KEY POINTS
- Endoanal ultrasound is superior to other diagnostic methods, with an accuracy of over 90% in detecting sphincter injuries, compared to 75% for manometry, 75% for electromyography, and 50% for clinical assessment.
- Pelvic floor rehabilitation with biofeedback/electrical stimulation is the mainstay nonsurgical treatment. Some centers report success rates as high as 70%.
- Consider surgery only for distinct anatomic defects, and only when nonsurgical interventions have not succeeded.
Thanks to improvements in our understanding of the causes of uncontrolled defecation and an increasing array of diagnostic and treatment options, physicians can now manage this condition more effectively.
Fecal incontinence is a relevant clinical issue for Ob/Gyns, and requires compassion and emotional support on the part of the physician and health-care team. This debilitating problem is underreported, but is thought to affect 2.2% of the general population. Women are 8 times more likely to have fecal incontinence than men, in age-controlled groups.1
Although sphincter damage during vaginal delivery—even in deliveries over an intact perineum2,3—may be clinically silent in most women, these women are at risk of developing overt fecal incontinence with subsequent deliveries, and with aging and its decompensating factors (FIGURE 1).
A directed examination, optimal diagnostic testing, and a step-by-step treatment algorithm are the basis of effective management.
FIGURE 1 Common pathway leading to fecal incontinence
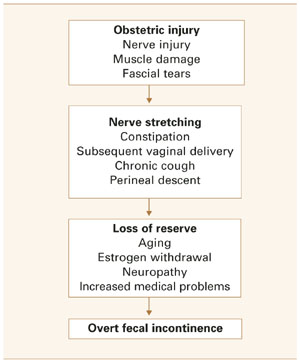
How ‘silent’ sphincter damage can lead to incontinence
Obstetric disruption of the anal sphincter structure or function is a common cause of fecal incontinence, although it is usually multifactorial, involving abnormalities of 1 or more continence mechanisms (FIGURE 2).
Weakening of the sphincter mechanism after vaginal delivery is attributed to both direct trauma to the muscle and indirect trauma to the pudendal nerve (unilateral or bilateral). Anatomic injury usually occurs in the anterior portion of the sphincter—a site amenable to direct repair, with good results.
Of the various investigational diagnostic modalities available, endoanal ultrasound has been superior, though not perfect. In 1 series, endoanal sonography detected anal sphincter tears in 35% of primiparous and 40% of multiparous women; of these, 13% and 23%, respectively, had symptoms of fecal incontinence or urgency.4
The pudendal nerve is susceptible to traction injury from childbirth and chronic straining. In a prospective study of the effect of vaginal deliveries on the pelvic floor, 80% of primigravidas sustained reversible pudendal nerve damage—which, in some women, persisted for up to 5 years.5
Obstetric risk factors include:
- infant weighing more than 4,000 g,
- use of forceps,
- prolonged second stage of labor,
- midline episiotomy,
- occipitoposterior position, and
- failed detection or suboptimal repair of anal sphincterinjuryat the time of vaginaldelivery.
Onset of menopause and subsequent pelvic floor weakness and perineal descent aggravates this occult neuropathy.
Minor incontinence is also common in patients with advanced age, internal sphincter defects, prolapsing hemorrhoids, rectal prolapse, and fecal impaction (the rectum chronically distends with feces, continuously inducing internal anal sphincter relaxation and resulting in leakage of stool).
Evaluation: Directed history, 4-point physical exam
A directed history helps indicate which diagnostic tests are most relevant. Establish severity and frequency of fecal incontinence, presence of fecal urgency, pad use, type of incontinence (solid, liquid, or gas), and presence of associated urinary incontinence and prolapse.
Obstetric history should identify:
- parity,
- duration of the second stage of labor,
- occipitoposterior presentation,
- use of forceps,
- extent of vaginal lacerations, and
- weight of the infant.
Dietary habits (especially fiber intake) and chronic laxative use should be noted.
Also note any history of abdominopelvic surgery, radiation, back injury, and neurologic disorders.
4-point physical exam
- Inspect the perineum/perianal area for evidence of dermatitis, infection, fistula, hemorrhoids, and deformities of the anus. Ask the patient to bear down as you look for evidence of pelvic floor weakness and rectal prolapse.
- Assess the anal wink (cutaneoanal contractile reflex) by stroking the skin surrounding the anus. Absence of a reflexive contraction of the external anal sphincter suggests nerve damage or spinal arc interruption.
- Perform a vaginal exam to identify pelvic prolapse and exclude rectovaginal fistula. At this time assess pelvic muscle strength and teach the patient proper pelvic floor exercises.
- Conduct a digital rectal examination to assess the length and orientation of the analcanal, bulk of the perianal tissues, and tone of the anal sphincters, as well as to rule out a mass or impaction. Repeat digital examination with the patient bearing down to assess the squeeze pressures, movement of the puborectalis muscle, and extent of pelvic floor descent.
These findings are predominantly subjective and depend on operator experience. In general, they correlate poorly with objective measurements of sphincter pressures.6
If a rectovaginal fistula is suspected, try retrograde filling of the rectum with 200 cc of dye-stained fluid (using a 50-cc catheter tip syringe), then observe vaginal extravasation.