Jean Lud Cadet, MD Senior Investigator Chief, Molecular Neuropsychiatry Research Branch National Institute on Drug Abuse Intramural Research Program Baltimore, Maryland
Mark Gold, MD Adjunct Professor of Psychiatry Washington University School of Medicine St. Louis, Missouri Chair, Scientific Advisory Boards RiverMend Health Atlanta, Georgia
Disclosures The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Treatment needs to take into account persistent cognitive impairment and comorbid disorders
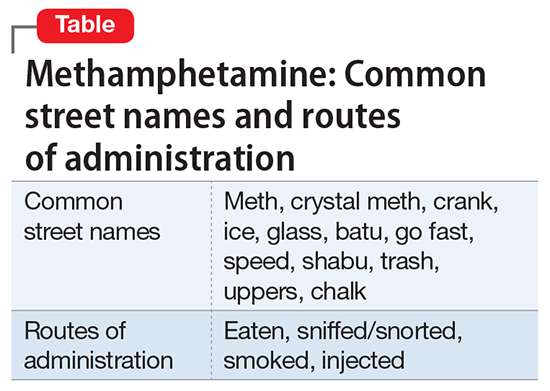
Use of methamphetamine, an N-methyl analog of amphetamine, is a serious public health problem; throughout the world an estimated 35.7 million people use the drug recreationally.1 Methamphetamine is easy to obtain because it is cheap to produce and can be synthesized anywhere. In the United States, methamphetamine is commonly manufactured in small-scale laboratories using relatively inexpensive, legally available ingredients. Large-scale manufacturing in clandestine laboratories also contributes to methamphetamine abuse. The drug, known as meth, crystal meth, ice, and other names, is available as a powder, tablet, or crystalline salt, and is used by various routes of administration (Table).
The basis for methamphetamine abuse/dependence lies with the basic biochemical effects of the drug on the brain, where it functions as a potent releaser of monoamines,2 including dopamine, in brain regions that subsume rewarding effects of various substances, including food and sexual activities.3 These biochemical effects occur through the binding of the drug to dopamine transporters and vesicular monoamine transporter 2.2
Although FDA-approved for treating attention-deficit/hyperactivity disorder, methamphetamine is taken recreationally for its euphoric effects; however, it also produces anhedonia, paranoia, and a host of cognitive deficits and other adverse effects.
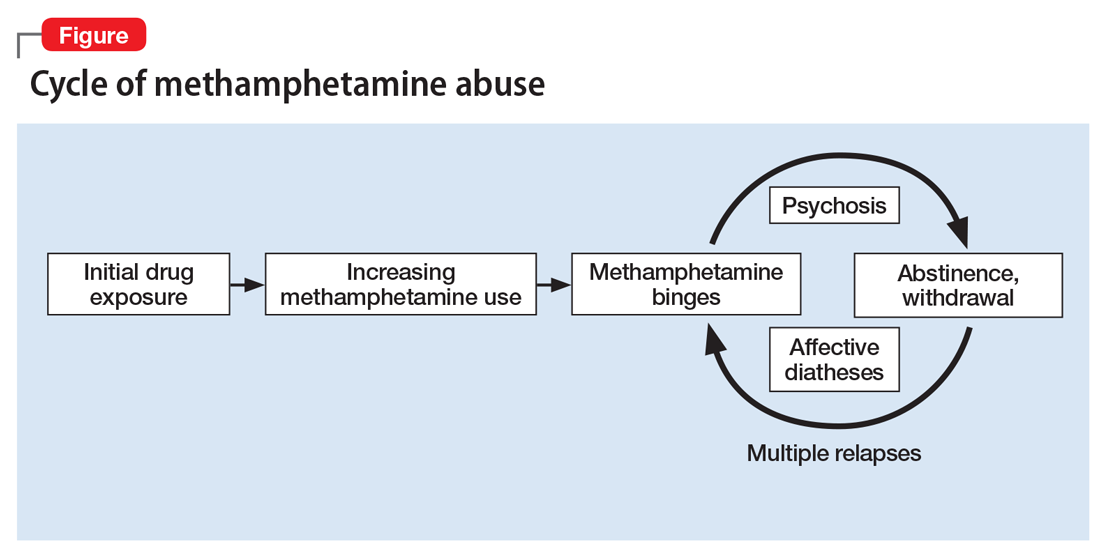
Methamphetamine causes psychiatric diseases that resemble naturally occurring illnesses but are more difficult to treat. Dependence occurs over a period of escalating use (Figure). Long-term exposure to the drug has been shown to cause severe neurotoxic and neuropathological effects with consequent disturbances in several cognitive domains.4
Despite advances in understanding the basic neurobiology of methamphetamine-induced effects on the brain, much remains to be done to translate this knowledge to treating patients and the complications that result from chronic abuse of this stimulant. In this review, we:
provide a brief synopsis of the clinical presentation of patients who use methamphetamine
describe some of the complications of methamphetamine abuse/dependence, focusing on methamphetamine-induced psychosis
suggest ways to approach the treatment of these patients, including those with methamphetamine-induced psychosis.