Clinical implications
Nonadherence with oral antipsychotics is a common problem for patients with schizophrenia, one that is often underappreciated by clinicians.5 Whether one uses 70% or 80% as the measure of oral medication adherence, at least 50% of schizophrenia patients are nonadherent, with resultant increased risks for symptom exacerbation and hospitalization.5,6 Although 2 LAI forms of aripiprazole have been introduced over the past few years, neither was designed to be loaded, resulting in the need for 2 or 3 weeks of oral antipsychotic coverage following the first injectable dose.1 The primary reason for LAI antipsychotic therapy is oral medication nonadherence, and thus the need for 14 to 21 days of oral coverage at the outset of treatment creates a risk for symptom exacerbation if the patient is nonadherent with this oral bridging therapy which is needed to achieve the necessary serum concentrations until the long-acting formulation takes over.
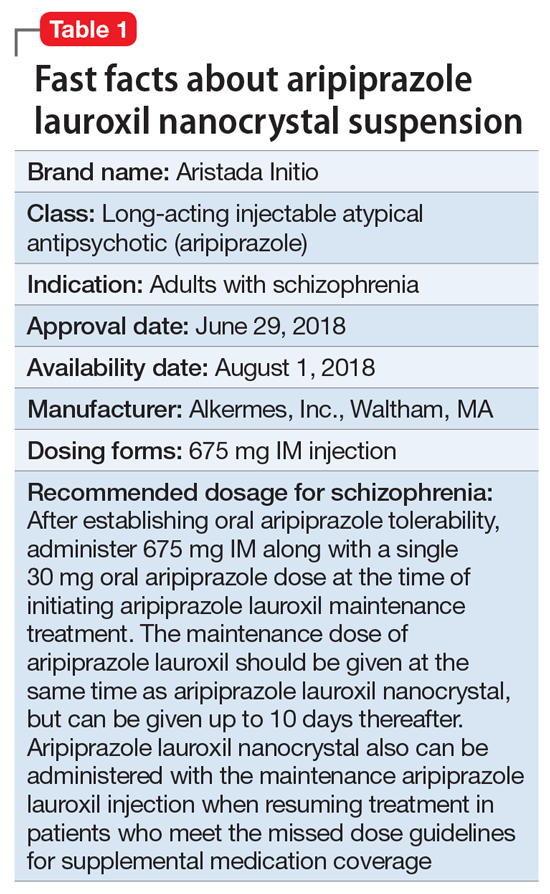
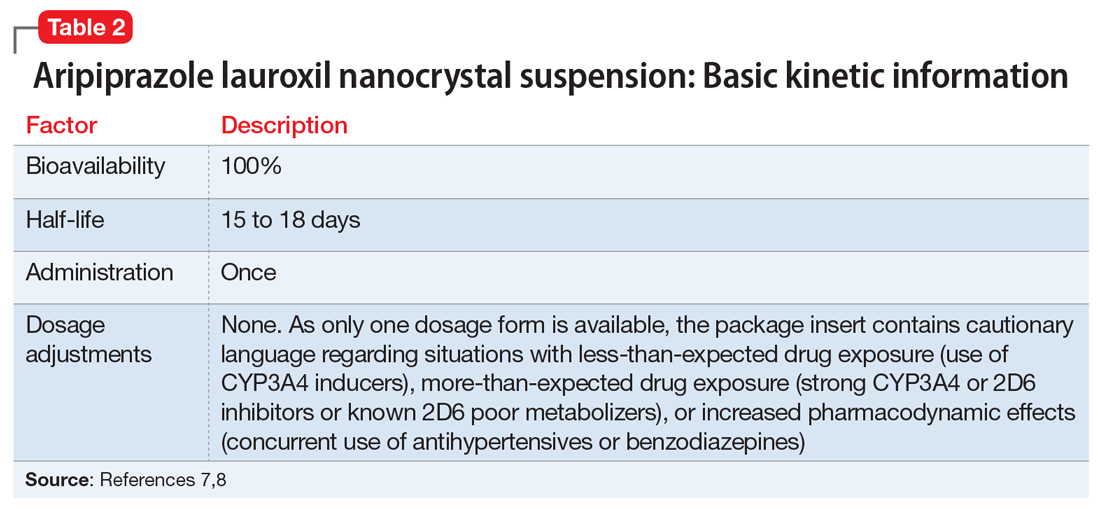
One approach was to create a new form of AL using smaller nanomolecular particles rather than the micron-sized particles used for maintenance AL injections.3,4 This nanocrystal suspension is called Aristada Initio (ALncd) and has a median Tmax that ranges from 16 to 35 days, compared with 41 days for single-dose injections of AL. ALncd also has a much shorter median half-life of 15 to 18 days, compared with 53.9 to 57.2 days for AL (Table 27,8). Utilizing these kinetic differences, a 1-day initiation regimen was developed to dispense with the need for 3 weeks of oral medication coverage when commencing AL treatment.3,4 In lieu of 3 weeks of oral coverage starting at the time of the first AL injection, patients instead will receive an injection of ALncd 675 mg, and a single oral 30 mg aripiprazole dose. The combination of ALncd and the single 30 mg oral dose when added to the initial AL injection provides aripiprazole levels in the first weeks of therapy that are comparable to those seen in the previous paradigm, when patients took 21 days of oral aripiprazole after the first AL injection.3
Use in adults with schizophrenia. After establishing tolerability with oral aripiprazole, ALncd675 mg is administered as an IM injection by a health care professional, and the patient is concomitantly given a single 30 mg oral dose of aripiprazole. Only one dosage form of ALncd is available: 675 mg. The maintenance AL dose chosen by the clinician (441, 662, 882, or 1,064 mg) is also administered at the same time, but must be injected in the other deltoid or gluteal muscle. The injection volume for ALncd is 2.4 mL and can be administered in the deltoid or gluteus muscle.9 If the patient prefers not to have 2 injections on the same day, the AL dose can be administered up to 10 days thereafter.9 This 10-day window for administering AL relates to the long time to maximum plasma levels from single AL injections. The relevant drug levels during the first weeks are provided predominantly from the initiation regimen of ALncd injection plus the single 30 mg oral dose.3 In instances when a patient agrees to receive both ALncd and AL injections but refuses the 30 mg oral dose, effective plasma levels will be seen in the middle of the second week of therapy.
Continue to: Pharmacologic profile, adverse reactions