Most studies of pregnant women taking fluoxetine in the first trimester have found no increased risk of obstetrical complications—including spontaneous pregnancy loss, preterm labor, or low birth weight—compared with women not taking fluoxetine. Taking fluoxetine during the third trimester may increase the risk for perinatal complications,27 although this has been inconsistently reported and requires further study. Effects of other SSRIs in the third trimester have not been systematically explored.
Case reports and one controlled study have addressed possible neonatal perinatal symptoms from in utero exposure to SSRIs.28,29 Preliminary data show no adverse neurobehavioral function in exposed neonates.26
Electroconvulsive therapy (ECT) has been proven effective for acute mania and depression, demonstrating few deleterious effects on neonates. ECT has few side effects and may be safer than drug therapy in this population. Two reviews support the efficacy and relative safety of ECT treatment during pregnancy, although more evidence is needed.30,31
RECOMMENDATIONS
Discuss pregnancy and medication risks with all bipolar women, regardless of proximal plans for pregnancy. If psychotropic medication is used, prescribe carefully during the first trimester, using the minimum number of drugs and the lowest dosages needed to restore or maintain well-being.32
Pros and cons of switching. Some clinicians may encourage a patient to taper a medication during the first trimester because of its unknown or high teratogenicity. Depending on the patient’s illness severity, this might not be the optimal decision. A more conservative option would be to switch to a lower-risk drug during pregnancy.
Lithium has both antidepressant and antimanic properties and is less teratogenic compared with first-trimester exposure to an anticonvulsant. However, if lithium has not been successful for the woman’s mania prophylaxis in the past and she has demonstrated antimanic response to an anticonvulsant, switching to lithium or another anticonvulsant is not recommended.
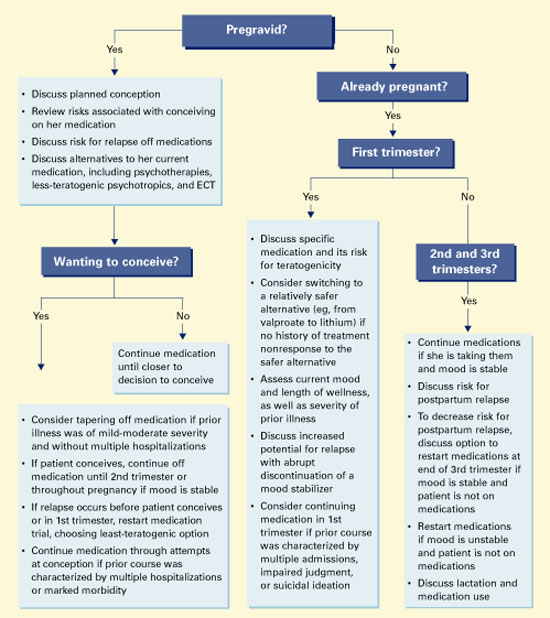
Algorithm Suggested approach to the bipolar patient who wishes to conceive or is pregnant
Folate and neural tube defects. As first-trimester exposure to carbamazepine or valproate increases the risk for neural tube defects, using the lowest available dosage may decrease the risk for spina bifida, at least with valproate.
Low maternal folate levels are often associated with neural tube defects from any cause.33 Valproate lowers folate levels by inhibiting one of the enzymes necessary for its formation, which may be a mechanism for the increased risk of spina bifida.34
Folate supplementation. To date, no study has demonstrated that giving folate supplements to women taking anticonvulsants during pregnancy reduces the risk of neural tube defects.35 Nonetheless, we recommend that women who continue to take valproate or carbamazepine during pregnancy receive folate, 3 to 4 mg/d, as a precaution.
Treating manic relapse. Data show high rates of relapse in patients who stop taking lithium, particularly if done abruptly.3 Counsel women taking lithium to plan their pregnancies to allow enough time to taper off the medication prior to conception, if they want to try this. Lithium should be decreased slowly—approximately 50% every 2 weeks—to avoid relapse.
Treat aggressively if relapse occurs during pregnancy. Consider:
- psychiatric hospitalization in case of suicidality or psychosis
- reinstituting drug therapy with a less-teratogenic agent
- ECT for a manic or depressive episode.
As the pregnancy advances and the mother’s volume of distribution increases, dosage increases may be needed to maintain therapeutic drug levels.
Treating depressive relapse. Should depression occur in pregnancy, SSRIs or tricyclics added to mood stabilizer therapy have been shown to be effective, with few teratogenic effects.
Cognitive-behavioral and interpersonal psychotherapies also have shown efficacy in pregnant women with major depressive disorder36 and may be effective for women with bipolar disorder in pregnancy. Cognitive psychotherapies, when used with medication, have been reported effective in preventing relapse in nongravid bipolar patients.36-37
Related resources
Psychiatric disorders during pregnancy. Massachusetts General Hospital Center for Women’s Health. Perinatal Resource Center. www.womensmentalhealth.org/topics/pregnancy_lib.html
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Lithobid et al
- Methylphenidate • Ritalin et al
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Phenelzine • Nardil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproate • Depakote et al
Disclosure
Dr. Altshuler receives research support from Abbott Laboratories, is a consultant to Abbott Laboratories, Forest Laboratories, and Eli Lilly & Co., and is a speaker for GlaxoSmithKline and Janssen Pharmaceutica.
Ms. Richards reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Yonkers receives research support from GlaxoSmithKline and Berlex Laboratories, is a consultant to GlaxoSmithKline, and is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Wyeth Pharmaceuticals.