Advances in wound management offer help and promise
Vacuum-assisted closure
The vacuum-assisted wound closure system is a device that speeds healing and reduces the risk of complication. It consists of a sponge dressing that can be sized to fit an open wound and connected to an apparatus that generates negative pressure. The device enhances healing by removing excess fluid and debris and decreasing wound edema.
Argenta and associates reported successful use of this system to expedite healing in three cases of wound failure.16 It can be employed in the home-health setting by nurses trained in its use.
Human acellular dermal matrix
Occasionally, breakdown of a wound creates marked fascial defects that preclude secondary closure. Synthetic materials—both absorbable and nonabsorbable varieties—have been employed to bridge the defect, but their use sometimes leads to adhesions, infection, and cutaneous fistula. These risks are of special concern when the wound is already contaminated or otherwise compromised.
One alternative is human acellular dermal matrix (AlloDerm, LifeCell Corp). Tung and colleagues described its use for repair of a fascial defect in a previously irradiated cancer patient whose postoperative course was complicated by pelvic infection.17 This dermal matrix, a basement membrane taken from cadaveric skin, promotes neovascularization and is thought to be associated with a lower incidence of infection and adhesions than is traditional mesh. It is widely used in the burn setting and in the repair of ventral hernia, but is a relatively new addition to the management of fascial defects associated with wound breakdown.
Growth factors
Wound healing is regulated by a number of entities, including cytokines and growth factors, so it is no surprise that research has turned its focus on them. In a preliminary study, investigators found that separated abdominal wounds closed faster when recombinant human platelet-derived growth factor BB was topically administered than they did when they were left open to close by secondary intention.18
Although their use is not commonplace in wound management, research suggests that growth factors may one day be helpful adjuncts in the care of wound complications.
Complete fascial dehiscence is a “catastrophic” complication
Complete dehiscence of the fascia and extrusion of intra-abdominal contents is a serious catastrophic complication that is associated with a mortality rate of about 20%. It typically occurs between the third and seventh postoperative days, although later occurrences have been reported.
Warning signs of impending evisceration include serous drainage in the absence of obvious infection, and a “popping” sensation on the part of the patient—a feeling that something is “giving way.”
If evisceration occurs, cover exposed bowel with packs soaked in saline or povidone-iodine and prepare the patient for emergency surgery. Institute both hydration and broad-spectrum antibiotics.
Before replacing the abdominal contents, thoroughly irrigate the peritoneal cavity and inspect the bowel carefully, excising any necrotic tissue.
Reapproximate the fascia using interrupted #1 or #2 monofilament suture. Also consider placing retention sutures, particularly when the patient has multiple risk factors for wound complications (FIGURE). Leave the wound open, prepared for later closure.
If the abdomen cannot be closed because of peritonitis or bowel edema, or there is an insufficient amount of fascia remaining, approximate the abdominal wall using bridging sutures over a gauze pack as a temporizing measure until reconstruction can be performed. Consultation with a plastic surgeon or trauma specialist is recommended.
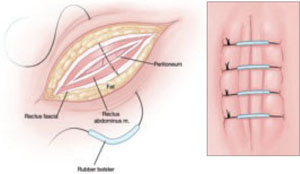
FIGURE Consider retention sutures for high-risk patients
Retention sutures are placed in interrupted fashion to support the primary suture line and are carried through the full thickness of the tissue, from the abdominal wall skin through the fascia and, if possible, the peritoneum. A rubber bolster placed across each suture keeps the suture from cutting into the skin (inset).
Necrotizing fasciitis: Worst of the worst
Necrotizing fasciitis is a dangerous, synergistic, bacterial infection involving the fascia, subcutaneous tissue, and skin. The culprits are multiple bacterial pathogens that include Streptococcus pyogenes, staphylococcal species, gram-negative aerobes, and anaerobes. The infection typically originates at a localized area, spreads along the fascial planes, and ultimately causes septic thrombosis of the vessels penetrating the skin and deeper layers. The result is necrosis. The associated mortality rate is approximately 20%.
The patient who has necrotizing fasciitis typically displays severe pain; anesthetic, edematous skin; purple, necrotic wound edges; hemorrhagic bullae; and crepitus.
Frank necrosis subsequently develops, with surrounding inflammation and edema, and leads to systemic toxicity, with fever, hemodynamic abnormality, and shock. In advanced stages, gangrene is present.
Laboratory evaluation includes a white blood cell count. Biopsy also is recommended. If necrotizing fasciitis is present, biopsy will reveal necrosis and thrombi of vessels passing through the fascia.