User login
High Olive Oil Intake Linked to Lower Dementia-Related Death
, a new study suggested.
Data from a prospective study of more than 92,000 people showed consuming at least 7 g of olive oil a day — about half a tablespoon — was associated with a 28% lower risk for dementia-related death.
Replacing one teaspoon of margarine and mayonnaise with the equivalent amount of olive oil was associated with an 8%-14% lower risk for dementia-related mortality.
“Opting for olive oil, a natural product, instead of more processed fats such as margarine and mayonnaise, is a safe choice and may reduce risk of fatal dementia,” said lead investigator Anne-Julie Tessier, RD, PhD, research associate, Department of Nutrition, Harvard T.H. Chan School of Public Health, Boston.
However, “intervention studies are needed to confirm causal effect and optimal quantity of olive oil intake,” she added.
The study was published online in JAMA Network Open.
A Spoonful of Olive Oil
A growing body of evidence has shown a link between the Mediterranean diet and preserved cognitive function and lower risk for cardiovascular disease (CVD). But its association with dementia mortality was unknown.
Investigators analyzed data on over 92,000 participants (66% women; mean age, 56 years) in the Nurses’ Health Study (NHS) and Health Professionals Follow-Up Study (HPFS) who were free of CVD and cancer at baseline.
Both studies were conducted between 1990 and 2018, with olive oil intake assessed every 4 years using a food frequency questionnaire. Dementia-related mortality was ascertained from death records.
The researchers also evaluated the joint association of diet quality (particularly adherence to the Mediterranean diet and Alternative Healthy Eating Index score) and olive oil consumption with the risk for dementia-related mortality. And they estimated the difference in the risk for dementia-related mortality when other dietary fats were substituted with an equivalent amount of olive oil.
There were 4751 dementia-related deaths during the 28-year follow-up period. People with two copies of the apolipoprotein epsilon-4 (APOE epsilon-4) allele — a known risk factor for Alzheimer’s disease — had a fivefold to ninefold greater likelihood of dementia-related death.
Compared with no or rare olive oil intake, consumption of 7 g of olive oil or more per day was associated with a 28% lower risk for dementia-related mortality (adjusted hazard ratio [HR], 0.72; P < .001), after adjusting for lifestyle and socioeconomic factors. The finding remained consistent even with further adjustment for the APOE epsilon-4 allele.
Each 5-g increment in olive oil consumption had an inverse association with dementia-related death in women (HR, 0.88; 95% CI, 0.84-0.93) but not in men (HR, 0.96; 95% CI, 0.88-1.04).
No interaction by diet quality scores was found.
No Link With Diet Quality
“Typically, people who use olive oil for cooking or as a dressing have an overall better quality of their diet, but interestingly, we found the association between more olive oil and reduced risk of dementia-related death to be regardless of this factor,” Dr. Tessier said.
Replacing 5 g per day of margarine and mayonnaise with the equivalent amount of olive oil was associated with an 8%-14% lower risk for dementia mortality. Substitutions for other vegetable oils or butter were not significant.
“Some antioxidant compounds in olive oil can cross the blood-brain barrier, potentially having a direct effect on the brain,” Dr. Tessier said. “It is also possible that olive oil has an indirect effect on brain health by benefiting cardiovascular health.”
The authors noted several study limitations, including the possibility of reverse causation, due to the observational nature of the study.
It is also plausible that higher olive oil intake could be indicative of a healthier diet and higher socioeconomic status, although the results remained consistent after accounting these factors, the authors noted.
The study population included only healthcare professionals and was primarily non-Hispanic White people, which could limit generalizability.
Causality Versus Connection
Commenting on the findings, Rebecca M. Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association, cautioned that the study was designed to show correlation, not causation.
Other notable limitations include measuring prevalence or incidence of dementia from death records because dementia and Alzheimer’s disease are often underreported as a cause of death.
Moreover, people in the highest olive oil consumption group also had better diet quality, higher alcohol intake, were more physically active, and less likely to smoke, Dr. Edelmayer said.
“All of these factors may have an impact on risk of cognitive decline and dementia, separately from or in addition to olive oil consumption,” said Dr. Edelmayer, who was not involved with the study.
She echoed the authors’ concerns that the study was conducted in predominantly non-Hispanic White people and noted that the protective benefits of olive oil were no longer statistically significant for men after adjusting for potential confounders.
It “would be wonderful if a particular food could delay or prevent Alzheimer’s disease, but we do not have scientific evidence that these claims are true,” Dr. Edelmayer said. “We need randomized controlled clinical trials to evaluate whether any foods have a scientifically proven beneficial effect.”
This study is supported by a research grant from the National Institutes of Health to the senior author. The NHS, NHSII, and HPFS are supported by grants from the National Institutes of Health. Tessier is supported by the Canadian Institutes of Health Research Postdoctoral Fellowship Award. Senior author Guasch-Ferré is supported by a Novo Nordisk Foundation grant. Dr. Tessier reported no other relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. Edelmayer reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
, a new study suggested.
Data from a prospective study of more than 92,000 people showed consuming at least 7 g of olive oil a day — about half a tablespoon — was associated with a 28% lower risk for dementia-related death.
Replacing one teaspoon of margarine and mayonnaise with the equivalent amount of olive oil was associated with an 8%-14% lower risk for dementia-related mortality.
“Opting for olive oil, a natural product, instead of more processed fats such as margarine and mayonnaise, is a safe choice and may reduce risk of fatal dementia,” said lead investigator Anne-Julie Tessier, RD, PhD, research associate, Department of Nutrition, Harvard T.H. Chan School of Public Health, Boston.
However, “intervention studies are needed to confirm causal effect and optimal quantity of olive oil intake,” she added.
The study was published online in JAMA Network Open.
A Spoonful of Olive Oil
A growing body of evidence has shown a link between the Mediterranean diet and preserved cognitive function and lower risk for cardiovascular disease (CVD). But its association with dementia mortality was unknown.
Investigators analyzed data on over 92,000 participants (66% women; mean age, 56 years) in the Nurses’ Health Study (NHS) and Health Professionals Follow-Up Study (HPFS) who were free of CVD and cancer at baseline.
Both studies were conducted between 1990 and 2018, with olive oil intake assessed every 4 years using a food frequency questionnaire. Dementia-related mortality was ascertained from death records.
The researchers also evaluated the joint association of diet quality (particularly adherence to the Mediterranean diet and Alternative Healthy Eating Index score) and olive oil consumption with the risk for dementia-related mortality. And they estimated the difference in the risk for dementia-related mortality when other dietary fats were substituted with an equivalent amount of olive oil.
There were 4751 dementia-related deaths during the 28-year follow-up period. People with two copies of the apolipoprotein epsilon-4 (APOE epsilon-4) allele — a known risk factor for Alzheimer’s disease — had a fivefold to ninefold greater likelihood of dementia-related death.
Compared with no or rare olive oil intake, consumption of 7 g of olive oil or more per day was associated with a 28% lower risk for dementia-related mortality (adjusted hazard ratio [HR], 0.72; P < .001), after adjusting for lifestyle and socioeconomic factors. The finding remained consistent even with further adjustment for the APOE epsilon-4 allele.
Each 5-g increment in olive oil consumption had an inverse association with dementia-related death in women (HR, 0.88; 95% CI, 0.84-0.93) but not in men (HR, 0.96; 95% CI, 0.88-1.04).
No interaction by diet quality scores was found.
No Link With Diet Quality
“Typically, people who use olive oil for cooking or as a dressing have an overall better quality of their diet, but interestingly, we found the association between more olive oil and reduced risk of dementia-related death to be regardless of this factor,” Dr. Tessier said.
Replacing 5 g per day of margarine and mayonnaise with the equivalent amount of olive oil was associated with an 8%-14% lower risk for dementia mortality. Substitutions for other vegetable oils or butter were not significant.
“Some antioxidant compounds in olive oil can cross the blood-brain barrier, potentially having a direct effect on the brain,” Dr. Tessier said. “It is also possible that olive oil has an indirect effect on brain health by benefiting cardiovascular health.”
The authors noted several study limitations, including the possibility of reverse causation, due to the observational nature of the study.
It is also plausible that higher olive oil intake could be indicative of a healthier diet and higher socioeconomic status, although the results remained consistent after accounting these factors, the authors noted.
The study population included only healthcare professionals and was primarily non-Hispanic White people, which could limit generalizability.
Causality Versus Connection
Commenting on the findings, Rebecca M. Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association, cautioned that the study was designed to show correlation, not causation.
Other notable limitations include measuring prevalence or incidence of dementia from death records because dementia and Alzheimer’s disease are often underreported as a cause of death.
Moreover, people in the highest olive oil consumption group also had better diet quality, higher alcohol intake, were more physically active, and less likely to smoke, Dr. Edelmayer said.
“All of these factors may have an impact on risk of cognitive decline and dementia, separately from or in addition to olive oil consumption,” said Dr. Edelmayer, who was not involved with the study.
She echoed the authors’ concerns that the study was conducted in predominantly non-Hispanic White people and noted that the protective benefits of olive oil were no longer statistically significant for men after adjusting for potential confounders.
It “would be wonderful if a particular food could delay or prevent Alzheimer’s disease, but we do not have scientific evidence that these claims are true,” Dr. Edelmayer said. “We need randomized controlled clinical trials to evaluate whether any foods have a scientifically proven beneficial effect.”
This study is supported by a research grant from the National Institutes of Health to the senior author. The NHS, NHSII, and HPFS are supported by grants from the National Institutes of Health. Tessier is supported by the Canadian Institutes of Health Research Postdoctoral Fellowship Award. Senior author Guasch-Ferré is supported by a Novo Nordisk Foundation grant. Dr. Tessier reported no other relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. Edelmayer reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
, a new study suggested.
Data from a prospective study of more than 92,000 people showed consuming at least 7 g of olive oil a day — about half a tablespoon — was associated with a 28% lower risk for dementia-related death.
Replacing one teaspoon of margarine and mayonnaise with the equivalent amount of olive oil was associated with an 8%-14% lower risk for dementia-related mortality.
“Opting for olive oil, a natural product, instead of more processed fats such as margarine and mayonnaise, is a safe choice and may reduce risk of fatal dementia,” said lead investigator Anne-Julie Tessier, RD, PhD, research associate, Department of Nutrition, Harvard T.H. Chan School of Public Health, Boston.
However, “intervention studies are needed to confirm causal effect and optimal quantity of olive oil intake,” she added.
The study was published online in JAMA Network Open.
A Spoonful of Olive Oil
A growing body of evidence has shown a link between the Mediterranean diet and preserved cognitive function and lower risk for cardiovascular disease (CVD). But its association with dementia mortality was unknown.
Investigators analyzed data on over 92,000 participants (66% women; mean age, 56 years) in the Nurses’ Health Study (NHS) and Health Professionals Follow-Up Study (HPFS) who were free of CVD and cancer at baseline.
Both studies were conducted between 1990 and 2018, with olive oil intake assessed every 4 years using a food frequency questionnaire. Dementia-related mortality was ascertained from death records.
The researchers also evaluated the joint association of diet quality (particularly adherence to the Mediterranean diet and Alternative Healthy Eating Index score) and olive oil consumption with the risk for dementia-related mortality. And they estimated the difference in the risk for dementia-related mortality when other dietary fats were substituted with an equivalent amount of olive oil.
There were 4751 dementia-related deaths during the 28-year follow-up period. People with two copies of the apolipoprotein epsilon-4 (APOE epsilon-4) allele — a known risk factor for Alzheimer’s disease — had a fivefold to ninefold greater likelihood of dementia-related death.
Compared with no or rare olive oil intake, consumption of 7 g of olive oil or more per day was associated with a 28% lower risk for dementia-related mortality (adjusted hazard ratio [HR], 0.72; P < .001), after adjusting for lifestyle and socioeconomic factors. The finding remained consistent even with further adjustment for the APOE epsilon-4 allele.
Each 5-g increment in olive oil consumption had an inverse association with dementia-related death in women (HR, 0.88; 95% CI, 0.84-0.93) but not in men (HR, 0.96; 95% CI, 0.88-1.04).
No interaction by diet quality scores was found.
No Link With Diet Quality
“Typically, people who use olive oil for cooking or as a dressing have an overall better quality of their diet, but interestingly, we found the association between more olive oil and reduced risk of dementia-related death to be regardless of this factor,” Dr. Tessier said.
Replacing 5 g per day of margarine and mayonnaise with the equivalent amount of olive oil was associated with an 8%-14% lower risk for dementia mortality. Substitutions for other vegetable oils or butter were not significant.
“Some antioxidant compounds in olive oil can cross the blood-brain barrier, potentially having a direct effect on the brain,” Dr. Tessier said. “It is also possible that olive oil has an indirect effect on brain health by benefiting cardiovascular health.”
The authors noted several study limitations, including the possibility of reverse causation, due to the observational nature of the study.
It is also plausible that higher olive oil intake could be indicative of a healthier diet and higher socioeconomic status, although the results remained consistent after accounting these factors, the authors noted.
The study population included only healthcare professionals and was primarily non-Hispanic White people, which could limit generalizability.
Causality Versus Connection
Commenting on the findings, Rebecca M. Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association, cautioned that the study was designed to show correlation, not causation.
Other notable limitations include measuring prevalence or incidence of dementia from death records because dementia and Alzheimer’s disease are often underreported as a cause of death.
Moreover, people in the highest olive oil consumption group also had better diet quality, higher alcohol intake, were more physically active, and less likely to smoke, Dr. Edelmayer said.
“All of these factors may have an impact on risk of cognitive decline and dementia, separately from or in addition to olive oil consumption,” said Dr. Edelmayer, who was not involved with the study.
She echoed the authors’ concerns that the study was conducted in predominantly non-Hispanic White people and noted that the protective benefits of olive oil were no longer statistically significant for men after adjusting for potential confounders.
It “would be wonderful if a particular food could delay or prevent Alzheimer’s disease, but we do not have scientific evidence that these claims are true,” Dr. Edelmayer said. “We need randomized controlled clinical trials to evaluate whether any foods have a scientifically proven beneficial effect.”
This study is supported by a research grant from the National Institutes of Health to the senior author. The NHS, NHSII, and HPFS are supported by grants from the National Institutes of Health. Tessier is supported by the Canadian Institutes of Health Research Postdoctoral Fellowship Award. Senior author Guasch-Ferré is supported by a Novo Nordisk Foundation grant. Dr. Tessier reported no other relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. Edelmayer reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM JAMA NETWORK OPEN
ADHD Tied to Risk for Lewy Body Disease, Dementia, MCI
, results of a new study showed.
“Determining whether there is an association between ADHD and subsequent conversion to a specific type of dementia is important. This information could generate opportunities for prevention and early treatment, as well as initiate research into the pathophysiological processes involved in understanding the process of cognitive decline,” the researchers, led by Ángel Golimstok, MD, of Hospital Italiano, Buenos Aires, Argentina, wrote.
The findings were published online in The American Journal of Geriatric Psychiatry.
Seeking Confirmation
The researchers first identified a link between DLB and ADHD in 2011. Since then, there have been eight additional studies from other groups also showing a possible link between ADHD and DLB.
To confirm the relationship, the researchers recruited 270 individuals between the ages of 45 and 70 years between 2007 and 2012. Of these, 161 had ADHD, and 109 were healthy controls.
Participants with ADHD met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, text revision criteria for a diagnosis in the past and had a chronic course of ADHD symptoms from adolescence to adulthood that caused mild to severe impairment.
Investigators excluded participants who had been taking ADHD medications for 6 months or more, those with MCI at study initiation, and those with other comorbid psychiatric disorders.
At baseline, all participants received a physical exam, an MRI, and a neuropsychological exam to test for any type of dementia-related impairment.
Study participants were followed for an average of 12 years. A total of 27 individuals with ADHD developed dementia versus four patients in the control group (17% vs 4%, respectively), and 19 of those also had DLB (P = .002 for both).
Of those who developed any type of dementia, 87% were from the ADHD group. The most frequent type of dementia was DLB, 95% of which occurred in the ADHD group. Overall, DLB represented 70% of the dementia cases among participants with ADHD.
A total of 108 participants with ADHD were subsequently diagnosed with naMCI versus 19 healthy controls (67% vs 17%; P < .001).
“Although this pattern of deficits is reasonably expected in early DLB, these results should be interpreted with caution because they may be related to the overlap of symptoms and cognitive deficits between ADHD and naMCI, which may lead to an overestimation of the degenerative phenomenon. Thus, our cases of naMCI could correspond to the natural aging of ADHD patients and not to pathological deterioration,” the authors wrote.
The researchers pointed out that the sample of patients with ADHD originally sought evaluation because of a cognitive complaint or their own motivation. Therefore, the study results are not generalizable to all patients with ADHD. Another limitation was the relatively small number of patients included in the sample.
There was no reported source of funding, and there were no relevant disclosures reported.
A version of this article appeared on Medscape.com.
, results of a new study showed.
“Determining whether there is an association between ADHD and subsequent conversion to a specific type of dementia is important. This information could generate opportunities for prevention and early treatment, as well as initiate research into the pathophysiological processes involved in understanding the process of cognitive decline,” the researchers, led by Ángel Golimstok, MD, of Hospital Italiano, Buenos Aires, Argentina, wrote.
The findings were published online in The American Journal of Geriatric Psychiatry.
Seeking Confirmation
The researchers first identified a link between DLB and ADHD in 2011. Since then, there have been eight additional studies from other groups also showing a possible link between ADHD and DLB.
To confirm the relationship, the researchers recruited 270 individuals between the ages of 45 and 70 years between 2007 and 2012. Of these, 161 had ADHD, and 109 were healthy controls.
Participants with ADHD met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, text revision criteria for a diagnosis in the past and had a chronic course of ADHD symptoms from adolescence to adulthood that caused mild to severe impairment.
Investigators excluded participants who had been taking ADHD medications for 6 months or more, those with MCI at study initiation, and those with other comorbid psychiatric disorders.
At baseline, all participants received a physical exam, an MRI, and a neuropsychological exam to test for any type of dementia-related impairment.
Study participants were followed for an average of 12 years. A total of 27 individuals with ADHD developed dementia versus four patients in the control group (17% vs 4%, respectively), and 19 of those also had DLB (P = .002 for both).
Of those who developed any type of dementia, 87% were from the ADHD group. The most frequent type of dementia was DLB, 95% of which occurred in the ADHD group. Overall, DLB represented 70% of the dementia cases among participants with ADHD.
A total of 108 participants with ADHD were subsequently diagnosed with naMCI versus 19 healthy controls (67% vs 17%; P < .001).
“Although this pattern of deficits is reasonably expected in early DLB, these results should be interpreted with caution because they may be related to the overlap of symptoms and cognitive deficits between ADHD and naMCI, which may lead to an overestimation of the degenerative phenomenon. Thus, our cases of naMCI could correspond to the natural aging of ADHD patients and not to pathological deterioration,” the authors wrote.
The researchers pointed out that the sample of patients with ADHD originally sought evaluation because of a cognitive complaint or their own motivation. Therefore, the study results are not generalizable to all patients with ADHD. Another limitation was the relatively small number of patients included in the sample.
There was no reported source of funding, and there were no relevant disclosures reported.
A version of this article appeared on Medscape.com.
, results of a new study showed.
“Determining whether there is an association between ADHD and subsequent conversion to a specific type of dementia is important. This information could generate opportunities for prevention and early treatment, as well as initiate research into the pathophysiological processes involved in understanding the process of cognitive decline,” the researchers, led by Ángel Golimstok, MD, of Hospital Italiano, Buenos Aires, Argentina, wrote.
The findings were published online in The American Journal of Geriatric Psychiatry.
Seeking Confirmation
The researchers first identified a link between DLB and ADHD in 2011. Since then, there have been eight additional studies from other groups also showing a possible link between ADHD and DLB.
To confirm the relationship, the researchers recruited 270 individuals between the ages of 45 and 70 years between 2007 and 2012. Of these, 161 had ADHD, and 109 were healthy controls.
Participants with ADHD met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, text revision criteria for a diagnosis in the past and had a chronic course of ADHD symptoms from adolescence to adulthood that caused mild to severe impairment.
Investigators excluded participants who had been taking ADHD medications for 6 months or more, those with MCI at study initiation, and those with other comorbid psychiatric disorders.
At baseline, all participants received a physical exam, an MRI, and a neuropsychological exam to test for any type of dementia-related impairment.
Study participants were followed for an average of 12 years. A total of 27 individuals with ADHD developed dementia versus four patients in the control group (17% vs 4%, respectively), and 19 of those also had DLB (P = .002 for both).
Of those who developed any type of dementia, 87% were from the ADHD group. The most frequent type of dementia was DLB, 95% of which occurred in the ADHD group. Overall, DLB represented 70% of the dementia cases among participants with ADHD.
A total of 108 participants with ADHD were subsequently diagnosed with naMCI versus 19 healthy controls (67% vs 17%; P < .001).
“Although this pattern of deficits is reasonably expected in early DLB, these results should be interpreted with caution because they may be related to the overlap of symptoms and cognitive deficits between ADHD and naMCI, which may lead to an overestimation of the degenerative phenomenon. Thus, our cases of naMCI could correspond to the natural aging of ADHD patients and not to pathological deterioration,” the authors wrote.
The researchers pointed out that the sample of patients with ADHD originally sought evaluation because of a cognitive complaint or their own motivation. Therefore, the study results are not generalizable to all patients with ADHD. Another limitation was the relatively small number of patients included in the sample.
There was no reported source of funding, and there were no relevant disclosures reported.
A version of this article appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF GERIATRIC PSYCHIATRY
TMS May Be a Good Alternative to ECT in Depression
DENVER — , according to results from a retrospective study of patients treated in the past 20 years.
“We always learn in our textbooks that after about two or three medication trials is when you can start exploring more serious treatment protocols, such as ECT or TMS, but a lot of these patients weren’t going forward with it, and I was curious about it. I figured that TMS, which is a less expensive, less scary procedure that patients would more likely be open to, that is also approved for treatment resistant depression, would be a good alternative to ECT,” said Anuttham Kandhadai, a third-year medical student at University of Texas Medical Branch at Galveston, who presented the study at the 2024 annual meeting of the American Academy of Neurology.
Study Findings Lead to More Questions
The researchers found lower rates of depressive episodes, suicidal attempts, and suicidal ideation among patients treated with TMS, but an important limitation was that the researchers did not know the severity of the depression in the two patient groups, according to Branch Coslett, MD, who attended the session and has performed research with TMS to treat aphasia in stroke patients. “I think it’s a very interesting study, and certainly something worth pursuing, but given that ECT is only used as a last resort, whereas TMS is often used as a second-line therapy, I think you’re really talking about very different populations that have had these treatments,” said Dr. Coslett.
Mr. Kandhadai recognized the limitations of the study and looks forward to expanding the research. “I’d love to explore cost effectiveness of the treatments. I’d love to explore patient familiarity and patient comfort with different treatments. And I’d also love to explore a more controlled study that can determine how severe someone’s depression is, and then be able to control for that and explore the outcomes based on the treatment protocol,” he said.
The ideal comparative study would be prospective, “but that will never be done. One Flew Over the Cuckoo’s Nest and similar sources of information have really poisoned the well,” said Dr. Coslett. However, he noted that advances have been made in ECT, and that targeting the right hemisphere produces fewer side effects: “The outcomes from unilateral right hemisphere stimulation are said to be every bit as good or maybe better, and you don’t get the confusion, you don’t get the memory loss, you don’t get all that sort of stuff that you’d expect when somebody has a prolonged, generalized tonic-clonic seizure.”
Still, people are naturally reluctant to undergo ECT. “I’ve seen it. It’s pretty barbaric. It’s better now and at my institution, people do get it, but they really, really have to be intractable,” he said.
Comparing Treatment Options
Mr. Kandhadai and his co-authors used the TriNetX database to identify patients with treatment-resistant major depressive disorder who received TMS or ECT in the past 20 years. There were 2,916 patients in both cohorts, who were matched by age, sex, ethnicity, mood and behavioral disorders, endocrine disorders, intellectual disabilities, cerebrovascular disease, and other nervous system disorders. The mean age at treatment was 48.2 years, 38.5% were male, and 3.1% were Black or African American.
Short-term outcomes favored TMS, including the frequency of disorientation (0.41% vs 2.81%), retrograde amnesia (0.34% vs 0.65%), and headache (4.36% vs 7.20%). Long-term outcomes from 1 month to 5 years post treatment were also better in the TMS group, including depressive episodes (44.99% vs 53.77%), suicide attempts (3.98% vs 6.86%), and suicidal ideation (12.38% vs 23.49%). Kaplan-Meier curve analysis between 1 month and 5 years showed a benefit to TMS in probability of not experiencing a depressive episode, and not experiencing suicidal ideation.
“ECT has been the gold standard of treatment resistant depression for a long time, and it deserves to be. I think it’s something you should offer your patients. Not everyone might be comfortable with it, and if they’re not, I think it’s important to not stop the conversation there, but to offer something like TMS because TMS is something that might be more accessible to patients. It might be more affordable, and it might be less scary,” said Mr. Kandhadai
Mr. Kandhadai and Dr. Coslett have no relevant financial disclosures.
DENVER — , according to results from a retrospective study of patients treated in the past 20 years.
“We always learn in our textbooks that after about two or three medication trials is when you can start exploring more serious treatment protocols, such as ECT or TMS, but a lot of these patients weren’t going forward with it, and I was curious about it. I figured that TMS, which is a less expensive, less scary procedure that patients would more likely be open to, that is also approved for treatment resistant depression, would be a good alternative to ECT,” said Anuttham Kandhadai, a third-year medical student at University of Texas Medical Branch at Galveston, who presented the study at the 2024 annual meeting of the American Academy of Neurology.
Study Findings Lead to More Questions
The researchers found lower rates of depressive episodes, suicidal attempts, and suicidal ideation among patients treated with TMS, but an important limitation was that the researchers did not know the severity of the depression in the two patient groups, according to Branch Coslett, MD, who attended the session and has performed research with TMS to treat aphasia in stroke patients. “I think it’s a very interesting study, and certainly something worth pursuing, but given that ECT is only used as a last resort, whereas TMS is often used as a second-line therapy, I think you’re really talking about very different populations that have had these treatments,” said Dr. Coslett.
Mr. Kandhadai recognized the limitations of the study and looks forward to expanding the research. “I’d love to explore cost effectiveness of the treatments. I’d love to explore patient familiarity and patient comfort with different treatments. And I’d also love to explore a more controlled study that can determine how severe someone’s depression is, and then be able to control for that and explore the outcomes based on the treatment protocol,” he said.
The ideal comparative study would be prospective, “but that will never be done. One Flew Over the Cuckoo’s Nest and similar sources of information have really poisoned the well,” said Dr. Coslett. However, he noted that advances have been made in ECT, and that targeting the right hemisphere produces fewer side effects: “The outcomes from unilateral right hemisphere stimulation are said to be every bit as good or maybe better, and you don’t get the confusion, you don’t get the memory loss, you don’t get all that sort of stuff that you’d expect when somebody has a prolonged, generalized tonic-clonic seizure.”
Still, people are naturally reluctant to undergo ECT. “I’ve seen it. It’s pretty barbaric. It’s better now and at my institution, people do get it, but they really, really have to be intractable,” he said.
Comparing Treatment Options
Mr. Kandhadai and his co-authors used the TriNetX database to identify patients with treatment-resistant major depressive disorder who received TMS or ECT in the past 20 years. There were 2,916 patients in both cohorts, who were matched by age, sex, ethnicity, mood and behavioral disorders, endocrine disorders, intellectual disabilities, cerebrovascular disease, and other nervous system disorders. The mean age at treatment was 48.2 years, 38.5% were male, and 3.1% were Black or African American.
Short-term outcomes favored TMS, including the frequency of disorientation (0.41% vs 2.81%), retrograde amnesia (0.34% vs 0.65%), and headache (4.36% vs 7.20%). Long-term outcomes from 1 month to 5 years post treatment were also better in the TMS group, including depressive episodes (44.99% vs 53.77%), suicide attempts (3.98% vs 6.86%), and suicidal ideation (12.38% vs 23.49%). Kaplan-Meier curve analysis between 1 month and 5 years showed a benefit to TMS in probability of not experiencing a depressive episode, and not experiencing suicidal ideation.
“ECT has been the gold standard of treatment resistant depression for a long time, and it deserves to be. I think it’s something you should offer your patients. Not everyone might be comfortable with it, and if they’re not, I think it’s important to not stop the conversation there, but to offer something like TMS because TMS is something that might be more accessible to patients. It might be more affordable, and it might be less scary,” said Mr. Kandhadai
Mr. Kandhadai and Dr. Coslett have no relevant financial disclosures.
DENVER — , according to results from a retrospective study of patients treated in the past 20 years.
“We always learn in our textbooks that after about two or three medication trials is when you can start exploring more serious treatment protocols, such as ECT or TMS, but a lot of these patients weren’t going forward with it, and I was curious about it. I figured that TMS, which is a less expensive, less scary procedure that patients would more likely be open to, that is also approved for treatment resistant depression, would be a good alternative to ECT,” said Anuttham Kandhadai, a third-year medical student at University of Texas Medical Branch at Galveston, who presented the study at the 2024 annual meeting of the American Academy of Neurology.
Study Findings Lead to More Questions
The researchers found lower rates of depressive episodes, suicidal attempts, and suicidal ideation among patients treated with TMS, but an important limitation was that the researchers did not know the severity of the depression in the two patient groups, according to Branch Coslett, MD, who attended the session and has performed research with TMS to treat aphasia in stroke patients. “I think it’s a very interesting study, and certainly something worth pursuing, but given that ECT is only used as a last resort, whereas TMS is often used as a second-line therapy, I think you’re really talking about very different populations that have had these treatments,” said Dr. Coslett.
Mr. Kandhadai recognized the limitations of the study and looks forward to expanding the research. “I’d love to explore cost effectiveness of the treatments. I’d love to explore patient familiarity and patient comfort with different treatments. And I’d also love to explore a more controlled study that can determine how severe someone’s depression is, and then be able to control for that and explore the outcomes based on the treatment protocol,” he said.
The ideal comparative study would be prospective, “but that will never be done. One Flew Over the Cuckoo’s Nest and similar sources of information have really poisoned the well,” said Dr. Coslett. However, he noted that advances have been made in ECT, and that targeting the right hemisphere produces fewer side effects: “The outcomes from unilateral right hemisphere stimulation are said to be every bit as good or maybe better, and you don’t get the confusion, you don’t get the memory loss, you don’t get all that sort of stuff that you’d expect when somebody has a prolonged, generalized tonic-clonic seizure.”
Still, people are naturally reluctant to undergo ECT. “I’ve seen it. It’s pretty barbaric. It’s better now and at my institution, people do get it, but they really, really have to be intractable,” he said.
Comparing Treatment Options
Mr. Kandhadai and his co-authors used the TriNetX database to identify patients with treatment-resistant major depressive disorder who received TMS or ECT in the past 20 years. There were 2,916 patients in both cohorts, who were matched by age, sex, ethnicity, mood and behavioral disorders, endocrine disorders, intellectual disabilities, cerebrovascular disease, and other nervous system disorders. The mean age at treatment was 48.2 years, 38.5% were male, and 3.1% were Black or African American.
Short-term outcomes favored TMS, including the frequency of disorientation (0.41% vs 2.81%), retrograde amnesia (0.34% vs 0.65%), and headache (4.36% vs 7.20%). Long-term outcomes from 1 month to 5 years post treatment were also better in the TMS group, including depressive episodes (44.99% vs 53.77%), suicide attempts (3.98% vs 6.86%), and suicidal ideation (12.38% vs 23.49%). Kaplan-Meier curve analysis between 1 month and 5 years showed a benefit to TMS in probability of not experiencing a depressive episode, and not experiencing suicidal ideation.
“ECT has been the gold standard of treatment resistant depression for a long time, and it deserves to be. I think it’s something you should offer your patients. Not everyone might be comfortable with it, and if they’re not, I think it’s important to not stop the conversation there, but to offer something like TMS because TMS is something that might be more accessible to patients. It might be more affordable, and it might be less scary,” said Mr. Kandhadai
Mr. Kandhadai and Dr. Coslett have no relevant financial disclosures.
FROM AAN 2024
Major Gaps in Care and Management of Neurologic Diseases
DENVER –
Investigators led by Nikki Win, PhD, medical manager/team lead, OMNI Scientific Strategy and Collaborations, US Medical Affairs, Genentech/Roche, found that patients with Parkinson’s disease were referred to a specialist most often, followed by those with MS and those with AD.
The findings were presented at the 2024 annual meeting of the American Academy of Neurology (AAN).
National Neurologist Shortage
The national neurologist shortage, coupled with the growing incidence of Alzheimer’s disease, Parkinson’s disease, MS, and other conditions has led the AAN and other organizations to call for expanding the role of primary care physicians in the diagnosis and management of neurologic disorders, the leading global cause of disability.
“These neurological conditions are increasing in prevalence and there’s a limited number of neurologists, so we wanted to understand what this looks like in the US,” Dr. Win said.
“There is a need to understand the patient journey from primary care to neurology care, from presentation of a suspected neurological disorder to diagnosis, referral to a specialist, and the time elapsed before the specialist visit for Alzheimer’s disease, MS, and Parkinson’s disease in the US,” Dr. Win added.
Timely and accurate diagnoses of neurologic disorders can optimize treatment outcomes. Because many of these diseases are first detected during a visit with a primary care physician, it is important to understand the timeline from the initial visit to a specialist referral, the investigators noted.
Analyzing Trends in Specialist Referrals
Using claims data from the Optum Normative Health Information database, researchers identified 48,525 adults with Alzheimer’s disease, 26,431 with Parkinson’s disease, and 8169 with MS who received a diagnosis from a primary care physician between 2016 and 2021.
They examined the proportion, timing, and demographic factors associated with referrals from primary care clinicians or other healthcare providers to specialists including neurologists, neurosurgeons, psychiatrists, and geriatric medicine specialists.
Results showed that patients with Parkinson’s disease were referred to a specialist most often (53%), followed by those with MS (42%) and those with Alzheimer’s disease (27%).
Individuals with Alzheimer’s disease waited the longest for a specialist referral, with a median of 10 months between the time of referral and the first specialist visit compared with 5.7 months for patients with Parkinson’s disease and 2.6 months for MS patients.
“Some patients with common conditions like Alzheimer’s disease, MS, and Parkinson’s disease don’t see a neurologist, and when they do, it can take as long as 10 months,” said Dr. Win.
Using zip code heatmaps, researchers found that the proportion of referrals for all neurologic disorders was higher in the Midwest and Northeast, whereas patients in the South and West were less likely to receive a referral.
Referrals for Alzheimer’s disease were low nationwide, except for some areas of Michigan and New England. California had the lowest referral rate for MS, followed by regions in the South and Northeast. Patients with Parkinson’s disease living in the Midwest and Northeast were more likely than those in the West to receive a specialist referral.
Previous studies have reported regional shortages of neurologists, said Dr. Win. “Our data seem to correlate that in terms of the areas with lower referral patterns, but as to whether that is causative or correlative, we don’t know.”
Odds of referral were also influenced by demographic characteristics such as sex, age, race, and ethnicity, investigators found.
For example, there were fewer referrals with increasing age across all three neurologic disorders, and men were more likely than women to be referred for Alzheimer’s disease and Parkinson’s disease. Compared with White patients, Parkinson’s disease referrals were less likely among African American, Asian, and Hispanic patients and Alzheimer’s disease referrals were less common among Asian and Hispanic patients.
Insurance status also affected referrals. People with MS and Parkinson’s disease who had commercial insurance were referred more often than were those with Medicare Advantage, said Dr. Win.
She also noted, “Additional research is needed to understand how being referred or not being referred to a neurologist actually impacts patient treatment, care and outcomes.”
Neurology Challenges
Commenting on the research, Thomas Vidic, MD, a community neurologist in Elkhart, Indiana, and clinical professor of neurology at Indiana University School of Medicine at South Bend, said that he was surprised by the variation in wait times for patients.
This, he said, could reflect a study limitation or a higher comfort level among primary care doctors in treating dementia.
With respect to MS, Dr. Vidic said that he believes primary care physicians may not be uncertain about prescribing the approved medications for the disease because there are so many of them.
In addition, patients with Alzheimer’s disease are older and perhaps less accepting of being referred to a specialist that may be hours away.
The bottom line for Dr. Vidic, though, is the lack of specialists. “It comes back to the fact we’re not doing a good job of having community neurologists available to take care of these problems,” he said.
The issue of community neurologist shortages was underlined by the study’s findings about geographic gaps in specialist referrals across the country, he said.
Neurologists make up about 2% of the medical workforce and this has remained static for some time, Dr. Vidic noted. Meanwhile, people are living longer and developing more neurologic diseases.
Dr. Vidic also pointed to the lack of neurology training programs. “There has not been a significant change in the number of programs in the last 10-15 years,” he said.
Study funding was not disclosed. Dr. Win reports receiving personal compensation for serving as an employee of Genentech and has stock in Genentech. Dr. Vidic reports no relevant financial disclosures.
A version of this article appeared on Medscape.com.
DENVER –
Investigators led by Nikki Win, PhD, medical manager/team lead, OMNI Scientific Strategy and Collaborations, US Medical Affairs, Genentech/Roche, found that patients with Parkinson’s disease were referred to a specialist most often, followed by those with MS and those with AD.
The findings were presented at the 2024 annual meeting of the American Academy of Neurology (AAN).
National Neurologist Shortage
The national neurologist shortage, coupled with the growing incidence of Alzheimer’s disease, Parkinson’s disease, MS, and other conditions has led the AAN and other organizations to call for expanding the role of primary care physicians in the diagnosis and management of neurologic disorders, the leading global cause of disability.
“These neurological conditions are increasing in prevalence and there’s a limited number of neurologists, so we wanted to understand what this looks like in the US,” Dr. Win said.
“There is a need to understand the patient journey from primary care to neurology care, from presentation of a suspected neurological disorder to diagnosis, referral to a specialist, and the time elapsed before the specialist visit for Alzheimer’s disease, MS, and Parkinson’s disease in the US,” Dr. Win added.
Timely and accurate diagnoses of neurologic disorders can optimize treatment outcomes. Because many of these diseases are first detected during a visit with a primary care physician, it is important to understand the timeline from the initial visit to a specialist referral, the investigators noted.
Analyzing Trends in Specialist Referrals
Using claims data from the Optum Normative Health Information database, researchers identified 48,525 adults with Alzheimer’s disease, 26,431 with Parkinson’s disease, and 8169 with MS who received a diagnosis from a primary care physician between 2016 and 2021.
They examined the proportion, timing, and demographic factors associated with referrals from primary care clinicians or other healthcare providers to specialists including neurologists, neurosurgeons, psychiatrists, and geriatric medicine specialists.
Results showed that patients with Parkinson’s disease were referred to a specialist most often (53%), followed by those with MS (42%) and those with Alzheimer’s disease (27%).
Individuals with Alzheimer’s disease waited the longest for a specialist referral, with a median of 10 months between the time of referral and the first specialist visit compared with 5.7 months for patients with Parkinson’s disease and 2.6 months for MS patients.
“Some patients with common conditions like Alzheimer’s disease, MS, and Parkinson’s disease don’t see a neurologist, and when they do, it can take as long as 10 months,” said Dr. Win.
Using zip code heatmaps, researchers found that the proportion of referrals for all neurologic disorders was higher in the Midwest and Northeast, whereas patients in the South and West were less likely to receive a referral.
Referrals for Alzheimer’s disease were low nationwide, except for some areas of Michigan and New England. California had the lowest referral rate for MS, followed by regions in the South and Northeast. Patients with Parkinson’s disease living in the Midwest and Northeast were more likely than those in the West to receive a specialist referral.
Previous studies have reported regional shortages of neurologists, said Dr. Win. “Our data seem to correlate that in terms of the areas with lower referral patterns, but as to whether that is causative or correlative, we don’t know.”
Odds of referral were also influenced by demographic characteristics such as sex, age, race, and ethnicity, investigators found.
For example, there were fewer referrals with increasing age across all three neurologic disorders, and men were more likely than women to be referred for Alzheimer’s disease and Parkinson’s disease. Compared with White patients, Parkinson’s disease referrals were less likely among African American, Asian, and Hispanic patients and Alzheimer’s disease referrals were less common among Asian and Hispanic patients.
Insurance status also affected referrals. People with MS and Parkinson’s disease who had commercial insurance were referred more often than were those with Medicare Advantage, said Dr. Win.
She also noted, “Additional research is needed to understand how being referred or not being referred to a neurologist actually impacts patient treatment, care and outcomes.”
Neurology Challenges
Commenting on the research, Thomas Vidic, MD, a community neurologist in Elkhart, Indiana, and clinical professor of neurology at Indiana University School of Medicine at South Bend, said that he was surprised by the variation in wait times for patients.
This, he said, could reflect a study limitation or a higher comfort level among primary care doctors in treating dementia.
With respect to MS, Dr. Vidic said that he believes primary care physicians may not be uncertain about prescribing the approved medications for the disease because there are so many of them.
In addition, patients with Alzheimer’s disease are older and perhaps less accepting of being referred to a specialist that may be hours away.
The bottom line for Dr. Vidic, though, is the lack of specialists. “It comes back to the fact we’re not doing a good job of having community neurologists available to take care of these problems,” he said.
The issue of community neurologist shortages was underlined by the study’s findings about geographic gaps in specialist referrals across the country, he said.
Neurologists make up about 2% of the medical workforce and this has remained static for some time, Dr. Vidic noted. Meanwhile, people are living longer and developing more neurologic diseases.
Dr. Vidic also pointed to the lack of neurology training programs. “There has not been a significant change in the number of programs in the last 10-15 years,” he said.
Study funding was not disclosed. Dr. Win reports receiving personal compensation for serving as an employee of Genentech and has stock in Genentech. Dr. Vidic reports no relevant financial disclosures.
A version of this article appeared on Medscape.com.
DENVER –
Investigators led by Nikki Win, PhD, medical manager/team lead, OMNI Scientific Strategy and Collaborations, US Medical Affairs, Genentech/Roche, found that patients with Parkinson’s disease were referred to a specialist most often, followed by those with MS and those with AD.
The findings were presented at the 2024 annual meeting of the American Academy of Neurology (AAN).
National Neurologist Shortage
The national neurologist shortage, coupled with the growing incidence of Alzheimer’s disease, Parkinson’s disease, MS, and other conditions has led the AAN and other organizations to call for expanding the role of primary care physicians in the diagnosis and management of neurologic disorders, the leading global cause of disability.
“These neurological conditions are increasing in prevalence and there’s a limited number of neurologists, so we wanted to understand what this looks like in the US,” Dr. Win said.
“There is a need to understand the patient journey from primary care to neurology care, from presentation of a suspected neurological disorder to diagnosis, referral to a specialist, and the time elapsed before the specialist visit for Alzheimer’s disease, MS, and Parkinson’s disease in the US,” Dr. Win added.
Timely and accurate diagnoses of neurologic disorders can optimize treatment outcomes. Because many of these diseases are first detected during a visit with a primary care physician, it is important to understand the timeline from the initial visit to a specialist referral, the investigators noted.
Analyzing Trends in Specialist Referrals
Using claims data from the Optum Normative Health Information database, researchers identified 48,525 adults with Alzheimer’s disease, 26,431 with Parkinson’s disease, and 8169 with MS who received a diagnosis from a primary care physician between 2016 and 2021.
They examined the proportion, timing, and demographic factors associated with referrals from primary care clinicians or other healthcare providers to specialists including neurologists, neurosurgeons, psychiatrists, and geriatric medicine specialists.
Results showed that patients with Parkinson’s disease were referred to a specialist most often (53%), followed by those with MS (42%) and those with Alzheimer’s disease (27%).
Individuals with Alzheimer’s disease waited the longest for a specialist referral, with a median of 10 months between the time of referral and the first specialist visit compared with 5.7 months for patients with Parkinson’s disease and 2.6 months for MS patients.
“Some patients with common conditions like Alzheimer’s disease, MS, and Parkinson’s disease don’t see a neurologist, and when they do, it can take as long as 10 months,” said Dr. Win.
Using zip code heatmaps, researchers found that the proportion of referrals for all neurologic disorders was higher in the Midwest and Northeast, whereas patients in the South and West were less likely to receive a referral.
Referrals for Alzheimer’s disease were low nationwide, except for some areas of Michigan and New England. California had the lowest referral rate for MS, followed by regions in the South and Northeast. Patients with Parkinson’s disease living in the Midwest and Northeast were more likely than those in the West to receive a specialist referral.
Previous studies have reported regional shortages of neurologists, said Dr. Win. “Our data seem to correlate that in terms of the areas with lower referral patterns, but as to whether that is causative or correlative, we don’t know.”
Odds of referral were also influenced by demographic characteristics such as sex, age, race, and ethnicity, investigators found.
For example, there were fewer referrals with increasing age across all three neurologic disorders, and men were more likely than women to be referred for Alzheimer’s disease and Parkinson’s disease. Compared with White patients, Parkinson’s disease referrals were less likely among African American, Asian, and Hispanic patients and Alzheimer’s disease referrals were less common among Asian and Hispanic patients.
Insurance status also affected referrals. People with MS and Parkinson’s disease who had commercial insurance were referred more often than were those with Medicare Advantage, said Dr. Win.
She also noted, “Additional research is needed to understand how being referred or not being referred to a neurologist actually impacts patient treatment, care and outcomes.”
Neurology Challenges
Commenting on the research, Thomas Vidic, MD, a community neurologist in Elkhart, Indiana, and clinical professor of neurology at Indiana University School of Medicine at South Bend, said that he was surprised by the variation in wait times for patients.
This, he said, could reflect a study limitation or a higher comfort level among primary care doctors in treating dementia.
With respect to MS, Dr. Vidic said that he believes primary care physicians may not be uncertain about prescribing the approved medications for the disease because there are so many of them.
In addition, patients with Alzheimer’s disease are older and perhaps less accepting of being referred to a specialist that may be hours away.
The bottom line for Dr. Vidic, though, is the lack of specialists. “It comes back to the fact we’re not doing a good job of having community neurologists available to take care of these problems,” he said.
The issue of community neurologist shortages was underlined by the study’s findings about geographic gaps in specialist referrals across the country, he said.
Neurologists make up about 2% of the medical workforce and this has remained static for some time, Dr. Vidic noted. Meanwhile, people are living longer and developing more neurologic diseases.
Dr. Vidic also pointed to the lack of neurology training programs. “There has not been a significant change in the number of programs in the last 10-15 years,” he said.
Study funding was not disclosed. Dr. Win reports receiving personal compensation for serving as an employee of Genentech and has stock in Genentech. Dr. Vidic reports no relevant financial disclosures.
A version of this article appeared on Medscape.com.
FROM AAN 2024
New Genetic Variant May Guard Against Alzheimer’s in High-Risk Individuals
, new research suggests.
The variant occurs on the fibronectin 1 (FN1) gene, which expresses fibronectin, an adhesive glycoprotein that lines the blood vessels at the blood-brain barrier and controls substances that move in and out of the brain.
While fibronectin is normally present in the blood-brain barrier in small amounts, individuals with Alzheimer’s disease tend to have it in excess. Normally, patients with Alzheimer’s disease have amyloid deposits that collect in the brain, but those with the FN1 variant appear to have the ability to amyloid from the brain before symptoms begin.
The researchers estimate that 1%-3% of APOE4 carriers in the United States — roughly 200,000-620,000 people — may have the protective mutation.
“Alzheimer’s disease may get started with amyloid deposits in the brain, but the disease manifestations are the result of changes that happen after the deposits appear,” Caghan Kizil, PhD, of Columbia University Vagelos College of Physicians and Surgeons in New York City, and a co-leader of the study, said in a press release.
The findings were published online in Acta Neuropathologica,
Combing Genetic Data
To find potentially protective Alzheimer’s disease variants, the investigators sequenced the genomes of more than 3500 APOE4 carriers older than 70 years with and without Alzheimer’s disease from various ethnic backgrounds.
They identified two variants on the FN1 gene, rs116558455 and rs140926439, present in healthy APOE4 carriers, that protected the APOE4 carriers against Alzheimer’s disease.
After Dr. Kizil and colleagues published their findings in a preprint, another research group that included investigators from Stanford and Washington Universities replicated the Columbia results in an independent sample of more than 7000 APOE4 carriers aged 60 years who were of European descent and identified the same FN1 variant.
The two research groups then combined their data on 11,000 participants and found that the FN1 variant rs140926439 was associated with a significantly reduced risk for Alzheimer’s disease in APOE4 carriers (odds ratio, 0.29; P = .014). A secondary analysis showed that the variant delayed Alzheimer’s disease symptom onset by 3.4 years (P = .025).
The investigators hope to use these findings to develop therapies to protect APOE4 carriers against Alzheimer’s disease.
“Anything that reduces excess fibronectin should provide some protection, and a drug that does this could be a significant step forward in the fight against this debilitating condition,” Dr. Kizil said.
Study limitations included a lack of longitudinal data on the relationship between amyloid concentration and fibronectin and the fact that investigators conducted the studies in clinically assessed individuals. Given the rare occurrence of the FN1 mutation, researchers do not have neuropathological assessments of study participants with the variant.
The study was funded by the National Institute on Aging, the Schaefer Research Scholars Program Award, Taub Institute Grants for Emerging Research, the National Institute of General Medical Sciences, and the Thompson Family Foundation Program for Accelerated Medicine Exploration in Alzheimer’s Disease and Related Disorders of the Nervous System. There were no disclosures reported.
A version of this article appeared on Medscape.com.
, new research suggests.
The variant occurs on the fibronectin 1 (FN1) gene, which expresses fibronectin, an adhesive glycoprotein that lines the blood vessels at the blood-brain barrier and controls substances that move in and out of the brain.
While fibronectin is normally present in the blood-brain barrier in small amounts, individuals with Alzheimer’s disease tend to have it in excess. Normally, patients with Alzheimer’s disease have amyloid deposits that collect in the brain, but those with the FN1 variant appear to have the ability to amyloid from the brain before symptoms begin.
The researchers estimate that 1%-3% of APOE4 carriers in the United States — roughly 200,000-620,000 people — may have the protective mutation.
“Alzheimer’s disease may get started with amyloid deposits in the brain, but the disease manifestations are the result of changes that happen after the deposits appear,” Caghan Kizil, PhD, of Columbia University Vagelos College of Physicians and Surgeons in New York City, and a co-leader of the study, said in a press release.
The findings were published online in Acta Neuropathologica,
Combing Genetic Data
To find potentially protective Alzheimer’s disease variants, the investigators sequenced the genomes of more than 3500 APOE4 carriers older than 70 years with and without Alzheimer’s disease from various ethnic backgrounds.
They identified two variants on the FN1 gene, rs116558455 and rs140926439, present in healthy APOE4 carriers, that protected the APOE4 carriers against Alzheimer’s disease.
After Dr. Kizil and colleagues published their findings in a preprint, another research group that included investigators from Stanford and Washington Universities replicated the Columbia results in an independent sample of more than 7000 APOE4 carriers aged 60 years who were of European descent and identified the same FN1 variant.
The two research groups then combined their data on 11,000 participants and found that the FN1 variant rs140926439 was associated with a significantly reduced risk for Alzheimer’s disease in APOE4 carriers (odds ratio, 0.29; P = .014). A secondary analysis showed that the variant delayed Alzheimer’s disease symptom onset by 3.4 years (P = .025).
The investigators hope to use these findings to develop therapies to protect APOE4 carriers against Alzheimer’s disease.
“Anything that reduces excess fibronectin should provide some protection, and a drug that does this could be a significant step forward in the fight against this debilitating condition,” Dr. Kizil said.
Study limitations included a lack of longitudinal data on the relationship between amyloid concentration and fibronectin and the fact that investigators conducted the studies in clinically assessed individuals. Given the rare occurrence of the FN1 mutation, researchers do not have neuropathological assessments of study participants with the variant.
The study was funded by the National Institute on Aging, the Schaefer Research Scholars Program Award, Taub Institute Grants for Emerging Research, the National Institute of General Medical Sciences, and the Thompson Family Foundation Program for Accelerated Medicine Exploration in Alzheimer’s Disease and Related Disorders of the Nervous System. There were no disclosures reported.
A version of this article appeared on Medscape.com.
, new research suggests.
The variant occurs on the fibronectin 1 (FN1) gene, which expresses fibronectin, an adhesive glycoprotein that lines the blood vessels at the blood-brain barrier and controls substances that move in and out of the brain.
While fibronectin is normally present in the blood-brain barrier in small amounts, individuals with Alzheimer’s disease tend to have it in excess. Normally, patients with Alzheimer’s disease have amyloid deposits that collect in the brain, but those with the FN1 variant appear to have the ability to amyloid from the brain before symptoms begin.
The researchers estimate that 1%-3% of APOE4 carriers in the United States — roughly 200,000-620,000 people — may have the protective mutation.
“Alzheimer’s disease may get started with amyloid deposits in the brain, but the disease manifestations are the result of changes that happen after the deposits appear,” Caghan Kizil, PhD, of Columbia University Vagelos College of Physicians and Surgeons in New York City, and a co-leader of the study, said in a press release.
The findings were published online in Acta Neuropathologica,
Combing Genetic Data
To find potentially protective Alzheimer’s disease variants, the investigators sequenced the genomes of more than 3500 APOE4 carriers older than 70 years with and without Alzheimer’s disease from various ethnic backgrounds.
They identified two variants on the FN1 gene, rs116558455 and rs140926439, present in healthy APOE4 carriers, that protected the APOE4 carriers against Alzheimer’s disease.
After Dr. Kizil and colleagues published their findings in a preprint, another research group that included investigators from Stanford and Washington Universities replicated the Columbia results in an independent sample of more than 7000 APOE4 carriers aged 60 years who were of European descent and identified the same FN1 variant.
The two research groups then combined their data on 11,000 participants and found that the FN1 variant rs140926439 was associated with a significantly reduced risk for Alzheimer’s disease in APOE4 carriers (odds ratio, 0.29; P = .014). A secondary analysis showed that the variant delayed Alzheimer’s disease symptom onset by 3.4 years (P = .025).
The investigators hope to use these findings to develop therapies to protect APOE4 carriers against Alzheimer’s disease.
“Anything that reduces excess fibronectin should provide some protection, and a drug that does this could be a significant step forward in the fight against this debilitating condition,” Dr. Kizil said.
Study limitations included a lack of longitudinal data on the relationship between amyloid concentration and fibronectin and the fact that investigators conducted the studies in clinically assessed individuals. Given the rare occurrence of the FN1 mutation, researchers do not have neuropathological assessments of study participants with the variant.
The study was funded by the National Institute on Aging, the Schaefer Research Scholars Program Award, Taub Institute Grants for Emerging Research, the National Institute of General Medical Sciences, and the Thompson Family Foundation Program for Accelerated Medicine Exploration in Alzheimer’s Disease and Related Disorders of the Nervous System. There were no disclosures reported.
A version of this article appeared on Medscape.com.
FROM ACTA NEUROPATHOLOGICA
Antidepressants and Dementia Risk: Reassuring Data
TOPLINE:
, new research suggests.
METHODOLOGY:
- Investigators studied 5511 individuals (58% women; mean age, 71 years) from the Rotterdam study, an ongoing prospective population-based cohort study.
- Participants were free from dementia at baseline, and incident dementia was monitored from baseline until 2018 with repeated cognitive assessments using the Mini-Mental Status Examination (MMSE) and the Geriatric Mental Schedule, as well as MRIs.
- Information on participants’ antidepressant use was extracted from pharmacy records from 1992 until baseline (2002-2008).
- During a mean follow-up of 10 years, 12% of participants developed dementia.
TAKEAWAY:
- Overall, 17% of participants had used antidepressants during the roughly 10-year period prior to baseline, and 4.1% were still using antidepressants at baseline.
- Medication use at baseline was more common in women than in men (21% vs 18%), and use increased with age: From 2.1% in participants aged between 45 and 50 years to 4.5% in those older than 80 years.
- After adjustment for confounders, there was no association between antidepressant use and dementia risk (hazard ratio [HR], 1.14; 95% CI, 0.92-1.41), accelerated cognitive decline, or atrophy of white and gray matter.
- However, tricyclic antidepressant use was associated with increased dementia risk (HR, 1.36; 95% CI, 1.01-1.83) compared with the use of selective serotonin reuptake inhibitors (HR, 1.12; 95% CI, 0.81-1.54).
IN PRACTICE:
“Although prescription of antidepressant medication in older individuals, in particular those with some cognitive impairment, may have acute symptomatic anticholinergic effects that warrant consideration in clinical practice, our results show that long-term antidepressant use does not have lasting effects on cognition or brain health in older adults without indication of cognitive impairment,” the authors wrote.
SOURCE:
Frank J. Wolters, MD, of the Department of Epidemiology and the Department of Radiology and Nuclear Medicine and Alzheimer Center, Erasmus University Medical Center, Rotterdam, the Netherlands, was the senior author on this study that was published online in Alzheimer’s and Dementia.
LIMITATIONS:
Limitations included the concern that although exclusion of participants with MMSE < 26 at baseline prevented reversed causation (ie, antidepressant use in response to depression during the prodromal phase of dementia), it may have introduced selection bias by disregarding the effects of antidepressant use prior to baseline and excluding participants with lower education.
DISCLOSURES:
This study was conducted as part of the Netherlands Consortium of Dementia Cohorts, which receives funding in the context of Deltaplan Dementie from ZonMW Memorabel and Alzheimer Nederland. Further funding was also obtained from the Stichting Erasmus Trustfonds. This study was further supported by a 2020 NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation. The authors reported no conflicts of interest or relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
, new research suggests.
METHODOLOGY:
- Investigators studied 5511 individuals (58% women; mean age, 71 years) from the Rotterdam study, an ongoing prospective population-based cohort study.
- Participants were free from dementia at baseline, and incident dementia was monitored from baseline until 2018 with repeated cognitive assessments using the Mini-Mental Status Examination (MMSE) and the Geriatric Mental Schedule, as well as MRIs.
- Information on participants’ antidepressant use was extracted from pharmacy records from 1992 until baseline (2002-2008).
- During a mean follow-up of 10 years, 12% of participants developed dementia.
TAKEAWAY:
- Overall, 17% of participants had used antidepressants during the roughly 10-year period prior to baseline, and 4.1% were still using antidepressants at baseline.
- Medication use at baseline was more common in women than in men (21% vs 18%), and use increased with age: From 2.1% in participants aged between 45 and 50 years to 4.5% in those older than 80 years.
- After adjustment for confounders, there was no association between antidepressant use and dementia risk (hazard ratio [HR], 1.14; 95% CI, 0.92-1.41), accelerated cognitive decline, or atrophy of white and gray matter.
- However, tricyclic antidepressant use was associated with increased dementia risk (HR, 1.36; 95% CI, 1.01-1.83) compared with the use of selective serotonin reuptake inhibitors (HR, 1.12; 95% CI, 0.81-1.54).
IN PRACTICE:
“Although prescription of antidepressant medication in older individuals, in particular those with some cognitive impairment, may have acute symptomatic anticholinergic effects that warrant consideration in clinical practice, our results show that long-term antidepressant use does not have lasting effects on cognition or brain health in older adults without indication of cognitive impairment,” the authors wrote.
SOURCE:
Frank J. Wolters, MD, of the Department of Epidemiology and the Department of Radiology and Nuclear Medicine and Alzheimer Center, Erasmus University Medical Center, Rotterdam, the Netherlands, was the senior author on this study that was published online in Alzheimer’s and Dementia.
LIMITATIONS:
Limitations included the concern that although exclusion of participants with MMSE < 26 at baseline prevented reversed causation (ie, antidepressant use in response to depression during the prodromal phase of dementia), it may have introduced selection bias by disregarding the effects of antidepressant use prior to baseline and excluding participants with lower education.
DISCLOSURES:
This study was conducted as part of the Netherlands Consortium of Dementia Cohorts, which receives funding in the context of Deltaplan Dementie from ZonMW Memorabel and Alzheimer Nederland. Further funding was also obtained from the Stichting Erasmus Trustfonds. This study was further supported by a 2020 NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation. The authors reported no conflicts of interest or relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
, new research suggests.
METHODOLOGY:
- Investigators studied 5511 individuals (58% women; mean age, 71 years) from the Rotterdam study, an ongoing prospective population-based cohort study.
- Participants were free from dementia at baseline, and incident dementia was monitored from baseline until 2018 with repeated cognitive assessments using the Mini-Mental Status Examination (MMSE) and the Geriatric Mental Schedule, as well as MRIs.
- Information on participants’ antidepressant use was extracted from pharmacy records from 1992 until baseline (2002-2008).
- During a mean follow-up of 10 years, 12% of participants developed dementia.
TAKEAWAY:
- Overall, 17% of participants had used antidepressants during the roughly 10-year period prior to baseline, and 4.1% were still using antidepressants at baseline.
- Medication use at baseline was more common in women than in men (21% vs 18%), and use increased with age: From 2.1% in participants aged between 45 and 50 years to 4.5% in those older than 80 years.
- After adjustment for confounders, there was no association between antidepressant use and dementia risk (hazard ratio [HR], 1.14; 95% CI, 0.92-1.41), accelerated cognitive decline, or atrophy of white and gray matter.
- However, tricyclic antidepressant use was associated with increased dementia risk (HR, 1.36; 95% CI, 1.01-1.83) compared with the use of selective serotonin reuptake inhibitors (HR, 1.12; 95% CI, 0.81-1.54).
IN PRACTICE:
“Although prescription of antidepressant medication in older individuals, in particular those with some cognitive impairment, may have acute symptomatic anticholinergic effects that warrant consideration in clinical practice, our results show that long-term antidepressant use does not have lasting effects on cognition or brain health in older adults without indication of cognitive impairment,” the authors wrote.
SOURCE:
Frank J. Wolters, MD, of the Department of Epidemiology and the Department of Radiology and Nuclear Medicine and Alzheimer Center, Erasmus University Medical Center, Rotterdam, the Netherlands, was the senior author on this study that was published online in Alzheimer’s and Dementia.
LIMITATIONS:
Limitations included the concern that although exclusion of participants with MMSE < 26 at baseline prevented reversed causation (ie, antidepressant use in response to depression during the prodromal phase of dementia), it may have introduced selection bias by disregarding the effects of antidepressant use prior to baseline and excluding participants with lower education.
DISCLOSURES:
This study was conducted as part of the Netherlands Consortium of Dementia Cohorts, which receives funding in the context of Deltaplan Dementie from ZonMW Memorabel and Alzheimer Nederland. Further funding was also obtained from the Stichting Erasmus Trustfonds. This study was further supported by a 2020 NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation. The authors reported no conflicts of interest or relevant financial relationships.
A version of this article appeared on Medscape.com.
Mandatory DMV Reporting Tied to Dementia Underdiagnosis
, new research suggests.
Investigators found that primary care physicians (PCPs) in states with clinician reporting mandates had a 59% higher probability of underdiagnosing dementia compared with their counterparts in states that require patients to self-report or that have no reporting mandates.
“Our findings in this cross-sectional study raise concerns about potential adverse effects of mandatory clinician reporting for dementia diagnosis and underscore the need for careful consideration of the effect of such policies,” wrote the investigators, led by Soeren Mattke, MD, DSc, director of the USC Brain Health Observatory and research professor of economics at the University of Southern California, Los Angeles.
The study was published online in JAMA Network Open.
Lack of Guidance
As the US population ages, the number of older drivers is increasing, with 55.8 million drivers 65 years old or older. Approximately 7 million people in this age group have dementia — an estimate that is expected to increase to nearly 12 million by 2040.
The aging population raises a “critical policy question” about how to ensure road safety. Although the American Medical Association’s Code of Ethics outlines a physician’s obligation to identify drivers with medical impairments that impede safe driving, guidance restricting cognitively impaired drivers from driving is lacking.
In addition, evidence as to whether cognitive impairment indeed poses a threat to driving safety is mixed and has led to a lack of uniform policies with respect to reporting dementia.
Four states explicitly require clinicians to report dementia diagnoses to the DMV, which will then determine the patient’s fitness to drive, whereas 14 states require people with dementia to self-report. The remaining states have no explicit reporting requirements.
The issue of mandatory reporting is controversial, the researchers noted. On the one hand, physicians could protect patients and others by reporting potentially unsafe drivers.
On the other hand, evidence of an association with lower accident risks in patients with dementia is sparse and mandatory reporting may adversely affect physician-patient relationships. Empirical evidence for unintended consequences of reporting laws is lacking.
To examine the potential link between dementia underdiagnosis and mandatory reporting policies, the investigators analyzed the 100% data from the Medicare fee-for-service program and Medicare Advantage plans from 2017 to 2019, which included 223,036 PCPs with a panel of 25 or more Medicare patients.
The researchers examined dementia diagnosis rates in the patient panel of PCPs, rather than neurologists or gerontologists, regardless of who documented the diagnosis. Dr. Mattke said that it is possible that the diagnosis was established after referral to a specialist.
Each physician’s expected number of dementia cases was estimated using a predictive model based on patient characteristics. The researchers then compared the estimate with observed dementia diagnoses, thereby identifying clinicians who underdiagnosed dementia after sampling errors were accounted for.
‘Heavy-Handed Interference’
The researchers adjusted for several covariates potentially associated with a clinician’s probability of underdiagnosing dementia. These included sex, office location, practice specialty, racial/ethnic composition of the patient panel, and percentage of patients dually eligible for Medicare and Medicaid. The table shows PCP characteristics.
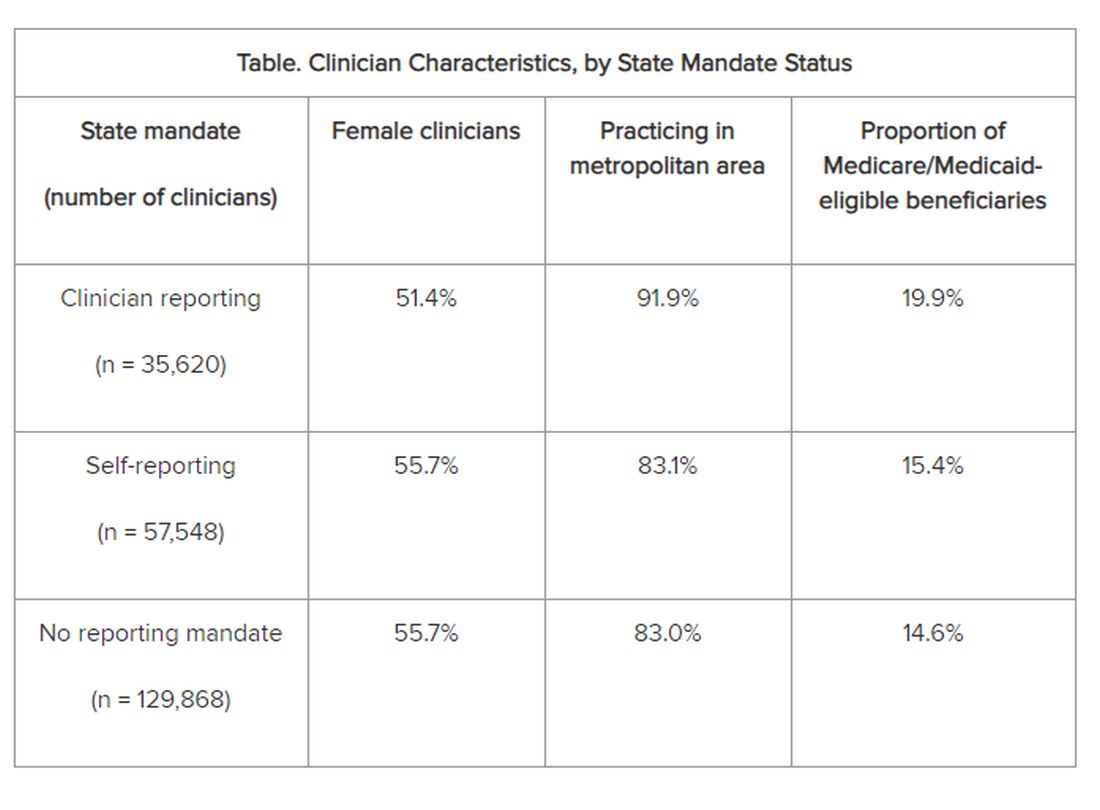
Adjusted results showed that PCPs practicing in states with clinician reporting mandates had a 12.4% (95% confidence interval [CI], 10.5%-14.2%) probability of underdiagnosing dementia versus 7.8% (95% CI, 6.9%-8.7%) in states with self-reporting and 7.7% (95% CI, 6.9%-8.4%) in states with no mandates, translating into a 4–percentage point difference (P < .001).
“Our study is the first to provide empirical evidence for the potential adverse effects of reporting policies,” the researchers noted. “Although we found that some clinicians underdiagnosed dementia regardless of state mandates, the key finding of this study reveals that primary care clinicians who practice in states with clinician reporting mandates were 59% more likely to do so…compared with those states with no reporting requirements…or driver self-reporting requirements.”
The investigators suggested that one potential explanation for underdiagnosis is patient resistance to cognitive testing. If patients were aware that the clinician was obligated by law to report their dementia diagnosis to the DMV, “they might be more inclined to conceal their symptoms or refuse further assessments, in addition to the general stigma and resistance to a formal assessment after a positive dementia screening result.”
“The findings suggest that policymakers might want to rethink those physician reporting mandates, since we also could not find conclusive evidence that they improve road safety,” Dr. Mattke said. “Maybe patients and their physicians can arrive at a sensible approach to determine driving fitness without such heavy-handed interference.”
However, he cautioned that the findings are not definitive and further study is needed before firm recommendations either for or against mandatory reporting.
In addition, the researchers noted several study limitations. One is that dementia underdiagnosis may also be associated with factors not captured in their model, including physician-patient relationships, health literacy, or language barriers.
However, Dr. Mattke noted, “ my sense is that those unobservable factors are not systematically related to state reporting policies and having omitted them would therefore not bias our results.”
Experts Weigh In
Commenting on the research, Morgan Daven, MA, the Alzheimer’s Association vice president of health systems, said that dementia is widely and significantly underdiagnosed, and not only in the states with dementia reporting mandates. Many factors may contribute to underdiagnosis, and although the study shows an association between reporting mandates and underdiagnosis, it does not demonstrate causation.
That said, Mr. Daven added, “fear and stigma related to dementia may inhibit the clinician, the patient, and their family from pursuing detection and diagnosis for dementia. As a society, we need to address dementia fear and stigma for all parties.”
He noted that useful tools include healthcare policies, workforce training, public awareness and education, and public policies to mitigate fear and stigma and their negative effects on diagnosis, care, support, and communication.
A potential study limitation is that it relied only on diagnoses by PCPs. Mr. Daven noted that the diagnosis of Alzheimer’ disease — the most common cause of dementia — is confirmation of amyloid buildup via a biomarker test, using PET or cerebrospinal fluid analysis.
“Both of these tests are extremely limited in their use and accessibility in a primary care setting. Inclusion of diagnoses by dementia specialists would provide a more complete picture,” he said.
Mr. Daven added that the Alzheimer’s Association encourages families to proactively discuss driving and other disease-related safety concerns as soon as possible. The Alzheimer’s Association Dementia and Driving webpage offers tips and strategies to discuss driving concerns with a family member.
In an accompanying editorial, Donald Redelmeier, MD, MS(HSR), and Vidhi Bhatt, BSc, both of the Department of Medicine, University of Toronto, differentiate the mandate for physicians to warn patients with dementia about traffic safety from the mandate for reporting child maltreatment, gunshot victims, or communicable diseases. They noted that mandated warnings “are not easy, can engender patient dissatisfaction, and need to be handled with tact.”
Yet, they pointed out, “breaking bad news is what practicing medicine entails.” They emphasized that, regardless of government mandates, “counseling patients for more road safety is an essential skill for clinicians in diverse states who hope to help their patients avoid becoming more traffic statistics.”
Research reported in this publication was supported by Genentech, a member of the Roche Group, and a grant from the National Institute on Aging of the National Institutes of Health. Dr. Mattke reported receiving grants from Genentech for a research contract with USC during the conduct of the study; personal fees from Eisai, Biogen, C2N, Novo Nordisk, Novartis, and Roche Genentech; and serving on the Senscio Systems board of directors, ALZpath scientific advisory board, AiCure scientific advisory board, and Boston Millennia Partners scientific advisory board outside the submitted work. The other authors’ disclosures are listed on the original paper. The editorial was supported by the Canada Research Chair in Medical Decision Sciences, the Canadian Institutes of Health Research, Kimel-Schatzky Traumatic Brain Injury Research Fund, and the Graduate Diploma Program in Health Research at the University of Toronto. The editorial authors report no other relevant financial relationships.
A version of this article appeared on Medscape.com.
, new research suggests.
Investigators found that primary care physicians (PCPs) in states with clinician reporting mandates had a 59% higher probability of underdiagnosing dementia compared with their counterparts in states that require patients to self-report or that have no reporting mandates.
“Our findings in this cross-sectional study raise concerns about potential adverse effects of mandatory clinician reporting for dementia diagnosis and underscore the need for careful consideration of the effect of such policies,” wrote the investigators, led by Soeren Mattke, MD, DSc, director of the USC Brain Health Observatory and research professor of economics at the University of Southern California, Los Angeles.
The study was published online in JAMA Network Open.
Lack of Guidance
As the US population ages, the number of older drivers is increasing, with 55.8 million drivers 65 years old or older. Approximately 7 million people in this age group have dementia — an estimate that is expected to increase to nearly 12 million by 2040.
The aging population raises a “critical policy question” about how to ensure road safety. Although the American Medical Association’s Code of Ethics outlines a physician’s obligation to identify drivers with medical impairments that impede safe driving, guidance restricting cognitively impaired drivers from driving is lacking.
In addition, evidence as to whether cognitive impairment indeed poses a threat to driving safety is mixed and has led to a lack of uniform policies with respect to reporting dementia.
Four states explicitly require clinicians to report dementia diagnoses to the DMV, which will then determine the patient’s fitness to drive, whereas 14 states require people with dementia to self-report. The remaining states have no explicit reporting requirements.
The issue of mandatory reporting is controversial, the researchers noted. On the one hand, physicians could protect patients and others by reporting potentially unsafe drivers.
On the other hand, evidence of an association with lower accident risks in patients with dementia is sparse and mandatory reporting may adversely affect physician-patient relationships. Empirical evidence for unintended consequences of reporting laws is lacking.
To examine the potential link between dementia underdiagnosis and mandatory reporting policies, the investigators analyzed the 100% data from the Medicare fee-for-service program and Medicare Advantage plans from 2017 to 2019, which included 223,036 PCPs with a panel of 25 or more Medicare patients.
The researchers examined dementia diagnosis rates in the patient panel of PCPs, rather than neurologists or gerontologists, regardless of who documented the diagnosis. Dr. Mattke said that it is possible that the diagnosis was established after referral to a specialist.
Each physician’s expected number of dementia cases was estimated using a predictive model based on patient characteristics. The researchers then compared the estimate with observed dementia diagnoses, thereby identifying clinicians who underdiagnosed dementia after sampling errors were accounted for.
‘Heavy-Handed Interference’
The researchers adjusted for several covariates potentially associated with a clinician’s probability of underdiagnosing dementia. These included sex, office location, practice specialty, racial/ethnic composition of the patient panel, and percentage of patients dually eligible for Medicare and Medicaid. The table shows PCP characteristics.
Adjusted results showed that PCPs practicing in states with clinician reporting mandates had a 12.4% (95% confidence interval [CI], 10.5%-14.2%) probability of underdiagnosing dementia versus 7.8% (95% CI, 6.9%-8.7%) in states with self-reporting and 7.7% (95% CI, 6.9%-8.4%) in states with no mandates, translating into a 4–percentage point difference (P < .001).
“Our study is the first to provide empirical evidence for the potential adverse effects of reporting policies,” the researchers noted. “Although we found that some clinicians underdiagnosed dementia regardless of state mandates, the key finding of this study reveals that primary care clinicians who practice in states with clinician reporting mandates were 59% more likely to do so…compared with those states with no reporting requirements…or driver self-reporting requirements.”
The investigators suggested that one potential explanation for underdiagnosis is patient resistance to cognitive testing. If patients were aware that the clinician was obligated by law to report their dementia diagnosis to the DMV, “they might be more inclined to conceal their symptoms or refuse further assessments, in addition to the general stigma and resistance to a formal assessment after a positive dementia screening result.”
“The findings suggest that policymakers might want to rethink those physician reporting mandates, since we also could not find conclusive evidence that they improve road safety,” Dr. Mattke said. “Maybe patients and their physicians can arrive at a sensible approach to determine driving fitness without such heavy-handed interference.”
However, he cautioned that the findings are not definitive and further study is needed before firm recommendations either for or against mandatory reporting.
In addition, the researchers noted several study limitations. One is that dementia underdiagnosis may also be associated with factors not captured in their model, including physician-patient relationships, health literacy, or language barriers.
However, Dr. Mattke noted, “ my sense is that those unobservable factors are not systematically related to state reporting policies and having omitted them would therefore not bias our results.”
Experts Weigh In
Commenting on the research, Morgan Daven, MA, the Alzheimer’s Association vice president of health systems, said that dementia is widely and significantly underdiagnosed, and not only in the states with dementia reporting mandates. Many factors may contribute to underdiagnosis, and although the study shows an association between reporting mandates and underdiagnosis, it does not demonstrate causation.
That said, Mr. Daven added, “fear and stigma related to dementia may inhibit the clinician, the patient, and their family from pursuing detection and diagnosis for dementia. As a society, we need to address dementia fear and stigma for all parties.”
He noted that useful tools include healthcare policies, workforce training, public awareness and education, and public policies to mitigate fear and stigma and their negative effects on diagnosis, care, support, and communication.
A potential study limitation is that it relied only on diagnoses by PCPs. Mr. Daven noted that the diagnosis of Alzheimer’ disease — the most common cause of dementia — is confirmation of amyloid buildup via a biomarker test, using PET or cerebrospinal fluid analysis.
“Both of these tests are extremely limited in their use and accessibility in a primary care setting. Inclusion of diagnoses by dementia specialists would provide a more complete picture,” he said.
Mr. Daven added that the Alzheimer’s Association encourages families to proactively discuss driving and other disease-related safety concerns as soon as possible. The Alzheimer’s Association Dementia and Driving webpage offers tips and strategies to discuss driving concerns with a family member.
In an accompanying editorial, Donald Redelmeier, MD, MS(HSR), and Vidhi Bhatt, BSc, both of the Department of Medicine, University of Toronto, differentiate the mandate for physicians to warn patients with dementia about traffic safety from the mandate for reporting child maltreatment, gunshot victims, or communicable diseases. They noted that mandated warnings “are not easy, can engender patient dissatisfaction, and need to be handled with tact.”
Yet, they pointed out, “breaking bad news is what practicing medicine entails.” They emphasized that, regardless of government mandates, “counseling patients for more road safety is an essential skill for clinicians in diverse states who hope to help their patients avoid becoming more traffic statistics.”
Research reported in this publication was supported by Genentech, a member of the Roche Group, and a grant from the National Institute on Aging of the National Institutes of Health. Dr. Mattke reported receiving grants from Genentech for a research contract with USC during the conduct of the study; personal fees from Eisai, Biogen, C2N, Novo Nordisk, Novartis, and Roche Genentech; and serving on the Senscio Systems board of directors, ALZpath scientific advisory board, AiCure scientific advisory board, and Boston Millennia Partners scientific advisory board outside the submitted work. The other authors’ disclosures are listed on the original paper. The editorial was supported by the Canada Research Chair in Medical Decision Sciences, the Canadian Institutes of Health Research, Kimel-Schatzky Traumatic Brain Injury Research Fund, and the Graduate Diploma Program in Health Research at the University of Toronto. The editorial authors report no other relevant financial relationships.
A version of this article appeared on Medscape.com.
, new research suggests.
Investigators found that primary care physicians (PCPs) in states with clinician reporting mandates had a 59% higher probability of underdiagnosing dementia compared with their counterparts in states that require patients to self-report or that have no reporting mandates.
“Our findings in this cross-sectional study raise concerns about potential adverse effects of mandatory clinician reporting for dementia diagnosis and underscore the need for careful consideration of the effect of such policies,” wrote the investigators, led by Soeren Mattke, MD, DSc, director of the USC Brain Health Observatory and research professor of economics at the University of Southern California, Los Angeles.
The study was published online in JAMA Network Open.
Lack of Guidance
As the US population ages, the number of older drivers is increasing, with 55.8 million drivers 65 years old or older. Approximately 7 million people in this age group have dementia — an estimate that is expected to increase to nearly 12 million by 2040.
The aging population raises a “critical policy question” about how to ensure road safety. Although the American Medical Association’s Code of Ethics outlines a physician’s obligation to identify drivers with medical impairments that impede safe driving, guidance restricting cognitively impaired drivers from driving is lacking.
In addition, evidence as to whether cognitive impairment indeed poses a threat to driving safety is mixed and has led to a lack of uniform policies with respect to reporting dementia.
Four states explicitly require clinicians to report dementia diagnoses to the DMV, which will then determine the patient’s fitness to drive, whereas 14 states require people with dementia to self-report. The remaining states have no explicit reporting requirements.
The issue of mandatory reporting is controversial, the researchers noted. On the one hand, physicians could protect patients and others by reporting potentially unsafe drivers.
On the other hand, evidence of an association with lower accident risks in patients with dementia is sparse and mandatory reporting may adversely affect physician-patient relationships. Empirical evidence for unintended consequences of reporting laws is lacking.
To examine the potential link between dementia underdiagnosis and mandatory reporting policies, the investigators analyzed the 100% data from the Medicare fee-for-service program and Medicare Advantage plans from 2017 to 2019, which included 223,036 PCPs with a panel of 25 or more Medicare patients.
The researchers examined dementia diagnosis rates in the patient panel of PCPs, rather than neurologists or gerontologists, regardless of who documented the diagnosis. Dr. Mattke said that it is possible that the diagnosis was established after referral to a specialist.
Each physician’s expected number of dementia cases was estimated using a predictive model based on patient characteristics. The researchers then compared the estimate with observed dementia diagnoses, thereby identifying clinicians who underdiagnosed dementia after sampling errors were accounted for.
‘Heavy-Handed Interference’
The researchers adjusted for several covariates potentially associated with a clinician’s probability of underdiagnosing dementia. These included sex, office location, practice specialty, racial/ethnic composition of the patient panel, and percentage of patients dually eligible for Medicare and Medicaid. The table shows PCP characteristics.
Adjusted results showed that PCPs practicing in states with clinician reporting mandates had a 12.4% (95% confidence interval [CI], 10.5%-14.2%) probability of underdiagnosing dementia versus 7.8% (95% CI, 6.9%-8.7%) in states with self-reporting and 7.7% (95% CI, 6.9%-8.4%) in states with no mandates, translating into a 4–percentage point difference (P < .001).
“Our study is the first to provide empirical evidence for the potential adverse effects of reporting policies,” the researchers noted. “Although we found that some clinicians underdiagnosed dementia regardless of state mandates, the key finding of this study reveals that primary care clinicians who practice in states with clinician reporting mandates were 59% more likely to do so…compared with those states with no reporting requirements…or driver self-reporting requirements.”
The investigators suggested that one potential explanation for underdiagnosis is patient resistance to cognitive testing. If patients were aware that the clinician was obligated by law to report their dementia diagnosis to the DMV, “they might be more inclined to conceal their symptoms or refuse further assessments, in addition to the general stigma and resistance to a formal assessment after a positive dementia screening result.”
“The findings suggest that policymakers might want to rethink those physician reporting mandates, since we also could not find conclusive evidence that they improve road safety,” Dr. Mattke said. “Maybe patients and their physicians can arrive at a sensible approach to determine driving fitness without such heavy-handed interference.”
However, he cautioned that the findings are not definitive and further study is needed before firm recommendations either for or against mandatory reporting.
In addition, the researchers noted several study limitations. One is that dementia underdiagnosis may also be associated with factors not captured in their model, including physician-patient relationships, health literacy, or language barriers.
However, Dr. Mattke noted, “ my sense is that those unobservable factors are not systematically related to state reporting policies and having omitted them would therefore not bias our results.”
Experts Weigh In
Commenting on the research, Morgan Daven, MA, the Alzheimer’s Association vice president of health systems, said that dementia is widely and significantly underdiagnosed, and not only in the states with dementia reporting mandates. Many factors may contribute to underdiagnosis, and although the study shows an association between reporting mandates and underdiagnosis, it does not demonstrate causation.
That said, Mr. Daven added, “fear and stigma related to dementia may inhibit the clinician, the patient, and their family from pursuing detection and diagnosis for dementia. As a society, we need to address dementia fear and stigma for all parties.”
He noted that useful tools include healthcare policies, workforce training, public awareness and education, and public policies to mitigate fear and stigma and their negative effects on diagnosis, care, support, and communication.
A potential study limitation is that it relied only on diagnoses by PCPs. Mr. Daven noted that the diagnosis of Alzheimer’ disease — the most common cause of dementia — is confirmation of amyloid buildup via a biomarker test, using PET or cerebrospinal fluid analysis.
“Both of these tests are extremely limited in their use and accessibility in a primary care setting. Inclusion of diagnoses by dementia specialists would provide a more complete picture,” he said.
Mr. Daven added that the Alzheimer’s Association encourages families to proactively discuss driving and other disease-related safety concerns as soon as possible. The Alzheimer’s Association Dementia and Driving webpage offers tips and strategies to discuss driving concerns with a family member.
In an accompanying editorial, Donald Redelmeier, MD, MS(HSR), and Vidhi Bhatt, BSc, both of the Department of Medicine, University of Toronto, differentiate the mandate for physicians to warn patients with dementia about traffic safety from the mandate for reporting child maltreatment, gunshot victims, or communicable diseases. They noted that mandated warnings “are not easy, can engender patient dissatisfaction, and need to be handled with tact.”
Yet, they pointed out, “breaking bad news is what practicing medicine entails.” They emphasized that, regardless of government mandates, “counseling patients for more road safety is an essential skill for clinicians in diverse states who hope to help their patients avoid becoming more traffic statistics.”
Research reported in this publication was supported by Genentech, a member of the Roche Group, and a grant from the National Institute on Aging of the National Institutes of Health. Dr. Mattke reported receiving grants from Genentech for a research contract with USC during the conduct of the study; personal fees from Eisai, Biogen, C2N, Novo Nordisk, Novartis, and Roche Genentech; and serving on the Senscio Systems board of directors, ALZpath scientific advisory board, AiCure scientific advisory board, and Boston Millennia Partners scientific advisory board outside the submitted work. The other authors’ disclosures are listed on the original paper. The editorial was supported by the Canada Research Chair in Medical Decision Sciences, the Canadian Institutes of Health Research, Kimel-Schatzky Traumatic Brain Injury Research Fund, and the Graduate Diploma Program in Health Research at the University of Toronto. The editorial authors report no other relevant financial relationships.
A version of this article appeared on Medscape.com.
From JAMA Network Open
Does ‘Brain Training’ Really Improve Cognition and Forestall Cognitive Decline?
The concept that cognitive health can be preserved or improved is often expressed as “use it or lose it.” Numerous modifiable risk factors are associated with “losing” cognitive abilities with age, and a cognitively active lifestyle may have a protective effect.
But what is a “cognitively active lifestyle” — do crosswords and Sudoku count?
One popular approach is “brain training.” While not a scientific term with an established definition, it “typically refers to tasks or drills that are designed to strengthen specific aspects of one’s cognitive function,” explained Yuko Hara, PhD, director of Aging and Alzheimer’s Prevention at the Alzheimer’s Drug Discovery Foundation.
Manuel Montero-Odasso, MD, PhD, director of the Gait and Brain Lab, Parkwood Institute, London, Ontario, Canada, elaborated: “Cognitive training involves performing a definitive task or set of tasks where you increase attentional demands to improve focus and concentration and memory. You try to execute the new things that you’ve learned and to remember them.”
In a commentary published by this news organization in 2022, neuroscientist Michael Merzenich, PhD, professor emeritus at University of California San Francisco, said that growing a person’s cognitive reserve and actively managing brain health can play an important role in preventing or delaying Alzheimer’s disease. Important components of this include brain training and physical exercise.
Brain Training: Mechanism of Action
Dr. Montero-Odasso, team leader at the Canadian Consortium on Neurodegeneration in Aging and team co-leader at the Ontario Neurodegenerative Research Initiative, explained that cognitive training creates new synapses in the brain, thus stimulating neuroplasticity.
“When we try to activate networks mainly in the frontal lobe, the prefrontal cortex, a key mechanism underlying this process is enhancement of the synaptic plasticity at excitatory synapses, which connect neurons into networks; in other words, we generate new synapses, and that’s how we enhance brain health and cognitive abilities.”
The more neural connections, the greater the processing speed of the brain, he continued. “Cognitive training creates an anatomical change in the brain.”
Executive functions, which include attention, inhibition, planning, and multitasking, are regulated predominantly by the prefrontal cortex. Damage in this region of the brain is also implicated in dementia. Alterations in the connectivity of this area are associated with cognitive impairment, independent of other structural pathological aberrations (eg, gray matter atrophy). These patterns may precede structural pathological changes associated with cognitive impairment and dementia.
Neuroplasticity changes have been corroborated through neuroimaging, which has demonstrated that after cognitive training, there is more activation in the prefrontal cortex that correlates with new synapses, Dr. Montero-Odasso said.
Henry Mahncke, PhD, CEO of the brain training company Posit Science/BrainHQ, explained that early research was conducted on rodents and monkeys, with Dr. Merzenich as one of the leading pioneers in developing the concept of brain plasticity. Dr. Merzenich cofounded Posit Science and is currently its chief scientific officer.
Dr. Mahncke recounted that as a graduate student, he had worked with Dr. Merzenich researching brain plasticity. When Dr. Merzenich founded Posit Science, he asked Dr. Mahncke to join the company to help develop approaches to enhance brain plasticity — building the brain-training exercises and running the clinical trials.
“It’s now well understood that the brain can rewire itself at any age and in almost any condition,” Dr. Mahncke said. “In kids and in younger and older adults, whether with healthy or unhealthy brains, the fundamental way the brain works is by continually rewiring and rebuilding itself, based on what we ask it to do.”
Dr. Mahncke said.
Unsubstantiated Claims and Controversy
Brain training is not without controversy, Dr. Hara pointed out. “Some manufacturers of brain games have been criticized and even fined for making unsubstantiated claims,” she said.
A 2016 review found that brain-training interventions do improve performance on specific trained tasks, but there is less evidence that they improve performance on closely related tasks and little evidence that training improves everyday cognitive performance. A 2017 review reached similar conclusions, calling evidence regarding prevention or delay of cognitive decline or dementia through brain games “insufficient,” although cognitive training could “improve cognition in the domain trained.”
“The general consensus is that for most brain-training programs, people may get better at specific tasks through practice, but these improvements don’t necessarily translate into improvement in other tasks that require other cognitive domains or prevention of dementia or age-related cognitive decline,” Dr. Hara said.
She noted that most brain-training programs “have not been rigorously tested in clinical trials” — although some, such as those featured in the ACTIVE trial, did show evidence of effectiveness.
Dr. Mahncke agreed. “Asking whether brain training works is like asking whether small molecules improve health,” he said noting that some brain-training programs are nonsense and not evidence based. He believes that his company’s product, BrainHQ, and some others are “backed by robust evidence in their ability to stave off, slow, or even reverse cognitive changes.”
BrainHQ is a web-based brain game suite that can be used independently as an app or in group settings (classes and webinars) and is covered by some Medicare Advantage insurance plans. It encompasses “dozens of individual brain-training exercises, linked by a common thread. Each one is intensively designed to make the brain faster and more accurate,” said Dr. Mahncke.
He explained that human brains “get noisy as people get older, like a radio which is wearing out, so there’s static in the background. This makes the music hard to hear, and in the case of the human brain, it makes it difficult to pay attention.” The exercises are “designed to tamp down the ‘noise,’ speed up the brain, and make information processing more accurate.”
Dr. Mahncke called this a “bottom-up” approach, in contrast to many previous cognitive-training approaches that come from the brain injury rehabilitation field. They teach “top-down” skills and strategies designed to compensate for deficits in specific domains, such as reading, concentration, or fine motor skills.
By contrast, the approach of BrainHQ is “to improve the overall processing system of the brain with speed, attention, working memory, and executive function, which will in turn impact all skills and activities.”
Supporting Evidence
Dr. Mahncke cited several supporting studies. For example, the IMPACT study randomized 487 adults (aged ≥ 65 years) to receive either a brain plasticity–based computerized cognitive training program (BrainHQ) or a novelty- and intensity-matched general cognitive stimulation treatment program (intervention and control group, respectively) for an 8-week period.
Those who underwent brain training showed significantly greater improvement in the repeatable Battery for the Assessment of Neuropsychological Status (RBANS Auditory Memory/Attention) compared with those in the control group (3.9 vs 1.8, respectively; P =.02). The intervention group also showed significant improvements on multiple secondary measures of attention and memory. The magnitude of the effect sizes suggests that the results are clinically significant, according to the authors.
The ACTIVE study tested the effects of different cognitive training programs on cognitive function and time to dementia. The researchers randomized 2802 healthy older adults (mean age, 74 years) to a control group with no cognitive training or one of three brain-training groups comprising:
1. In-person training on verbal memory skills
2. In-person training on reasoning and problem-solving
3. Computer-based speed-of-processing training on visual attention
Participants in the training groups completed 10 sessions, each lasting 60-75 minutes, over a 5- to 6-week period. A random subsample of each training group was selected to receive “booster” sessions, with four-session booster training delivered at 11 and 35 months. All study participants completed follow-up tests of cognition and function after 1, 2, 3, 5, and 10 years.
At the end of 10 years, those assigned to the speed-of-processing training, now part of BrainHQ, had a 29% lower risk for dementia than those in the control group who received no training. No reduction was found in the memory or reasoning training groups. Participants who completed the “booster” sessions had an even greater reduction: Each additional booster session was associated with a 10% lower risk for dementia.
Dr. Montero-Odasso was involved in the SYNERGIC study that randomized 175 participants with mild cognitive impairment (MCI; average age, 73 years) to one of five study arms:
1. Multidomain intervention with exercise, cognitive training, and vitamin D
2. Exercise, cognitive training, and placebo
3. Exercise, sham cognitive training, and vitamin D
4. Exercise, sham cognitive training, and placebo
5. Control group with balance-toning exercise, sham cognitive training, and placebo
“Sham” cognitive training consisted of alternating between two tasks (touristic search and video watching) performed on a tablet, with the same time exposure as the intervention training.
The researchers found that after 6 months of interventions, all active arms with aerobic-resistance exercise showed improvement in the ADAS-Cog-13, an established outcome to evaluate dementia treatments, when compared with the control group — regardless of the addition of cognitive training or vitamin D.
Compared with exercise alone (arms 3 and 4), those who did exercise plus cognitive training (arms 1 and 2) showed greater improvements in their ADAS-Cog-13l score, with a mean difference of −1.45 points (P = .02). The greatest improvement was seen in those who underwent the multidomain intervention in arm 1.
The authors noted that the mean 2.64-point improvement seen in the ADAS-Cog-13 for the multidomain intervention is actually larger than changes seen in previous pharmaceutical trials among individuals with MCI or mild dementia and “approaches” the three points considered clinically meaningful.
“We found that older adults with MCI who received aerobic-resistance exercise with sequential computerized cognitive training significantly improved cognition,” Dr. Montero-Odasso said. “The cognitive training we used was called Neuropeak, a multidomain lifestyle training delivered through a web-based platform developed by our co-leader Louis Bherer at Université de Montréal.”
He explained that the purpose “is to challenge your brain to the point where you need to make an effort to remember things, pay attention, and later to execute tasks. The evidence from clinical trials, including ours, shows this type of brain challenge is effective in slowing and even reversing cognitive decline.”
A follow-up study, SYNERGIC 2.0, is ongoing.
Puzzles, Board Games, and New Challenges
Formal brain-training programs aren’t the only way to improve brain plasticity, Dr. Hara said. Observational studies suggested an association between improved cognitive performance and/or lower dementia risk and engaging in number and word puzzles, such as crosswords, cards, or board games.
Some studies suggested that older adults who use technology might also protect their cognitive reserve. Dr. Hara cited a US longitudinal study of more than 18,000 older adults suggesting that regular Internet users had roughly half the risk for dementia compared to nonregular Internet users. Estimates of daily Internet use suggested a U-shaped relationship with dementia with 0.1-2.0 hours daily (excluding time spent watching television or movies online) associated with the lowest risk. Similar associations between Internet use and a lower risk for cognitive decline have been reported in the United Kingdom and Europe.
“Engaging in mentally stimulating activities can increase ‘cognitive reserve’ — meaning, capacity of the brain to resist the effects of age-related changes or disease-related pathology, such that one can maintain cognitive function for longer,” Dr. Hara said. “Cognitively stimulating activities, regardless of the type, may help delay the onset of cognitive decline.”
She listed several examples of activities that are stimulating to the brain, including learning a new game or puzzle, a new language, or a new dance, and learning how to play a musical instrument.
Dr. Montero-Odasso emphasized that the “newness” is key to increasing and preserving cognitive reserve. “Just surfing the Internet, playing word or board games, or doing crossword puzzles won’t be enough if you’ve been doing these things all your life,” he said. “It won’t hurt, of course, but it won’t necessarily increase your cognitive abilities.
“For example, a person who regularly engages in public speaking may not improve cognition by taking a public-speaking course, but someone who has never spoken before an audience might show cognitive improvements as a result of learning a new skill,” he said. “Or someone who knows several languages already might gain from learning a brand-new language.”
He cited research supporting the benefits of dancing, which he called “an ideal activity because it’s physical, so it provides the exercise that’s been associated with improved cognition. But it also requires learning new steps and moves, which builds the synapses in the brain. And the socialization of dance classes adds another component that can improve cognition.”
Dr. Mahncke hopes that beyond engaging in day-to-day new activities, seniors will participate in computerized brain training. “There’s no reason that evidence-based training can’t be offered in senior and community centers, as yoga and swimming are,” he said. “It doesn’t have to be simply something people do on their own virtually.”
Zoom classes and Medicare reimbursements are “good steps in the right direction, but it’s time to expand this potentially life-transformative intervention so that it reaches the ever-expanding population of seniors in the United States and beyond.”
Dr. Hara reported having no disclosures. Dr. Montero-Odasso reported having no commercial or financial interest related to this topic. He serves as the president of the Canadian Geriatrics Société and is team leader in the Canadian Consortium of Neurodegeneration in Aging. Dr. Mahncke is CEO of the brain training company Posit Science/BrainHQ.
A version of this article appeared on Medscape.com.
The concept that cognitive health can be preserved or improved is often expressed as “use it or lose it.” Numerous modifiable risk factors are associated with “losing” cognitive abilities with age, and a cognitively active lifestyle may have a protective effect.
But what is a “cognitively active lifestyle” — do crosswords and Sudoku count?
One popular approach is “brain training.” While not a scientific term with an established definition, it “typically refers to tasks or drills that are designed to strengthen specific aspects of one’s cognitive function,” explained Yuko Hara, PhD, director of Aging and Alzheimer’s Prevention at the Alzheimer’s Drug Discovery Foundation.
Manuel Montero-Odasso, MD, PhD, director of the Gait and Brain Lab, Parkwood Institute, London, Ontario, Canada, elaborated: “Cognitive training involves performing a definitive task or set of tasks where you increase attentional demands to improve focus and concentration and memory. You try to execute the new things that you’ve learned and to remember them.”
In a commentary published by this news organization in 2022, neuroscientist Michael Merzenich, PhD, professor emeritus at University of California San Francisco, said that growing a person’s cognitive reserve and actively managing brain health can play an important role in preventing or delaying Alzheimer’s disease. Important components of this include brain training and physical exercise.
Brain Training: Mechanism of Action
Dr. Montero-Odasso, team leader at the Canadian Consortium on Neurodegeneration in Aging and team co-leader at the Ontario Neurodegenerative Research Initiative, explained that cognitive training creates new synapses in the brain, thus stimulating neuroplasticity.
“When we try to activate networks mainly in the frontal lobe, the prefrontal cortex, a key mechanism underlying this process is enhancement of the synaptic plasticity at excitatory synapses, which connect neurons into networks; in other words, we generate new synapses, and that’s how we enhance brain health and cognitive abilities.”
The more neural connections, the greater the processing speed of the brain, he continued. “Cognitive training creates an anatomical change in the brain.”
Executive functions, which include attention, inhibition, planning, and multitasking, are regulated predominantly by the prefrontal cortex. Damage in this region of the brain is also implicated in dementia. Alterations in the connectivity of this area are associated with cognitive impairment, independent of other structural pathological aberrations (eg, gray matter atrophy). These patterns may precede structural pathological changes associated with cognitive impairment and dementia.
Neuroplasticity changes have been corroborated through neuroimaging, which has demonstrated that after cognitive training, there is more activation in the prefrontal cortex that correlates with new synapses, Dr. Montero-Odasso said.
Henry Mahncke, PhD, CEO of the brain training company Posit Science/BrainHQ, explained that early research was conducted on rodents and monkeys, with Dr. Merzenich as one of the leading pioneers in developing the concept of brain plasticity. Dr. Merzenich cofounded Posit Science and is currently its chief scientific officer.
Dr. Mahncke recounted that as a graduate student, he had worked with Dr. Merzenich researching brain plasticity. When Dr. Merzenich founded Posit Science, he asked Dr. Mahncke to join the company to help develop approaches to enhance brain plasticity — building the brain-training exercises and running the clinical trials.
“It’s now well understood that the brain can rewire itself at any age and in almost any condition,” Dr. Mahncke said. “In kids and in younger and older adults, whether with healthy or unhealthy brains, the fundamental way the brain works is by continually rewiring and rebuilding itself, based on what we ask it to do.”
Dr. Mahncke said.
Unsubstantiated Claims and Controversy
Brain training is not without controversy, Dr. Hara pointed out. “Some manufacturers of brain games have been criticized and even fined for making unsubstantiated claims,” she said.
A 2016 review found that brain-training interventions do improve performance on specific trained tasks, but there is less evidence that they improve performance on closely related tasks and little evidence that training improves everyday cognitive performance. A 2017 review reached similar conclusions, calling evidence regarding prevention or delay of cognitive decline or dementia through brain games “insufficient,” although cognitive training could “improve cognition in the domain trained.”
“The general consensus is that for most brain-training programs, people may get better at specific tasks through practice, but these improvements don’t necessarily translate into improvement in other tasks that require other cognitive domains or prevention of dementia or age-related cognitive decline,” Dr. Hara said.
She noted that most brain-training programs “have not been rigorously tested in clinical trials” — although some, such as those featured in the ACTIVE trial, did show evidence of effectiveness.
Dr. Mahncke agreed. “Asking whether brain training works is like asking whether small molecules improve health,” he said noting that some brain-training programs are nonsense and not evidence based. He believes that his company’s product, BrainHQ, and some others are “backed by robust evidence in their ability to stave off, slow, or even reverse cognitive changes.”
BrainHQ is a web-based brain game suite that can be used independently as an app or in group settings (classes and webinars) and is covered by some Medicare Advantage insurance plans. It encompasses “dozens of individual brain-training exercises, linked by a common thread. Each one is intensively designed to make the brain faster and more accurate,” said Dr. Mahncke.
He explained that human brains “get noisy as people get older, like a radio which is wearing out, so there’s static in the background. This makes the music hard to hear, and in the case of the human brain, it makes it difficult to pay attention.” The exercises are “designed to tamp down the ‘noise,’ speed up the brain, and make information processing more accurate.”
Dr. Mahncke called this a “bottom-up” approach, in contrast to many previous cognitive-training approaches that come from the brain injury rehabilitation field. They teach “top-down” skills and strategies designed to compensate for deficits in specific domains, such as reading, concentration, or fine motor skills.
By contrast, the approach of BrainHQ is “to improve the overall processing system of the brain with speed, attention, working memory, and executive function, which will in turn impact all skills and activities.”
Supporting Evidence
Dr. Mahncke cited several supporting studies. For example, the IMPACT study randomized 487 adults (aged ≥ 65 years) to receive either a brain plasticity–based computerized cognitive training program (BrainHQ) or a novelty- and intensity-matched general cognitive stimulation treatment program (intervention and control group, respectively) for an 8-week period.
Those who underwent brain training showed significantly greater improvement in the repeatable Battery for the Assessment of Neuropsychological Status (RBANS Auditory Memory/Attention) compared with those in the control group (3.9 vs 1.8, respectively; P =.02). The intervention group also showed significant improvements on multiple secondary measures of attention and memory. The magnitude of the effect sizes suggests that the results are clinically significant, according to the authors.
The ACTIVE study tested the effects of different cognitive training programs on cognitive function and time to dementia. The researchers randomized 2802 healthy older adults (mean age, 74 years) to a control group with no cognitive training or one of three brain-training groups comprising:
1. In-person training on verbal memory skills
2. In-person training on reasoning and problem-solving
3. Computer-based speed-of-processing training on visual attention
Participants in the training groups completed 10 sessions, each lasting 60-75 minutes, over a 5- to 6-week period. A random subsample of each training group was selected to receive “booster” sessions, with four-session booster training delivered at 11 and 35 months. All study participants completed follow-up tests of cognition and function after 1, 2, 3, 5, and 10 years.
At the end of 10 years, those assigned to the speed-of-processing training, now part of BrainHQ, had a 29% lower risk for dementia than those in the control group who received no training. No reduction was found in the memory or reasoning training groups. Participants who completed the “booster” sessions had an even greater reduction: Each additional booster session was associated with a 10% lower risk for dementia.
Dr. Montero-Odasso was involved in the SYNERGIC study that randomized 175 participants with mild cognitive impairment (MCI; average age, 73 years) to one of five study arms:
1. Multidomain intervention with exercise, cognitive training, and vitamin D
2. Exercise, cognitive training, and placebo
3. Exercise, sham cognitive training, and vitamin D
4. Exercise, sham cognitive training, and placebo
5. Control group with balance-toning exercise, sham cognitive training, and placebo
“Sham” cognitive training consisted of alternating between two tasks (touristic search and video watching) performed on a tablet, with the same time exposure as the intervention training.
The researchers found that after 6 months of interventions, all active arms with aerobic-resistance exercise showed improvement in the ADAS-Cog-13, an established outcome to evaluate dementia treatments, when compared with the control group — regardless of the addition of cognitive training or vitamin D.
Compared with exercise alone (arms 3 and 4), those who did exercise plus cognitive training (arms 1 and 2) showed greater improvements in their ADAS-Cog-13l score, with a mean difference of −1.45 points (P = .02). The greatest improvement was seen in those who underwent the multidomain intervention in arm 1.
The authors noted that the mean 2.64-point improvement seen in the ADAS-Cog-13 for the multidomain intervention is actually larger than changes seen in previous pharmaceutical trials among individuals with MCI or mild dementia and “approaches” the three points considered clinically meaningful.
“We found that older adults with MCI who received aerobic-resistance exercise with sequential computerized cognitive training significantly improved cognition,” Dr. Montero-Odasso said. “The cognitive training we used was called Neuropeak, a multidomain lifestyle training delivered through a web-based platform developed by our co-leader Louis Bherer at Université de Montréal.”
He explained that the purpose “is to challenge your brain to the point where you need to make an effort to remember things, pay attention, and later to execute tasks. The evidence from clinical trials, including ours, shows this type of brain challenge is effective in slowing and even reversing cognitive decline.”
A follow-up study, SYNERGIC 2.0, is ongoing.
Puzzles, Board Games, and New Challenges
Formal brain-training programs aren’t the only way to improve brain plasticity, Dr. Hara said. Observational studies suggested an association between improved cognitive performance and/or lower dementia risk and engaging in number and word puzzles, such as crosswords, cards, or board games.
Some studies suggested that older adults who use technology might also protect their cognitive reserve. Dr. Hara cited a US longitudinal study of more than 18,000 older adults suggesting that regular Internet users had roughly half the risk for dementia compared to nonregular Internet users. Estimates of daily Internet use suggested a U-shaped relationship with dementia with 0.1-2.0 hours daily (excluding time spent watching television or movies online) associated with the lowest risk. Similar associations between Internet use and a lower risk for cognitive decline have been reported in the United Kingdom and Europe.
“Engaging in mentally stimulating activities can increase ‘cognitive reserve’ — meaning, capacity of the brain to resist the effects of age-related changes or disease-related pathology, such that one can maintain cognitive function for longer,” Dr. Hara said. “Cognitively stimulating activities, regardless of the type, may help delay the onset of cognitive decline.”
She listed several examples of activities that are stimulating to the brain, including learning a new game or puzzle, a new language, or a new dance, and learning how to play a musical instrument.
Dr. Montero-Odasso emphasized that the “newness” is key to increasing and preserving cognitive reserve. “Just surfing the Internet, playing word or board games, or doing crossword puzzles won’t be enough if you’ve been doing these things all your life,” he said. “It won’t hurt, of course, but it won’t necessarily increase your cognitive abilities.
“For example, a person who regularly engages in public speaking may not improve cognition by taking a public-speaking course, but someone who has never spoken before an audience might show cognitive improvements as a result of learning a new skill,” he said. “Or someone who knows several languages already might gain from learning a brand-new language.”
He cited research supporting the benefits of dancing, which he called “an ideal activity because it’s physical, so it provides the exercise that’s been associated with improved cognition. But it also requires learning new steps and moves, which builds the synapses in the brain. And the socialization of dance classes adds another component that can improve cognition.”
Dr. Mahncke hopes that beyond engaging in day-to-day new activities, seniors will participate in computerized brain training. “There’s no reason that evidence-based training can’t be offered in senior and community centers, as yoga and swimming are,” he said. “It doesn’t have to be simply something people do on their own virtually.”
Zoom classes and Medicare reimbursements are “good steps in the right direction, but it’s time to expand this potentially life-transformative intervention so that it reaches the ever-expanding population of seniors in the United States and beyond.”
Dr. Hara reported having no disclosures. Dr. Montero-Odasso reported having no commercial or financial interest related to this topic. He serves as the president of the Canadian Geriatrics Société and is team leader in the Canadian Consortium of Neurodegeneration in Aging. Dr. Mahncke is CEO of the brain training company Posit Science/BrainHQ.
A version of this article appeared on Medscape.com.
The concept that cognitive health can be preserved or improved is often expressed as “use it or lose it.” Numerous modifiable risk factors are associated with “losing” cognitive abilities with age, and a cognitively active lifestyle may have a protective effect.
But what is a “cognitively active lifestyle” — do crosswords and Sudoku count?
One popular approach is “brain training.” While not a scientific term with an established definition, it “typically refers to tasks or drills that are designed to strengthen specific aspects of one’s cognitive function,” explained Yuko Hara, PhD, director of Aging and Alzheimer’s Prevention at the Alzheimer’s Drug Discovery Foundation.
Manuel Montero-Odasso, MD, PhD, director of the Gait and Brain Lab, Parkwood Institute, London, Ontario, Canada, elaborated: “Cognitive training involves performing a definitive task or set of tasks where you increase attentional demands to improve focus and concentration and memory. You try to execute the new things that you’ve learned and to remember them.”
In a commentary published by this news organization in 2022, neuroscientist Michael Merzenich, PhD, professor emeritus at University of California San Francisco, said that growing a person’s cognitive reserve and actively managing brain health can play an important role in preventing or delaying Alzheimer’s disease. Important components of this include brain training and physical exercise.
Brain Training: Mechanism of Action
Dr. Montero-Odasso, team leader at the Canadian Consortium on Neurodegeneration in Aging and team co-leader at the Ontario Neurodegenerative Research Initiative, explained that cognitive training creates new synapses in the brain, thus stimulating neuroplasticity.
“When we try to activate networks mainly in the frontal lobe, the prefrontal cortex, a key mechanism underlying this process is enhancement of the synaptic plasticity at excitatory synapses, which connect neurons into networks; in other words, we generate new synapses, and that’s how we enhance brain health and cognitive abilities.”
The more neural connections, the greater the processing speed of the brain, he continued. “Cognitive training creates an anatomical change in the brain.”
Executive functions, which include attention, inhibition, planning, and multitasking, are regulated predominantly by the prefrontal cortex. Damage in this region of the brain is also implicated in dementia. Alterations in the connectivity of this area are associated with cognitive impairment, independent of other structural pathological aberrations (eg, gray matter atrophy). These patterns may precede structural pathological changes associated with cognitive impairment and dementia.
Neuroplasticity changes have been corroborated through neuroimaging, which has demonstrated that after cognitive training, there is more activation in the prefrontal cortex that correlates with new synapses, Dr. Montero-Odasso said.
Henry Mahncke, PhD, CEO of the brain training company Posit Science/BrainHQ, explained that early research was conducted on rodents and monkeys, with Dr. Merzenich as one of the leading pioneers in developing the concept of brain plasticity. Dr. Merzenich cofounded Posit Science and is currently its chief scientific officer.
Dr. Mahncke recounted that as a graduate student, he had worked with Dr. Merzenich researching brain plasticity. When Dr. Merzenich founded Posit Science, he asked Dr. Mahncke to join the company to help develop approaches to enhance brain plasticity — building the brain-training exercises and running the clinical trials.
“It’s now well understood that the brain can rewire itself at any age and in almost any condition,” Dr. Mahncke said. “In kids and in younger and older adults, whether with healthy or unhealthy brains, the fundamental way the brain works is by continually rewiring and rebuilding itself, based on what we ask it to do.”
Dr. Mahncke said.
Unsubstantiated Claims and Controversy
Brain training is not without controversy, Dr. Hara pointed out. “Some manufacturers of brain games have been criticized and even fined for making unsubstantiated claims,” she said.
A 2016 review found that brain-training interventions do improve performance on specific trained tasks, but there is less evidence that they improve performance on closely related tasks and little evidence that training improves everyday cognitive performance. A 2017 review reached similar conclusions, calling evidence regarding prevention or delay of cognitive decline or dementia through brain games “insufficient,” although cognitive training could “improve cognition in the domain trained.”
“The general consensus is that for most brain-training programs, people may get better at specific tasks through practice, but these improvements don’t necessarily translate into improvement in other tasks that require other cognitive domains or prevention of dementia or age-related cognitive decline,” Dr. Hara said.
She noted that most brain-training programs “have not been rigorously tested in clinical trials” — although some, such as those featured in the ACTIVE trial, did show evidence of effectiveness.
Dr. Mahncke agreed. “Asking whether brain training works is like asking whether small molecules improve health,” he said noting that some brain-training programs are nonsense and not evidence based. He believes that his company’s product, BrainHQ, and some others are “backed by robust evidence in their ability to stave off, slow, or even reverse cognitive changes.”
BrainHQ is a web-based brain game suite that can be used independently as an app or in group settings (classes and webinars) and is covered by some Medicare Advantage insurance plans. It encompasses “dozens of individual brain-training exercises, linked by a common thread. Each one is intensively designed to make the brain faster and more accurate,” said Dr. Mahncke.
He explained that human brains “get noisy as people get older, like a radio which is wearing out, so there’s static in the background. This makes the music hard to hear, and in the case of the human brain, it makes it difficult to pay attention.” The exercises are “designed to tamp down the ‘noise,’ speed up the brain, and make information processing more accurate.”
Dr. Mahncke called this a “bottom-up” approach, in contrast to many previous cognitive-training approaches that come from the brain injury rehabilitation field. They teach “top-down” skills and strategies designed to compensate for deficits in specific domains, such as reading, concentration, or fine motor skills.
By contrast, the approach of BrainHQ is “to improve the overall processing system of the brain with speed, attention, working memory, and executive function, which will in turn impact all skills and activities.”
Supporting Evidence
Dr. Mahncke cited several supporting studies. For example, the IMPACT study randomized 487 adults (aged ≥ 65 years) to receive either a brain plasticity–based computerized cognitive training program (BrainHQ) or a novelty- and intensity-matched general cognitive stimulation treatment program (intervention and control group, respectively) for an 8-week period.
Those who underwent brain training showed significantly greater improvement in the repeatable Battery for the Assessment of Neuropsychological Status (RBANS Auditory Memory/Attention) compared with those in the control group (3.9 vs 1.8, respectively; P =.02). The intervention group also showed significant improvements on multiple secondary measures of attention and memory. The magnitude of the effect sizes suggests that the results are clinically significant, according to the authors.
The ACTIVE study tested the effects of different cognitive training programs on cognitive function and time to dementia. The researchers randomized 2802 healthy older adults (mean age, 74 years) to a control group with no cognitive training or one of three brain-training groups comprising:
1. In-person training on verbal memory skills
2. In-person training on reasoning and problem-solving
3. Computer-based speed-of-processing training on visual attention
Participants in the training groups completed 10 sessions, each lasting 60-75 minutes, over a 5- to 6-week period. A random subsample of each training group was selected to receive “booster” sessions, with four-session booster training delivered at 11 and 35 months. All study participants completed follow-up tests of cognition and function after 1, 2, 3, 5, and 10 years.
At the end of 10 years, those assigned to the speed-of-processing training, now part of BrainHQ, had a 29% lower risk for dementia than those in the control group who received no training. No reduction was found in the memory or reasoning training groups. Participants who completed the “booster” sessions had an even greater reduction: Each additional booster session was associated with a 10% lower risk for dementia.
Dr. Montero-Odasso was involved in the SYNERGIC study that randomized 175 participants with mild cognitive impairment (MCI; average age, 73 years) to one of five study arms:
1. Multidomain intervention with exercise, cognitive training, and vitamin D
2. Exercise, cognitive training, and placebo
3. Exercise, sham cognitive training, and vitamin D
4. Exercise, sham cognitive training, and placebo
5. Control group with balance-toning exercise, sham cognitive training, and placebo
“Sham” cognitive training consisted of alternating between two tasks (touristic search and video watching) performed on a tablet, with the same time exposure as the intervention training.
The researchers found that after 6 months of interventions, all active arms with aerobic-resistance exercise showed improvement in the ADAS-Cog-13, an established outcome to evaluate dementia treatments, when compared with the control group — regardless of the addition of cognitive training or vitamin D.
Compared with exercise alone (arms 3 and 4), those who did exercise plus cognitive training (arms 1 and 2) showed greater improvements in their ADAS-Cog-13l score, with a mean difference of −1.45 points (P = .02). The greatest improvement was seen in those who underwent the multidomain intervention in arm 1.
The authors noted that the mean 2.64-point improvement seen in the ADAS-Cog-13 for the multidomain intervention is actually larger than changes seen in previous pharmaceutical trials among individuals with MCI or mild dementia and “approaches” the three points considered clinically meaningful.
“We found that older adults with MCI who received aerobic-resistance exercise with sequential computerized cognitive training significantly improved cognition,” Dr. Montero-Odasso said. “The cognitive training we used was called Neuropeak, a multidomain lifestyle training delivered through a web-based platform developed by our co-leader Louis Bherer at Université de Montréal.”
He explained that the purpose “is to challenge your brain to the point where you need to make an effort to remember things, pay attention, and later to execute tasks. The evidence from clinical trials, including ours, shows this type of brain challenge is effective in slowing and even reversing cognitive decline.”
A follow-up study, SYNERGIC 2.0, is ongoing.
Puzzles, Board Games, and New Challenges
Formal brain-training programs aren’t the only way to improve brain plasticity, Dr. Hara said. Observational studies suggested an association between improved cognitive performance and/or lower dementia risk and engaging in number and word puzzles, such as crosswords, cards, or board games.
Some studies suggested that older adults who use technology might also protect their cognitive reserve. Dr. Hara cited a US longitudinal study of more than 18,000 older adults suggesting that regular Internet users had roughly half the risk for dementia compared to nonregular Internet users. Estimates of daily Internet use suggested a U-shaped relationship with dementia with 0.1-2.0 hours daily (excluding time spent watching television or movies online) associated with the lowest risk. Similar associations between Internet use and a lower risk for cognitive decline have been reported in the United Kingdom and Europe.
“Engaging in mentally stimulating activities can increase ‘cognitive reserve’ — meaning, capacity of the brain to resist the effects of age-related changes or disease-related pathology, such that one can maintain cognitive function for longer,” Dr. Hara said. “Cognitively stimulating activities, regardless of the type, may help delay the onset of cognitive decline.”
She listed several examples of activities that are stimulating to the brain, including learning a new game or puzzle, a new language, or a new dance, and learning how to play a musical instrument.
Dr. Montero-Odasso emphasized that the “newness” is key to increasing and preserving cognitive reserve. “Just surfing the Internet, playing word or board games, or doing crossword puzzles won’t be enough if you’ve been doing these things all your life,” he said. “It won’t hurt, of course, but it won’t necessarily increase your cognitive abilities.
“For example, a person who regularly engages in public speaking may not improve cognition by taking a public-speaking course, but someone who has never spoken before an audience might show cognitive improvements as a result of learning a new skill,” he said. “Or someone who knows several languages already might gain from learning a brand-new language.”
He cited research supporting the benefits of dancing, which he called “an ideal activity because it’s physical, so it provides the exercise that’s been associated with improved cognition. But it also requires learning new steps and moves, which builds the synapses in the brain. And the socialization of dance classes adds another component that can improve cognition.”
Dr. Mahncke hopes that beyond engaging in day-to-day new activities, seniors will participate in computerized brain training. “There’s no reason that evidence-based training can’t be offered in senior and community centers, as yoga and swimming are,” he said. “It doesn’t have to be simply something people do on their own virtually.”
Zoom classes and Medicare reimbursements are “good steps in the right direction, but it’s time to expand this potentially life-transformative intervention so that it reaches the ever-expanding population of seniors in the United States and beyond.”
Dr. Hara reported having no disclosures. Dr. Montero-Odasso reported having no commercial or financial interest related to this topic. He serves as the president of the Canadian Geriatrics Société and is team leader in the Canadian Consortium of Neurodegeneration in Aging. Dr. Mahncke is CEO of the brain training company Posit Science/BrainHQ.
A version of this article appeared on Medscape.com.
Novel Agent Curbs Alzheimer’s-Related Agitation
DENVER —
More than half of participants in the open-label extension period of the randomized clinical trial responded to the medication, which was associated with a 3.6-fold lower risk for relapse compared with placebo.
“The positive efficacy and favorable safety results with AXS-05 support its potential to fulfill a high unmet need for the treatment of Alzheimer’s disease agitation,” said Anton P. Porsteinsson, MD, director of the Alzheimer’s Disease Care, Research and Education Program, University of Rochester, New York.
The findings were presented at the 2024 annual meeting of the American Academy of Neurology.
Common and Disruptive
Agitation is reported in up to 70% of patients with Alzheimer’s disease and is characterized by emotional distress, aggressive behaviors, disruptive irritability, and disinhibition. Alzheimer’s disease-related agitation has been associated with increased caregiver burden, decreased functioning, accelerated cognitive decline, earlier nursing home placement, and increased mortality.
A previous phase 2/3 study of AXS-05 showed that the investigative agent led to rapid and significantly improvement in Alzheimer’s disease agitation, as measured by the Cohen-Mansfield Agitation Inventory (CMAI) total score, compared with placebo.
ACCORD was a phase 3, randomized, double-blind, placebo-controlled withdrawal trial evaluating the efficacy and safety of AXS-05 in patients with Alzheimer’s disease agitation.
In the open-label period, 178 adults with probable Alzheimer’s disease and clinically significant agitation received AXS-05 (titrated to 45 mg dextromethorphan/105 mg bupropion twice daily) for up to 9 weeks.
A total of 108 (61%) patients had a sustained response, with 30% or more improvement from baseline in the CMAI total score and improvement on the Patient Global Impression of Change that were both maintained for 4 or more consecutive weeks. These patients entered the double-blind phase and were randomly allocated to receive twice-daily AXS-05 or placebo for up to 26 weeks.
In the double-blind period, AXS-05 “substantially and statistically” increased the time to relapse of agitation symptoms compared with placebo (hazard ratio [HR], 0.275; P = .014).
“The risk of relapse was 3.6-fold lower with AXS-05 compared with placebo,” Dr. Porsteinsson reported.
AXS-05 was also associated with a significantly lower relapse rate compared with placebo (7.5% vs 25.9%; P = .018).
Rates of discontinuation in the double-blind period owing to adverse events (AEs) were low (0% for AXS-05 and 1.9% for placebo). Three serious AEs were reported: one in the AXS-05 group (fecaloma), which was not related to study medication, and two in the placebo group (cardiac arrest, femur fracture).
Falls were reported in four participants in the AXS-05 group, none of which were related to study medication or associated with serious AEs, and in two participants in the placebo group, one of which was associated with femur fracture.
One death was reported in the placebo group. There was no evidence of cognitive decline with AXS-05, and treatment was not associated with sedation.
Promising Agent
Commenting on this research, Glen R. Finney, MD, director of the Geisinger Memory and Cognition Clinic in Wilkes-Barre, Pennsylvania, said the data “look promising as a safe way to help address acute agitation and reduce agitation reoccurrence.
“Agitation is a common, distressing, and sometimes safety issue for people fighting Alzheimer’s disease, and there’s very little evidence for efficacy and significant side effect issues for current medical management of agitation in Alzheimer’s disease,” said Dr. Finney, who was not part of the study.
He noted that first-line strategies for addressing agitation involve behavioral and environmental interventions.
“See if there’s a reason for the agitation and address that. Look for triggers for agitation and avoid those. Find places, things, and interactions that help people with Alzheimer’s disease avoid agitation: familiar locations, music, simple engaging activities. Reassurance, redirection, and distraction can help de-escalate agitation. Provide a safe environment that reduces safety risks,” Dr. Finney explained.
The next step, when medically appropriate, is trying acetylcholinesterase inhibitors such as donepezil, rivastigmine, and galantamine, and then adding memantine, a weak N-methyl-D-aspartate receptor antagonist.
“These medications can help reduce the risk of agitation,” Dr. Finney said.
“Beyond that, the evidence becomes weaker for any specific treatments, and that is where treatments with emerging evidence of efficacy and safety like dextromethorphan-bupropion become important,” Dr. Finney added.
Last May, the US Food and Drug Administration (FDA) approved the antipsychotic brexpiprazole (Rexulti) for Alzheimer’s disease-related agitation, making it the first FDA-approved drug for this indication.
The drug includes a boxed warning for medications in this class that older patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk for death.
“There’s certainly a need to have multiple options for treating agitation in individuals with Alzheimer’s disease,” said Rebecca Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association.
Dr. Edelmayer, who was not part of the study, noted that in the ACCORD study, AXS-05 “significantly delayed the relapse or prevented the relapse with Alzheimer’s disease agitation compared with the placebo group and it was generally well tolerated, but it will be important to make sure that there’s more thorough review of the data overall to be sure that it’s both safe and effective.”
The study was funded by Axsome Therapeutics, the manufacturer of AXS-05. Dr. Porsteinsson has disclosed no relevant conflicts of interest. Dr. Finney and Dr. Edelmayer have no relevant disclosures.
A version of this article appeared on Medscape.com.
DENVER —
More than half of participants in the open-label extension period of the randomized clinical trial responded to the medication, which was associated with a 3.6-fold lower risk for relapse compared with placebo.
“The positive efficacy and favorable safety results with AXS-05 support its potential to fulfill a high unmet need for the treatment of Alzheimer’s disease agitation,” said Anton P. Porsteinsson, MD, director of the Alzheimer’s Disease Care, Research and Education Program, University of Rochester, New York.
The findings were presented at the 2024 annual meeting of the American Academy of Neurology.
Common and Disruptive
Agitation is reported in up to 70% of patients with Alzheimer’s disease and is characterized by emotional distress, aggressive behaviors, disruptive irritability, and disinhibition. Alzheimer’s disease-related agitation has been associated with increased caregiver burden, decreased functioning, accelerated cognitive decline, earlier nursing home placement, and increased mortality.
A previous phase 2/3 study of AXS-05 showed that the investigative agent led to rapid and significantly improvement in Alzheimer’s disease agitation, as measured by the Cohen-Mansfield Agitation Inventory (CMAI) total score, compared with placebo.
ACCORD was a phase 3, randomized, double-blind, placebo-controlled withdrawal trial evaluating the efficacy and safety of AXS-05 in patients with Alzheimer’s disease agitation.
In the open-label period, 178 adults with probable Alzheimer’s disease and clinically significant agitation received AXS-05 (titrated to 45 mg dextromethorphan/105 mg bupropion twice daily) for up to 9 weeks.
A total of 108 (61%) patients had a sustained response, with 30% or more improvement from baseline in the CMAI total score and improvement on the Patient Global Impression of Change that were both maintained for 4 or more consecutive weeks. These patients entered the double-blind phase and were randomly allocated to receive twice-daily AXS-05 or placebo for up to 26 weeks.
In the double-blind period, AXS-05 “substantially and statistically” increased the time to relapse of agitation symptoms compared with placebo (hazard ratio [HR], 0.275; P = .014).
“The risk of relapse was 3.6-fold lower with AXS-05 compared with placebo,” Dr. Porsteinsson reported.
AXS-05 was also associated with a significantly lower relapse rate compared with placebo (7.5% vs 25.9%; P = .018).
Rates of discontinuation in the double-blind period owing to adverse events (AEs) were low (0% for AXS-05 and 1.9% for placebo). Three serious AEs were reported: one in the AXS-05 group (fecaloma), which was not related to study medication, and two in the placebo group (cardiac arrest, femur fracture).
Falls were reported in four participants in the AXS-05 group, none of which were related to study medication or associated with serious AEs, and in two participants in the placebo group, one of which was associated with femur fracture.
One death was reported in the placebo group. There was no evidence of cognitive decline with AXS-05, and treatment was not associated with sedation.
Promising Agent
Commenting on this research, Glen R. Finney, MD, director of the Geisinger Memory and Cognition Clinic in Wilkes-Barre, Pennsylvania, said the data “look promising as a safe way to help address acute agitation and reduce agitation reoccurrence.
“Agitation is a common, distressing, and sometimes safety issue for people fighting Alzheimer’s disease, and there’s very little evidence for efficacy and significant side effect issues for current medical management of agitation in Alzheimer’s disease,” said Dr. Finney, who was not part of the study.
He noted that first-line strategies for addressing agitation involve behavioral and environmental interventions.
“See if there’s a reason for the agitation and address that. Look for triggers for agitation and avoid those. Find places, things, and interactions that help people with Alzheimer’s disease avoid agitation: familiar locations, music, simple engaging activities. Reassurance, redirection, and distraction can help de-escalate agitation. Provide a safe environment that reduces safety risks,” Dr. Finney explained.
The next step, when medically appropriate, is trying acetylcholinesterase inhibitors such as donepezil, rivastigmine, and galantamine, and then adding memantine, a weak N-methyl-D-aspartate receptor antagonist.
“These medications can help reduce the risk of agitation,” Dr. Finney said.
“Beyond that, the evidence becomes weaker for any specific treatments, and that is where treatments with emerging evidence of efficacy and safety like dextromethorphan-bupropion become important,” Dr. Finney added.
Last May, the US Food and Drug Administration (FDA) approved the antipsychotic brexpiprazole (Rexulti) for Alzheimer’s disease-related agitation, making it the first FDA-approved drug for this indication.
The drug includes a boxed warning for medications in this class that older patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk for death.
“There’s certainly a need to have multiple options for treating agitation in individuals with Alzheimer’s disease,” said Rebecca Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association.
Dr. Edelmayer, who was not part of the study, noted that in the ACCORD study, AXS-05 “significantly delayed the relapse or prevented the relapse with Alzheimer’s disease agitation compared with the placebo group and it was generally well tolerated, but it will be important to make sure that there’s more thorough review of the data overall to be sure that it’s both safe and effective.”
The study was funded by Axsome Therapeutics, the manufacturer of AXS-05. Dr. Porsteinsson has disclosed no relevant conflicts of interest. Dr. Finney and Dr. Edelmayer have no relevant disclosures.
A version of this article appeared on Medscape.com.
DENVER —
More than half of participants in the open-label extension period of the randomized clinical trial responded to the medication, which was associated with a 3.6-fold lower risk for relapse compared with placebo.
“The positive efficacy and favorable safety results with AXS-05 support its potential to fulfill a high unmet need for the treatment of Alzheimer’s disease agitation,” said Anton P. Porsteinsson, MD, director of the Alzheimer’s Disease Care, Research and Education Program, University of Rochester, New York.
The findings were presented at the 2024 annual meeting of the American Academy of Neurology.
Common and Disruptive
Agitation is reported in up to 70% of patients with Alzheimer’s disease and is characterized by emotional distress, aggressive behaviors, disruptive irritability, and disinhibition. Alzheimer’s disease-related agitation has been associated with increased caregiver burden, decreased functioning, accelerated cognitive decline, earlier nursing home placement, and increased mortality.
A previous phase 2/3 study of AXS-05 showed that the investigative agent led to rapid and significantly improvement in Alzheimer’s disease agitation, as measured by the Cohen-Mansfield Agitation Inventory (CMAI) total score, compared with placebo.
ACCORD was a phase 3, randomized, double-blind, placebo-controlled withdrawal trial evaluating the efficacy and safety of AXS-05 in patients with Alzheimer’s disease agitation.
In the open-label period, 178 adults with probable Alzheimer’s disease and clinically significant agitation received AXS-05 (titrated to 45 mg dextromethorphan/105 mg bupropion twice daily) for up to 9 weeks.
A total of 108 (61%) patients had a sustained response, with 30% or more improvement from baseline in the CMAI total score and improvement on the Patient Global Impression of Change that were both maintained for 4 or more consecutive weeks. These patients entered the double-blind phase and were randomly allocated to receive twice-daily AXS-05 or placebo for up to 26 weeks.
In the double-blind period, AXS-05 “substantially and statistically” increased the time to relapse of agitation symptoms compared with placebo (hazard ratio [HR], 0.275; P = .014).
“The risk of relapse was 3.6-fold lower with AXS-05 compared with placebo,” Dr. Porsteinsson reported.
AXS-05 was also associated with a significantly lower relapse rate compared with placebo (7.5% vs 25.9%; P = .018).
Rates of discontinuation in the double-blind period owing to adverse events (AEs) were low (0% for AXS-05 and 1.9% for placebo). Three serious AEs were reported: one in the AXS-05 group (fecaloma), which was not related to study medication, and two in the placebo group (cardiac arrest, femur fracture).
Falls were reported in four participants in the AXS-05 group, none of which were related to study medication or associated with serious AEs, and in two participants in the placebo group, one of which was associated with femur fracture.
One death was reported in the placebo group. There was no evidence of cognitive decline with AXS-05, and treatment was not associated with sedation.
Promising Agent
Commenting on this research, Glen R. Finney, MD, director of the Geisinger Memory and Cognition Clinic in Wilkes-Barre, Pennsylvania, said the data “look promising as a safe way to help address acute agitation and reduce agitation reoccurrence.
“Agitation is a common, distressing, and sometimes safety issue for people fighting Alzheimer’s disease, and there’s very little evidence for efficacy and significant side effect issues for current medical management of agitation in Alzheimer’s disease,” said Dr. Finney, who was not part of the study.
He noted that first-line strategies for addressing agitation involve behavioral and environmental interventions.
“See if there’s a reason for the agitation and address that. Look for triggers for agitation and avoid those. Find places, things, and interactions that help people with Alzheimer’s disease avoid agitation: familiar locations, music, simple engaging activities. Reassurance, redirection, and distraction can help de-escalate agitation. Provide a safe environment that reduces safety risks,” Dr. Finney explained.
The next step, when medically appropriate, is trying acetylcholinesterase inhibitors such as donepezil, rivastigmine, and galantamine, and then adding memantine, a weak N-methyl-D-aspartate receptor antagonist.
“These medications can help reduce the risk of agitation,” Dr. Finney said.
“Beyond that, the evidence becomes weaker for any specific treatments, and that is where treatments with emerging evidence of efficacy and safety like dextromethorphan-bupropion become important,” Dr. Finney added.
Last May, the US Food and Drug Administration (FDA) approved the antipsychotic brexpiprazole (Rexulti) for Alzheimer’s disease-related agitation, making it the first FDA-approved drug for this indication.
The drug includes a boxed warning for medications in this class that older patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk for death.
“There’s certainly a need to have multiple options for treating agitation in individuals with Alzheimer’s disease,” said Rebecca Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association.
Dr. Edelmayer, who was not part of the study, noted that in the ACCORD study, AXS-05 “significantly delayed the relapse or prevented the relapse with Alzheimer’s disease agitation compared with the placebo group and it was generally well tolerated, but it will be important to make sure that there’s more thorough review of the data overall to be sure that it’s both safe and effective.”
The study was funded by Axsome Therapeutics, the manufacturer of AXS-05. Dr. Porsteinsson has disclosed no relevant conflicts of interest. Dr. Finney and Dr. Edelmayer have no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM AAN 2024
Antipsychotics for Dementia Pose Wide-Ranging Health Risks
Antipsychotic use in older adults with dementia is associated with a significant increased risk for stroke, myocardial infarction, heart failure, pneumonia, fracture, acute kidney injury, and a range of other health problems compared with nonuse, new research showed.
The adverse events are far broader and pose more severe health risks than previously reported, investigators noted, and suggested greater caution is needed when prescribing antipsychotics to treat psychological symptoms of dementia.
The matched cohort study used patient registry data on nearly 174,000 people with dementia and compared those who were prescribed an antipsychotic on or after their dementia diagnosis with those who had not received a prescription for the drugs.
Any antipsychotic use was associated with double the risk for pneumonia, a 1.7-fold increased risk for acute kidney injury, and 1.6-fold higher odds of venous thromboembolism compared to nonuse.
Investigators found an increased risk for all outcomes studied, except for ventricular arrythmia, and risk was highest for most within the first week of treatment.
“Any potential benefits of antipsychotic treatment therefore need to be weighed against the risk of serious harm across multiple outcomes. Although there may be times when an antipsychotic prescription is the least bad option, clinicians should actively consider the risks, considering patients’ pre-existing comorbidities and living support,” lead investigator Pearl Mok, research fellow at the Centre for Pharmacoepidemiology and Drug Safety, The University of Manchester, Manchester, England, and colleagues wrote.
The findings were published online in The BMJ.
High Risk
Depression, aggression, anxiety, psychosis, and other behavioral and psychological symptoms are common in people with dementia. Despite earlier reports of increased risk for stroke and mortality with antipsychotic use, the drugs are frequently prescribed to treat these symptoms.
While some preliminary studies identified other adverse outcomes from antipsychotic use, results are limited and inconsistent.
Investigators used primary and secondary care data from the Clinical Practice Research Datalink in England. A total of 173,910 adults (63% women) had a dementia diagnosis between January 1998 and May 2018.
Of the total cohort, 35,339 patients were prescribed an antipsychotic on, or after, a dementia diagnosis. Each was matched with up to 15 patients with dementia with no history of antipsychotic use following diagnosis.
Almost 80% of antipsychotic prescriptions were for risperidone, quetiapine, haloperidol, and olanzapine.
Any antipsychotic use was associated with significantly higher risks for pneumonia (hazard ratio [HR], 2.03; 95% CI, 1.96-2.10), acute kidney injury (HR, 1.57; 95% CI, 1.48-1.66), stroke (HR, 1.54; 95% CI, 1.46-1.63), venous thromboembolism (HR, 1.52; 95% CI, 1.38-1.67), fracture (HR, 1.36; 95% CI, 1.30-1.44), myocardial infarction (HR, 1.22; 95% CI, 1.12-1.34), and heart failure (HR, 1.16; 95% CI, 1.09-1.24).
The risk for all conditions was highest within the first 3 months of treatment, with a cumulative incidence of pneumonia among antipsychotic users of 4.48% vs 1.49% among nonusers. At 1 year, this increased to 10.41% for users vs 5.63% for nonusers.
“Given the higher risks of adverse events in the early days after drug initiation, clinical examinations should be taken before, and clinical reviews conducted shortly after, the start of treatment,” the authors wrote. “Our study reaffirms that these drugs should only be prescribed for the shortest period possible.”
‘Serious Harms’
In an accompanying editorial, Raya Elfadel Kheirbek, MD, and Cristina LaFont, Department of Medicine, University of Maryland School of Medicine, Baltimore, Maryland, said the findings “highlight the need for careful justification of antipsychotic use in dementia care, including a comprehensive assessment of the benefits weighed against a broader range of serious harms than previously acknowledged.”
“Using antipsychotics for the management of dementia-related behaviors requires nuanced decision-making after careful assessment, informed by a personalized approach,” they continued. “Dr. Mok and colleagues call for a critical re-evaluation of antipsychotic use in this clinical setting.”
While the findings add to and expand what was already known, “we need to be clear that they don’t show antipsychotics cause all the adverse outcomes reported,” Masud Husain, DPhil, professor of neurology, University of Oxford, England, said in a statement.
While investigators attempted to use matched controls with dementia who had not received antipsychotics, “the people who were prescribed the drugs may simply have been more vulnerable to some of the conditions that occurred more frequently in them, such as pneumonia and cardiovascular disorders,” said Dr. Husain, who was not part of the research.
Although the study was not designed to explore reverse causality, the findings are important for clinicians who prescribe antipsychotics for patients with dementia, Robert Howard, professor of old age psychiatry, at the University of College London, London, England said in a statement.
“Initiation of these drugs in people with dementia should only ever be under specialist supervision, with involvement of patients and family members in informed discussion and review,” said Dr. Howard, who was not involved in the study.
The study was funded by the National Institute for Health and Care Research. Dr. Mok reported no relevant conflicts. Other authors’ disclosures are included in the original article. Dr. Hussain, Dr. Howard, Dr. Kheirbek, and Dr. LeFon reported no relevant conflicts.
A version of this article appeared on Medscape.com.
Antipsychotic use in older adults with dementia is associated with a significant increased risk for stroke, myocardial infarction, heart failure, pneumonia, fracture, acute kidney injury, and a range of other health problems compared with nonuse, new research showed.
The adverse events are far broader and pose more severe health risks than previously reported, investigators noted, and suggested greater caution is needed when prescribing antipsychotics to treat psychological symptoms of dementia.
The matched cohort study used patient registry data on nearly 174,000 people with dementia and compared those who were prescribed an antipsychotic on or after their dementia diagnosis with those who had not received a prescription for the drugs.
Any antipsychotic use was associated with double the risk for pneumonia, a 1.7-fold increased risk for acute kidney injury, and 1.6-fold higher odds of venous thromboembolism compared to nonuse.
Investigators found an increased risk for all outcomes studied, except for ventricular arrythmia, and risk was highest for most within the first week of treatment.
“Any potential benefits of antipsychotic treatment therefore need to be weighed against the risk of serious harm across multiple outcomes. Although there may be times when an antipsychotic prescription is the least bad option, clinicians should actively consider the risks, considering patients’ pre-existing comorbidities and living support,” lead investigator Pearl Mok, research fellow at the Centre for Pharmacoepidemiology and Drug Safety, The University of Manchester, Manchester, England, and colleagues wrote.
The findings were published online in The BMJ.
High Risk
Depression, aggression, anxiety, psychosis, and other behavioral and psychological symptoms are common in people with dementia. Despite earlier reports of increased risk for stroke and mortality with antipsychotic use, the drugs are frequently prescribed to treat these symptoms.
While some preliminary studies identified other adverse outcomes from antipsychotic use, results are limited and inconsistent.
Investigators used primary and secondary care data from the Clinical Practice Research Datalink in England. A total of 173,910 adults (63% women) had a dementia diagnosis between January 1998 and May 2018.
Of the total cohort, 35,339 patients were prescribed an antipsychotic on, or after, a dementia diagnosis. Each was matched with up to 15 patients with dementia with no history of antipsychotic use following diagnosis.
Almost 80% of antipsychotic prescriptions were for risperidone, quetiapine, haloperidol, and olanzapine.
Any antipsychotic use was associated with significantly higher risks for pneumonia (hazard ratio [HR], 2.03; 95% CI, 1.96-2.10), acute kidney injury (HR, 1.57; 95% CI, 1.48-1.66), stroke (HR, 1.54; 95% CI, 1.46-1.63), venous thromboembolism (HR, 1.52; 95% CI, 1.38-1.67), fracture (HR, 1.36; 95% CI, 1.30-1.44), myocardial infarction (HR, 1.22; 95% CI, 1.12-1.34), and heart failure (HR, 1.16; 95% CI, 1.09-1.24).
The risk for all conditions was highest within the first 3 months of treatment, with a cumulative incidence of pneumonia among antipsychotic users of 4.48% vs 1.49% among nonusers. At 1 year, this increased to 10.41% for users vs 5.63% for nonusers.
“Given the higher risks of adverse events in the early days after drug initiation, clinical examinations should be taken before, and clinical reviews conducted shortly after, the start of treatment,” the authors wrote. “Our study reaffirms that these drugs should only be prescribed for the shortest period possible.”
‘Serious Harms’
In an accompanying editorial, Raya Elfadel Kheirbek, MD, and Cristina LaFont, Department of Medicine, University of Maryland School of Medicine, Baltimore, Maryland, said the findings “highlight the need for careful justification of antipsychotic use in dementia care, including a comprehensive assessment of the benefits weighed against a broader range of serious harms than previously acknowledged.”
“Using antipsychotics for the management of dementia-related behaviors requires nuanced decision-making after careful assessment, informed by a personalized approach,” they continued. “Dr. Mok and colleagues call for a critical re-evaluation of antipsychotic use in this clinical setting.”
While the findings add to and expand what was already known, “we need to be clear that they don’t show antipsychotics cause all the adverse outcomes reported,” Masud Husain, DPhil, professor of neurology, University of Oxford, England, said in a statement.
While investigators attempted to use matched controls with dementia who had not received antipsychotics, “the people who were prescribed the drugs may simply have been more vulnerable to some of the conditions that occurred more frequently in them, such as pneumonia and cardiovascular disorders,” said Dr. Husain, who was not part of the research.
Although the study was not designed to explore reverse causality, the findings are important for clinicians who prescribe antipsychotics for patients with dementia, Robert Howard, professor of old age psychiatry, at the University of College London, London, England said in a statement.
“Initiation of these drugs in people with dementia should only ever be under specialist supervision, with involvement of patients and family members in informed discussion and review,” said Dr. Howard, who was not involved in the study.
The study was funded by the National Institute for Health and Care Research. Dr. Mok reported no relevant conflicts. Other authors’ disclosures are included in the original article. Dr. Hussain, Dr. Howard, Dr. Kheirbek, and Dr. LeFon reported no relevant conflicts.
A version of this article appeared on Medscape.com.
Antipsychotic use in older adults with dementia is associated with a significant increased risk for stroke, myocardial infarction, heart failure, pneumonia, fracture, acute kidney injury, and a range of other health problems compared with nonuse, new research showed.
The adverse events are far broader and pose more severe health risks than previously reported, investigators noted, and suggested greater caution is needed when prescribing antipsychotics to treat psychological symptoms of dementia.
The matched cohort study used patient registry data on nearly 174,000 people with dementia and compared those who were prescribed an antipsychotic on or after their dementia diagnosis with those who had not received a prescription for the drugs.
Any antipsychotic use was associated with double the risk for pneumonia, a 1.7-fold increased risk for acute kidney injury, and 1.6-fold higher odds of venous thromboembolism compared to nonuse.
Investigators found an increased risk for all outcomes studied, except for ventricular arrythmia, and risk was highest for most within the first week of treatment.
“Any potential benefits of antipsychotic treatment therefore need to be weighed against the risk of serious harm across multiple outcomes. Although there may be times when an antipsychotic prescription is the least bad option, clinicians should actively consider the risks, considering patients’ pre-existing comorbidities and living support,” lead investigator Pearl Mok, research fellow at the Centre for Pharmacoepidemiology and Drug Safety, The University of Manchester, Manchester, England, and colleagues wrote.
The findings were published online in The BMJ.
High Risk
Depression, aggression, anxiety, psychosis, and other behavioral and psychological symptoms are common in people with dementia. Despite earlier reports of increased risk for stroke and mortality with antipsychotic use, the drugs are frequently prescribed to treat these symptoms.
While some preliminary studies identified other adverse outcomes from antipsychotic use, results are limited and inconsistent.
Investigators used primary and secondary care data from the Clinical Practice Research Datalink in England. A total of 173,910 adults (63% women) had a dementia diagnosis between January 1998 and May 2018.
Of the total cohort, 35,339 patients were prescribed an antipsychotic on, or after, a dementia diagnosis. Each was matched with up to 15 patients with dementia with no history of antipsychotic use following diagnosis.
Almost 80% of antipsychotic prescriptions were for risperidone, quetiapine, haloperidol, and olanzapine.
Any antipsychotic use was associated with significantly higher risks for pneumonia (hazard ratio [HR], 2.03; 95% CI, 1.96-2.10), acute kidney injury (HR, 1.57; 95% CI, 1.48-1.66), stroke (HR, 1.54; 95% CI, 1.46-1.63), venous thromboembolism (HR, 1.52; 95% CI, 1.38-1.67), fracture (HR, 1.36; 95% CI, 1.30-1.44), myocardial infarction (HR, 1.22; 95% CI, 1.12-1.34), and heart failure (HR, 1.16; 95% CI, 1.09-1.24).
The risk for all conditions was highest within the first 3 months of treatment, with a cumulative incidence of pneumonia among antipsychotic users of 4.48% vs 1.49% among nonusers. At 1 year, this increased to 10.41% for users vs 5.63% for nonusers.
“Given the higher risks of adverse events in the early days after drug initiation, clinical examinations should be taken before, and clinical reviews conducted shortly after, the start of treatment,” the authors wrote. “Our study reaffirms that these drugs should only be prescribed for the shortest period possible.”
‘Serious Harms’
In an accompanying editorial, Raya Elfadel Kheirbek, MD, and Cristina LaFont, Department of Medicine, University of Maryland School of Medicine, Baltimore, Maryland, said the findings “highlight the need for careful justification of antipsychotic use in dementia care, including a comprehensive assessment of the benefits weighed against a broader range of serious harms than previously acknowledged.”
“Using antipsychotics for the management of dementia-related behaviors requires nuanced decision-making after careful assessment, informed by a personalized approach,” they continued. “Dr. Mok and colleagues call for a critical re-evaluation of antipsychotic use in this clinical setting.”
While the findings add to and expand what was already known, “we need to be clear that they don’t show antipsychotics cause all the adverse outcomes reported,” Masud Husain, DPhil, professor of neurology, University of Oxford, England, said in a statement.
While investigators attempted to use matched controls with dementia who had not received antipsychotics, “the people who were prescribed the drugs may simply have been more vulnerable to some of the conditions that occurred more frequently in them, such as pneumonia and cardiovascular disorders,” said Dr. Husain, who was not part of the research.
Although the study was not designed to explore reverse causality, the findings are important for clinicians who prescribe antipsychotics for patients with dementia, Robert Howard, professor of old age psychiatry, at the University of College London, London, England said in a statement.
“Initiation of these drugs in people with dementia should only ever be under specialist supervision, with involvement of patients and family members in informed discussion and review,” said Dr. Howard, who was not involved in the study.
The study was funded by the National Institute for Health and Care Research. Dr. Mok reported no relevant conflicts. Other authors’ disclosures are included in the original article. Dr. Hussain, Dr. Howard, Dr. Kheirbek, and Dr. LeFon reported no relevant conflicts.
A version of this article appeared on Medscape.com.
FROM THE BMJ