IN THIS ARTICLE
<huc>Q</huc> What’s your diagnosis?
A 24-year-old woman at 22 weeks’ gestation came to OB triage with abdominal pain, nausea, and vomiting. She said that sharp pain began the night before, starting at the umbilicus and radiating toward her right side. She rated her pain level at 7. She felt no contractions and had no vaginal bleeding, fluid leaking, or dysuria. She had GERD at times and chills the day before, but no fever. Similar pain 1 month before had resolved spontaneously, and no cause was determined. She had no notable personal or family medical history. On examination, she was afebrile, normotensive, and in no apparent distress. Heart and lungs were normal. Her abdomen was soft and gravid with a fundal height of 22 cm. Bowel sounds were present in all 4 quadrants. Fetal heart tones were normal, and there was no indication of contractions. Her abdomen was diffusely tender, with significant tenderness to deep palpation in the right upper quadrant at first. There was no rebound or guarding. The psoas sign was negative. The obturator sign was positive, with increased pain, level 4, in the right lower quadrant. There were no abdominal masses. Digital rectal examination found no masses, and a guaiac stool test was negative. A few hours later, the tenderness seemed to move toward the right lower quadrant (FIGURES 1 AND 2).
FIGURE 1 Ultrasound of RLQ

Ultrasound view of the right lower quadrant with cecum labeled.
FIGURE 2 A second ultrasound of RLQ

A second, graded compression ultrasound was obtained, rather than a CT study, to avoid exposing the fetus to radiation.
<huc>A</huc> The most likely diagnoses are cholecystitis and appendicitis, given the location of the pain and the lack of vaginal bleeding.
Diagnostic imaging and radiation exposure
We performed laboratory analyses, including a complete blood count, chemistry panel including electrolytes and liver function studies, amylase, lipase, and a urinalysis. The test results were all normal. Her white blood cell count was 15,000/mL, which can be normal in pregnancy.
Differential diagnosis of abdominal pain in pregnancy
| Placental abruption |
| Cholecystitis |
| Pancreatitis |
| Appendicitis |
| Intussusception |
| Pyelonephritis |
| Round ligament syndrome |
| Hydronephrosis |
| Ovarian torsion |
| Uterine fibroid degeneration |
| Ovarian cysts or tumors |
| Intra-abdominal and rectus muscle abscess |
| Crohn’s disease with diffuse peritoneal inflammation |
Gallstones ruled out
The initial evaluating physician had obtained a right upper quadrant ultrasound, which showed no gallstones or bilateral hydronephrosis.
Unfortunately, no attempt was made to visualize the right lower quadrant or appendix at that time.
In light of the physical exam findings and the absence of gallstones, the patient was admitted to rule out appendicitis. The surgery team at the university hospital was consulted. They requested a computed tomography (CT) scan of the abdomen with and without contrast. To avoid the risk of radiation to the fetus, another ultrasound was obtained. The ultrasound showed an enlarged and inflamed appendix with a transverse diameter of 13 mm (normal is <6 mm) (FIGURES 3 AND 4).1
Graded compression was used to assess the appendix. This involves using pressure of the ultrasound probe, starting above the area of tenderness and working toward the tender area while scanning for the appendix. This showed obvious peristalsis in the cecum and no movement within the appendix, indicating obstruction or inflammation.
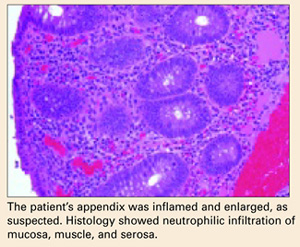
Open appendectomy was performed. The appendix was inflamed and enlarged. Histology showed neutrophilic infiltration of mucosa, muscle, and serosa (BOX).
Postoperatively, the patient recovered in the labor and delivery unit, to monitor for possible preterm labor. She did not develop any signs or symptoms of preterm labor, and was transferred to an antepartum unit after 6 hours of observation.
She did well during hospitalization, and was sent home on post-op day 2. Her abdominal pain had resolved, and she had very little post-op tenderness.
FIGURE 3 Appendix: Longitudinal view
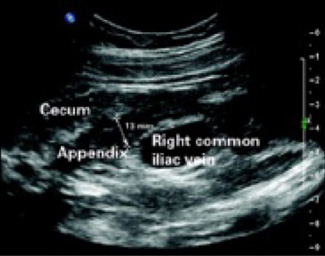
Longitudinal view by ultrasound of enlarged appendix with diameter equal to 13 mm (normal is <6 mm).
FIGURE 4 Appendix: Transverse view

Transverse view of inflamed appendix by ultrasound with wall thickening. Ultrasound showed peristalsis in the cecum and no movement in the appendix, indicating obstruction or inflammation.
Treatment of acute appendicitis in pregnancy

Is appendectomy avoidable? The treatment for nonperforated acute appendicitis in pregnancy is appendectomy.
Which approach? In the first trimester, a laparoscopic appendectomy may be performed.2
Antibiotics. Intravenous antibiotics are indicated with perforation, peritonitis, or abscess formation.2,5
Tocolysis. Though unnecessary in uncomplicated appendicitis, tocolysis may be indicated if the patient goes into labor after surgery.
Cesarean. In the late third trimester, with perforation or peritonitis, a cesarean section is indicated.