User login
When and how to use long-acting injectable antipsychotics
Discuss this article at www.facebook.com/CurrentPsychiatry
• Long-acting injectable antipsychotics (LAIs) are an important therapeutic option for patients with schizophrenia that allows clinicians to tailor pharmacotherapy to each patient’s needs.
• When selecting a specific LAI, consider class similarities and individual antipsychotic differences.
• Although some LAIs are expensive, they potentially reduce the financial burden of schizophrenia and improve quality of life.
Long-acting injectable antipsychotics (LAIs) are a pharmacotherapeutic option to help clinicians individualize schizophrenia treatment. LAIs have been available since the 1960s, starting with fluphenazine and later haloperidol; however, second-generation antipsychotics were not available in the United States until 20071,2 and more are in development (Box).3,4
Aripiprazole microsphere long-acting injectable (LAI) is a phase III investigational drug that at press time was being reviewed by the FDA. This formulation appears to be similar to risperidone LAI. The active antipsychotic differs in side effect profile and pharmacokinetics. Because the pharmaceutical science of microsphere construction allows many variations, it is not possible to determine the strengths and weaknesses of aripiprazole LAI compared with risperidone LAI microspheres at this time. The dosing intervals currently under investigation are 14 and 28 days.3
Iloperidone crystalline LAI is a phase II-III investigational drug. FDA registration documents and early publication and presentation data report that iloperidone LAI will be a crystalline salt structure pharmaceutically similar to paliperidone and olanzapine LAI formulations.4 The dosing interval under investigation is 28 days.
Up to one-half of patients with schizophrenia do not adhere to their medications.5 LAI use may mitigate relapse in acute schizophrenia that is caused by poor adherence to oral medications. LAIs may have a lower risk of dose-related adverse effects because of lower peak antipsychotic plasma levels and less variation between peak and trough plasma levels. LAIs may decrease the financial burden of schizophrenia and increase individual quality of life because patients spend fewer days hospitalized due to acute exacerbations.6
Some widely used schizophrenia treatment algorithms, such as the Harvard Schizophrenia Algorithm, neglect LAIs. Also, LAIs have not been well studied for maintenance treatment of bipolar disorder (BD) even though nonadherence is a substantial problem in these patients. Patients, families, and legal guardians may choose LAI antipsychotics over oral formulations to decrease the frequency and severity of psychotic relapse or for convenience because patients who receive LAIs do not need to take a medication every day.
Understanding the similarities and differences among LAIs7 and potential interpatient variability of each LAI allows prescribers to tailor the dosing regimen to the patient more safely and efficiently (Table).1,8-11 All LAI antipsychotic formulations rely on absorption pharmacokinetics (PK) rather than elimination PK, which generally is true for sustained-release oral formulations as well. Absorption half-life duration and absorption half-life variability are key concepts in LAI dosing.
Table
Characteristics of long-acting injectable antipsychotics
| Antipsychotic | Oral elimination half-life | Formulation | Absorption half-life | Time between injections | Clinically relevant PK/PD variabilitya | Oral overlapping taper necessary? | Loading dose possible? |
|---|---|---|---|---|---|---|---|
| Fluphenazine | 1 day | Decanoate in organic oil | 14 days | 7 to 21 days | +++ | Yes | No |
| Haloperidol | 1 day | Decanoate in organic oil | 21 days | 28 days | +/- | No | Yes |
| Olanzapine | 1.5 days | Pamoate crystalline | 30 days | 14 to 28 days | ++ | Maybe | No |
| Risperidone | 1 day | Microspheres | 5 days | 14 days | ++ | Yes | No |
| Paliperidone | 1 day | Palmitate crystalline | 45 days | 28 days | + | No | Yes |
| aMore + indicates greater variability among patients PD: pharmacodynamics; PK: pharmacokinetics Source: References 1,8-11 | |||||||
Clinical pearls
Before prescribing an LAI, check that your patient has no known contraindications to the active drug or delivery method. Peak-related adverse effects typically are not contraindications, although they may prompt you to start at a lower dose.
Ensure that your patient will have long-term outpatient access to the LAI and the entire treatment team—inpatient and outpatient—is committed to LAI treatment.
Do not rule out first-generation LAIs such as haloperidol and fluphenazine. The Clinical Antipsychotic Trials of Intervention Effectiveness study, Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study, and other published data suggest older antipsychotics are not inferior to newer medications.12,13
Verify that your patient has had an oral trial of the active drug—ideally in the last 12 months—that resulted in at least partial positive response and no serious adverse drug effects (ADEs). Oral medications’ shorter duration of action may help identify ADEs before administering an LAI.1
Discontinue the oral medication as quickly as evidence, guidance, and good clinical judgment allow. Develop a plan to transition from oral to LAI that you will follow unless the patient develops intolerable ADEs or other problems. There is no evidence to suggest that patients who receive partial LAI therapy decompensate less frequently or less severely than those who take oral medication.
If antipsychotic polypharmacy is necessary, document your rationale.
In patients who are naïve to a specific LAI dosage form, ensure that the first dose does not exceed FDA and evidence-based guidelines for the initial dose (eg, 100 mg intramuscular [IM] for haloperidol decanoate).1
Consider a loading dose strategy to minimize the time a patient has to take an oral and LAI antipsychotic combination.14
Ensure that the total volume injected intramuscularly is not >3 ml per injection site per dose.
Use the recommended injection technique for the particular LAI (eg, Z-tract).1,15
Individualize the dose and dosing interval based on patient response, peak-related adverse effects (time to peak is approximately 5 half-lives for most drugs), and possible reduced symptom control at the end of the dosing interval.8
If your patient does not respond as expected, taking an antipsychotic plasma level to assess drug metabolism and other PK factors and characteristics may be useful.
LAI options
Fluphenazine decanoate is an older, inexpensive LAI with considerable interpatient variability in absorption rate and peak effects, and a relatively short duration of action. Dosing every 7 days may be necessary to avoid peak plasma level adverse effects or symptom recurrence. Variable PK make it difficult to accurately calculate an empiric conversion dose from oral to LAI; therefore, start at the low end (eg, 1.2 to 1.6 times the total daily oral dose) or 12.5 or 25 mg for the initial IM fluphenazine decanoate dose. A short overlap period—usually 1 to 2 weeks—may be necessary. Successful subcutaneous administration is possible.2
Haloperidol decanoate. A 28-day dosing interval is effective for most patients. It is possible to administer a loading dose so that no overlapping taper is required. My team has had good results using an initial loading dose 15 to 20 times the effective oral dose and a second dose 28 days later of 10 times the oral daily maintenance dose, with the same dose every month thereafter. If a patient is receiving his or her first haloperidol decanoate injection, the initial dose should not exceed 100 mg. The remainder of the loading dose may be administered 3 to 7 days later if no adverse effects occur. Similar to fluphenazine decanoate, haloperidol decanoate is relatively inexpensive. When considering giving a haloperidol decanoate loading dose >400 mg or a maintenance dose >200 mg every 28 days, carefully document the rationale (eg, rapid metabolism).16
Olanzapine pamoate. Clinicians who administer olanzapine pamoate must enroll in a national registry that documents the incidence of rare but serious ADEs, particularly hypotension, orthostatis, and post-injection delirium/sedation syndrome (0.1% incidence) at every injection, not just for drug-naïve patients. Patients should be observed for 3 hours after every dose and oral medication overlap may be necessary in some cases.10 Similar to clozapine, these monitoring difficulties and the expense may have inhibited olanzapine LAI use, even in patients who are likely to benefit.
Risperidone microspheres. This agent has been evolutionary, if not revolutionary, in schizophrenia treatment and data on its efficacy for BD will be available soon. Its 2-week dosing interval, necessity of oral overlap, and anecdotal reports of “dose dumping” possibly because of fragility of the microsphere formulation suggest the need for an improved version, which was addressed by the introduction of paliperidone palmitate.10,17,18
Paliperidone palmitate has a 28-day dosing interval. No overlapping oral taper is necessary. Details of a week-long, 2-dose loading dose strategy is provided in the package insert.11 It may be safe to use a more aggressive loading dose strategy.15,19
Related Resources
- Rothschild AJ. The evidence-based guide to antipsychotic medications. Arlington, VA: American Psychiatric Publishing, Inc.; 2010.
- Cañas F, Möller HJ. Long-acting atypical injectable antipsychotics in the treatment of schizophrenia: safety and tolerability review. Expert Opin Drug Saf. 2010;9(5):683-697.
Drug Brand Names
- Aripiprazole • Abilify
- Fluphenazine deconoate • Prolixin Deconoate
- Haloperidol deconoate • Haldol Deconoate
- Iloperidone • Fanapt
- Olanzapine pamoate • Zyprexa Relprevv
- Paliperidone palmitate • Invega Sustenna
- Risperidone • Risperdal Consta
Disclosures
Dr. Kennedy receives grant or research support from Janssen and Johnson and Johnson.
1. Haloperidol decanoate [package insert]. Irvine CA: Teva Parenteral Medicines, Inc; 2009.
2. Fluphenazine decanoate [package insert]. Schaumburg IL: APP Pharmaceuticals, LLC; 2010.
3. A study of ALKS 9072 in subjects with chronic stable schizophrenia. http://clinicaltrials.gov/ct2/show/NCT01493726. Published December 12 2011. Accessed December 16, 2011.
4. Hill CL, Phadke D, Boyce KM. Four-week iloperidone depot injectable: safety and pharmacokinetic profile in patients with schizophrenia and schizoaffective disorder. Poster presented at: 161st annual meeting of the American Psychiatric Association; May 3-8 2008; Washington, DC.
5. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892-909.
6. Keith SJ, Kane JM, Turner M, et al. Academic highlights: guidelines for the use of long-acting injectable atypical antipsychotics. J Clin Psychiatry. 2004;65(1):120-131.
7. McEvoy JP. Risks versus benefits of different types of long-acting injectable antipsychotics. J Clin Psychiatry. 2006;67 (suppl 5):15-18.
8. Gitlin M, Midha KK, Fogelson D, et al. Persistence of fluphenazine in plasma after decanoate withdrawal. J Clin Psychopharmacol. 1988;8(1):53-56.
9. Wilson WH. A visual guide to expected blood levels of long-acting injectable risperidone in clinical practice. J Psychiatr Pract. 2004;10(6):393-401.
10. Zyprexa Relprevv [package insert]. Indianapolis IN: Eli Lilly and Company; 2011.
11. Invega Sustenna [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
12. Lieberman JA, Stroup TS, McEvoy JP, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
13. Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia. Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1). Arch Gen Psychiatry. 2006;63(10):1079-1087.
14. Wei FC, Jann MW, Lin HN, et al. A practical loading dose method for converting schizophrenic patients from oral to depot haloperidol therapy. J Clin Psychiatry. 1996;57(7):298-302.
15. Samtani MN, Vermeulen A, Stuyckens K. Population pharmacokinetics of intramuscular paliperidone palmitate in patients with schizophrenia. Clin Pharmacokinetics. 2009;48(9):585-600.
16. Kapur SJ, Zipursky R, Jones C, et al. Relationship between dopamine D2 occupancy, clinical response and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry. 2000;157(4):514-520.
17. Deeks ED. Risperidone long-acting injection: in bipolar I disorder. Drugs. 2010;70(8):1001-1012.
18. Risperdal Consta [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
19. Samtani MN, Haskins JT, Alphs L, et al. Initiation dosing of deltoid intramuscular paliperidone palmitate in schizophrenia – pharmacokinetic rationale based on modeling and simulation. Poster presented at: 49th annual NCDEU meeting; June 29-July 2, 2009; Hollywood, FL.
William Klugh Kennedy, PharmD, BCPP, FASHP
Dr. Kennedy is Clinical Associate Professor of Pharmacy Practice and Psychiatry, Mercer University, Memorial University Medical Center, Savannah, GA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
William Klugh Kennedy, PharmD, BCPP, FASHP
Dr. Kennedy is Clinical Associate Professor of Pharmacy Practice and Psychiatry, Mercer University, Memorial University Medical Center, Savannah, GA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
William Klugh Kennedy, PharmD, BCPP, FASHP
Dr. Kennedy is Clinical Associate Professor of Pharmacy Practice and Psychiatry, Mercer University, Memorial University Medical Center, Savannah, GA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Discuss this article at www.facebook.com/CurrentPsychiatry
• Long-acting injectable antipsychotics (LAIs) are an important therapeutic option for patients with schizophrenia that allows clinicians to tailor pharmacotherapy to each patient’s needs.
• When selecting a specific LAI, consider class similarities and individual antipsychotic differences.
• Although some LAIs are expensive, they potentially reduce the financial burden of schizophrenia and improve quality of life.
Long-acting injectable antipsychotics (LAIs) are a pharmacotherapeutic option to help clinicians individualize schizophrenia treatment. LAIs have been available since the 1960s, starting with fluphenazine and later haloperidol; however, second-generation antipsychotics were not available in the United States until 20071,2 and more are in development (Box).3,4
Aripiprazole microsphere long-acting injectable (LAI) is a phase III investigational drug that at press time was being reviewed by the FDA. This formulation appears to be similar to risperidone LAI. The active antipsychotic differs in side effect profile and pharmacokinetics. Because the pharmaceutical science of microsphere construction allows many variations, it is not possible to determine the strengths and weaknesses of aripiprazole LAI compared with risperidone LAI microspheres at this time. The dosing intervals currently under investigation are 14 and 28 days.3
Iloperidone crystalline LAI is a phase II-III investigational drug. FDA registration documents and early publication and presentation data report that iloperidone LAI will be a crystalline salt structure pharmaceutically similar to paliperidone and olanzapine LAI formulations.4 The dosing interval under investigation is 28 days.
Up to one-half of patients with schizophrenia do not adhere to their medications.5 LAI use may mitigate relapse in acute schizophrenia that is caused by poor adherence to oral medications. LAIs may have a lower risk of dose-related adverse effects because of lower peak antipsychotic plasma levels and less variation between peak and trough plasma levels. LAIs may decrease the financial burden of schizophrenia and increase individual quality of life because patients spend fewer days hospitalized due to acute exacerbations.6
Some widely used schizophrenia treatment algorithms, such as the Harvard Schizophrenia Algorithm, neglect LAIs. Also, LAIs have not been well studied for maintenance treatment of bipolar disorder (BD) even though nonadherence is a substantial problem in these patients. Patients, families, and legal guardians may choose LAI antipsychotics over oral formulations to decrease the frequency and severity of psychotic relapse or for convenience because patients who receive LAIs do not need to take a medication every day.
Understanding the similarities and differences among LAIs7 and potential interpatient variability of each LAI allows prescribers to tailor the dosing regimen to the patient more safely and efficiently (Table).1,8-11 All LAI antipsychotic formulations rely on absorption pharmacokinetics (PK) rather than elimination PK, which generally is true for sustained-release oral formulations as well. Absorption half-life duration and absorption half-life variability are key concepts in LAI dosing.
Table
Characteristics of long-acting injectable antipsychotics
| Antipsychotic | Oral elimination half-life | Formulation | Absorption half-life | Time between injections | Clinically relevant PK/PD variabilitya | Oral overlapping taper necessary? | Loading dose possible? |
|---|---|---|---|---|---|---|---|
| Fluphenazine | 1 day | Decanoate in organic oil | 14 days | 7 to 21 days | +++ | Yes | No |
| Haloperidol | 1 day | Decanoate in organic oil | 21 days | 28 days | +/- | No | Yes |
| Olanzapine | 1.5 days | Pamoate crystalline | 30 days | 14 to 28 days | ++ | Maybe | No |
| Risperidone | 1 day | Microspheres | 5 days | 14 days | ++ | Yes | No |
| Paliperidone | 1 day | Palmitate crystalline | 45 days | 28 days | + | No | Yes |
| aMore + indicates greater variability among patients PD: pharmacodynamics; PK: pharmacokinetics Source: References 1,8-11 | |||||||
Clinical pearls
Before prescribing an LAI, check that your patient has no known contraindications to the active drug or delivery method. Peak-related adverse effects typically are not contraindications, although they may prompt you to start at a lower dose.
Ensure that your patient will have long-term outpatient access to the LAI and the entire treatment team—inpatient and outpatient—is committed to LAI treatment.
Do not rule out first-generation LAIs such as haloperidol and fluphenazine. The Clinical Antipsychotic Trials of Intervention Effectiveness study, Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study, and other published data suggest older antipsychotics are not inferior to newer medications.12,13
Verify that your patient has had an oral trial of the active drug—ideally in the last 12 months—that resulted in at least partial positive response and no serious adverse drug effects (ADEs). Oral medications’ shorter duration of action may help identify ADEs before administering an LAI.1
Discontinue the oral medication as quickly as evidence, guidance, and good clinical judgment allow. Develop a plan to transition from oral to LAI that you will follow unless the patient develops intolerable ADEs or other problems. There is no evidence to suggest that patients who receive partial LAI therapy decompensate less frequently or less severely than those who take oral medication.
If antipsychotic polypharmacy is necessary, document your rationale.
In patients who are naïve to a specific LAI dosage form, ensure that the first dose does not exceed FDA and evidence-based guidelines for the initial dose (eg, 100 mg intramuscular [IM] for haloperidol decanoate).1
Consider a loading dose strategy to minimize the time a patient has to take an oral and LAI antipsychotic combination.14
Ensure that the total volume injected intramuscularly is not >3 ml per injection site per dose.
Use the recommended injection technique for the particular LAI (eg, Z-tract).1,15
Individualize the dose and dosing interval based on patient response, peak-related adverse effects (time to peak is approximately 5 half-lives for most drugs), and possible reduced symptom control at the end of the dosing interval.8
If your patient does not respond as expected, taking an antipsychotic plasma level to assess drug metabolism and other PK factors and characteristics may be useful.
LAI options
Fluphenazine decanoate is an older, inexpensive LAI with considerable interpatient variability in absorption rate and peak effects, and a relatively short duration of action. Dosing every 7 days may be necessary to avoid peak plasma level adverse effects or symptom recurrence. Variable PK make it difficult to accurately calculate an empiric conversion dose from oral to LAI; therefore, start at the low end (eg, 1.2 to 1.6 times the total daily oral dose) or 12.5 or 25 mg for the initial IM fluphenazine decanoate dose. A short overlap period—usually 1 to 2 weeks—may be necessary. Successful subcutaneous administration is possible.2
Haloperidol decanoate. A 28-day dosing interval is effective for most patients. It is possible to administer a loading dose so that no overlapping taper is required. My team has had good results using an initial loading dose 15 to 20 times the effective oral dose and a second dose 28 days later of 10 times the oral daily maintenance dose, with the same dose every month thereafter. If a patient is receiving his or her first haloperidol decanoate injection, the initial dose should not exceed 100 mg. The remainder of the loading dose may be administered 3 to 7 days later if no adverse effects occur. Similar to fluphenazine decanoate, haloperidol decanoate is relatively inexpensive. When considering giving a haloperidol decanoate loading dose >400 mg or a maintenance dose >200 mg every 28 days, carefully document the rationale (eg, rapid metabolism).16
Olanzapine pamoate. Clinicians who administer olanzapine pamoate must enroll in a national registry that documents the incidence of rare but serious ADEs, particularly hypotension, orthostatis, and post-injection delirium/sedation syndrome (0.1% incidence) at every injection, not just for drug-naïve patients. Patients should be observed for 3 hours after every dose and oral medication overlap may be necessary in some cases.10 Similar to clozapine, these monitoring difficulties and the expense may have inhibited olanzapine LAI use, even in patients who are likely to benefit.
Risperidone microspheres. This agent has been evolutionary, if not revolutionary, in schizophrenia treatment and data on its efficacy for BD will be available soon. Its 2-week dosing interval, necessity of oral overlap, and anecdotal reports of “dose dumping” possibly because of fragility of the microsphere formulation suggest the need for an improved version, which was addressed by the introduction of paliperidone palmitate.10,17,18
Paliperidone palmitate has a 28-day dosing interval. No overlapping oral taper is necessary. Details of a week-long, 2-dose loading dose strategy is provided in the package insert.11 It may be safe to use a more aggressive loading dose strategy.15,19
Related Resources
- Rothschild AJ. The evidence-based guide to antipsychotic medications. Arlington, VA: American Psychiatric Publishing, Inc.; 2010.
- Cañas F, Möller HJ. Long-acting atypical injectable antipsychotics in the treatment of schizophrenia: safety and tolerability review. Expert Opin Drug Saf. 2010;9(5):683-697.
Drug Brand Names
- Aripiprazole • Abilify
- Fluphenazine deconoate • Prolixin Deconoate
- Haloperidol deconoate • Haldol Deconoate
- Iloperidone • Fanapt
- Olanzapine pamoate • Zyprexa Relprevv
- Paliperidone palmitate • Invega Sustenna
- Risperidone • Risperdal Consta
Disclosures
Dr. Kennedy receives grant or research support from Janssen and Johnson and Johnson.
Discuss this article at www.facebook.com/CurrentPsychiatry
• Long-acting injectable antipsychotics (LAIs) are an important therapeutic option for patients with schizophrenia that allows clinicians to tailor pharmacotherapy to each patient’s needs.
• When selecting a specific LAI, consider class similarities and individual antipsychotic differences.
• Although some LAIs are expensive, they potentially reduce the financial burden of schizophrenia and improve quality of life.
Long-acting injectable antipsychotics (LAIs) are a pharmacotherapeutic option to help clinicians individualize schizophrenia treatment. LAIs have been available since the 1960s, starting with fluphenazine and later haloperidol; however, second-generation antipsychotics were not available in the United States until 20071,2 and more are in development (Box).3,4
Aripiprazole microsphere long-acting injectable (LAI) is a phase III investigational drug that at press time was being reviewed by the FDA. This formulation appears to be similar to risperidone LAI. The active antipsychotic differs in side effect profile and pharmacokinetics. Because the pharmaceutical science of microsphere construction allows many variations, it is not possible to determine the strengths and weaknesses of aripiprazole LAI compared with risperidone LAI microspheres at this time. The dosing intervals currently under investigation are 14 and 28 days.3
Iloperidone crystalline LAI is a phase II-III investigational drug. FDA registration documents and early publication and presentation data report that iloperidone LAI will be a crystalline salt structure pharmaceutically similar to paliperidone and olanzapine LAI formulations.4 The dosing interval under investigation is 28 days.
Up to one-half of patients with schizophrenia do not adhere to their medications.5 LAI use may mitigate relapse in acute schizophrenia that is caused by poor adherence to oral medications. LAIs may have a lower risk of dose-related adverse effects because of lower peak antipsychotic plasma levels and less variation between peak and trough plasma levels. LAIs may decrease the financial burden of schizophrenia and increase individual quality of life because patients spend fewer days hospitalized due to acute exacerbations.6
Some widely used schizophrenia treatment algorithms, such as the Harvard Schizophrenia Algorithm, neglect LAIs. Also, LAIs have not been well studied for maintenance treatment of bipolar disorder (BD) even though nonadherence is a substantial problem in these patients. Patients, families, and legal guardians may choose LAI antipsychotics over oral formulations to decrease the frequency and severity of psychotic relapse or for convenience because patients who receive LAIs do not need to take a medication every day.
Understanding the similarities and differences among LAIs7 and potential interpatient variability of each LAI allows prescribers to tailor the dosing regimen to the patient more safely and efficiently (Table).1,8-11 All LAI antipsychotic formulations rely on absorption pharmacokinetics (PK) rather than elimination PK, which generally is true for sustained-release oral formulations as well. Absorption half-life duration and absorption half-life variability are key concepts in LAI dosing.
Table
Characteristics of long-acting injectable antipsychotics
| Antipsychotic | Oral elimination half-life | Formulation | Absorption half-life | Time between injections | Clinically relevant PK/PD variabilitya | Oral overlapping taper necessary? | Loading dose possible? |
|---|---|---|---|---|---|---|---|
| Fluphenazine | 1 day | Decanoate in organic oil | 14 days | 7 to 21 days | +++ | Yes | No |
| Haloperidol | 1 day | Decanoate in organic oil | 21 days | 28 days | +/- | No | Yes |
| Olanzapine | 1.5 days | Pamoate crystalline | 30 days | 14 to 28 days | ++ | Maybe | No |
| Risperidone | 1 day | Microspheres | 5 days | 14 days | ++ | Yes | No |
| Paliperidone | 1 day | Palmitate crystalline | 45 days | 28 days | + | No | Yes |
| aMore + indicates greater variability among patients PD: pharmacodynamics; PK: pharmacokinetics Source: References 1,8-11 | |||||||
Clinical pearls
Before prescribing an LAI, check that your patient has no known contraindications to the active drug or delivery method. Peak-related adverse effects typically are not contraindications, although they may prompt you to start at a lower dose.
Ensure that your patient will have long-term outpatient access to the LAI and the entire treatment team—inpatient and outpatient—is committed to LAI treatment.
Do not rule out first-generation LAIs such as haloperidol and fluphenazine. The Clinical Antipsychotic Trials of Intervention Effectiveness study, Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study, and other published data suggest older antipsychotics are not inferior to newer medications.12,13
Verify that your patient has had an oral trial of the active drug—ideally in the last 12 months—that resulted in at least partial positive response and no serious adverse drug effects (ADEs). Oral medications’ shorter duration of action may help identify ADEs before administering an LAI.1
Discontinue the oral medication as quickly as evidence, guidance, and good clinical judgment allow. Develop a plan to transition from oral to LAI that you will follow unless the patient develops intolerable ADEs or other problems. There is no evidence to suggest that patients who receive partial LAI therapy decompensate less frequently or less severely than those who take oral medication.
If antipsychotic polypharmacy is necessary, document your rationale.
In patients who are naïve to a specific LAI dosage form, ensure that the first dose does not exceed FDA and evidence-based guidelines for the initial dose (eg, 100 mg intramuscular [IM] for haloperidol decanoate).1
Consider a loading dose strategy to minimize the time a patient has to take an oral and LAI antipsychotic combination.14
Ensure that the total volume injected intramuscularly is not >3 ml per injection site per dose.
Use the recommended injection technique for the particular LAI (eg, Z-tract).1,15
Individualize the dose and dosing interval based on patient response, peak-related adverse effects (time to peak is approximately 5 half-lives for most drugs), and possible reduced symptom control at the end of the dosing interval.8
If your patient does not respond as expected, taking an antipsychotic plasma level to assess drug metabolism and other PK factors and characteristics may be useful.
LAI options
Fluphenazine decanoate is an older, inexpensive LAI with considerable interpatient variability in absorption rate and peak effects, and a relatively short duration of action. Dosing every 7 days may be necessary to avoid peak plasma level adverse effects or symptom recurrence. Variable PK make it difficult to accurately calculate an empiric conversion dose from oral to LAI; therefore, start at the low end (eg, 1.2 to 1.6 times the total daily oral dose) or 12.5 or 25 mg for the initial IM fluphenazine decanoate dose. A short overlap period—usually 1 to 2 weeks—may be necessary. Successful subcutaneous administration is possible.2
Haloperidol decanoate. A 28-day dosing interval is effective for most patients. It is possible to administer a loading dose so that no overlapping taper is required. My team has had good results using an initial loading dose 15 to 20 times the effective oral dose and a second dose 28 days later of 10 times the oral daily maintenance dose, with the same dose every month thereafter. If a patient is receiving his or her first haloperidol decanoate injection, the initial dose should not exceed 100 mg. The remainder of the loading dose may be administered 3 to 7 days later if no adverse effects occur. Similar to fluphenazine decanoate, haloperidol decanoate is relatively inexpensive. When considering giving a haloperidol decanoate loading dose >400 mg or a maintenance dose >200 mg every 28 days, carefully document the rationale (eg, rapid metabolism).16
Olanzapine pamoate. Clinicians who administer olanzapine pamoate must enroll in a national registry that documents the incidence of rare but serious ADEs, particularly hypotension, orthostatis, and post-injection delirium/sedation syndrome (0.1% incidence) at every injection, not just for drug-naïve patients. Patients should be observed for 3 hours after every dose and oral medication overlap may be necessary in some cases.10 Similar to clozapine, these monitoring difficulties and the expense may have inhibited olanzapine LAI use, even in patients who are likely to benefit.
Risperidone microspheres. This agent has been evolutionary, if not revolutionary, in schizophrenia treatment and data on its efficacy for BD will be available soon. Its 2-week dosing interval, necessity of oral overlap, and anecdotal reports of “dose dumping” possibly because of fragility of the microsphere formulation suggest the need for an improved version, which was addressed by the introduction of paliperidone palmitate.10,17,18
Paliperidone palmitate has a 28-day dosing interval. No overlapping oral taper is necessary. Details of a week-long, 2-dose loading dose strategy is provided in the package insert.11 It may be safe to use a more aggressive loading dose strategy.15,19
Related Resources
- Rothschild AJ. The evidence-based guide to antipsychotic medications. Arlington, VA: American Psychiatric Publishing, Inc.; 2010.
- Cañas F, Möller HJ. Long-acting atypical injectable antipsychotics in the treatment of schizophrenia: safety and tolerability review. Expert Opin Drug Saf. 2010;9(5):683-697.
Drug Brand Names
- Aripiprazole • Abilify
- Fluphenazine deconoate • Prolixin Deconoate
- Haloperidol deconoate • Haldol Deconoate
- Iloperidone • Fanapt
- Olanzapine pamoate • Zyprexa Relprevv
- Paliperidone palmitate • Invega Sustenna
- Risperidone • Risperdal Consta
Disclosures
Dr. Kennedy receives grant or research support from Janssen and Johnson and Johnson.
1. Haloperidol decanoate [package insert]. Irvine CA: Teva Parenteral Medicines, Inc; 2009.
2. Fluphenazine decanoate [package insert]. Schaumburg IL: APP Pharmaceuticals, LLC; 2010.
3. A study of ALKS 9072 in subjects with chronic stable schizophrenia. http://clinicaltrials.gov/ct2/show/NCT01493726. Published December 12 2011. Accessed December 16, 2011.
4. Hill CL, Phadke D, Boyce KM. Four-week iloperidone depot injectable: safety and pharmacokinetic profile in patients with schizophrenia and schizoaffective disorder. Poster presented at: 161st annual meeting of the American Psychiatric Association; May 3-8 2008; Washington, DC.
5. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892-909.
6. Keith SJ, Kane JM, Turner M, et al. Academic highlights: guidelines for the use of long-acting injectable atypical antipsychotics. J Clin Psychiatry. 2004;65(1):120-131.
7. McEvoy JP. Risks versus benefits of different types of long-acting injectable antipsychotics. J Clin Psychiatry. 2006;67 (suppl 5):15-18.
8. Gitlin M, Midha KK, Fogelson D, et al. Persistence of fluphenazine in plasma after decanoate withdrawal. J Clin Psychopharmacol. 1988;8(1):53-56.
9. Wilson WH. A visual guide to expected blood levels of long-acting injectable risperidone in clinical practice. J Psychiatr Pract. 2004;10(6):393-401.
10. Zyprexa Relprevv [package insert]. Indianapolis IN: Eli Lilly and Company; 2011.
11. Invega Sustenna [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
12. Lieberman JA, Stroup TS, McEvoy JP, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
13. Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia. Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1). Arch Gen Psychiatry. 2006;63(10):1079-1087.
14. Wei FC, Jann MW, Lin HN, et al. A practical loading dose method for converting schizophrenic patients from oral to depot haloperidol therapy. J Clin Psychiatry. 1996;57(7):298-302.
15. Samtani MN, Vermeulen A, Stuyckens K. Population pharmacokinetics of intramuscular paliperidone palmitate in patients with schizophrenia. Clin Pharmacokinetics. 2009;48(9):585-600.
16. Kapur SJ, Zipursky R, Jones C, et al. Relationship between dopamine D2 occupancy, clinical response and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry. 2000;157(4):514-520.
17. Deeks ED. Risperidone long-acting injection: in bipolar I disorder. Drugs. 2010;70(8):1001-1012.
18. Risperdal Consta [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
19. Samtani MN, Haskins JT, Alphs L, et al. Initiation dosing of deltoid intramuscular paliperidone palmitate in schizophrenia – pharmacokinetic rationale based on modeling and simulation. Poster presented at: 49th annual NCDEU meeting; June 29-July 2, 2009; Hollywood, FL.
1. Haloperidol decanoate [package insert]. Irvine CA: Teva Parenteral Medicines, Inc; 2009.
2. Fluphenazine decanoate [package insert]. Schaumburg IL: APP Pharmaceuticals, LLC; 2010.
3. A study of ALKS 9072 in subjects with chronic stable schizophrenia. http://clinicaltrials.gov/ct2/show/NCT01493726. Published December 12 2011. Accessed December 16, 2011.
4. Hill CL, Phadke D, Boyce KM. Four-week iloperidone depot injectable: safety and pharmacokinetic profile in patients with schizophrenia and schizoaffective disorder. Poster presented at: 161st annual meeting of the American Psychiatric Association; May 3-8 2008; Washington, DC.
5. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892-909.
6. Keith SJ, Kane JM, Turner M, et al. Academic highlights: guidelines for the use of long-acting injectable atypical antipsychotics. J Clin Psychiatry. 2004;65(1):120-131.
7. McEvoy JP. Risks versus benefits of different types of long-acting injectable antipsychotics. J Clin Psychiatry. 2006;67 (suppl 5):15-18.
8. Gitlin M, Midha KK, Fogelson D, et al. Persistence of fluphenazine in plasma after decanoate withdrawal. J Clin Psychopharmacol. 1988;8(1):53-56.
9. Wilson WH. A visual guide to expected blood levels of long-acting injectable risperidone in clinical practice. J Psychiatr Pract. 2004;10(6):393-401.
10. Zyprexa Relprevv [package insert]. Indianapolis IN: Eli Lilly and Company; 2011.
11. Invega Sustenna [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
12. Lieberman JA, Stroup TS, McEvoy JP, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
13. Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia. Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1). Arch Gen Psychiatry. 2006;63(10):1079-1087.
14. Wei FC, Jann MW, Lin HN, et al. A practical loading dose method for converting schizophrenic patients from oral to depot haloperidol therapy. J Clin Psychiatry. 1996;57(7):298-302.
15. Samtani MN, Vermeulen A, Stuyckens K. Population pharmacokinetics of intramuscular paliperidone palmitate in patients with schizophrenia. Clin Pharmacokinetics. 2009;48(9):585-600.
16. Kapur SJ, Zipursky R, Jones C, et al. Relationship between dopamine D2 occupancy, clinical response and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry. 2000;157(4):514-520.
17. Deeks ED. Risperidone long-acting injection: in bipolar I disorder. Drugs. 2010;70(8):1001-1012.
18. Risperdal Consta [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
19. Samtani MN, Haskins JT, Alphs L, et al. Initiation dosing of deltoid intramuscular paliperidone palmitate in schizophrenia – pharmacokinetic rationale based on modeling and simulation. Poster presented at: 49th annual NCDEU meeting; June 29-July 2, 2009; Hollywood, FL.
PTSD nightmares: Prazosin and atypical antipsychotics
• Prazosin is recommended as a first-line therapy for nighttime PTSD symptoms, such as nightmares or sleep disturbances—especially among veterans—because of superior long-term effectiveness.
• Risk of metabolic syndrome, which has been reported with low-dose atypical antipsychotics used for treating insomnia, limits their use for PTSD-related nightmares.
Mr. S, a 45-year-old veteran, was diagnosed with posttraumatic stress disorder (PTSD) 18 years ago after a tour of duty in the Persian Gulf. He had combat-related flashbacks triggered by the smell of gasoline or smoke from a fire, was easily startled, and began to isolate himself socially. However, his symptoms improved when he started volunteering at his local Veterans Affairs Medical Center. After he lost his job 3 years ago, Mr. S started experiencing flashbacks. He was irritable, easily startled, and avoided things that reminded him of his time in the Persian Gulf. His psychiatrist prescribed sertraline, titrated to 200 mg/d. The drug reduced the severity of his avoidance and hyperarousal symptoms and improved his mood.
During a clinic visit, Mr. S says he is doing well and can fall asleep at night but is having recurring nightmares about traumatic events that occurred during combat. These nightmares wake him up and have become more frequent, occurring once per night for the past month. Mr. S says he has been watching more news programs about conflicts in Afghanistan and Iraq since the nightmares began. His psychiatrist starts quetiapine, 50 mg at bedtime for 7 nights then 100 mg at bedtime, but after 6 weeks Mr. S says his nightmares continue.
PTSD occurs in approximately 19% of Vietnam war combat veterans1 and 14% of service members returning from Iraq and Afghanistan.2 PTSD symptoms are classified into clusters: intrusive/re-experiencing; avoidant/numbing; and hyperarousal.3 Nightmares are part of the intrusive/re-experiencing cluster, which is Criterion B in DSM-IV-TR. See Table 1 for a description of DSM-IV-TR PTSD criteria. Among PTSD patients, 50% to 70% report PTSD-associated nightmares.4 Despite adequate treatment targeted to improve PTSD’s core symptoms, symptoms such as sleep disturbances or nightmares often persist.
Table 1
DSM-IV-TR diagnostic criteria for posttraumatic stress disorder
|
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Nightmares and other sleep disturbances are associated with significant distress and daytime impairment and can interfere with PTSD recovery4-8 by disrupting sleep-dependent processing of emotional experiences and causing repeated resensitization to trauma cues (Table 2).8
Table 2
Psychosocial consequences of sleep disruption in PTSD
| Increased reactivity to emotional cues |
| Compromised ability to function in social and occupational roles |
| Negative psychiatric outcomes, including suicidal ideation or worsening of depression or psychosis |
| Interference of natural recovery from trauma exposure |
| Repeated resensitization to trauma cues |
| Neurocognitive deficits |
| Neuroendocrine abnormalities |
| PTSD: posttraumatic stress disorder Source: Adapted from reference 8 |
Few randomized controlled medication trials specifically address PTSD-related nightmares. Most PTSD studies do not examine sleep outcomes as a primary measure, and comprehensive literature reviews could not offer evidence-based recommendations.9,10 The American Academy of Sleep Medicine (AASM) also noted a paucity of PTSD studies that identified nightmares as a primary outcome measure.11 See Table 3 for a list of recommended medication options for PTSD-associated nightmares.
Table 3
Recommended medication treatments for PTSD-associated nightmares
| Evidence level | Medication | Evidence |
|---|---|---|
| Recommended for treating PTSD-associated nightmares | ||
| 1, 4 | Prazosin | In 3 level 1 studies, adding prazosin (mean dose 3 mg/d) significantly decreased trauma-related nightmares according to the CAPS “recurrent distressing dreams” item after 3 to 9 weeks of treatment vs placebo in veteran and civilian patients (N = 57) |
| Not suggested for treating PTSD-associated nightmares | ||
| 1 | Venlafaxine | No difference between extended-release venlafaxine (37.5 to 300 mg/d) and placebo in the CAPS-SX17 “distressing dreams” item at 12 weeks in 340 PTSD patients |
| May be considered for treating PTSD-associated nightmares | ||
| 4 | Clonidine | Reduced the number of nightmares in 11 of 13 refugees for 2 weeks to 3 months (dose: 0.2 to 0.6 mg/d) |
| May be considered for treating PTSD-associated nightmares, but data are low grade and sparse | ||
| 4 | Trazodone | Although trazodone (25 to 600 mg) significantly decreased nightmare frequency in veteran patients during an 8-week hospital stay (N = 60), 19% discontinued therapy because of side effects |
| 4 | Olanzapine | Adjunctive olanzapine (10 to 20 mg) rapidly improved sleep in a case series of combat-related PTSD patients resistant to SSRIs and benzodiazepines (N = 5) |
| 4 | Risperidone | In case series, risperidone (0.5 to 3 mg) significantly decreased CAPS scores for recurrent distressing dreams and proportion of traumatic dreams documented in diaries of combat veterans over 6 weeks (N = 17), and improved nightmares in adult burn patients taking pain medications after 1 to 2 days (N = 10) |
| 4 | Aripiprazole | In a case series, aripiprazole (15 to 30 mg at bedtime) with CBT or sertraline significantly improved nightmares in 4 of 5 combat-related PTSD patients |
| 4 | Topiramate | Topiramate reduced nightmares in 79% of civilians with PTSD and fully suppressed nightmares in 50% of patients in a case series (N = 35) |
| 4 | Low-dose cortisol | Significant decrease in frequency but not intensity of nightmares with low-dose cortisol (10 mg/d) in civilians with PTSD (N = 3) |
| 4 | Fluvoxamine | In 2 case series, fluvoxamine (up to 300 mg/d) significantly decreased the IES-R level of “dreams about combat trauma” but not the SRRS “bad dreams” rating at 10 weeks (N = 21). During 4 to 12 weeks of follow-up there was a qualitative decrease in reported nightmares in veteran patients (n = 12) |
| 2 | Triazolam/nitrazepam | Limited data showed triazolam (0.5 mg) and nitrazepam (5 mg) provide equal efficacy in decreasing the number of patients who experience unpleasant dreams over 1 night |
| 4 | Phenelzine | One study showed phenelzine monotherapy (30 to 90 mg) resulted in elimination of nightmares within 1 month (N = 5); another reported “moderately reduced traumatic dreams” (N = 21) in veterans. Therapy was discontinued because of short-lived efficacy or plateau effect |
| 4 | Gabapentin | Adjunctive gabapentin (300 to 3,600 mg/d) improved insomnia and decreased nightmare frequency and/or intensity over 1 to 36 months in 30 veterans with PTSD |
| 4 | Cyproheptadine | Conflicting data ranges from eliminating nightmares to no changes in the presence or intensity of nightmares |
| 4 | TCAs | Among 10 Cambodian concentration camp survivors treated with TCAs, 4 reported their nightmares ceased and 4 reported improvement after 1-year follow-up |
| 4 | Nefazodone | Reduced nightmare occurrence in 3 open-label studies as monotherapy (386 to 600 mg/d). Not recommended first line because of hepatotoxicity risk |
| No recommendation because of sparse data | ||
| 2 | Clonazepam | Clonazepam (1 to 2 mg/d) was ineffective in decreasing frequency or intensity of combat-related PTSD nightmares in veterans (N = 6) |
Evidence levels:
| ||
| CAPS: Clinician-Administered PTSD Scale; CAPS-SX17: 17-item Clinician-Administered PTSD Scale; CBT: cognitive-behavioral therapy; IES-R: Impact of Event Scale-Revised; PTSD: posttraumatic stress disorder; SRRS: Stress Response Rating Scale; SSRI: selective serotonin reuptake inhibitor; TCAs: tricyclic antidepressants Source: Adapted from Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401 | ||
CASE CONTINUED: Medication change, improvement
After reviewing AASM’s treatment recommendations, we prescribe prazosin, 1 mg at bedtime for 7 nights, then increase by 1 mg at bedtime each week until Mr. S’s nightmares improve. He reports a substantial improvement in nightmare severity and frequency after a few weeks of treatment with prazosin, 5 mg at bedtime.
Prazosin
Prazosin is an α1-adrenergic receptor antagonist with good CNS penetrability. The rationale for reducing adrenergic activity to address intrusive PTSD symptoms has been well documented.12,13 In open-label trials,14-18 a chart review,19 and placebo-controlled trials,20-22prazosin reduced trauma nightmares and improved sleep quality and global clinical status more than placebo (Table 4). In these studies, prazosin doses ranged from 1 to 20 mg/d, with an average of 3 mg at bedtime and a starting dose of 1 mg. Prazosin is the only agent recommended in the AASM’s Best Practice Guide for treating PTSD-related nightmares.11
Table 4
RCTs of prazosin for trauma-related nightmares
| Study | Design | Patients | Results |
|---|---|---|---|
| Raskind et al, 200320 | 20-week, double-blind, placebo-controlled, crossover study (mean dose 9.5 mg/d at bedtime) | 10 Vietnam veterans with chronic PTSD and severe trauma-related nightmares | Prazosin was superior to placebo on scores on the recurrent distressing dreams item and difficulty falling/staying asleep item of the CAPS and change in PTSD severity and functional status on the CGI-C |
| Raskind et al, 200721 | 8-week, placebo-controlled, parallel study (mean dose 13.3 ± 3 mg/d in the evening) | 40 veterans with chronic PTSD, distressing trauma nightmares, and sleep disturbance | Prazosin was superior to placebo in reducing trauma nightmares and improving sleep quality and global clinical status; prazosin also shifted dream characteristics of trauma-related nightmares to those typical of normal dreams |
| Taylor et al, 200822 | 7-week, randomized, placebo-controlled, crossover trial (mean dose 3.1 ± 1.3 mg) | 13 outpatients with chronic civilian trauma PTSD, frequent nightmares, and sleep disturbance | Prazosin significantly increased total sleep time and REM sleep time; reduced trauma-related nightmares, distressed awakenings, and total PCL-C scores; improved CGI-I scores; and changed PDRS scores toward normal dreaming |
| CAPS: Clinician-Administered PTSD Scale; CGI-C: Clinical Global Impression of Change; CGI-I: Clinical Global Impression of Improvement; PCL-C: PTSD Checklist-Civilian; PDRS: PTSD Dream Rating Scale; PTSD: posttraumatic stress disorder; RCTs: randomized controlled trials; REM: rapid eye movement | |||
Atypical antipsychotics
Atypical antipsychotics have been used to reduce nightmares in PTSD; however, most of the evidence from studies evaluated in the AASM’s Best Practice Guide were considered to be low quality.11 Quetiapine and ziprasidone were not included in the AASM review. See (Table 5) for a review of the evidence for atypical antipsychotics for treating PTSD nightmares.
Table 5
Combat-related nightmares: Evidence for atypical antipsychotics
| Study | Design | Patients/dosage | Results |
|---|---|---|---|
| Aripiprazole | |||
| Lambert, 2006 a | Case report | 4 veterans with combat-related PTSD (3 male, 1 female; age 22 to 24); dose: 15 to 30 mg; concurrent treatment sertraline or CBT | Decreased frequency of weekly nightmares and agitated sleep by at least 50% |
| Olanzapine | |||
| Stein et al, 2002 b | 8-week, double-blind, placebo-controlled study | 19 male veterans with combat-related PTSD (olanzapine group mean age: 55.2 ± 6.6; placebo group 51.1 ± 8.1); mean dose: 15 mg/d | Significantly greater reduction in sleep disturbances (PSQI: -3.29 vs 1.57; P = .01); significantly higher weight gain (13.2 lbs vs -3 lbs; P = .001) |
| Jakovljevic et al, 2003 c | Case reports | 5 veterans with combat-related PTSD for 6 to 7 years (age: 28 to 50); dose: 10 to 20 mg; adjunct treatment | Decreased frequency of nightmares within 3 days |
| Labbate et al, 2000 d | Case report | 1 male veteran (age: 58) with a 20-year history of combat-related PTSD; dose: 5 mg at bedtime; concurrent treatment with sertraline (200 mg/d), bupropion (150 mg/d), and diazepam (15 mg/d) | Eliminated nightmares after 1 week and improved sleep quality |
| Quetiapine | |||
| Ahearn et al, 2006 e | 8-week, open-label trial | 15 PTSD patients (8 male; 7 female; 5 with combat-related PTSD; mean age: 49); mean dose: 216 mg/d (100 to 400 mg/d) | Significantly improved re-experiencing (CAPS: 10 vs 23; P = .0012) and sleep (PSQI: 17.5 vs 30; P = .0044) at 8 weeks compared with baseline |
| Robert et al, 2005 f | 6-week, open-label trial | 19 combat veterans; mean dose: 100 ± 70 mg/d (25 to 300 mg/d); adjunct treatment | Significantly improved sleep quality (PSQI: 1.67 vs 2.41; P = .006), latency (PSQI: 1.5 vs 2.65; P = .002), duration (PSQI: 1.31 vs 2.71; P < .001), and sleep disturbances (PSQI: 1.22 vs 1.71; P = .034) and decreased terror episodes (PSQI-A: 0.73 vs 0.91; P = .040) and acting out dreams (PSQI-A: 1.07 vs 1.35; P = .013); however, no difference in nightmares caused by trauma (PSQI-A: 1.53 vs 2.06) |
| Sokolski et al, 2003 g | Retrospective chart review | 68 male Vietnam War combat veterans (mean age: 55 ± 3.5); mean dose: 155 ± 130 mg (25 to 700 mg); adjunct treatment | Improved sleep disturbances in 62% and nightmares in 25% of patients |
| Ahearn et al, 2003 h | Case report | 2 male patients with combat-related PTSD (age 53, 72); dose: 25 to 50 mg; adjunct to SSRI therapy | Decreased frequency of nightmares with increased sleep duration |
| Risperidone | |||
| David et al, 2006 i | 6-week, open-label trial | 17 male veterans with combat-related PTSD (mean age: 53.7 ± 3.8); mean maximum dose: 2.3 ± 0.6 mg (range: 1 to 3 mg) | Improved recurrent distressing dreams (CAPS B-2: 3.8 vs 5.4; P = .04), but not with the PSQI subscale (PSQI bad dreams: 2.5 vs 2.7; NS). Decreased nighttime awakenings (1.9 vs 2.8; P = .003) and trauma dreams (19% vs 38%; P = .04) |
| Leyba et al, 1998 j | Case reports | 3 male patients (age 43 to 46); dose: 1 to 3 mg; adjunct therapy | Decreased occurrence of nightmares |
| Ziprasidone | |||
| Siddiqui et al, 2005 k | Case report | 1 male veteran with chronic combat-related PTSD (age 55); dose: 80 to 120 mg/d; adjunct with trazodone (100 mg) and topiramate | Improved occurrence of nightmares up to 4 months |
CAPS: Clinician-Administered PTSD Scale; CAPS B-2: Clinician-Administered PTSD Scale B-2 (recurrent distressing dreams of the event); CBT: cognitive-behavioral therapy; PSQI: Pittsburgh Sleep Quality Index; PSQI-A: Pittsburgh Sleep Quality Index Addendum for PTSD; NS: not significant; PTSD: posttraumatic stress disorder; SSRI: selective serotonin reuptake inhibitor References
| |||
Comparing prazosin and quetiapine. A historical prospective cohort study of 237 veterans with PTSD receiving prazosin or quetiapine for nighttime PTSD symptoms demonstrated that although the 2 drugs have similar efficacy (defined as symptomatic improvement) for short-term, 6-month treatment (61% vs 62%; P=.54), a higher percentage of patients continued prazosin long-term (3 to 6 years) than those taking quetiapine (48% vs 24%; P < .001).23 Twenty-five percent of patients taking quetiapine switched to prazosin during the study, and approximately one-half of these patients remained on prazosin until the study’s end. Only 8% of prazosin patients switched to quetiapine, and none continued this therapy until study end.23 Patients in the quetiapine group were more likely to discontinue the drug because of lack of efficacy (13% vs 3%; P=.03) and adverse effects (35% vs 18%; P=.008), specifically sedation (21% vs 2%; P < .001) and metabolic effects (9% vs 0%; P=.014), compared with prazosin. Although this trial may be the only published comparison study of prazosin and quetiapine, its methodological quality has been questioned, which makes it difficult to draw definitive conclusions.
Metabolic syndrome—elevated diastolic blood pressure, increased waist circumference, and low high-density lipoprotein cholesterol—is common among PTSD patients treated with antipsychotics.24 This syndrome may be caused by medications, lifestyle factors, or long-term overactivation of stress-response pathways. A retrospective chart review at a community mental health center revealed that patients taking even low doses of quetiapine for insomnia gained an average of 5 lbs (P=.037).25 Another retrospective chart review at 2 military hospitals reported that patients receiving low-dose quetiapine (≤100 mg/d) gained an average of slightly less than 1 lb per month, which adds up to approximately 10 lbs per year (P < .001).26 The benefit of using atypical antipsychotics may be outweighed by metabolic risks such as obesity, new-onset diabetes, and dyslipidemia.27
Prazosin is considered a first-line treatment for sleep disturbances and nightmares in PTSD because of its superior long-term efficacy and decreased adverse effects compared with quetiapine.
Related Resources
- American Psychiatric Association. Practice guidelines for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Arlington, VA: American Psychiatric Publishing, Inc.; 2004.
- Veterans Affairs/Department of Defense clinical practice guidelines. Management of traumatic stress disorder and acute stress reaction. www.healthquality.va.gov/Post_Traumatic_Stress_Disorder_PTSD.asp.
Drug Brand Names
- Prazosin • Minipress
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Dohrenwend BP, Turner JB, Turse NA, et al. The psychological risks of Vietnam for U.S. veterans: a revisit with new data and methods. Science. 2006;313(5789):979-982.
2. Tanielian T, Jaycox L. eds. Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND Corporation; 2008.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
4. Wittmann L, Schredl M, Kramer M. Dreaming in posttraumatic stress disorder: a critical review of phenomenology psychophysiology and treatment. Psychother Psychosom. 2007;76(1):25-39.
5. Clum GA, Nishith P, Resick PA. Trauma-related sleep disturbance and self-reported physical health symptoms in treatment-seeking female rape victims. J Nerv Ment Dis. 2001;189(9):618-622.
6. Kramer TL, Booth BM, Han X, et al. Service utilization and outcomes in medically ill veterans with posttraumatic stress and depressive disorders. J Trauma Stress. 2003;16(3):211-219.
7. Neylan TC, Marmar CR, Metzler TJ, et al. Sleep disturbances in the Vietnam generation: findings from a nationally representative sample of male Vietnam veterans. Am J Psychiatry. 1998;155(7):929-933.
8. Nappi CM, Drummond SP, Hall JM. Treating nightmares and insomnia in posttraumatic stress disorder: a review of current evidence. Neuropharmacology. 2012;62(2):576-585.
9. Maher MJ, Rego SA, Asnis GM. Sleep disturbances in patients with post-traumatic stress disorder: epidemiology impact and approaches to management. CNS Drugs. 2006;20(7):567-590.
10. van Liempt S, Vermetten E, Geuze E, et al. Pharmacotherapy for disordered sleep in post-traumatic stress disorder: a systematic review. Int Clin Psychopharmacol. 2006;21(4):193-202.
11. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401.
12. Boehnlein JK, Kinzie JD. Pharmacologic reduction of CNS noradrenergic activity in PTSD: the case for clonidine and prazosin. J Psychiatr Pract. 2007;13(2):72-78.
13. Strawn JR, Geracioti TD, Jr. Noradrenergic dysfunction and the psychopharmacology of posttraumatic stress disorder. Depress Anxiety. 2008;25(3):260-271.
14. Calohan J, Peterson K, Peskind ER, et al. Prazosin treatment of trauma nightmares and sleep disturbance in soldiers deployed in Iraq. J Trauma Stress. 2010;23(5):645-648.
15. Daly CM, Doyle ME, Radkind M, et al. Clinical case series: the use of Prazosin for combat-related recurrent nightmares among Operation Iraqi Freedom combat veterans. Mil Med. 2005;170(6):513-515.
16. Peskind ER, Bonner LT, Hoff DJ, et al. Prazosin reduces trauma-related nightmares in older men with chronic posttraumatic stress disorder. J Geriatr Psychiatry Neurol. 2003;16(3):165-171.
17. Raskind MA, Dobie DJ, Kanter ED, et al. The alpha1-adrenergic antagonist prazosin ameliorates combat trauma nightmares in veterans with posttraumatic stress disorder: a report of 4 cases. J Clin Psychiatry. 2000;61(2):129-133.
18. Taylor F, Raskind MA. The alpha1-adrenergic antagonist prazosin improves sleep and nightmares in civilian trauma posttraumatic stress disorder. J Clin Psychopharmacol. 2002;22(1):82-85.
19. Raskind MA, Thompson C, Petrie EC, et al. Prazosin reduces nightmares in combat veterans with posttraumatic stress disorder. J Clin Psychiatry. 2002;63(7):565-568.
20. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry. 2003;160(2):371-373.
21. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry. 2007;61(8):928-934.
22. Taylor FB, Martin P, Thompson C, et al. Prazosin effects on objective sleep measures and clinical symptoms in civilian trauma posttraumatic stress disorder: a placebo-controlled study. Biol Psychiatry. 2008;63(6):629-632.
23. Byers MG, Allison KM, Wendel CS, et al. Prazosin versus quetiapine for nighttime posttraumatic stress disorder symptoms in veterans: an assessment of long-term comparative effectiveness and safety. J Clin Psychopharmacol. 2010;30(3):225-229.
24. Jin H, Lanouette NM, Mudaliar S, et al. Association of posttraumatic stress disorder with increased prevalence of metabolic syndrome. J Clin Psychopharmacol. 2009;29(3):210-215.
25. Cates ME, Jackson CW, Feldman JM, et al. Metabolic consequences of using low-dose quetiapine for insomnia in psychiatric patients. Community Ment Health J. 2009;45(4):251-254.
26. Williams SG, Alinejad NA, Williams JA, et al. Statistically significant increase in weight caused by low-dose quetiapine. Pharmacotherapy. 2010;30(10):1011-1015.
27. American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65(2):267-272.
Rebecca L. Graham, PharmD
Dr. Graham is a Second-Year Psychiatric Pharmacy Resident, Veterans Affairs San Diego Healthcare System (VASDHS)
Susan G. Leckband, RPh, BCPP
Ms. Leckband is a Clinical Psychiatric Pharmacist Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego
Rene A. Endow-Eyer, PharmD, BCPP
Dr. Endow-Eyer is Psychiatric Clinical Pharmacy Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego, San Diego, CA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Rebecca L. Graham, PharmD
Dr. Graham is a Second-Year Psychiatric Pharmacy Resident, Veterans Affairs San Diego Healthcare System (VASDHS)
Susan G. Leckband, RPh, BCPP
Ms. Leckband is a Clinical Psychiatric Pharmacist Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego
Rene A. Endow-Eyer, PharmD, BCPP
Dr. Endow-Eyer is Psychiatric Clinical Pharmacy Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego, San Diego, CA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Rebecca L. Graham, PharmD
Dr. Graham is a Second-Year Psychiatric Pharmacy Resident, Veterans Affairs San Diego Healthcare System (VASDHS)
Susan G. Leckband, RPh, BCPP
Ms. Leckband is a Clinical Psychiatric Pharmacist Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego
Rene A. Endow-Eyer, PharmD, BCPP
Dr. Endow-Eyer is Psychiatric Clinical Pharmacy Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego, San Diego, CA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
• Prazosin is recommended as a first-line therapy for nighttime PTSD symptoms, such as nightmares or sleep disturbances—especially among veterans—because of superior long-term effectiveness.
• Risk of metabolic syndrome, which has been reported with low-dose atypical antipsychotics used for treating insomnia, limits their use for PTSD-related nightmares.
Mr. S, a 45-year-old veteran, was diagnosed with posttraumatic stress disorder (PTSD) 18 years ago after a tour of duty in the Persian Gulf. He had combat-related flashbacks triggered by the smell of gasoline or smoke from a fire, was easily startled, and began to isolate himself socially. However, his symptoms improved when he started volunteering at his local Veterans Affairs Medical Center. After he lost his job 3 years ago, Mr. S started experiencing flashbacks. He was irritable, easily startled, and avoided things that reminded him of his time in the Persian Gulf. His psychiatrist prescribed sertraline, titrated to 200 mg/d. The drug reduced the severity of his avoidance and hyperarousal symptoms and improved his mood.
During a clinic visit, Mr. S says he is doing well and can fall asleep at night but is having recurring nightmares about traumatic events that occurred during combat. These nightmares wake him up and have become more frequent, occurring once per night for the past month. Mr. S says he has been watching more news programs about conflicts in Afghanistan and Iraq since the nightmares began. His psychiatrist starts quetiapine, 50 mg at bedtime for 7 nights then 100 mg at bedtime, but after 6 weeks Mr. S says his nightmares continue.
PTSD occurs in approximately 19% of Vietnam war combat veterans1 and 14% of service members returning from Iraq and Afghanistan.2 PTSD symptoms are classified into clusters: intrusive/re-experiencing; avoidant/numbing; and hyperarousal.3 Nightmares are part of the intrusive/re-experiencing cluster, which is Criterion B in DSM-IV-TR. See Table 1 for a description of DSM-IV-TR PTSD criteria. Among PTSD patients, 50% to 70% report PTSD-associated nightmares.4 Despite adequate treatment targeted to improve PTSD’s core symptoms, symptoms such as sleep disturbances or nightmares often persist.
Table 1
DSM-IV-TR diagnostic criteria for posttraumatic stress disorder
|
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Nightmares and other sleep disturbances are associated with significant distress and daytime impairment and can interfere with PTSD recovery4-8 by disrupting sleep-dependent processing of emotional experiences and causing repeated resensitization to trauma cues (Table 2).8
Table 2
Psychosocial consequences of sleep disruption in PTSD
| Increased reactivity to emotional cues |
| Compromised ability to function in social and occupational roles |
| Negative psychiatric outcomes, including suicidal ideation or worsening of depression or psychosis |
| Interference of natural recovery from trauma exposure |
| Repeated resensitization to trauma cues |
| Neurocognitive deficits |
| Neuroendocrine abnormalities |
| PTSD: posttraumatic stress disorder Source: Adapted from reference 8 |
Few randomized controlled medication trials specifically address PTSD-related nightmares. Most PTSD studies do not examine sleep outcomes as a primary measure, and comprehensive literature reviews could not offer evidence-based recommendations.9,10 The American Academy of Sleep Medicine (AASM) also noted a paucity of PTSD studies that identified nightmares as a primary outcome measure.11 See Table 3 for a list of recommended medication options for PTSD-associated nightmares.
Table 3
Recommended medication treatments for PTSD-associated nightmares
| Evidence level | Medication | Evidence |
|---|---|---|
| Recommended for treating PTSD-associated nightmares | ||
| 1, 4 | Prazosin | In 3 level 1 studies, adding prazosin (mean dose 3 mg/d) significantly decreased trauma-related nightmares according to the CAPS “recurrent distressing dreams” item after 3 to 9 weeks of treatment vs placebo in veteran and civilian patients (N = 57) |
| Not suggested for treating PTSD-associated nightmares | ||
| 1 | Venlafaxine | No difference between extended-release venlafaxine (37.5 to 300 mg/d) and placebo in the CAPS-SX17 “distressing dreams” item at 12 weeks in 340 PTSD patients |
| May be considered for treating PTSD-associated nightmares | ||
| 4 | Clonidine | Reduced the number of nightmares in 11 of 13 refugees for 2 weeks to 3 months (dose: 0.2 to 0.6 mg/d) |
| May be considered for treating PTSD-associated nightmares, but data are low grade and sparse | ||
| 4 | Trazodone | Although trazodone (25 to 600 mg) significantly decreased nightmare frequency in veteran patients during an 8-week hospital stay (N = 60), 19% discontinued therapy because of side effects |
| 4 | Olanzapine | Adjunctive olanzapine (10 to 20 mg) rapidly improved sleep in a case series of combat-related PTSD patients resistant to SSRIs and benzodiazepines (N = 5) |
| 4 | Risperidone | In case series, risperidone (0.5 to 3 mg) significantly decreased CAPS scores for recurrent distressing dreams and proportion of traumatic dreams documented in diaries of combat veterans over 6 weeks (N = 17), and improved nightmares in adult burn patients taking pain medications after 1 to 2 days (N = 10) |
| 4 | Aripiprazole | In a case series, aripiprazole (15 to 30 mg at bedtime) with CBT or sertraline significantly improved nightmares in 4 of 5 combat-related PTSD patients |
| 4 | Topiramate | Topiramate reduced nightmares in 79% of civilians with PTSD and fully suppressed nightmares in 50% of patients in a case series (N = 35) |
| 4 | Low-dose cortisol | Significant decrease in frequency but not intensity of nightmares with low-dose cortisol (10 mg/d) in civilians with PTSD (N = 3) |
| 4 | Fluvoxamine | In 2 case series, fluvoxamine (up to 300 mg/d) significantly decreased the IES-R level of “dreams about combat trauma” but not the SRRS “bad dreams” rating at 10 weeks (N = 21). During 4 to 12 weeks of follow-up there was a qualitative decrease in reported nightmares in veteran patients (n = 12) |
| 2 | Triazolam/nitrazepam | Limited data showed triazolam (0.5 mg) and nitrazepam (5 mg) provide equal efficacy in decreasing the number of patients who experience unpleasant dreams over 1 night |
| 4 | Phenelzine | One study showed phenelzine monotherapy (30 to 90 mg) resulted in elimination of nightmares within 1 month (N = 5); another reported “moderately reduced traumatic dreams” (N = 21) in veterans. Therapy was discontinued because of short-lived efficacy or plateau effect |
| 4 | Gabapentin | Adjunctive gabapentin (300 to 3,600 mg/d) improved insomnia and decreased nightmare frequency and/or intensity over 1 to 36 months in 30 veterans with PTSD |
| 4 | Cyproheptadine | Conflicting data ranges from eliminating nightmares to no changes in the presence or intensity of nightmares |
| 4 | TCAs | Among 10 Cambodian concentration camp survivors treated with TCAs, 4 reported their nightmares ceased and 4 reported improvement after 1-year follow-up |
| 4 | Nefazodone | Reduced nightmare occurrence in 3 open-label studies as monotherapy (386 to 600 mg/d). Not recommended first line because of hepatotoxicity risk |
| No recommendation because of sparse data | ||
| 2 | Clonazepam | Clonazepam (1 to 2 mg/d) was ineffective in decreasing frequency or intensity of combat-related PTSD nightmares in veterans (N = 6) |
Evidence levels:
| ||
| CAPS: Clinician-Administered PTSD Scale; CAPS-SX17: 17-item Clinician-Administered PTSD Scale; CBT: cognitive-behavioral therapy; IES-R: Impact of Event Scale-Revised; PTSD: posttraumatic stress disorder; SRRS: Stress Response Rating Scale; SSRI: selective serotonin reuptake inhibitor; TCAs: tricyclic antidepressants Source: Adapted from Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401 | ||
CASE CONTINUED: Medication change, improvement
After reviewing AASM’s treatment recommendations, we prescribe prazosin, 1 mg at bedtime for 7 nights, then increase by 1 mg at bedtime each week until Mr. S’s nightmares improve. He reports a substantial improvement in nightmare severity and frequency after a few weeks of treatment with prazosin, 5 mg at bedtime.
Prazosin
Prazosin is an α1-adrenergic receptor antagonist with good CNS penetrability. The rationale for reducing adrenergic activity to address intrusive PTSD symptoms has been well documented.12,13 In open-label trials,14-18 a chart review,19 and placebo-controlled trials,20-22prazosin reduced trauma nightmares and improved sleep quality and global clinical status more than placebo (Table 4). In these studies, prazosin doses ranged from 1 to 20 mg/d, with an average of 3 mg at bedtime and a starting dose of 1 mg. Prazosin is the only agent recommended in the AASM’s Best Practice Guide for treating PTSD-related nightmares.11
Table 4
RCTs of prazosin for trauma-related nightmares
| Study | Design | Patients | Results |
|---|---|---|---|
| Raskind et al, 200320 | 20-week, double-blind, placebo-controlled, crossover study (mean dose 9.5 mg/d at bedtime) | 10 Vietnam veterans with chronic PTSD and severe trauma-related nightmares | Prazosin was superior to placebo on scores on the recurrent distressing dreams item and difficulty falling/staying asleep item of the CAPS and change in PTSD severity and functional status on the CGI-C |
| Raskind et al, 200721 | 8-week, placebo-controlled, parallel study (mean dose 13.3 ± 3 mg/d in the evening) | 40 veterans with chronic PTSD, distressing trauma nightmares, and sleep disturbance | Prazosin was superior to placebo in reducing trauma nightmares and improving sleep quality and global clinical status; prazosin also shifted dream characteristics of trauma-related nightmares to those typical of normal dreams |
| Taylor et al, 200822 | 7-week, randomized, placebo-controlled, crossover trial (mean dose 3.1 ± 1.3 mg) | 13 outpatients with chronic civilian trauma PTSD, frequent nightmares, and sleep disturbance | Prazosin significantly increased total sleep time and REM sleep time; reduced trauma-related nightmares, distressed awakenings, and total PCL-C scores; improved CGI-I scores; and changed PDRS scores toward normal dreaming |
| CAPS: Clinician-Administered PTSD Scale; CGI-C: Clinical Global Impression of Change; CGI-I: Clinical Global Impression of Improvement; PCL-C: PTSD Checklist-Civilian; PDRS: PTSD Dream Rating Scale; PTSD: posttraumatic stress disorder; RCTs: randomized controlled trials; REM: rapid eye movement | |||
Atypical antipsychotics
Atypical antipsychotics have been used to reduce nightmares in PTSD; however, most of the evidence from studies evaluated in the AASM’s Best Practice Guide were considered to be low quality.11 Quetiapine and ziprasidone were not included in the AASM review. See (Table 5) for a review of the evidence for atypical antipsychotics for treating PTSD nightmares.
Table 5
Combat-related nightmares: Evidence for atypical antipsychotics
| Study | Design | Patients/dosage | Results |
|---|---|---|---|
| Aripiprazole | |||
| Lambert, 2006 a | Case report | 4 veterans with combat-related PTSD (3 male, 1 female; age 22 to 24); dose: 15 to 30 mg; concurrent treatment sertraline or CBT | Decreased frequency of weekly nightmares and agitated sleep by at least 50% |
| Olanzapine | |||
| Stein et al, 2002 b | 8-week, double-blind, placebo-controlled study | 19 male veterans with combat-related PTSD (olanzapine group mean age: 55.2 ± 6.6; placebo group 51.1 ± 8.1); mean dose: 15 mg/d | Significantly greater reduction in sleep disturbances (PSQI: -3.29 vs 1.57; P = .01); significantly higher weight gain (13.2 lbs vs -3 lbs; P = .001) |
| Jakovljevic et al, 2003 c | Case reports | 5 veterans with combat-related PTSD for 6 to 7 years (age: 28 to 50); dose: 10 to 20 mg; adjunct treatment | Decreased frequency of nightmares within 3 days |
| Labbate et al, 2000 d | Case report | 1 male veteran (age: 58) with a 20-year history of combat-related PTSD; dose: 5 mg at bedtime; concurrent treatment with sertraline (200 mg/d), bupropion (150 mg/d), and diazepam (15 mg/d) | Eliminated nightmares after 1 week and improved sleep quality |
| Quetiapine | |||
| Ahearn et al, 2006 e | 8-week, open-label trial | 15 PTSD patients (8 male; 7 female; 5 with combat-related PTSD; mean age: 49); mean dose: 216 mg/d (100 to 400 mg/d) | Significantly improved re-experiencing (CAPS: 10 vs 23; P = .0012) and sleep (PSQI: 17.5 vs 30; P = .0044) at 8 weeks compared with baseline |
| Robert et al, 2005 f | 6-week, open-label trial | 19 combat veterans; mean dose: 100 ± 70 mg/d (25 to 300 mg/d); adjunct treatment | Significantly improved sleep quality (PSQI: 1.67 vs 2.41; P = .006), latency (PSQI: 1.5 vs 2.65; P = .002), duration (PSQI: 1.31 vs 2.71; P < .001), and sleep disturbances (PSQI: 1.22 vs 1.71; P = .034) and decreased terror episodes (PSQI-A: 0.73 vs 0.91; P = .040) and acting out dreams (PSQI-A: 1.07 vs 1.35; P = .013); however, no difference in nightmares caused by trauma (PSQI-A: 1.53 vs 2.06) |
| Sokolski et al, 2003 g | Retrospective chart review | 68 male Vietnam War combat veterans (mean age: 55 ± 3.5); mean dose: 155 ± 130 mg (25 to 700 mg); adjunct treatment | Improved sleep disturbances in 62% and nightmares in 25% of patients |
| Ahearn et al, 2003 h | Case report | 2 male patients with combat-related PTSD (age 53, 72); dose: 25 to 50 mg; adjunct to SSRI therapy | Decreased frequency of nightmares with increased sleep duration |
| Risperidone | |||
| David et al, 2006 i | 6-week, open-label trial | 17 male veterans with combat-related PTSD (mean age: 53.7 ± 3.8); mean maximum dose: 2.3 ± 0.6 mg (range: 1 to 3 mg) | Improved recurrent distressing dreams (CAPS B-2: 3.8 vs 5.4; P = .04), but not with the PSQI subscale (PSQI bad dreams: 2.5 vs 2.7; NS). Decreased nighttime awakenings (1.9 vs 2.8; P = .003) and trauma dreams (19% vs 38%; P = .04) |
| Leyba et al, 1998 j | Case reports | 3 male patients (age 43 to 46); dose: 1 to 3 mg; adjunct therapy | Decreased occurrence of nightmares |
| Ziprasidone | |||
| Siddiqui et al, 2005 k | Case report | 1 male veteran with chronic combat-related PTSD (age 55); dose: 80 to 120 mg/d; adjunct with trazodone (100 mg) and topiramate | Improved occurrence of nightmares up to 4 months |
CAPS: Clinician-Administered PTSD Scale; CAPS B-2: Clinician-Administered PTSD Scale B-2 (recurrent distressing dreams of the event); CBT: cognitive-behavioral therapy; PSQI: Pittsburgh Sleep Quality Index; PSQI-A: Pittsburgh Sleep Quality Index Addendum for PTSD; NS: not significant; PTSD: posttraumatic stress disorder; SSRI: selective serotonin reuptake inhibitor References
| |||
Comparing prazosin and quetiapine. A historical prospective cohort study of 237 veterans with PTSD receiving prazosin or quetiapine for nighttime PTSD symptoms demonstrated that although the 2 drugs have similar efficacy (defined as symptomatic improvement) for short-term, 6-month treatment (61% vs 62%; P=.54), a higher percentage of patients continued prazosin long-term (3 to 6 years) than those taking quetiapine (48% vs 24%; P < .001).23 Twenty-five percent of patients taking quetiapine switched to prazosin during the study, and approximately one-half of these patients remained on prazosin until the study’s end. Only 8% of prazosin patients switched to quetiapine, and none continued this therapy until study end.23 Patients in the quetiapine group were more likely to discontinue the drug because of lack of efficacy (13% vs 3%; P=.03) and adverse effects (35% vs 18%; P=.008), specifically sedation (21% vs 2%; P < .001) and metabolic effects (9% vs 0%; P=.014), compared with prazosin. Although this trial may be the only published comparison study of prazosin and quetiapine, its methodological quality has been questioned, which makes it difficult to draw definitive conclusions.
Metabolic syndrome—elevated diastolic blood pressure, increased waist circumference, and low high-density lipoprotein cholesterol—is common among PTSD patients treated with antipsychotics.24 This syndrome may be caused by medications, lifestyle factors, or long-term overactivation of stress-response pathways. A retrospective chart review at a community mental health center revealed that patients taking even low doses of quetiapine for insomnia gained an average of 5 lbs (P=.037).25 Another retrospective chart review at 2 military hospitals reported that patients receiving low-dose quetiapine (≤100 mg/d) gained an average of slightly less than 1 lb per month, which adds up to approximately 10 lbs per year (P < .001).26 The benefit of using atypical antipsychotics may be outweighed by metabolic risks such as obesity, new-onset diabetes, and dyslipidemia.27
Prazosin is considered a first-line treatment for sleep disturbances and nightmares in PTSD because of its superior long-term efficacy and decreased adverse effects compared with quetiapine.
Related Resources
- American Psychiatric Association. Practice guidelines for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Arlington, VA: American Psychiatric Publishing, Inc.; 2004.
- Veterans Affairs/Department of Defense clinical practice guidelines. Management of traumatic stress disorder and acute stress reaction. www.healthquality.va.gov/Post_Traumatic_Stress_Disorder_PTSD.asp.
Drug Brand Names
- Prazosin • Minipress
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
• Prazosin is recommended as a first-line therapy for nighttime PTSD symptoms, such as nightmares or sleep disturbances—especially among veterans—because of superior long-term effectiveness.
• Risk of metabolic syndrome, which has been reported with low-dose atypical antipsychotics used for treating insomnia, limits their use for PTSD-related nightmares.
Mr. S, a 45-year-old veteran, was diagnosed with posttraumatic stress disorder (PTSD) 18 years ago after a tour of duty in the Persian Gulf. He had combat-related flashbacks triggered by the smell of gasoline or smoke from a fire, was easily startled, and began to isolate himself socially. However, his symptoms improved when he started volunteering at his local Veterans Affairs Medical Center. After he lost his job 3 years ago, Mr. S started experiencing flashbacks. He was irritable, easily startled, and avoided things that reminded him of his time in the Persian Gulf. His psychiatrist prescribed sertraline, titrated to 200 mg/d. The drug reduced the severity of his avoidance and hyperarousal symptoms and improved his mood.
During a clinic visit, Mr. S says he is doing well and can fall asleep at night but is having recurring nightmares about traumatic events that occurred during combat. These nightmares wake him up and have become more frequent, occurring once per night for the past month. Mr. S says he has been watching more news programs about conflicts in Afghanistan and Iraq since the nightmares began. His psychiatrist starts quetiapine, 50 mg at bedtime for 7 nights then 100 mg at bedtime, but after 6 weeks Mr. S says his nightmares continue.
PTSD occurs in approximately 19% of Vietnam war combat veterans1 and 14% of service members returning from Iraq and Afghanistan.2 PTSD symptoms are classified into clusters: intrusive/re-experiencing; avoidant/numbing; and hyperarousal.3 Nightmares are part of the intrusive/re-experiencing cluster, which is Criterion B in DSM-IV-TR. See Table 1 for a description of DSM-IV-TR PTSD criteria. Among PTSD patients, 50% to 70% report PTSD-associated nightmares.4 Despite adequate treatment targeted to improve PTSD’s core symptoms, symptoms such as sleep disturbances or nightmares often persist.
Table 1
DSM-IV-TR diagnostic criteria for posttraumatic stress disorder
|
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Nightmares and other sleep disturbances are associated with significant distress and daytime impairment and can interfere with PTSD recovery4-8 by disrupting sleep-dependent processing of emotional experiences and causing repeated resensitization to trauma cues (Table 2).8
Table 2
Psychosocial consequences of sleep disruption in PTSD
| Increased reactivity to emotional cues |
| Compromised ability to function in social and occupational roles |
| Negative psychiatric outcomes, including suicidal ideation or worsening of depression or psychosis |
| Interference of natural recovery from trauma exposure |
| Repeated resensitization to trauma cues |
| Neurocognitive deficits |
| Neuroendocrine abnormalities |
| PTSD: posttraumatic stress disorder Source: Adapted from reference 8 |
Few randomized controlled medication trials specifically address PTSD-related nightmares. Most PTSD studies do not examine sleep outcomes as a primary measure, and comprehensive literature reviews could not offer evidence-based recommendations.9,10 The American Academy of Sleep Medicine (AASM) also noted a paucity of PTSD studies that identified nightmares as a primary outcome measure.11 See Table 3 for a list of recommended medication options for PTSD-associated nightmares.
Table 3
Recommended medication treatments for PTSD-associated nightmares
| Evidence level | Medication | Evidence |
|---|---|---|
| Recommended for treating PTSD-associated nightmares | ||
| 1, 4 | Prazosin | In 3 level 1 studies, adding prazosin (mean dose 3 mg/d) significantly decreased trauma-related nightmares according to the CAPS “recurrent distressing dreams” item after 3 to 9 weeks of treatment vs placebo in veteran and civilian patients (N = 57) |
| Not suggested for treating PTSD-associated nightmares | ||
| 1 | Venlafaxine | No difference between extended-release venlafaxine (37.5 to 300 mg/d) and placebo in the CAPS-SX17 “distressing dreams” item at 12 weeks in 340 PTSD patients |
| May be considered for treating PTSD-associated nightmares | ||
| 4 | Clonidine | Reduced the number of nightmares in 11 of 13 refugees for 2 weeks to 3 months (dose: 0.2 to 0.6 mg/d) |
| May be considered for treating PTSD-associated nightmares, but data are low grade and sparse | ||
| 4 | Trazodone | Although trazodone (25 to 600 mg) significantly decreased nightmare frequency in veteran patients during an 8-week hospital stay (N = 60), 19% discontinued therapy because of side effects |
| 4 | Olanzapine | Adjunctive olanzapine (10 to 20 mg) rapidly improved sleep in a case series of combat-related PTSD patients resistant to SSRIs and benzodiazepines (N = 5) |
| 4 | Risperidone | In case series, risperidone (0.5 to 3 mg) significantly decreased CAPS scores for recurrent distressing dreams and proportion of traumatic dreams documented in diaries of combat veterans over 6 weeks (N = 17), and improved nightmares in adult burn patients taking pain medications after 1 to 2 days (N = 10) |
| 4 | Aripiprazole | In a case series, aripiprazole (15 to 30 mg at bedtime) with CBT or sertraline significantly improved nightmares in 4 of 5 combat-related PTSD patients |
| 4 | Topiramate | Topiramate reduced nightmares in 79% of civilians with PTSD and fully suppressed nightmares in 50% of patients in a case series (N = 35) |
| 4 | Low-dose cortisol | Significant decrease in frequency but not intensity of nightmares with low-dose cortisol (10 mg/d) in civilians with PTSD (N = 3) |
| 4 | Fluvoxamine | In 2 case series, fluvoxamine (up to 300 mg/d) significantly decreased the IES-R level of “dreams about combat trauma” but not the SRRS “bad dreams” rating at 10 weeks (N = 21). During 4 to 12 weeks of follow-up there was a qualitative decrease in reported nightmares in veteran patients (n = 12) |
| 2 | Triazolam/nitrazepam | Limited data showed triazolam (0.5 mg) and nitrazepam (5 mg) provide equal efficacy in decreasing the number of patients who experience unpleasant dreams over 1 night |
| 4 | Phenelzine | One study showed phenelzine monotherapy (30 to 90 mg) resulted in elimination of nightmares within 1 month (N = 5); another reported “moderately reduced traumatic dreams” (N = 21) in veterans. Therapy was discontinued because of short-lived efficacy or plateau effect |
| 4 | Gabapentin | Adjunctive gabapentin (300 to 3,600 mg/d) improved insomnia and decreased nightmare frequency and/or intensity over 1 to 36 months in 30 veterans with PTSD |
| 4 | Cyproheptadine | Conflicting data ranges from eliminating nightmares to no changes in the presence or intensity of nightmares |
| 4 | TCAs | Among 10 Cambodian concentration camp survivors treated with TCAs, 4 reported their nightmares ceased and 4 reported improvement after 1-year follow-up |
| 4 | Nefazodone | Reduced nightmare occurrence in 3 open-label studies as monotherapy (386 to 600 mg/d). Not recommended first line because of hepatotoxicity risk |
| No recommendation because of sparse data | ||
| 2 | Clonazepam | Clonazepam (1 to 2 mg/d) was ineffective in decreasing frequency or intensity of combat-related PTSD nightmares in veterans (N = 6) |
Evidence levels:
| ||
| CAPS: Clinician-Administered PTSD Scale; CAPS-SX17: 17-item Clinician-Administered PTSD Scale; CBT: cognitive-behavioral therapy; IES-R: Impact of Event Scale-Revised; PTSD: posttraumatic stress disorder; SRRS: Stress Response Rating Scale; SSRI: selective serotonin reuptake inhibitor; TCAs: tricyclic antidepressants Source: Adapted from Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401 | ||
CASE CONTINUED: Medication change, improvement
After reviewing AASM’s treatment recommendations, we prescribe prazosin, 1 mg at bedtime for 7 nights, then increase by 1 mg at bedtime each week until Mr. S’s nightmares improve. He reports a substantial improvement in nightmare severity and frequency after a few weeks of treatment with prazosin, 5 mg at bedtime.
Prazosin
Prazosin is an α1-adrenergic receptor antagonist with good CNS penetrability. The rationale for reducing adrenergic activity to address intrusive PTSD symptoms has been well documented.12,13 In open-label trials,14-18 a chart review,19 and placebo-controlled trials,20-22prazosin reduced trauma nightmares and improved sleep quality and global clinical status more than placebo (Table 4). In these studies, prazosin doses ranged from 1 to 20 mg/d, with an average of 3 mg at bedtime and a starting dose of 1 mg. Prazosin is the only agent recommended in the AASM’s Best Practice Guide for treating PTSD-related nightmares.11
Table 4
RCTs of prazosin for trauma-related nightmares
| Study | Design | Patients | Results |
|---|---|---|---|
| Raskind et al, 200320 | 20-week, double-blind, placebo-controlled, crossover study (mean dose 9.5 mg/d at bedtime) | 10 Vietnam veterans with chronic PTSD and severe trauma-related nightmares | Prazosin was superior to placebo on scores on the recurrent distressing dreams item and difficulty falling/staying asleep item of the CAPS and change in PTSD severity and functional status on the CGI-C |
| Raskind et al, 200721 | 8-week, placebo-controlled, parallel study (mean dose 13.3 ± 3 mg/d in the evening) | 40 veterans with chronic PTSD, distressing trauma nightmares, and sleep disturbance | Prazosin was superior to placebo in reducing trauma nightmares and improving sleep quality and global clinical status; prazosin also shifted dream characteristics of trauma-related nightmares to those typical of normal dreams |
| Taylor et al, 200822 | 7-week, randomized, placebo-controlled, crossover trial (mean dose 3.1 ± 1.3 mg) | 13 outpatients with chronic civilian trauma PTSD, frequent nightmares, and sleep disturbance | Prazosin significantly increased total sleep time and REM sleep time; reduced trauma-related nightmares, distressed awakenings, and total PCL-C scores; improved CGI-I scores; and changed PDRS scores toward normal dreaming |
| CAPS: Clinician-Administered PTSD Scale; CGI-C: Clinical Global Impression of Change; CGI-I: Clinical Global Impression of Improvement; PCL-C: PTSD Checklist-Civilian; PDRS: PTSD Dream Rating Scale; PTSD: posttraumatic stress disorder; RCTs: randomized controlled trials; REM: rapid eye movement | |||
Atypical antipsychotics
Atypical antipsychotics have been used to reduce nightmares in PTSD; however, most of the evidence from studies evaluated in the AASM’s Best Practice Guide were considered to be low quality.11 Quetiapine and ziprasidone were not included in the AASM review. See (Table 5) for a review of the evidence for atypical antipsychotics for treating PTSD nightmares.
Table 5
Combat-related nightmares: Evidence for atypical antipsychotics
| Study | Design | Patients/dosage | Results |
|---|---|---|---|
| Aripiprazole | |||
| Lambert, 2006 a | Case report | 4 veterans with combat-related PTSD (3 male, 1 female; age 22 to 24); dose: 15 to 30 mg; concurrent treatment sertraline or CBT | Decreased frequency of weekly nightmares and agitated sleep by at least 50% |
| Olanzapine | |||
| Stein et al, 2002 b | 8-week, double-blind, placebo-controlled study | 19 male veterans with combat-related PTSD (olanzapine group mean age: 55.2 ± 6.6; placebo group 51.1 ± 8.1); mean dose: 15 mg/d | Significantly greater reduction in sleep disturbances (PSQI: -3.29 vs 1.57; P = .01); significantly higher weight gain (13.2 lbs vs -3 lbs; P = .001) |
| Jakovljevic et al, 2003 c | Case reports | 5 veterans with combat-related PTSD for 6 to 7 years (age: 28 to 50); dose: 10 to 20 mg; adjunct treatment | Decreased frequency of nightmares within 3 days |
| Labbate et al, 2000 d | Case report | 1 male veteran (age: 58) with a 20-year history of combat-related PTSD; dose: 5 mg at bedtime; concurrent treatment with sertraline (200 mg/d), bupropion (150 mg/d), and diazepam (15 mg/d) | Eliminated nightmares after 1 week and improved sleep quality |
| Quetiapine | |||
| Ahearn et al, 2006 e | 8-week, open-label trial | 15 PTSD patients (8 male; 7 female; 5 with combat-related PTSD; mean age: 49); mean dose: 216 mg/d (100 to 400 mg/d) | Significantly improved re-experiencing (CAPS: 10 vs 23; P = .0012) and sleep (PSQI: 17.5 vs 30; P = .0044) at 8 weeks compared with baseline |
| Robert et al, 2005 f | 6-week, open-label trial | 19 combat veterans; mean dose: 100 ± 70 mg/d (25 to 300 mg/d); adjunct treatment | Significantly improved sleep quality (PSQI: 1.67 vs 2.41; P = .006), latency (PSQI: 1.5 vs 2.65; P = .002), duration (PSQI: 1.31 vs 2.71; P < .001), and sleep disturbances (PSQI: 1.22 vs 1.71; P = .034) and decreased terror episodes (PSQI-A: 0.73 vs 0.91; P = .040) and acting out dreams (PSQI-A: 1.07 vs 1.35; P = .013); however, no difference in nightmares caused by trauma (PSQI-A: 1.53 vs 2.06) |
| Sokolski et al, 2003 g | Retrospective chart review | 68 male Vietnam War combat veterans (mean age: 55 ± 3.5); mean dose: 155 ± 130 mg (25 to 700 mg); adjunct treatment | Improved sleep disturbances in 62% and nightmares in 25% of patients |
| Ahearn et al, 2003 h | Case report | 2 male patients with combat-related PTSD (age 53, 72); dose: 25 to 50 mg; adjunct to SSRI therapy | Decreased frequency of nightmares with increased sleep duration |
| Risperidone | |||
| David et al, 2006 i | 6-week, open-label trial | 17 male veterans with combat-related PTSD (mean age: 53.7 ± 3.8); mean maximum dose: 2.3 ± 0.6 mg (range: 1 to 3 mg) | Improved recurrent distressing dreams (CAPS B-2: 3.8 vs 5.4; P = .04), but not with the PSQI subscale (PSQI bad dreams: 2.5 vs 2.7; NS). Decreased nighttime awakenings (1.9 vs 2.8; P = .003) and trauma dreams (19% vs 38%; P = .04) |
| Leyba et al, 1998 j | Case reports | 3 male patients (age 43 to 46); dose: 1 to 3 mg; adjunct therapy | Decreased occurrence of nightmares |
| Ziprasidone | |||
| Siddiqui et al, 2005 k | Case report | 1 male veteran with chronic combat-related PTSD (age 55); dose: 80 to 120 mg/d; adjunct with trazodone (100 mg) and topiramate | Improved occurrence of nightmares up to 4 months |
CAPS: Clinician-Administered PTSD Scale; CAPS B-2: Clinician-Administered PTSD Scale B-2 (recurrent distressing dreams of the event); CBT: cognitive-behavioral therapy; PSQI: Pittsburgh Sleep Quality Index; PSQI-A: Pittsburgh Sleep Quality Index Addendum for PTSD; NS: not significant; PTSD: posttraumatic stress disorder; SSRI: selective serotonin reuptake inhibitor References
| |||
Comparing prazosin and quetiapine. A historical prospective cohort study of 237 veterans with PTSD receiving prazosin or quetiapine for nighttime PTSD symptoms demonstrated that although the 2 drugs have similar efficacy (defined as symptomatic improvement) for short-term, 6-month treatment (61% vs 62%; P=.54), a higher percentage of patients continued prazosin long-term (3 to 6 years) than those taking quetiapine (48% vs 24%; P < .001).23 Twenty-five percent of patients taking quetiapine switched to prazosin during the study, and approximately one-half of these patients remained on prazosin until the study’s end. Only 8% of prazosin patients switched to quetiapine, and none continued this therapy until study end.23 Patients in the quetiapine group were more likely to discontinue the drug because of lack of efficacy (13% vs 3%; P=.03) and adverse effects (35% vs 18%; P=.008), specifically sedation (21% vs 2%; P < .001) and metabolic effects (9% vs 0%; P=.014), compared with prazosin. Although this trial may be the only published comparison study of prazosin and quetiapine, its methodological quality has been questioned, which makes it difficult to draw definitive conclusions.
Metabolic syndrome—elevated diastolic blood pressure, increased waist circumference, and low high-density lipoprotein cholesterol—is common among PTSD patients treated with antipsychotics.24 This syndrome may be caused by medications, lifestyle factors, or long-term overactivation of stress-response pathways. A retrospective chart review at a community mental health center revealed that patients taking even low doses of quetiapine for insomnia gained an average of 5 lbs (P=.037).25 Another retrospective chart review at 2 military hospitals reported that patients receiving low-dose quetiapine (≤100 mg/d) gained an average of slightly less than 1 lb per month, which adds up to approximately 10 lbs per year (P < .001).26 The benefit of using atypical antipsychotics may be outweighed by metabolic risks such as obesity, new-onset diabetes, and dyslipidemia.27
Prazosin is considered a first-line treatment for sleep disturbances and nightmares in PTSD because of its superior long-term efficacy and decreased adverse effects compared with quetiapine.
Related Resources
- American Psychiatric Association. Practice guidelines for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Arlington, VA: American Psychiatric Publishing, Inc.; 2004.
- Veterans Affairs/Department of Defense clinical practice guidelines. Management of traumatic stress disorder and acute stress reaction. www.healthquality.va.gov/Post_Traumatic_Stress_Disorder_PTSD.asp.
Drug Brand Names
- Prazosin • Minipress
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Dohrenwend BP, Turner JB, Turse NA, et al. The psychological risks of Vietnam for U.S. veterans: a revisit with new data and methods. Science. 2006;313(5789):979-982.
2. Tanielian T, Jaycox L. eds. Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND Corporation; 2008.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
4. Wittmann L, Schredl M, Kramer M. Dreaming in posttraumatic stress disorder: a critical review of phenomenology psychophysiology and treatment. Psychother Psychosom. 2007;76(1):25-39.
5. Clum GA, Nishith P, Resick PA. Trauma-related sleep disturbance and self-reported physical health symptoms in treatment-seeking female rape victims. J Nerv Ment Dis. 2001;189(9):618-622.
6. Kramer TL, Booth BM, Han X, et al. Service utilization and outcomes in medically ill veterans with posttraumatic stress and depressive disorders. J Trauma Stress. 2003;16(3):211-219.
7. Neylan TC, Marmar CR, Metzler TJ, et al. Sleep disturbances in the Vietnam generation: findings from a nationally representative sample of male Vietnam veterans. Am J Psychiatry. 1998;155(7):929-933.
8. Nappi CM, Drummond SP, Hall JM. Treating nightmares and insomnia in posttraumatic stress disorder: a review of current evidence. Neuropharmacology. 2012;62(2):576-585.
9. Maher MJ, Rego SA, Asnis GM. Sleep disturbances in patients with post-traumatic stress disorder: epidemiology impact and approaches to management. CNS Drugs. 2006;20(7):567-590.
10. van Liempt S, Vermetten E, Geuze E, et al. Pharmacotherapy for disordered sleep in post-traumatic stress disorder: a systematic review. Int Clin Psychopharmacol. 2006;21(4):193-202.
11. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401.
12. Boehnlein JK, Kinzie JD. Pharmacologic reduction of CNS noradrenergic activity in PTSD: the case for clonidine and prazosin. J Psychiatr Pract. 2007;13(2):72-78.
13. Strawn JR, Geracioti TD, Jr. Noradrenergic dysfunction and the psychopharmacology of posttraumatic stress disorder. Depress Anxiety. 2008;25(3):260-271.
14. Calohan J, Peterson K, Peskind ER, et al. Prazosin treatment of trauma nightmares and sleep disturbance in soldiers deployed in Iraq. J Trauma Stress. 2010;23(5):645-648.
15. Daly CM, Doyle ME, Radkind M, et al. Clinical case series: the use of Prazosin for combat-related recurrent nightmares among Operation Iraqi Freedom combat veterans. Mil Med. 2005;170(6):513-515.
16. Peskind ER, Bonner LT, Hoff DJ, et al. Prazosin reduces trauma-related nightmares in older men with chronic posttraumatic stress disorder. J Geriatr Psychiatry Neurol. 2003;16(3):165-171.
17. Raskind MA, Dobie DJ, Kanter ED, et al. The alpha1-adrenergic antagonist prazosin ameliorates combat trauma nightmares in veterans with posttraumatic stress disorder: a report of 4 cases. J Clin Psychiatry. 2000;61(2):129-133.
18. Taylor F, Raskind MA. The alpha1-adrenergic antagonist prazosin improves sleep and nightmares in civilian trauma posttraumatic stress disorder. J Clin Psychopharmacol. 2002;22(1):82-85.
19. Raskind MA, Thompson C, Petrie EC, et al. Prazosin reduces nightmares in combat veterans with posttraumatic stress disorder. J Clin Psychiatry. 2002;63(7):565-568.
20. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry. 2003;160(2):371-373.
21. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry. 2007;61(8):928-934.
22. Taylor FB, Martin P, Thompson C, et al. Prazosin effects on objective sleep measures and clinical symptoms in civilian trauma posttraumatic stress disorder: a placebo-controlled study. Biol Psychiatry. 2008;63(6):629-632.
23. Byers MG, Allison KM, Wendel CS, et al. Prazosin versus quetiapine for nighttime posttraumatic stress disorder symptoms in veterans: an assessment of long-term comparative effectiveness and safety. J Clin Psychopharmacol. 2010;30(3):225-229.
24. Jin H, Lanouette NM, Mudaliar S, et al. Association of posttraumatic stress disorder with increased prevalence of metabolic syndrome. J Clin Psychopharmacol. 2009;29(3):210-215.
25. Cates ME, Jackson CW, Feldman JM, et al. Metabolic consequences of using low-dose quetiapine for insomnia in psychiatric patients. Community Ment Health J. 2009;45(4):251-254.
26. Williams SG, Alinejad NA, Williams JA, et al. Statistically significant increase in weight caused by low-dose quetiapine. Pharmacotherapy. 2010;30(10):1011-1015.
27. American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65(2):267-272.
1. Dohrenwend BP, Turner JB, Turse NA, et al. The psychological risks of Vietnam for U.S. veterans: a revisit with new data and methods. Science. 2006;313(5789):979-982.
2. Tanielian T, Jaycox L. eds. Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND Corporation; 2008.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
4. Wittmann L, Schredl M, Kramer M. Dreaming in posttraumatic stress disorder: a critical review of phenomenology psychophysiology and treatment. Psychother Psychosom. 2007;76(1):25-39.
5. Clum GA, Nishith P, Resick PA. Trauma-related sleep disturbance and self-reported physical health symptoms in treatment-seeking female rape victims. J Nerv Ment Dis. 2001;189(9):618-622.
6. Kramer TL, Booth BM, Han X, et al. Service utilization and outcomes in medically ill veterans with posttraumatic stress and depressive disorders. J Trauma Stress. 2003;16(3):211-219.
7. Neylan TC, Marmar CR, Metzler TJ, et al. Sleep disturbances in the Vietnam generation: findings from a nationally representative sample of male Vietnam veterans. Am J Psychiatry. 1998;155(7):929-933.
8. Nappi CM, Drummond SP, Hall JM. Treating nightmares and insomnia in posttraumatic stress disorder: a review of current evidence. Neuropharmacology. 2012;62(2):576-585.
9. Maher MJ, Rego SA, Asnis GM. Sleep disturbances in patients with post-traumatic stress disorder: epidemiology impact and approaches to management. CNS Drugs. 2006;20(7):567-590.
10. van Liempt S, Vermetten E, Geuze E, et al. Pharmacotherapy for disordered sleep in post-traumatic stress disorder: a systematic review. Int Clin Psychopharmacol. 2006;21(4):193-202.
11. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401.
12. Boehnlein JK, Kinzie JD. Pharmacologic reduction of CNS noradrenergic activity in PTSD: the case for clonidine and prazosin. J Psychiatr Pract. 2007;13(2):72-78.
13. Strawn JR, Geracioti TD, Jr. Noradrenergic dysfunction and the psychopharmacology of posttraumatic stress disorder. Depress Anxiety. 2008;25(3):260-271.
14. Calohan J, Peterson K, Peskind ER, et al. Prazosin treatment of trauma nightmares and sleep disturbance in soldiers deployed in Iraq. J Trauma Stress. 2010;23(5):645-648.
15. Daly CM, Doyle ME, Radkind M, et al. Clinical case series: the use of Prazosin for combat-related recurrent nightmares among Operation Iraqi Freedom combat veterans. Mil Med. 2005;170(6):513-515.
16. Peskind ER, Bonner LT, Hoff DJ, et al. Prazosin reduces trauma-related nightmares in older men with chronic posttraumatic stress disorder. J Geriatr Psychiatry Neurol. 2003;16(3):165-171.
17. Raskind MA, Dobie DJ, Kanter ED, et al. The alpha1-adrenergic antagonist prazosin ameliorates combat trauma nightmares in veterans with posttraumatic stress disorder: a report of 4 cases. J Clin Psychiatry. 2000;61(2):129-133.
18. Taylor F, Raskind MA. The alpha1-adrenergic antagonist prazosin improves sleep and nightmares in civilian trauma posttraumatic stress disorder. J Clin Psychopharmacol. 2002;22(1):82-85.
19. Raskind MA, Thompson C, Petrie EC, et al. Prazosin reduces nightmares in combat veterans with posttraumatic stress disorder. J Clin Psychiatry. 2002;63(7):565-568.
20. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry. 2003;160(2):371-373.
21. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry. 2007;61(8):928-934.
22. Taylor FB, Martin P, Thompson C, et al. Prazosin effects on objective sleep measures and clinical symptoms in civilian trauma posttraumatic stress disorder: a placebo-controlled study. Biol Psychiatry. 2008;63(6):629-632.
23. Byers MG, Allison KM, Wendel CS, et al. Prazosin versus quetiapine for nighttime posttraumatic stress disorder symptoms in veterans: an assessment of long-term comparative effectiveness and safety. J Clin Psychopharmacol. 2010;30(3):225-229.
24. Jin H, Lanouette NM, Mudaliar S, et al. Association of posttraumatic stress disorder with increased prevalence of metabolic syndrome. J Clin Psychopharmacol. 2009;29(3):210-215.
25. Cates ME, Jackson CW, Feldman JM, et al. Metabolic consequences of using low-dose quetiapine for insomnia in psychiatric patients. Community Ment Health J. 2009;45(4):251-254.
26. Williams SG, Alinejad NA, Williams JA, et al. Statistically significant increase in weight caused by low-dose quetiapine. Pharmacotherapy. 2010;30(10):1011-1015.
27. American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65(2):267-272.
P-glycoprotein: Why this drug transporter may be clinically important
Discuss this article at www.facebook.com/CurrentPsychiatry
• Venlafaxine has been shown to decrease indinavir concentrations in cellular models and healthy individuals in a controlled trial.
• It is not known if this effect would occur with other protease inhibitors; however, most protease inhibitors are P-glycoprotein substrates.
• In preliminary cellular models, desvenlafaxine did not have the same effect.
• It is not known if other psychotropics have the same effect on P-glycoprotein or other efflux proteins.
Mr. B, age 32, was diagnosed with human immunodeficiency virus (HIV) approximately 10 years ago. His current HIV regimen is highly active antiretroviral therapy, which includes the protease inhibitor (PI) indinavir and the combination product lamivudine and zidovudine, 2 nucleoside reverse transcriptase inhibitors. He shows no symptoms and his viral load has been undetectable for 9 years.
Several months ago, Mr. B reported to his primary care physician feelings of depressed mood, anhedonia, significant weight loss, fatigue, and feelings of worthlessness. He was diagnosed with major depressive disorder and started venlafaxine, 150 mg/d. The depressive episode is now in remission and the only major side effect he experiences is lethargy. His physician decides to check Mr. B’s viral load, which is 1,100 copies/mL. This viral load value indicates a significant elevation from the baseline (<48 copies/mL), which although still low, is considered virologic failure.1 To rule out a lab error the viral load test is replicated, but the result is the same.
Mr. B’s case may represent an interaction between his antidepressant and one of his antiviral drugs that is a P-glycoprotein substrate. This protein transports a variety of drug substrates across cell membranes and affects the distribution and elimination of many prescription and nonprescription medications. Whether a drug induces or inhibits P-glycoprotein can affect plasma and cellular concentrations of drugs and can lead to unexpected increases or decreases in plasma concentrations of the affected drug. Understanding P-glycoprotein’s role can help you choose effective psychotropics for patients such as Mr. B.
Change in drug effect
Because depression is common among patients with HIV, my colleagues and I evaluated the pharmacokinetic effects of indinavir on venlafaxine and venlafaxine on indinavir to determine if venlafaxine would be safe to use in a patient taking a PI because of potential cytochrome P450 (CYP450) drug interactions in both classes of medications.2 Adding venlafaxine resulted in a 36% decrease in maximum concentrations for indinavir and a 28% decrease in area under the curve Figure.2 Study participants were healthy individuals; however, we concluded that had we studied patients with HIV, indinavir efficacy could decrease, resulting in an increased viral load. After this study, the manufacturer of venlafaxine included a caution about this combination in the product labeling.3 Because the extended-release formulation includes the same compound, the same effect could be expected and was included in the most recent version of the extended-release venlafaxine prescribing information.4
What is interesting about the venlafaxine-indinavir interaction is that there was no change in either agent’s half-life and therefore no reason to assume this effect was a traditional CYP450 drug interaction. The investigators considered other types of drug interactions and focused on mechanisms that could be presystemic, ie, affecting the absorption and bioavailability of indinavir. This led investigators to believe that the mechanism involved a drug transport protein such as P-glycoprotein, which is present in gut lumen. Subsequent studies have shown in a cellular model that venlafaxine—but not desvenlafaxine—is an inducer of P-glycoprotein and breast cancer resistant protein (BCRP).5,6 Researchers are conducting animal studies to attempt to duplicate the cellular models. However, it could be presumed that the study of venlafaxine and indinavir in healthy individuals already had demonstrated this effect.2
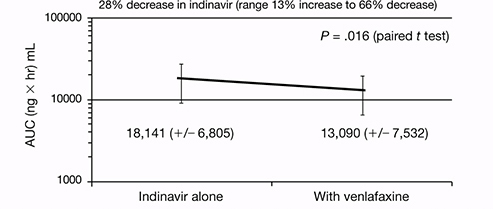
Figure: Indinavir area under the curve before and after steady state venlafaxine
Decrease in area under the curve (AUC) for indinavir when healthy individuals achieved steady state dosing of venlafaxine
Source: Reference 2
Cause and effect
P-glycoprotein transports drugs or other foreign compounds out of the cells (efflux) of the target tissue so they can be further metabolized by metabolic enzymes for elimination. These proteins are called efflux proteins. There are many efflux proteins in addition to P-glycoprotein; a common one is BCRP, which confers resistance to some anticancer drugs. In addition to the gut lumen and breast tissue, efflux proteins are present in most tissues throughout the body, including the blood-brain barrier.
If drug A inhibits an efflux protein, then drug B would be able to enter the target tissue with greater ease and not be “kicked out” because the efflux system would be disabled. This could result in higher-than-expected tissue concentrations of drug B. Pharmaceutical companies often perform P-glycoprotein inhibition studies before a drug is marketed and include this data in the prescribing information.
If, on the other hand, drug A induces an efflux protein, then drug B would be “kicked out” at a greater rate than normal because the efflux system would be working in overdrive. In this case, tissue concentrations of drug B would be lower than expected and could lead to therapeutic failure. Typically, pharmaceutical companies either do not conduct these induction studies, or if they are performed, they often are not described in prescribing information. This lack of efficacy has been well documented with chemotherapeutic failure caused by drug efflux by BCRP.7 It is likely that Mr. B’s viral load increased when venlafaxine was added to his regimen—the antidepressant induced P-glycoprotein, which reduced indinavir concentrations and subsequent therapeutic effect.
Clinicians should review specific medications they are considering using if the drugs have a narrow therapeutic index or if therapeutic failure from subtherapeutic or supratherapeutic doses would be considered problematic Table.8 Kim9 provides a comprehensive list of P-glycoprotein substrates, inhibitors, and inducers. However, keep in mind that the list of substrates, inhibitors, and inducers changes regularly as new research becomes available.
Table
Selected psychotropics that affect P-glycoprotein
| Substrates | |
| Amitriptyline | Paroxetine |
| Carbamazepine | Quetiapine |
| Chlorpromazine | Risperidone |
| Citalopram | Sertraline |
| Doxepin | Topiramate |
| Nortriptyline | Venlafaxine |
| Olanzapine | |
| Inhibitors | |
| Amitriptyline | Imipramine |
| Carbamazepine | Nefazodone |
| Chlorpromazine | Paroxetine |
| Desipramine | Sertraline |
| Disulfiram | Thioridazine |
| Fluoxetine | Trifluoperazine |
| Fluvoxamine | Trimipramine |
| Haloperidol | |
| Inducersa | |
| Amitriptyline | Phenothiazines |
| Nefazodone | Trazodone |
| aData supporting induction is limited Source: Reference 8 | |
- Linnet K, Ejsing TB. A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol. 2008;18(3):157-169.
- Weiss J, Dormann SM, Martin-Facklam M, et al. Inhibition of P-glycoprotein by newer antidepressants. J Pharmacol Exp Ther. 2003;305(1):197-204.
Drug Brand Names
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Desipramine • Norpramin
- Desvenlafaxine • Pristiq
- Disulfiram • Antabuse
- Doxepin • Adapin, Silenor
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Indinavir • Crixivan
- Lamivudine and zidovudine • Combivir
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Melleril
- Topiramate • Topamax
- Trazodone • Desyrel, Oleptro
- Trifluoperazine • Stelazine
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Disclosure
Dr. Levin receives grant/research support from Pfizer.
1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington DC: Department of Health and Human Services; January 10, 2011;1-166.
2. Levin GM, Nelson LA, DeVane CL, et al. A pharmacokinetic drug-drug interaction study of venlafaxine and indinavir. Psychopharmacol Bull. 2001;35(2):62-71.
3. Effexor [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2010.
4. Effexor XR [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2011.
5. Ehret MJ, Levin GM, Narasimhan M, et al. Venlafaxine induces P-glycoprotein in human Caco-2 cells. Hum Psychopharmacol. 2007;22(1):49-53.
6. Bachmeier CJ, Beaulieu-Abdelahad D, Ganey NJ, et al. Induction of drug efflux protein expression by venlafaxine but not desvenlafaxine. Biopharm Drug Dispos. 2011;32(4):233-244.
7. Rosenberg MF, Bikadi Z, Chan J, et al. The human breast cancer resistance protein (BCRP/ABCG2) shows conformational changes with mitoxantrone. Structure. 2010;18(4):482-493.
8. Oesterheld J. P-glycoprotein (PGP) table - the effect of drugs and foods. http://www.genemedrx.com/PGPtable.php. Accessed February 3 2012.
9. Kim RB. Drugs as P-glycoprotein substrates inhibitors, and inducers. Drug Metab Rev. 2002;34(1-2):47-54.
Gary M. Levin, PharmD, BCPP, FCCP
Dr. Levin is Associate Dean for Clinical Programs and Professor of Pharmacy Practice, College of Pharmacy, Roseman University of Health Sciences, Henderson, NV.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Gary M. Levin, PharmD, BCPP, FCCP
Dr. Levin is Associate Dean for Clinical Programs and Professor of Pharmacy Practice, College of Pharmacy, Roseman University of Health Sciences, Henderson, NV.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Gary M. Levin, PharmD, BCPP, FCCP
Dr. Levin is Associate Dean for Clinical Programs and Professor of Pharmacy Practice, College of Pharmacy, Roseman University of Health Sciences, Henderson, NV.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Discuss this article at www.facebook.com/CurrentPsychiatry
• Venlafaxine has been shown to decrease indinavir concentrations in cellular models and healthy individuals in a controlled trial.
• It is not known if this effect would occur with other protease inhibitors; however, most protease inhibitors are P-glycoprotein substrates.
• In preliminary cellular models, desvenlafaxine did not have the same effect.
• It is not known if other psychotropics have the same effect on P-glycoprotein or other efflux proteins.
Mr. B, age 32, was diagnosed with human immunodeficiency virus (HIV) approximately 10 years ago. His current HIV regimen is highly active antiretroviral therapy, which includes the protease inhibitor (PI) indinavir and the combination product lamivudine and zidovudine, 2 nucleoside reverse transcriptase inhibitors. He shows no symptoms and his viral load has been undetectable for 9 years.
Several months ago, Mr. B reported to his primary care physician feelings of depressed mood, anhedonia, significant weight loss, fatigue, and feelings of worthlessness. He was diagnosed with major depressive disorder and started venlafaxine, 150 mg/d. The depressive episode is now in remission and the only major side effect he experiences is lethargy. His physician decides to check Mr. B’s viral load, which is 1,100 copies/mL. This viral load value indicates a significant elevation from the baseline (<48 copies/mL), which although still low, is considered virologic failure.1 To rule out a lab error the viral load test is replicated, but the result is the same.
Mr. B’s case may represent an interaction between his antidepressant and one of his antiviral drugs that is a P-glycoprotein substrate. This protein transports a variety of drug substrates across cell membranes and affects the distribution and elimination of many prescription and nonprescription medications. Whether a drug induces or inhibits P-glycoprotein can affect plasma and cellular concentrations of drugs and can lead to unexpected increases or decreases in plasma concentrations of the affected drug. Understanding P-glycoprotein’s role can help you choose effective psychotropics for patients such as Mr. B.
Change in drug effect
Because depression is common among patients with HIV, my colleagues and I evaluated the pharmacokinetic effects of indinavir on venlafaxine and venlafaxine on indinavir to determine if venlafaxine would be safe to use in a patient taking a PI because of potential cytochrome P450 (CYP450) drug interactions in both classes of medications.2 Adding venlafaxine resulted in a 36% decrease in maximum concentrations for indinavir and a 28% decrease in area under the curve Figure.2 Study participants were healthy individuals; however, we concluded that had we studied patients with HIV, indinavir efficacy could decrease, resulting in an increased viral load. After this study, the manufacturer of venlafaxine included a caution about this combination in the product labeling.3 Because the extended-release formulation includes the same compound, the same effect could be expected and was included in the most recent version of the extended-release venlafaxine prescribing information.4
What is interesting about the venlafaxine-indinavir interaction is that there was no change in either agent’s half-life and therefore no reason to assume this effect was a traditional CYP450 drug interaction. The investigators considered other types of drug interactions and focused on mechanisms that could be presystemic, ie, affecting the absorption and bioavailability of indinavir. This led investigators to believe that the mechanism involved a drug transport protein such as P-glycoprotein, which is present in gut lumen. Subsequent studies have shown in a cellular model that venlafaxine—but not desvenlafaxine—is an inducer of P-glycoprotein and breast cancer resistant protein (BCRP).5,6 Researchers are conducting animal studies to attempt to duplicate the cellular models. However, it could be presumed that the study of venlafaxine and indinavir in healthy individuals already had demonstrated this effect.2
Figure: Indinavir area under the curve before and after steady state venlafaxine
Decrease in area under the curve (AUC) for indinavir when healthy individuals achieved steady state dosing of venlafaxine
Source: Reference 2
Cause and effect
P-glycoprotein transports drugs or other foreign compounds out of the cells (efflux) of the target tissue so they can be further metabolized by metabolic enzymes for elimination. These proteins are called efflux proteins. There are many efflux proteins in addition to P-glycoprotein; a common one is BCRP, which confers resistance to some anticancer drugs. In addition to the gut lumen and breast tissue, efflux proteins are present in most tissues throughout the body, including the blood-brain barrier.
If drug A inhibits an efflux protein, then drug B would be able to enter the target tissue with greater ease and not be “kicked out” because the efflux system would be disabled. This could result in higher-than-expected tissue concentrations of drug B. Pharmaceutical companies often perform P-glycoprotein inhibition studies before a drug is marketed and include this data in the prescribing information.
If, on the other hand, drug A induces an efflux protein, then drug B would be “kicked out” at a greater rate than normal because the efflux system would be working in overdrive. In this case, tissue concentrations of drug B would be lower than expected and could lead to therapeutic failure. Typically, pharmaceutical companies either do not conduct these induction studies, or if they are performed, they often are not described in prescribing information. This lack of efficacy has been well documented with chemotherapeutic failure caused by drug efflux by BCRP.7 It is likely that Mr. B’s viral load increased when venlafaxine was added to his regimen—the antidepressant induced P-glycoprotein, which reduced indinavir concentrations and subsequent therapeutic effect.
Clinicians should review specific medications they are considering using if the drugs have a narrow therapeutic index or if therapeutic failure from subtherapeutic or supratherapeutic doses would be considered problematic Table.8 Kim9 provides a comprehensive list of P-glycoprotein substrates, inhibitors, and inducers. However, keep in mind that the list of substrates, inhibitors, and inducers changes regularly as new research becomes available.
Table
Selected psychotropics that affect P-glycoprotein
| Substrates | |
| Amitriptyline | Paroxetine |
| Carbamazepine | Quetiapine |
| Chlorpromazine | Risperidone |
| Citalopram | Sertraline |
| Doxepin | Topiramate |
| Nortriptyline | Venlafaxine |
| Olanzapine | |
| Inhibitors | |
| Amitriptyline | Imipramine |
| Carbamazepine | Nefazodone |
| Chlorpromazine | Paroxetine |
| Desipramine | Sertraline |
| Disulfiram | Thioridazine |
| Fluoxetine | Trifluoperazine |
| Fluvoxamine | Trimipramine |
| Haloperidol | |
| Inducersa | |
| Amitriptyline | Phenothiazines |
| Nefazodone | Trazodone |
| aData supporting induction is limited Source: Reference 8 | |
- Linnet K, Ejsing TB. A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol. 2008;18(3):157-169.
- Weiss J, Dormann SM, Martin-Facklam M, et al. Inhibition of P-glycoprotein by newer antidepressants. J Pharmacol Exp Ther. 2003;305(1):197-204.
Drug Brand Names
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Desipramine • Norpramin
- Desvenlafaxine • Pristiq
- Disulfiram • Antabuse
- Doxepin • Adapin, Silenor
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Indinavir • Crixivan
- Lamivudine and zidovudine • Combivir
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Melleril
- Topiramate • Topamax
- Trazodone • Desyrel, Oleptro
- Trifluoperazine • Stelazine
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Disclosure
Dr. Levin receives grant/research support from Pfizer.
Discuss this article at www.facebook.com/CurrentPsychiatry
• Venlafaxine has been shown to decrease indinavir concentrations in cellular models and healthy individuals in a controlled trial.
• It is not known if this effect would occur with other protease inhibitors; however, most protease inhibitors are P-glycoprotein substrates.
• In preliminary cellular models, desvenlafaxine did not have the same effect.
• It is not known if other psychotropics have the same effect on P-glycoprotein or other efflux proteins.
Mr. B, age 32, was diagnosed with human immunodeficiency virus (HIV) approximately 10 years ago. His current HIV regimen is highly active antiretroviral therapy, which includes the protease inhibitor (PI) indinavir and the combination product lamivudine and zidovudine, 2 nucleoside reverse transcriptase inhibitors. He shows no symptoms and his viral load has been undetectable for 9 years.
Several months ago, Mr. B reported to his primary care physician feelings of depressed mood, anhedonia, significant weight loss, fatigue, and feelings of worthlessness. He was diagnosed with major depressive disorder and started venlafaxine, 150 mg/d. The depressive episode is now in remission and the only major side effect he experiences is lethargy. His physician decides to check Mr. B’s viral load, which is 1,100 copies/mL. This viral load value indicates a significant elevation from the baseline (<48 copies/mL), which although still low, is considered virologic failure.1 To rule out a lab error the viral load test is replicated, but the result is the same.
Mr. B’s case may represent an interaction between his antidepressant and one of his antiviral drugs that is a P-glycoprotein substrate. This protein transports a variety of drug substrates across cell membranes and affects the distribution and elimination of many prescription and nonprescription medications. Whether a drug induces or inhibits P-glycoprotein can affect plasma and cellular concentrations of drugs and can lead to unexpected increases or decreases in plasma concentrations of the affected drug. Understanding P-glycoprotein’s role can help you choose effective psychotropics for patients such as Mr. B.
Change in drug effect
Because depression is common among patients with HIV, my colleagues and I evaluated the pharmacokinetic effects of indinavir on venlafaxine and venlafaxine on indinavir to determine if venlafaxine would be safe to use in a patient taking a PI because of potential cytochrome P450 (CYP450) drug interactions in both classes of medications.2 Adding venlafaxine resulted in a 36% decrease in maximum concentrations for indinavir and a 28% decrease in area under the curve Figure.2 Study participants were healthy individuals; however, we concluded that had we studied patients with HIV, indinavir efficacy could decrease, resulting in an increased viral load. After this study, the manufacturer of venlafaxine included a caution about this combination in the product labeling.3 Because the extended-release formulation includes the same compound, the same effect could be expected and was included in the most recent version of the extended-release venlafaxine prescribing information.4
What is interesting about the venlafaxine-indinavir interaction is that there was no change in either agent’s half-life and therefore no reason to assume this effect was a traditional CYP450 drug interaction. The investigators considered other types of drug interactions and focused on mechanisms that could be presystemic, ie, affecting the absorption and bioavailability of indinavir. This led investigators to believe that the mechanism involved a drug transport protein such as P-glycoprotein, which is present in gut lumen. Subsequent studies have shown in a cellular model that venlafaxine—but not desvenlafaxine—is an inducer of P-glycoprotein and breast cancer resistant protein (BCRP).5,6 Researchers are conducting animal studies to attempt to duplicate the cellular models. However, it could be presumed that the study of venlafaxine and indinavir in healthy individuals already had demonstrated this effect.2
Figure: Indinavir area under the curve before and after steady state venlafaxine
Decrease in area under the curve (AUC) for indinavir when healthy individuals achieved steady state dosing of venlafaxine
Source: Reference 2
Cause and effect
P-glycoprotein transports drugs or other foreign compounds out of the cells (efflux) of the target tissue so they can be further metabolized by metabolic enzymes for elimination. These proteins are called efflux proteins. There are many efflux proteins in addition to P-glycoprotein; a common one is BCRP, which confers resistance to some anticancer drugs. In addition to the gut lumen and breast tissue, efflux proteins are present in most tissues throughout the body, including the blood-brain barrier.
If drug A inhibits an efflux protein, then drug B would be able to enter the target tissue with greater ease and not be “kicked out” because the efflux system would be disabled. This could result in higher-than-expected tissue concentrations of drug B. Pharmaceutical companies often perform P-glycoprotein inhibition studies before a drug is marketed and include this data in the prescribing information.
If, on the other hand, drug A induces an efflux protein, then drug B would be “kicked out” at a greater rate than normal because the efflux system would be working in overdrive. In this case, tissue concentrations of drug B would be lower than expected and could lead to therapeutic failure. Typically, pharmaceutical companies either do not conduct these induction studies, or if they are performed, they often are not described in prescribing information. This lack of efficacy has been well documented with chemotherapeutic failure caused by drug efflux by BCRP.7 It is likely that Mr. B’s viral load increased when venlafaxine was added to his regimen—the antidepressant induced P-glycoprotein, which reduced indinavir concentrations and subsequent therapeutic effect.
Clinicians should review specific medications they are considering using if the drugs have a narrow therapeutic index or if therapeutic failure from subtherapeutic or supratherapeutic doses would be considered problematic Table.8 Kim9 provides a comprehensive list of P-glycoprotein substrates, inhibitors, and inducers. However, keep in mind that the list of substrates, inhibitors, and inducers changes regularly as new research becomes available.
Table
Selected psychotropics that affect P-glycoprotein
| Substrates | |
| Amitriptyline | Paroxetine |
| Carbamazepine | Quetiapine |
| Chlorpromazine | Risperidone |
| Citalopram | Sertraline |
| Doxepin | Topiramate |
| Nortriptyline | Venlafaxine |
| Olanzapine | |
| Inhibitors | |
| Amitriptyline | Imipramine |
| Carbamazepine | Nefazodone |
| Chlorpromazine | Paroxetine |
| Desipramine | Sertraline |
| Disulfiram | Thioridazine |
| Fluoxetine | Trifluoperazine |
| Fluvoxamine | Trimipramine |
| Haloperidol | |
| Inducersa | |
| Amitriptyline | Phenothiazines |
| Nefazodone | Trazodone |
| aData supporting induction is limited Source: Reference 8 | |
- Linnet K, Ejsing TB. A review on the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol. 2008;18(3):157-169.
- Weiss J, Dormann SM, Martin-Facklam M, et al. Inhibition of P-glycoprotein by newer antidepressants. J Pharmacol Exp Ther. 2003;305(1):197-204.
Drug Brand Names
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Desipramine • Norpramin
- Desvenlafaxine • Pristiq
- Disulfiram • Antabuse
- Doxepin • Adapin, Silenor
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Indinavir • Crixivan
- Lamivudine and zidovudine • Combivir
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Melleril
- Topiramate • Topamax
- Trazodone • Desyrel, Oleptro
- Trifluoperazine • Stelazine
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Disclosure
Dr. Levin receives grant/research support from Pfizer.
1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington DC: Department of Health and Human Services; January 10, 2011;1-166.
2. Levin GM, Nelson LA, DeVane CL, et al. A pharmacokinetic drug-drug interaction study of venlafaxine and indinavir. Psychopharmacol Bull. 2001;35(2):62-71.
3. Effexor [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2010.
4. Effexor XR [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2011.
5. Ehret MJ, Levin GM, Narasimhan M, et al. Venlafaxine induces P-glycoprotein in human Caco-2 cells. Hum Psychopharmacol. 2007;22(1):49-53.
6. Bachmeier CJ, Beaulieu-Abdelahad D, Ganey NJ, et al. Induction of drug efflux protein expression by venlafaxine but not desvenlafaxine. Biopharm Drug Dispos. 2011;32(4):233-244.
7. Rosenberg MF, Bikadi Z, Chan J, et al. The human breast cancer resistance protein (BCRP/ABCG2) shows conformational changes with mitoxantrone. Structure. 2010;18(4):482-493.
8. Oesterheld J. P-glycoprotein (PGP) table - the effect of drugs and foods. http://www.genemedrx.com/PGPtable.php. Accessed February 3 2012.
9. Kim RB. Drugs as P-glycoprotein substrates inhibitors, and inducers. Drug Metab Rev. 2002;34(1-2):47-54.
1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington DC: Department of Health and Human Services; January 10, 2011;1-166.
2. Levin GM, Nelson LA, DeVane CL, et al. A pharmacokinetic drug-drug interaction study of venlafaxine and indinavir. Psychopharmacol Bull. 2001;35(2):62-71.
3. Effexor [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2010.
4. Effexor XR [package insert]. Philadelphia PA: Wyeth Pharmaceuticals Inc.; 2011.
5. Ehret MJ, Levin GM, Narasimhan M, et al. Venlafaxine induces P-glycoprotein in human Caco-2 cells. Hum Psychopharmacol. 2007;22(1):49-53.
6. Bachmeier CJ, Beaulieu-Abdelahad D, Ganey NJ, et al. Induction of drug efflux protein expression by venlafaxine but not desvenlafaxine. Biopharm Drug Dispos. 2011;32(4):233-244.
7. Rosenberg MF, Bikadi Z, Chan J, et al. The human breast cancer resistance protein (BCRP/ABCG2) shows conformational changes with mitoxantrone. Structure. 2010;18(4):482-493.
8. Oesterheld J. P-glycoprotein (PGP) table - the effect of drugs and foods. http://www.genemedrx.com/PGPtable.php. Accessed February 3 2012.
9. Kim RB. Drugs as P-glycoprotein substrates inhibitors, and inducers. Drug Metab Rev. 2002;34(1-2):47-54.
Smoking cessation: What to tell patients about over-the-counter treatments
Discuss this article at www.facebook.com/CurrentPsychiatry
• Over-the-counter smoking cessation products likely will be the most appropriate first-line choice for many individuals before trying prescription products.
• Instruct patients to avoid smoking while using nicotine replacement therapy and educate them about the immediate and long-term benefits of quitting.
• Encourage patients to seek psychosocial counseling along with pharmacotherapy.
• Urge patients to engage in other quitting strategies by referring them to online and telephone resources (Related Resources). Also, encourage them to attend follow-up appointments to assess cessation therapy.
Mr. T, age 56, has major depressive disorder that is well controlled with fluoxetine, 40 mg/d. He has smoked ≥1 packs of cigarettes per day for the last 25 years. On a recent visit, he indicates that he has begun using a 21-mg nicotine patch as advised by his pharmacist and that things are going OK, although he has had some “slip ups.” He is on week 7 of his quitting regimen and now is stepping down the patch dosage.
Upon further questioning he says that he has been cutting the 21-mg patches in half to save money. Mr. T also explains that occasionally he has given in to a strong urge to smoke because it was “too much to handle.” He states that he does not think this is a big deal because he uses electronic cigarettes and has heard that these products don’t contain “the bad cancer stuff.” At the end of Mr. T’s visit, he asks for something to help him sleep because has been unable to sleep consistently and has been having vivid dreams since starting the patch. He also wants to know how to reduce itching from the patch.
Approximately 46 million Americans smoke and cigarette smoking accounts for 1 of every 5 deaths in the United States each year.1 Since the advent of “Stop Smoking” campaigns, bans on smoking in public buildings, over-the-counter (OTC) nicotine replacement products, and Surgeon General recommendations, discussing smoking cessation with patients has become standard practice.
Research suggests that treatment to quit smoking should include a combination of pharmacotherapy and counseling, such as cognitive-behavioral strategies, support groups, and quitting hotlines.2 Pharmacotherapy consists of OTC nicotine replacement therapy (NRT) products and prescription medications. This article briefly highlights how to counsel patients about using OTC NRT products (Table 1).2-5 See Table 2 for a summary of prescription smoking cessation agents
Table 1
Over-the-counter nicotine replacement therapy products
| Product | Dosage | Side effects | Amount of nicotine | Costa | Comments |
|---|---|---|---|---|---|
| Nicotine transdermal patches | For patients who smoked >.5 PPD: 21 mg/d for 6 weeks; 14 mg/d for 2 weeks; 7 mg/d for 2 weeks | Local skin irritation, sleep disturbances, and vivid dreams | 7, 14, or 21 mg /d | 21 mg: $32 for 14 patches 14 mg: $32 for 14 patches 7 mg: $19 for 7 patches | Alternate sites. Do not cut. Do not leave on skin for longer than life of patch (24 hours). Washing, bathing, swimming are OK. Remove patch if undergoing MRI because of reports of burns |
| For patients who smoked <.5 PPD: 14 mg/d for 6 weeks; 7 mg/d for 2 weeks | |||||
| Nicotine polacrilex gum | For patients who smoked ≥1.25 PPD: 4 mg | Unpleasant taste, jaw soreness, hiccups, dyspepsia, hypersalivation, and nausea (from chewing gum too quickly) | 2 or 4 mg per piece | 4 mg: $50 for 170 pieces 2 mg: $50 for 170 pieces | Use “chew and park” method. As part of combination therapy, use only as needed. No more than 24 pieces per day; use caution with patients with jaw or mouth conditions |
| For patients who smoked <1.25 PPD: 2 mg Weeks 1 to 6: 1 piece every 1 to 2 hours Weeks 7 to 9: 1 piece every 2 to 4 hours Weeks 10 to 12: 1 piece every 4 to 8 hours | |||||
| Nicotine polacrilex lozenge | For patients who smoked 1st cigarette within 30 minutes of waking: 4 mg | Mouth irritation, hiccups, nausea, cough, and insomnia | 2 or 4 mg per lozenge | 4 mg: $43 for 72 lozenges 2 mg: $43 for 72 lozenges | Dissolve lozenge in mouth for 20 to 30 minutes. Rotate lozenge to different parts of mouth occasionally. Do not chew. No more than 5 lozenges in 6 hours or 20 per day. Same taper schedule as nicotine gum |
| For patients who smoked 1st cigarette >30 minutes after waking: 2 mg | |||||
| aAll prices taken from drugstore.com on September 26, 2011 PPD: packs per day Source: References 2-5 | |||||
Patches
Nicotine replacement patches are best used for maintenance treatment of nicotine cravings. They deliver a fixed amount of nicotine over 24 hours.3 Patches have a specially formulated transdermal matrix system and should not be cut. Doing so damages the drug delivery system and could lead to drug evaporation from the cut edges.4 Mr. T’s psychiatrist advises him not to cut patches but instead purchase the 14-mg patch because he is at this step of the smoking cessation regimen.
Skin irritation caused by adhesive is a common adverse event from nicotine patches. Rotating the location of each patch to a different hairless body area is the best way to prevent or combat skin irritation. If rotating the location of the patch does not relieve irritation, patients can apply a thin layer of an OTC hydrocortisone 1% cream to the affected site 2 to 4 times a day after gently washing the area.5 Instruct patients to avoid using occlusive dressings over the topical application.
Nicotine replacement patches also have been reported to cause vivid dreams and insomnia.3 These side effects may be caused by nighttime nicotine absorption, which might be avoided by switching to a different NRT product or removing the 24-hour patch when going to bed.4
Combining treatments
Many patients experience nicotine cravings while using the nicotine replacement patch. Stressful situations and events can trigger a patient’s desire for nicotine and withdrawal symptoms that a patch that delivers a continuous amount of nicotine over 24 hours cannot alleviate. Combining different forms of treatment could combat these symptoms.2,3,5
Combination therapy might consist of using sustained-release bupropion or a nicotine patch with rapid-acting NRT products such as a lozenge, gum, nasal spray, or inhaler. In Mr. T’s case, clinicians recommend that he use nicotine polacrilex gum in addition to the patch to quell his cravings. Also, he is instructed to stop using electronic cigarettes because they are considered tobacco products, are not regulated by the FDA, and may contain toxic substances.6
Instruct patients who use nicotine gum to employ the “chew and park” method.4 First, they should chew the gum very slowly until they notice a minty taste or tingling feeling, then “park” the gum between the cheek and gums for 1 to 2 minutes to allow nicotine to be absorbed across the gum lining. After 2 minutes or when tingling ceases, patients should slowly resume chewing until a tingling or minty taste returns and then “park” the gum again in a different area of the gums. Tell patients to repeat the “chew and park” method until there is no more taste or tingling (approximately 30 minutes). Explain that chewing the gum too fast may result in nausea or lightheadedness and patients should refrain from eating or drinking 15 minutes before or while using the gum. Mr. T is instructed to use the gum only when the urge to smoke is overbearing, and not regularly.
The nicotine polacrilex gum is more viscous than ordinary chewing gum and may stick to or possibly damage dental work such as fillings, dentures, crowns, and braces. An acceptable alternative is the nicotine polacrilex lozenge. Advise patients who want to try lozenges to:
- place the lozenge in the mouth and allow it to dissolve slowly over 20 to 30 minutes (during this time patients may experience a tingling sensation as nicotine is released)
- rotate the lozenge to different areas of the mouth every few minutes to lessen irritation
- avoid chewing or swallowing the lozenge because doing so will lead to improper release of nicotine and side effects, including nausea, hiccups, and heartburn
- refrain from eating or drinking 15 minutes before or while using the lozenge.
For many patients, the breadth of pharmacologic agents available for smoking cessation has made quitting a more attainable goal. OTC smoking cessation products are available in most drug stores, which gives smokers easy access to taking this important step. Counseling patients on the proper use of OTC products may help them successfully stop smoking.7
Although a patient’s medical history, including cardiac status, must be considered before starting specific agents, in many instances patient preference is the prevailing factor when choosing therapy. Often, the risks of continued smoking outweigh the risks of using smoking cessation products. OTC smoking cessation products may be an appropriate first-line treatment for many individuals before trying prescription medications, such as bupropion or varenicline.
For patients
- Treat Tobacco. www.treatobacco.net.
- Smokefree.gov mobile application. http://smokefree.gov/apps.
- Medline Plus. Quitting smoking. www.nlm.nih.gov/medlineplus/quittingsmoking.html.
- Quit for Life Program. www.quitnow.net.
- American Lung Association. Stop Smoking. www.lungusa.org/stop-smoking.
For clinicians
- Agency for Health Research and Quality. Treating tobacco use and dependence: 2008 update. www.ahrq.gov/path/tobacco.htm#clinicians.
Drug Brand Names
- Bupropion SR • Zyban, Wellbutrin SR
- Fluoxetine • Prozac
- Varenicline • Chantix
Disclosure
Dr. Ellingrod receives grant/research support from the National Institute of Mental Health.
Dr. Burghardt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table 2
Prescription smoking cessation productsa
| Product | Dosage | Side effects | Amount of nicotine | Costb | Notes |
|---|---|---|---|---|---|
| Nicotine inhaler | 6 to 16 cartridges/d | Throat/mouth irritation and cough | 10 mg cartridges deliver 4 mg of nicotine | 10 mg inhaler with 168 cartridges: $213 | Vapor, not smoke, is released and deposited in mouth. Similar mechanism of action to nicotine gum. Continuously puff for ~20 minutes. Gradually reduce dosage over 12 weeks. Helps with patients who need the “action” of smoking. Caution in patients who have a history of bronchospastic disease because of potential airway irritation |
| Nicotine nasal spray | 10 mg/ml bottle 8 to 40 doses/d One dose is a spray to each nostril | Initial (~10 week) watery eyes, coughing, and nasal and throat irritation | 0.5 mg/spray | 10 ml bottle: $186 | Fastest delivery of nicotine vs other products. Tilt head back slightly when delivering spray. Do not sniff, swallow, or inhale through the nose. Continue treatment for 3 to 6 months with an individualized reduction in usage |
| Bupropion SR | 150 mg/d for 3 days, then 300 mg/d for 7 to 12 weeks or longer | Weight change, constipation, confusion, headache, and insomnia | N/A | 60 tablets: $106 | Patients should stop smoking during the second week of treatment. Combination treatment has achieved higher cessation rates. Avoid bedtime dosing to minimize insomnia (eg, 7 AM and 3 PM dosing strategy). Avoid in patients with seizure disorders |
| Varenicline | Days 1 to 3: 0.5 mg/d Days 4 to 7: 1 mg/d Day 8 to end of treatment: 2 mg/d Start treatment 1 week before quitting and continue for 3 to 6 months | Constipation, flatulence, nausea, vomiting, insomnia, and headache | N/A | Starting pack: $179 Continuing pack: $177 | Partial agonist of nicotinic acetylcholine receptor. Superiority to placebo has been shown but more studies are needed to show superiority to NRT. Safety and efficacy of combination therapy has not been established. Pack titrates dosage to 2 mg/d to decrease nausea. Take with water and food. Has a “black-box” warning for serious neuropsychiatric events, including suicidal ideations and behavior |
1. Centers for Disease Control and Prevention Smoking and Tobacco Use. Adult cigarette smoking in the United States: current estimate. http://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm. Accessed November 29 2011.
2. Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel, Liaisons, and Staff. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
3. Physicians’ Desk Reference. 64th ed. Montvale, NJ: Thomson PDR; 2010.
4. Kroon LA, Hudmon KS, Corelli RL. Smoking cessation. In: Berardi RR Ferreri SP, Hume AL, et al, eds. Handbook of nonprescription drugs: an interactive approach to self-care. 16th ed. Washington, DC: American Pharmacists Association; 2009:883–916.
5. Doering PL, Kennedy WK, Boothby LA. Substance-related disorders: alcohol nicotine, and caffeine. In: DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: a pathophysiologic approach. 7th ed. New York, NY: McGraw-Hill; 2008:1083–1098.
6. U.S. Food and Drug Administration. Electronic cigarettes. http://www.fda.gov/NewsEvents/PublicHealthFocus/ucm172906.htm. Accessed November 29, 2011.
7. Prokhorov AV, Hudmon KS, Marani S, et al. Engaging physicians and pharmacists in providing smoking cessation counseling. Arch Intern Med. 2010;170(18):1640-1646.
Kyle Burghardt, PharmD
Dr. Burghardt is a Research Fellow, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Dr. Ellingrod is Associate Professor, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Kyle Burghardt, PharmD
Dr. Burghardt is a Research Fellow, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Dr. Ellingrod is Associate Professor, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Kyle Burghardt, PharmD
Dr. Burghardt is a Research Fellow, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Dr. Ellingrod is Associate Professor, University of Michigan College of Pharmacy and School of Medicine, Department of Psychiatry, Ann Arbor, MI
Discuss this article at www.facebook.com/CurrentPsychiatry
• Over-the-counter smoking cessation products likely will be the most appropriate first-line choice for many individuals before trying prescription products.
• Instruct patients to avoid smoking while using nicotine replacement therapy and educate them about the immediate and long-term benefits of quitting.
• Encourage patients to seek psychosocial counseling along with pharmacotherapy.
• Urge patients to engage in other quitting strategies by referring them to online and telephone resources (Related Resources). Also, encourage them to attend follow-up appointments to assess cessation therapy.
Mr. T, age 56, has major depressive disorder that is well controlled with fluoxetine, 40 mg/d. He has smoked ≥1 packs of cigarettes per day for the last 25 years. On a recent visit, he indicates that he has begun using a 21-mg nicotine patch as advised by his pharmacist and that things are going OK, although he has had some “slip ups.” He is on week 7 of his quitting regimen and now is stepping down the patch dosage.
Upon further questioning he says that he has been cutting the 21-mg patches in half to save money. Mr. T also explains that occasionally he has given in to a strong urge to smoke because it was “too much to handle.” He states that he does not think this is a big deal because he uses electronic cigarettes and has heard that these products don’t contain “the bad cancer stuff.” At the end of Mr. T’s visit, he asks for something to help him sleep because has been unable to sleep consistently and has been having vivid dreams since starting the patch. He also wants to know how to reduce itching from the patch.
Approximately 46 million Americans smoke and cigarette smoking accounts for 1 of every 5 deaths in the United States each year.1 Since the advent of “Stop Smoking” campaigns, bans on smoking in public buildings, over-the-counter (OTC) nicotine replacement products, and Surgeon General recommendations, discussing smoking cessation with patients has become standard practice.
Research suggests that treatment to quit smoking should include a combination of pharmacotherapy and counseling, such as cognitive-behavioral strategies, support groups, and quitting hotlines.2 Pharmacotherapy consists of OTC nicotine replacement therapy (NRT) products and prescription medications. This article briefly highlights how to counsel patients about using OTC NRT products (Table 1).2-5 See Table 2 for a summary of prescription smoking cessation agents
Table 1
Over-the-counter nicotine replacement therapy products
| Product | Dosage | Side effects | Amount of nicotine | Costa | Comments |
|---|---|---|---|---|---|
| Nicotine transdermal patches | For patients who smoked >.5 PPD: 21 mg/d for 6 weeks; 14 mg/d for 2 weeks; 7 mg/d for 2 weeks | Local skin irritation, sleep disturbances, and vivid dreams | 7, 14, or 21 mg /d | 21 mg: $32 for 14 patches 14 mg: $32 for 14 patches 7 mg: $19 for 7 patches | Alternate sites. Do not cut. Do not leave on skin for longer than life of patch (24 hours). Washing, bathing, swimming are OK. Remove patch if undergoing MRI because of reports of burns |
| For patients who smoked <.5 PPD: 14 mg/d for 6 weeks; 7 mg/d for 2 weeks | |||||
| Nicotine polacrilex gum | For patients who smoked ≥1.25 PPD: 4 mg | Unpleasant taste, jaw soreness, hiccups, dyspepsia, hypersalivation, and nausea (from chewing gum too quickly) | 2 or 4 mg per piece | 4 mg: $50 for 170 pieces 2 mg: $50 for 170 pieces | Use “chew and park” method. As part of combination therapy, use only as needed. No more than 24 pieces per day; use caution with patients with jaw or mouth conditions |
| For patients who smoked <1.25 PPD: 2 mg Weeks 1 to 6: 1 piece every 1 to 2 hours Weeks 7 to 9: 1 piece every 2 to 4 hours Weeks 10 to 12: 1 piece every 4 to 8 hours | |||||
| Nicotine polacrilex lozenge | For patients who smoked 1st cigarette within 30 minutes of waking: 4 mg | Mouth irritation, hiccups, nausea, cough, and insomnia | 2 or 4 mg per lozenge | 4 mg: $43 for 72 lozenges 2 mg: $43 for 72 lozenges | Dissolve lozenge in mouth for 20 to 30 minutes. Rotate lozenge to different parts of mouth occasionally. Do not chew. No more than 5 lozenges in 6 hours or 20 per day. Same taper schedule as nicotine gum |
| For patients who smoked 1st cigarette >30 minutes after waking: 2 mg | |||||
| aAll prices taken from drugstore.com on September 26, 2011 PPD: packs per day Source: References 2-5 | |||||
Patches
Nicotine replacement patches are best used for maintenance treatment of nicotine cravings. They deliver a fixed amount of nicotine over 24 hours.3 Patches have a specially formulated transdermal matrix system and should not be cut. Doing so damages the drug delivery system and could lead to drug evaporation from the cut edges.4 Mr. T’s psychiatrist advises him not to cut patches but instead purchase the 14-mg patch because he is at this step of the smoking cessation regimen.
Skin irritation caused by adhesive is a common adverse event from nicotine patches. Rotating the location of each patch to a different hairless body area is the best way to prevent or combat skin irritation. If rotating the location of the patch does not relieve irritation, patients can apply a thin layer of an OTC hydrocortisone 1% cream to the affected site 2 to 4 times a day after gently washing the area.5 Instruct patients to avoid using occlusive dressings over the topical application.
Nicotine replacement patches also have been reported to cause vivid dreams and insomnia.3 These side effects may be caused by nighttime nicotine absorption, which might be avoided by switching to a different NRT product or removing the 24-hour patch when going to bed.4
Combining treatments
Many patients experience nicotine cravings while using the nicotine replacement patch. Stressful situations and events can trigger a patient’s desire for nicotine and withdrawal symptoms that a patch that delivers a continuous amount of nicotine over 24 hours cannot alleviate. Combining different forms of treatment could combat these symptoms.2,3,5
Combination therapy might consist of using sustained-release bupropion or a nicotine patch with rapid-acting NRT products such as a lozenge, gum, nasal spray, or inhaler. In Mr. T’s case, clinicians recommend that he use nicotine polacrilex gum in addition to the patch to quell his cravings. Also, he is instructed to stop using electronic cigarettes because they are considered tobacco products, are not regulated by the FDA, and may contain toxic substances.6
Instruct patients who use nicotine gum to employ the “chew and park” method.4 First, they should chew the gum very slowly until they notice a minty taste or tingling feeling, then “park” the gum between the cheek and gums for 1 to 2 minutes to allow nicotine to be absorbed across the gum lining. After 2 minutes or when tingling ceases, patients should slowly resume chewing until a tingling or minty taste returns and then “park” the gum again in a different area of the gums. Tell patients to repeat the “chew and park” method until there is no more taste or tingling (approximately 30 minutes). Explain that chewing the gum too fast may result in nausea or lightheadedness and patients should refrain from eating or drinking 15 minutes before or while using the gum. Mr. T is instructed to use the gum only when the urge to smoke is overbearing, and not regularly.
The nicotine polacrilex gum is more viscous than ordinary chewing gum and may stick to or possibly damage dental work such as fillings, dentures, crowns, and braces. An acceptable alternative is the nicotine polacrilex lozenge. Advise patients who want to try lozenges to:
- place the lozenge in the mouth and allow it to dissolve slowly over 20 to 30 minutes (during this time patients may experience a tingling sensation as nicotine is released)
- rotate the lozenge to different areas of the mouth every few minutes to lessen irritation
- avoid chewing or swallowing the lozenge because doing so will lead to improper release of nicotine and side effects, including nausea, hiccups, and heartburn
- refrain from eating or drinking 15 minutes before or while using the lozenge.
For many patients, the breadth of pharmacologic agents available for smoking cessation has made quitting a more attainable goal. OTC smoking cessation products are available in most drug stores, which gives smokers easy access to taking this important step. Counseling patients on the proper use of OTC products may help them successfully stop smoking.7
Although a patient’s medical history, including cardiac status, must be considered before starting specific agents, in many instances patient preference is the prevailing factor when choosing therapy. Often, the risks of continued smoking outweigh the risks of using smoking cessation products. OTC smoking cessation products may be an appropriate first-line treatment for many individuals before trying prescription medications, such as bupropion or varenicline.
For patients
- Treat Tobacco. www.treatobacco.net.
- Smokefree.gov mobile application. http://smokefree.gov/apps.
- Medline Plus. Quitting smoking. www.nlm.nih.gov/medlineplus/quittingsmoking.html.
- Quit for Life Program. www.quitnow.net.
- American Lung Association. Stop Smoking. www.lungusa.org/stop-smoking.
For clinicians
- Agency for Health Research and Quality. Treating tobacco use and dependence: 2008 update. www.ahrq.gov/path/tobacco.htm#clinicians.
Drug Brand Names
- Bupropion SR • Zyban, Wellbutrin SR
- Fluoxetine • Prozac
- Varenicline • Chantix
Disclosure
Dr. Ellingrod receives grant/research support from the National Institute of Mental Health.
Dr. Burghardt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table 2
Prescription smoking cessation productsa
| Product | Dosage | Side effects | Amount of nicotine | Costb | Notes |
|---|---|---|---|---|---|
| Nicotine inhaler | 6 to 16 cartridges/d | Throat/mouth irritation and cough | 10 mg cartridges deliver 4 mg of nicotine | 10 mg inhaler with 168 cartridges: $213 | Vapor, not smoke, is released and deposited in mouth. Similar mechanism of action to nicotine gum. Continuously puff for ~20 minutes. Gradually reduce dosage over 12 weeks. Helps with patients who need the “action” of smoking. Caution in patients who have a history of bronchospastic disease because of potential airway irritation |
| Nicotine nasal spray | 10 mg/ml bottle 8 to 40 doses/d One dose is a spray to each nostril | Initial (~10 week) watery eyes, coughing, and nasal and throat irritation | 0.5 mg/spray | 10 ml bottle: $186 | Fastest delivery of nicotine vs other products. Tilt head back slightly when delivering spray. Do not sniff, swallow, or inhale through the nose. Continue treatment for 3 to 6 months with an individualized reduction in usage |
| Bupropion SR | 150 mg/d for 3 days, then 300 mg/d for 7 to 12 weeks or longer | Weight change, constipation, confusion, headache, and insomnia | N/A | 60 tablets: $106 | Patients should stop smoking during the second week of treatment. Combination treatment has achieved higher cessation rates. Avoid bedtime dosing to minimize insomnia (eg, 7 AM and 3 PM dosing strategy). Avoid in patients with seizure disorders |
| Varenicline | Days 1 to 3: 0.5 mg/d Days 4 to 7: 1 mg/d Day 8 to end of treatment: 2 mg/d Start treatment 1 week before quitting and continue for 3 to 6 months | Constipation, flatulence, nausea, vomiting, insomnia, and headache | N/A | Starting pack: $179 Continuing pack: $177 | Partial agonist of nicotinic acetylcholine receptor. Superiority to placebo has been shown but more studies are needed to show superiority to NRT. Safety and efficacy of combination therapy has not been established. Pack titrates dosage to 2 mg/d to decrease nausea. Take with water and food. Has a “black-box” warning for serious neuropsychiatric events, including suicidal ideations and behavior |
Discuss this article at www.facebook.com/CurrentPsychiatry
• Over-the-counter smoking cessation products likely will be the most appropriate first-line choice for many individuals before trying prescription products.
• Instruct patients to avoid smoking while using nicotine replacement therapy and educate them about the immediate and long-term benefits of quitting.
• Encourage patients to seek psychosocial counseling along with pharmacotherapy.
• Urge patients to engage in other quitting strategies by referring them to online and telephone resources (Related Resources). Also, encourage them to attend follow-up appointments to assess cessation therapy.
Mr. T, age 56, has major depressive disorder that is well controlled with fluoxetine, 40 mg/d. He has smoked ≥1 packs of cigarettes per day for the last 25 years. On a recent visit, he indicates that he has begun using a 21-mg nicotine patch as advised by his pharmacist and that things are going OK, although he has had some “slip ups.” He is on week 7 of his quitting regimen and now is stepping down the patch dosage.
Upon further questioning he says that he has been cutting the 21-mg patches in half to save money. Mr. T also explains that occasionally he has given in to a strong urge to smoke because it was “too much to handle.” He states that he does not think this is a big deal because he uses electronic cigarettes and has heard that these products don’t contain “the bad cancer stuff.” At the end of Mr. T’s visit, he asks for something to help him sleep because has been unable to sleep consistently and has been having vivid dreams since starting the patch. He also wants to know how to reduce itching from the patch.
Approximately 46 million Americans smoke and cigarette smoking accounts for 1 of every 5 deaths in the United States each year.1 Since the advent of “Stop Smoking” campaigns, bans on smoking in public buildings, over-the-counter (OTC) nicotine replacement products, and Surgeon General recommendations, discussing smoking cessation with patients has become standard practice.
Research suggests that treatment to quit smoking should include a combination of pharmacotherapy and counseling, such as cognitive-behavioral strategies, support groups, and quitting hotlines.2 Pharmacotherapy consists of OTC nicotine replacement therapy (NRT) products and prescription medications. This article briefly highlights how to counsel patients about using OTC NRT products (Table 1).2-5 See Table 2 for a summary of prescription smoking cessation agents
Table 1
Over-the-counter nicotine replacement therapy products
| Product | Dosage | Side effects | Amount of nicotine | Costa | Comments |
|---|---|---|---|---|---|
| Nicotine transdermal patches | For patients who smoked >.5 PPD: 21 mg/d for 6 weeks; 14 mg/d for 2 weeks; 7 mg/d for 2 weeks | Local skin irritation, sleep disturbances, and vivid dreams | 7, 14, or 21 mg /d | 21 mg: $32 for 14 patches 14 mg: $32 for 14 patches 7 mg: $19 for 7 patches | Alternate sites. Do not cut. Do not leave on skin for longer than life of patch (24 hours). Washing, bathing, swimming are OK. Remove patch if undergoing MRI because of reports of burns |
| For patients who smoked <.5 PPD: 14 mg/d for 6 weeks; 7 mg/d for 2 weeks | |||||
| Nicotine polacrilex gum | For patients who smoked ≥1.25 PPD: 4 mg | Unpleasant taste, jaw soreness, hiccups, dyspepsia, hypersalivation, and nausea (from chewing gum too quickly) | 2 or 4 mg per piece | 4 mg: $50 for 170 pieces 2 mg: $50 for 170 pieces | Use “chew and park” method. As part of combination therapy, use only as needed. No more than 24 pieces per day; use caution with patients with jaw or mouth conditions |
| For patients who smoked <1.25 PPD: 2 mg Weeks 1 to 6: 1 piece every 1 to 2 hours Weeks 7 to 9: 1 piece every 2 to 4 hours Weeks 10 to 12: 1 piece every 4 to 8 hours | |||||
| Nicotine polacrilex lozenge | For patients who smoked 1st cigarette within 30 minutes of waking: 4 mg | Mouth irritation, hiccups, nausea, cough, and insomnia | 2 or 4 mg per lozenge | 4 mg: $43 for 72 lozenges 2 mg: $43 for 72 lozenges | Dissolve lozenge in mouth for 20 to 30 minutes. Rotate lozenge to different parts of mouth occasionally. Do not chew. No more than 5 lozenges in 6 hours or 20 per day. Same taper schedule as nicotine gum |
| For patients who smoked 1st cigarette >30 minutes after waking: 2 mg | |||||
| aAll prices taken from drugstore.com on September 26, 2011 PPD: packs per day Source: References 2-5 | |||||
Patches
Nicotine replacement patches are best used for maintenance treatment of nicotine cravings. They deliver a fixed amount of nicotine over 24 hours.3 Patches have a specially formulated transdermal matrix system and should not be cut. Doing so damages the drug delivery system and could lead to drug evaporation from the cut edges.4 Mr. T’s psychiatrist advises him not to cut patches but instead purchase the 14-mg patch because he is at this step of the smoking cessation regimen.
Skin irritation caused by adhesive is a common adverse event from nicotine patches. Rotating the location of each patch to a different hairless body area is the best way to prevent or combat skin irritation. If rotating the location of the patch does not relieve irritation, patients can apply a thin layer of an OTC hydrocortisone 1% cream to the affected site 2 to 4 times a day after gently washing the area.5 Instruct patients to avoid using occlusive dressings over the topical application.
Nicotine replacement patches also have been reported to cause vivid dreams and insomnia.3 These side effects may be caused by nighttime nicotine absorption, which might be avoided by switching to a different NRT product or removing the 24-hour patch when going to bed.4
Combining treatments
Many patients experience nicotine cravings while using the nicotine replacement patch. Stressful situations and events can trigger a patient’s desire for nicotine and withdrawal symptoms that a patch that delivers a continuous amount of nicotine over 24 hours cannot alleviate. Combining different forms of treatment could combat these symptoms.2,3,5
Combination therapy might consist of using sustained-release bupropion or a nicotine patch with rapid-acting NRT products such as a lozenge, gum, nasal spray, or inhaler. In Mr. T’s case, clinicians recommend that he use nicotine polacrilex gum in addition to the patch to quell his cravings. Also, he is instructed to stop using electronic cigarettes because they are considered tobacco products, are not regulated by the FDA, and may contain toxic substances.6
Instruct patients who use nicotine gum to employ the “chew and park” method.4 First, they should chew the gum very slowly until they notice a minty taste or tingling feeling, then “park” the gum between the cheek and gums for 1 to 2 minutes to allow nicotine to be absorbed across the gum lining. After 2 minutes or when tingling ceases, patients should slowly resume chewing until a tingling or minty taste returns and then “park” the gum again in a different area of the gums. Tell patients to repeat the “chew and park” method until there is no more taste or tingling (approximately 30 minutes). Explain that chewing the gum too fast may result in nausea or lightheadedness and patients should refrain from eating or drinking 15 minutes before or while using the gum. Mr. T is instructed to use the gum only when the urge to smoke is overbearing, and not regularly.
The nicotine polacrilex gum is more viscous than ordinary chewing gum and may stick to or possibly damage dental work such as fillings, dentures, crowns, and braces. An acceptable alternative is the nicotine polacrilex lozenge. Advise patients who want to try lozenges to:
- place the lozenge in the mouth and allow it to dissolve slowly over 20 to 30 minutes (during this time patients may experience a tingling sensation as nicotine is released)
- rotate the lozenge to different areas of the mouth every few minutes to lessen irritation
- avoid chewing or swallowing the lozenge because doing so will lead to improper release of nicotine and side effects, including nausea, hiccups, and heartburn
- refrain from eating or drinking 15 minutes before or while using the lozenge.
For many patients, the breadth of pharmacologic agents available for smoking cessation has made quitting a more attainable goal. OTC smoking cessation products are available in most drug stores, which gives smokers easy access to taking this important step. Counseling patients on the proper use of OTC products may help them successfully stop smoking.7
Although a patient’s medical history, including cardiac status, must be considered before starting specific agents, in many instances patient preference is the prevailing factor when choosing therapy. Often, the risks of continued smoking outweigh the risks of using smoking cessation products. OTC smoking cessation products may be an appropriate first-line treatment for many individuals before trying prescription medications, such as bupropion or varenicline.
For patients
- Treat Tobacco. www.treatobacco.net.
- Smokefree.gov mobile application. http://smokefree.gov/apps.
- Medline Plus. Quitting smoking. www.nlm.nih.gov/medlineplus/quittingsmoking.html.
- Quit for Life Program. www.quitnow.net.
- American Lung Association. Stop Smoking. www.lungusa.org/stop-smoking.
For clinicians
- Agency for Health Research and Quality. Treating tobacco use and dependence: 2008 update. www.ahrq.gov/path/tobacco.htm#clinicians.
Drug Brand Names
- Bupropion SR • Zyban, Wellbutrin SR
- Fluoxetine • Prozac
- Varenicline • Chantix
Disclosure
Dr. Ellingrod receives grant/research support from the National Institute of Mental Health.
Dr. Burghardt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table 2
Prescription smoking cessation productsa
| Product | Dosage | Side effects | Amount of nicotine | Costb | Notes |
|---|---|---|---|---|---|
| Nicotine inhaler | 6 to 16 cartridges/d | Throat/mouth irritation and cough | 10 mg cartridges deliver 4 mg of nicotine | 10 mg inhaler with 168 cartridges: $213 | Vapor, not smoke, is released and deposited in mouth. Similar mechanism of action to nicotine gum. Continuously puff for ~20 minutes. Gradually reduce dosage over 12 weeks. Helps with patients who need the “action” of smoking. Caution in patients who have a history of bronchospastic disease because of potential airway irritation |
| Nicotine nasal spray | 10 mg/ml bottle 8 to 40 doses/d One dose is a spray to each nostril | Initial (~10 week) watery eyes, coughing, and nasal and throat irritation | 0.5 mg/spray | 10 ml bottle: $186 | Fastest delivery of nicotine vs other products. Tilt head back slightly when delivering spray. Do not sniff, swallow, or inhale through the nose. Continue treatment for 3 to 6 months with an individualized reduction in usage |
| Bupropion SR | 150 mg/d for 3 days, then 300 mg/d for 7 to 12 weeks or longer | Weight change, constipation, confusion, headache, and insomnia | N/A | 60 tablets: $106 | Patients should stop smoking during the second week of treatment. Combination treatment has achieved higher cessation rates. Avoid bedtime dosing to minimize insomnia (eg, 7 AM and 3 PM dosing strategy). Avoid in patients with seizure disorders |
| Varenicline | Days 1 to 3: 0.5 mg/d Days 4 to 7: 1 mg/d Day 8 to end of treatment: 2 mg/d Start treatment 1 week before quitting and continue for 3 to 6 months | Constipation, flatulence, nausea, vomiting, insomnia, and headache | N/A | Starting pack: $179 Continuing pack: $177 | Partial agonist of nicotinic acetylcholine receptor. Superiority to placebo has been shown but more studies are needed to show superiority to NRT. Safety and efficacy of combination therapy has not been established. Pack titrates dosage to 2 mg/d to decrease nausea. Take with water and food. Has a “black-box” warning for serious neuropsychiatric events, including suicidal ideations and behavior |
1. Centers for Disease Control and Prevention Smoking and Tobacco Use. Adult cigarette smoking in the United States: current estimate. http://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm. Accessed November 29 2011.
2. Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel, Liaisons, and Staff. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
3. Physicians’ Desk Reference. 64th ed. Montvale, NJ: Thomson PDR; 2010.
4. Kroon LA, Hudmon KS, Corelli RL. Smoking cessation. In: Berardi RR Ferreri SP, Hume AL, et al, eds. Handbook of nonprescription drugs: an interactive approach to self-care. 16th ed. Washington, DC: American Pharmacists Association; 2009:883–916.
5. Doering PL, Kennedy WK, Boothby LA. Substance-related disorders: alcohol nicotine, and caffeine. In: DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: a pathophysiologic approach. 7th ed. New York, NY: McGraw-Hill; 2008:1083–1098.
6. U.S. Food and Drug Administration. Electronic cigarettes. http://www.fda.gov/NewsEvents/PublicHealthFocus/ucm172906.htm. Accessed November 29, 2011.
7. Prokhorov AV, Hudmon KS, Marani S, et al. Engaging physicians and pharmacists in providing smoking cessation counseling. Arch Intern Med. 2010;170(18):1640-1646.
1. Centers for Disease Control and Prevention Smoking and Tobacco Use. Adult cigarette smoking in the United States: current estimate. http://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm. Accessed November 29 2011.
2. Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel, Liaisons, and Staff. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
3. Physicians’ Desk Reference. 64th ed. Montvale, NJ: Thomson PDR; 2010.
4. Kroon LA, Hudmon KS, Corelli RL. Smoking cessation. In: Berardi RR Ferreri SP, Hume AL, et al, eds. Handbook of nonprescription drugs: an interactive approach to self-care. 16th ed. Washington, DC: American Pharmacists Association; 2009:883–916.
5. Doering PL, Kennedy WK, Boothby LA. Substance-related disorders: alcohol nicotine, and caffeine. In: DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: a pathophysiologic approach. 7th ed. New York, NY: McGraw-Hill; 2008:1083–1098.
6. U.S. Food and Drug Administration. Electronic cigarettes. http://www.fda.gov/NewsEvents/PublicHealthFocus/ucm172906.htm. Accessed November 29, 2011.
7. Prokhorov AV, Hudmon KS, Marani S, et al. Engaging physicians and pharmacists in providing smoking cessation counseling. Arch Intern Med. 2010;170(18):1640-1646.
Is there a link between aripiprazole and treatment-emergent psychosis?
Discuss this article at www.facebook.com/CurrentPsychiatry
• Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonist.
• Clinical predictors of aripiprazole-associated worsening of psychosis include low baseline level of psychopathology and previous treatment with high-dose antipsychotics.
• Rapid transition from a medication with significant anticholinergic properties to 1 without these properties may result in symptoms of activation, including restlessness, insomnia, and anxiety, which can be mistaken for worsening psychosis.
• Akathisia, a common adverse effect of aripiprazole, may masquerade as treatment-emergent worsening of psychotic symptoms.
Mr. N, age 29, presents to the emergency department at the urging of his family because of poor self-care, bizarre behavior, and disturbed sleep. He first experienced psychiatric symptoms 10 years ago after his mother died. He became dysphoric and paranoid, displaying bizarre responses and behaviors with poor self-care and a gradual functional decline. He has been taking sertraline, 100 mg/d, for 10 years.
Upon arrival at the hospital’s inpatient unit, Mr. N is unkempt, oddly related, and paranoid. His affect is constricted. Mr. N displays thought blocking and possibly is responding to internal stimuli. Sertraline is continued and haloperidol, 1 mg/d, is initiated. For the next 2 weeks, Mr. N continues to be oddly related, irritable, and paranoid, and experiences disturbed sleep and thought blocking. After an episode of impulsive aggression, the treatment team initiates aripiprazole, which is titrated to 30 mg/d for 1 week. Mr. N’s clinical status worsens; he is menacing toward other patients and his thinking is more disorganized, with loose associations and ideas of reference. He requires 4 injections of IM haloperidol, 5 mg, and several visits to the seclusion room over the next week. Haloperidol is increased to 30 mg/d over the next 10 days, then aripiprazole is discontinued because of a putative drug interaction with haloperidol. Following the medication changes Mr. N demonstrates better behavioral control, but still is grossly psychotic. While awaiting transfer to a state hospital, Mr. N receives a trial of olanzapine, 20 to 40 mg/d, for 2 weeks without significant benefit.
Several clinical trials demonstrate a significant reduction in intensity of psychotic symptoms with aripiprazole, which has a unique mechanism of action.1 However, since its FDA approval in 2002, several case reports have described treatment-emergent psychotic symptoms associated with aripiprazole initiation. Over the past 40 years, reports of worsening psychosis associated with antipsychotics have been limited to patients with schizophrenia who were taking high dosages or who had high plasma concentrations, when anticholinergic delirium may have explained increased psychotic symptoms.2-4
How can a drug effectively treat psychotic symptoms and occasionally worsen them? In this article, we discuss the relevant pharmacology and clinical literature on aripiprazole and try to make sense of this apparent paradox.
Unique pharmacologic profile
Antipsychotics have been reported to be either neutral antagonists or inverse agonists at the D2 receptor, based on in vitro data.5 Aripiprazole and its main metabolite, dehydroaripiprazole, originally were described as partial agonists at D2 dopamine receptors.6,7 However, it appears aripiprazole’s pharmacologic action is better explained by the concept of functional selectivity. Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonistic.5
Researchers have hypothesized that the pathophysiology of schizophrenia may, in part, be caused by dysfunction of mesocorticolimbic dopaminergic neurons characterized by an enhanced sensitivity of postsynaptic D2 receptors and increased sensitivity to dopaminergic drugs.8,9 In addition, chronic treatment with a D2 receptor antagonist is associated with increases in postsynaptic dopamine receptor density (ie, an increase in receptor reserve).10,11 Upregulation of D2 receptors may explain several features seen in patients chronically treated with antipsychotics, including tardive dyskinesia12 and rapid psychotic relapse after discontinuing an antipsychotic (supersensitivity psychosis).13 Because chronic antipsychotic treatment leads to high postsynaptic receptor reserve, aripiprazole initiation may produce overactivation of D2 receptors, which might worsen a patient’s condition.14 In vitro data15-18 and clinical observations indicate that aripiprazole has intrinsic efficacy at D2 receptors, as do clinical observations, such as:
- its propensity to reduce serum prolactin19
- a decreased likelihood of producing extrapyramidal side effects despite >80% occupancy of D2 receptors6
- case reports documenting aripiprazole-associated mania,20 improvement of risperidone-associated cognitive impairment,21 and pathologic gambling.22
Emergence or worsening of psychotic symptoms or a marginal antipsychotic effect may occur if aripiprazole is indeed a postsynaptic D2 receptor agonist. An individual patient’s outcome likely would depend on his or her sensitivity to psychosis and concurrent or previous exposure to a D2 receptor antagonist. For example, stimulation of postsynaptic D2 receptors may be further augmented if the dosage of the previous antipsychotic was reduced or withdrawn before initiating aripiprazole because additional receptors would be available for interaction with aripiprazole.
Case reports
A literature review revealed 23 reports of treatment-emergent psychosis associated with aripiprazole initiation (Table). The mean age of the patients was 47 (range: 17 to 69) and 57% were men. Most patients (87%) were diagnosed with a schizophrenia-spectrum illness before aripiprazole initiation. Most (57%) had mild, stable, or no psychotic symptoms before aripiprazole initiation. Most were receiving relatively high doses of antipsychotics (average chlorpromazine equivalents [CPZE]: 648 mg/d) before aripiprazole initiation. This medication was either decreased or discontinued in 70% of patients.
Emergence or worsening of psychotic symptoms included agitation, aggressive behavior, and increased psychomotor activity. However, akathisia evaluation was described in only 2 reports: 1 author identified akathisia symptoms, but attributed them to a concomitant antipsychotic (fluphenazine)23 and the other report specifically excluded the possibility of akathisia.24 Two systematic studies have attempted to establish risk factors for aripiprazole-associated worsening psychosis (Box).14,25
In our literature review, the mean final dose of aripiprazole was 21.5 mg/d (range: 2 to 60 mg/d). In the cases describing subsequent treatment, all but 1 patient were switched to another antipsychotic, including 2 whose psychotic symptoms stabilized with continuation of aripiprazole and addition of a second antipsychotic. Interestingly, in the case reported by Adan-Manes et al,26 initial treatment with aripiprazole monotherapy was efficacious, but a subsequent trial of adjunctive aripiprazole resulted in worsening psychosis.
Table
Case reports: Treatment-emergent psychosis associated with aripiprazole
| Study | Age, sex | Diagnosis | Before aripiprazole initiation | Pre-aripiprazole treatment | Aripiprazole dose | Concomitant psychotropic treatment | Subsequent treatment |
|---|---|---|---|---|---|---|---|
| Chiu et al, 2011a | 39, M | Schizophrenia | Psychiatrically stable, tardive dystonia | Clozapine, 300 mg/d | 10 mg/d | Valproic acid, 1,000 mg/d, clonazepam, 2 mg/d, mephenoxalone, 800 mg/d | Clozapine |
| Ekinci et al, 2010b | 17, M | ADHD | Inattention and impulsive aggression | Tapered and discontinued risperidone, 2.5 mg/d | 5 mg/d | Methylphenidate, 54 mg/d | Risperidone, 2 mg/d, methylphenidate, 36 mg/d |
| Selvaraj et al, 2010c | 49, F | Chronic depression | Depressive symptoms, suicidal ideation | None stated | 2 mg/d | Duloxetine, 80 mg/d, clonazepam, 2 mg/d | Duloxetine, 120 mg/d |
| Adan-Manes et al, 2009d | 23, M | Schizophrenia | No psychotic symptoms | Abrupt decrease of amisulpride dose from 800 mg/d to 400 mg/d | 20 mg/d | Biperiden, 4 mg/d | Amisulpride, 800 mg/d |
| Cho et al, 2009e | 45, F | Schizophrenia | Persistent psychotic symptoms, new onset diabetes with acute ketoacidosis | Haloperidol, 20 mg/d, abrupt clozapine discontinuation | 15 mg/d | Valproic acid, nortriptyline | Molindone, 150 mg/d |
| Ahuja et al, 2007f | 35, F | Schizoaffective disorder | Stable before medication change | Tapered amisulpride, 400 mg/d, over 6 weeks | 15 mg/d | None | Amisulpride, 600 mg/d |
| Lea et al, 2007g | 57, M | Schizophrenia | Persistent psychotic symptoms, treatment resistance, recent recovery from NMS | Discontinued ziprasidone, 200 mg/d | 30 mg/d | Lorazepam, 2 mg/d, amantadine, 100 mg, sertraline, 50 mg/d | Clozapine |
| Lea et al, 2007g | 49, M | Schizoaffective disorder | Delusions, verbal aggression, substance abuse, HCV | Decreased quetiapine dose from 800 mg/d to 400 mg/d | 15 mg/d | Divalproex, 1,000 mg/d, fluvoxamine, 200 mg/d, clonazepam, 2 mg/d | Lithium, quetiapine, 500 mg/d, haloperidol, 2 mg/d |
| Lea et al, 2007g | 60, M | Schizophrenia | Delusions, labile mood, aggression | Risperidone, 3 mg/d, interruption of fluphenazine, 75 mg/d | 20 mg/d | Divalproex, 4,500 mg/d, benztropine, 3 mg/d | Not discussed |
| Raja, 2007h | 30, M | Schizoaffective disorder | Negative symptoms, otherwise stable, recent citalopram discontinuation | Discontinued amisulpride, 800 mg/d over 2 weeks | 30 mg/d | Lithium | Amisulpride, 500 mg/d |
| Raja, 2007h | 69, F | Bipolar disorder | History of multiple relapses; presented with tremor, akathisia, weight gain | Discontinued risperidone, 2 mg/d, over 2 weeks | 15 mg/d | Lithium | Risperidone, 4 mg |
| Raja, 2007h | 59, F | Schizophrenia | Negative symptoms, otherwise stable | Reduced risperidone dosage from 5 mg/d to 4 mg/d | 7.5 mg/d | None | Risperidone, 5 mg/d |
| Thone, 2007i | 31, M | Schizophrenia | Confusion, agitation, delusions worsened with aripiprazole dose increase | None | 60 mg/d | None | Aripiprazole dose reduction to 15 mg/d, olanzapine, 10 mg/d |
| Glick et al, 2006j | 55, F | Schizophrenia | Stable before medication change | Tapered and discontinued thioridazine, 600 mg/d, over 3 months | 30 mg/d | None | Chlorpromazine, 200 mg/d, aripiprazole, 30 mg/d |
| Glick et al, 2006j | 52, M | Schizophrenia | Negative symptoms | Decreased olanzapine dose from 30 mg/d to 20 mg/d | 30 mg/d | None | Olanzapine, 30 mg/d |
| Barnas et al, 2005k | 57, F | Schizoaffective disorder | Stable before medication change | Discontinued perphenazine, 8 mg/d | 30 mg/d | None | Quetiapine, 350 mg/d |
| DeQuardo, 2004l | 54, M | Schizophrenia | History of aggression, residual paranoia, severe EPS | Haloperidol, 200 mg/d | 15 mg/d | Benztropine | Haloperidol |
| DeQuardo, 2004l | 51, M | Schizophrenia | History of aggression, persistent psychotic symptoms, treatment resistance | Olanzapine, 60 mg/d | 10 mg/d | None | Olanzapine |
| Ramaswamy et al, 2004m | 43, F | Schizoaffective disorder | Psychiatrically stable, multiple medication changes, including substituting carbamazepine for valproic acid | Discontinued ziprasidone, 160 mg/d, discontinued quetiapine, 400 mg/d, over 2 weeks | 30 mg/d | Propranolol, 30 mg/d, l-thyroxine, .05 mg/d, carbamazepine, 600 mg/d | Not available |
| Ramaswawamy et al, 2004m | 57, F | Schizoaffective disorder | History of multiple hospitalizations, but stable before medication change | Decreased olanzapine dose from 20 mg/d to 15 mg/d | 30 mg/d | Valproic acid, 2,000 mg/d | Ziprasidone |
| Ramaswawamy et al, 2004m | 67, F | Schizophrenia | Remote hospitalizations, recent worsened psychosis | Decreased ziprasidone dose from 200 mg/d to 160 mg/d 2 months previously | 30 mg/d | Carbamazepine, 200 mg/d | Not discussed |
| Ramaswamy et al, 2004m | 46, M | Schizophrenia | Persistent delusions while receiving risperidone, TD | Risperidone, 3 mg/d | 15 mg/d | Valproic acid, 1,500 mg/d | Risperidone, 3 mg/d |
| Reeves et al, 2004n | 50, M | Schizoaffective disorder | Relatively stable with nonthreatening delusions, hallucinations | Quetiapine, 800 mg/d | 30 mg/d | Divalproex, 2,000 mg/d | Olanzapine, 20 mg/d |
| ADHD: attention-deficit/hyperactivity disorder; EPS: extrapyramidal symptoms; HCV: hepatitis C virus; NMS: neuroleptic malignant syndrome; TD: tardive dyskinesia Source: References a. Chiu YH, Chen CH, Lu ML. Worsening psychosis after adding aripiprazole to clozapine. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):291-292. b. Ekinci O, Sabuncuoglu O. Psychosis associated with switching from risperidone to aripiprazole in an adolescent on methylphenidate treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(2):648-649. c. Selvaraj V, Ramaswamy S, Sharma A, et al. New-onset psychosis and emergence of suicidal ideation with aripiprazole. Am J Psychiatry. 2010;167(12):1535-1536. d. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246. e. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143. f. Ahuja N, Lloyd AJ. Aripiprazole and worsening of psychosis: a case report. J Clin Psychiatry. 2007;68(5):805-806. g. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342. h. Raja M. Improvement or worsening of psychotic symptoms after treatment with low doses of aripiprazole. Int J Neuropsychopharmacol. 2007;10(1):107-110. i. Thone J. Worsened agitation and confusion in schizophrenia subsequent to high-dose aripiprazole. J Neuropsychiatry Clin Neurosci. 2007;19(4):481-482. j. Glick ID, Duggal V, Hodulik C. Aripiprazole as a dopamine partial agonist: positive and negative effects. J Clin Psychopharmacol. 2006;26(1):101-103. k. Barnas ME, Hussain N, Petrides G. Treatment-emergent psychosis with aripiprazole. J Clin Psychiatry. 2005;66(10):1339. l. DeQuardo JR. Worsened agitation with aripiprazole: adverse effect of dopamine partial agonism? J Clin Psychiatry. 2004;65(1):132-133. m. Ramaswamy S, Vijay D, William M, et al. Aripiprazole possibly worsens psychosis. Int Clin Psychopharmacol. 2004;19(1):45-48. n. Reeves RR, Mack JE. Worsening schizoaffective disorder with aripiprazole. Am J Psychiatry. 2004;161(7):1308. | |||||||
Takeuchi et al14 aimed to establish predictors of worsening psychosis in a naturalistic setting where patients slowly transitioned to aripiprazole from previous antipsychotic treatment. Patients were required to be on a stable dose of an antipsychotic before participating in the study. Aripiprazole was started at 12 mg/d for 2 weeks with flexible dosing from weeks 2 to 52. Previous antipsychotic therapy was reduced biweekly by 25%. The incidence of worsening psychopathology after aripiprazole initiation was higher in the group of patients who had previously received high-dose antipsychotic therapy (average chlorpromazine equivalents [CPZE]: 727 mg/d) compared with the group on low dosages (average CPZE: 382 mg/d). It is possible that previous high-dose antipsychotic therapy was indicative of more significant baseline psychopathology; however, the worsened group and stabilized group had similar baseline Clinical Global Impressions-Severity scores.
Pae et al25 aimed to find predictors of worsening psychosis with aripiprazole in patients whose previous antipsychotic therapy was immediately discontinued. They found lower baseline disease severity was associated with significant worsening during the first month of aripiprazole treatment.
Other potential explanations
Aripiprazole’s manufacturer reported the incidence of psychosis-related adverse events in an analysis of 9 randomized schizophrenia trials.27 The rates of psychosis-related adverse events ranged from 0.6% to 18%, but there was no apparent relationship to study design or method of transitioning to aripiprazole. Rates of psychosis-related adverse events were similar between aripiprazole and the control group (placebo in 3 studies, another antipsychotic in 2 studies).
Emergence or worsening of psychotic symptoms temporally associated with aripiprazole initiation does not necessarily imply causation. As in Mr. N’s case, it is not always possible to determine whether worsening psychosis is the natural disease course or a treatment effect. In addition, it is not possible to differentiate lack of efficacy from a true propensity for aripiprazole to worsen psychosis.
It also is conceivable discontinuation or dosage reduction of a previous antipsychotic would worsen psychotic symptoms or cause side effects. When significant changes in psychopathology or side effects develop during the transition from 1 antipsychotic to another, it is difficult to determine etiology. Specifically, rapid transition from a medication with significant anticholinergic and antihistaminic properties—such as quetiapine or olanzapine—to 1 without these properties—such as aripiprazole—may result in symptoms of activation, including restlessness, insomnia, and anxiety. Consequently, these symptoms could be mistaken for worsening psychosis.28 Only 1 patient in this series was reported to abruptly discontinue an antipsychotic with significant anticholinergic properties (clozapine) before initiating aripiprazole.24 Studies by Takeuchi et al14 and Pae et al25 did not report the relative baseline use of antipsychotic medication with anticholinergic properties.
In a pooled analysis of treatment-emergent adverse events in 5 randomized clinical trials of patients receiving aripiprazole for acute relapse of schizophrenia, the incidence of akathisia was 10%, although it is not clear if this is a dose-related adverse effect.29 Because akathisia may be confused for worsening psychosis,30 it is possible akathisia was mistakenly identified as worsening psychotic symptoms in Mr. N’s case, as well as several reports from our literature review.
Covert akathisia is unlikely to explain worsening psychopathology observed in all patients in our literature review because confusion of akathisia and worsening psychosis is not a widespread phenomenon. In a post hoc analysis of pooled safety data from aripiprazole trials, Kane et al31 did not find a correlation between presence of akathisia and aripiprazole efficacy as measured by the Positive and Negative Syndrome Scale (PANSS) total, PANSS positive, PANSS negative, Clinical Global Impressions-Severity, Clinical Global Impressions-Improvement, and percentage of responders. Pae et al25 also noted there was no correlation between scores on the Barnes Akathisia Rating Scale and worsening psychopathology in patients switched to aripiprazole.
An antagonist always is an antagonist and clinicians have appreciated this concept since the days of chlorpromazine. The activity of aripiprazole, however, is on a pharmacologic continuum between a neutral antagonist and full agonist and currently there is no way to precisely determine the level of D2 receptor agonist action in a patient.
Although it is interesting to speculate that aripiprazole’s D2 receptor agonist action may contribute to worsening psychosis,32-34 there are other plausible explanations to consider. Rapid transition from a drug with significant anticholinergic properties and aripiprazole-associated akathisia may contribute to worsening psychopathology in patients starting aripiprazole. Because covert side effects may be incorrectly identified as psychotic agitation, we cannot exclude this as a possible etiologic factor in Mr. N’s case as well as the cases in our literature review.
Related Resource
- Abilify [package insert]. Princeton, NJ: Bristol-Myers Squibb; 2011.
Drug Brand Names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Biperiden • Akineton
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fluphenazine • Permitil, Prolixin
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Nortriptyline • Aventyl, Pamelor
- Methylphenidate • Concerta
- Molindone • Moban
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Mellaril
- Thyroxine • Synthroid
- Valproic acid • Depakene
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Citrome L. A review of aripiprazole in the treatment of patients with schizophrenia or bipolar I disorder. Neuropsychiatr Dis Treat. 2006;2(4):427-443.
2. Chong SA, Tan CH, Lee HS. Worsening of psychosis with clozapine and selective serotonin reuptake inhibitor combination: two case reports. J Clin Psychopharmacol. 1997;17(1):68-69.
3. Bowers MB Jr, Swigar ME. Psychotic patients who become worse on neuroleptics. J Clin Psychopharmacol. 1988;8(6):417-421.
4. Tornatore FL, Lee D, Sramek JJ. Psychotic exacerbation with haloperidol. Drug Intell Clin Pharm. 1981;15(3):209-213.
5. Beaulieu JM, Gainetdinov RR. The physiology signaling, and pharmacology of dopamine receptors. Pharmacol Rev. 2011;63(1):182-217.
6. Grunder G, Carlsson A, Wong DF. Mechanism of new antipsychotic medications: occupancy is not just antagonism. Arch Gen Psychiatry. 2003;60(10):974-977.
7. Wood MD, Scott C, Clarke K, et al. Aripiprazole and its human metabolite are partial agonists at the human dopamine D2 receptor, but the rodent metabolite displays antagonist properties. Eur J Pharmacol. 2006;546(1-3):88-94.
8. Seeman P, Weinshenker D, Quirion R, et al. Dopamine supersensitivity correlates with D2High states, implying many paths to psychosis. Proc Natl Acad Sci U S A. 2005;102(9):3513-3518.
9. Seeman P, Ko F, Jack E, et al. Consistent with dopamine supersensitivity, RGS9 expression is diminished in the amphetamine-treated animal model of schizophrenia and in postmortem schizophrenia brain. Synapse. 2007;61(5):303-309.
10. Burt DR, Creese I, Snyder SH. Antischizophrenic drugs: chronic treatment elevates dopamine receptor binding in brain. Science. 1977;196(4287):326-328.
11. Silvestri S, Seeman MV, Negrete JC, et al. Increased dopamine D2 receptor binding after long-term treatment with antipsychotics in humans: a clinical PET study. Psychopharmacology (Berl). 2000;152(2):174-180.
12. Sayers AC, Bürki HR, Ruch W, et al. Neuroleptic-induced hypersensitivity of striatal dopamine receptors in the rat as a model of tardive dyskinesias. Effects of clozapine, haloperidol, loxapine and chlorpromazine. Psychopharmacologia. 1975;41(2):97-104.
13. Moncrieff J. Does antipsychotic withdrawal provoke psychosis? Review of the literature on rapid onset psychosis (supersensitivity psychosis) and withdrawal-related relapse. Acta Psychiatr Scand. 2006;114(1):3-13.
14. Takeuchi H, Uchida H, Suzuki T, et al. Predictors of clinical worsening after a switch to aripiprazole in patients with schizophrenia: a 1-year naturalistic follow-up study. J Clin Psychopharmacol. 2009;29(4):394-395.
15. Shapiro DA, Renock S, Arrington E, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology. 2003;28(8):1400-1411.
16. Urban JD, Vargas GA, von Zastrow M, et al. Aripiprazole has functionally selective actions at dopamine D2 receptor-mediated signaling pathways. Neuropsychopharmacology. 2007;32(1):67-77.
17. Klewe IV, Nielsen SM, Tarpo L, et al. Recruitment of beta-arrestin2 to the dopamine D2 receptor: Insights into anti-psychotic and anti-parkinsonian drug receptor signaling. Neuropharmacology. 2008;54(8):1215-1222.
18. Masri B, Salahpour A, Didriksen M, et al. Antagonism of dopamine D2 receptor/beta-arrestin 2 interaction is a common property of clinically effective antipsychotics. Proc Natl Acad Sci U S A. 2008;105(36):13656-13661.
19. Shim JC, Shin JG, Kelly DL, et al. Adjunctive treatment with a dopamine partial agonist, aripiprazole, for antipsychotic-induced hyperprolactinemia: a placebo-controlled trial. Am J Psychiatry. 2007;164(9):1404-1410.
20. Padala PR, Wengel SP, Petty F. Manic episode during treatment with aripiprazole. Am J Psychiatry. 2007;164(1):172-173.
21. Hu CH, Pai N, Huang XF, et al. Potential control of risperidone-related cognitive deficits by adjunctive aripiprazole treatment. J Clin Psychopharmacol. 2011;31(1):135-136;author reply 136–137.
22. Cohen J, Magalon D, Boyer L, et al. Aripiprazole-induced pathological gambling: a report of 3 cases. Curr Drug Saf. 2011;6(1):51-53.
23. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342.
24. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143.
25. Pae CU, Chiesa A, Mandelli L, et al. Predictors of early worsening after switch to aripiprazole: a randomized, controlled, open-label study. Clin Drug Investig. 2010;30(3):187-193.
26. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246.
27. Cognata-Smith C, Baker RA, Pikalov A, et al. Analysis of nine aripiprazole trials to evaluate strategies for switching patients with schizophrenia to aripiprazole. Paper presented at: 162nd Annual Meeting American Psychiatric Association; May 16-21, 2009; San Francisco, CA.
28. Lieberman J. Cholinergic rebound in neuroleptic withdrawal syndromes. Psychosomatics. 1981;22(3):253-254.
29. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: Safety and tolerability in short-term, placebo-controlled trials. Schizophr Res. 2003;61(2-3):123-136.
30. Kane JM, Fleischhacker WW, Hansen L, et al. Akathisia: an updated review focusing on second-generation antipsychotics. J Clin Psychiatry. 2009;70(5):627-643.
31. Kane JM, Barnes TR, Correll CU, et al. Evaluation of akathisia in patients with schizophrenia, schizoaffective disorder, or bipolar I disorder: A post hoc analysis of pooled data from short- and long-term aripiprazole trials. J Psychopharmacol. 2010;24(7):1019-1029.
32. Fleischhacker WW, McQuade RD, Marcus RN, et al. A double-blind, randomized comparative study of aripiprazole and olanzapine in patients with schizophrenia. Biol Psychiatry. 2009;65(6):510-517.
33. Kane JM, Osuntokun O, Kryzhanovskaya LA, et al. A 28-week, randomized, double-blind study of olanzapine versus aripiprazole in the treatment of schizophrenia. J Clin Psychiatry. 2009;70(4):572-581.
34. Kane JM, Correll CU, Goff DC, et al. A multicenter, randomized, double-blind, placebo-controlled, 16-week study of adjunctive aripiprazole for schizophrenia or schizoaffective disorder inadequately treated with quetiapine or risperidone monotherapy. J Clin Psychiatry. 2009;70(10):1348-1357.
James J. Gugger, PharmD, BCPP
Dr. Gugger is Assistant Clinical Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Courtney L. Tam, PharmD
Dr. Tam is Pharmacy Practice Resident, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Charles R. Ashby, Jr, PhD
Dr. Ashby is Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
James J. Gugger, PharmD, BCPP
Dr. Gugger is Assistant Clinical Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Courtney L. Tam, PharmD
Dr. Tam is Pharmacy Practice Resident, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Charles R. Ashby, Jr, PhD
Dr. Ashby is Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
James J. Gugger, PharmD, BCPP
Dr. Gugger is Assistant Clinical Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Courtney L. Tam, PharmD
Dr. Tam is Pharmacy Practice Resident, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Charles R. Ashby, Jr, PhD
Dr. Ashby is Professor, St. John’s University, College of Pharmacy and Allied Health Professions, Queens, NY
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Discuss this article at www.facebook.com/CurrentPsychiatry
• Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonist.
• Clinical predictors of aripiprazole-associated worsening of psychosis include low baseline level of psychopathology and previous treatment with high-dose antipsychotics.
• Rapid transition from a medication with significant anticholinergic properties to 1 without these properties may result in symptoms of activation, including restlessness, insomnia, and anxiety, which can be mistaken for worsening psychosis.
• Akathisia, a common adverse effect of aripiprazole, may masquerade as treatment-emergent worsening of psychotic symptoms.
Mr. N, age 29, presents to the emergency department at the urging of his family because of poor self-care, bizarre behavior, and disturbed sleep. He first experienced psychiatric symptoms 10 years ago after his mother died. He became dysphoric and paranoid, displaying bizarre responses and behaviors with poor self-care and a gradual functional decline. He has been taking sertraline, 100 mg/d, for 10 years.
Upon arrival at the hospital’s inpatient unit, Mr. N is unkempt, oddly related, and paranoid. His affect is constricted. Mr. N displays thought blocking and possibly is responding to internal stimuli. Sertraline is continued and haloperidol, 1 mg/d, is initiated. For the next 2 weeks, Mr. N continues to be oddly related, irritable, and paranoid, and experiences disturbed sleep and thought blocking. After an episode of impulsive aggression, the treatment team initiates aripiprazole, which is titrated to 30 mg/d for 1 week. Mr. N’s clinical status worsens; he is menacing toward other patients and his thinking is more disorganized, with loose associations and ideas of reference. He requires 4 injections of IM haloperidol, 5 mg, and several visits to the seclusion room over the next week. Haloperidol is increased to 30 mg/d over the next 10 days, then aripiprazole is discontinued because of a putative drug interaction with haloperidol. Following the medication changes Mr. N demonstrates better behavioral control, but still is grossly psychotic. While awaiting transfer to a state hospital, Mr. N receives a trial of olanzapine, 20 to 40 mg/d, for 2 weeks without significant benefit.
Several clinical trials demonstrate a significant reduction in intensity of psychotic symptoms with aripiprazole, which has a unique mechanism of action.1 However, since its FDA approval in 2002, several case reports have described treatment-emergent psychotic symptoms associated with aripiprazole initiation. Over the past 40 years, reports of worsening psychosis associated with antipsychotics have been limited to patients with schizophrenia who were taking high dosages or who had high plasma concentrations, when anticholinergic delirium may have explained increased psychotic symptoms.2-4
How can a drug effectively treat psychotic symptoms and occasionally worsen them? In this article, we discuss the relevant pharmacology and clinical literature on aripiprazole and try to make sense of this apparent paradox.
Unique pharmacologic profile
Antipsychotics have been reported to be either neutral antagonists or inverse agonists at the D2 receptor, based on in vitro data.5 Aripiprazole and its main metabolite, dehydroaripiprazole, originally were described as partial agonists at D2 dopamine receptors.6,7 However, it appears aripiprazole’s pharmacologic action is better explained by the concept of functional selectivity. Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonistic.5
Researchers have hypothesized that the pathophysiology of schizophrenia may, in part, be caused by dysfunction of mesocorticolimbic dopaminergic neurons characterized by an enhanced sensitivity of postsynaptic D2 receptors and increased sensitivity to dopaminergic drugs.8,9 In addition, chronic treatment with a D2 receptor antagonist is associated with increases in postsynaptic dopamine receptor density (ie, an increase in receptor reserve).10,11 Upregulation of D2 receptors may explain several features seen in patients chronically treated with antipsychotics, including tardive dyskinesia12 and rapid psychotic relapse after discontinuing an antipsychotic (supersensitivity psychosis).13 Because chronic antipsychotic treatment leads to high postsynaptic receptor reserve, aripiprazole initiation may produce overactivation of D2 receptors, which might worsen a patient’s condition.14 In vitro data15-18 and clinical observations indicate that aripiprazole has intrinsic efficacy at D2 receptors, as do clinical observations, such as:
- its propensity to reduce serum prolactin19
- a decreased likelihood of producing extrapyramidal side effects despite >80% occupancy of D2 receptors6
- case reports documenting aripiprazole-associated mania,20 improvement of risperidone-associated cognitive impairment,21 and pathologic gambling.22
Emergence or worsening of psychotic symptoms or a marginal antipsychotic effect may occur if aripiprazole is indeed a postsynaptic D2 receptor agonist. An individual patient’s outcome likely would depend on his or her sensitivity to psychosis and concurrent or previous exposure to a D2 receptor antagonist. For example, stimulation of postsynaptic D2 receptors may be further augmented if the dosage of the previous antipsychotic was reduced or withdrawn before initiating aripiprazole because additional receptors would be available for interaction with aripiprazole.
Case reports
A literature review revealed 23 reports of treatment-emergent psychosis associated with aripiprazole initiation (Table). The mean age of the patients was 47 (range: 17 to 69) and 57% were men. Most patients (87%) were diagnosed with a schizophrenia-spectrum illness before aripiprazole initiation. Most (57%) had mild, stable, or no psychotic symptoms before aripiprazole initiation. Most were receiving relatively high doses of antipsychotics (average chlorpromazine equivalents [CPZE]: 648 mg/d) before aripiprazole initiation. This medication was either decreased or discontinued in 70% of patients.
Emergence or worsening of psychotic symptoms included agitation, aggressive behavior, and increased psychomotor activity. However, akathisia evaluation was described in only 2 reports: 1 author identified akathisia symptoms, but attributed them to a concomitant antipsychotic (fluphenazine)23 and the other report specifically excluded the possibility of akathisia.24 Two systematic studies have attempted to establish risk factors for aripiprazole-associated worsening psychosis (Box).14,25
In our literature review, the mean final dose of aripiprazole was 21.5 mg/d (range: 2 to 60 mg/d). In the cases describing subsequent treatment, all but 1 patient were switched to another antipsychotic, including 2 whose psychotic symptoms stabilized with continuation of aripiprazole and addition of a second antipsychotic. Interestingly, in the case reported by Adan-Manes et al,26 initial treatment with aripiprazole monotherapy was efficacious, but a subsequent trial of adjunctive aripiprazole resulted in worsening psychosis.
Table
Case reports: Treatment-emergent psychosis associated with aripiprazole
| Study | Age, sex | Diagnosis | Before aripiprazole initiation | Pre-aripiprazole treatment | Aripiprazole dose | Concomitant psychotropic treatment | Subsequent treatment |
|---|---|---|---|---|---|---|---|
| Chiu et al, 2011a | 39, M | Schizophrenia | Psychiatrically stable, tardive dystonia | Clozapine, 300 mg/d | 10 mg/d | Valproic acid, 1,000 mg/d, clonazepam, 2 mg/d, mephenoxalone, 800 mg/d | Clozapine |
| Ekinci et al, 2010b | 17, M | ADHD | Inattention and impulsive aggression | Tapered and discontinued risperidone, 2.5 mg/d | 5 mg/d | Methylphenidate, 54 mg/d | Risperidone, 2 mg/d, methylphenidate, 36 mg/d |
| Selvaraj et al, 2010c | 49, F | Chronic depression | Depressive symptoms, suicidal ideation | None stated | 2 mg/d | Duloxetine, 80 mg/d, clonazepam, 2 mg/d | Duloxetine, 120 mg/d |
| Adan-Manes et al, 2009d | 23, M | Schizophrenia | No psychotic symptoms | Abrupt decrease of amisulpride dose from 800 mg/d to 400 mg/d | 20 mg/d | Biperiden, 4 mg/d | Amisulpride, 800 mg/d |
| Cho et al, 2009e | 45, F | Schizophrenia | Persistent psychotic symptoms, new onset diabetes with acute ketoacidosis | Haloperidol, 20 mg/d, abrupt clozapine discontinuation | 15 mg/d | Valproic acid, nortriptyline | Molindone, 150 mg/d |
| Ahuja et al, 2007f | 35, F | Schizoaffective disorder | Stable before medication change | Tapered amisulpride, 400 mg/d, over 6 weeks | 15 mg/d | None | Amisulpride, 600 mg/d |
| Lea et al, 2007g | 57, M | Schizophrenia | Persistent psychotic symptoms, treatment resistance, recent recovery from NMS | Discontinued ziprasidone, 200 mg/d | 30 mg/d | Lorazepam, 2 mg/d, amantadine, 100 mg, sertraline, 50 mg/d | Clozapine |
| Lea et al, 2007g | 49, M | Schizoaffective disorder | Delusions, verbal aggression, substance abuse, HCV | Decreased quetiapine dose from 800 mg/d to 400 mg/d | 15 mg/d | Divalproex, 1,000 mg/d, fluvoxamine, 200 mg/d, clonazepam, 2 mg/d | Lithium, quetiapine, 500 mg/d, haloperidol, 2 mg/d |
| Lea et al, 2007g | 60, M | Schizophrenia | Delusions, labile mood, aggression | Risperidone, 3 mg/d, interruption of fluphenazine, 75 mg/d | 20 mg/d | Divalproex, 4,500 mg/d, benztropine, 3 mg/d | Not discussed |
| Raja, 2007h | 30, M | Schizoaffective disorder | Negative symptoms, otherwise stable, recent citalopram discontinuation | Discontinued amisulpride, 800 mg/d over 2 weeks | 30 mg/d | Lithium | Amisulpride, 500 mg/d |
| Raja, 2007h | 69, F | Bipolar disorder | History of multiple relapses; presented with tremor, akathisia, weight gain | Discontinued risperidone, 2 mg/d, over 2 weeks | 15 mg/d | Lithium | Risperidone, 4 mg |
| Raja, 2007h | 59, F | Schizophrenia | Negative symptoms, otherwise stable | Reduced risperidone dosage from 5 mg/d to 4 mg/d | 7.5 mg/d | None | Risperidone, 5 mg/d |
| Thone, 2007i | 31, M | Schizophrenia | Confusion, agitation, delusions worsened with aripiprazole dose increase | None | 60 mg/d | None | Aripiprazole dose reduction to 15 mg/d, olanzapine, 10 mg/d |
| Glick et al, 2006j | 55, F | Schizophrenia | Stable before medication change | Tapered and discontinued thioridazine, 600 mg/d, over 3 months | 30 mg/d | None | Chlorpromazine, 200 mg/d, aripiprazole, 30 mg/d |
| Glick et al, 2006j | 52, M | Schizophrenia | Negative symptoms | Decreased olanzapine dose from 30 mg/d to 20 mg/d | 30 mg/d | None | Olanzapine, 30 mg/d |
| Barnas et al, 2005k | 57, F | Schizoaffective disorder | Stable before medication change | Discontinued perphenazine, 8 mg/d | 30 mg/d | None | Quetiapine, 350 mg/d |
| DeQuardo, 2004l | 54, M | Schizophrenia | History of aggression, residual paranoia, severe EPS | Haloperidol, 200 mg/d | 15 mg/d | Benztropine | Haloperidol |
| DeQuardo, 2004l | 51, M | Schizophrenia | History of aggression, persistent psychotic symptoms, treatment resistance | Olanzapine, 60 mg/d | 10 mg/d | None | Olanzapine |
| Ramaswamy et al, 2004m | 43, F | Schizoaffective disorder | Psychiatrically stable, multiple medication changes, including substituting carbamazepine for valproic acid | Discontinued ziprasidone, 160 mg/d, discontinued quetiapine, 400 mg/d, over 2 weeks | 30 mg/d | Propranolol, 30 mg/d, l-thyroxine, .05 mg/d, carbamazepine, 600 mg/d | Not available |
| Ramaswawamy et al, 2004m | 57, F | Schizoaffective disorder | History of multiple hospitalizations, but stable before medication change | Decreased olanzapine dose from 20 mg/d to 15 mg/d | 30 mg/d | Valproic acid, 2,000 mg/d | Ziprasidone |
| Ramaswawamy et al, 2004m | 67, F | Schizophrenia | Remote hospitalizations, recent worsened psychosis | Decreased ziprasidone dose from 200 mg/d to 160 mg/d 2 months previously | 30 mg/d | Carbamazepine, 200 mg/d | Not discussed |
| Ramaswamy et al, 2004m | 46, M | Schizophrenia | Persistent delusions while receiving risperidone, TD | Risperidone, 3 mg/d | 15 mg/d | Valproic acid, 1,500 mg/d | Risperidone, 3 mg/d |
| Reeves et al, 2004n | 50, M | Schizoaffective disorder | Relatively stable with nonthreatening delusions, hallucinations | Quetiapine, 800 mg/d | 30 mg/d | Divalproex, 2,000 mg/d | Olanzapine, 20 mg/d |
| ADHD: attention-deficit/hyperactivity disorder; EPS: extrapyramidal symptoms; HCV: hepatitis C virus; NMS: neuroleptic malignant syndrome; TD: tardive dyskinesia Source: References a. Chiu YH, Chen CH, Lu ML. Worsening psychosis after adding aripiprazole to clozapine. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):291-292. b. Ekinci O, Sabuncuoglu O. Psychosis associated with switching from risperidone to aripiprazole in an adolescent on methylphenidate treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(2):648-649. c. Selvaraj V, Ramaswamy S, Sharma A, et al. New-onset psychosis and emergence of suicidal ideation with aripiprazole. Am J Psychiatry. 2010;167(12):1535-1536. d. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246. e. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143. f. Ahuja N, Lloyd AJ. Aripiprazole and worsening of psychosis: a case report. J Clin Psychiatry. 2007;68(5):805-806. g. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342. h. Raja M. Improvement or worsening of psychotic symptoms after treatment with low doses of aripiprazole. Int J Neuropsychopharmacol. 2007;10(1):107-110. i. Thone J. Worsened agitation and confusion in schizophrenia subsequent to high-dose aripiprazole. J Neuropsychiatry Clin Neurosci. 2007;19(4):481-482. j. Glick ID, Duggal V, Hodulik C. Aripiprazole as a dopamine partial agonist: positive and negative effects. J Clin Psychopharmacol. 2006;26(1):101-103. k. Barnas ME, Hussain N, Petrides G. Treatment-emergent psychosis with aripiprazole. J Clin Psychiatry. 2005;66(10):1339. l. DeQuardo JR. Worsened agitation with aripiprazole: adverse effect of dopamine partial agonism? J Clin Psychiatry. 2004;65(1):132-133. m. Ramaswamy S, Vijay D, William M, et al. Aripiprazole possibly worsens psychosis. Int Clin Psychopharmacol. 2004;19(1):45-48. n. Reeves RR, Mack JE. Worsening schizoaffective disorder with aripiprazole. Am J Psychiatry. 2004;161(7):1308. | |||||||
Takeuchi et al14 aimed to establish predictors of worsening psychosis in a naturalistic setting where patients slowly transitioned to aripiprazole from previous antipsychotic treatment. Patients were required to be on a stable dose of an antipsychotic before participating in the study. Aripiprazole was started at 12 mg/d for 2 weeks with flexible dosing from weeks 2 to 52. Previous antipsychotic therapy was reduced biweekly by 25%. The incidence of worsening psychopathology after aripiprazole initiation was higher in the group of patients who had previously received high-dose antipsychotic therapy (average chlorpromazine equivalents [CPZE]: 727 mg/d) compared with the group on low dosages (average CPZE: 382 mg/d). It is possible that previous high-dose antipsychotic therapy was indicative of more significant baseline psychopathology; however, the worsened group and stabilized group had similar baseline Clinical Global Impressions-Severity scores.
Pae et al25 aimed to find predictors of worsening psychosis with aripiprazole in patients whose previous antipsychotic therapy was immediately discontinued. They found lower baseline disease severity was associated with significant worsening during the first month of aripiprazole treatment.
Other potential explanations
Aripiprazole’s manufacturer reported the incidence of psychosis-related adverse events in an analysis of 9 randomized schizophrenia trials.27 The rates of psychosis-related adverse events ranged from 0.6% to 18%, but there was no apparent relationship to study design or method of transitioning to aripiprazole. Rates of psychosis-related adverse events were similar between aripiprazole and the control group (placebo in 3 studies, another antipsychotic in 2 studies).
Emergence or worsening of psychotic symptoms temporally associated with aripiprazole initiation does not necessarily imply causation. As in Mr. N’s case, it is not always possible to determine whether worsening psychosis is the natural disease course or a treatment effect. In addition, it is not possible to differentiate lack of efficacy from a true propensity for aripiprazole to worsen psychosis.
It also is conceivable discontinuation or dosage reduction of a previous antipsychotic would worsen psychotic symptoms or cause side effects. When significant changes in psychopathology or side effects develop during the transition from 1 antipsychotic to another, it is difficult to determine etiology. Specifically, rapid transition from a medication with significant anticholinergic and antihistaminic properties—such as quetiapine or olanzapine—to 1 without these properties—such as aripiprazole—may result in symptoms of activation, including restlessness, insomnia, and anxiety. Consequently, these symptoms could be mistaken for worsening psychosis.28 Only 1 patient in this series was reported to abruptly discontinue an antipsychotic with significant anticholinergic properties (clozapine) before initiating aripiprazole.24 Studies by Takeuchi et al14 and Pae et al25 did not report the relative baseline use of antipsychotic medication with anticholinergic properties.
In a pooled analysis of treatment-emergent adverse events in 5 randomized clinical trials of patients receiving aripiprazole for acute relapse of schizophrenia, the incidence of akathisia was 10%, although it is not clear if this is a dose-related adverse effect.29 Because akathisia may be confused for worsening psychosis,30 it is possible akathisia was mistakenly identified as worsening psychotic symptoms in Mr. N’s case, as well as several reports from our literature review.
Covert akathisia is unlikely to explain worsening psychopathology observed in all patients in our literature review because confusion of akathisia and worsening psychosis is not a widespread phenomenon. In a post hoc analysis of pooled safety data from aripiprazole trials, Kane et al31 did not find a correlation between presence of akathisia and aripiprazole efficacy as measured by the Positive and Negative Syndrome Scale (PANSS) total, PANSS positive, PANSS negative, Clinical Global Impressions-Severity, Clinical Global Impressions-Improvement, and percentage of responders. Pae et al25 also noted there was no correlation between scores on the Barnes Akathisia Rating Scale and worsening psychopathology in patients switched to aripiprazole.
An antagonist always is an antagonist and clinicians have appreciated this concept since the days of chlorpromazine. The activity of aripiprazole, however, is on a pharmacologic continuum between a neutral antagonist and full agonist and currently there is no way to precisely determine the level of D2 receptor agonist action in a patient.
Although it is interesting to speculate that aripiprazole’s D2 receptor agonist action may contribute to worsening psychosis,32-34 there are other plausible explanations to consider. Rapid transition from a drug with significant anticholinergic properties and aripiprazole-associated akathisia may contribute to worsening psychopathology in patients starting aripiprazole. Because covert side effects may be incorrectly identified as psychotic agitation, we cannot exclude this as a possible etiologic factor in Mr. N’s case as well as the cases in our literature review.
Related Resource
- Abilify [package insert]. Princeton, NJ: Bristol-Myers Squibb; 2011.
Drug Brand Names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Biperiden • Akineton
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fluphenazine • Permitil, Prolixin
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Nortriptyline • Aventyl, Pamelor
- Methylphenidate • Concerta
- Molindone • Moban
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Mellaril
- Thyroxine • Synthroid
- Valproic acid • Depakene
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
• Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonist.
• Clinical predictors of aripiprazole-associated worsening of psychosis include low baseline level of psychopathology and previous treatment with high-dose antipsychotics.
• Rapid transition from a medication with significant anticholinergic properties to 1 without these properties may result in symptoms of activation, including restlessness, insomnia, and anxiety, which can be mistaken for worsening psychosis.
• Akathisia, a common adverse effect of aripiprazole, may masquerade as treatment-emergent worsening of psychotic symptoms.
Mr. N, age 29, presents to the emergency department at the urging of his family because of poor self-care, bizarre behavior, and disturbed sleep. He first experienced psychiatric symptoms 10 years ago after his mother died. He became dysphoric and paranoid, displaying bizarre responses and behaviors with poor self-care and a gradual functional decline. He has been taking sertraline, 100 mg/d, for 10 years.
Upon arrival at the hospital’s inpatient unit, Mr. N is unkempt, oddly related, and paranoid. His affect is constricted. Mr. N displays thought blocking and possibly is responding to internal stimuli. Sertraline is continued and haloperidol, 1 mg/d, is initiated. For the next 2 weeks, Mr. N continues to be oddly related, irritable, and paranoid, and experiences disturbed sleep and thought blocking. After an episode of impulsive aggression, the treatment team initiates aripiprazole, which is titrated to 30 mg/d for 1 week. Mr. N’s clinical status worsens; he is menacing toward other patients and his thinking is more disorganized, with loose associations and ideas of reference. He requires 4 injections of IM haloperidol, 5 mg, and several visits to the seclusion room over the next week. Haloperidol is increased to 30 mg/d over the next 10 days, then aripiprazole is discontinued because of a putative drug interaction with haloperidol. Following the medication changes Mr. N demonstrates better behavioral control, but still is grossly psychotic. While awaiting transfer to a state hospital, Mr. N receives a trial of olanzapine, 20 to 40 mg/d, for 2 weeks without significant benefit.
Several clinical trials demonstrate a significant reduction in intensity of psychotic symptoms with aripiprazole, which has a unique mechanism of action.1 However, since its FDA approval in 2002, several case reports have described treatment-emergent psychotic symptoms associated with aripiprazole initiation. Over the past 40 years, reports of worsening psychosis associated with antipsychotics have been limited to patients with schizophrenia who were taking high dosages or who had high plasma concentrations, when anticholinergic delirium may have explained increased psychotic symptoms.2-4
How can a drug effectively treat psychotic symptoms and occasionally worsen them? In this article, we discuss the relevant pharmacology and clinical literature on aripiprazole and try to make sense of this apparent paradox.
Unique pharmacologic profile
Antipsychotics have been reported to be either neutral antagonists or inverse agonists at the D2 receptor, based on in vitro data.5 Aripiprazole and its main metabolite, dehydroaripiprazole, originally were described as partial agonists at D2 dopamine receptors.6,7 However, it appears aripiprazole’s pharmacologic action is better explained by the concept of functional selectivity. Aripiprazole may interact preferentially with distinct conformations of the D2 receptor, leading to a spectrum of pharmacologic effects, including acting as a full agonist, partial agonist, or antagonistic.5
Researchers have hypothesized that the pathophysiology of schizophrenia may, in part, be caused by dysfunction of mesocorticolimbic dopaminergic neurons characterized by an enhanced sensitivity of postsynaptic D2 receptors and increased sensitivity to dopaminergic drugs.8,9 In addition, chronic treatment with a D2 receptor antagonist is associated with increases in postsynaptic dopamine receptor density (ie, an increase in receptor reserve).10,11 Upregulation of D2 receptors may explain several features seen in patients chronically treated with antipsychotics, including tardive dyskinesia12 and rapid psychotic relapse after discontinuing an antipsychotic (supersensitivity psychosis).13 Because chronic antipsychotic treatment leads to high postsynaptic receptor reserve, aripiprazole initiation may produce overactivation of D2 receptors, which might worsen a patient’s condition.14 In vitro data15-18 and clinical observations indicate that aripiprazole has intrinsic efficacy at D2 receptors, as do clinical observations, such as:
- its propensity to reduce serum prolactin19
- a decreased likelihood of producing extrapyramidal side effects despite >80% occupancy of D2 receptors6
- case reports documenting aripiprazole-associated mania,20 improvement of risperidone-associated cognitive impairment,21 and pathologic gambling.22
Emergence or worsening of psychotic symptoms or a marginal antipsychotic effect may occur if aripiprazole is indeed a postsynaptic D2 receptor agonist. An individual patient’s outcome likely would depend on his or her sensitivity to psychosis and concurrent or previous exposure to a D2 receptor antagonist. For example, stimulation of postsynaptic D2 receptors may be further augmented if the dosage of the previous antipsychotic was reduced or withdrawn before initiating aripiprazole because additional receptors would be available for interaction with aripiprazole.
Case reports
A literature review revealed 23 reports of treatment-emergent psychosis associated with aripiprazole initiation (Table). The mean age of the patients was 47 (range: 17 to 69) and 57% were men. Most patients (87%) were diagnosed with a schizophrenia-spectrum illness before aripiprazole initiation. Most (57%) had mild, stable, or no psychotic symptoms before aripiprazole initiation. Most were receiving relatively high doses of antipsychotics (average chlorpromazine equivalents [CPZE]: 648 mg/d) before aripiprazole initiation. This medication was either decreased or discontinued in 70% of patients.
Emergence or worsening of psychotic symptoms included agitation, aggressive behavior, and increased psychomotor activity. However, akathisia evaluation was described in only 2 reports: 1 author identified akathisia symptoms, but attributed them to a concomitant antipsychotic (fluphenazine)23 and the other report specifically excluded the possibility of akathisia.24 Two systematic studies have attempted to establish risk factors for aripiprazole-associated worsening psychosis (Box).14,25
In our literature review, the mean final dose of aripiprazole was 21.5 mg/d (range: 2 to 60 mg/d). In the cases describing subsequent treatment, all but 1 patient were switched to another antipsychotic, including 2 whose psychotic symptoms stabilized with continuation of aripiprazole and addition of a second antipsychotic. Interestingly, in the case reported by Adan-Manes et al,26 initial treatment with aripiprazole monotherapy was efficacious, but a subsequent trial of adjunctive aripiprazole resulted in worsening psychosis.
Table
Case reports: Treatment-emergent psychosis associated with aripiprazole
| Study | Age, sex | Diagnosis | Before aripiprazole initiation | Pre-aripiprazole treatment | Aripiprazole dose | Concomitant psychotropic treatment | Subsequent treatment |
|---|---|---|---|---|---|---|---|
| Chiu et al, 2011a | 39, M | Schizophrenia | Psychiatrically stable, tardive dystonia | Clozapine, 300 mg/d | 10 mg/d | Valproic acid, 1,000 mg/d, clonazepam, 2 mg/d, mephenoxalone, 800 mg/d | Clozapine |
| Ekinci et al, 2010b | 17, M | ADHD | Inattention and impulsive aggression | Tapered and discontinued risperidone, 2.5 mg/d | 5 mg/d | Methylphenidate, 54 mg/d | Risperidone, 2 mg/d, methylphenidate, 36 mg/d |
| Selvaraj et al, 2010c | 49, F | Chronic depression | Depressive symptoms, suicidal ideation | None stated | 2 mg/d | Duloxetine, 80 mg/d, clonazepam, 2 mg/d | Duloxetine, 120 mg/d |
| Adan-Manes et al, 2009d | 23, M | Schizophrenia | No psychotic symptoms | Abrupt decrease of amisulpride dose from 800 mg/d to 400 mg/d | 20 mg/d | Biperiden, 4 mg/d | Amisulpride, 800 mg/d |
| Cho et al, 2009e | 45, F | Schizophrenia | Persistent psychotic symptoms, new onset diabetes with acute ketoacidosis | Haloperidol, 20 mg/d, abrupt clozapine discontinuation | 15 mg/d | Valproic acid, nortriptyline | Molindone, 150 mg/d |
| Ahuja et al, 2007f | 35, F | Schizoaffective disorder | Stable before medication change | Tapered amisulpride, 400 mg/d, over 6 weeks | 15 mg/d | None | Amisulpride, 600 mg/d |
| Lea et al, 2007g | 57, M | Schizophrenia | Persistent psychotic symptoms, treatment resistance, recent recovery from NMS | Discontinued ziprasidone, 200 mg/d | 30 mg/d | Lorazepam, 2 mg/d, amantadine, 100 mg, sertraline, 50 mg/d | Clozapine |
| Lea et al, 2007g | 49, M | Schizoaffective disorder | Delusions, verbal aggression, substance abuse, HCV | Decreased quetiapine dose from 800 mg/d to 400 mg/d | 15 mg/d | Divalproex, 1,000 mg/d, fluvoxamine, 200 mg/d, clonazepam, 2 mg/d | Lithium, quetiapine, 500 mg/d, haloperidol, 2 mg/d |
| Lea et al, 2007g | 60, M | Schizophrenia | Delusions, labile mood, aggression | Risperidone, 3 mg/d, interruption of fluphenazine, 75 mg/d | 20 mg/d | Divalproex, 4,500 mg/d, benztropine, 3 mg/d | Not discussed |
| Raja, 2007h | 30, M | Schizoaffective disorder | Negative symptoms, otherwise stable, recent citalopram discontinuation | Discontinued amisulpride, 800 mg/d over 2 weeks | 30 mg/d | Lithium | Amisulpride, 500 mg/d |
| Raja, 2007h | 69, F | Bipolar disorder | History of multiple relapses; presented with tremor, akathisia, weight gain | Discontinued risperidone, 2 mg/d, over 2 weeks | 15 mg/d | Lithium | Risperidone, 4 mg |
| Raja, 2007h | 59, F | Schizophrenia | Negative symptoms, otherwise stable | Reduced risperidone dosage from 5 mg/d to 4 mg/d | 7.5 mg/d | None | Risperidone, 5 mg/d |
| Thone, 2007i | 31, M | Schizophrenia | Confusion, agitation, delusions worsened with aripiprazole dose increase | None | 60 mg/d | None | Aripiprazole dose reduction to 15 mg/d, olanzapine, 10 mg/d |
| Glick et al, 2006j | 55, F | Schizophrenia | Stable before medication change | Tapered and discontinued thioridazine, 600 mg/d, over 3 months | 30 mg/d | None | Chlorpromazine, 200 mg/d, aripiprazole, 30 mg/d |
| Glick et al, 2006j | 52, M | Schizophrenia | Negative symptoms | Decreased olanzapine dose from 30 mg/d to 20 mg/d | 30 mg/d | None | Olanzapine, 30 mg/d |
| Barnas et al, 2005k | 57, F | Schizoaffective disorder | Stable before medication change | Discontinued perphenazine, 8 mg/d | 30 mg/d | None | Quetiapine, 350 mg/d |
| DeQuardo, 2004l | 54, M | Schizophrenia | History of aggression, residual paranoia, severe EPS | Haloperidol, 200 mg/d | 15 mg/d | Benztropine | Haloperidol |
| DeQuardo, 2004l | 51, M | Schizophrenia | History of aggression, persistent psychotic symptoms, treatment resistance | Olanzapine, 60 mg/d | 10 mg/d | None | Olanzapine |
| Ramaswamy et al, 2004m | 43, F | Schizoaffective disorder | Psychiatrically stable, multiple medication changes, including substituting carbamazepine for valproic acid | Discontinued ziprasidone, 160 mg/d, discontinued quetiapine, 400 mg/d, over 2 weeks | 30 mg/d | Propranolol, 30 mg/d, l-thyroxine, .05 mg/d, carbamazepine, 600 mg/d | Not available |
| Ramaswawamy et al, 2004m | 57, F | Schizoaffective disorder | History of multiple hospitalizations, but stable before medication change | Decreased olanzapine dose from 20 mg/d to 15 mg/d | 30 mg/d | Valproic acid, 2,000 mg/d | Ziprasidone |
| Ramaswawamy et al, 2004m | 67, F | Schizophrenia | Remote hospitalizations, recent worsened psychosis | Decreased ziprasidone dose from 200 mg/d to 160 mg/d 2 months previously | 30 mg/d | Carbamazepine, 200 mg/d | Not discussed |
| Ramaswamy et al, 2004m | 46, M | Schizophrenia | Persistent delusions while receiving risperidone, TD | Risperidone, 3 mg/d | 15 mg/d | Valproic acid, 1,500 mg/d | Risperidone, 3 mg/d |
| Reeves et al, 2004n | 50, M | Schizoaffective disorder | Relatively stable with nonthreatening delusions, hallucinations | Quetiapine, 800 mg/d | 30 mg/d | Divalproex, 2,000 mg/d | Olanzapine, 20 mg/d |
| ADHD: attention-deficit/hyperactivity disorder; EPS: extrapyramidal symptoms; HCV: hepatitis C virus; NMS: neuroleptic malignant syndrome; TD: tardive dyskinesia Source: References a. Chiu YH, Chen CH, Lu ML. Worsening psychosis after adding aripiprazole to clozapine. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):291-292. b. Ekinci O, Sabuncuoglu O. Psychosis associated with switching from risperidone to aripiprazole in an adolescent on methylphenidate treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(2):648-649. c. Selvaraj V, Ramaswamy S, Sharma A, et al. New-onset psychosis and emergence of suicidal ideation with aripiprazole. Am J Psychiatry. 2010;167(12):1535-1536. d. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246. e. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143. f. Ahuja N, Lloyd AJ. Aripiprazole and worsening of psychosis: a case report. J Clin Psychiatry. 2007;68(5):805-806. g. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342. h. Raja M. Improvement or worsening of psychotic symptoms after treatment with low doses of aripiprazole. Int J Neuropsychopharmacol. 2007;10(1):107-110. i. Thone J. Worsened agitation and confusion in schizophrenia subsequent to high-dose aripiprazole. J Neuropsychiatry Clin Neurosci. 2007;19(4):481-482. j. Glick ID, Duggal V, Hodulik C. Aripiprazole as a dopamine partial agonist: positive and negative effects. J Clin Psychopharmacol. 2006;26(1):101-103. k. Barnas ME, Hussain N, Petrides G. Treatment-emergent psychosis with aripiprazole. J Clin Psychiatry. 2005;66(10):1339. l. DeQuardo JR. Worsened agitation with aripiprazole: adverse effect of dopamine partial agonism? J Clin Psychiatry. 2004;65(1):132-133. m. Ramaswamy S, Vijay D, William M, et al. Aripiprazole possibly worsens psychosis. Int Clin Psychopharmacol. 2004;19(1):45-48. n. Reeves RR, Mack JE. Worsening schizoaffective disorder with aripiprazole. Am J Psychiatry. 2004;161(7):1308. | |||||||
Takeuchi et al14 aimed to establish predictors of worsening psychosis in a naturalistic setting where patients slowly transitioned to aripiprazole from previous antipsychotic treatment. Patients were required to be on a stable dose of an antipsychotic before participating in the study. Aripiprazole was started at 12 mg/d for 2 weeks with flexible dosing from weeks 2 to 52. Previous antipsychotic therapy was reduced biweekly by 25%. The incidence of worsening psychopathology after aripiprazole initiation was higher in the group of patients who had previously received high-dose antipsychotic therapy (average chlorpromazine equivalents [CPZE]: 727 mg/d) compared with the group on low dosages (average CPZE: 382 mg/d). It is possible that previous high-dose antipsychotic therapy was indicative of more significant baseline psychopathology; however, the worsened group and stabilized group had similar baseline Clinical Global Impressions-Severity scores.
Pae et al25 aimed to find predictors of worsening psychosis with aripiprazole in patients whose previous antipsychotic therapy was immediately discontinued. They found lower baseline disease severity was associated with significant worsening during the first month of aripiprazole treatment.
Other potential explanations
Aripiprazole’s manufacturer reported the incidence of psychosis-related adverse events in an analysis of 9 randomized schizophrenia trials.27 The rates of psychosis-related adverse events ranged from 0.6% to 18%, but there was no apparent relationship to study design or method of transitioning to aripiprazole. Rates of psychosis-related adverse events were similar between aripiprazole and the control group (placebo in 3 studies, another antipsychotic in 2 studies).
Emergence or worsening of psychotic symptoms temporally associated with aripiprazole initiation does not necessarily imply causation. As in Mr. N’s case, it is not always possible to determine whether worsening psychosis is the natural disease course or a treatment effect. In addition, it is not possible to differentiate lack of efficacy from a true propensity for aripiprazole to worsen psychosis.
It also is conceivable discontinuation or dosage reduction of a previous antipsychotic would worsen psychotic symptoms or cause side effects. When significant changes in psychopathology or side effects develop during the transition from 1 antipsychotic to another, it is difficult to determine etiology. Specifically, rapid transition from a medication with significant anticholinergic and antihistaminic properties—such as quetiapine or olanzapine—to 1 without these properties—such as aripiprazole—may result in symptoms of activation, including restlessness, insomnia, and anxiety. Consequently, these symptoms could be mistaken for worsening psychosis.28 Only 1 patient in this series was reported to abruptly discontinue an antipsychotic with significant anticholinergic properties (clozapine) before initiating aripiprazole.24 Studies by Takeuchi et al14 and Pae et al25 did not report the relative baseline use of antipsychotic medication with anticholinergic properties.
In a pooled analysis of treatment-emergent adverse events in 5 randomized clinical trials of patients receiving aripiprazole for acute relapse of schizophrenia, the incidence of akathisia was 10%, although it is not clear if this is a dose-related adverse effect.29 Because akathisia may be confused for worsening psychosis,30 it is possible akathisia was mistakenly identified as worsening psychotic symptoms in Mr. N’s case, as well as several reports from our literature review.
Covert akathisia is unlikely to explain worsening psychopathology observed in all patients in our literature review because confusion of akathisia and worsening psychosis is not a widespread phenomenon. In a post hoc analysis of pooled safety data from aripiprazole trials, Kane et al31 did not find a correlation between presence of akathisia and aripiprazole efficacy as measured by the Positive and Negative Syndrome Scale (PANSS) total, PANSS positive, PANSS negative, Clinical Global Impressions-Severity, Clinical Global Impressions-Improvement, and percentage of responders. Pae et al25 also noted there was no correlation between scores on the Barnes Akathisia Rating Scale and worsening psychopathology in patients switched to aripiprazole.
An antagonist always is an antagonist and clinicians have appreciated this concept since the days of chlorpromazine. The activity of aripiprazole, however, is on a pharmacologic continuum between a neutral antagonist and full agonist and currently there is no way to precisely determine the level of D2 receptor agonist action in a patient.
Although it is interesting to speculate that aripiprazole’s D2 receptor agonist action may contribute to worsening psychosis,32-34 there are other plausible explanations to consider. Rapid transition from a drug with significant anticholinergic properties and aripiprazole-associated akathisia may contribute to worsening psychopathology in patients starting aripiprazole. Because covert side effects may be incorrectly identified as psychotic agitation, we cannot exclude this as a possible etiologic factor in Mr. N’s case as well as the cases in our literature review.
Related Resource
- Abilify [package insert]. Princeton, NJ: Bristol-Myers Squibb; 2011.
Drug Brand Names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Biperiden • Akineton
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fluphenazine • Permitil, Prolixin
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Nortriptyline • Aventyl, Pamelor
- Methylphenidate • Concerta
- Molindone • Moban
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Mellaril
- Thyroxine • Synthroid
- Valproic acid • Depakene
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Citrome L. A review of aripiprazole in the treatment of patients with schizophrenia or bipolar I disorder. Neuropsychiatr Dis Treat. 2006;2(4):427-443.
2. Chong SA, Tan CH, Lee HS. Worsening of psychosis with clozapine and selective serotonin reuptake inhibitor combination: two case reports. J Clin Psychopharmacol. 1997;17(1):68-69.
3. Bowers MB Jr, Swigar ME. Psychotic patients who become worse on neuroleptics. J Clin Psychopharmacol. 1988;8(6):417-421.
4. Tornatore FL, Lee D, Sramek JJ. Psychotic exacerbation with haloperidol. Drug Intell Clin Pharm. 1981;15(3):209-213.
5. Beaulieu JM, Gainetdinov RR. The physiology signaling, and pharmacology of dopamine receptors. Pharmacol Rev. 2011;63(1):182-217.
6. Grunder G, Carlsson A, Wong DF. Mechanism of new antipsychotic medications: occupancy is not just antagonism. Arch Gen Psychiatry. 2003;60(10):974-977.
7. Wood MD, Scott C, Clarke K, et al. Aripiprazole and its human metabolite are partial agonists at the human dopamine D2 receptor, but the rodent metabolite displays antagonist properties. Eur J Pharmacol. 2006;546(1-3):88-94.
8. Seeman P, Weinshenker D, Quirion R, et al. Dopamine supersensitivity correlates with D2High states, implying many paths to psychosis. Proc Natl Acad Sci U S A. 2005;102(9):3513-3518.
9. Seeman P, Ko F, Jack E, et al. Consistent with dopamine supersensitivity, RGS9 expression is diminished in the amphetamine-treated animal model of schizophrenia and in postmortem schizophrenia brain. Synapse. 2007;61(5):303-309.
10. Burt DR, Creese I, Snyder SH. Antischizophrenic drugs: chronic treatment elevates dopamine receptor binding in brain. Science. 1977;196(4287):326-328.
11. Silvestri S, Seeman MV, Negrete JC, et al. Increased dopamine D2 receptor binding after long-term treatment with antipsychotics in humans: a clinical PET study. Psychopharmacology (Berl). 2000;152(2):174-180.
12. Sayers AC, Bürki HR, Ruch W, et al. Neuroleptic-induced hypersensitivity of striatal dopamine receptors in the rat as a model of tardive dyskinesias. Effects of clozapine, haloperidol, loxapine and chlorpromazine. Psychopharmacologia. 1975;41(2):97-104.
13. Moncrieff J. Does antipsychotic withdrawal provoke psychosis? Review of the literature on rapid onset psychosis (supersensitivity psychosis) and withdrawal-related relapse. Acta Psychiatr Scand. 2006;114(1):3-13.
14. Takeuchi H, Uchida H, Suzuki T, et al. Predictors of clinical worsening after a switch to aripiprazole in patients with schizophrenia: a 1-year naturalistic follow-up study. J Clin Psychopharmacol. 2009;29(4):394-395.
15. Shapiro DA, Renock S, Arrington E, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology. 2003;28(8):1400-1411.
16. Urban JD, Vargas GA, von Zastrow M, et al. Aripiprazole has functionally selective actions at dopamine D2 receptor-mediated signaling pathways. Neuropsychopharmacology. 2007;32(1):67-77.
17. Klewe IV, Nielsen SM, Tarpo L, et al. Recruitment of beta-arrestin2 to the dopamine D2 receptor: Insights into anti-psychotic and anti-parkinsonian drug receptor signaling. Neuropharmacology. 2008;54(8):1215-1222.
18. Masri B, Salahpour A, Didriksen M, et al. Antagonism of dopamine D2 receptor/beta-arrestin 2 interaction is a common property of clinically effective antipsychotics. Proc Natl Acad Sci U S A. 2008;105(36):13656-13661.
19. Shim JC, Shin JG, Kelly DL, et al. Adjunctive treatment with a dopamine partial agonist, aripiprazole, for antipsychotic-induced hyperprolactinemia: a placebo-controlled trial. Am J Psychiatry. 2007;164(9):1404-1410.
20. Padala PR, Wengel SP, Petty F. Manic episode during treatment with aripiprazole. Am J Psychiatry. 2007;164(1):172-173.
21. Hu CH, Pai N, Huang XF, et al. Potential control of risperidone-related cognitive deficits by adjunctive aripiprazole treatment. J Clin Psychopharmacol. 2011;31(1):135-136;author reply 136–137.
22. Cohen J, Magalon D, Boyer L, et al. Aripiprazole-induced pathological gambling: a report of 3 cases. Curr Drug Saf. 2011;6(1):51-53.
23. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342.
24. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143.
25. Pae CU, Chiesa A, Mandelli L, et al. Predictors of early worsening after switch to aripiprazole: a randomized, controlled, open-label study. Clin Drug Investig. 2010;30(3):187-193.
26. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246.
27. Cognata-Smith C, Baker RA, Pikalov A, et al. Analysis of nine aripiprazole trials to evaluate strategies for switching patients with schizophrenia to aripiprazole. Paper presented at: 162nd Annual Meeting American Psychiatric Association; May 16-21, 2009; San Francisco, CA.
28. Lieberman J. Cholinergic rebound in neuroleptic withdrawal syndromes. Psychosomatics. 1981;22(3):253-254.
29. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: Safety and tolerability in short-term, placebo-controlled trials. Schizophr Res. 2003;61(2-3):123-136.
30. Kane JM, Fleischhacker WW, Hansen L, et al. Akathisia: an updated review focusing on second-generation antipsychotics. J Clin Psychiatry. 2009;70(5):627-643.
31. Kane JM, Barnes TR, Correll CU, et al. Evaluation of akathisia in patients with schizophrenia, schizoaffective disorder, or bipolar I disorder: A post hoc analysis of pooled data from short- and long-term aripiprazole trials. J Psychopharmacol. 2010;24(7):1019-1029.
32. Fleischhacker WW, McQuade RD, Marcus RN, et al. A double-blind, randomized comparative study of aripiprazole and olanzapine in patients with schizophrenia. Biol Psychiatry. 2009;65(6):510-517.
33. Kane JM, Osuntokun O, Kryzhanovskaya LA, et al. A 28-week, randomized, double-blind study of olanzapine versus aripiprazole in the treatment of schizophrenia. J Clin Psychiatry. 2009;70(4):572-581.
34. Kane JM, Correll CU, Goff DC, et al. A multicenter, randomized, double-blind, placebo-controlled, 16-week study of adjunctive aripiprazole for schizophrenia or schizoaffective disorder inadequately treated with quetiapine or risperidone monotherapy. J Clin Psychiatry. 2009;70(10):1348-1357.
1. Citrome L. A review of aripiprazole in the treatment of patients with schizophrenia or bipolar I disorder. Neuropsychiatr Dis Treat. 2006;2(4):427-443.
2. Chong SA, Tan CH, Lee HS. Worsening of psychosis with clozapine and selective serotonin reuptake inhibitor combination: two case reports. J Clin Psychopharmacol. 1997;17(1):68-69.
3. Bowers MB Jr, Swigar ME. Psychotic patients who become worse on neuroleptics. J Clin Psychopharmacol. 1988;8(6):417-421.
4. Tornatore FL, Lee D, Sramek JJ. Psychotic exacerbation with haloperidol. Drug Intell Clin Pharm. 1981;15(3):209-213.
5. Beaulieu JM, Gainetdinov RR. The physiology signaling, and pharmacology of dopamine receptors. Pharmacol Rev. 2011;63(1):182-217.
6. Grunder G, Carlsson A, Wong DF. Mechanism of new antipsychotic medications: occupancy is not just antagonism. Arch Gen Psychiatry. 2003;60(10):974-977.
7. Wood MD, Scott C, Clarke K, et al. Aripiprazole and its human metabolite are partial agonists at the human dopamine D2 receptor, but the rodent metabolite displays antagonist properties. Eur J Pharmacol. 2006;546(1-3):88-94.
8. Seeman P, Weinshenker D, Quirion R, et al. Dopamine supersensitivity correlates with D2High states, implying many paths to psychosis. Proc Natl Acad Sci U S A. 2005;102(9):3513-3518.
9. Seeman P, Ko F, Jack E, et al. Consistent with dopamine supersensitivity, RGS9 expression is diminished in the amphetamine-treated animal model of schizophrenia and in postmortem schizophrenia brain. Synapse. 2007;61(5):303-309.
10. Burt DR, Creese I, Snyder SH. Antischizophrenic drugs: chronic treatment elevates dopamine receptor binding in brain. Science. 1977;196(4287):326-328.
11. Silvestri S, Seeman MV, Negrete JC, et al. Increased dopamine D2 receptor binding after long-term treatment with antipsychotics in humans: a clinical PET study. Psychopharmacology (Berl). 2000;152(2):174-180.
12. Sayers AC, Bürki HR, Ruch W, et al. Neuroleptic-induced hypersensitivity of striatal dopamine receptors in the rat as a model of tardive dyskinesias. Effects of clozapine, haloperidol, loxapine and chlorpromazine. Psychopharmacologia. 1975;41(2):97-104.
13. Moncrieff J. Does antipsychotic withdrawal provoke psychosis? Review of the literature on rapid onset psychosis (supersensitivity psychosis) and withdrawal-related relapse. Acta Psychiatr Scand. 2006;114(1):3-13.
14. Takeuchi H, Uchida H, Suzuki T, et al. Predictors of clinical worsening after a switch to aripiprazole in patients with schizophrenia: a 1-year naturalistic follow-up study. J Clin Psychopharmacol. 2009;29(4):394-395.
15. Shapiro DA, Renock S, Arrington E, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology. 2003;28(8):1400-1411.
16. Urban JD, Vargas GA, von Zastrow M, et al. Aripiprazole has functionally selective actions at dopamine D2 receptor-mediated signaling pathways. Neuropsychopharmacology. 2007;32(1):67-77.
17. Klewe IV, Nielsen SM, Tarpo L, et al. Recruitment of beta-arrestin2 to the dopamine D2 receptor: Insights into anti-psychotic and anti-parkinsonian drug receptor signaling. Neuropharmacology. 2008;54(8):1215-1222.
18. Masri B, Salahpour A, Didriksen M, et al. Antagonism of dopamine D2 receptor/beta-arrestin 2 interaction is a common property of clinically effective antipsychotics. Proc Natl Acad Sci U S A. 2008;105(36):13656-13661.
19. Shim JC, Shin JG, Kelly DL, et al. Adjunctive treatment with a dopamine partial agonist, aripiprazole, for antipsychotic-induced hyperprolactinemia: a placebo-controlled trial. Am J Psychiatry. 2007;164(9):1404-1410.
20. Padala PR, Wengel SP, Petty F. Manic episode during treatment with aripiprazole. Am J Psychiatry. 2007;164(1):172-173.
21. Hu CH, Pai N, Huang XF, et al. Potential control of risperidone-related cognitive deficits by adjunctive aripiprazole treatment. J Clin Psychopharmacol. 2011;31(1):135-136;author reply 136–137.
22. Cohen J, Magalon D, Boyer L, et al. Aripiprazole-induced pathological gambling: a report of 3 cases. Curr Drug Saf. 2011;6(1):51-53.
23. Lea JW, Stoner SC, Lafollette J. Agitation associated with aripiprazole initiation. Pharmacotherapy. 2007;27(9):1339-1342.
24. Cho DY, Lindenmayer JP. Aripiprazole-induced agitation after clozapine discontinuation: a case report. J Clin Psychiatry. 2009;70(1):141-143.
25. Pae CU, Chiesa A, Mandelli L, et al. Predictors of early worsening after switch to aripiprazole: a randomized, controlled, open-label study. Clin Drug Investig. 2010;30(3):187-193.
26. Adan-Manes J, Garcia-Parajua P. Aripiprazole in combination with other antipsychotic drugs may worsen psychosis. J Clin Pharm Ther. 2009;34(2):245-246.
27. Cognata-Smith C, Baker RA, Pikalov A, et al. Analysis of nine aripiprazole trials to evaluate strategies for switching patients with schizophrenia to aripiprazole. Paper presented at: 162nd Annual Meeting American Psychiatric Association; May 16-21, 2009; San Francisco, CA.
28. Lieberman J. Cholinergic rebound in neuroleptic withdrawal syndromes. Psychosomatics. 1981;22(3):253-254.
29. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: Safety and tolerability in short-term, placebo-controlled trials. Schizophr Res. 2003;61(2-3):123-136.
30. Kane JM, Fleischhacker WW, Hansen L, et al. Akathisia: an updated review focusing on second-generation antipsychotics. J Clin Psychiatry. 2009;70(5):627-643.
31. Kane JM, Barnes TR, Correll CU, et al. Evaluation of akathisia in patients with schizophrenia, schizoaffective disorder, or bipolar I disorder: A post hoc analysis of pooled data from short- and long-term aripiprazole trials. J Psychopharmacol. 2010;24(7):1019-1029.
32. Fleischhacker WW, McQuade RD, Marcus RN, et al. A double-blind, randomized comparative study of aripiprazole and olanzapine in patients with schizophrenia. Biol Psychiatry. 2009;65(6):510-517.
33. Kane JM, Osuntokun O, Kryzhanovskaya LA, et al. A 28-week, randomized, double-blind study of olanzapine versus aripiprazole in the treatment of schizophrenia. J Clin Psychiatry. 2009;70(4):572-581.
34. Kane JM, Correll CU, Goff DC, et al. A multicenter, randomized, double-blind, placebo-controlled, 16-week study of adjunctive aripiprazole for schizophrenia or schizoaffective disorder inadequately treated with quetiapine or risperidone monotherapy. J Clin Psychiatry. 2009;70(10):1348-1357.
Opiates and psychotropics: Pharmacokinetics for practitioners
• When choosing pharmacologic therapy, make sure that all medications your patient takes are documented, consider drug-drug interactions, and instruct the patient to notify you of any new medications.
• In addition to toxicity, loss of efficacy of some opiate drugs may occur as a result of metabolic inhibition or induction by psychotropic medications.
• Collaborate with the physician who is prescribing the opioid if psychotropic choices are limited. The patient’s pain may be treated adequately with another analgesic that does not interact with the psychotropic that has been chosen.
As prescribed by his internist, Mr. G, age 44, takes 10 mg of methadone every 4 hours for chronic back pain secondary to a work-related injury 3 years ago. He experiences minimal sedation. Mr. G presents for psychiatric evaluation with complaints of increasing irritability, poor focus, low energy, and lack of interest in usual activities. The psychiatrist diagnoses him with depressive disorder not otherwise specified, and prescribes fluoxetine, 20 mg/d. Three weeks later, Mr. G’s wife contacts the psychiatrist reporting that her husband seems “overmedicated” and describes excess drowsiness and slowed thought processing.
After discussion with Mr. G’s internist and pharmacist, the psychiatrist decides that this oversedation may represent a drug-drug interaction between methadone and fluoxetine resulting in higher-than-expected methadone serum levels. Mr. G is instructed to stop fluoxetine with no taper, and his methadone dose is lowered with good results. Over the next 2 weeks Mr. G is titrated back to his original methadone dose and is re-evaluated by the psychiatrist to discuss medication options to address his depression.
Psychiatrists commonly encounter patients who receive opiate medications for chronic pain. Being aware of potential drug-drug interactions between opiate medications and psychotropics can help avoid adverse effects and combinations that may affect the efficacy of either drug. Pharmacokinetic interactions may affect your choice of psychiatric medication and should be taken into account when addressing adverse effects in any patient who takes opiates and psychotropics.
Metabolic pathways
The primary metabolic pathways for opiate metabolism are the cytochrome P450 (CYP) 2D6 and 3A4 isoenzymes. Depending on the agent used, prescribers may need to consider interactions for both pathways (Table 11,2 and Table 21). For example, oxycodone is metabolized via 2D6 and 3A4 isoenzymes and is a potent analgesic with oxymorphone and noroxycodone as its active metabolites. These metabolites, however, make a negligible contribution to oxycodone’s analgesic effect.3,4 Metabolism by the 3A4 isoenzyme is the principal oxidative pathway and the 2D6 site accounts for approximately 10% of oxycodone metabolism. A randomized, placebo-controlled, crossover study showed that 2D6 inhibition by paroxetine had no significant effect on oxycodone levels; however, a combination of paroxetine and itraconazole, a potent 3A4 inhibitor, resulted in substantial increases in oxycodone plasma levels.5 Remain vigilant for possible opiate toxicity when administering oxycodone with 3A4 inhibitors.
Methadone and meperidine also involve dual pathways. Methadone is metabolized primarily by 3A4 and 2B6, with 2D6 playing a smaller role.6 CYP2D6 seems to play an important part in metabolizing the R-enantiomer of methadone, which is largely responsible for the drug’s opiate effects, such as analgesia and respiratory depression.7,8 Induction of the 3A4 isoenzyme may result in methadone withdrawal, and inhibition may cause methadone toxicity.9 Inducers of 3A4, such as carbamazepine, and inhibitors, such as fluoxetine and fluvoxamine, should be avoided or used very cautiously in patients taking methadone. The 2B6 and 2D6 isoenzymes also may increase or decrease methadone levels and should be treated similarly. In Mr. G’s case, fluoxetine inhibited all 3 isoenzymes that are primarily responsible for methadone metabolism. A better antidepressant choice for Mr. G may have been venlafaxine, which is known to only mildly inhibit 2D6, or mirtazapine, which does not seem to inhibit the major CYP isoforms to an appreciable degree.10
Although the full scope of meperidine metabolism has not been identified,9 an in vitro test demonstrated that 2B6 and 3A4 play important roles in metabolizing meperidine to normeperidine, its major metabolite.11 Normeperidine does not provide analgesia and is associated with neurotoxicity, including anxiety, tremor, muscle twitching, and seizure.12 Agents that induce 3A4—such as carbamazepine or St. John’s wort—may contribute to neurotoxicity.9 Inhibition of these isoenzymes may increase meperidine levels and lead to anticholinergic toxicity or respiratory and central nervous system depression.13,14
Opiates metabolized by the 2D6 isoenzyme include codeine, hydrocodone, and tramadol. The analgesic effect of codeine seems dependent on 2D6 metabolism. Via this pathway, codeine is converted into morphine, which has a 300-times stronger affinity for the μ opioid receptor compared with codeine. 2D6 poor metabolizers have shown codeine intolerance and toxicity.3 Psychotropics known to strongly inhibit 2D6 isoenzyme processes—such as paroxetine, fluoxetine, and bupropion—should be avoided in patients taking codeine to prevent adverse effects and potential loss of efficacy. Better antidepressant choices include citalopram or venlafaxine, which inhibit 2D6 to a lesser degree.
Hydrocodone may be a viable option for patients taking 2D6 inhibitors. Hydrocodone is metabolized by 2D6 into hydromorphone, which is 7 to 33 times more potent than hydrocodone.15 Unlike codeine, 2D6 inhibition may have little effect on hydrocodone’s analgesic properties. Animal studies have shown that inhibition of the CYP analog to 2D6 does not affect analgesic response. In humans, 2D6 inhibition does not seem to affect hydrocodone’s abuse liability.16 Two case reports describe known 2D6 poor metabolizers who showed at least a partial response to hydrocodone.15,16
Tramadol’s analgesic properties may be related to serotonin and norepinephrine reuptake inhibition. It is less potent than codeine but is metabolized via the 2D6 isoenzyme into 0-desmethyltramadol, which is up to 200 times stronger than its parent compound.17 Clinicians should be aware that tramadol’s efficacy may be decreased when coadministered with 2D6 inhibitors. In a randomized, placebo-controlled trial, paroxetine, a potent 2D6 inhibitor, was shown to lessen the analgesic effect of tramadol.18
The 3A4 site is the primary pathway for fentanyl metabolism. Agents that inhibit 3A4 could increase fentanyl plasma concentration, leading to respiratory depression.19 Examples of 3A4 inhibitors include fluoxetine and fluvoxamine.
Psychotropics may inhibit or induce P450 isoenzymes to varying degrees. For example, paroxetine and citalopram are known to inhibit 2D6 but paroxetine is a stronger inhibitor; therefore, a significant drug-drug interaction is more likely with paroxetine and a 2D6 substrate than the same substrate administered with citalopram.
Table 1
Cytochrome P450 isoenzymes inhibited and induced by psychotropics
| Isoenzyme | Potency | Psychotropic(s) |
|---|---|---|
| 2B6 inducer | Moderate | Carbamazepine |
| 2B6 inhibitors | Mild to moderate | Fluoxetine, fluvoxamine |
| Moderate | Sertraline | |
| Potent | Paroxetine | |
| 2D6 inhibitors | Mild | Venlafaxine |
| Mild to moderate | Citalopram, escitalopram, fluvoxamine, risperidone | |
| Moderate | Duloxetine | |
| Moderate to potent | Bupropion | |
| Potent | Fluoxetine, haloperidol, paroxetine | |
| Dose-dependent | Sertraline | |
| 3A4 inducer | Potent | Carbamazepine |
| 3A4 inhibitors | Mild | Sertraline |
| Mild to moderate | Fluoxetine, fluvoxamine | |
| Source: References 1,2 | ||
Table 2
Cytochrome P450 isoenzymes inhibiting and inducing opiate metabolism
| Isoenzyme | Opiates |
|---|---|
| 2B6 inducer | Methadone |
| 2B6 inhibitors | Meperidine, methadone |
| 2D6 inhibitors | Codeine (may involve loss of efficacy as well as toxicity), methadone, tramadol (may involve loss of efficacy) |
| 3A4 inducer | Meperidine, methadone |
| 3A4 inhibitors | Fentanyl, oxycodone, meperidine, methadone |
| Source: Reference 1 | |
Other considerations
In addition to pharmacokinetic interactions, it is important to consider synergistic effects of some opiates and psychotropics. Examples include:
- additive effect on respiratory depression by benzodiazepines and opiates
- increased risk of serotonin syndrome and seizure when using tramadol with selective serotonin reuptake inhibitors or tricyclic antidepressants
- additive prolongation of the QTc interval by methadone when used with psychotropics known to prolong the QTc, such as ziprasidone.9,17,20
Careful attention to these interactions and collaboration among providers can ensure the best outcome for our patients. In Mr. G’s case, collaboration with his internist would be in order, particularly if antidepressant choices are limited. In consultation with the psychiatrist, the internist might choose another opiate to treat Mr. G’s pain that would not interact with fluoxetine. If Mr. G and his physician have struggled to manage his pain and if he is stable on the current regimen, selecting a different antidepressant may be warranted.
Related Resources
- Indiana University School of Medicine drug interactions: cytochrome P450 drug interaction table. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
- Ferrando SJ, Levenson JL, Owen JA, eds. Clinical manual of psychopharmacology in the medically ill. Arlington, VA: American Psychiatric Publishing, Inc; 2010.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fentanyl • Duragesic, Actiq
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Hydrocodone • Lortab, Vicodin, others
- Itraconazole • Sporanox
- Meperidine • Demerol
- Methadone • Dolophine, Methadose
- Mirtazapine • Remeron
- Morphine • Avinza, Duramorph, others
- Oxycodone • OxyContin, Roxicodone
- Paroxetine • Paxil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sandson NB, Armstrong SC, Cozza KL. An overview of psychotropic drug-drug interactions. Psychosomatics. 2005;46:464-494.
2. Faucette SR, Wang H, Hamilton GA. Regulation of CYP2B6 in primary human hepatocytes by prototypical inducers. Drug Metab Dispos. 2004;32(3):348-358.
3. Smith HS. Opioid metabolism. Mayo Clin Proc. 2009;84:613-624.
4. Armstrong SC, Cozza KL. Pharmacokinetic drug interactions of morphine codeine, and their derivatives: theory and clinical reality, part II. Psychosomatics. 2003;44:515-520.
5. Grönlund J, Saari TI, Hagelberg NM, et al. Exposure to oral oxycodone is increased by concomitant inhibition of CYP2D6 and 3A4 pathways, but not by inhibition of CYP2D6 alone. Br J Clin Pharmacol. 2010;70:78-87.
6. Leavitt SB. Methadone-drug* interactions. (*medications illicit drugs, and other substances). 3rd ed. Mundelein, IL: Addiction Treatment Forum; 2005.
7. Pérez de los Cobos J, Siñol N, Trujols J, et al. Association of CYP2D6 ultrarapid metabolizer genotype with deficient patient satisfaction regarding methadone maintenance treatment. Drug Alcohol Depend. 2007;89:190-194.
8. Kristensen K, Christensen CB, Christrup LL. The mu1 mu2, delta, kappa opioid receptor binding profiles of methadone stereoisomers and morphine. Life Sci. 1995;56:PL45-50.
9. Armstrong SC, Wynn GH, Sandson NB. Pharmacokinetic drug interactions of synthetic opiate analgesics. Psychosomatics. 2009;50:169-176.
10. Spina E, Santoro V, D’Arrigo C. Clinically relevant pharmacokinetic drug interactions with second-generation antidepressants: an update. Clin Ther. 2008;30:1206-1227.
11. Ramírez J, Innocenti F, Schuetz EG, et al. CYP2B6, CYP3A4, and CYP2C19 are responsible for the in vitro N-demethylation of meperidine in human liver microsomes. Drug Metab Dispos. 2004;32:930-936.
12. Kaiko RF, Foley KM, Grabinski PY, et al. Central nervous system excitatory effects of meperidine in cancer patients. Ann Neurol. 1983;13:180-185.
13. Chalverus C. Clinically important meperidine toxicities. Journal of Pharmaceutical Care in Pain and Symptom Control. 2001;9:37-55.
14. Beckwith MC, Fox ER, Chandramouli J. Removing meperidine from the health-system formulary—frequently asked questions. J Pain Palliat Care Pharmacother. 2002;16:45-59.
15. Foster A, Mobley E, Wang Z. Complicated pain management in a CYP450 2D6 poor metabolizer. Pain Pract. 2007;7:352-356.
16. Susce MT, Murray-Carmichael E, de Leon J. Response to hydrocodone codeine and oxycodone in a CYP2D6 poor metabolizer. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30:1356-1358.
17. Sansone RA, Sansone LA. Tramadol: seizures serotonin syndrome, and coadministered antidepressants. Psychiatry (Edgmont). 2009;6:17-21.
18. Laugesen S, Enggaard TP, Pedersen RS, et al. Paroxetine, a cytochrome P450 2D6 inhibitor, diminishes the stereoselective O-demethylation and reduces the hypoalgesic effect of tramadol. Clin Pharmacol Ther. 2005;77:312-323.
19. Duragesic [package insert]. Raritan NJ: Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2009.
20. Caplehorn JR, Drummer OH. Fatal methadone toxicity: signs and circumstances and the role of benzodiazepines. Aust N Z J Public Health. 2002;26:358-362;discussion 362–363.
Aaron M. Pierce, DO
Dr. Pierce is Medical Director, Psychiatry Clinic, Assistant Professor, Department of Psychiatry, University of Oklahoma School of Community Medicine, Tulsa, OK.
Nancy C. Brahm, PharmD, MS, BCPP
Dr. Brahm is Clinical Associate Professor, Department of Pharmacy Practice: Clinical and Administrative Sciences-Tulsa, University of Oklahoma College of Pharmacy, Tulsa, OK.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Aaron M. Pierce, DO
Dr. Pierce is Medical Director, Psychiatry Clinic, Assistant Professor, Department of Psychiatry, University of Oklahoma School of Community Medicine, Tulsa, OK.
Nancy C. Brahm, PharmD, MS, BCPP
Dr. Brahm is Clinical Associate Professor, Department of Pharmacy Practice: Clinical and Administrative Sciences-Tulsa, University of Oklahoma College of Pharmacy, Tulsa, OK.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Aaron M. Pierce, DO
Dr. Pierce is Medical Director, Psychiatry Clinic, Assistant Professor, Department of Psychiatry, University of Oklahoma School of Community Medicine, Tulsa, OK.
Nancy C. Brahm, PharmD, MS, BCPP
Dr. Brahm is Clinical Associate Professor, Department of Pharmacy Practice: Clinical and Administrative Sciences-Tulsa, University of Oklahoma College of Pharmacy, Tulsa, OK.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
• When choosing pharmacologic therapy, make sure that all medications your patient takes are documented, consider drug-drug interactions, and instruct the patient to notify you of any new medications.
• In addition to toxicity, loss of efficacy of some opiate drugs may occur as a result of metabolic inhibition or induction by psychotropic medications.
• Collaborate with the physician who is prescribing the opioid if psychotropic choices are limited. The patient’s pain may be treated adequately with another analgesic that does not interact with the psychotropic that has been chosen.
As prescribed by his internist, Mr. G, age 44, takes 10 mg of methadone every 4 hours for chronic back pain secondary to a work-related injury 3 years ago. He experiences minimal sedation. Mr. G presents for psychiatric evaluation with complaints of increasing irritability, poor focus, low energy, and lack of interest in usual activities. The psychiatrist diagnoses him with depressive disorder not otherwise specified, and prescribes fluoxetine, 20 mg/d. Three weeks later, Mr. G’s wife contacts the psychiatrist reporting that her husband seems “overmedicated” and describes excess drowsiness and slowed thought processing.
After discussion with Mr. G’s internist and pharmacist, the psychiatrist decides that this oversedation may represent a drug-drug interaction between methadone and fluoxetine resulting in higher-than-expected methadone serum levels. Mr. G is instructed to stop fluoxetine with no taper, and his methadone dose is lowered with good results. Over the next 2 weeks Mr. G is titrated back to his original methadone dose and is re-evaluated by the psychiatrist to discuss medication options to address his depression.
Psychiatrists commonly encounter patients who receive opiate medications for chronic pain. Being aware of potential drug-drug interactions between opiate medications and psychotropics can help avoid adverse effects and combinations that may affect the efficacy of either drug. Pharmacokinetic interactions may affect your choice of psychiatric medication and should be taken into account when addressing adverse effects in any patient who takes opiates and psychotropics.
Metabolic pathways
The primary metabolic pathways for opiate metabolism are the cytochrome P450 (CYP) 2D6 and 3A4 isoenzymes. Depending on the agent used, prescribers may need to consider interactions for both pathways (Table 11,2 and Table 21). For example, oxycodone is metabolized via 2D6 and 3A4 isoenzymes and is a potent analgesic with oxymorphone and noroxycodone as its active metabolites. These metabolites, however, make a negligible contribution to oxycodone’s analgesic effect.3,4 Metabolism by the 3A4 isoenzyme is the principal oxidative pathway and the 2D6 site accounts for approximately 10% of oxycodone metabolism. A randomized, placebo-controlled, crossover study showed that 2D6 inhibition by paroxetine had no significant effect on oxycodone levels; however, a combination of paroxetine and itraconazole, a potent 3A4 inhibitor, resulted in substantial increases in oxycodone plasma levels.5 Remain vigilant for possible opiate toxicity when administering oxycodone with 3A4 inhibitors.
Methadone and meperidine also involve dual pathways. Methadone is metabolized primarily by 3A4 and 2B6, with 2D6 playing a smaller role.6 CYP2D6 seems to play an important part in metabolizing the R-enantiomer of methadone, which is largely responsible for the drug’s opiate effects, such as analgesia and respiratory depression.7,8 Induction of the 3A4 isoenzyme may result in methadone withdrawal, and inhibition may cause methadone toxicity.9 Inducers of 3A4, such as carbamazepine, and inhibitors, such as fluoxetine and fluvoxamine, should be avoided or used very cautiously in patients taking methadone. The 2B6 and 2D6 isoenzymes also may increase or decrease methadone levels and should be treated similarly. In Mr. G’s case, fluoxetine inhibited all 3 isoenzymes that are primarily responsible for methadone metabolism. A better antidepressant choice for Mr. G may have been venlafaxine, which is known to only mildly inhibit 2D6, or mirtazapine, which does not seem to inhibit the major CYP isoforms to an appreciable degree.10
Although the full scope of meperidine metabolism has not been identified,9 an in vitro test demonstrated that 2B6 and 3A4 play important roles in metabolizing meperidine to normeperidine, its major metabolite.11 Normeperidine does not provide analgesia and is associated with neurotoxicity, including anxiety, tremor, muscle twitching, and seizure.12 Agents that induce 3A4—such as carbamazepine or St. John’s wort—may contribute to neurotoxicity.9 Inhibition of these isoenzymes may increase meperidine levels and lead to anticholinergic toxicity or respiratory and central nervous system depression.13,14
Opiates metabolized by the 2D6 isoenzyme include codeine, hydrocodone, and tramadol. The analgesic effect of codeine seems dependent on 2D6 metabolism. Via this pathway, codeine is converted into morphine, which has a 300-times stronger affinity for the μ opioid receptor compared with codeine. 2D6 poor metabolizers have shown codeine intolerance and toxicity.3 Psychotropics known to strongly inhibit 2D6 isoenzyme processes—such as paroxetine, fluoxetine, and bupropion—should be avoided in patients taking codeine to prevent adverse effects and potential loss of efficacy. Better antidepressant choices include citalopram or venlafaxine, which inhibit 2D6 to a lesser degree.
Hydrocodone may be a viable option for patients taking 2D6 inhibitors. Hydrocodone is metabolized by 2D6 into hydromorphone, which is 7 to 33 times more potent than hydrocodone.15 Unlike codeine, 2D6 inhibition may have little effect on hydrocodone’s analgesic properties. Animal studies have shown that inhibition of the CYP analog to 2D6 does not affect analgesic response. In humans, 2D6 inhibition does not seem to affect hydrocodone’s abuse liability.16 Two case reports describe known 2D6 poor metabolizers who showed at least a partial response to hydrocodone.15,16
Tramadol’s analgesic properties may be related to serotonin and norepinephrine reuptake inhibition. It is less potent than codeine but is metabolized via the 2D6 isoenzyme into 0-desmethyltramadol, which is up to 200 times stronger than its parent compound.17 Clinicians should be aware that tramadol’s efficacy may be decreased when coadministered with 2D6 inhibitors. In a randomized, placebo-controlled trial, paroxetine, a potent 2D6 inhibitor, was shown to lessen the analgesic effect of tramadol.18
The 3A4 site is the primary pathway for fentanyl metabolism. Agents that inhibit 3A4 could increase fentanyl plasma concentration, leading to respiratory depression.19 Examples of 3A4 inhibitors include fluoxetine and fluvoxamine.
Psychotropics may inhibit or induce P450 isoenzymes to varying degrees. For example, paroxetine and citalopram are known to inhibit 2D6 but paroxetine is a stronger inhibitor; therefore, a significant drug-drug interaction is more likely with paroxetine and a 2D6 substrate than the same substrate administered with citalopram.
Table 1
Cytochrome P450 isoenzymes inhibited and induced by psychotropics
| Isoenzyme | Potency | Psychotropic(s) |
|---|---|---|
| 2B6 inducer | Moderate | Carbamazepine |
| 2B6 inhibitors | Mild to moderate | Fluoxetine, fluvoxamine |
| Moderate | Sertraline | |
| Potent | Paroxetine | |
| 2D6 inhibitors | Mild | Venlafaxine |
| Mild to moderate | Citalopram, escitalopram, fluvoxamine, risperidone | |
| Moderate | Duloxetine | |
| Moderate to potent | Bupropion | |
| Potent | Fluoxetine, haloperidol, paroxetine | |
| Dose-dependent | Sertraline | |
| 3A4 inducer | Potent | Carbamazepine |
| 3A4 inhibitors | Mild | Sertraline |
| Mild to moderate | Fluoxetine, fluvoxamine | |
| Source: References 1,2 | ||
Table 2
Cytochrome P450 isoenzymes inhibiting and inducing opiate metabolism
| Isoenzyme | Opiates |
|---|---|
| 2B6 inducer | Methadone |
| 2B6 inhibitors | Meperidine, methadone |
| 2D6 inhibitors | Codeine (may involve loss of efficacy as well as toxicity), methadone, tramadol (may involve loss of efficacy) |
| 3A4 inducer | Meperidine, methadone |
| 3A4 inhibitors | Fentanyl, oxycodone, meperidine, methadone |
| Source: Reference 1 | |
Other considerations
In addition to pharmacokinetic interactions, it is important to consider synergistic effects of some opiates and psychotropics. Examples include:
- additive effect on respiratory depression by benzodiazepines and opiates
- increased risk of serotonin syndrome and seizure when using tramadol with selective serotonin reuptake inhibitors or tricyclic antidepressants
- additive prolongation of the QTc interval by methadone when used with psychotropics known to prolong the QTc, such as ziprasidone.9,17,20
Careful attention to these interactions and collaboration among providers can ensure the best outcome for our patients. In Mr. G’s case, collaboration with his internist would be in order, particularly if antidepressant choices are limited. In consultation with the psychiatrist, the internist might choose another opiate to treat Mr. G’s pain that would not interact with fluoxetine. If Mr. G and his physician have struggled to manage his pain and if he is stable on the current regimen, selecting a different antidepressant may be warranted.
Related Resources
- Indiana University School of Medicine drug interactions: cytochrome P450 drug interaction table. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
- Ferrando SJ, Levenson JL, Owen JA, eds. Clinical manual of psychopharmacology in the medically ill. Arlington, VA: American Psychiatric Publishing, Inc; 2010.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fentanyl • Duragesic, Actiq
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Hydrocodone • Lortab, Vicodin, others
- Itraconazole • Sporanox
- Meperidine • Demerol
- Methadone • Dolophine, Methadose
- Mirtazapine • Remeron
- Morphine • Avinza, Duramorph, others
- Oxycodone • OxyContin, Roxicodone
- Paroxetine • Paxil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
• When choosing pharmacologic therapy, make sure that all medications your patient takes are documented, consider drug-drug interactions, and instruct the patient to notify you of any new medications.
• In addition to toxicity, loss of efficacy of some opiate drugs may occur as a result of metabolic inhibition or induction by psychotropic medications.
• Collaborate with the physician who is prescribing the opioid if psychotropic choices are limited. The patient’s pain may be treated adequately with another analgesic that does not interact with the psychotropic that has been chosen.
As prescribed by his internist, Mr. G, age 44, takes 10 mg of methadone every 4 hours for chronic back pain secondary to a work-related injury 3 years ago. He experiences minimal sedation. Mr. G presents for psychiatric evaluation with complaints of increasing irritability, poor focus, low energy, and lack of interest in usual activities. The psychiatrist diagnoses him with depressive disorder not otherwise specified, and prescribes fluoxetine, 20 mg/d. Three weeks later, Mr. G’s wife contacts the psychiatrist reporting that her husband seems “overmedicated” and describes excess drowsiness and slowed thought processing.
After discussion with Mr. G’s internist and pharmacist, the psychiatrist decides that this oversedation may represent a drug-drug interaction between methadone and fluoxetine resulting in higher-than-expected methadone serum levels. Mr. G is instructed to stop fluoxetine with no taper, and his methadone dose is lowered with good results. Over the next 2 weeks Mr. G is titrated back to his original methadone dose and is re-evaluated by the psychiatrist to discuss medication options to address his depression.
Psychiatrists commonly encounter patients who receive opiate medications for chronic pain. Being aware of potential drug-drug interactions between opiate medications and psychotropics can help avoid adverse effects and combinations that may affect the efficacy of either drug. Pharmacokinetic interactions may affect your choice of psychiatric medication and should be taken into account when addressing adverse effects in any patient who takes opiates and psychotropics.
Metabolic pathways
The primary metabolic pathways for opiate metabolism are the cytochrome P450 (CYP) 2D6 and 3A4 isoenzymes. Depending on the agent used, prescribers may need to consider interactions for both pathways (Table 11,2 and Table 21). For example, oxycodone is metabolized via 2D6 and 3A4 isoenzymes and is a potent analgesic with oxymorphone and noroxycodone as its active metabolites. These metabolites, however, make a negligible contribution to oxycodone’s analgesic effect.3,4 Metabolism by the 3A4 isoenzyme is the principal oxidative pathway and the 2D6 site accounts for approximately 10% of oxycodone metabolism. A randomized, placebo-controlled, crossover study showed that 2D6 inhibition by paroxetine had no significant effect on oxycodone levels; however, a combination of paroxetine and itraconazole, a potent 3A4 inhibitor, resulted in substantial increases in oxycodone plasma levels.5 Remain vigilant for possible opiate toxicity when administering oxycodone with 3A4 inhibitors.
Methadone and meperidine also involve dual pathways. Methadone is metabolized primarily by 3A4 and 2B6, with 2D6 playing a smaller role.6 CYP2D6 seems to play an important part in metabolizing the R-enantiomer of methadone, which is largely responsible for the drug’s opiate effects, such as analgesia and respiratory depression.7,8 Induction of the 3A4 isoenzyme may result in methadone withdrawal, and inhibition may cause methadone toxicity.9 Inducers of 3A4, such as carbamazepine, and inhibitors, such as fluoxetine and fluvoxamine, should be avoided or used very cautiously in patients taking methadone. The 2B6 and 2D6 isoenzymes also may increase or decrease methadone levels and should be treated similarly. In Mr. G’s case, fluoxetine inhibited all 3 isoenzymes that are primarily responsible for methadone metabolism. A better antidepressant choice for Mr. G may have been venlafaxine, which is known to only mildly inhibit 2D6, or mirtazapine, which does not seem to inhibit the major CYP isoforms to an appreciable degree.10
Although the full scope of meperidine metabolism has not been identified,9 an in vitro test demonstrated that 2B6 and 3A4 play important roles in metabolizing meperidine to normeperidine, its major metabolite.11 Normeperidine does not provide analgesia and is associated with neurotoxicity, including anxiety, tremor, muscle twitching, and seizure.12 Agents that induce 3A4—such as carbamazepine or St. John’s wort—may contribute to neurotoxicity.9 Inhibition of these isoenzymes may increase meperidine levels and lead to anticholinergic toxicity or respiratory and central nervous system depression.13,14
Opiates metabolized by the 2D6 isoenzyme include codeine, hydrocodone, and tramadol. The analgesic effect of codeine seems dependent on 2D6 metabolism. Via this pathway, codeine is converted into morphine, which has a 300-times stronger affinity for the μ opioid receptor compared with codeine. 2D6 poor metabolizers have shown codeine intolerance and toxicity.3 Psychotropics known to strongly inhibit 2D6 isoenzyme processes—such as paroxetine, fluoxetine, and bupropion—should be avoided in patients taking codeine to prevent adverse effects and potential loss of efficacy. Better antidepressant choices include citalopram or venlafaxine, which inhibit 2D6 to a lesser degree.
Hydrocodone may be a viable option for patients taking 2D6 inhibitors. Hydrocodone is metabolized by 2D6 into hydromorphone, which is 7 to 33 times more potent than hydrocodone.15 Unlike codeine, 2D6 inhibition may have little effect on hydrocodone’s analgesic properties. Animal studies have shown that inhibition of the CYP analog to 2D6 does not affect analgesic response. In humans, 2D6 inhibition does not seem to affect hydrocodone’s abuse liability.16 Two case reports describe known 2D6 poor metabolizers who showed at least a partial response to hydrocodone.15,16
Tramadol’s analgesic properties may be related to serotonin and norepinephrine reuptake inhibition. It is less potent than codeine but is metabolized via the 2D6 isoenzyme into 0-desmethyltramadol, which is up to 200 times stronger than its parent compound.17 Clinicians should be aware that tramadol’s efficacy may be decreased when coadministered with 2D6 inhibitors. In a randomized, placebo-controlled trial, paroxetine, a potent 2D6 inhibitor, was shown to lessen the analgesic effect of tramadol.18
The 3A4 site is the primary pathway for fentanyl metabolism. Agents that inhibit 3A4 could increase fentanyl plasma concentration, leading to respiratory depression.19 Examples of 3A4 inhibitors include fluoxetine and fluvoxamine.
Psychotropics may inhibit or induce P450 isoenzymes to varying degrees. For example, paroxetine and citalopram are known to inhibit 2D6 but paroxetine is a stronger inhibitor; therefore, a significant drug-drug interaction is more likely with paroxetine and a 2D6 substrate than the same substrate administered with citalopram.
Table 1
Cytochrome P450 isoenzymes inhibited and induced by psychotropics
| Isoenzyme | Potency | Psychotropic(s) |
|---|---|---|
| 2B6 inducer | Moderate | Carbamazepine |
| 2B6 inhibitors | Mild to moderate | Fluoxetine, fluvoxamine |
| Moderate | Sertraline | |
| Potent | Paroxetine | |
| 2D6 inhibitors | Mild | Venlafaxine |
| Mild to moderate | Citalopram, escitalopram, fluvoxamine, risperidone | |
| Moderate | Duloxetine | |
| Moderate to potent | Bupropion | |
| Potent | Fluoxetine, haloperidol, paroxetine | |
| Dose-dependent | Sertraline | |
| 3A4 inducer | Potent | Carbamazepine |
| 3A4 inhibitors | Mild | Sertraline |
| Mild to moderate | Fluoxetine, fluvoxamine | |
| Source: References 1,2 | ||
Table 2
Cytochrome P450 isoenzymes inhibiting and inducing opiate metabolism
| Isoenzyme | Opiates |
|---|---|
| 2B6 inducer | Methadone |
| 2B6 inhibitors | Meperidine, methadone |
| 2D6 inhibitors | Codeine (may involve loss of efficacy as well as toxicity), methadone, tramadol (may involve loss of efficacy) |
| 3A4 inducer | Meperidine, methadone |
| 3A4 inhibitors | Fentanyl, oxycodone, meperidine, methadone |
| Source: Reference 1 | |
Other considerations
In addition to pharmacokinetic interactions, it is important to consider synergistic effects of some opiates and psychotropics. Examples include:
- additive effect on respiratory depression by benzodiazepines and opiates
- increased risk of serotonin syndrome and seizure when using tramadol with selective serotonin reuptake inhibitors or tricyclic antidepressants
- additive prolongation of the QTc interval by methadone when used with psychotropics known to prolong the QTc, such as ziprasidone.9,17,20
Careful attention to these interactions and collaboration among providers can ensure the best outcome for our patients. In Mr. G’s case, collaboration with his internist would be in order, particularly if antidepressant choices are limited. In consultation with the psychiatrist, the internist might choose another opiate to treat Mr. G’s pain that would not interact with fluoxetine. If Mr. G and his physician have struggled to manage his pain and if he is stable on the current regimen, selecting a different antidepressant may be warranted.
Related Resources
- Indiana University School of Medicine drug interactions: cytochrome P450 drug interaction table. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
- Ferrando SJ, Levenson JL, Owen JA, eds. Clinical manual of psychopharmacology in the medically ill. Arlington, VA: American Psychiatric Publishing, Inc; 2010.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fentanyl • Duragesic, Actiq
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Hydrocodone • Lortab, Vicodin, others
- Itraconazole • Sporanox
- Meperidine • Demerol
- Methadone • Dolophine, Methadose
- Mirtazapine • Remeron
- Morphine • Avinza, Duramorph, others
- Oxycodone • OxyContin, Roxicodone
- Paroxetine • Paxil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sandson NB, Armstrong SC, Cozza KL. An overview of psychotropic drug-drug interactions. Psychosomatics. 2005;46:464-494.
2. Faucette SR, Wang H, Hamilton GA. Regulation of CYP2B6 in primary human hepatocytes by prototypical inducers. Drug Metab Dispos. 2004;32(3):348-358.
3. Smith HS. Opioid metabolism. Mayo Clin Proc. 2009;84:613-624.
4. Armstrong SC, Cozza KL. Pharmacokinetic drug interactions of morphine codeine, and their derivatives: theory and clinical reality, part II. Psychosomatics. 2003;44:515-520.
5. Grönlund J, Saari TI, Hagelberg NM, et al. Exposure to oral oxycodone is increased by concomitant inhibition of CYP2D6 and 3A4 pathways, but not by inhibition of CYP2D6 alone. Br J Clin Pharmacol. 2010;70:78-87.
6. Leavitt SB. Methadone-drug* interactions. (*medications illicit drugs, and other substances). 3rd ed. Mundelein, IL: Addiction Treatment Forum; 2005.
7. Pérez de los Cobos J, Siñol N, Trujols J, et al. Association of CYP2D6 ultrarapid metabolizer genotype with deficient patient satisfaction regarding methadone maintenance treatment. Drug Alcohol Depend. 2007;89:190-194.
8. Kristensen K, Christensen CB, Christrup LL. The mu1 mu2, delta, kappa opioid receptor binding profiles of methadone stereoisomers and morphine. Life Sci. 1995;56:PL45-50.
9. Armstrong SC, Wynn GH, Sandson NB. Pharmacokinetic drug interactions of synthetic opiate analgesics. Psychosomatics. 2009;50:169-176.
10. Spina E, Santoro V, D’Arrigo C. Clinically relevant pharmacokinetic drug interactions with second-generation antidepressants: an update. Clin Ther. 2008;30:1206-1227.
11. Ramírez J, Innocenti F, Schuetz EG, et al. CYP2B6, CYP3A4, and CYP2C19 are responsible for the in vitro N-demethylation of meperidine in human liver microsomes. Drug Metab Dispos. 2004;32:930-936.
12. Kaiko RF, Foley KM, Grabinski PY, et al. Central nervous system excitatory effects of meperidine in cancer patients. Ann Neurol. 1983;13:180-185.
13. Chalverus C. Clinically important meperidine toxicities. Journal of Pharmaceutical Care in Pain and Symptom Control. 2001;9:37-55.
14. Beckwith MC, Fox ER, Chandramouli J. Removing meperidine from the health-system formulary—frequently asked questions. J Pain Palliat Care Pharmacother. 2002;16:45-59.
15. Foster A, Mobley E, Wang Z. Complicated pain management in a CYP450 2D6 poor metabolizer. Pain Pract. 2007;7:352-356.
16. Susce MT, Murray-Carmichael E, de Leon J. Response to hydrocodone codeine and oxycodone in a CYP2D6 poor metabolizer. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30:1356-1358.
17. Sansone RA, Sansone LA. Tramadol: seizures serotonin syndrome, and coadministered antidepressants. Psychiatry (Edgmont). 2009;6:17-21.
18. Laugesen S, Enggaard TP, Pedersen RS, et al. Paroxetine, a cytochrome P450 2D6 inhibitor, diminishes the stereoselective O-demethylation and reduces the hypoalgesic effect of tramadol. Clin Pharmacol Ther. 2005;77:312-323.
19. Duragesic [package insert]. Raritan NJ: Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2009.
20. Caplehorn JR, Drummer OH. Fatal methadone toxicity: signs and circumstances and the role of benzodiazepines. Aust N Z J Public Health. 2002;26:358-362;discussion 362–363.
1. Sandson NB, Armstrong SC, Cozza KL. An overview of psychotropic drug-drug interactions. Psychosomatics. 2005;46:464-494.
2. Faucette SR, Wang H, Hamilton GA. Regulation of CYP2B6 in primary human hepatocytes by prototypical inducers. Drug Metab Dispos. 2004;32(3):348-358.
3. Smith HS. Opioid metabolism. Mayo Clin Proc. 2009;84:613-624.
4. Armstrong SC, Cozza KL. Pharmacokinetic drug interactions of morphine codeine, and their derivatives: theory and clinical reality, part II. Psychosomatics. 2003;44:515-520.
5. Grönlund J, Saari TI, Hagelberg NM, et al. Exposure to oral oxycodone is increased by concomitant inhibition of CYP2D6 and 3A4 pathways, but not by inhibition of CYP2D6 alone. Br J Clin Pharmacol. 2010;70:78-87.
6. Leavitt SB. Methadone-drug* interactions. (*medications illicit drugs, and other substances). 3rd ed. Mundelein, IL: Addiction Treatment Forum; 2005.
7. Pérez de los Cobos J, Siñol N, Trujols J, et al. Association of CYP2D6 ultrarapid metabolizer genotype with deficient patient satisfaction regarding methadone maintenance treatment. Drug Alcohol Depend. 2007;89:190-194.
8. Kristensen K, Christensen CB, Christrup LL. The mu1 mu2, delta, kappa opioid receptor binding profiles of methadone stereoisomers and morphine. Life Sci. 1995;56:PL45-50.
9. Armstrong SC, Wynn GH, Sandson NB. Pharmacokinetic drug interactions of synthetic opiate analgesics. Psychosomatics. 2009;50:169-176.
10. Spina E, Santoro V, D’Arrigo C. Clinically relevant pharmacokinetic drug interactions with second-generation antidepressants: an update. Clin Ther. 2008;30:1206-1227.
11. Ramírez J, Innocenti F, Schuetz EG, et al. CYP2B6, CYP3A4, and CYP2C19 are responsible for the in vitro N-demethylation of meperidine in human liver microsomes. Drug Metab Dispos. 2004;32:930-936.
12. Kaiko RF, Foley KM, Grabinski PY, et al. Central nervous system excitatory effects of meperidine in cancer patients. Ann Neurol. 1983;13:180-185.
13. Chalverus C. Clinically important meperidine toxicities. Journal of Pharmaceutical Care in Pain and Symptom Control. 2001;9:37-55.
14. Beckwith MC, Fox ER, Chandramouli J. Removing meperidine from the health-system formulary—frequently asked questions. J Pain Palliat Care Pharmacother. 2002;16:45-59.
15. Foster A, Mobley E, Wang Z. Complicated pain management in a CYP450 2D6 poor metabolizer. Pain Pract. 2007;7:352-356.
16. Susce MT, Murray-Carmichael E, de Leon J. Response to hydrocodone codeine and oxycodone in a CYP2D6 poor metabolizer. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30:1356-1358.
17. Sansone RA, Sansone LA. Tramadol: seizures serotonin syndrome, and coadministered antidepressants. Psychiatry (Edgmont). 2009;6:17-21.
18. Laugesen S, Enggaard TP, Pedersen RS, et al. Paroxetine, a cytochrome P450 2D6 inhibitor, diminishes the stereoselective O-demethylation and reduces the hypoalgesic effect of tramadol. Clin Pharmacol Ther. 2005;77:312-323.
19. Duragesic [package insert]. Raritan NJ: Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2009.
20. Caplehorn JR, Drummer OH. Fatal methadone toxicity: signs and circumstances and the role of benzodiazepines. Aust N Z J Public Health. 2002;26:358-362;discussion 362–363.
Abuse of second-generation antipsychotics: What prescribers need to know
• Antipsychotics have been abused and misused by inpatients and outpatients.
• Most published case reports of antipsychotic abuse involve quetiapine, although some describe misuse of other agents, including olanzapine.
• Serotonin, histamine, and α-adrenergic neurotransmitter systems may play a role in second-generation antipsychotics’ abuse potential.
• Although individuals have misused quetiapine and olanzapine, evidence indicates that these drugs may be effective for treating substance use disorders.
Mr. Z, age 27, seeks treatment for substance abuse at a mental health clinic. He has a 7-year substance use history and his last urine drug screen 1 month ago was positive for marijuana, opiates, and benzodiazepines. Mr. Z reveals that he purchases prescription drugs on the street, including hydrocodone, diazepam, and quetiapine. He states that when he takes a 100-mg dose of quetiapine, he feels happy, relaxed, and “drunk without the mind-numbing effects that you get with alcohol.” Mr. Z often takes quetiapine while smoking marijuana. He sleeps well with this and does not experience a hangover effect.
Although clinicians always are vigilant about patients’ misuse of psychoactive substances, recent case reports have described abuse of antipsychotics, particularly second-generation antipsychotics (SGAs). A PubMed and PsycINFO literature search revealed several case reports of quetiapine abuse (Table)1-6 and 2 case reports of olanzapine misuse.
Table
Case reports of quetiapine abuse
| Reference | Patient | Setting | Description of abuse |
|---|---|---|---|
| Hussain et al, 20051 | Woman, age 34, with history of polysubstance abuse, depression, and borderline personality traits | Prison | Crushed tablets dissolved in water and injected intravenously |
| Morin, 20072 | Woman, age 28, with history of schizoaffective disorder, polysubstance abuse, and personality disorder not otherwise specified | Hospital | Tablets crushed with aspirin and inhaled intranasally |
| Waters et al, 20073 | Man, age 33, with history of polysubstance abuse | Outpatient | Crushed tablets dissolved in water and injected intravenously |
| Reeves et al, 20074 | Man, age 49, with history of alcohol dependence and benzodiazepine abuse | Outpatient | Misuse without psychiatric symptoms or a diagnosed psychiatric disorder |
| Man, age 23, with history of benzodiazepine dependence | Outpatient | Misuse without psychiatric symptoms or a diagnosed psychiatric disorder | |
| Man, age 39, with history of bipolar disorder | Outpatient | Oral use in doses more than the prescribed amount | |
| Murphy et al, 20085 | Man, age 29, with unclear history of schizophrenia | Psychiatric walk-in clinic | Malingering psychiatric symptoms to obtain an oral dose and overnight stay |
| Fischer et al, 20096 | Man, age 53, with history of depressive symptoms | Court-mandated outpatient clinic | Malingering psychiatric symptoms to obtain higher oral doses |
Quetiapine
Methods of quetiapine misuse include ingesting pills, inhaling crushed tablets, and injecting a solution of dissolved tablets.1-7 In case studies, patients report abusing quetiapine for its sedative, anxiolytic, and calming effects.1,2,4-7 One patient reported snorting crushed quetiapine tablets combined with cocaine for “hallucinogenic” effects.3 Street names for quetiapine include “quell,” “Susie-Q,” and “baby heroin,” and “Q-ball” refers to a combination of cocaine and quetiapine.8 Quetiapine tablets have a street value of $3 to $8 for doses ranging from 25 mg to 100 mg.9 Although outpatient misuse of quetiapine is common, abuse in correctional settings also is becoming more frequent.10 Residents of jails and prisons misuse quetiapine for reasons similar to those cited by outpatients: sedation, relief of anxiety, and hallucinogenic effects or “getting high.”1,2,10 Clinicians must differentiate inmates who have legitimate psychiatric symptoms that require antipsychotic treatment from those who are malingering to obtain the drug. Efforts to treat inmates for substance use disorders may be thwarted by the easy availability of drugs in correctional settings.10
Other SGAs
The incidence of misuse of olanzapine and other SGAs is more difficult to ascertain. Only 2 case reports describe olanzapine abuse, both in outpatient settings. One describes a patient treated for depression with psychosis who was using increasingly higher doses of olanzapine to obtain euphoric effects.11 Switching to aripiprazole effectively treated her illness and addressed her olanzapine misuse.
In the other case, a patient with bipolar disorder was able to obtain olanzapine, 40 mg/d, by complaining of worsened manic symptoms.12 He described the experience of misusing olanzapine as getting a “buzz,” feeling “very relaxed,” and blunting the negative jitteriness he felt when he used cocaine.12 This patient stated that he had observed others abusing olanzapine, both orally and intravenously.
Although the literature lacks reports on the risks of antipsychotic abuse, numerous Web sites purport to sell these drugs without a prescription and some describe the experience of illicit use of drugs such as haloperidol, risperidone, quetiapine, and olanzapine and ways to “enhance” the experience by combining drugs.13 Reported experiences with risperidone tend to be negative, citing extrapyramidal side effects and feeling “numb,” whereas olanzapine and quetiapine users describe feeling “drunk without the bad effects of alcohol” and “really happy, calm.” These sites also describe hallucinogenic effects of these agents.13
Mechanism of action
The neuropharmacologic reasons for antipsychotics’ abuse potential are difficult to quantify. Quetiapine and olanzapine have been used to treat cocaine and alcohol abuse, and work perhaps by decreasing the dopamine reward system response to substance use.14,15 Quetiapine’s rapid dissociation from the dopamine receptor has been theorized to contribute to the drug’s abuse potential, possibly through relatively lower potency and decreased residence time at the dopamine receptor.14-16 This mechanism also contributes to quetiapine’s lower risk of extrapyramidal side effects, which make the drug easier to tolerate.
Although dopamine is a factor in substance abuse and treatment of psychotic disorders, other neuropharmacologic mechanisms must be considered. SGAs are theorized to cause dopamine release in the frontal cortex through effects as 5-HT1A agonists and 5-HT2A antagonists.16 Antagonism of α-adrenergic and histaminic receptors may account for these agents’ anxiolytic and sedative properties.8
Misuse of anticholinergic agents has been reported for >50 years.17 Psychiatric patients have been reported to increase use of anticholinergics for their movement side effects as well as hallucinogenic effects.18
Treatment
Regardless of the substance that patients abuse, the treatment goals are the same: to reduce use and achieve recovery. If a patient with psychosis is abusing an SGA, consider switching to an antipsychotic with less abuse potential. Another option is to limit the supply of the abused drug by prescribing smaller quantities or increase the frequency of follow-up visits to ensure compliant use.
Related Resources
- Substance Abuse and Mental Health Services Administration. www.samhsa.gov.
- Galanter M, Kelber HD. The American Psychiatric Publishing textbook of substance abuse treatment. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
Drug Brand Names
- Aripiprazole • Abilify
- Diazepam • Valium
- Haloperidol • Haldol
- Hydrocodone/acetaminophen • Vicodin
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Hussain MZ, Waheed W, Hussain S. Intravenous quetiapine abuse. Am J Psychiatry. 2005;162:1755-1756.
2. Morin AK. Possible intranasal quetiapine misuse. Am J Health Syst Pharm. 2007;64:723-725.
3. Waters BM, Joshi KG. Intravenous quetiapine-cocaine use (“Q-ball”). Am J Psychiatry. 2007;164:1.-
4. Reeves RR, Brister JC. Additional evidence of the abuse potential of quetiapine. S Med J. 2007;100:834-836.
5. Murphy D, Bailey K, Stone M, et al. Addictive potential of quetiapine. Am J Psychiatry. 2008;165:7.-
6. Fischer BA, Boggs DL. The role of antihistaminic effects in the misuse of quetiapine: a case report and review of the literature. Neurosci Biobehav Rev. 2009;34:555-558.
7. Pierre JM, Shnayder I, Wirshing DA, et al. Intranasal quetiapine abuse. Am J Psychiatry. 2004;161(9):1718.-
8. Sansone RA, Sansone LA. Is seroquel developing an illicit reputation for misuse/abuse? Psychiatry (Edgemont). 2010;7(1):13-16.
9. Tarasoff G, Osti K. Black-market value of antipsychotics antidepressants, and hypnotics in Las Vegas, Nevada. Am J Psychiatry. 2007;164:350.-
10. Keltner NL, Vance DE. Biological perspectives: incarcerated care and quetiapine abuse. Perspect Psychiatr Care. 2008;44(3):202-206.
11. Lai CH. Olanzapine abuse was relieved after switching to aripiprazole in a patient with psychotic depression. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(7):1363-1364.
12. Reeves RR. Abuse of olanzapine by substance abusers. J Psychoactive Drugs. 2007;39(3):297-299.
13. The Vaults of Erowid. Available at: . Accessed April 1 2011.
14. Hanley NJ, Kenna GA. Quetiapine: treatment for substance abuse and drug of abuse. Am J Health Syst Pharm. 2008;65:611-618.
15. Tcheremissine OV. Is quetiapine a drug of abuse? Reexamining the issue of addiction. Expert Opin Drug Saf. 2008;7:739-748.
16. Kuroki T, Nagao N, Nakahara T. Neuropharmacology of second-generation antipsychotic drugs: a validity of the serotonin-dopamine hypothesis. Prog Brain Res. 2008;172:199-212.
17. Smith JM. Abuse of the antiparkinson drugs: a review of the literature. J Clin Psychiatry. 1980;41(10):351-354.
18. Land W, Pinsky D, Salzman C. Abuse and misuse of anticholinergic medications. Hosp Community Psychiatry. 1991;42:580-581.
Gregory T. Bogart, PharmD
Dr. Bogart is a Second-Year Psychiatric Pharmacy Resident
Carol A. Ott, PharmD, BCPP
Dr. Ott is a Clinical Assistant Professor of Pharmacy Practice, Purdue University College of Pharmacy, Indianapolis, IN.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Gregory T. Bogart, PharmD
Dr. Bogart is a Second-Year Psychiatric Pharmacy Resident
Carol A. Ott, PharmD, BCPP
Dr. Ott is a Clinical Assistant Professor of Pharmacy Practice, Purdue University College of Pharmacy, Indianapolis, IN.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Gregory T. Bogart, PharmD
Dr. Bogart is a Second-Year Psychiatric Pharmacy Resident
Carol A. Ott, PharmD, BCPP
Dr. Ott is a Clinical Assistant Professor of Pharmacy Practice, Purdue University College of Pharmacy, Indianapolis, IN.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
• Antipsychotics have been abused and misused by inpatients and outpatients.
• Most published case reports of antipsychotic abuse involve quetiapine, although some describe misuse of other agents, including olanzapine.
• Serotonin, histamine, and α-adrenergic neurotransmitter systems may play a role in second-generation antipsychotics’ abuse potential.
• Although individuals have misused quetiapine and olanzapine, evidence indicates that these drugs may be effective for treating substance use disorders.
Mr. Z, age 27, seeks treatment for substance abuse at a mental health clinic. He has a 7-year substance use history and his last urine drug screen 1 month ago was positive for marijuana, opiates, and benzodiazepines. Mr. Z reveals that he purchases prescription drugs on the street, including hydrocodone, diazepam, and quetiapine. He states that when he takes a 100-mg dose of quetiapine, he feels happy, relaxed, and “drunk without the mind-numbing effects that you get with alcohol.” Mr. Z often takes quetiapine while smoking marijuana. He sleeps well with this and does not experience a hangover effect.
Although clinicians always are vigilant about patients’ misuse of psychoactive substances, recent case reports have described abuse of antipsychotics, particularly second-generation antipsychotics (SGAs). A PubMed and PsycINFO literature search revealed several case reports of quetiapine abuse (Table)1-6 and 2 case reports of olanzapine misuse.
Table
Case reports of quetiapine abuse
| Reference | Patient | Setting | Description of abuse |
|---|---|---|---|
| Hussain et al, 20051 | Woman, age 34, with history of polysubstance abuse, depression, and borderline personality traits | Prison | Crushed tablets dissolved in water and injected intravenously |
| Morin, 20072 | Woman, age 28, with history of schizoaffective disorder, polysubstance abuse, and personality disorder not otherwise specified | Hospital | Tablets crushed with aspirin and inhaled intranasally |
| Waters et al, 20073 | Man, age 33, with history of polysubstance abuse | Outpatient | Crushed tablets dissolved in water and injected intravenously |
| Reeves et al, 20074 | Man, age 49, with history of alcohol dependence and benzodiazepine abuse | Outpatient | Misuse without psychiatric symptoms or a diagnosed psychiatric disorder |
| Man, age 23, with history of benzodiazepine dependence | Outpatient | Misuse without psychiatric symptoms or a diagnosed psychiatric disorder | |
| Man, age 39, with history of bipolar disorder | Outpatient | Oral use in doses more than the prescribed amount | |
| Murphy et al, 20085 | Man, age 29, with unclear history of schizophrenia | Psychiatric walk-in clinic | Malingering psychiatric symptoms to obtain an oral dose and overnight stay |
| Fischer et al, 20096 | Man, age 53, with history of depressive symptoms | Court-mandated outpatient clinic | Malingering psychiatric symptoms to obtain higher oral doses |
Quetiapine
Methods of quetiapine misuse include ingesting pills, inhaling crushed tablets, and injecting a solution of dissolved tablets.1-7 In case studies, patients report abusing quetiapine for its sedative, anxiolytic, and calming effects.1,2,4-7 One patient reported snorting crushed quetiapine tablets combined with cocaine for “hallucinogenic” effects.3 Street names for quetiapine include “quell,” “Susie-Q,” and “baby heroin,” and “Q-ball” refers to a combination of cocaine and quetiapine.8 Quetiapine tablets have a street value of $3 to $8 for doses ranging from 25 mg to 100 mg.9 Although outpatient misuse of quetiapine is common, abuse in correctional settings also is becoming more frequent.10 Residents of jails and prisons misuse quetiapine for reasons similar to those cited by outpatients: sedation, relief of anxiety, and hallucinogenic effects or “getting high.”1,2,10 Clinicians must differentiate inmates who have legitimate psychiatric symptoms that require antipsychotic treatment from those who are malingering to obtain the drug. Efforts to treat inmates for substance use disorders may be thwarted by the easy availability of drugs in correctional settings.10
Other SGAs
The incidence of misuse of olanzapine and other SGAs is more difficult to ascertain. Only 2 case reports describe olanzapine abuse, both in outpatient settings. One describes a patient treated for depression with psychosis who was using increasingly higher doses of olanzapine to obtain euphoric effects.11 Switching to aripiprazole effectively treated her illness and addressed her olanzapine misuse.
In the other case, a patient with bipolar disorder was able to obtain olanzapine, 40 mg/d, by complaining of worsened manic symptoms.12 He described the experience of misusing olanzapine as getting a “buzz,” feeling “very relaxed,” and blunting the negative jitteriness he felt when he used cocaine.12 This patient stated that he had observed others abusing olanzapine, both orally and intravenously.
Although the literature lacks reports on the risks of antipsychotic abuse, numerous Web sites purport to sell these drugs without a prescription and some describe the experience of illicit use of drugs such as haloperidol, risperidone, quetiapine, and olanzapine and ways to “enhance” the experience by combining drugs.13 Reported experiences with risperidone tend to be negative, citing extrapyramidal side effects and feeling “numb,” whereas olanzapine and quetiapine users describe feeling “drunk without the bad effects of alcohol” and “really happy, calm.” These sites also describe hallucinogenic effects of these agents.13
Mechanism of action
The neuropharmacologic reasons for antipsychotics’ abuse potential are difficult to quantify. Quetiapine and olanzapine have been used to treat cocaine and alcohol abuse, and work perhaps by decreasing the dopamine reward system response to substance use.14,15 Quetiapine’s rapid dissociation from the dopamine receptor has been theorized to contribute to the drug’s abuse potential, possibly through relatively lower potency and decreased residence time at the dopamine receptor.14-16 This mechanism also contributes to quetiapine’s lower risk of extrapyramidal side effects, which make the drug easier to tolerate.
Although dopamine is a factor in substance abuse and treatment of psychotic disorders, other neuropharmacologic mechanisms must be considered. SGAs are theorized to cause dopamine release in the frontal cortex through effects as 5-HT1A agonists and 5-HT2A antagonists.16 Antagonism of α-adrenergic and histaminic receptors may account for these agents’ anxiolytic and sedative properties.8
Misuse of anticholinergic agents has been reported for >50 years.17 Psychiatric patients have been reported to increase use of anticholinergics for their movement side effects as well as hallucinogenic effects.18
Treatment
Regardless of the substance that patients abuse, the treatment goals are the same: to reduce use and achieve recovery. If a patient with psychosis is abusing an SGA, consider switching to an antipsychotic with less abuse potential. Another option is to limit the supply of the abused drug by prescribing smaller quantities or increase the frequency of follow-up visits to ensure compliant use.
Related Resources
- Substance Abuse and Mental Health Services Administration. www.samhsa.gov.
- Galanter M, Kelber HD. The American Psychiatric Publishing textbook of substance abuse treatment. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
Drug Brand Names
- Aripiprazole • Abilify
- Diazepam • Valium
- Haloperidol • Haldol
- Hydrocodone/acetaminophen • Vicodin
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
• Antipsychotics have been abused and misused by inpatients and outpatients.
• Most published case reports of antipsychotic abuse involve quetiapine, although some describe misuse of other agents, including olanzapine.
• Serotonin, histamine, and α-adrenergic neurotransmitter systems may play a role in second-generation antipsychotics’ abuse potential.
• Although individuals have misused quetiapine and olanzapine, evidence indicates that these drugs may be effective for treating substance use disorders.
Mr. Z, age 27, seeks treatment for substance abuse at a mental health clinic. He has a 7-year substance use history and his last urine drug screen 1 month ago was positive for marijuana, opiates, and benzodiazepines. Mr. Z reveals that he purchases prescription drugs on the street, including hydrocodone, diazepam, and quetiapine. He states that when he takes a 100-mg dose of quetiapine, he feels happy, relaxed, and “drunk without the mind-numbing effects that you get with alcohol.” Mr. Z often takes quetiapine while smoking marijuana. He sleeps well with this and does not experience a hangover effect.
Although clinicians always are vigilant about patients’ misuse of psychoactive substances, recent case reports have described abuse of antipsychotics, particularly second-generation antipsychotics (SGAs). A PubMed and PsycINFO literature search revealed several case reports of quetiapine abuse (Table)1-6 and 2 case reports of olanzapine misuse.
Table
Case reports of quetiapine abuse
| Reference | Patient | Setting | Description of abuse |
|---|---|---|---|
| Hussain et al, 20051 | Woman, age 34, with history of polysubstance abuse, depression, and borderline personality traits | Prison | Crushed tablets dissolved in water and injected intravenously |
| Morin, 20072 | Woman, age 28, with history of schizoaffective disorder, polysubstance abuse, and personality disorder not otherwise specified | Hospital | Tablets crushed with aspirin and inhaled intranasally |
| Waters et al, 20073 | Man, age 33, with history of polysubstance abuse | Outpatient | Crushed tablets dissolved in water and injected intravenously |
| Reeves et al, 20074 | Man, age 49, with history of alcohol dependence and benzodiazepine abuse | Outpatient | Misuse without psychiatric symptoms or a diagnosed psychiatric disorder |
| Man, age 23, with history of benzodiazepine dependence | Outpatient | Misuse without psychiatric symptoms or a diagnosed psychiatric disorder | |
| Man, age 39, with history of bipolar disorder | Outpatient | Oral use in doses more than the prescribed amount | |
| Murphy et al, 20085 | Man, age 29, with unclear history of schizophrenia | Psychiatric walk-in clinic | Malingering psychiatric symptoms to obtain an oral dose and overnight stay |
| Fischer et al, 20096 | Man, age 53, with history of depressive symptoms | Court-mandated outpatient clinic | Malingering psychiatric symptoms to obtain higher oral doses |
Quetiapine
Methods of quetiapine misuse include ingesting pills, inhaling crushed tablets, and injecting a solution of dissolved tablets.1-7 In case studies, patients report abusing quetiapine for its sedative, anxiolytic, and calming effects.1,2,4-7 One patient reported snorting crushed quetiapine tablets combined with cocaine for “hallucinogenic” effects.3 Street names for quetiapine include “quell,” “Susie-Q,” and “baby heroin,” and “Q-ball” refers to a combination of cocaine and quetiapine.8 Quetiapine tablets have a street value of $3 to $8 for doses ranging from 25 mg to 100 mg.9 Although outpatient misuse of quetiapine is common, abuse in correctional settings also is becoming more frequent.10 Residents of jails and prisons misuse quetiapine for reasons similar to those cited by outpatients: sedation, relief of anxiety, and hallucinogenic effects or “getting high.”1,2,10 Clinicians must differentiate inmates who have legitimate psychiatric symptoms that require antipsychotic treatment from those who are malingering to obtain the drug. Efforts to treat inmates for substance use disorders may be thwarted by the easy availability of drugs in correctional settings.10
Other SGAs
The incidence of misuse of olanzapine and other SGAs is more difficult to ascertain. Only 2 case reports describe olanzapine abuse, both in outpatient settings. One describes a patient treated for depression with psychosis who was using increasingly higher doses of olanzapine to obtain euphoric effects.11 Switching to aripiprazole effectively treated her illness and addressed her olanzapine misuse.
In the other case, a patient with bipolar disorder was able to obtain olanzapine, 40 mg/d, by complaining of worsened manic symptoms.12 He described the experience of misusing olanzapine as getting a “buzz,” feeling “very relaxed,” and blunting the negative jitteriness he felt when he used cocaine.12 This patient stated that he had observed others abusing olanzapine, both orally and intravenously.
Although the literature lacks reports on the risks of antipsychotic abuse, numerous Web sites purport to sell these drugs without a prescription and some describe the experience of illicit use of drugs such as haloperidol, risperidone, quetiapine, and olanzapine and ways to “enhance” the experience by combining drugs.13 Reported experiences with risperidone tend to be negative, citing extrapyramidal side effects and feeling “numb,” whereas olanzapine and quetiapine users describe feeling “drunk without the bad effects of alcohol” and “really happy, calm.” These sites also describe hallucinogenic effects of these agents.13
Mechanism of action
The neuropharmacologic reasons for antipsychotics’ abuse potential are difficult to quantify. Quetiapine and olanzapine have been used to treat cocaine and alcohol abuse, and work perhaps by decreasing the dopamine reward system response to substance use.14,15 Quetiapine’s rapid dissociation from the dopamine receptor has been theorized to contribute to the drug’s abuse potential, possibly through relatively lower potency and decreased residence time at the dopamine receptor.14-16 This mechanism also contributes to quetiapine’s lower risk of extrapyramidal side effects, which make the drug easier to tolerate.
Although dopamine is a factor in substance abuse and treatment of psychotic disorders, other neuropharmacologic mechanisms must be considered. SGAs are theorized to cause dopamine release in the frontal cortex through effects as 5-HT1A agonists and 5-HT2A antagonists.16 Antagonism of α-adrenergic and histaminic receptors may account for these agents’ anxiolytic and sedative properties.8
Misuse of anticholinergic agents has been reported for >50 years.17 Psychiatric patients have been reported to increase use of anticholinergics for their movement side effects as well as hallucinogenic effects.18
Treatment
Regardless of the substance that patients abuse, the treatment goals are the same: to reduce use and achieve recovery. If a patient with psychosis is abusing an SGA, consider switching to an antipsychotic with less abuse potential. Another option is to limit the supply of the abused drug by prescribing smaller quantities or increase the frequency of follow-up visits to ensure compliant use.
Related Resources
- Substance Abuse and Mental Health Services Administration. www.samhsa.gov.
- Galanter M, Kelber HD. The American Psychiatric Publishing textbook of substance abuse treatment. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
Drug Brand Names
- Aripiprazole • Abilify
- Diazepam • Valium
- Haloperidol • Haldol
- Hydrocodone/acetaminophen • Vicodin
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Hussain MZ, Waheed W, Hussain S. Intravenous quetiapine abuse. Am J Psychiatry. 2005;162:1755-1756.
2. Morin AK. Possible intranasal quetiapine misuse. Am J Health Syst Pharm. 2007;64:723-725.
3. Waters BM, Joshi KG. Intravenous quetiapine-cocaine use (“Q-ball”). Am J Psychiatry. 2007;164:1.-
4. Reeves RR, Brister JC. Additional evidence of the abuse potential of quetiapine. S Med J. 2007;100:834-836.
5. Murphy D, Bailey K, Stone M, et al. Addictive potential of quetiapine. Am J Psychiatry. 2008;165:7.-
6. Fischer BA, Boggs DL. The role of antihistaminic effects in the misuse of quetiapine: a case report and review of the literature. Neurosci Biobehav Rev. 2009;34:555-558.
7. Pierre JM, Shnayder I, Wirshing DA, et al. Intranasal quetiapine abuse. Am J Psychiatry. 2004;161(9):1718.-
8. Sansone RA, Sansone LA. Is seroquel developing an illicit reputation for misuse/abuse? Psychiatry (Edgemont). 2010;7(1):13-16.
9. Tarasoff G, Osti K. Black-market value of antipsychotics antidepressants, and hypnotics in Las Vegas, Nevada. Am J Psychiatry. 2007;164:350.-
10. Keltner NL, Vance DE. Biological perspectives: incarcerated care and quetiapine abuse. Perspect Psychiatr Care. 2008;44(3):202-206.
11. Lai CH. Olanzapine abuse was relieved after switching to aripiprazole in a patient with psychotic depression. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(7):1363-1364.
12. Reeves RR. Abuse of olanzapine by substance abusers. J Psychoactive Drugs. 2007;39(3):297-299.
13. The Vaults of Erowid. Available at: . Accessed April 1 2011.
14. Hanley NJ, Kenna GA. Quetiapine: treatment for substance abuse and drug of abuse. Am J Health Syst Pharm. 2008;65:611-618.
15. Tcheremissine OV. Is quetiapine a drug of abuse? Reexamining the issue of addiction. Expert Opin Drug Saf. 2008;7:739-748.
16. Kuroki T, Nagao N, Nakahara T. Neuropharmacology of second-generation antipsychotic drugs: a validity of the serotonin-dopamine hypothesis. Prog Brain Res. 2008;172:199-212.
17. Smith JM. Abuse of the antiparkinson drugs: a review of the literature. J Clin Psychiatry. 1980;41(10):351-354.
18. Land W, Pinsky D, Salzman C. Abuse and misuse of anticholinergic medications. Hosp Community Psychiatry. 1991;42:580-581.
1. Hussain MZ, Waheed W, Hussain S. Intravenous quetiapine abuse. Am J Psychiatry. 2005;162:1755-1756.
2. Morin AK. Possible intranasal quetiapine misuse. Am J Health Syst Pharm. 2007;64:723-725.
3. Waters BM, Joshi KG. Intravenous quetiapine-cocaine use (“Q-ball”). Am J Psychiatry. 2007;164:1.-
4. Reeves RR, Brister JC. Additional evidence of the abuse potential of quetiapine. S Med J. 2007;100:834-836.
5. Murphy D, Bailey K, Stone M, et al. Addictive potential of quetiapine. Am J Psychiatry. 2008;165:7.-
6. Fischer BA, Boggs DL. The role of antihistaminic effects in the misuse of quetiapine: a case report and review of the literature. Neurosci Biobehav Rev. 2009;34:555-558.
7. Pierre JM, Shnayder I, Wirshing DA, et al. Intranasal quetiapine abuse. Am J Psychiatry. 2004;161(9):1718.-
8. Sansone RA, Sansone LA. Is seroquel developing an illicit reputation for misuse/abuse? Psychiatry (Edgemont). 2010;7(1):13-16.
9. Tarasoff G, Osti K. Black-market value of antipsychotics antidepressants, and hypnotics in Las Vegas, Nevada. Am J Psychiatry. 2007;164:350.-
10. Keltner NL, Vance DE. Biological perspectives: incarcerated care and quetiapine abuse. Perspect Psychiatr Care. 2008;44(3):202-206.
11. Lai CH. Olanzapine abuse was relieved after switching to aripiprazole in a patient with psychotic depression. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(7):1363-1364.
12. Reeves RR. Abuse of olanzapine by substance abusers. J Psychoactive Drugs. 2007;39(3):297-299.
13. The Vaults of Erowid. Available at: . Accessed April 1 2011.
14. Hanley NJ, Kenna GA. Quetiapine: treatment for substance abuse and drug of abuse. Am J Health Syst Pharm. 2008;65:611-618.
15. Tcheremissine OV. Is quetiapine a drug of abuse? Reexamining the issue of addiction. Expert Opin Drug Saf. 2008;7:739-748.
16. Kuroki T, Nagao N, Nakahara T. Neuropharmacology of second-generation antipsychotic drugs: a validity of the serotonin-dopamine hypothesis. Prog Brain Res. 2008;172:199-212.
17. Smith JM. Abuse of the antiparkinson drugs: a review of the literature. J Clin Psychiatry. 1980;41(10):351-354.
18. Land W, Pinsky D, Salzman C. Abuse and misuse of anticholinergic medications. Hosp Community Psychiatry. 1991;42:580-581.
How to prevent serotonin syndrome from drug-drug interactions
• Know which drugs are associated with serotonin syndrome.
• Understand the types of drug interactions that may precipitate serotonin syndrome and use drug information resources such as Micromedex, Lexicomp, Physicians’ Desk Reference, AHFS Drug Information, and Facts and Comparisons.
• Know what prescription medications your patient is receiving from other providers as well as any over-the-counter and illicit drugs they may be using.
Ms. B, age 22, is brought to the emergency department (ED) by her roommate for evaluation of confusion. Ms. B has a history of migraines and major depressive disorder and has been taking fluoxetine, 40 mg/d, for 1 year. A week ago, she started amitriptyline, 50 mg/d, when her migraines became more frequent. According to her roommate, Ms. B experienced a migraine early in the morning and had taken 2 doses of sumatriptan, 50 mg. She later complained of nausea and vomiting, and when her roommate returned from work that evening Ms. B was disoriented and her leg muscles would not stop twitching.
In the ED, Ms. B is diaphoretic and increasingly agitated. Blood alcohol and urine drug screens are negative. Blood glucose is 95 mg/dL. Complete blood count, basic metabolic panel, liver function, and kidney function tests are within normal limits. Her physical examination reveals a blood pressure of 130/85 mm Hg, heart rate of 130 beats per minute, respiratory rate of 21 breaths per minute, and body temperature of 38.6°C (101. 4°F). Myoclonus and hyperreflexia affect her lower extremities. Ms. B is admitted with a preliminary diagnosis of serotonin (5-HT) syndrome.
Serotonin syndrome: What is it?
Serotonin syndrome is a rare but potentially serious adverse event resulting from excess serotonergic activity at central and peripheral 5-HT2A and 5-HT1A receptors. Serotonin syndrome toxicity ranges from relatively mild to severe, and may be lethal. Symptoms develop rapidly—within hours—and may include altered mental status, clonus, tremor, hyperthermia, diaphoresis, tachycardia, mydriasis, and akathisia ( Table 1 ).1-3 Fortunately, if recognized promptly and offending agents are discontinued, serotonin syndrome often resolves within a couple of days.
The differential diagnosis includes neuroleptic malignant syndrome (NMS), anticholinergic toxicity, and malignant hyperthermia.1 Differentiating serotonin syndrome from NMS can be difficult. NMS results from dopamine blockade; however, many NMS symptoms are similar to those experienced with serotonin syndrome. Obtaining a history of recent medication and/or illicit drug use, conducting a physical exam, and evaluating the patient’s clinical course help clarify a likely diagnosis. NMS generally has a slower onset—within days—and patients demonstrate neuromuscular rigidity and bradykinesia rather than the neuromuscular hyperreactivity (myoclonus, hyperreflexia) seen with serotonin syndrome.
Table 1
Characteristics of serotonin syndrome*
| Recent addition or dose increase of a serotonergic agent |
| Tremor plus hyperreflexia |
| Muscle rigidity plus fever plus clonus |
| Spontaneous clonus |
| Ocular clonus plus agitation or diaphoresis |
| Inducible clonus plus agitation or diaphoresis |
| *A combination of these characteristics may indicate serotonin syndrome |
| Source: References 1-3 |
Interactions that increase risk
A drug interaction is a pharmacologic or clinical response to a combination of medications that differs from the agents’ known effects if given on their own. In the context of serotonin syndrome, the serotonergic activity of a drug can be increased as a result of a pharmacokinetic (PK) interaction, a pharmacodynamic (PD) interaction, or a combination of both.
PK interactions may result from the coadministration of a drug that alters absorption, distribution, metabolism, or elimination parameters of \>1 other drugs. Serotonergic antidepressants usually are metabolized by cytochrome P450 (CYP450) enzymes. Any drug that inhibits a CYP450 enzyme responsible for biotransformation of 1 of these antidepressants may increase exposure to the antidepressant and raise the risk of serotonin syndrome. CYP450 inhibitors include prescription medications as well as seemingly benign over-the-counter (OTC) drugs.
PD interactions may result from an additive or synergistic pharmacologic effect caused by coadministration of 2 agents that produce the same or similar end result. In Ms. B’s case, agents inhibiting 5-HT reuptake (fluoxetine and amitriptyline) were combined with a direct 5-HT agonist (sumatriptan). The resulting potentiation of 5-HT via 2 distinct mechanisms increased Ms. B’s risk of serotonin syndrome. Similarly, simultaneous use of 2 agents potentiating 5-HT through identical mechanisms, such as combining 2 serotonin reuptake inhibitors, also may increase the risk of serotonin syndrome ( Table 2 ).1
A combination of PK and PD interactions also may increase the risk of serotonin syndrome. For example, Ms. B is taking fluoxetine and amitriptyline for different therapeutic reasons. Both of these agents inhibit 5-HT reuptake, potentiating 5-HT. In addition, amitriptyline is a substrate for CYP2D6 and fluoxetine is a robust CYP2D6 inhibitor. The coadministration of fluoxetine with tricyclic antidepressants (TCAs) results in a 4- to 5-fold increase in TCA exposure, which may increase the risk of serotonin syndrome and other sequelae from TCA toxicity.4,5
Table 2
Drugs associated with serotonin syndrome
| Drugs that increase 5-HT release | Amphetamine, cocaine, MDMA (ecstasy), mirtazapine, phentermine, reserpine |
| Drugs that inhibit 5-HT reuptake | Amitriptyline, amphetamine, bupropion, Citalopram, clomipramine, cocaine, desipramine, dextromethorphan, doxepin, duloxetine, escitalopram, fentanyl, fluoxetine, fluvoxamine, Hypericum perforatum (St. John’s wort), imipramine, MDMA, meperidine, nefazodone, nortriptyline, paroxetine, protriptyline, sertraline, tramadol, trazodone, venlafaxine |
| Drugs that decrease 5-HT metabolism | Isocarboxazid, linezolid, phenelzine, selegiline, tranylcypromine |
| Drugs that are direct 5-HT agonists | Almotriptan, buspirone, dihydroergotamine, eletriptan, frovatriptan, LSD, naratriptan, rizatriptan, sumatriptan, zolmitriptan |
| Others | L-tryptophan, carbamazepine, carisoprodol, droperidol, levodopa, lithium, metoclopramide, pentazocine, phenylpropanolamine |
| 5-HT: serotonin; LSD: lysergic acid; MDMA: methylenedioxymethamphetamine | |
| Source: Reference 1 | |
Preventing serotonin syndrome
The warnings highlighted in drug interaction references or pharmacy databases often mean that clinicians have to evaluate whether the risk of combining medications outweighs the therapeutic benefits. It is unknown why some patients tolerate multiple agents potentiating 5-HT, and practitioners cannot predict when and in whom serotonin syndrome may occur. However, the following strategies may help minimize these risks:
Know which drugs are associated with serotonin syndrome. Concomitant use of these drugs and agents that inhibit metabolism of these drugs increases risk.
Know which drugs your patient is taking. Patients may see several prescribers, which makes it essential to ask what they are receiving from other practitioners. Also inquire about OTC and illicit drug use.
Check for interactions. If you are unfamiliar with a new drug or drug-drug combination, check multiple resources for potential interactions. The potential severity of an interaction and the detail in which interactions are described—such as class effects vs documented cases or studies—differs among drug interaction resources, which means a potential interaction may be “flagged” in 1 source but not another. Electronic resources such as Micromedex and Lexicomp often have detailed literature summaries and citations so clinicians can review primary literature that lead to the categorization of an interaction. Using multiple sources is helpful when trying to translate warnings in the context of a clinical scenario.
Weigh the risks and benefits. Prescribers know that not all treatments are benign, but not treating a condition also may be detrimental. Identify potential alternative pharmacologic or nonpharmacologic treatments when possible. Discuss the risks and benefits of drug therapy with patients.
Counsel your patients. Although it is not possible to predict who may experience serotonin syndrome, educate patients on what symptoms to look for. Instruct them to call their prescriber or pharmacist if they show symptoms that may be consistent with serotonin syndrome.
Related Resource
• MedWatch: The FDA Safety Information and Adverse Event Reporting Program. www.fda.gov/Safety/MedWatch.
Drug Brand Names
- Aripiprazole • Abilify
- Almotriptan • Axert
- Amitriptyline • Elavil
- Bupropion • Wellbutrin, Zyban
- Buspirone • BuSpar
- Carbamazepine • Carbatrol, Equetro, others
- Carisoprodol • Soma
- Citalopram • Celexa
- Desipramine • Norpramin
- Dihydroergotamine • Migranal
- Doxepin • Adapin, Silenor
- Droperidol • Inapsine
- Duloxetine • Cymbalta
- Eletriptan • Relpax
- Escitalopram • Lexapro
- Fentanyl • Sublimaze, others
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Frovatriptan • Frova
- Imipramine • Tofranil
- Isocarboxazid • Marplan
- Levodopa • Dopar, Larodopa, others
- Linezolid • Zyvox
- Lithium • Eskalith, Lithobid
- Meperidine • Demerol
- Metoclopramide • Reglan, Metozol
- Mirtazapine • Remeron
- Naratriptan • Amerge
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Paroxetine • Paxil
- Pentazocine • Talwin
- Phenelzine • Nardil
- Phentermine • Fastin, Adipex-P
- Protriptyline • Vivactil
- Reserpine • Serpasil
- Rizatriptan • Maxalt
- Selegiline • Carbex, Eldepryl, others
- Sertraline • Zoloft
- Sumatriptan • Imitrex, Alsuma
- Tramadol • Ultram, Ultracet, others
- Tranylcypromine • Parnate
- Trazodone • Desyrel, Oleptro
- Venlafaxine • Effexor
- Zolmitriptan • Zomig
Disclosures
Dr. Jeffrey Bishop receives grant/research support from Ortho-McNeil-Janssen.
Dr. Danielle Bishop reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Beyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352:1112-1120.
2. Dunkley EJ, Isbister GK, Sibbritt D, et al. The TTunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM. 2003;96:635-642.
3. Sternbach H. The serotonin syndrome. Am J Psychiatry. 1991;148:705-713.
4. Preskorn SH, Beber JH, Faul JC, et al. Serious adverse effects of combining fluoxetine and tricyclic antidepressants. Am J Psychiatry. 1990;147-532.
5. Preskorn SH, Alderman J, Chung M, et al. Pharmacokinetics of desipramine coadministered with sertraline or fluoxetine. J Clin Psychopharmacol. 1994;14:90-98.
Jeffrey R. Bishop, PharmD, BCPP
Dr. Jeffrey R. Bishop is Assistant Professor, Department of Pharmacy Practice, University of Illinois at Chicago College of Pharmacy.
Danielle L. Bishop, PharmD, BCPP
Dr. Danielle L. Bishop is Clinical Pharmacy Specialist, Department of Pharmacy, Rush University Medical Center, Chicago, IL.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Jeffrey R. Bishop, PharmD, BCPP
Dr. Jeffrey R. Bishop is Assistant Professor, Department of Pharmacy Practice, University of Illinois at Chicago College of Pharmacy.
Danielle L. Bishop, PharmD, BCPP
Dr. Danielle L. Bishop is Clinical Pharmacy Specialist, Department of Pharmacy, Rush University Medical Center, Chicago, IL.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Jeffrey R. Bishop, PharmD, BCPP
Dr. Jeffrey R. Bishop is Assistant Professor, Department of Pharmacy Practice, University of Illinois at Chicago College of Pharmacy.
Danielle L. Bishop, PharmD, BCPP
Dr. Danielle L. Bishop is Clinical Pharmacy Specialist, Department of Pharmacy, Rush University Medical Center, Chicago, IL.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
• Know which drugs are associated with serotonin syndrome.
• Understand the types of drug interactions that may precipitate serotonin syndrome and use drug information resources such as Micromedex, Lexicomp, Physicians’ Desk Reference, AHFS Drug Information, and Facts and Comparisons.
• Know what prescription medications your patient is receiving from other providers as well as any over-the-counter and illicit drugs they may be using.
Ms. B, age 22, is brought to the emergency department (ED) by her roommate for evaluation of confusion. Ms. B has a history of migraines and major depressive disorder and has been taking fluoxetine, 40 mg/d, for 1 year. A week ago, she started amitriptyline, 50 mg/d, when her migraines became more frequent. According to her roommate, Ms. B experienced a migraine early in the morning and had taken 2 doses of sumatriptan, 50 mg. She later complained of nausea and vomiting, and when her roommate returned from work that evening Ms. B was disoriented and her leg muscles would not stop twitching.
In the ED, Ms. B is diaphoretic and increasingly agitated. Blood alcohol and urine drug screens are negative. Blood glucose is 95 mg/dL. Complete blood count, basic metabolic panel, liver function, and kidney function tests are within normal limits. Her physical examination reveals a blood pressure of 130/85 mm Hg, heart rate of 130 beats per minute, respiratory rate of 21 breaths per minute, and body temperature of 38.6°C (101. 4°F). Myoclonus and hyperreflexia affect her lower extremities. Ms. B is admitted with a preliminary diagnosis of serotonin (5-HT) syndrome.
Serotonin syndrome: What is it?
Serotonin syndrome is a rare but potentially serious adverse event resulting from excess serotonergic activity at central and peripheral 5-HT2A and 5-HT1A receptors. Serotonin syndrome toxicity ranges from relatively mild to severe, and may be lethal. Symptoms develop rapidly—within hours—and may include altered mental status, clonus, tremor, hyperthermia, diaphoresis, tachycardia, mydriasis, and akathisia ( Table 1 ).1-3 Fortunately, if recognized promptly and offending agents are discontinued, serotonin syndrome often resolves within a couple of days.
The differential diagnosis includes neuroleptic malignant syndrome (NMS), anticholinergic toxicity, and malignant hyperthermia.1 Differentiating serotonin syndrome from NMS can be difficult. NMS results from dopamine blockade; however, many NMS symptoms are similar to those experienced with serotonin syndrome. Obtaining a history of recent medication and/or illicit drug use, conducting a physical exam, and evaluating the patient’s clinical course help clarify a likely diagnosis. NMS generally has a slower onset—within days—and patients demonstrate neuromuscular rigidity and bradykinesia rather than the neuromuscular hyperreactivity (myoclonus, hyperreflexia) seen with serotonin syndrome.
Table 1
Characteristics of serotonin syndrome*
| Recent addition or dose increase of a serotonergic agent |
| Tremor plus hyperreflexia |
| Muscle rigidity plus fever plus clonus |
| Spontaneous clonus |
| Ocular clonus plus agitation or diaphoresis |
| Inducible clonus plus agitation or diaphoresis |
| *A combination of these characteristics may indicate serotonin syndrome |
| Source: References 1-3 |
Interactions that increase risk
A drug interaction is a pharmacologic or clinical response to a combination of medications that differs from the agents’ known effects if given on their own. In the context of serotonin syndrome, the serotonergic activity of a drug can be increased as a result of a pharmacokinetic (PK) interaction, a pharmacodynamic (PD) interaction, or a combination of both.
PK interactions may result from the coadministration of a drug that alters absorption, distribution, metabolism, or elimination parameters of \>1 other drugs. Serotonergic antidepressants usually are metabolized by cytochrome P450 (CYP450) enzymes. Any drug that inhibits a CYP450 enzyme responsible for biotransformation of 1 of these antidepressants may increase exposure to the antidepressant and raise the risk of serotonin syndrome. CYP450 inhibitors include prescription medications as well as seemingly benign over-the-counter (OTC) drugs.
PD interactions may result from an additive or synergistic pharmacologic effect caused by coadministration of 2 agents that produce the same or similar end result. In Ms. B’s case, agents inhibiting 5-HT reuptake (fluoxetine and amitriptyline) were combined with a direct 5-HT agonist (sumatriptan). The resulting potentiation of 5-HT via 2 distinct mechanisms increased Ms. B’s risk of serotonin syndrome. Similarly, simultaneous use of 2 agents potentiating 5-HT through identical mechanisms, such as combining 2 serotonin reuptake inhibitors, also may increase the risk of serotonin syndrome ( Table 2 ).1
A combination of PK and PD interactions also may increase the risk of serotonin syndrome. For example, Ms. B is taking fluoxetine and amitriptyline for different therapeutic reasons. Both of these agents inhibit 5-HT reuptake, potentiating 5-HT. In addition, amitriptyline is a substrate for CYP2D6 and fluoxetine is a robust CYP2D6 inhibitor. The coadministration of fluoxetine with tricyclic antidepressants (TCAs) results in a 4- to 5-fold increase in TCA exposure, which may increase the risk of serotonin syndrome and other sequelae from TCA toxicity.4,5
Table 2
Drugs associated with serotonin syndrome
| Drugs that increase 5-HT release | Amphetamine, cocaine, MDMA (ecstasy), mirtazapine, phentermine, reserpine |
| Drugs that inhibit 5-HT reuptake | Amitriptyline, amphetamine, bupropion, Citalopram, clomipramine, cocaine, desipramine, dextromethorphan, doxepin, duloxetine, escitalopram, fentanyl, fluoxetine, fluvoxamine, Hypericum perforatum (St. John’s wort), imipramine, MDMA, meperidine, nefazodone, nortriptyline, paroxetine, protriptyline, sertraline, tramadol, trazodone, venlafaxine |
| Drugs that decrease 5-HT metabolism | Isocarboxazid, linezolid, phenelzine, selegiline, tranylcypromine |
| Drugs that are direct 5-HT agonists | Almotriptan, buspirone, dihydroergotamine, eletriptan, frovatriptan, LSD, naratriptan, rizatriptan, sumatriptan, zolmitriptan |
| Others | L-tryptophan, carbamazepine, carisoprodol, droperidol, levodopa, lithium, metoclopramide, pentazocine, phenylpropanolamine |
| 5-HT: serotonin; LSD: lysergic acid; MDMA: methylenedioxymethamphetamine | |
| Source: Reference 1 | |
Preventing serotonin syndrome
The warnings highlighted in drug interaction references or pharmacy databases often mean that clinicians have to evaluate whether the risk of combining medications outweighs the therapeutic benefits. It is unknown why some patients tolerate multiple agents potentiating 5-HT, and practitioners cannot predict when and in whom serotonin syndrome may occur. However, the following strategies may help minimize these risks:
Know which drugs are associated with serotonin syndrome. Concomitant use of these drugs and agents that inhibit metabolism of these drugs increases risk.
Know which drugs your patient is taking. Patients may see several prescribers, which makes it essential to ask what they are receiving from other practitioners. Also inquire about OTC and illicit drug use.
Check for interactions. If you are unfamiliar with a new drug or drug-drug combination, check multiple resources for potential interactions. The potential severity of an interaction and the detail in which interactions are described—such as class effects vs documented cases or studies—differs among drug interaction resources, which means a potential interaction may be “flagged” in 1 source but not another. Electronic resources such as Micromedex and Lexicomp often have detailed literature summaries and citations so clinicians can review primary literature that lead to the categorization of an interaction. Using multiple sources is helpful when trying to translate warnings in the context of a clinical scenario.
Weigh the risks and benefits. Prescribers know that not all treatments are benign, but not treating a condition also may be detrimental. Identify potential alternative pharmacologic or nonpharmacologic treatments when possible. Discuss the risks and benefits of drug therapy with patients.
Counsel your patients. Although it is not possible to predict who may experience serotonin syndrome, educate patients on what symptoms to look for. Instruct them to call their prescriber or pharmacist if they show symptoms that may be consistent with serotonin syndrome.
Related Resource
• MedWatch: The FDA Safety Information and Adverse Event Reporting Program. www.fda.gov/Safety/MedWatch.
Drug Brand Names
- Aripiprazole • Abilify
- Almotriptan • Axert
- Amitriptyline • Elavil
- Bupropion • Wellbutrin, Zyban
- Buspirone • BuSpar
- Carbamazepine • Carbatrol, Equetro, others
- Carisoprodol • Soma
- Citalopram • Celexa
- Desipramine • Norpramin
- Dihydroergotamine • Migranal
- Doxepin • Adapin, Silenor
- Droperidol • Inapsine
- Duloxetine • Cymbalta
- Eletriptan • Relpax
- Escitalopram • Lexapro
- Fentanyl • Sublimaze, others
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Frovatriptan • Frova
- Imipramine • Tofranil
- Isocarboxazid • Marplan
- Levodopa • Dopar, Larodopa, others
- Linezolid • Zyvox
- Lithium • Eskalith, Lithobid
- Meperidine • Demerol
- Metoclopramide • Reglan, Metozol
- Mirtazapine • Remeron
- Naratriptan • Amerge
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Paroxetine • Paxil
- Pentazocine • Talwin
- Phenelzine • Nardil
- Phentermine • Fastin, Adipex-P
- Protriptyline • Vivactil
- Reserpine • Serpasil
- Rizatriptan • Maxalt
- Selegiline • Carbex, Eldepryl, others
- Sertraline • Zoloft
- Sumatriptan • Imitrex, Alsuma
- Tramadol • Ultram, Ultracet, others
- Tranylcypromine • Parnate
- Trazodone • Desyrel, Oleptro
- Venlafaxine • Effexor
- Zolmitriptan • Zomig
Disclosures
Dr. Jeffrey Bishop receives grant/research support from Ortho-McNeil-Janssen.
Dr. Danielle Bishop reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
• Know which drugs are associated with serotonin syndrome.
• Understand the types of drug interactions that may precipitate serotonin syndrome and use drug information resources such as Micromedex, Lexicomp, Physicians’ Desk Reference, AHFS Drug Information, and Facts and Comparisons.
• Know what prescription medications your patient is receiving from other providers as well as any over-the-counter and illicit drugs they may be using.
Ms. B, age 22, is brought to the emergency department (ED) by her roommate for evaluation of confusion. Ms. B has a history of migraines and major depressive disorder and has been taking fluoxetine, 40 mg/d, for 1 year. A week ago, she started amitriptyline, 50 mg/d, when her migraines became more frequent. According to her roommate, Ms. B experienced a migraine early in the morning and had taken 2 doses of sumatriptan, 50 mg. She later complained of nausea and vomiting, and when her roommate returned from work that evening Ms. B was disoriented and her leg muscles would not stop twitching.
In the ED, Ms. B is diaphoretic and increasingly agitated. Blood alcohol and urine drug screens are negative. Blood glucose is 95 mg/dL. Complete blood count, basic metabolic panel, liver function, and kidney function tests are within normal limits. Her physical examination reveals a blood pressure of 130/85 mm Hg, heart rate of 130 beats per minute, respiratory rate of 21 breaths per minute, and body temperature of 38.6°C (101. 4°F). Myoclonus and hyperreflexia affect her lower extremities. Ms. B is admitted with a preliminary diagnosis of serotonin (5-HT) syndrome.
Serotonin syndrome: What is it?
Serotonin syndrome is a rare but potentially serious adverse event resulting from excess serotonergic activity at central and peripheral 5-HT2A and 5-HT1A receptors. Serotonin syndrome toxicity ranges from relatively mild to severe, and may be lethal. Symptoms develop rapidly—within hours—and may include altered mental status, clonus, tremor, hyperthermia, diaphoresis, tachycardia, mydriasis, and akathisia ( Table 1 ).1-3 Fortunately, if recognized promptly and offending agents are discontinued, serotonin syndrome often resolves within a couple of days.
The differential diagnosis includes neuroleptic malignant syndrome (NMS), anticholinergic toxicity, and malignant hyperthermia.1 Differentiating serotonin syndrome from NMS can be difficult. NMS results from dopamine blockade; however, many NMS symptoms are similar to those experienced with serotonin syndrome. Obtaining a history of recent medication and/or illicit drug use, conducting a physical exam, and evaluating the patient’s clinical course help clarify a likely diagnosis. NMS generally has a slower onset—within days—and patients demonstrate neuromuscular rigidity and bradykinesia rather than the neuromuscular hyperreactivity (myoclonus, hyperreflexia) seen with serotonin syndrome.
Table 1
Characteristics of serotonin syndrome*
| Recent addition or dose increase of a serotonergic agent |
| Tremor plus hyperreflexia |
| Muscle rigidity plus fever plus clonus |
| Spontaneous clonus |
| Ocular clonus plus agitation or diaphoresis |
| Inducible clonus plus agitation or diaphoresis |
| *A combination of these characteristics may indicate serotonin syndrome |
| Source: References 1-3 |
Interactions that increase risk
A drug interaction is a pharmacologic or clinical response to a combination of medications that differs from the agents’ known effects if given on their own. In the context of serotonin syndrome, the serotonergic activity of a drug can be increased as a result of a pharmacokinetic (PK) interaction, a pharmacodynamic (PD) interaction, or a combination of both.
PK interactions may result from the coadministration of a drug that alters absorption, distribution, metabolism, or elimination parameters of \>1 other drugs. Serotonergic antidepressants usually are metabolized by cytochrome P450 (CYP450) enzymes. Any drug that inhibits a CYP450 enzyme responsible for biotransformation of 1 of these antidepressants may increase exposure to the antidepressant and raise the risk of serotonin syndrome. CYP450 inhibitors include prescription medications as well as seemingly benign over-the-counter (OTC) drugs.
PD interactions may result from an additive or synergistic pharmacologic effect caused by coadministration of 2 agents that produce the same or similar end result. In Ms. B’s case, agents inhibiting 5-HT reuptake (fluoxetine and amitriptyline) were combined with a direct 5-HT agonist (sumatriptan). The resulting potentiation of 5-HT via 2 distinct mechanisms increased Ms. B’s risk of serotonin syndrome. Similarly, simultaneous use of 2 agents potentiating 5-HT through identical mechanisms, such as combining 2 serotonin reuptake inhibitors, also may increase the risk of serotonin syndrome ( Table 2 ).1
A combination of PK and PD interactions also may increase the risk of serotonin syndrome. For example, Ms. B is taking fluoxetine and amitriptyline for different therapeutic reasons. Both of these agents inhibit 5-HT reuptake, potentiating 5-HT. In addition, amitriptyline is a substrate for CYP2D6 and fluoxetine is a robust CYP2D6 inhibitor. The coadministration of fluoxetine with tricyclic antidepressants (TCAs) results in a 4- to 5-fold increase in TCA exposure, which may increase the risk of serotonin syndrome and other sequelae from TCA toxicity.4,5
Table 2
Drugs associated with serotonin syndrome
| Drugs that increase 5-HT release | Amphetamine, cocaine, MDMA (ecstasy), mirtazapine, phentermine, reserpine |
| Drugs that inhibit 5-HT reuptake | Amitriptyline, amphetamine, bupropion, Citalopram, clomipramine, cocaine, desipramine, dextromethorphan, doxepin, duloxetine, escitalopram, fentanyl, fluoxetine, fluvoxamine, Hypericum perforatum (St. John’s wort), imipramine, MDMA, meperidine, nefazodone, nortriptyline, paroxetine, protriptyline, sertraline, tramadol, trazodone, venlafaxine |
| Drugs that decrease 5-HT metabolism | Isocarboxazid, linezolid, phenelzine, selegiline, tranylcypromine |
| Drugs that are direct 5-HT agonists | Almotriptan, buspirone, dihydroergotamine, eletriptan, frovatriptan, LSD, naratriptan, rizatriptan, sumatriptan, zolmitriptan |
| Others | L-tryptophan, carbamazepine, carisoprodol, droperidol, levodopa, lithium, metoclopramide, pentazocine, phenylpropanolamine |
| 5-HT: serotonin; LSD: lysergic acid; MDMA: methylenedioxymethamphetamine | |
| Source: Reference 1 | |
Preventing serotonin syndrome
The warnings highlighted in drug interaction references or pharmacy databases often mean that clinicians have to evaluate whether the risk of combining medications outweighs the therapeutic benefits. It is unknown why some patients tolerate multiple agents potentiating 5-HT, and practitioners cannot predict when and in whom serotonin syndrome may occur. However, the following strategies may help minimize these risks:
Know which drugs are associated with serotonin syndrome. Concomitant use of these drugs and agents that inhibit metabolism of these drugs increases risk.
Know which drugs your patient is taking. Patients may see several prescribers, which makes it essential to ask what they are receiving from other practitioners. Also inquire about OTC and illicit drug use.
Check for interactions. If you are unfamiliar with a new drug or drug-drug combination, check multiple resources for potential interactions. The potential severity of an interaction and the detail in which interactions are described—such as class effects vs documented cases or studies—differs among drug interaction resources, which means a potential interaction may be “flagged” in 1 source but not another. Electronic resources such as Micromedex and Lexicomp often have detailed literature summaries and citations so clinicians can review primary literature that lead to the categorization of an interaction. Using multiple sources is helpful when trying to translate warnings in the context of a clinical scenario.
Weigh the risks and benefits. Prescribers know that not all treatments are benign, but not treating a condition also may be detrimental. Identify potential alternative pharmacologic or nonpharmacologic treatments when possible. Discuss the risks and benefits of drug therapy with patients.
Counsel your patients. Although it is not possible to predict who may experience serotonin syndrome, educate patients on what symptoms to look for. Instruct them to call their prescriber or pharmacist if they show symptoms that may be consistent with serotonin syndrome.
Related Resource
• MedWatch: The FDA Safety Information and Adverse Event Reporting Program. www.fda.gov/Safety/MedWatch.
Drug Brand Names
- Aripiprazole • Abilify
- Almotriptan • Axert
- Amitriptyline • Elavil
- Bupropion • Wellbutrin, Zyban
- Buspirone • BuSpar
- Carbamazepine • Carbatrol, Equetro, others
- Carisoprodol • Soma
- Citalopram • Celexa
- Desipramine • Norpramin
- Dihydroergotamine • Migranal
- Doxepin • Adapin, Silenor
- Droperidol • Inapsine
- Duloxetine • Cymbalta
- Eletriptan • Relpax
- Escitalopram • Lexapro
- Fentanyl • Sublimaze, others
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Frovatriptan • Frova
- Imipramine • Tofranil
- Isocarboxazid • Marplan
- Levodopa • Dopar, Larodopa, others
- Linezolid • Zyvox
- Lithium • Eskalith, Lithobid
- Meperidine • Demerol
- Metoclopramide • Reglan, Metozol
- Mirtazapine • Remeron
- Naratriptan • Amerge
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Paroxetine • Paxil
- Pentazocine • Talwin
- Phenelzine • Nardil
- Phentermine • Fastin, Adipex-P
- Protriptyline • Vivactil
- Reserpine • Serpasil
- Rizatriptan • Maxalt
- Selegiline • Carbex, Eldepryl, others
- Sertraline • Zoloft
- Sumatriptan • Imitrex, Alsuma
- Tramadol • Ultram, Ultracet, others
- Tranylcypromine • Parnate
- Trazodone • Desyrel, Oleptro
- Venlafaxine • Effexor
- Zolmitriptan • Zomig
Disclosures
Dr. Jeffrey Bishop receives grant/research support from Ortho-McNeil-Janssen.
Dr. Danielle Bishop reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Beyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352:1112-1120.
2. Dunkley EJ, Isbister GK, Sibbritt D, et al. The TTunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM. 2003;96:635-642.
3. Sternbach H. The serotonin syndrome. Am J Psychiatry. 1991;148:705-713.
4. Preskorn SH, Beber JH, Faul JC, et al. Serious adverse effects of combining fluoxetine and tricyclic antidepressants. Am J Psychiatry. 1990;147-532.
5. Preskorn SH, Alderman J, Chung M, et al. Pharmacokinetics of desipramine coadministered with sertraline or fluoxetine. J Clin Psychopharmacol. 1994;14:90-98.
1. Beyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352:1112-1120.
2. Dunkley EJ, Isbister GK, Sibbritt D, et al. The TTunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM. 2003;96:635-642.
3. Sternbach H. The serotonin syndrome. Am J Psychiatry. 1991;148:705-713.
4. Preskorn SH, Beber JH, Faul JC, et al. Serious adverse effects of combining fluoxetine and tricyclic antidepressants. Am J Psychiatry. 1990;147-532.
5. Preskorn SH, Alderman J, Chung M, et al. Pharmacokinetics of desipramine coadministered with sertraline or fluoxetine. J Clin Psychopharmacol. 1994;14:90-98.
The heart of depression: Treating patients who have cardiovascular disease
Mrs. T, age 59, sustained an ST-elevation myocardial infarction (MI) 6 weeks ago. She has a history of hypertension, hyperlipidemia, and major depressive disorder (MDD). Before her MI, Mrs. T’s MDD was well managed with cognitive-behavioral therapy (CBT). She states that her depressive symptoms have worsened since her MI, and clinicians determine that she is experiencing an acute depressive episode severe enough to require pharmacotherapy. Past medication trials for her depression include sertraline, up to 150 mg/d, and duloxetine, 60 mg/d, but her provider determined they were ineffective after an adequate trial duration. Her hypertension is well controlled on her current regimen, which includes lisinopril, 20 mg/d, metoprolol, 50 mg/d, simvastatin, 40 mg/d, and clopidogrel, 75 mg/d. Her father experienced sudden cardiac death and her mother and younger brother have a history of severe MDD.
- Selective serotonin reuptake inhibitors, particularly citalopram and sertraline, are generally well tolerated, effective, and safe to use in patients with cardiovascular disease (CVD), although clinicians must be aware of the risk of drug-drug interactions with these agents.
- Tricyclic antidepressants and monoamine oxidase inhibitors are contraindicated in patients with CVD.
- The FDA warns against using desipramine in patients with cardiovascular disease; fluoxetine and other CYP2C19 inhibitors may reduce the efficacy of clopidogrel.
- Whether pharmacologic or nonpharmacologic treatment of depression improves long-term cardiac outcomes needs to be clarified with sufficiently powered studies.
Depression is more prevalent in patients with cardiovascular disease (CVD) than in the general population, with estimates as high as 23%.1 Possible mechanisms to help explain the relationship between CVD and depression are summarized in Table 1.2 Appropriate antidepressant selection and depression management strategies in patients with CVD, particularly after MI, may reduce the risk for additional cardiac events and reduce mortality.1,2
Table 1
The link between depression and cardiovascular disease
Depressed patients with CVD often exhibit:
|
Other factors that impact cardiovascular risk in patients with depression include:
|
| CRP: C-reactive protein; CVD: cardiovascular disease; TNF: tumor necrosis factor Source: Reference 2 |
Antidepressant choices by class
Many older antidepressants, including tricyclic antidepressants (TCAs), are:
- contraindicated during acute recovery from MI
- cardiotoxic
- lethal in overdose
- not recommended for patients with CVD.1,3
The FDA recently mandated additional labeling for desipramine to alert health care providers to the risk of using this agent in patients with CVD or a family history of sudden death, arrhythmias, or conduction abnormalities.3 Similar to TCAs, monoamine oxidase inhibitors (MAOIs) generally are not recommended for use in this population because of the risk of hypertensive crisis, orthostatic hypotension, tachycardia, and increased QTc interval.2 Trazodone, which might help relieve insomnia, is associated with orthostasis and tachycardia. These effects may occur more frequently in patients with cardiac disease.4
Selective serotonin reuptake inhibitors (SSRIs) are effective antidepressants post-MI, have antiplatelet activity, and may improve surrogate markers of cardiac risk, although further research is needed.5,6 Individual SSRIs vary in their effects on the cytochrome P450 (CYP450) system, and therefore carry different risks of drug-drug interactions (see Related Resources).
The cardiovascular impact of serotonin-norepinephrine reuptake inhibitors is unknown. These agents may be associated with hypertension and tachycardia.7 Additional research on the use of bupropion and mirtazapine in patients with CVD also is warranted. However, bupropion has been used to help patients with CVD stop smoking and likely is safe, although it may be associated with an increase in blood pressure.2,7 Bupropion and mirtazapine also can affect appetite and weight, which require monitoring in CVD patients. The Myocardial Infarction and Depression-Intervention Trial (MIND-IT) reveals that antidepressant treatment with mirtazapine or citalopram does not increase the incidence of cardiac events and does not improve long-term depression status compared with treatment as usual in depressed post-MI patients.8 Orthostatic hypotension is a possible adverse effect of mirtazapine,7 and this antidepressant may reduce the antihypertensive effect of clonidine.
Monitor for interactions
Drug interaction databases—including Micromedex, Lexi-Comp, or Facts and Comparisons—can differ with regard to identifying and classifying drug interactions. Therefore, individual clinicians often carry the burden of recognizing potential drug-drug interactions. Preskorn and Flockhart9 suggest developing a “personal formulary” of the medications clinicians regularly prescribe to minimize drug-drug interactions. This formulary includes knowledge of a drug’s:
- enzymes responsible for elimination
- half-life
- relevant clinical trials
- receptor affinities
- common adverse effects.
Following these recommendations reveals several considerations when selecting an antidepressant for Mrs. T:
- Studies of SSRIs have shown them to be safe and well tolerated in post-MI patients. Because Mrs. T failed only 1 previous SSRI trial (sertraline), it would be reasonable to select an alternate agent within this class.
- An FDA alert highlights the risk of using clopidogrel in combination with drugs such as omeprazole, ketoconazole, fluoxetine, and fluvoxamine.10 These medications are CYP2C19 inhibitors, which can reduce clopidogrel’s effect by inhibiting conversion of the parent drug to its active metabolite.
- Adding a strong CYP2D6 inhibitor, such as fluoxetine or paroxetine, could increase the effects of metoprolol, which is a CYP2D6 substrate.11
Cardiac outcomes
Evidence is insufficient to ascertain whether pharmacologic management of depression can reduce the risk of future cardiac events. Data evaluating SSRIs’ effects on cardiac outcomes are equivocal5,12,13 and limited by inadequate power.14,15 Preliminary evidence suggests patients who respond to antidepressant treatment may have improved cardiovascular outcomes.16,17 Evidence obtained from the Sertraline Antidepressant Heart Attack Randomized Trial (SADHART), the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) trial, and the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial suggest the SSRIs sertraline and citalopram can be used safely, with minimal bleeding risk, to treat depression in CVD patients (Table 2).14,15,18 When treating depressed patients who have CVD, remember to include nonpharmacologic options, such as psychotherapy, in the treatment plan, although studies have not yet shown improved cardiovascular mortality rates in patients receiving CBT.8,17,18
Although other SSRIs may be helpful for Mrs. T, citalopram is one of the best-studied agents post-MI, with the CREATE study supporting its efficacy and tolerability in this population. Citalopram has negligible drug interactions, although it is a weak inhibitor of CYP2D6 and the possibility of increasing metoprolol’s effects should be monitored. All SSRIs are associated with an increased risk of bleeding in patients receiving antiplatelet therapy; however, in Mrs. T’s case the risks are minimal, which makes citalopram a reasonable option. CBT also could be resumed to optimize Mrs. T’s treatment.
Table 2
SSRIs and cardiovascular disease: Results from RCTs
| Study | Design | Results |
|---|---|---|
| SADHART14 | Randomized, double-blind trial of sertraline vs placebo for 24 weeks for depression following MI or unstable angina (N=369) | Sertraline was more effective than placebo as measured by CGI-I, but not HAM-D in the total sample; both measures demonstrated statistical significance in patients with a history of MDD and those with HAM-D score >18 with 2 past episodes of MDD; incidence of severe cardiovascular events was 14.5% with sertraline and 22.4% with placebo (P=NS) |
| ENRICHD18 | Randomized, double-blind, controlled trial of early CBT supplemented with SSRI (usually sertraline) if necessary vs usual care for depression and low perceived social support after MI (N=2,481) | Intervention had a modest effect on depressive symptoms; antidepressant use reduced the risk of death or nonfatal MI |
| CREATE15 | Randomized, controlled, 12-week, parallel-group trial of 284 depressed patients with coronary artery disease first randomized to weekly interpersonal psychotherapy for 12 weeks plus clinical management or clinical management only, then randomized to citalopram or placebo for 12 weeks | Although the effect size was small, citalopram was more effective for depression than placebo and did not differ in effect on cardiac parameters, such as blood pressure, heart rate, or ECG change (P=.005) |
| CBT: cognitive-behavioral therapy; CGI-I: Clinical Global Impressions-Improvement scale; CREATE: Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy; ENRICHD: Enhancing Recovery in Coronary Heart Disease Patients; HAM-D: Hamilton Depression Rating Scale; MDD: major depressive disorder; MI: myocardial infarction; NS: nonsignificant; RCT: randomized controlled trial; SADHART: Sertraline Antidepressant Heart Attack Randomized Trial; SSRI: selective serotonin reuptake inhibitor | ||
- Summers KM, Martin KE, Watson K. Impact and clinical management of depression in patients with coronary artery disease. Pharmacotherapy. 2010;30:304-322.
- Indiana University School of Medicine. P450 drug interaction table. Indiana University School of Medicine. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Clopidogrel • Plavix
- Desipramine • Norpramin
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Ketoconazole • Nizoral
- Lisinopril • Prinivil, Zestril
- Metoprolol • Lopressor, Toprol
- Mirtazapine • Remeron
- Omeprazole • Prilosec
- Paroxetine • Paxil
- Sertraline • Zoloft
- Simvastatin • Zocor
- Trazodone • Desyrel
Disclosure
Dr. Bostwick reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Musselman DL, Evans DL, Nemeroff CB. The relationship of depression to cardiovascular disease: epidemiology, biology, and treatment. Arch Gen Psychiatry. 1998;55:580-592.
2. Carney RM, Freedland KE. Depression in patients with coronary heart disease. Am J Med. 2008;121(11 suppl 2):S20-27.
3. Norpramin [package insert]. Bridgewater, NJ: sanofi-aventis; 2009.
4. American Psychiatric Association. Treatment of patients with major depressive disorder, 3rd ed. Available at: http://www.psychiatryonline.com/pracGuide/pracGuideChapToc_7.aspx. Accessed December 2, 2010.
5. Bush DE, Ziegelstein RC, Patel UV, et al. Post-myocardial infarction depression. Summary, evidence report/ technology assessment: number 123. Rockville, MD: Agency for Healthcare Research and Quality; May 2005. AHRQ publication 05-E018-1.
6. Roose SP, Miyazaki M. Pharmacologic treatment of depression in patients with heart disease. Psychosom Med. 2005;(67 suppl 1):S54-57.
7. Alvarez W Jr, Pickworth KK. Safety of antidepressant drugs in the patient with cardiac disease: a review of the literature. Pharmacotherapy. 2003;23:754-771.
8. van Melle JP, de Jonge P, Honig A, et al. Effects of antidepressant treatment following myocardial infarction. Br J Psychiatry. 2007;190:460-466.
9. Preskorn SH, Flockhart D. 2006 guide to psychiatric drug interactions. Primary Psychiatry. 2006;13(4):35-64.
10. U.S. Food and Drug Administration. Information for healthcare professionals: update to the labeling of clopidogrel bisulfate (marketed as Plavix) to alert healthcare professionals about a drug interaction with omeprazole (marketed as Prilosec and Prilosec OTC). Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/
DrugSafetyInformationforHeathcareProfessionals/ucm190787.htm. Accessed January 24, 2010.
11. Spina E, Santoro V, D’Arrigo C. Clinically relevant pharmacokinetic drug interactions with second-generation antidepressants: an update. Clin Ther. 2008;30:1206-1227.
12. Von Ruden AE, Adson DE, Kotlyar M. Effect of selective serotonin reuptake inhibitors on cardiovascular morbidity and mortality. J Cardiovasc Pharmacol Ther. 2008;13(1):32-40.
13. Glassman A. Depression and cardiovascular disease. Pharmacopsychiatry. 2008;41(6):221-225.
14. Glassman AH, O’Connor CM, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA. 2002;288:701-709.
15. Lespérance F, Frasure-Smith N, Koszycki D, et al. Effects of citalopram and interpersonal psychotherapy on depression in patients with coronary artery disease: the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial. JAMA. 2007;297:367-379.
16. de Jonge P, Honig A, van Melle JP, et al. Nonresponse to treatment for depression following myocardial infarction: association with subsequent cardiac events. Am J Psychiatry. 2007;164:1371-1378.
17. Summers KM, Martin KE, Watson K. Impact and clinical management of depression in patients with coronary artery disease. Pharmacotherapy. 2010;30:304-322.
18. Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA 2003;289:3106-3116.
Jolene Bostwick, PharmD, BCPS, BCPP
Dr. Bostwick is Clinical Assistant Professor of Pharmacy at the University of Michigan College of Pharmacy and Clinical Pharmacist at the University of Michigan Health System, Ann Arbor, MI.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Jolene Bostwick, PharmD, BCPS, BCPP
Dr. Bostwick is Clinical Assistant Professor of Pharmacy at the University of Michigan College of Pharmacy and Clinical Pharmacist at the University of Michigan Health System, Ann Arbor, MI.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Jolene Bostwick, PharmD, BCPS, BCPP
Dr. Bostwick is Clinical Assistant Professor of Pharmacy at the University of Michigan College of Pharmacy and Clinical Pharmacist at the University of Michigan Health System, Ann Arbor, MI.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Mrs. T, age 59, sustained an ST-elevation myocardial infarction (MI) 6 weeks ago. She has a history of hypertension, hyperlipidemia, and major depressive disorder (MDD). Before her MI, Mrs. T’s MDD was well managed with cognitive-behavioral therapy (CBT). She states that her depressive symptoms have worsened since her MI, and clinicians determine that she is experiencing an acute depressive episode severe enough to require pharmacotherapy. Past medication trials for her depression include sertraline, up to 150 mg/d, and duloxetine, 60 mg/d, but her provider determined they were ineffective after an adequate trial duration. Her hypertension is well controlled on her current regimen, which includes lisinopril, 20 mg/d, metoprolol, 50 mg/d, simvastatin, 40 mg/d, and clopidogrel, 75 mg/d. Her father experienced sudden cardiac death and her mother and younger brother have a history of severe MDD.
- Selective serotonin reuptake inhibitors, particularly citalopram and sertraline, are generally well tolerated, effective, and safe to use in patients with cardiovascular disease (CVD), although clinicians must be aware of the risk of drug-drug interactions with these agents.
- Tricyclic antidepressants and monoamine oxidase inhibitors are contraindicated in patients with CVD.
- The FDA warns against using desipramine in patients with cardiovascular disease; fluoxetine and other CYP2C19 inhibitors may reduce the efficacy of clopidogrel.
- Whether pharmacologic or nonpharmacologic treatment of depression improves long-term cardiac outcomes needs to be clarified with sufficiently powered studies.
Depression is more prevalent in patients with cardiovascular disease (CVD) than in the general population, with estimates as high as 23%.1 Possible mechanisms to help explain the relationship between CVD and depression are summarized in Table 1.2 Appropriate antidepressant selection and depression management strategies in patients with CVD, particularly after MI, may reduce the risk for additional cardiac events and reduce mortality.1,2
Table 1
The link between depression and cardiovascular disease
Depressed patients with CVD often exhibit:
|
Other factors that impact cardiovascular risk in patients with depression include:
|
| CRP: C-reactive protein; CVD: cardiovascular disease; TNF: tumor necrosis factor Source: Reference 2 |
Antidepressant choices by class
Many older antidepressants, including tricyclic antidepressants (TCAs), are:
- contraindicated during acute recovery from MI
- cardiotoxic
- lethal in overdose
- not recommended for patients with CVD.1,3
The FDA recently mandated additional labeling for desipramine to alert health care providers to the risk of using this agent in patients with CVD or a family history of sudden death, arrhythmias, or conduction abnormalities.3 Similar to TCAs, monoamine oxidase inhibitors (MAOIs) generally are not recommended for use in this population because of the risk of hypertensive crisis, orthostatic hypotension, tachycardia, and increased QTc interval.2 Trazodone, which might help relieve insomnia, is associated with orthostasis and tachycardia. These effects may occur more frequently in patients with cardiac disease.4
Selective serotonin reuptake inhibitors (SSRIs) are effective antidepressants post-MI, have antiplatelet activity, and may improve surrogate markers of cardiac risk, although further research is needed.5,6 Individual SSRIs vary in their effects on the cytochrome P450 (CYP450) system, and therefore carry different risks of drug-drug interactions (see Related Resources).
The cardiovascular impact of serotonin-norepinephrine reuptake inhibitors is unknown. These agents may be associated with hypertension and tachycardia.7 Additional research on the use of bupropion and mirtazapine in patients with CVD also is warranted. However, bupropion has been used to help patients with CVD stop smoking and likely is safe, although it may be associated with an increase in blood pressure.2,7 Bupropion and mirtazapine also can affect appetite and weight, which require monitoring in CVD patients. The Myocardial Infarction and Depression-Intervention Trial (MIND-IT) reveals that antidepressant treatment with mirtazapine or citalopram does not increase the incidence of cardiac events and does not improve long-term depression status compared with treatment as usual in depressed post-MI patients.8 Orthostatic hypotension is a possible adverse effect of mirtazapine,7 and this antidepressant may reduce the antihypertensive effect of clonidine.
Monitor for interactions
Drug interaction databases—including Micromedex, Lexi-Comp, or Facts and Comparisons—can differ with regard to identifying and classifying drug interactions. Therefore, individual clinicians often carry the burden of recognizing potential drug-drug interactions. Preskorn and Flockhart9 suggest developing a “personal formulary” of the medications clinicians regularly prescribe to minimize drug-drug interactions. This formulary includes knowledge of a drug’s:
- enzymes responsible for elimination
- half-life
- relevant clinical trials
- receptor affinities
- common adverse effects.
Following these recommendations reveals several considerations when selecting an antidepressant for Mrs. T:
- Studies of SSRIs have shown them to be safe and well tolerated in post-MI patients. Because Mrs. T failed only 1 previous SSRI trial (sertraline), it would be reasonable to select an alternate agent within this class.
- An FDA alert highlights the risk of using clopidogrel in combination with drugs such as omeprazole, ketoconazole, fluoxetine, and fluvoxamine.10 These medications are CYP2C19 inhibitors, which can reduce clopidogrel’s effect by inhibiting conversion of the parent drug to its active metabolite.
- Adding a strong CYP2D6 inhibitor, such as fluoxetine or paroxetine, could increase the effects of metoprolol, which is a CYP2D6 substrate.11
Cardiac outcomes
Evidence is insufficient to ascertain whether pharmacologic management of depression can reduce the risk of future cardiac events. Data evaluating SSRIs’ effects on cardiac outcomes are equivocal5,12,13 and limited by inadequate power.14,15 Preliminary evidence suggests patients who respond to antidepressant treatment may have improved cardiovascular outcomes.16,17 Evidence obtained from the Sertraline Antidepressant Heart Attack Randomized Trial (SADHART), the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) trial, and the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial suggest the SSRIs sertraline and citalopram can be used safely, with minimal bleeding risk, to treat depression in CVD patients (Table 2).14,15,18 When treating depressed patients who have CVD, remember to include nonpharmacologic options, such as psychotherapy, in the treatment plan, although studies have not yet shown improved cardiovascular mortality rates in patients receiving CBT.8,17,18
Although other SSRIs may be helpful for Mrs. T, citalopram is one of the best-studied agents post-MI, with the CREATE study supporting its efficacy and tolerability in this population. Citalopram has negligible drug interactions, although it is a weak inhibitor of CYP2D6 and the possibility of increasing metoprolol’s effects should be monitored. All SSRIs are associated with an increased risk of bleeding in patients receiving antiplatelet therapy; however, in Mrs. T’s case the risks are minimal, which makes citalopram a reasonable option. CBT also could be resumed to optimize Mrs. T’s treatment.
Table 2
SSRIs and cardiovascular disease: Results from RCTs
| Study | Design | Results |
|---|---|---|
| SADHART14 | Randomized, double-blind trial of sertraline vs placebo for 24 weeks for depression following MI or unstable angina (N=369) | Sertraline was more effective than placebo as measured by CGI-I, but not HAM-D in the total sample; both measures demonstrated statistical significance in patients with a history of MDD and those with HAM-D score >18 with 2 past episodes of MDD; incidence of severe cardiovascular events was 14.5% with sertraline and 22.4% with placebo (P=NS) |
| ENRICHD18 | Randomized, double-blind, controlled trial of early CBT supplemented with SSRI (usually sertraline) if necessary vs usual care for depression and low perceived social support after MI (N=2,481) | Intervention had a modest effect on depressive symptoms; antidepressant use reduced the risk of death or nonfatal MI |
| CREATE15 | Randomized, controlled, 12-week, parallel-group trial of 284 depressed patients with coronary artery disease first randomized to weekly interpersonal psychotherapy for 12 weeks plus clinical management or clinical management only, then randomized to citalopram or placebo for 12 weeks | Although the effect size was small, citalopram was more effective for depression than placebo and did not differ in effect on cardiac parameters, such as blood pressure, heart rate, or ECG change (P=.005) |
| CBT: cognitive-behavioral therapy; CGI-I: Clinical Global Impressions-Improvement scale; CREATE: Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy; ENRICHD: Enhancing Recovery in Coronary Heart Disease Patients; HAM-D: Hamilton Depression Rating Scale; MDD: major depressive disorder; MI: myocardial infarction; NS: nonsignificant; RCT: randomized controlled trial; SADHART: Sertraline Antidepressant Heart Attack Randomized Trial; SSRI: selective serotonin reuptake inhibitor | ||
- Summers KM, Martin KE, Watson K. Impact and clinical management of depression in patients with coronary artery disease. Pharmacotherapy. 2010;30:304-322.
- Indiana University School of Medicine. P450 drug interaction table. Indiana University School of Medicine. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Clopidogrel • Plavix
- Desipramine • Norpramin
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Ketoconazole • Nizoral
- Lisinopril • Prinivil, Zestril
- Metoprolol • Lopressor, Toprol
- Mirtazapine • Remeron
- Omeprazole • Prilosec
- Paroxetine • Paxil
- Sertraline • Zoloft
- Simvastatin • Zocor
- Trazodone • Desyrel
Disclosure
Dr. Bostwick reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mrs. T, age 59, sustained an ST-elevation myocardial infarction (MI) 6 weeks ago. She has a history of hypertension, hyperlipidemia, and major depressive disorder (MDD). Before her MI, Mrs. T’s MDD was well managed with cognitive-behavioral therapy (CBT). She states that her depressive symptoms have worsened since her MI, and clinicians determine that she is experiencing an acute depressive episode severe enough to require pharmacotherapy. Past medication trials for her depression include sertraline, up to 150 mg/d, and duloxetine, 60 mg/d, but her provider determined they were ineffective after an adequate trial duration. Her hypertension is well controlled on her current regimen, which includes lisinopril, 20 mg/d, metoprolol, 50 mg/d, simvastatin, 40 mg/d, and clopidogrel, 75 mg/d. Her father experienced sudden cardiac death and her mother and younger brother have a history of severe MDD.
- Selective serotonin reuptake inhibitors, particularly citalopram and sertraline, are generally well tolerated, effective, and safe to use in patients with cardiovascular disease (CVD), although clinicians must be aware of the risk of drug-drug interactions with these agents.
- Tricyclic antidepressants and monoamine oxidase inhibitors are contraindicated in patients with CVD.
- The FDA warns against using desipramine in patients with cardiovascular disease; fluoxetine and other CYP2C19 inhibitors may reduce the efficacy of clopidogrel.
- Whether pharmacologic or nonpharmacologic treatment of depression improves long-term cardiac outcomes needs to be clarified with sufficiently powered studies.
Depression is more prevalent in patients with cardiovascular disease (CVD) than in the general population, with estimates as high as 23%.1 Possible mechanisms to help explain the relationship between CVD and depression are summarized in Table 1.2 Appropriate antidepressant selection and depression management strategies in patients with CVD, particularly after MI, may reduce the risk for additional cardiac events and reduce mortality.1,2
Table 1
The link between depression and cardiovascular disease
Depressed patients with CVD often exhibit:
|
Other factors that impact cardiovascular risk in patients with depression include:
|
| CRP: C-reactive protein; CVD: cardiovascular disease; TNF: tumor necrosis factor Source: Reference 2 |
Antidepressant choices by class
Many older antidepressants, including tricyclic antidepressants (TCAs), are:
- contraindicated during acute recovery from MI
- cardiotoxic
- lethal in overdose
- not recommended for patients with CVD.1,3
The FDA recently mandated additional labeling for desipramine to alert health care providers to the risk of using this agent in patients with CVD or a family history of sudden death, arrhythmias, or conduction abnormalities.3 Similar to TCAs, monoamine oxidase inhibitors (MAOIs) generally are not recommended for use in this population because of the risk of hypertensive crisis, orthostatic hypotension, tachycardia, and increased QTc interval.2 Trazodone, which might help relieve insomnia, is associated with orthostasis and tachycardia. These effects may occur more frequently in patients with cardiac disease.4
Selective serotonin reuptake inhibitors (SSRIs) are effective antidepressants post-MI, have antiplatelet activity, and may improve surrogate markers of cardiac risk, although further research is needed.5,6 Individual SSRIs vary in their effects on the cytochrome P450 (CYP450) system, and therefore carry different risks of drug-drug interactions (see Related Resources).
The cardiovascular impact of serotonin-norepinephrine reuptake inhibitors is unknown. These agents may be associated with hypertension and tachycardia.7 Additional research on the use of bupropion and mirtazapine in patients with CVD also is warranted. However, bupropion has been used to help patients with CVD stop smoking and likely is safe, although it may be associated with an increase in blood pressure.2,7 Bupropion and mirtazapine also can affect appetite and weight, which require monitoring in CVD patients. The Myocardial Infarction and Depression-Intervention Trial (MIND-IT) reveals that antidepressant treatment with mirtazapine or citalopram does not increase the incidence of cardiac events and does not improve long-term depression status compared with treatment as usual in depressed post-MI patients.8 Orthostatic hypotension is a possible adverse effect of mirtazapine,7 and this antidepressant may reduce the antihypertensive effect of clonidine.
Monitor for interactions
Drug interaction databases—including Micromedex, Lexi-Comp, or Facts and Comparisons—can differ with regard to identifying and classifying drug interactions. Therefore, individual clinicians often carry the burden of recognizing potential drug-drug interactions. Preskorn and Flockhart9 suggest developing a “personal formulary” of the medications clinicians regularly prescribe to minimize drug-drug interactions. This formulary includes knowledge of a drug’s:
- enzymes responsible for elimination
- half-life
- relevant clinical trials
- receptor affinities
- common adverse effects.
Following these recommendations reveals several considerations when selecting an antidepressant for Mrs. T:
- Studies of SSRIs have shown them to be safe and well tolerated in post-MI patients. Because Mrs. T failed only 1 previous SSRI trial (sertraline), it would be reasonable to select an alternate agent within this class.
- An FDA alert highlights the risk of using clopidogrel in combination with drugs such as omeprazole, ketoconazole, fluoxetine, and fluvoxamine.10 These medications are CYP2C19 inhibitors, which can reduce clopidogrel’s effect by inhibiting conversion of the parent drug to its active metabolite.
- Adding a strong CYP2D6 inhibitor, such as fluoxetine or paroxetine, could increase the effects of metoprolol, which is a CYP2D6 substrate.11
Cardiac outcomes
Evidence is insufficient to ascertain whether pharmacologic management of depression can reduce the risk of future cardiac events. Data evaluating SSRIs’ effects on cardiac outcomes are equivocal5,12,13 and limited by inadequate power.14,15 Preliminary evidence suggests patients who respond to antidepressant treatment may have improved cardiovascular outcomes.16,17 Evidence obtained from the Sertraline Antidepressant Heart Attack Randomized Trial (SADHART), the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) trial, and the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial suggest the SSRIs sertraline and citalopram can be used safely, with minimal bleeding risk, to treat depression in CVD patients (Table 2).14,15,18 When treating depressed patients who have CVD, remember to include nonpharmacologic options, such as psychotherapy, in the treatment plan, although studies have not yet shown improved cardiovascular mortality rates in patients receiving CBT.8,17,18
Although other SSRIs may be helpful for Mrs. T, citalopram is one of the best-studied agents post-MI, with the CREATE study supporting its efficacy and tolerability in this population. Citalopram has negligible drug interactions, although it is a weak inhibitor of CYP2D6 and the possibility of increasing metoprolol’s effects should be monitored. All SSRIs are associated with an increased risk of bleeding in patients receiving antiplatelet therapy; however, in Mrs. T’s case the risks are minimal, which makes citalopram a reasonable option. CBT also could be resumed to optimize Mrs. T’s treatment.
Table 2
SSRIs and cardiovascular disease: Results from RCTs
| Study | Design | Results |
|---|---|---|
| SADHART14 | Randomized, double-blind trial of sertraline vs placebo for 24 weeks for depression following MI or unstable angina (N=369) | Sertraline was more effective than placebo as measured by CGI-I, but not HAM-D in the total sample; both measures demonstrated statistical significance in patients with a history of MDD and those with HAM-D score >18 with 2 past episodes of MDD; incidence of severe cardiovascular events was 14.5% with sertraline and 22.4% with placebo (P=NS) |
| ENRICHD18 | Randomized, double-blind, controlled trial of early CBT supplemented with SSRI (usually sertraline) if necessary vs usual care for depression and low perceived social support after MI (N=2,481) | Intervention had a modest effect on depressive symptoms; antidepressant use reduced the risk of death or nonfatal MI |
| CREATE15 | Randomized, controlled, 12-week, parallel-group trial of 284 depressed patients with coronary artery disease first randomized to weekly interpersonal psychotherapy for 12 weeks plus clinical management or clinical management only, then randomized to citalopram or placebo for 12 weeks | Although the effect size was small, citalopram was more effective for depression than placebo and did not differ in effect on cardiac parameters, such as blood pressure, heart rate, or ECG change (P=.005) |
| CBT: cognitive-behavioral therapy; CGI-I: Clinical Global Impressions-Improvement scale; CREATE: Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy; ENRICHD: Enhancing Recovery in Coronary Heart Disease Patients; HAM-D: Hamilton Depression Rating Scale; MDD: major depressive disorder; MI: myocardial infarction; NS: nonsignificant; RCT: randomized controlled trial; SADHART: Sertraline Antidepressant Heart Attack Randomized Trial; SSRI: selective serotonin reuptake inhibitor | ||
- Summers KM, Martin KE, Watson K. Impact and clinical management of depression in patients with coronary artery disease. Pharmacotherapy. 2010;30:304-322.
- Indiana University School of Medicine. P450 drug interaction table. Indiana University School of Medicine. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Clopidogrel • Plavix
- Desipramine • Norpramin
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Ketoconazole • Nizoral
- Lisinopril • Prinivil, Zestril
- Metoprolol • Lopressor, Toprol
- Mirtazapine • Remeron
- Omeprazole • Prilosec
- Paroxetine • Paxil
- Sertraline • Zoloft
- Simvastatin • Zocor
- Trazodone • Desyrel
Disclosure
Dr. Bostwick reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Musselman DL, Evans DL, Nemeroff CB. The relationship of depression to cardiovascular disease: epidemiology, biology, and treatment. Arch Gen Psychiatry. 1998;55:580-592.
2. Carney RM, Freedland KE. Depression in patients with coronary heart disease. Am J Med. 2008;121(11 suppl 2):S20-27.
3. Norpramin [package insert]. Bridgewater, NJ: sanofi-aventis; 2009.
4. American Psychiatric Association. Treatment of patients with major depressive disorder, 3rd ed. Available at: http://www.psychiatryonline.com/pracGuide/pracGuideChapToc_7.aspx. Accessed December 2, 2010.
5. Bush DE, Ziegelstein RC, Patel UV, et al. Post-myocardial infarction depression. Summary, evidence report/ technology assessment: number 123. Rockville, MD: Agency for Healthcare Research and Quality; May 2005. AHRQ publication 05-E018-1.
6. Roose SP, Miyazaki M. Pharmacologic treatment of depression in patients with heart disease. Psychosom Med. 2005;(67 suppl 1):S54-57.
7. Alvarez W Jr, Pickworth KK. Safety of antidepressant drugs in the patient with cardiac disease: a review of the literature. Pharmacotherapy. 2003;23:754-771.
8. van Melle JP, de Jonge P, Honig A, et al. Effects of antidepressant treatment following myocardial infarction. Br J Psychiatry. 2007;190:460-466.
9. Preskorn SH, Flockhart D. 2006 guide to psychiatric drug interactions. Primary Psychiatry. 2006;13(4):35-64.
10. U.S. Food and Drug Administration. Information for healthcare professionals: update to the labeling of clopidogrel bisulfate (marketed as Plavix) to alert healthcare professionals about a drug interaction with omeprazole (marketed as Prilosec and Prilosec OTC). Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/
DrugSafetyInformationforHeathcareProfessionals/ucm190787.htm. Accessed January 24, 2010.
11. Spina E, Santoro V, D’Arrigo C. Clinically relevant pharmacokinetic drug interactions with second-generation antidepressants: an update. Clin Ther. 2008;30:1206-1227.
12. Von Ruden AE, Adson DE, Kotlyar M. Effect of selective serotonin reuptake inhibitors on cardiovascular morbidity and mortality. J Cardiovasc Pharmacol Ther. 2008;13(1):32-40.
13. Glassman A. Depression and cardiovascular disease. Pharmacopsychiatry. 2008;41(6):221-225.
14. Glassman AH, O’Connor CM, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA. 2002;288:701-709.
15. Lespérance F, Frasure-Smith N, Koszycki D, et al. Effects of citalopram and interpersonal psychotherapy on depression in patients with coronary artery disease: the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial. JAMA. 2007;297:367-379.
16. de Jonge P, Honig A, van Melle JP, et al. Nonresponse to treatment for depression following myocardial infarction: association with subsequent cardiac events. Am J Psychiatry. 2007;164:1371-1378.
17. Summers KM, Martin KE, Watson K. Impact and clinical management of depression in patients with coronary artery disease. Pharmacotherapy. 2010;30:304-322.
18. Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA 2003;289:3106-3116.
1. Musselman DL, Evans DL, Nemeroff CB. The relationship of depression to cardiovascular disease: epidemiology, biology, and treatment. Arch Gen Psychiatry. 1998;55:580-592.
2. Carney RM, Freedland KE. Depression in patients with coronary heart disease. Am J Med. 2008;121(11 suppl 2):S20-27.
3. Norpramin [package insert]. Bridgewater, NJ: sanofi-aventis; 2009.
4. American Psychiatric Association. Treatment of patients with major depressive disorder, 3rd ed. Available at: http://www.psychiatryonline.com/pracGuide/pracGuideChapToc_7.aspx. Accessed December 2, 2010.
5. Bush DE, Ziegelstein RC, Patel UV, et al. Post-myocardial infarction depression. Summary, evidence report/ technology assessment: number 123. Rockville, MD: Agency for Healthcare Research and Quality; May 2005. AHRQ publication 05-E018-1.
6. Roose SP, Miyazaki M. Pharmacologic treatment of depression in patients with heart disease. Psychosom Med. 2005;(67 suppl 1):S54-57.
7. Alvarez W Jr, Pickworth KK. Safety of antidepressant drugs in the patient with cardiac disease: a review of the literature. Pharmacotherapy. 2003;23:754-771.
8. van Melle JP, de Jonge P, Honig A, et al. Effects of antidepressant treatment following myocardial infarction. Br J Psychiatry. 2007;190:460-466.
9. Preskorn SH, Flockhart D. 2006 guide to psychiatric drug interactions. Primary Psychiatry. 2006;13(4):35-64.
10. U.S. Food and Drug Administration. Information for healthcare professionals: update to the labeling of clopidogrel bisulfate (marketed as Plavix) to alert healthcare professionals about a drug interaction with omeprazole (marketed as Prilosec and Prilosec OTC). Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/
DrugSafetyInformationforHeathcareProfessionals/ucm190787.htm. Accessed January 24, 2010.
11. Spina E, Santoro V, D’Arrigo C. Clinically relevant pharmacokinetic drug interactions with second-generation antidepressants: an update. Clin Ther. 2008;30:1206-1227.
12. Von Ruden AE, Adson DE, Kotlyar M. Effect of selective serotonin reuptake inhibitors on cardiovascular morbidity and mortality. J Cardiovasc Pharmacol Ther. 2008;13(1):32-40.
13. Glassman A. Depression and cardiovascular disease. Pharmacopsychiatry. 2008;41(6):221-225.
14. Glassman AH, O’Connor CM, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA. 2002;288:701-709.
15. Lespérance F, Frasure-Smith N, Koszycki D, et al. Effects of citalopram and interpersonal psychotherapy on depression in patients with coronary artery disease: the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial. JAMA. 2007;297:367-379.
16. de Jonge P, Honig A, van Melle JP, et al. Nonresponse to treatment for depression following myocardial infarction: association with subsequent cardiac events. Am J Psychiatry. 2007;164:1371-1378.
17. Summers KM, Martin KE, Watson K. Impact and clinical management of depression in patients with coronary artery disease. Pharmacotherapy. 2010;30:304-322.
18. Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA 2003;289:3106-3116.
Antidepressants in geriatric patients: Reduce the risk of GI bleeding
Mr. M, age 70, presents to the emergency department (ED) complaining of new-onset fatigue, dizziness, and black, tarry stools. He is anemic (hemoglobin 8.9 g/dL) and his stool is positive for occult blood. Mr. M denies having any symptoms until 1 week ago and reports taking his medications as prescribed. An upper endoscopy reveals a gastrointestinal (GI) bleed and his physician stops his antiplatelet medications. Mr. M’s medical history includes hypertension, hyperlipidemia, and placement of a drug-eluding coronary artery stent 9 months ago. Before presenting to the ED, he had been maintained on lisinopril, 20 mg/d, simvastatin, 40 mg/d, aspirin, 325 mg/d, clopidogrel, 75 mg/d, and a daily multivitamin. Three weeks ago, Mr. M was started on citalopram, 20 mg/d, for depressed mood that he has had since his wife died a year ago.
The psychiatry service is consulted after Mr. M admits he has had thoughts of suicide and a few weeks ago was planning to take an overdose of his medications. He denies taking any extra medications and reports feeling more positive since starting citalopram. The psychiatrist discontinues citalopram, however, because of a possible drug interaction with antiplatelet medications, starts Mr. M on bupropion, 150 mg/d, and recommends he follow up with his primary care physician for management of his depressive symptoms.
- Geriatric patients who take multiple medications for various disease states are at increased risk for drug-drug interactions.
- Serotonergic antidepressants inhibit platelet aggregation, which may increase a patient’s risk of bleeding or bruising.
- Closely monitor patients receiving serotonergic antidepressants concomitantly with other medications that may increase bleeding risk.
- Consider prophylactic acid suppressive therapy for patients at high risk for GI bleeding who receive concomitant SSRIs.
Older patients frequently take multiple medications for various disease states, which increases their risk of drug-drug interactions. In addition, physiologic changes associated with aging alter how patients respond to medications. Drugs may interact pharmacokinetically and pharmacodynamically. Pharmacokinetic interactions are well understood and represent changes in absorption, distribution, metabolism, and elimination of specific medications. Pharmacodynamic drug-drug interactions, on the other hand, are less recognized and represent changes in medications’ mechanism of action. A clinician who understands pharmacodynamic interactions will be able to better identify potential drug-drug interactions and could avoid adverse events.1
Antidepressants and bleeding
In Mr. M’s case, a pharmacodynamic drug-drug interaction among citalopram, aspirin, and clopidogrel caused a GI bleed. This type of interaction may be overlooked because of the relatively safe drug-drug interaction profile of selective serotonin reuptake inhibitors (SSRIs). However, any antidepressant that increases serotonin concentration, including serotonin-norepinephrine reuptake inhibitors, may cause this pharmacodynamic interaction.1
Platelets release serotonin to promote aggregation, but do not produce it themselves and are dependent on the serotonin transporter system (reuptake pump) to acquire serotonin. Because SSRIs act on serotonin transporters found on platelet cell membranes, these drugs deplete platelets’ supply of serotonin, leading to diminished platelet aggregation. This effect may propagate the action of other medications that inhibit platelet aggregation, which may increase a patient’s risk of bruising and/or bleeding. This increased risk of bleeding is not associated with non-serotonergic antidepressants such as bupropion, and seems to decrease when SSRIs are discontinued.2
A modest increase in bleeding risk with SSRIs when used alone and with other platelet-inhibiting therapies has been described in case reports, case controlled studies, and chart reviews.2-4 The agents studied include aspirin and clopidogrel, which Mr. M was receiving, but also other, often-overlooked medications, including nonsteroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase-2 inhibitors, calcium channel blockers, and systemic corticosteroids. Patient factors and diseases—including a history of peptic ulcer disease, previous bleeding, heavy alcohol use, and older age—also may increase bleeding risk (Table).2-5
Serotonin reuptake inhibitor medications have been associated with various bleeding events.5 Most case-control and cohort analyses have examined the risk of GI bleeding with SSRIs; however, serotonergic antidepressants also have been associated with an increased risk of uterine bleeding and perioperative blood loss and transfusions in various surgical procedures.6 Some reports have suggested that there may be a small increase in the incidence of hemorrhagic and fatal stroke with SSRI use5,7; however, many studies have not found an association between SSRI use and increased risk of intracranial hemorrhage stroke.8 The Women’s Health Initiative Study, which reviewed cardiovascular morbidity and mortality data, showed that antidepressant use in postmenopausal women was associated with an increased risk of all-cause mortality, but not coronary heart disease.7 SSRI use was associated with an increased risk of stroke, specifically hemorrhagic stroke, although the absolute event risks were low and cannot be used to predict risk.
Table
Risk factors for gastrointestinal bleeding
| Medications | Corticosteroids, anticoagulants (warfarin), antiplatelets (clopidogrel), NSAIDs (including aspirin), calcium channel blockers, SSRIs, SNRIs, tricyclic antidepressants |
| Disease state/patient factors | Age (elderly are at higher risk), history of ulcer, chronic alcohol use, peptic ulcer disease, esophageal varices, gastric or colorectal cancer, gastritis, liver disease, coagulopathy |
| NSAIDs: nonsteroidal anti-inflammatory drugs; SNRIs: serotonin-norepinephrine reuptake inhibitors; SSRIs: selective serotonin reuptake inhibitors | |
| Source: References 2-5 | |
Reducing bleeding risk
In a case-control study, de Abajo et al4 found that patients taking acid-suppressing drugs—proton pump inhibitors and histamine H2 receptor antagonists—had a lower risk of upper GI tract bleeding associated with serotonergic antidepressants compared with those not taking acid-suppressing medications. These drugs further reduced the risk of bleeding in patients taking NSAIDs or antiplatelet medications concomitantly with SSRIs. We suggest initiating prophylactic acid suppression therapy for any patient who is considered at high risk for a GI bleed and is taking an SSRI with or without other medications that inhibit platelet aggregation. Specifically, start with an H2 antagonist because of these medications’ faster onset of action and lower cost vs proton pump inhibitors.
Although the association between SSRIs and bleeding have been described in observational studies, it is impossible to rule out alternate causes and potential confounders that may have contributed to these events. Due diligence and therapeutic drug monitoring of all known and predicted drug-drug interactions is warranted for all patients taking serotonergic antidepressants in combination with medications known to increase bleeding risk.
Related Resources
- Indiana University School of Medicine. P450 drug interaction table. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
- Hansten PD, Horn JR. The top 100 drug interactions: a guide to patient management. Edmonds, WA: H&H Publications; 2010.
Drug Brand Names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Clopidogrel • Plavix
- Lisinopril • Zestril, Prinivil
- Simvastatin • Zocor
- Warfarin • Coumadin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kutscher EC, Alexander B. A review of drug interactions with psychiatric medicines for the pharmacy practitioner. J Pharm Pract. 2007;20(4):327-333.
2. Targownik LE, Bolton JM, Metge CJ, et al. Selective serotonin reuptake inhibitors are associated with a modest increase in the risk of upper gastrointestinal bleeding. Am J Gastroenterol. 2009;104:1475-1482.
3. Opatrny L, Delaney JA, Suissa S. Gastro-intestinal haemorrhage risks of selective serotonin receptor antagonist therapy: a new look. Br J Clin Pharmacol. 2008;66(1):76-81.
4. de Abajo FJ, García-Rodríguez LA. Risk of upper gastrointestinal tract bleeding associated with selective serotonin reuptake inhibitors and venlafaxine therapy: interaction with nonsteroidal anti-inflammatory drugs and effect of acid-suppressing agents. Arch Gen Psychiatry. 2008;65(7):795-803.
5. Looper KJ. Potential medical and surgical complications of serotonergic antidepressant medications. Psychosomatics. 2007;48:1-9.
6. Gärtner R, Cronin-Fenton D, Hundborg HH, et al. Use of selective serotonin reuptake inhibitors and risk of re-operation due to post-surgical bleeding in breast cancer patients: a Danish population-based cohort study. BMC Surg. 2010;10:3.-
7. Smoller JW, Allison M, Cochrane BB, et al. Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women’s Health Initiative Study. Arch Intern Med. 2009;169(22):2128-2139.
8. Chen Y, Guo JJ, Patel NC. Hemorrhagic stroke associated with antidepressant use in patients with depression: does degree of serotonin reuptake inhibition matter? Pharmacoepidemiol Drug Saf. 2009;18(3):196-202.
Eric C. Kutscher, PharmD, BCPP
Megan Leloux, PharmD
Michael Lemon, PharmD
Dr. Kutscher is Associate Professor of Pharmacy Practice, South Dakota State University College of Pharmacy, Brookings, SD, Adjunct Associate Professor of Psychiatry, Sanford School of Medicine, University of South Dakota, Director of the Psychiatry Pharmacy Practice Residency Program, and Clinical Pharmacy Specialist, Avera Behavioral Health Center, Sioux Falls, SD. Dr. Leloux is a Psychiatric Pharmacy Practice Resident, Avera Behavioral Health Center, Sioux Falls, SD. Dr. Lemon is Professor of Pharmacy Practice, South Dakota State University College of Pharmacy, Brookings, SD, and VA Black Hills Health Care System, Fort Meade, SD.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Eric C. Kutscher, PharmD, BCPP
Megan Leloux, PharmD
Michael Lemon, PharmD
Dr. Kutscher is Associate Professor of Pharmacy Practice, South Dakota State University College of Pharmacy, Brookings, SD, Adjunct Associate Professor of Psychiatry, Sanford School of Medicine, University of South Dakota, Director of the Psychiatry Pharmacy Practice Residency Program, and Clinical Pharmacy Specialist, Avera Behavioral Health Center, Sioux Falls, SD. Dr. Leloux is a Psychiatric Pharmacy Practice Resident, Avera Behavioral Health Center, Sioux Falls, SD. Dr. Lemon is Professor of Pharmacy Practice, South Dakota State University College of Pharmacy, Brookings, SD, and VA Black Hills Health Care System, Fort Meade, SD.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Eric C. Kutscher, PharmD, BCPP
Megan Leloux, PharmD
Michael Lemon, PharmD
Dr. Kutscher is Associate Professor of Pharmacy Practice, South Dakota State University College of Pharmacy, Brookings, SD, Adjunct Associate Professor of Psychiatry, Sanford School of Medicine, University of South Dakota, Director of the Psychiatry Pharmacy Practice Residency Program, and Clinical Pharmacy Specialist, Avera Behavioral Health Center, Sioux Falls, SD. Dr. Leloux is a Psychiatric Pharmacy Practice Resident, Avera Behavioral Health Center, Sioux Falls, SD. Dr. Lemon is Professor of Pharmacy Practice, South Dakota State University College of Pharmacy, Brookings, SD, and VA Black Hills Health Care System, Fort Meade, SD.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Mr. M, age 70, presents to the emergency department (ED) complaining of new-onset fatigue, dizziness, and black, tarry stools. He is anemic (hemoglobin 8.9 g/dL) and his stool is positive for occult blood. Mr. M denies having any symptoms until 1 week ago and reports taking his medications as prescribed. An upper endoscopy reveals a gastrointestinal (GI) bleed and his physician stops his antiplatelet medications. Mr. M’s medical history includes hypertension, hyperlipidemia, and placement of a drug-eluding coronary artery stent 9 months ago. Before presenting to the ED, he had been maintained on lisinopril, 20 mg/d, simvastatin, 40 mg/d, aspirin, 325 mg/d, clopidogrel, 75 mg/d, and a daily multivitamin. Three weeks ago, Mr. M was started on citalopram, 20 mg/d, for depressed mood that he has had since his wife died a year ago.
The psychiatry service is consulted after Mr. M admits he has had thoughts of suicide and a few weeks ago was planning to take an overdose of his medications. He denies taking any extra medications and reports feeling more positive since starting citalopram. The psychiatrist discontinues citalopram, however, because of a possible drug interaction with antiplatelet medications, starts Mr. M on bupropion, 150 mg/d, and recommends he follow up with his primary care physician for management of his depressive symptoms.
- Geriatric patients who take multiple medications for various disease states are at increased risk for drug-drug interactions.
- Serotonergic antidepressants inhibit platelet aggregation, which may increase a patient’s risk of bleeding or bruising.
- Closely monitor patients receiving serotonergic antidepressants concomitantly with other medications that may increase bleeding risk.
- Consider prophylactic acid suppressive therapy for patients at high risk for GI bleeding who receive concomitant SSRIs.
Older patients frequently take multiple medications for various disease states, which increases their risk of drug-drug interactions. In addition, physiologic changes associated with aging alter how patients respond to medications. Drugs may interact pharmacokinetically and pharmacodynamically. Pharmacokinetic interactions are well understood and represent changes in absorption, distribution, metabolism, and elimination of specific medications. Pharmacodynamic drug-drug interactions, on the other hand, are less recognized and represent changes in medications’ mechanism of action. A clinician who understands pharmacodynamic interactions will be able to better identify potential drug-drug interactions and could avoid adverse events.1
Antidepressants and bleeding
In Mr. M’s case, a pharmacodynamic drug-drug interaction among citalopram, aspirin, and clopidogrel caused a GI bleed. This type of interaction may be overlooked because of the relatively safe drug-drug interaction profile of selective serotonin reuptake inhibitors (SSRIs). However, any antidepressant that increases serotonin concentration, including serotonin-norepinephrine reuptake inhibitors, may cause this pharmacodynamic interaction.1
Platelets release serotonin to promote aggregation, but do not produce it themselves and are dependent on the serotonin transporter system (reuptake pump) to acquire serotonin. Because SSRIs act on serotonin transporters found on platelet cell membranes, these drugs deplete platelets’ supply of serotonin, leading to diminished platelet aggregation. This effect may propagate the action of other medications that inhibit platelet aggregation, which may increase a patient’s risk of bruising and/or bleeding. This increased risk of bleeding is not associated with non-serotonergic antidepressants such as bupropion, and seems to decrease when SSRIs are discontinued.2
A modest increase in bleeding risk with SSRIs when used alone and with other platelet-inhibiting therapies has been described in case reports, case controlled studies, and chart reviews.2-4 The agents studied include aspirin and clopidogrel, which Mr. M was receiving, but also other, often-overlooked medications, including nonsteroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase-2 inhibitors, calcium channel blockers, and systemic corticosteroids. Patient factors and diseases—including a history of peptic ulcer disease, previous bleeding, heavy alcohol use, and older age—also may increase bleeding risk (Table).2-5
Serotonin reuptake inhibitor medications have been associated with various bleeding events.5 Most case-control and cohort analyses have examined the risk of GI bleeding with SSRIs; however, serotonergic antidepressants also have been associated with an increased risk of uterine bleeding and perioperative blood loss and transfusions in various surgical procedures.6 Some reports have suggested that there may be a small increase in the incidence of hemorrhagic and fatal stroke with SSRI use5,7; however, many studies have not found an association between SSRI use and increased risk of intracranial hemorrhage stroke.8 The Women’s Health Initiative Study, which reviewed cardiovascular morbidity and mortality data, showed that antidepressant use in postmenopausal women was associated with an increased risk of all-cause mortality, but not coronary heart disease.7 SSRI use was associated with an increased risk of stroke, specifically hemorrhagic stroke, although the absolute event risks were low and cannot be used to predict risk.
Table
Risk factors for gastrointestinal bleeding
| Medications | Corticosteroids, anticoagulants (warfarin), antiplatelets (clopidogrel), NSAIDs (including aspirin), calcium channel blockers, SSRIs, SNRIs, tricyclic antidepressants |
| Disease state/patient factors | Age (elderly are at higher risk), history of ulcer, chronic alcohol use, peptic ulcer disease, esophageal varices, gastric or colorectal cancer, gastritis, liver disease, coagulopathy |
| NSAIDs: nonsteroidal anti-inflammatory drugs; SNRIs: serotonin-norepinephrine reuptake inhibitors; SSRIs: selective serotonin reuptake inhibitors | |
| Source: References 2-5 | |
Reducing bleeding risk
In a case-control study, de Abajo et al4 found that patients taking acid-suppressing drugs—proton pump inhibitors and histamine H2 receptor antagonists—had a lower risk of upper GI tract bleeding associated with serotonergic antidepressants compared with those not taking acid-suppressing medications. These drugs further reduced the risk of bleeding in patients taking NSAIDs or antiplatelet medications concomitantly with SSRIs. We suggest initiating prophylactic acid suppression therapy for any patient who is considered at high risk for a GI bleed and is taking an SSRI with or without other medications that inhibit platelet aggregation. Specifically, start with an H2 antagonist because of these medications’ faster onset of action and lower cost vs proton pump inhibitors.
Although the association between SSRIs and bleeding have been described in observational studies, it is impossible to rule out alternate causes and potential confounders that may have contributed to these events. Due diligence and therapeutic drug monitoring of all known and predicted drug-drug interactions is warranted for all patients taking serotonergic antidepressants in combination with medications known to increase bleeding risk.
Related Resources
- Indiana University School of Medicine. P450 drug interaction table. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
- Hansten PD, Horn JR. The top 100 drug interactions: a guide to patient management. Edmonds, WA: H&H Publications; 2010.
Drug Brand Names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Clopidogrel • Plavix
- Lisinopril • Zestril, Prinivil
- Simvastatin • Zocor
- Warfarin • Coumadin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. M, age 70, presents to the emergency department (ED) complaining of new-onset fatigue, dizziness, and black, tarry stools. He is anemic (hemoglobin 8.9 g/dL) and his stool is positive for occult blood. Mr. M denies having any symptoms until 1 week ago and reports taking his medications as prescribed. An upper endoscopy reveals a gastrointestinal (GI) bleed and his physician stops his antiplatelet medications. Mr. M’s medical history includes hypertension, hyperlipidemia, and placement of a drug-eluding coronary artery stent 9 months ago. Before presenting to the ED, he had been maintained on lisinopril, 20 mg/d, simvastatin, 40 mg/d, aspirin, 325 mg/d, clopidogrel, 75 mg/d, and a daily multivitamin. Three weeks ago, Mr. M was started on citalopram, 20 mg/d, for depressed mood that he has had since his wife died a year ago.
The psychiatry service is consulted after Mr. M admits he has had thoughts of suicide and a few weeks ago was planning to take an overdose of his medications. He denies taking any extra medications and reports feeling more positive since starting citalopram. The psychiatrist discontinues citalopram, however, because of a possible drug interaction with antiplatelet medications, starts Mr. M on bupropion, 150 mg/d, and recommends he follow up with his primary care physician for management of his depressive symptoms.
- Geriatric patients who take multiple medications for various disease states are at increased risk for drug-drug interactions.
- Serotonergic antidepressants inhibit platelet aggregation, which may increase a patient’s risk of bleeding or bruising.
- Closely monitor patients receiving serotonergic antidepressants concomitantly with other medications that may increase bleeding risk.
- Consider prophylactic acid suppressive therapy for patients at high risk for GI bleeding who receive concomitant SSRIs.
Older patients frequently take multiple medications for various disease states, which increases their risk of drug-drug interactions. In addition, physiologic changes associated with aging alter how patients respond to medications. Drugs may interact pharmacokinetically and pharmacodynamically. Pharmacokinetic interactions are well understood and represent changes in absorption, distribution, metabolism, and elimination of specific medications. Pharmacodynamic drug-drug interactions, on the other hand, are less recognized and represent changes in medications’ mechanism of action. A clinician who understands pharmacodynamic interactions will be able to better identify potential drug-drug interactions and could avoid adverse events.1
Antidepressants and bleeding
In Mr. M’s case, a pharmacodynamic drug-drug interaction among citalopram, aspirin, and clopidogrel caused a GI bleed. This type of interaction may be overlooked because of the relatively safe drug-drug interaction profile of selective serotonin reuptake inhibitors (SSRIs). However, any antidepressant that increases serotonin concentration, including serotonin-norepinephrine reuptake inhibitors, may cause this pharmacodynamic interaction.1
Platelets release serotonin to promote aggregation, but do not produce it themselves and are dependent on the serotonin transporter system (reuptake pump) to acquire serotonin. Because SSRIs act on serotonin transporters found on platelet cell membranes, these drugs deplete platelets’ supply of serotonin, leading to diminished platelet aggregation. This effect may propagate the action of other medications that inhibit platelet aggregation, which may increase a patient’s risk of bruising and/or bleeding. This increased risk of bleeding is not associated with non-serotonergic antidepressants such as bupropion, and seems to decrease when SSRIs are discontinued.2
A modest increase in bleeding risk with SSRIs when used alone and with other platelet-inhibiting therapies has been described in case reports, case controlled studies, and chart reviews.2-4 The agents studied include aspirin and clopidogrel, which Mr. M was receiving, but also other, often-overlooked medications, including nonsteroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase-2 inhibitors, calcium channel blockers, and systemic corticosteroids. Patient factors and diseases—including a history of peptic ulcer disease, previous bleeding, heavy alcohol use, and older age—also may increase bleeding risk (Table).2-5
Serotonin reuptake inhibitor medications have been associated with various bleeding events.5 Most case-control and cohort analyses have examined the risk of GI bleeding with SSRIs; however, serotonergic antidepressants also have been associated with an increased risk of uterine bleeding and perioperative blood loss and transfusions in various surgical procedures.6 Some reports have suggested that there may be a small increase in the incidence of hemorrhagic and fatal stroke with SSRI use5,7; however, many studies have not found an association between SSRI use and increased risk of intracranial hemorrhage stroke.8 The Women’s Health Initiative Study, which reviewed cardiovascular morbidity and mortality data, showed that antidepressant use in postmenopausal women was associated with an increased risk of all-cause mortality, but not coronary heart disease.7 SSRI use was associated with an increased risk of stroke, specifically hemorrhagic stroke, although the absolute event risks were low and cannot be used to predict risk.
Table
Risk factors for gastrointestinal bleeding
| Medications | Corticosteroids, anticoagulants (warfarin), antiplatelets (clopidogrel), NSAIDs (including aspirin), calcium channel blockers, SSRIs, SNRIs, tricyclic antidepressants |
| Disease state/patient factors | Age (elderly are at higher risk), history of ulcer, chronic alcohol use, peptic ulcer disease, esophageal varices, gastric or colorectal cancer, gastritis, liver disease, coagulopathy |
| NSAIDs: nonsteroidal anti-inflammatory drugs; SNRIs: serotonin-norepinephrine reuptake inhibitors; SSRIs: selective serotonin reuptake inhibitors | |
| Source: References 2-5 | |
Reducing bleeding risk
In a case-control study, de Abajo et al4 found that patients taking acid-suppressing drugs—proton pump inhibitors and histamine H2 receptor antagonists—had a lower risk of upper GI tract bleeding associated with serotonergic antidepressants compared with those not taking acid-suppressing medications. These drugs further reduced the risk of bleeding in patients taking NSAIDs or antiplatelet medications concomitantly with SSRIs. We suggest initiating prophylactic acid suppression therapy for any patient who is considered at high risk for a GI bleed and is taking an SSRI with or without other medications that inhibit platelet aggregation. Specifically, start with an H2 antagonist because of these medications’ faster onset of action and lower cost vs proton pump inhibitors.
Although the association between SSRIs and bleeding have been described in observational studies, it is impossible to rule out alternate causes and potential confounders that may have contributed to these events. Due diligence and therapeutic drug monitoring of all known and predicted drug-drug interactions is warranted for all patients taking serotonergic antidepressants in combination with medications known to increase bleeding risk.
Related Resources
- Indiana University School of Medicine. P450 drug interaction table. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
- Hansten PD, Horn JR. The top 100 drug interactions: a guide to patient management. Edmonds, WA: H&H Publications; 2010.
Drug Brand Names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Clopidogrel • Plavix
- Lisinopril • Zestril, Prinivil
- Simvastatin • Zocor
- Warfarin • Coumadin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kutscher EC, Alexander B. A review of drug interactions with psychiatric medicines for the pharmacy practitioner. J Pharm Pract. 2007;20(4):327-333.
2. Targownik LE, Bolton JM, Metge CJ, et al. Selective serotonin reuptake inhibitors are associated with a modest increase in the risk of upper gastrointestinal bleeding. Am J Gastroenterol. 2009;104:1475-1482.
3. Opatrny L, Delaney JA, Suissa S. Gastro-intestinal haemorrhage risks of selective serotonin receptor antagonist therapy: a new look. Br J Clin Pharmacol. 2008;66(1):76-81.
4. de Abajo FJ, García-Rodríguez LA. Risk of upper gastrointestinal tract bleeding associated with selective serotonin reuptake inhibitors and venlafaxine therapy: interaction with nonsteroidal anti-inflammatory drugs and effect of acid-suppressing agents. Arch Gen Psychiatry. 2008;65(7):795-803.
5. Looper KJ. Potential medical and surgical complications of serotonergic antidepressant medications. Psychosomatics. 2007;48:1-9.
6. Gärtner R, Cronin-Fenton D, Hundborg HH, et al. Use of selective serotonin reuptake inhibitors and risk of re-operation due to post-surgical bleeding in breast cancer patients: a Danish population-based cohort study. BMC Surg. 2010;10:3.-
7. Smoller JW, Allison M, Cochrane BB, et al. Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women’s Health Initiative Study. Arch Intern Med. 2009;169(22):2128-2139.
8. Chen Y, Guo JJ, Patel NC. Hemorrhagic stroke associated with antidepressant use in patients with depression: does degree of serotonin reuptake inhibition matter? Pharmacoepidemiol Drug Saf. 2009;18(3):196-202.
1. Kutscher EC, Alexander B. A review of drug interactions with psychiatric medicines for the pharmacy practitioner. J Pharm Pract. 2007;20(4):327-333.
2. Targownik LE, Bolton JM, Metge CJ, et al. Selective serotonin reuptake inhibitors are associated with a modest increase in the risk of upper gastrointestinal bleeding. Am J Gastroenterol. 2009;104:1475-1482.
3. Opatrny L, Delaney JA, Suissa S. Gastro-intestinal haemorrhage risks of selective serotonin receptor antagonist therapy: a new look. Br J Clin Pharmacol. 2008;66(1):76-81.
4. de Abajo FJ, García-Rodríguez LA. Risk of upper gastrointestinal tract bleeding associated with selective serotonin reuptake inhibitors and venlafaxine therapy: interaction with nonsteroidal anti-inflammatory drugs and effect of acid-suppressing agents. Arch Gen Psychiatry. 2008;65(7):795-803.
5. Looper KJ. Potential medical and surgical complications of serotonergic antidepressant medications. Psychosomatics. 2007;48:1-9.
6. Gärtner R, Cronin-Fenton D, Hundborg HH, et al. Use of selective serotonin reuptake inhibitors and risk of re-operation due to post-surgical bleeding in breast cancer patients: a Danish population-based cohort study. BMC Surg. 2010;10:3.-
7. Smoller JW, Allison M, Cochrane BB, et al. Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women’s Health Initiative Study. Arch Intern Med. 2009;169(22):2128-2139.
8. Chen Y, Guo JJ, Patel NC. Hemorrhagic stroke associated with antidepressant use in patients with depression: does degree of serotonin reuptake inhibition matter? Pharmacoepidemiol Drug Saf. 2009;18(3):196-202.