

Preparing tissue for the pathologist
Here are 5 tips for preparing the biopsied specimen for pathology:
- Include a question for the pathologist, such as “rule out lichen sclerosus or lichen simplex chronicus.” The majority of specimens should be sent in formalin. At times, frozen sections are done in the operating room.
- Double-check that the proper paperwork is included with every specimen and be very specific regarding the exact location of the lesion on the vulva. Include photographs whenever possible.
- Request that a dermatopathologist or a gynecologic pathologist with a special interest in vulvar dermatology, when feasible, review the tissue.
- Check your laboratory’s protocol for sending biopsies from areas around ulcerated tissue. Often, special medium is required for immunohistochemistry stains.
- Call your pathologist with questions about results; he or she often is happy to clarify, and together you may be able to arrive at a diagnosis to better serve your patient.3
Complications and how to avoid them
Bleeding. Any procedure has bleeding risks. To avoid bleeding, review the patient’s medication list and medical history prior to biopsy, as certain medications, such as blood thinners, increase risk for bleeding. Counseling a patient on applying direct pressure to the biopsy site for 2 minutes is generally sufficient for any bleeding that may occur once she is discharged from the clinic.
Infection. With aseptic technique, infection of a biopsy site is rare. We use nonsterile gloves for biopsy procedures. This does not increase the risk of infection.4 If a patient has iodine allergy, dilute chlorhexidine is a reasonable alternative for skin cleansing. Instruct the patient to keep the site clean and dry; if the biopsy proximity is close to the urethra or anus, use of a peri-bottle may be preferred after toileting. Instruct patients not to pull sutures. While instructions are specific for each patient, we generally advise that patients wait 4 to 7 days before resuming use of topical medications.
Scarring or tattooing. Avoid using dyed suture on skin surfaces and counsel the patient that silver nitrate can permanently stain tissue. Usually, small biopsies heal well but a small scar is possible.
Key points to keep in mind
- Counsel patients on biopsy risks, benefits, and alternatives. Counsel regarding possible inconclusive results.
- Take time in choosing the biopsy site and consider multiple biopsies.
- Have all anticipated equipment available; consider using premade biopsy kits.
- Consider performing a stitch biopsy to avoid crush injury.
- Take photographs of the area to be biopsied and communicate with your pathologist to facilitate diagnosis.
Vulvar biopsy established the diagnosis in these cases
 A 62-year-old woman with a history of vulvar lichen sclerosus presents for examination reporting symptoms of perianal irritation. Vulvar examination is consistent with lichen sclerosus, with an area of erosion on the right labium majus. In addition, thickened tissue firm to the touch raises concern. The clinician recommends a vulvar biopsy to evaluate for lichen sclerosus, differentiated vulvar intraepithelial neoplasia (dVIN), and vulvar cancer.
A 22-year-old woman presents with concerns of raised bumps on the vulva. The bumps can be itchy and irritating but are not painful. They seem to have grown and spread since she first noticed them.
A 30-year-old woman presents with concern of a raised area on the vulva. It is itchy and sometimes painful. Acetic acid is applied to the vulva and acetowhite changes are noted. 4-mm punch biopsies are obtained in multiple areas.
A 19-year-old woman presents with concerns of a pigmented, darkened area on the vulva. She is not sure how long the lesion has been present. It is not itchy and does not cause pain or irritation.
A 56-year-old woman presents with a 2-year history of vulvar irritation, burning, and itching. Examination reveals vulvar paleness in an hourglass configuration. There is loss of the labia minora and phimosis of the prepuce overlying the clitoris.
A 65-year-old woman with a long history of lichen sclerosus presents with painful bleeding and a raised lesion on the vulva. Examination reveals a firm raised area that is friable to touch.
A 62-year-old woman with a history of vulvar lichen sclerosus presents for examination reporting symptoms of perianal irritation. Vulvar examination is consistent with lichen sclerosus, with an area of erosion on the right labium majus. In addition, thickened tissue firm to the touch raises concern. The clinician recommends a vulvar biopsy to evaluate for lichen sclerosus, differentiated vulvar intraepithelial neoplasia (dVIN), and vulvar cancer.
A 22-year-old woman presents with concerns of raised bumps on the vulva. The bumps can be itchy and irritating but are not painful. They seem to have grown and spread since she first noticed them.
A 30-year-old woman presents with concern of a raised area on the vulva. It is itchy and sometimes painful. Acetic acid is applied to the vulva and acetowhite changes are noted. 4-mm punch biopsies are obtained in multiple areas.
A 19-year-old woman presents with concerns of a pigmented, darkened area on the vulva. She is not sure how long the lesion has been present. It is not itchy and does not cause pain or irritation.
A 56-year-old woman presents with a 2-year history of vulvar irritation, burning, and itching. Examination reveals vulvar paleness in an hourglass configuration. There is loss of the labia minora and phimosis of the prepuce overlying the clitoris.
A 65-year-old woman with a long history of lichen sclerosus presents with painful bleeding and a raised lesion on the vulva. Examination reveals a firm raised area that is friable to touch.
Case 1

Biopsies were obtained of the areas highlighted in the photo. Pathology shows dVIN.
Image courtesy of Hope Haefner, MD.
Case 2

The examination is consistent with condylomata acuminata and biopsy is recommended with a 4-mm punch. Biopsy results are consistent with condylomata acuminata.
Image courtesy of Hope Haefner, MD.
Case 3

The final pathology shows high-grade squamous intraepithelial lesions (HSIL) of the vulva.
Image courtesy of Hope Haefner, MD.
Case 4
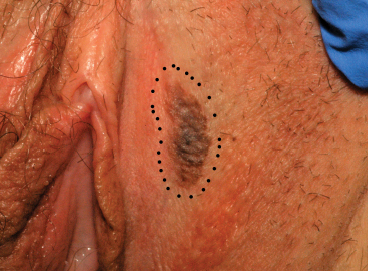
This presentation is an excellent opportunity for an excisional biopsy of the vulva. A marking pen is used to draw margins. A No. 15 blade is used to outline and then undermine the lesion, removing it in its entirety.
Final pathology shows a compound nevus of the vulva.
Image courtesy of Hope Haefner, MD.
Case 5

A 4-mm punch biopsy result is consistent with a diagnosis of lichen sclerosus.
Image courtesy of Hope Haefner, MD.
Case 6

A 4-mm punch biopsy result reveals that the pathology is significant for squamous cell carcinoma.
Image courtesy of Hope Haefner, MD.