Few medications remain in use 50 years after they were launched. Advances in drug development often render older drugs obsolete because newer drugs are more efficacious or safer, or both. Consider reserpine: Nowadays, no internist would use this drug to treat hypertension, even though it was the top-selling antihypertensive 50 years ago. Why? The adverse effects profile is no longer acceptable, with safer alternatives available.
Astonishingly, almost all first-generation psychotropics discovered 5 decades ago (neuroleptics, tricyclic antidepressants, monoamine oxidase inhibitors) are still on the formularies of most health care facilities and are used by many clinicians, especially those working with managed care organizations. Jails and prisons in the United States, where hundreds of thousands of seriously mentally ill patients are incarcerated, also use 50-year-old agents, without regard to the downside of older drugs on the body, brain, and quality of life of those incarcerated medically ill patients.
If clinicians who use these decades-old drugs were to keep up with medical research and advances in knowledge, we would realize what a travesty it is to use a brain-unfriendly drug such as haloperidol when we have many safer alternatives. A massive volume of knowledge has emerged over the past 15 years about the neurotoxicity of older neuroleptics, especially haloperidol—knowledge that was completely unknown before.a Second-generation antipsychotics have been shown to be much safer for the brain than their older-generation counterparts (although they are not more efficacious).
Changing awareness and changing practice
I used haloperidol for 20 years, and can vouch for its unquestionable efficacy in treating delusions and hallucinations. But I have avoided using it over the past 15 years, as the neuroscience literature about its harmful effects on brain tissue emerged and multiplied.
In addition, I came to realize that most psychiatric practitioners were unaware of the alarming deleterious neurologic effects of haloperidol—largely because the studies that reported those effects were published in neuroscience journals rarely read by practicing psychiatrists and nurse practitioners, and the pharmacists in charge of drug formularies at hospitals.
Evidence for the grave neurotoxicity of haloperidol and other older neuroleptics, compared with atypical antipsychotics, is substantial and multifaceted. The FDA would never approve haloperidol today, given the serious harm it can do to the brain, despite its efficacy for psychosis. (It’s interesting how the FDA bans a drug immediately if it causes tragic birth defects, such as thalidomide, but not if a drug is destructive to the brain tissue of a disabled adult patient. Invisible damage can be less alarming or urgent than visible damage.)
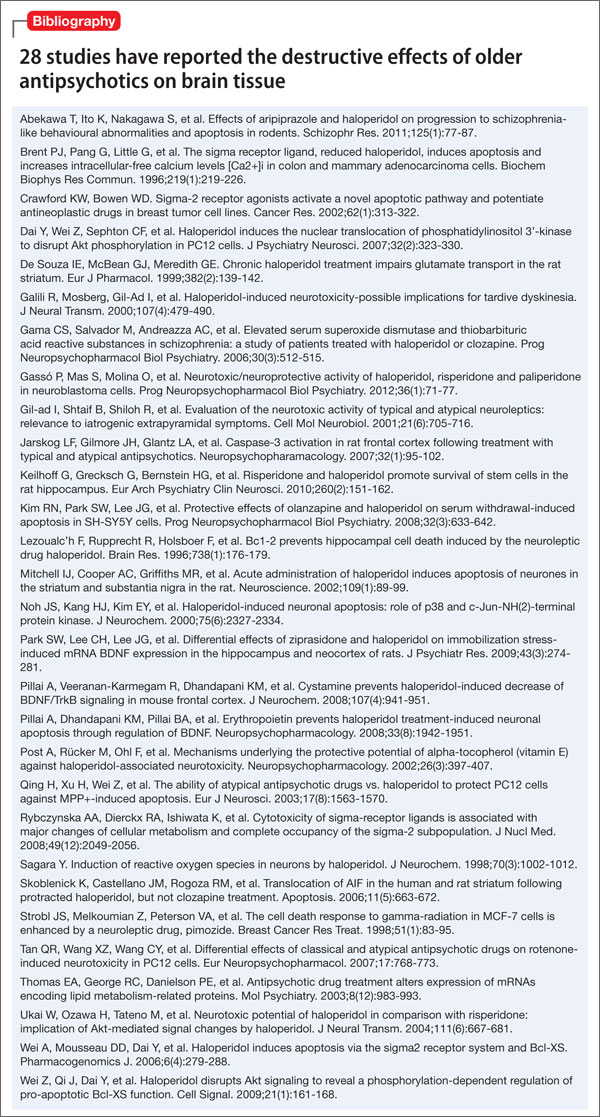
Twenty-eight studies reporting the various destructive effects of older antipsychotics (especially haloperidol) on brain tissue have been published in prominent neuroscience journals, based on work in animal models, cell culture, and post-mortem human tissue. Multiple molecular mechanisms, pathways, and cascades are involved, eventuating in neuronal death. The first review and discussion of these 28 neurotoxicity studies was presented at the annual meetings of the Society of Biological Psychiatry1 and the American Psychiatric Association2; a manuscript will soon be submitted for publication. See the bibliography below for a list of the 28 published studies.
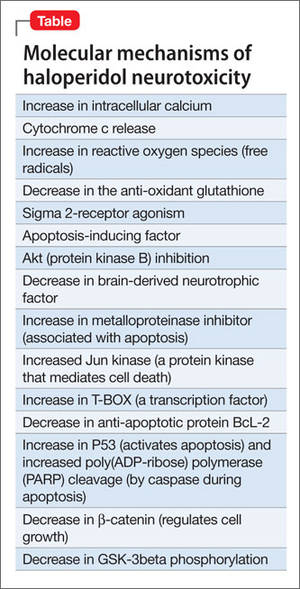
The molecular mechanisms of neurotoxicity of older-generation antipsychotics, including haloperidol, fall into several major categories:
• apoptosis
• necrosis
• decreased cell viability
• inhibition of cell growth
• increased caspase activity (the “death spiral”)
• impaired glutamate transport
• mitochondrial damage.
Examples of specific mechanisms of neurotoxicity among older-generation antipsychotics appear in this Table.
With this massive evidence of the serious neurotoxic effects of haloperidol, should it be banned? The risks of the drug far exceed the benefits—especially given the availability of 9 atypical antipsychotics that have been shown to exert neuroprotective properties, such as inducing neurogenesis and increasing neurotrophic factors.3 One of our foremost duties as medical professionals is to protect patients from harmful treatments that could exacerbate their disability. It’s time to retire this aging neuroleptic.