Medicare payments to hospitals for bariatric operations varied by nearly $2,000 per episode of care, mostly because of differences in costs incurred in the initial – or index – hospitalization.
The findings, published online Sept. 16 in JAMA Surgery, offer hospitals a guide to where cost variation is highest (doi:10.1001/jamasurg.2015.2394) for these procedures.
Knowing where costs vary the most is particularly important if hospitals opt to accept bundled Medicare payments for bariatric procedures, which are a proposed addition to 48 other episodes of care that can currently be reimbursed in this way. Under bundled care payment programs, hospitals receive a single payment for all services related to a surgery or other episode of care, thereby accepting more risk when inefficiencies occur.
For their research, Dr. Tyler R. Grenda and his colleagues at University of Michigan, Ann Arbor, Center for Healthcare Outcomes and Policy, looked at claims data for 24,647 patients receiving bariatric procedures at 463 hospitals during 2011-2012.
Operations included laparoscopic gastric banding, laparoscopic Roux-en-Y gastric bypass, and open Roux-en-Y gastric bypass, with fewer than 5% of patients receiving other interventions. Mean total payments varied from $11,086 to $13,073 per episode of care, defined as index hospitalization through 30 days postdischarge, for a 16.5% difference between the lowest and highest hospital quartiles.
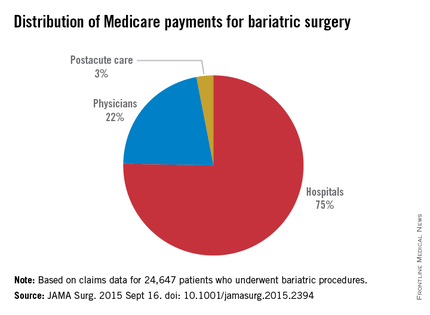
The index hospitalization was responsible for the largest portion of total payments (75%), seen in the study, followed by physician services (21%) and postacute care services (2.8%).
The large share of costs incurred during the index hospitalization was “likely owing to inpatient complications that drive [diagnosis-related group] up-coding,” the authors wrote, noting that DRG with complications result in higher Medicare payments.
Dr. Grenda and his colleagues concluded that bariatric surgery “appears to have a distinct pattern of hospital cost variation” unlike that seen in other procedures that have been studied to identify drivers of cost differences. “This difference in the pattern of variation emphasizes the importance of understanding cost variation specific to each procedure,” they wrote.
For example, a study that looked at hip fracture repair found that postacute care accounted for a large portion of variation in payments, while less variation was seen for the index hospitalization (Health Serv Res. 2010;45[6, pt 1]:1783-95).
In the current policy environment, in which bundled payments are seen as a way to shift cost accountability to hospitals, “a detailed understanding of variation in the costs for bariatric surgery will be essential for hospitals to identify areas of risk and opportunities for improvement,” the researchers wrote in their analysis.
Dr. Grenda and his colleagues’ research was funded by Agency for Healthcare Research and Quality. One coauthor and the supervisor of the study, Dr. Justin Dimnick, disclosed a financial relationship with ArborMetrix, a health care analytics firm not involved with the study; he is also an editor of JAMA Surgery, which published the study.