FIGURE 1 Hallmarks of a benign cyst
Cysts with smooth borders and without septations, excrescences, or solid parts are likely to be benign.
Management options for premenopausal patients
CASE What is the next step?
In Mrs. M’s case, the first option should be observation and a repeat sonogram in about 2 weeks. Analgesics and rest can be helpful to control pain. Reassure her that the pain should diminish in a few days, although it sometimes takes longer.
Skip the birth control pills
Even with unilocular cysts presumed to be follicular, oral contraceptives do not speed resolution. When 80 premenopausal women with 3- to 6-cm unilocular cysts were randomized to no therapy, low-dose oral contraceptives, or high-dose oral contraceptives and followed with sonography, resolution rates were the same in all 3 groups after 10 weeks.7 Almost 90% of the cysts had resolved after 5 weeks, even in women not taking oral contraceptives.
Pain may warrant surgery
In rare cases, a woman may have such severe pain that rest and analgesics are ineffective, and surgery is warranted for pain alone. In other cases, a cyst that appears functional or hemorrhagic on sonography but persists more than 8 weeks may justify removal to rule out neoplasia.
Intraoperative considerations
After the laparoscope and any accessory cannulas are inserted, wash the pelvis and upper abdomen with saline and collect a sample for cytologic analysis. Carefully assess the pelvis and upper abdomen; any peritoneal excrescences or thick adhesions to the mass should be noted, biopsied, and sent for frozen section.
Make every effort to save the ovary
In a premenopausal woman with a presumptively benign ovarian cyst who requires surgery for pain or because the cyst fails to resolve, surgery should aim to conserve the ovary, if at all possible. Even with a large cyst (6 cm or larger), ovarian conservation is possible. Laparoscopic surgery, which involves a short hospital stay and faster postoperative recovery, should be considered unless neoplasia is suspected.
Keep the cyst intact if possible
After placing the cannulas and assessing the pelvis and abdomen, grasp the utero-ovarian ligament with an atraumatic grasper to bring the ovary into view. Inspect the ovary and desiccate (with monopolar cautery) a 1-cm area of thick ovarian capsule, preferably on the less vascular, antimesenteric portion of the ovary.
Using the laparoscopic scissors, incise the capsule superficially along the long axis of the ovary, exposing the cyst wall below. Grasp the edge of the ovarian capsule with a 5-mm grasping forceps. Insert an irrigating instrument between the cyst wall and the ovarian capsule. Use a high-pressure stream of fluid and the blunt edge of the instrument to dissect the cyst away from the ovary.
Keep the cyst intact as long as possible to facilitate dissection. Once the cyst is as free as possible, incise and empty it using the suction irrigator. Grasp the cyst wall with the 5-mm ovarian biopsy forceps and the ovary itself with an atraumatic grasper. Using traction and countertraction, tease the cyst away from the ovarian capsule.
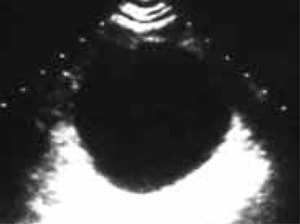
FIGURE 2 Hemorrhagic cyst at detection

Hemorrhagic cysts may have internal echoes, a sign of blood clots within the cyst.
...and 2 weeks later

Two weeks later the cyst is smaller and the clots are in the process of reabsorption.A cyst usually can be removed intact from the abdominal cavity through a 5- or 11-mm canula. If it is too large, bisect it prior to removal.
After removal, inspect the cyst for papillations, septa, or thickening of the wall. If malignancy is suspected, send the cyst for frozen section. If malignancy is confirmed, be prepared to proceed with staging laparotomy immediately.
Postmenopausal women
CASE Is a 4-cm cyst likely to be cancer?
Mrs. J, 67, visits her internist complaining of dull, achy abdominal pain associated with some bloating. A pelvic sonogram reveals a 4.1-cm cyst of the right ovary with well-defined borders; no septations, excrescences, or solid parts; and no free fluid in the pelvis. The left ovary is 3 cm and appears normal. The internist refers Mrs. J to you for further evaluation and management.
By the time you see her, Mrs. J is experiencing very little pain and bloating. However, she is concerned about the cyst and worries that she may have ovarian cancer. She has not experienced any increased abdominal girth, change in appetite or weight, or vaginal bleeding.
When you examine her, you find a normal abdomen with no ascites or abdominal mass. The pelvic exam is normal, too, except for a nontender, slightly enlarged right adnexa, which is difficult to palpate fully.