Ms. M, age 71, was diagnosed with Alzheimer’s disease several months ago and her clinical presentation and Mini-Mental Status Exam score of 22 indicates mild dementia. In addition to chronic medications for hypertension, Ms. M has been taking lorazepam, 1 mg, 3 times daily, for >15 years for unspecified anxiety.
Ms. M becomes more confused at home over the course of a few days, and her daughter brings her to her primary care physician for evaluation. Recognizing that benzodiazepines can contribute to delirium, the physician discontinues lorazepam. Three days later, Ms. M’s confusion worsens, and she develops nausea and a tremor. She is taken to the local emergency department where she is admitted for benzodiazepine withdrawal and diagnosed with a urinary tract infection.
Because dementia is a strong risk factor for developing delirium,1 withdrawing or changing
medications to rule out delirium in patients with mild dementia, such as Ms. M, is a common clinical scenario. Although delirium often is multifactorial, medications are frequent predisposing and precipitating factors and contribute to approximately 12% to 39% of delirium cases.1,2 A recently initiated medication is more likely to be a precipitant for delirium; however, long-term medications can contribute to delirium and should be evaluated to determine if they can be discontinued in a patient with symptoms consistent with delirium.1Consider withdrawing or replacing medications that are strongly implicated in causing delirium with another medication for the same indication with a lower potential for
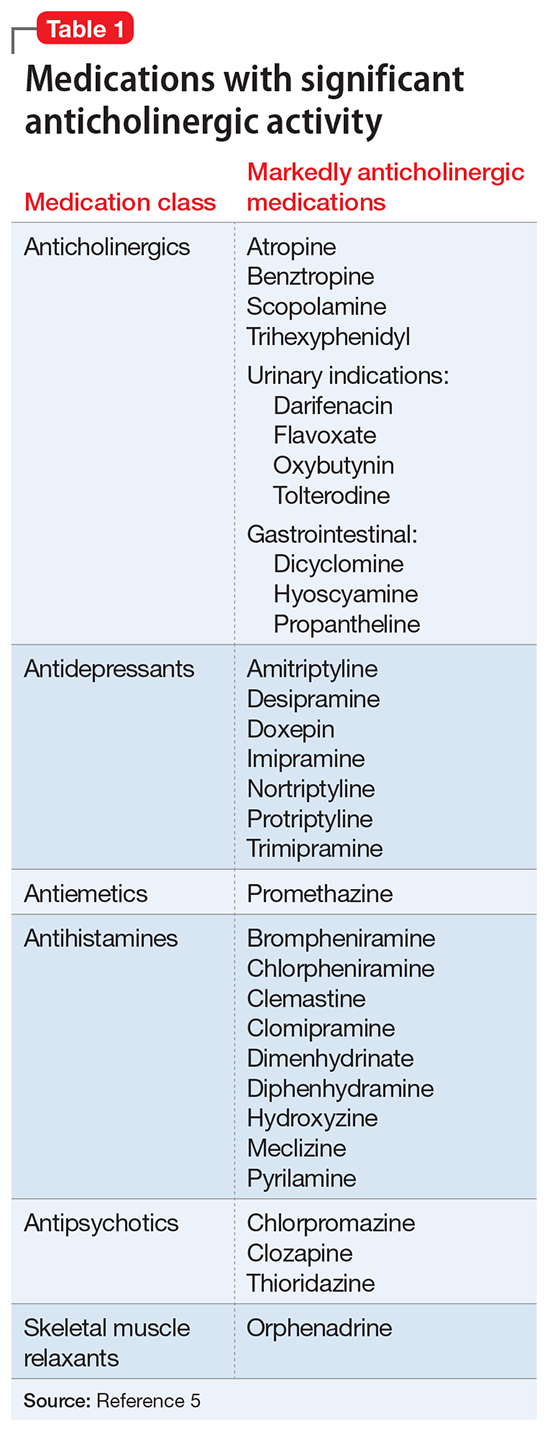
precipitating or exacerbating delirium. Benzodiazepines and opioids are medications most clearly associated with an increased risk for delirium,3 although medications with significant anticholinergic properties have been associated with increased severity of delirium in patients with and without underlying dementia4 and are consistently cited as common causes of drug-induced delirium.1,2 Table 15 lists medications that are known to be anticholinergic. The 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults added non-benzodiazepine receptor agonist hypnotics (ie, zolpidem, zaleplon, and eszopiclone) as medications to avoid in patients who have dementia because of adverse CNS effects.6 These drugs also would be appropriate targets for withdrawal or modification in patients with mild dementia and suspected delirium.