When I arrive as an emergency responder to a shoulder dystocia delivery, my preferred maneuver is to deliver the posterior arm. Many experts recommend prioritizing this maneuver when attempting to resolve a difficult shoulder dystocia.4-7
Delivery of the posterior arm is performed by inserting the hand and forearm into the sacral hollow. The left hand and forearm are used if the fetal spine is toward the mother’s left, and vice-versa. The posterior humerus is identified and followed to the elbow. The fetal forearm is flexed and swept across the fetal chest. The wrist or hand is then grasped and the arm is extended along the fetal trunk and face, which delivers the posterior arm from the vagina. This results in a reduction in the presenting diameter and the anterior shoulder usually can be delivered with minimal force.
If the delivery of the posterior arm does not resolve the shoulder dystocia, gently support the fetal head and posterior arm, and rotate the fetus 180° using pressure on the posterior surface of the shoulder.
When a fetus is macrosomic, the posterior arm can be fully extended in utero, with the hand below the level of the fetal groin. In such situations, it can be difficult to execute the delivery of the posterior arm.8 A back-up technique is to manipulate the posterior axilla to accomplish delivery.
Manipulation of the posterior axilla
One of the earliest written descriptions of resolving a severe shoulder dystocia by manipulating the posterior axilla was provided by Percival Willughby (born 1596, died 1685). He wrote:
- “After the head is born, if the child through the greatness of the shoulders, should stick at the neck, let the midwife put her fingers under the child’s armpit and give it a nudge, thrusting it to the other side with her finger, drawing the child or she may quickly bring forth the shoulders, without offering to put it forth by her hands clasped about the neck, which might endanger the breaking of the neck.”9
Manipulation of the posterior axilla can either involve a rotational maneuver (using the axilla to rotate the fetus through 180°) or it can be used to pull the posterior shoulder into the hollow of the sacrum and down the birth canal.
Schramm advocated using the posterior axilla to rotate the fetus. She recommended placing 1 or 2 fingers of the right hand in the posterior axilla and then rotating the posterior shoulder into the 12 o’clock position while simultaneously using the left hand to provide gentle guidance on the fetal neck.10
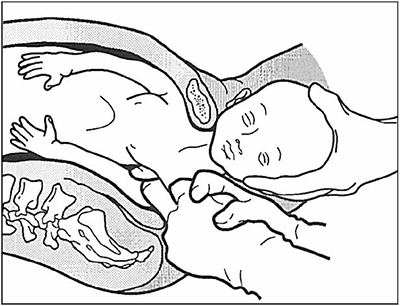
Menticoglou advocated using manipulation of the posterior axilla to draw the fetal shoulder into the sacral hollow and down the birth canal, thereby releasing the anterior shoulder. In the Menticoglou maneuver the middle fingers of the right and left hand of the obstetrician are hooked into the fetal axilla, one finger from the fetus’ front and the other from the fetus’ back. The fingers overlap each other within the fetal posterior axilla. Downward traction is then exerted on the fetal axilla and the posterior shoulder is pulled outward along the curve of the sacrum (FIGURE).11
Sandmire recommended combining fundal pressure with axillary traction and rotation to facilitate delivery.12
The posterior axillary maneuvers are seldom described in modern textbooks of obstetrics and represent a lost art. I have found that they can be useful when the posterior arm cannot be reached. The fetal posterior axilla is almost always closer to the vaginal introitus than the fetal hand or arm, and if the posterior arm cannot be reached, it is a valuable maneuver to have in your armamentarium.
Manipulation of the posterior axilla
The right and left third fingers are locked into the posterior axilla, one finger from the front and one from the back of the fetus. Gentle downward guidance is provided by the fingers to draw the posterior shoulder down and out along the curve of the sacrum, thus releasing the anterior shoulder. In this drawing, an assistant gently holds the head up.
(Menticoglou SM. A modified technique to deliver the posterior arm in severe shoulder dystocia. Obstet Gynecol. 2006;108:755–757. Reprinted with permission from Wolters Kluwer.)
Shoulder dystocia emergencies are an important cause of neonatal injury, including brachial plexus injury, fractures of the humerus, and hypoxic-ischemic encephalopathy. Obstetricians and midwives relentlessly train to resolve shoulder dystocia births with alacrity and minimal fetal trauma. When you are called as an emergency responder in a shoulder dystocia birth, I recommend that you prioritize a rotational maneuver or delivery of the posterior arm, and add manipulation of the posterior axilla to your armamentarium.