Edwin R. Raffi, MD, MPH Instructor in Psychiatry Harvard Medical School Center for Women’s Mental Health Massachusetts General Hospital Boston, Massachusetts
Marlene P. Freeman, MD Associate Professor in Psychiatry Harvard Medical School Associate Director Center for Women’s Mental Health Massachusetts General Hospital Boston, Massachusetts
Disclosures Dr. Raffi reports no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products. Dr. Freeman has received research support from JayMac, Sage, and Takeda; and has served on advisory boards for Janssen, JDS Therapeutics, and Sage. Dr. Freeman is an employee of Massachusetts General Hospital (MGH) and works with the MGH Pregnancy Registry; this registry is sponsored by Alkermes, Forest/Actavis, Otsuka, and Sunovion. As an employee of MGH, Dr. Freeman works with the MGH Clinical Trials Network and Institute, which has received research funding from multiple pharmaceutical companies and the National Institute of Mental Health.
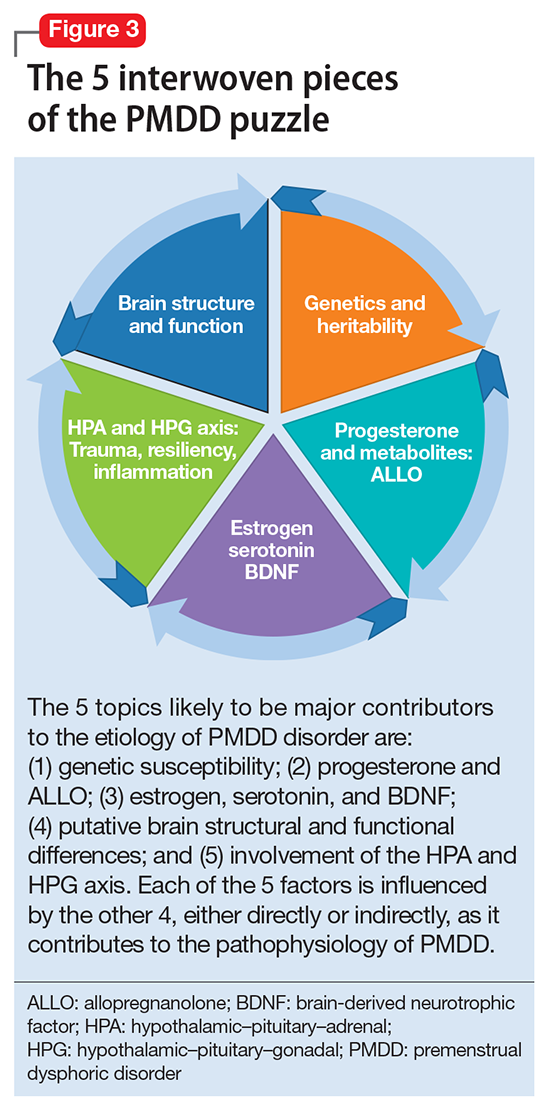
The many variables that contribute to the pathophysiology of PMDD overlap and should be considered connecting pieces in the puzzle that is the etiology of this disorder (Figure 3). In reviewing the literature, we have identified 5 topics likely to be major contributors to this disorder:
genetic susceptibility
progesterone and allopregnanolone (ALLO)
estrogen, serotonin, and brain-derived neurotrophic factor (BDNF)
putative brain structural and functional differences
further involvement of the hypothalamic–pituitary–adrenal (HPA) axis and hypothalamic–pituitary–gonadal (HPG) axis: trauma, resiliency, and inflammation.
Genetic susceptibility. PMDD is thought to have a heritability range between 30% to 80%.3 This is demonstrated by family and twin studies4-7 and specific genetic studies.8 The involvement of genetics means an underlying neurobiologic pathophysiology is in place.
Estrogen receptor alpha (ESR1) gene. Huo et al8 found an associated variation in ESR1 in women with PMDD compared with controls. They speculated that because ESR1 is important for arousal, if dysfunctional, this gene could be implicated in somatic as well as affective and cognitive deficits in PMDD patients. In another study, investigators reported a relationship between PMDD and heritable personality traits, as well as a link between these traits and ESR1 polymorphic variants.1 They suggested that personality traits (independent of affective state) might be used to distinguish patients with PMDD from controls.1
Studies on serotonin gene polymorphism and serotonin transporter genotype. Although a study of serotonin gene polymorphism did not find an association between serotonin1A gene polymorphism and PMDD, it did show that the presence of at least 1 C allele was associated with a 2.5-fold increased risk of PMDD.9 Another study did not find an association between the serotonin transporter genotype 5-HTTLPR and PMDD.10 However, it showed lower frontocingulate cortex activation during the luteal phase of PMDD patients compared with controls, suggesting that PMDD is linked to impaired frontocingulate cortex activation induced by emotions during the luteal phase.10
Seasonal affective disorder (SAD) and PMDD have shared clinical features. A polymorphism in the serotonin transporter promoter gene 5-HTTLPR has been associated with SAD. One study found that patients with comorbid SAD and PMDD are genetically more vulnerable to comorbid affective disorders compared with patients who have SAD only.11