CASE CONTINUED: Boy troubles
Kate tells you that in 9th grade she and her best friend, Ellen, would talk about boys for hours after school and try on sexually provocative outfits. They both liked Matt, a 10th grader, so when he asked Kate out, Ellen stopped speaking to her. Kate and Matt began some heavy petting, and Kate said she felt selfish and guilty about hurting Ellen. But when girls at school began spreading rumors that Kate was a “slut,” Kate blamed Ellen and told her, “I hate you!”
Soon after, Matt broke up with Kate. Distraught, she dreaded going to school and cried in her room at night for several weeks. She became chronically tired and had difficulty concentrating in class. She ruminated about losing Matt and worried that she was too fat, too ugly, or too flat-chested. She missed Ellen and felt no one liked her.
Table 2
Puberty’s developmental milestones in U.S. girls (averages)
| Correlate | African Americans | Whites | School grade* |
|---|---|---|---|
| Breast bud development | Age 9 | Age 10 | 4th to 5th |
| Girls with puberty onset by age 8 | 32% | 11% | 3rd |
| Girls with puberty onset by age 10 | 76% | 53% | 5th |
| Menarche onset | Age 12.1 | Age 12.6 | 7th |
| Tanner stage 5† onset | Age 13.9 | Age 15.5 | 8th to 9th |
| * Approximate grade level for age groups | |||
| † Pubic hair and breast development reach adult stage | |||
| Source: Data from references 6-9, including the Pediatric Research in Office Settings network and Third National Health and Nutrition Examination Survey, 1988-1994. | |||
Figure Hypothalamic-pituitary-ovarian axis: Turned on at puberty in girls
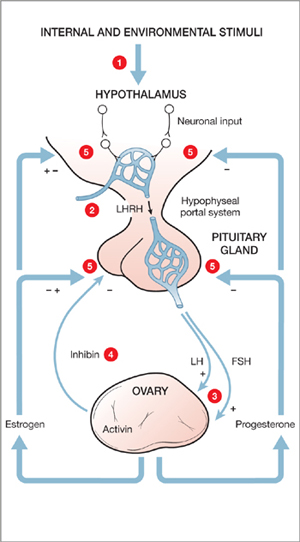
Puberty onset stimulates depression in genetically vulnerable girls; more likely after Tanner stage 3 (development of pubic and axillary hair and breast buds).
Male vs female teen brains
Depression after a relationship failure in teen girls often begins with ruminative thoughts about her flaws, mistakes, or appearance. These negative thoughts may preoccupy her day and night. Teen girls often feel confused by contradictory social pressures to look and dress provocatively but resist having sex. A sexual encounter can trigger shame and fear.
Although clinical and developmental studies indicate that teen girls respond more dramatically to relationship troubles than boys, the brain and hormone differences responsible for these effects remain unclear. Male hormones hugely increase in boys at puberty—up to 25-fold between ages 9 and 15—but do not cycle. Male brains do not have the same capacity as female brains to respond to cyclical hormonal activity because exposure to androgens during fetal development eliminates this ability. The fetal testosterone surge causes the area associated with sexual pursuit to double in the male brain.
Outside of fertility considerations, Baron-Cohen et al15 suggest that male brain circuits have been formed by fetal testosterone to focus more on systematization—which emphasizes figuring out how things work and performing tasks—rather than empathy and bonding in relationships. This difference has been shown in neuroimaging studies comparing the genders’ attentional systems.16,17 In contrast to the systematizing male brain, female brains are more likely to activate the mirror neuron system—the area required for empathizing.18
Female brains, of course, respond to cyclical hormonal activity. However, the regular monthly waves of estrogen and progesterone do not affect all female brains the same. A subset of women who experience premenstrual dysphoric disorder appear to have brains that trigger depressed moods and irritability during the last 2 weeks of the menstrual cycle.19 A genetic difference in these women is suspected as the culprit; these genes may affect the way their brains metabolize progesterone.
CASE CONTINUED: An overdose of stress
Kate’s poor concentration lingered, and her grades continued to drop. She tells you her parents were having marital problems and she did not want to bother them with her difficulties. Two days before her period was due, she learned she had failed 2 classes. That night, as she got some acetaminophen for a headache, she impulsively took the rest of the bottle.
After swallowing the pills, Kate panicked. She forced herself to vomit and tearfully told her parents what she had done. They took her to the emergency room, where she was medically stabilized, evaluated by a psychiatrist, and referred to you for outpatient treatment.
Treatment recommendations
A combination of factors—genetic, hormonal, and neurodevelopmental—probably contributed to Kate’s acute depressed mood and overdose. Thus, to treat depression in adolescent girls, emerging evidence supports:
- stabilizing hormonal fluctuations such as rapidly falling progesterone just before the start of menstrual periods with an extended-cycle contraceptive (we would try an ethinyl estradiol/levonorgestrel combination such as Seasonale®)
- treating depressive symptoms with a selective serotonin reuptake inhibitor such as citalopram, 10 mg once daily, with careful monitoring for suicidal thoughts or behavior
- providing tools to manage stress and impulsive behavior through weekly psychotherapy (such as cognitive-behavioral therapy, dialectical behavioral therapy, or supportive therapy).