause numerous defects in host defense mechanisms. We present a rare case of disseminated cryptococcosis in an HIV-negative patient with DM.
A 48-year-old man presented with raised lesions on the left side of the neck and the back of the right shoulder that had gradually increased in size over the last 4 months. The patient denied any history of antecedent trauma. Physical examination revealed a well-defined, tender, indurated, ulcerated plaque measuring 3×4 cm on the left side of the neck (Figure 1) and a single 1×1-cm erythematous nodule with a central ulcerated core on the right shoulder (Figure 2). Both lesions showed minimal seropurulent discharge. Genital examination showed evidence of candidal balanitis. Systemic examination was normal.
|
| Figure 1. A well-defined, tender, indurated, ulcerated plaque measuring 3×4 cm on the left side of the neck. |
|
| Figure 2. An erythematous 1×1-cm nodule with a central ulcerated core on the right shoulder. |
|
|
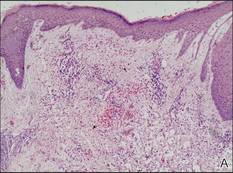
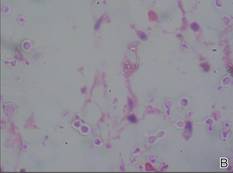
Figure 3. Skin biopsy revealed granulomatous and gelatinous tissue reaction with ovoid encapsulated spores (A)(H&E, original magnification ×40). Ovoid, budding, encapsulated spores of Cryptococcus were seen on higher power (B)(H&E, original magnification ×400). |
|
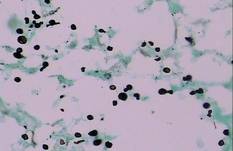
| Figure 4. Black-colored, ovoid, budding spores of Cryptococcus were seen (Gomori methenamine-silver, original magnification ×100). |
|
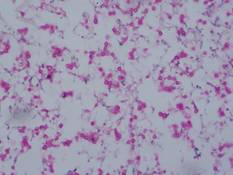
| Figure 5. Mucicarmine stain showed multiple red-colored, budding, capsulated spores (original magnification ×100). |
Keratoacanthoma, secondary syphilis, cutaneous tuberculosis, leishmaniasis, cryptococcosis, histoplasmosis, and leprosy were considered in the differential diagnosis. The complete blood cell count was normal. A VDRL test and enzyme-linked immunosorbent assay for HIV-1 and HIV-2 were nonreactive. The absolute CD4 count was 885 cells/µL (reference range, 404–1612 cells/µL), CD4 was 41% (reference range, 33%–58%), absolute CD8 count was 443 cells/µL (reference range, 220–1129 cells/µL), CD8 was 20% (reference range, 13%–39%), and CD4:CD8 ratio was 2.04 (reference range, 0.8–3.0). The fasting blood glucose level was elevated at 230 mg/dL (reference range, 80–120 mg/dL) and the postprandial glucose level was 348 mg/dL (reference range, 130–150 mg/dL). A chest radiograph revealed a nodular opacity in the right upper lobe of the lung with no evidence of cavitation. Ultrasonography of the abdomen and pelvis showed mild splenomegaly.
Gram stain and a potassium hydroxide (KOH) mount of a smear from the ulcerated lesion on the neck showed encapsulated budding spores. Histopathologic study of hematoxylin and eosin–stained sections from the noduloulcerative lesion on the shoulder demonstrated irregular acanthosis in the epidermis; a granulomatous reaction comprised of lymphocytes, histiocytes, neutrophils, plasma cells, and few giant cells; and a gelatinous tissue reaction with numerous ovoid encapsulated spores (Figure 3). Gomori methenamine-silver stain revealed black-colored, ovoid, budding spores (Figure 4), and periodic acid–Schiff stain also revealed narrow-based budding spores. Mucicarmine staining showed multiple red-colored, budding, capsulated spores (Figure 5). A culture on Sabouraud dextrose agar confirmed growth of C neoformans. Examination of sputum by KOH mount and india ink preparation demonstrated encapsulated spores of Cryptococcus. India ink staining of cerebrospinal fluid and urine was negative for Cryptococcus. Cerebrospinal fluid cytochemistry was within reference range. The final diagnosis was disseminated cryptococcosis in the setting of uncontrolled DM.
The patient was treated with oral fluconazole 200 mg twice daily. He also was started on metformin 500 mg daily, glipizide 5 mg twice daily, and pioglitazone 15 mg daily for treatment of DM. The lesions resolved with scarring after 8 months of treatment.
Cryptococcosis is a disease caused by C neoformans, an encapsulated yeast. There are 2 variants of cryptococcosis and 5 serotypes: C neoformans var neoformans (serotypes A, D, and AD) and C neoformans var gattii (serotypes B and C).1,2 The former is more common in Europe and much of the United States, while the latter is more common in the tropics.3Cryptococcus neoformans var neoformans is a saprophyte that commonly is found in soil rich in pigeon droppings, while C neoformans var gattii is found in tree bark (eg, eucalyptus).
Cryptococcal infection usually is acquired by respiratory transmission, though primary cutaneous lesions rarely may occur.4 The organisms are less than 2 µm in size and are unencapsulated; therefore, they can easily be inhaled into the alveolar space.2,5 The most important host response to cryptococcal infection is cell-mediated immunity, which explains the increased incidence of infection in immunosuppressed patients, especially in patients with HIV infection. It has been sporadically reported in HIV-negative patients in the setting of other causes of immunosuppression (eg, chronic corticosteroid use, organ transplantation, chemotherapy, hematologic malignancies, systemic lupus erythematosus, sarcoidosis, liver failure, renal failure, idiopathic CD4+ lymphocytopenia, monoclonal antibody therapy [eg, alemtuzumab, infliximab]).1,6,7