User login
For MD-IQ on Family Practice News, but a regular topic for Rheumatology News
Different triggers found for knee and hand OA
Mechanical stress is the most important underlying mechanism in osteoarthritis of the knees, while systemic processes may contribute most to hand osteoarthritis, Dutch researchers have found.
"How obesity results in osteoarthritis [OA] is not quite clear, but several mechanisms are thought to play a role, such as increased mechanical stress and systemic processes that are associated with adipose tissue," said senior study author Dr. Margreet Kloppenburg, professor of rheumatology at Leiden (the Netherlands) University Medical Center.

"Adipose tissue is known to be a source of active mediators, proinflammatory proteins and hormones, influencing inflammation, lipids, glucose metabolism, and insulin resistance," she said. "These systemic processes also could result in the development of OA. Our aim was to understand more about the link between obesity and OA because this insight could help us reach our ultimate goal: to improve treatment for OA patients."
Dr. Kloppenburg and her colleagues reviewed records from 6,628 participants in the Netherlands Epidemiology of Obesity (NEO) study, a population-based cohort of adults aged 45-65 years that is designed to investigate pathways leading to common diseases and conditions in overweight and obese individuals. Participants had a mean age of 56 years and a body mass index of 26 kg/m2; 56% were women. The estimated prevalence of OA was 10% in the knee, 8% in the hand, and 4% in both.
Researchers measured weight and fat mass and calculated fat-free mass. They also calculated odds ratios (ORs) to test for associations between surrogates for mechanical stress (weight and fat-free mass) and systemic processes (metabolic syndrome) with OA in knees alone, hands alone, or both knees and hands. Adjusted ORs were calculated for each OA type in three weight categories: less than 75 kg, 75-90 kg, and more than 90 kg.
After adjustment for metabolic factors, knee OA was significantly associated with weight (OR, 1.49) and fat-free mass (OR, 2.05). Similar results were observed for OA in both the knees and hands. In hand OA, however, investigators found the opposite: Hand OA was significantly associated with metabolic syndrome, independent of weight (OR, 1.46), and had no associations with weight and fat-free mass, Dr. Kloppenburg reported at the annual European Congress of Rheumatology.
"As we hypothesized, knee OA was predominantly associated with surrogates for mechanical stress, whereas hand OA was predominantly associated with surrogates for systemic processes," she said. "But what we had not expected was that surrogates for mechanical stress were predominantly associated with OA in both the knees and hands. This suggests that the co-occurrence of knee and hand OA may not be based on a common underlying pathogenic mechanism, but may represent the presence of two different types of OA."
Adjusted ORs for knee OA and for OA of both the knees and hands were greater in the higher weight categories, but, in hand OA, ORs did not increase with weight.
"Our study supports findings from clinical trials in obese patients with knee OA demonstrating that weight loss, together with exercise, which can potentially modify mechanical stress, is beneficial," she said. "It would be worthwhile to investigate whether weight loss also is beneficial in hand OA."
The NEO study is supported by the Dutch Arthritis Association, Leiden University Medical Center, and Leiden University. The investigators had no conflicts of interest to declare.
Mechanical stress is the most important underlying mechanism in osteoarthritis of the knees, while systemic processes may contribute most to hand osteoarthritis, Dutch researchers have found.
"How obesity results in osteoarthritis [OA] is not quite clear, but several mechanisms are thought to play a role, such as increased mechanical stress and systemic processes that are associated with adipose tissue," said senior study author Dr. Margreet Kloppenburg, professor of rheumatology at Leiden (the Netherlands) University Medical Center.
"Adipose tissue is known to be a source of active mediators, proinflammatory proteins and hormones, influencing inflammation, lipids, glucose metabolism, and insulin resistance," she said. "These systemic processes also could result in the development of OA. Our aim was to understand more about the link between obesity and OA because this insight could help us reach our ultimate goal: to improve treatment for OA patients."
Dr. Kloppenburg and her colleagues reviewed records from 6,628 participants in the Netherlands Epidemiology of Obesity (NEO) study, a population-based cohort of adults aged 45-65 years that is designed to investigate pathways leading to common diseases and conditions in overweight and obese individuals. Participants had a mean age of 56 years and a body mass index of 26 kg/m2; 56% were women. The estimated prevalence of OA was 10% in the knee, 8% in the hand, and 4% in both.
Researchers measured weight and fat mass and calculated fat-free mass. They also calculated odds ratios (ORs) to test for associations between surrogates for mechanical stress (weight and fat-free mass) and systemic processes (metabolic syndrome) with OA in knees alone, hands alone, or both knees and hands. Adjusted ORs were calculated for each OA type in three weight categories: less than 75 kg, 75-90 kg, and more than 90 kg.
After adjustment for metabolic factors, knee OA was significantly associated with weight (OR, 1.49) and fat-free mass (OR, 2.05). Similar results were observed for OA in both the knees and hands. In hand OA, however, investigators found the opposite: Hand OA was significantly associated with metabolic syndrome, independent of weight (OR, 1.46), and had no associations with weight and fat-free mass, Dr. Kloppenburg reported at the annual European Congress of Rheumatology.
"As we hypothesized, knee OA was predominantly associated with surrogates for mechanical stress, whereas hand OA was predominantly associated with surrogates for systemic processes," she said. "But what we had not expected was that surrogates for mechanical stress were predominantly associated with OA in both the knees and hands. This suggests that the co-occurrence of knee and hand OA may not be based on a common underlying pathogenic mechanism, but may represent the presence of two different types of OA."
Adjusted ORs for knee OA and for OA of both the knees and hands were greater in the higher weight categories, but, in hand OA, ORs did not increase with weight.
"Our study supports findings from clinical trials in obese patients with knee OA demonstrating that weight loss, together with exercise, which can potentially modify mechanical stress, is beneficial," she said. "It would be worthwhile to investigate whether weight loss also is beneficial in hand OA."
The NEO study is supported by the Dutch Arthritis Association, Leiden University Medical Center, and Leiden University. The investigators had no conflicts of interest to declare.
Mechanical stress is the most important underlying mechanism in osteoarthritis of the knees, while systemic processes may contribute most to hand osteoarthritis, Dutch researchers have found.
"How obesity results in osteoarthritis [OA] is not quite clear, but several mechanisms are thought to play a role, such as increased mechanical stress and systemic processes that are associated with adipose tissue," said senior study author Dr. Margreet Kloppenburg, professor of rheumatology at Leiden (the Netherlands) University Medical Center.
"Adipose tissue is known to be a source of active mediators, proinflammatory proteins and hormones, influencing inflammation, lipids, glucose metabolism, and insulin resistance," she said. "These systemic processes also could result in the development of OA. Our aim was to understand more about the link between obesity and OA because this insight could help us reach our ultimate goal: to improve treatment for OA patients."
Dr. Kloppenburg and her colleagues reviewed records from 6,628 participants in the Netherlands Epidemiology of Obesity (NEO) study, a population-based cohort of adults aged 45-65 years that is designed to investigate pathways leading to common diseases and conditions in overweight and obese individuals. Participants had a mean age of 56 years and a body mass index of 26 kg/m2; 56% were women. The estimated prevalence of OA was 10% in the knee, 8% in the hand, and 4% in both.
Researchers measured weight and fat mass and calculated fat-free mass. They also calculated odds ratios (ORs) to test for associations between surrogates for mechanical stress (weight and fat-free mass) and systemic processes (metabolic syndrome) with OA in knees alone, hands alone, or both knees and hands. Adjusted ORs were calculated for each OA type in three weight categories: less than 75 kg, 75-90 kg, and more than 90 kg.
After adjustment for metabolic factors, knee OA was significantly associated with weight (OR, 1.49) and fat-free mass (OR, 2.05). Similar results were observed for OA in both the knees and hands. In hand OA, however, investigators found the opposite: Hand OA was significantly associated with metabolic syndrome, independent of weight (OR, 1.46), and had no associations with weight and fat-free mass, Dr. Kloppenburg reported at the annual European Congress of Rheumatology.
"As we hypothesized, knee OA was predominantly associated with surrogates for mechanical stress, whereas hand OA was predominantly associated with surrogates for systemic processes," she said. "But what we had not expected was that surrogates for mechanical stress were predominantly associated with OA in both the knees and hands. This suggests that the co-occurrence of knee and hand OA may not be based on a common underlying pathogenic mechanism, but may represent the presence of two different types of OA."
Adjusted ORs for knee OA and for OA of both the knees and hands were greater in the higher weight categories, but, in hand OA, ORs did not increase with weight.
"Our study supports findings from clinical trials in obese patients with knee OA demonstrating that weight loss, together with exercise, which can potentially modify mechanical stress, is beneficial," she said. "It would be worthwhile to investigate whether weight loss also is beneficial in hand OA."
The NEO study is supported by the Dutch Arthritis Association, Leiden University Medical Center, and Leiden University. The investigators had no conflicts of interest to declare.
FROM THE EULAR CONGRESS 2014
Key clinical point: Weight loss may be a primary target for improving knee OA, but improvements in metabolic factors may most benefit hand OA.
Major finding: Hand OA was significantly associated with metabolic syndrome, independent of weight (OR, 1.46), and knee OA was significantly associated with weight (OR, 1.49) and fat-free mass (OR, 2.05), after adjustment for metabolic factors.
Data source: A population-based study of 6,628 individuals who were monitored for the development of hand or knee OA.
Disclosures: The NEO study is supported by the Dutch Arthritis Association, Leiden University Medical Center, and Leiden University. The investigators had no conflicts of interest to declare.

Three miRNA biomarkers predicted osteoarthritis severity
PARIS – Three micro RNAs have been shown to be associated with disease severity in patients with hip or knee osteoarthritis, based on data from a large population-based cohort in Italy*.
The presence of three specific miRNAs are biomarkers that might prove to be useful for predicting OA severity if validated in other cohorts and diverse populations of OA patients, Dr. Christian Beyer reported at a press conference during the annual European Congress of Rheumatology (Ann. Rheum. Dis. 2014 [doi:10.1136/annrheumdis-2013-204698]).

The miRNAs could also be a first step toward finding new OA therapies, such as approaches that avert cartilage loss, said Dr. Beyer of the University of Erlangen–Nuremberg (Germany).
For the study, serum samples from 816 cohort members who had osteoarthritis and were followed for at least 15 years were analyzed for the presence of any of the 374 miRNAs. A microarray screening identified 12 candidate miRNAs, validated in the entire cohort. Based on a regression analysis, the 67 cohort members who went on to have knee or hip arthroplasty were found to differentially express three of the miRNAs: let-7e, miR-454, and miR-885-5p. The most promising of the markers appears to be let-7e.
Let-7e was a negative predictor for total joint arthroplasty with an adjusted hazard ratio of 0.75 (95% confidence interval, 0.58-0.96; P = .021) when normalized to U6, and 0.76 (95% CI, 0.6-0.97; P = .026) after normalization to the Ct-average. However, miR-454 was inversely correlated with severe knee or hip osteoarthritis with an adjusted HR of 0.77 (95% CI, 0.61-0.97; P = .028) when normalized to U6. This correlation was lost when data were normalized to Ct-average (P = .118). Finally, miR-885-5p showed a trend toward a positive relationship with arthroplasty when normalized to U6 (HR, 1.24; 95% CI, 0.95-1.62; P = .107) or to Ct-average (HR, 1.30; 95% CI, 0.99-1.70; P = .056).
If specific miRNAs prove to be biomarkers to predict OA severity, it would offer the ability to use markers that are found in the peripheral circulation, stable over time, and not sex dependent. Such markers also could prove useful for finding new OA therapies, he said.
Next steps for further study include validation of the miRNA biomarkers in other OA cohorts, Dr. Beyer said. The well-defined Bruneck cohort is a stable community that has been extensively studied similar to the Framingham cohort in the United States. The Bruneck cohort is all white, however, and the results of this study need to be validated in diverse populations.
Dr. Beyer declared having no relevant financial disclosures.
On Twitter@maryjodales
CORRECTION, 6/12/2014: An earlier version of the article misstated the location of the study cohort.
PARIS – Three micro RNAs have been shown to be associated with disease severity in patients with hip or knee osteoarthritis, based on data from a large population-based cohort in Italy*.
The presence of three specific miRNAs are biomarkers that might prove to be useful for predicting OA severity if validated in other cohorts and diverse populations of OA patients, Dr. Christian Beyer reported at a press conference during the annual European Congress of Rheumatology (Ann. Rheum. Dis. 2014 [doi:10.1136/annrheumdis-2013-204698]).
The miRNAs could also be a first step toward finding new OA therapies, such as approaches that avert cartilage loss, said Dr. Beyer of the University of Erlangen–Nuremberg (Germany).
For the study, serum samples from 816 cohort members who had osteoarthritis and were followed for at least 15 years were analyzed for the presence of any of the 374 miRNAs. A microarray screening identified 12 candidate miRNAs, validated in the entire cohort. Based on a regression analysis, the 67 cohort members who went on to have knee or hip arthroplasty were found to differentially express three of the miRNAs: let-7e, miR-454, and miR-885-5p. The most promising of the markers appears to be let-7e.
Let-7e was a negative predictor for total joint arthroplasty with an adjusted hazard ratio of 0.75 (95% confidence interval, 0.58-0.96; P = .021) when normalized to U6, and 0.76 (95% CI, 0.6-0.97; P = .026) after normalization to the Ct-average. However, miR-454 was inversely correlated with severe knee or hip osteoarthritis with an adjusted HR of 0.77 (95% CI, 0.61-0.97; P = .028) when normalized to U6. This correlation was lost when data were normalized to Ct-average (P = .118). Finally, miR-885-5p showed a trend toward a positive relationship with arthroplasty when normalized to U6 (HR, 1.24; 95% CI, 0.95-1.62; P = .107) or to Ct-average (HR, 1.30; 95% CI, 0.99-1.70; P = .056).
If specific miRNAs prove to be biomarkers to predict OA severity, it would offer the ability to use markers that are found in the peripheral circulation, stable over time, and not sex dependent. Such markers also could prove useful for finding new OA therapies, he said.
Next steps for further study include validation of the miRNA biomarkers in other OA cohorts, Dr. Beyer said. The well-defined Bruneck cohort is a stable community that has been extensively studied similar to the Framingham cohort in the United States. The Bruneck cohort is all white, however, and the results of this study need to be validated in diverse populations.
Dr. Beyer declared having no relevant financial disclosures.
On Twitter@maryjodales
CORRECTION, 6/12/2014: An earlier version of the article misstated the location of the study cohort.
PARIS – Three micro RNAs have been shown to be associated with disease severity in patients with hip or knee osteoarthritis, based on data from a large population-based cohort in Italy*.
The presence of three specific miRNAs are biomarkers that might prove to be useful for predicting OA severity if validated in other cohorts and diverse populations of OA patients, Dr. Christian Beyer reported at a press conference during the annual European Congress of Rheumatology (Ann. Rheum. Dis. 2014 [doi:10.1136/annrheumdis-2013-204698]).
The miRNAs could also be a first step toward finding new OA therapies, such as approaches that avert cartilage loss, said Dr. Beyer of the University of Erlangen–Nuremberg (Germany).
For the study, serum samples from 816 cohort members who had osteoarthritis and were followed for at least 15 years were analyzed for the presence of any of the 374 miRNAs. A microarray screening identified 12 candidate miRNAs, validated in the entire cohort. Based on a regression analysis, the 67 cohort members who went on to have knee or hip arthroplasty were found to differentially express three of the miRNAs: let-7e, miR-454, and miR-885-5p. The most promising of the markers appears to be let-7e.
Let-7e was a negative predictor for total joint arthroplasty with an adjusted hazard ratio of 0.75 (95% confidence interval, 0.58-0.96; P = .021) when normalized to U6, and 0.76 (95% CI, 0.6-0.97; P = .026) after normalization to the Ct-average. However, miR-454 was inversely correlated with severe knee or hip osteoarthritis with an adjusted HR of 0.77 (95% CI, 0.61-0.97; P = .028) when normalized to U6. This correlation was lost when data were normalized to Ct-average (P = .118). Finally, miR-885-5p showed a trend toward a positive relationship with arthroplasty when normalized to U6 (HR, 1.24; 95% CI, 0.95-1.62; P = .107) or to Ct-average (HR, 1.30; 95% CI, 0.99-1.70; P = .056).
If specific miRNAs prove to be biomarkers to predict OA severity, it would offer the ability to use markers that are found in the peripheral circulation, stable over time, and not sex dependent. Such markers also could prove useful for finding new OA therapies, he said.
Next steps for further study include validation of the miRNA biomarkers in other OA cohorts, Dr. Beyer said. The well-defined Bruneck cohort is a stable community that has been extensively studied similar to the Framingham cohort in the United States. The Bruneck cohort is all white, however, and the results of this study need to be validated in diverse populations.
Dr. Beyer declared having no relevant financial disclosures.
On Twitter@maryjodales
CORRECTION, 6/12/2014: An earlier version of the article misstated the location of the study cohort.
AT THE EULAR CONGRESS 2014
Key clinical point: Biomarkers may allow early interventions to limit osteoarthritis risks, such as cartilage damage.
Major finding: Let-7e was a negative predictor for total joint arthroplasty with an adjusted HR of 0.75 (95% CI, 0.58-0.96; P = .021) when normalized to U6, and 0.76 (95% CI, 0.6-0.97; P = .026) after normalization to the Ct-average.
Data source: The large population-based Bruneck cohort in Italy.
Disclosures: Dr. Beyer had no relevant financial disclosures.

VIDEO: Micro RNA biomarkers hint at potential for predicting OA
PARIS – Newly discovered micro RNA molecules found in the blood of patients before they developed severe osteoarthritis may help predict the disease and potentially identify those who would most benefit from preventive interventions.
That finding emerged from a longitudinal study presented at the annual European Congress of Rheumatology.
By using a screening technique to search a broad array of micro RNAs (miRNAs), Dr. Christian Beyer of the University of Erlangen-Nuremberg (Germany) and his colleagues found several miRNAs that were differentially expressed in the blood of 67 people who developed severe osteoarthritis and underwent at least one total joint replacement and 749 who did not.
One miRNA molecule in particular, known as let-7e, appeared to be "very promising" in this regard, he said. Let-7e is inversely associated with the development of osteoarthritis, with levels correlating with the risk of developing OA, Dr. Beyer said in a video interview with Dr. Christopher Sparks of the University of Liverpool (England).
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PARIS – Newly discovered micro RNA molecules found in the blood of patients before they developed severe osteoarthritis may help predict the disease and potentially identify those who would most benefit from preventive interventions.
That finding emerged from a longitudinal study presented at the annual European Congress of Rheumatology.
By using a screening technique to search a broad array of micro RNAs (miRNAs), Dr. Christian Beyer of the University of Erlangen-Nuremberg (Germany) and his colleagues found several miRNAs that were differentially expressed in the blood of 67 people who developed severe osteoarthritis and underwent at least one total joint replacement and 749 who did not.
One miRNA molecule in particular, known as let-7e, appeared to be "very promising" in this regard, he said. Let-7e is inversely associated with the development of osteoarthritis, with levels correlating with the risk of developing OA, Dr. Beyer said in a video interview with Dr. Christopher Sparks of the University of Liverpool (England).
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PARIS – Newly discovered micro RNA molecules found in the blood of patients before they developed severe osteoarthritis may help predict the disease and potentially identify those who would most benefit from preventive interventions.
That finding emerged from a longitudinal study presented at the annual European Congress of Rheumatology.
By using a screening technique to search a broad array of micro RNAs (miRNAs), Dr. Christian Beyer of the University of Erlangen-Nuremberg (Germany) and his colleagues found several miRNAs that were differentially expressed in the blood of 67 people who developed severe osteoarthritis and underwent at least one total joint replacement and 749 who did not.
One miRNA molecule in particular, known as let-7e, appeared to be "very promising" in this regard, he said. Let-7e is inversely associated with the development of osteoarthritis, with levels correlating with the risk of developing OA, Dr. Beyer said in a video interview with Dr. Christopher Sparks of the University of Liverpool (England).
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE EULAR CONGRESS 2014

Naloxegol cut opioid-associated constipation without impairing pain relief
Treatment with opioid receptor-antagonist naloxegol significantly improved opioid-associated constipation, compared with placebo, without affecting pain scores or daily opioid requirements, according to data from two identical double-blind studies.
Outpatients with noncancer pain who were given 25 mg of naloxegol showed a significantly shorter time to first spontaneous bowel movement after treatment, compared with those given placebo – a median time of 5.9 hours and 12 hours in the two studies, compared with 35.8 hours and 37.2 hours with placebo, according to a study published online June 4 in the New England Journal of Medicine.
Treatment with naloxegol was also associated with a significantly greater number of spontaneous bowel movements over the course of the 12-week study period, compared with placebo, and an increase in the mean number of days per week with one or more spontaneous bowel movements.
The Food and Drug Administration is currently considering whether to approve naloxegol; the agency is expected to decide by Sept. 16, 2014.
The two phase III randomized, controlled studies were nearly identical in size – one including 652 individuals with opioid-induced constipation, and the other including 700 – and entirely identical in design: Participants were randomized to receive either 25 mg or 12.5 mg of naloxegol daily, or placebo.
"In both studies, naloxegol at a dose of 25 mg was associated with an increased rate of response (10-15 percentage points higher than the response with placebo) over a period of 12 weeks," wrote Dr. William D. Chey of the University of Michigan Health System, Ann Arbor, and his colleagues.
The higher dose of naloxegol also was associated with more significant improvements in severity of straining, stool consistency, and the frequency of days with complete, spontaneous bowel movements.
Naloxegol’s benefits were even greater among individuals who had previously failed to respond to laxatives before study enrollment, which accounted for 71% of participants, a prespecified subgroup analysis showed (N. Engl. J. Med. 2014 June 4 [doi:10.1056/NEJMoa1310246]).
"In clinical practice, osmotic and stimulant laxatives are likely to be used before more expensive prescription medications," the researchers wrote. "Thus, the finding that naloxegol proved beneficial in patients who had persistent symptoms of opioid-induced constipation despite using standard laxatives is of potential importance."
There were some dose-related side effects observed in the naloxegol group, including abdominal pain, nausea, diarrhea, and vomiting, occurring soon after initiation of treatment. But most of these effects were mild to moderate.
There had been concern about potential cardiovascular side effects, which had been observed previously with alvimopan, another peripherally-acting mu-opioid antagonist. However the incidence of major cardiovascular events was rare and similar across both active and placebo groups.
Researchers found no significant interaction between naloxegol treatment and daily opioid dose, and there also were no significant differences in the mean change from baseline in pain scores.
Around half of the patients enrolled were taking opioids for back pain, while other reasons included arthritis, joint pain, or fibromyalgia. On average, participants had been taking opioids for 3.65 years.
AstraZeneca supported the study, and the authors declared a range of grants, consultancies, and other financial relationships with several pharmaceutical companies, including AstraZeneca.
Treatment with opioid receptor-antagonist naloxegol significantly improved opioid-associated constipation, compared with placebo, without affecting pain scores or daily opioid requirements, according to data from two identical double-blind studies.
Outpatients with noncancer pain who were given 25 mg of naloxegol showed a significantly shorter time to first spontaneous bowel movement after treatment, compared with those given placebo – a median time of 5.9 hours and 12 hours in the two studies, compared with 35.8 hours and 37.2 hours with placebo, according to a study published online June 4 in the New England Journal of Medicine.
Treatment with naloxegol was also associated with a significantly greater number of spontaneous bowel movements over the course of the 12-week study period, compared with placebo, and an increase in the mean number of days per week with one or more spontaneous bowel movements.
The Food and Drug Administration is currently considering whether to approve naloxegol; the agency is expected to decide by Sept. 16, 2014.
The two phase III randomized, controlled studies were nearly identical in size – one including 652 individuals with opioid-induced constipation, and the other including 700 – and entirely identical in design: Participants were randomized to receive either 25 mg or 12.5 mg of naloxegol daily, or placebo.
"In both studies, naloxegol at a dose of 25 mg was associated with an increased rate of response (10-15 percentage points higher than the response with placebo) over a period of 12 weeks," wrote Dr. William D. Chey of the University of Michigan Health System, Ann Arbor, and his colleagues.
The higher dose of naloxegol also was associated with more significant improvements in severity of straining, stool consistency, and the frequency of days with complete, spontaneous bowel movements.
Naloxegol’s benefits were even greater among individuals who had previously failed to respond to laxatives before study enrollment, which accounted for 71% of participants, a prespecified subgroup analysis showed (N. Engl. J. Med. 2014 June 4 [doi:10.1056/NEJMoa1310246]).
"In clinical practice, osmotic and stimulant laxatives are likely to be used before more expensive prescription medications," the researchers wrote. "Thus, the finding that naloxegol proved beneficial in patients who had persistent symptoms of opioid-induced constipation despite using standard laxatives is of potential importance."
There were some dose-related side effects observed in the naloxegol group, including abdominal pain, nausea, diarrhea, and vomiting, occurring soon after initiation of treatment. But most of these effects were mild to moderate.
There had been concern about potential cardiovascular side effects, which had been observed previously with alvimopan, another peripherally-acting mu-opioid antagonist. However the incidence of major cardiovascular events was rare and similar across both active and placebo groups.
Researchers found no significant interaction between naloxegol treatment and daily opioid dose, and there also were no significant differences in the mean change from baseline in pain scores.
Around half of the patients enrolled were taking opioids for back pain, while other reasons included arthritis, joint pain, or fibromyalgia. On average, participants had been taking opioids for 3.65 years.
AstraZeneca supported the study, and the authors declared a range of grants, consultancies, and other financial relationships with several pharmaceutical companies, including AstraZeneca.
Treatment with opioid receptor-antagonist naloxegol significantly improved opioid-associated constipation, compared with placebo, without affecting pain scores or daily opioid requirements, according to data from two identical double-blind studies.
Outpatients with noncancer pain who were given 25 mg of naloxegol showed a significantly shorter time to first spontaneous bowel movement after treatment, compared with those given placebo – a median time of 5.9 hours and 12 hours in the two studies, compared with 35.8 hours and 37.2 hours with placebo, according to a study published online June 4 in the New England Journal of Medicine.
Treatment with naloxegol was also associated with a significantly greater number of spontaneous bowel movements over the course of the 12-week study period, compared with placebo, and an increase in the mean number of days per week with one or more spontaneous bowel movements.
The Food and Drug Administration is currently considering whether to approve naloxegol; the agency is expected to decide by Sept. 16, 2014.
The two phase III randomized, controlled studies were nearly identical in size – one including 652 individuals with opioid-induced constipation, and the other including 700 – and entirely identical in design: Participants were randomized to receive either 25 mg or 12.5 mg of naloxegol daily, or placebo.
"In both studies, naloxegol at a dose of 25 mg was associated with an increased rate of response (10-15 percentage points higher than the response with placebo) over a period of 12 weeks," wrote Dr. William D. Chey of the University of Michigan Health System, Ann Arbor, and his colleagues.
The higher dose of naloxegol also was associated with more significant improvements in severity of straining, stool consistency, and the frequency of days with complete, spontaneous bowel movements.
Naloxegol’s benefits were even greater among individuals who had previously failed to respond to laxatives before study enrollment, which accounted for 71% of participants, a prespecified subgroup analysis showed (N. Engl. J. Med. 2014 June 4 [doi:10.1056/NEJMoa1310246]).
"In clinical practice, osmotic and stimulant laxatives are likely to be used before more expensive prescription medications," the researchers wrote. "Thus, the finding that naloxegol proved beneficial in patients who had persistent symptoms of opioid-induced constipation despite using standard laxatives is of potential importance."
There were some dose-related side effects observed in the naloxegol group, including abdominal pain, nausea, diarrhea, and vomiting, occurring soon after initiation of treatment. But most of these effects were mild to moderate.
There had been concern about potential cardiovascular side effects, which had been observed previously with alvimopan, another peripherally-acting mu-opioid antagonist. However the incidence of major cardiovascular events was rare and similar across both active and placebo groups.
Researchers found no significant interaction between naloxegol treatment and daily opioid dose, and there also were no significant differences in the mean change from baseline in pain scores.
Around half of the patients enrolled were taking opioids for back pain, while other reasons included arthritis, joint pain, or fibromyalgia. On average, participants had been taking opioids for 3.65 years.
AstraZeneca supported the study, and the authors declared a range of grants, consultancies, and other financial relationships with several pharmaceutical companies, including AstraZeneca.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Naloxegol improves opioid-induced constipation without affecting pain relief.
Major finding: Treatment with naloxegol was associated with a significantly shorter time to first spontaneous bowel movement, a significantly greater number of spontaneous bowel movements, and an increase in the mean number of days per week with one or more spontaneous bowel movements, compared with placebo.
Data source: Two identical 12-week, phase III, double-blind, randomized, controlled trials in a total of 1,352 patients with opioid-associated constipation.
Disclosures: AstraZeneca supported the study, and the authors declared a range of grants, consultancies, and other financial relationships with several pharmaceutical companies including AstraZeneca.
Glucosamine, chondroitin combo found equal to celecoxib for severe knee OA pain
PARIS – A fixed-dose combination of glucosamine and chondroitin sulfate was as good as the cyclo-oxygenase-2 inhibitor celecoxib in relieving moderate to severe knee pain in patients with knee osteoarthritis in the double-blind, noninferiority MOVES trial.
Side effect profiles and tolerability were also similar with glucosamine/chondroitin (Droglican) and celecoxib (Celebrex), with 51% of patients overall experiencing treatment-emergent adverse events, Dr. Marc Hochberg reported at the World Congress on Osteoarthritis.

"In a group that is either contraindicated or relatively contraindicated to celecoxib, you get similar efficacy [with Droglican] at 6 months," he said in an interview.
Dr. Hochberg noted that the phase IV (MOVES) Multicentric Osteoarthritis Intervention Study enrolled patients who were consistent with the European label for celecoxib, meaning that those with prior coronary artery disease or peripheral artery disease were excluded, as were those with unstable diabetes or uncontrolled hypertension.
MOVES was designed to extend the findings of the GAIT (Glucosamine/Chondroitin Arthritis Intervention Trial), which suggested in exploratory analyses that combination 1,500 mg daily glucosamine and 1,200 mg daily chondroitin sulfate was effective in the subgroup with moderate to severe knee osteoarthritis pain, but that either agent alone or in combination was not effective in reducing osteoarthritis knee pain in the overall cohort (N. Engl. J. Med. 2006;354:795-808).
MOVES randomly assigned 606 patients in a double-blind, double-dummy fashion to receive either two capsules of Droglican (250 mg glucosamine and 200 mg chondroitin sulfate) three times daily or celecoxib 200 mg plus five placebo capsules per day. Two-thirds of patients (62.6%) had Kellgren-Lawrence grade 2 radiological changes, and 84% were female. Their mean age was 62.7 years.
At 180 days, the mean WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores in the Droglican and celecoxib groups improved from 372 and 370.6, respectively, to 185.8 and 184.7.
This corresponds to a mean difference of 1.11 units (95% confidence interval, –21.99-19.76; P = .917), which met the noninferiority margin, according to Dr. Hochberg, head of rheumatology and clinical immunology, University of Maryland, Baltimore.The results remained robust in sensitivity analyses.
There also were no significant differences between the two groups in the absolute improvement in the WOMAC stiffness and function scales and the five individual items of the WOMAC pain scale at 6 months, Dr. Hochberg reported at the meeting, sponsored by the Osteoarthritis Research Society International.
Dr. Hochberg reported no conflicts. His coauthors were employees or on the steering committee for Bioiberica, the study sponsor and maker of Droglican.
PARIS – A fixed-dose combination of glucosamine and chondroitin sulfate was as good as the cyclo-oxygenase-2 inhibitor celecoxib in relieving moderate to severe knee pain in patients with knee osteoarthritis in the double-blind, noninferiority MOVES trial.
Side effect profiles and tolerability were also similar with glucosamine/chondroitin (Droglican) and celecoxib (Celebrex), with 51% of patients overall experiencing treatment-emergent adverse events, Dr. Marc Hochberg reported at the World Congress on Osteoarthritis.
"In a group that is either contraindicated or relatively contraindicated to celecoxib, you get similar efficacy [with Droglican] at 6 months," he said in an interview.
Dr. Hochberg noted that the phase IV (MOVES) Multicentric Osteoarthritis Intervention Study enrolled patients who were consistent with the European label for celecoxib, meaning that those with prior coronary artery disease or peripheral artery disease were excluded, as were those with unstable diabetes or uncontrolled hypertension.
MOVES was designed to extend the findings of the GAIT (Glucosamine/Chondroitin Arthritis Intervention Trial), which suggested in exploratory analyses that combination 1,500 mg daily glucosamine and 1,200 mg daily chondroitin sulfate was effective in the subgroup with moderate to severe knee osteoarthritis pain, but that either agent alone or in combination was not effective in reducing osteoarthritis knee pain in the overall cohort (N. Engl. J. Med. 2006;354:795-808).
MOVES randomly assigned 606 patients in a double-blind, double-dummy fashion to receive either two capsules of Droglican (250 mg glucosamine and 200 mg chondroitin sulfate) three times daily or celecoxib 200 mg plus five placebo capsules per day. Two-thirds of patients (62.6%) had Kellgren-Lawrence grade 2 radiological changes, and 84% were female. Their mean age was 62.7 years.
At 180 days, the mean WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores in the Droglican and celecoxib groups improved from 372 and 370.6, respectively, to 185.8 and 184.7.
This corresponds to a mean difference of 1.11 units (95% confidence interval, –21.99-19.76; P = .917), which met the noninferiority margin, according to Dr. Hochberg, head of rheumatology and clinical immunology, University of Maryland, Baltimore.The results remained robust in sensitivity analyses.
There also were no significant differences between the two groups in the absolute improvement in the WOMAC stiffness and function scales and the five individual items of the WOMAC pain scale at 6 months, Dr. Hochberg reported at the meeting, sponsored by the Osteoarthritis Research Society International.
Dr. Hochberg reported no conflicts. His coauthors were employees or on the steering committee for Bioiberica, the study sponsor and maker of Droglican.
PARIS – A fixed-dose combination of glucosamine and chondroitin sulfate was as good as the cyclo-oxygenase-2 inhibitor celecoxib in relieving moderate to severe knee pain in patients with knee osteoarthritis in the double-blind, noninferiority MOVES trial.
Side effect profiles and tolerability were also similar with glucosamine/chondroitin (Droglican) and celecoxib (Celebrex), with 51% of patients overall experiencing treatment-emergent adverse events, Dr. Marc Hochberg reported at the World Congress on Osteoarthritis.
"In a group that is either contraindicated or relatively contraindicated to celecoxib, you get similar efficacy [with Droglican] at 6 months," he said in an interview.
Dr. Hochberg noted that the phase IV (MOVES) Multicentric Osteoarthritis Intervention Study enrolled patients who were consistent with the European label for celecoxib, meaning that those with prior coronary artery disease or peripheral artery disease were excluded, as were those with unstable diabetes or uncontrolled hypertension.
MOVES was designed to extend the findings of the GAIT (Glucosamine/Chondroitin Arthritis Intervention Trial), which suggested in exploratory analyses that combination 1,500 mg daily glucosamine and 1,200 mg daily chondroitin sulfate was effective in the subgroup with moderate to severe knee osteoarthritis pain, but that either agent alone or in combination was not effective in reducing osteoarthritis knee pain in the overall cohort (N. Engl. J. Med. 2006;354:795-808).
MOVES randomly assigned 606 patients in a double-blind, double-dummy fashion to receive either two capsules of Droglican (250 mg glucosamine and 200 mg chondroitin sulfate) three times daily or celecoxib 200 mg plus five placebo capsules per day. Two-thirds of patients (62.6%) had Kellgren-Lawrence grade 2 radiological changes, and 84% were female. Their mean age was 62.7 years.
At 180 days, the mean WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores in the Droglican and celecoxib groups improved from 372 and 370.6, respectively, to 185.8 and 184.7.
This corresponds to a mean difference of 1.11 units (95% confidence interval, –21.99-19.76; P = .917), which met the noninferiority margin, according to Dr. Hochberg, head of rheumatology and clinical immunology, University of Maryland, Baltimore.The results remained robust in sensitivity analyses.
There also were no significant differences between the two groups in the absolute improvement in the WOMAC stiffness and function scales and the five individual items of the WOMAC pain scale at 6 months, Dr. Hochberg reported at the meeting, sponsored by the Osteoarthritis Research Society International.
Dr. Hochberg reported no conflicts. His coauthors were employees or on the steering committee for Bioiberica, the study sponsor and maker of Droglican.
AT OARSI 2014
Key clinical point: Patients with moderate to severe knee OA pain who do not have prior coronary artery disease or peripheral artery disease or unstable diabetes or uncontrolled hypertension have similar reductions in pain with either celecoxib 200 mg daily or a combination of 250 mg glucosamine and 200 mg chondroitin sulfate three times daily.
Major finding: Mean WOMAC scores improved in the Droglican and celecoxib groups from 372 and 370.6 at baseline to 185.8 and 184.7 at 180 days.
Data source: A prospective, double-blind, double-dummy trial in 606 patients with moderate to severe knee OA pain.
Disclosures: Dr. Hochberg reported no conflicts. His coauthors were employees or on the steering committee for Bioiberica, the study sponsor and maker of Droglican.

Consider facet joint OA in older patients with low back pain
DESTIN, FLA. – Facet joint osteoarthritis likely accounts for much of what is classified as "nonspecific" low back pain, according to Dr. Alfred C. Gellhorn.
"Amazingly – and I think sadly for us – the lumbar facet joints really have received very little attention in the literature," Dr. Gellhorn, who works in the department of rehabilitation medicine at the University of Washington, Seattle, said at the annual Congress of Clinical Rheumatology.
Eight of every ten American will experience low back pain at some point during their lifetime; low back pain is second only to the common cold in frequency, is the most common reason for time off work, and has a total social cost of more than $100 billion annually. Up to 85% of patients never receive a definitive diagnosis and are classified has having nonspecific pain, he said.

The facet joints may be responsible for a significant proportion of that pain.
Facet joint cartilage is aneural, but a number of nociceptors exist in the subchondral bone, the synovial folds, and the capsule. Once activated – by synovial inflammation or mechanical factors such as trabecular microfractures, capsular distention, pressure on the subchondral bone as joint load increases, or intramedullary hypertension, for example – the nociceptors may cause secondary reflex contraction of paraspinal muscles.
Patients will report this as spasms, and the contractions can be palpated, Dr. Gellhorn said, noting that prolonged inflammation in and around the facet joints can lead to central sensitization, neuronal plasticity, and development of chronic low back pain.
Facet joint osteoarthritis (OA) is distinct from disc degeneration, but the two conditions are interdependent. Radiographic hallmarks of disc degeneration include disc height loss, dehydration, and endplate sclerosis, whereas radiographic hallmarks of facet joint OA include narrowing of the facet joint space, osteophytosis of articular processes, hypertrophy of articular processes, sclerosis, subchondral erosion, and subchondral cysts.
Older studies that looked at facet joint OA by comparing findings on imaging and symptoms found either no association or only minimal association between facet joint OA and low back pain, but the threshold used in those studies was mild to moderate OA in young and middle-aged subjects.
"That’s the wrong criterion to use," Dr. Gellhorn said, noting that mild facet joint OA is "essentially ubiquitous" by middle age. Moderate to severe facet OA, however, is more symptomatic, and predominantly affects older adults – and should be the criterion used in studies of the condition.
In a recent study of 252 patients with a mean age of 67 years who were participants in the Framingham heart study, severe OA affecting the facet joint was significantly associated with frequent low back pain (odds ratio, 2.2). Disc height narrowing was not associated with low back pain in these patients (Osteoarthritis Cartilage 2013;21:1199-206).
The findings contrast with those from prior studies, likely because the cohort was older (mean age of 67 years vs. 30s to 50s), he said.
It may be that with age, back pain classified as "nonspecific" shifts from discogenic pain in younger adults to facetogenic pain in older adults, he suggested.
Findings with respect to disc pathology and low back pain in young and middle-aged adults seem to support this hypothesis, he noted.
For example, in a study of patients with a mean age of 49 years, low back pain was associated with a twofold increased likelihood of disc height loss and annular tears, and in a study of patients aged 18-50 years, moderate disc height loss was also associated with a twofold increased likelihood of low back pain. In another study of patients with a mean age of 50 years, advanced disc height loss was associated with a threefold increased likelihood of prevalent low back pain.
In another study, severe disc height narrowing was associated with a threefold increase in the odds of low back pain in those younger than age 60 years but not in those over age 60 years.
There are markers for symptomatic facet joint OA. Despite the known association between severe facet joint OA and low back pain, "the truth is there is still limited positive predictive value for that," he said.
"Many older adults with severe facet joint OA on imaging are relatively asymptomatic," he added.
There are some additional imaging makers, however. Symptomatic facet join OA is apparent on single-photon emission computed tomography/computed tomography (SPECT/CT) or fluid-sensitive, fat-suppressed MRI. Also, 64% of patients with suspected facet joint pain in one study had bone marrow lesions on short T1 inversion recovery (STIR) MRI, which were well correlated to the side of pain, he said.
There are no serum biomarkers for the condition at present, he noted.
In addition to older age and these findings on imaging, other risk factors and correlates for facet joint OA include sex (women are 1.5-1.9 times more likely than men to have facet joint OA), race (African Americans are about 60% less likely than white Americans to have facet joint OA), and high body mass index (those with BMI of 25-30 and 30-35 have a three- and fivefold increased risk of lumbar pain associated with facet joint OA, respectively, compared with those with BMI below 25).
Abdominal aortic calcifications and more sagittal orientation of the joints (vs. coronal orientation), also are associated with facet joint OA, Dr. Gellhorn said.
With additional research, these factors could be useful for "disambiguating nonspecific low back pain," he said.
"I think we’re getting closer. We’re not there yet, but we’re getting closer," he said.
Clinically, facet joint OA often presents as localized back or neck pain at C5-C6 with some radiation into the scapular region.
"It’s less clear in the lumbar spine, but almost always people will have pain in the lumbar region, and almost always they will have pain that radiates into the buttocks," he said, noting that pain radiating into the anterior or lateral thighs can be associated with facet joint OA, but pain that extends below the knees is more likely to be radicular.
There are no specific examination maneuvers that are pathognomonic – or even particularly helpful – for the condition, he added.
It is important to keep in mind that many patients will have associated conditions, including spondylolisthesis, disc degeneration, scoliosis, muscle atrophy, and spinal stenosis.
"It’s easy to get overwhelmed in the face of this, but I would urge you not to, and to still try to disentangle some of these concepts of low back pain without throwing up your hands," he said.
Although anesthetic blockade of the medial branches of the dorsal primary ramus (or "medial branch blocks,") are considered the gold standard for diagnosis, they are controversial, have an unacceptably high rate of false-positive results with a single block, and thus may require comparative blocks, which can result in numerous spinal injections.
This is problematic; there is no good way to make the diagnosis before doing more rational, conservative treatment, he said.
"I think that there are probably better things than doing 30 injections into someone’s spine to establish a diagnosis," he said.
In fact, treatment for facet joint OA generally involves physical activity.
"You don’t want to push these people to their limits, but certainly it is important to have them move and to have them keep the strength in their spine," he said.
In the absence of good studies evaluating noninterventional therapy for confirmed facet joint pain, treatment is generally based on findings in patients with chronic nonspecific low back pain and knee OA, and there is evidence in both of those settings that suggest exercise is helpful for increasing strength and decreasing pain and disability.
A Cochrane review showed that exercise therapy provides mild to moderate benefit. Additional studies have suggested that early referral to physical therapy results in modest improvement in function at 12 months in older adults, suggesting physical therapy provides longer-term results than many other interventions for low back pain, which tend to provide only short-term relief, he noted.
Furthermore, patients who have physical therapy tend to require fewer interventions. Dr. Gellhorn found in a recent study that physical therapy in a Medicare population with low back pain was associated with fewer lumbar injections, physician office visits, and lumbar surgeries.
"So it’s very reasonable to send your patients with facet joint OA to PT," he said.
Other treatments that may have some benefit if physical activity is inadequate include intra-articular steroid injections and radiofrequency denervation.
In studies that used SPECT for inclusion criteria, intra-articular injections were better than medial branch blocks at 3 months, and were more effective at 1 month and 3 months than were injections used in studies that did not use SPECT for inclusion, he said.
Injections were not useful in studies that used physical examination or diagnostic block for inclusion.
"So if you’re basing it on metabolic activity, you’re likely to have a good outcome from your injection," he said.
Radiofrequency denervation tends to work better in the cervical spine than in the lumbar spine, but it is difficult to justify in practice because it requires medial branch block, or double or even triple block to optimize success, and because it is associated with a number of potential complications, such as loss of innervation to the multifidus muscles.
In his practice he first screens for red flags in patients who present with low back pain. Next, he gets an X-ray to look for alignment issues, and he "heavily considers – if the clinical picture fits" – whether facet joint OA might be the cause of the pain.
"I’ll talk to them about it, and then almost always, I’ll send them for an empiric trial of physical therapy plus or minus some analgesics – Tylenol or NSAIDs," he said.
If patients experience improved function and a decrease in symptoms within 6-8 weeks, he recommends that they begin a more interesting (than their home physical therapy regimen) exercise program, such as yoga or Pilates to help them maintain those gains; if they remain symptomatic, he images them.
He starts with SPECT/CT rather than MRI if facet joint OA is high on his differential list for the patient, and if that’s positive, he will consider intra-articular steroid injections. If the injections are effective he recommends yoga and/or Pilates for maintaining the gains.
In rare cases a patient doesn’t respond to the injections, and then he will consider more aggressive treatment, such as medial branch block or radiofrequency denervation.
Understanding of facet joint OA has been slow to emerge, but progress is being made, Dr. Gellhorn said.
For example, the work with SPECT/CT and STIR MRI is very exciting, he said.
"I think this is going to give us a number of things to work with: first and foremost, it’s going to give us better criteria to diagnose patients and enroll them in treatment studies," he said.
Serum, urine, and genetic biomarkers, on the other hand, are interesting and on the horizon, "but we’re not really there yet," he added.
"But I think we will be able to at least use imaging studies to monitor some response to treatment," he said.
Additional study is also needed with respect to conservative treatments. Studies comparing different exercise programs, including studies comparing strength vs. flexibility and extension vs. flexion, are needed.
Regenerative treatments, such as platelet rich plasma and autologous stem cells are another area of interest, he said.
Dr. Gellhorn reported having no disclosures.
DESTIN, FLA. – Facet joint osteoarthritis likely accounts for much of what is classified as "nonspecific" low back pain, according to Dr. Alfred C. Gellhorn.
"Amazingly – and I think sadly for us – the lumbar facet joints really have received very little attention in the literature," Dr. Gellhorn, who works in the department of rehabilitation medicine at the University of Washington, Seattle, said at the annual Congress of Clinical Rheumatology.
Eight of every ten American will experience low back pain at some point during their lifetime; low back pain is second only to the common cold in frequency, is the most common reason for time off work, and has a total social cost of more than $100 billion annually. Up to 85% of patients never receive a definitive diagnosis and are classified has having nonspecific pain, he said.
The facet joints may be responsible for a significant proportion of that pain.
Facet joint cartilage is aneural, but a number of nociceptors exist in the subchondral bone, the synovial folds, and the capsule. Once activated – by synovial inflammation or mechanical factors such as trabecular microfractures, capsular distention, pressure on the subchondral bone as joint load increases, or intramedullary hypertension, for example – the nociceptors may cause secondary reflex contraction of paraspinal muscles.
Patients will report this as spasms, and the contractions can be palpated, Dr. Gellhorn said, noting that prolonged inflammation in and around the facet joints can lead to central sensitization, neuronal plasticity, and development of chronic low back pain.
Facet joint osteoarthritis (OA) is distinct from disc degeneration, but the two conditions are interdependent. Radiographic hallmarks of disc degeneration include disc height loss, dehydration, and endplate sclerosis, whereas radiographic hallmarks of facet joint OA include narrowing of the facet joint space, osteophytosis of articular processes, hypertrophy of articular processes, sclerosis, subchondral erosion, and subchondral cysts.
Older studies that looked at facet joint OA by comparing findings on imaging and symptoms found either no association or only minimal association between facet joint OA and low back pain, but the threshold used in those studies was mild to moderate OA in young and middle-aged subjects.
"That’s the wrong criterion to use," Dr. Gellhorn said, noting that mild facet joint OA is "essentially ubiquitous" by middle age. Moderate to severe facet OA, however, is more symptomatic, and predominantly affects older adults – and should be the criterion used in studies of the condition.
In a recent study of 252 patients with a mean age of 67 years who were participants in the Framingham heart study, severe OA affecting the facet joint was significantly associated with frequent low back pain (odds ratio, 2.2). Disc height narrowing was not associated with low back pain in these patients (Osteoarthritis Cartilage 2013;21:1199-206).
The findings contrast with those from prior studies, likely because the cohort was older (mean age of 67 years vs. 30s to 50s), he said.
It may be that with age, back pain classified as "nonspecific" shifts from discogenic pain in younger adults to facetogenic pain in older adults, he suggested.
Findings with respect to disc pathology and low back pain in young and middle-aged adults seem to support this hypothesis, he noted.
For example, in a study of patients with a mean age of 49 years, low back pain was associated with a twofold increased likelihood of disc height loss and annular tears, and in a study of patients aged 18-50 years, moderate disc height loss was also associated with a twofold increased likelihood of low back pain. In another study of patients with a mean age of 50 years, advanced disc height loss was associated with a threefold increased likelihood of prevalent low back pain.
In another study, severe disc height narrowing was associated with a threefold increase in the odds of low back pain in those younger than age 60 years but not in those over age 60 years.
There are markers for symptomatic facet joint OA. Despite the known association between severe facet joint OA and low back pain, "the truth is there is still limited positive predictive value for that," he said.
"Many older adults with severe facet joint OA on imaging are relatively asymptomatic," he added.
There are some additional imaging makers, however. Symptomatic facet join OA is apparent on single-photon emission computed tomography/computed tomography (SPECT/CT) or fluid-sensitive, fat-suppressed MRI. Also, 64% of patients with suspected facet joint pain in one study had bone marrow lesions on short T1 inversion recovery (STIR) MRI, which were well correlated to the side of pain, he said.
There are no serum biomarkers for the condition at present, he noted.
In addition to older age and these findings on imaging, other risk factors and correlates for facet joint OA include sex (women are 1.5-1.9 times more likely than men to have facet joint OA), race (African Americans are about 60% less likely than white Americans to have facet joint OA), and high body mass index (those with BMI of 25-30 and 30-35 have a three- and fivefold increased risk of lumbar pain associated with facet joint OA, respectively, compared with those with BMI below 25).
Abdominal aortic calcifications and more sagittal orientation of the joints (vs. coronal orientation), also are associated with facet joint OA, Dr. Gellhorn said.
With additional research, these factors could be useful for "disambiguating nonspecific low back pain," he said.
"I think we’re getting closer. We’re not there yet, but we’re getting closer," he said.
Clinically, facet joint OA often presents as localized back or neck pain at C5-C6 with some radiation into the scapular region.
"It’s less clear in the lumbar spine, but almost always people will have pain in the lumbar region, and almost always they will have pain that radiates into the buttocks," he said, noting that pain radiating into the anterior or lateral thighs can be associated with facet joint OA, but pain that extends below the knees is more likely to be radicular.
There are no specific examination maneuvers that are pathognomonic – or even particularly helpful – for the condition, he added.
It is important to keep in mind that many patients will have associated conditions, including spondylolisthesis, disc degeneration, scoliosis, muscle atrophy, and spinal stenosis.
"It’s easy to get overwhelmed in the face of this, but I would urge you not to, and to still try to disentangle some of these concepts of low back pain without throwing up your hands," he said.
Although anesthetic blockade of the medial branches of the dorsal primary ramus (or "medial branch blocks,") are considered the gold standard for diagnosis, they are controversial, have an unacceptably high rate of false-positive results with a single block, and thus may require comparative blocks, which can result in numerous spinal injections.
This is problematic; there is no good way to make the diagnosis before doing more rational, conservative treatment, he said.
"I think that there are probably better things than doing 30 injections into someone’s spine to establish a diagnosis," he said.
In fact, treatment for facet joint OA generally involves physical activity.
"You don’t want to push these people to their limits, but certainly it is important to have them move and to have them keep the strength in their spine," he said.
In the absence of good studies evaluating noninterventional therapy for confirmed facet joint pain, treatment is generally based on findings in patients with chronic nonspecific low back pain and knee OA, and there is evidence in both of those settings that suggest exercise is helpful for increasing strength and decreasing pain and disability.
A Cochrane review showed that exercise therapy provides mild to moderate benefit. Additional studies have suggested that early referral to physical therapy results in modest improvement in function at 12 months in older adults, suggesting physical therapy provides longer-term results than many other interventions for low back pain, which tend to provide only short-term relief, he noted.
Furthermore, patients who have physical therapy tend to require fewer interventions. Dr. Gellhorn found in a recent study that physical therapy in a Medicare population with low back pain was associated with fewer lumbar injections, physician office visits, and lumbar surgeries.
"So it’s very reasonable to send your patients with facet joint OA to PT," he said.
Other treatments that may have some benefit if physical activity is inadequate include intra-articular steroid injections and radiofrequency denervation.
In studies that used SPECT for inclusion criteria, intra-articular injections were better than medial branch blocks at 3 months, and were more effective at 1 month and 3 months than were injections used in studies that did not use SPECT for inclusion, he said.
Injections were not useful in studies that used physical examination or diagnostic block for inclusion.
"So if you’re basing it on metabolic activity, you’re likely to have a good outcome from your injection," he said.
Radiofrequency denervation tends to work better in the cervical spine than in the lumbar spine, but it is difficult to justify in practice because it requires medial branch block, or double or even triple block to optimize success, and because it is associated with a number of potential complications, such as loss of innervation to the multifidus muscles.
In his practice he first screens for red flags in patients who present with low back pain. Next, he gets an X-ray to look for alignment issues, and he "heavily considers – if the clinical picture fits" – whether facet joint OA might be the cause of the pain.
"I’ll talk to them about it, and then almost always, I’ll send them for an empiric trial of physical therapy plus or minus some analgesics – Tylenol or NSAIDs," he said.
If patients experience improved function and a decrease in symptoms within 6-8 weeks, he recommends that they begin a more interesting (than their home physical therapy regimen) exercise program, such as yoga or Pilates to help them maintain those gains; if they remain symptomatic, he images them.
He starts with SPECT/CT rather than MRI if facet joint OA is high on his differential list for the patient, and if that’s positive, he will consider intra-articular steroid injections. If the injections are effective he recommends yoga and/or Pilates for maintaining the gains.
In rare cases a patient doesn’t respond to the injections, and then he will consider more aggressive treatment, such as medial branch block or radiofrequency denervation.
Understanding of facet joint OA has been slow to emerge, but progress is being made, Dr. Gellhorn said.
For example, the work with SPECT/CT and STIR MRI is very exciting, he said.
"I think this is going to give us a number of things to work with: first and foremost, it’s going to give us better criteria to diagnose patients and enroll them in treatment studies," he said.
Serum, urine, and genetic biomarkers, on the other hand, are interesting and on the horizon, "but we’re not really there yet," he added.
"But I think we will be able to at least use imaging studies to monitor some response to treatment," he said.
Additional study is also needed with respect to conservative treatments. Studies comparing different exercise programs, including studies comparing strength vs. flexibility and extension vs. flexion, are needed.
Regenerative treatments, such as platelet rich plasma and autologous stem cells are another area of interest, he said.
Dr. Gellhorn reported having no disclosures.
DESTIN, FLA. – Facet joint osteoarthritis likely accounts for much of what is classified as "nonspecific" low back pain, according to Dr. Alfred C. Gellhorn.
"Amazingly – and I think sadly for us – the lumbar facet joints really have received very little attention in the literature," Dr. Gellhorn, who works in the department of rehabilitation medicine at the University of Washington, Seattle, said at the annual Congress of Clinical Rheumatology.
Eight of every ten American will experience low back pain at some point during their lifetime; low back pain is second only to the common cold in frequency, is the most common reason for time off work, and has a total social cost of more than $100 billion annually. Up to 85% of patients never receive a definitive diagnosis and are classified has having nonspecific pain, he said.
The facet joints may be responsible for a significant proportion of that pain.
Facet joint cartilage is aneural, but a number of nociceptors exist in the subchondral bone, the synovial folds, and the capsule. Once activated – by synovial inflammation or mechanical factors such as trabecular microfractures, capsular distention, pressure on the subchondral bone as joint load increases, or intramedullary hypertension, for example – the nociceptors may cause secondary reflex contraction of paraspinal muscles.
Patients will report this as spasms, and the contractions can be palpated, Dr. Gellhorn said, noting that prolonged inflammation in and around the facet joints can lead to central sensitization, neuronal plasticity, and development of chronic low back pain.
Facet joint osteoarthritis (OA) is distinct from disc degeneration, but the two conditions are interdependent. Radiographic hallmarks of disc degeneration include disc height loss, dehydration, and endplate sclerosis, whereas radiographic hallmarks of facet joint OA include narrowing of the facet joint space, osteophytosis of articular processes, hypertrophy of articular processes, sclerosis, subchondral erosion, and subchondral cysts.
Older studies that looked at facet joint OA by comparing findings on imaging and symptoms found either no association or only minimal association between facet joint OA and low back pain, but the threshold used in those studies was mild to moderate OA in young and middle-aged subjects.
"That’s the wrong criterion to use," Dr. Gellhorn said, noting that mild facet joint OA is "essentially ubiquitous" by middle age. Moderate to severe facet OA, however, is more symptomatic, and predominantly affects older adults – and should be the criterion used in studies of the condition.
In a recent study of 252 patients with a mean age of 67 years who were participants in the Framingham heart study, severe OA affecting the facet joint was significantly associated with frequent low back pain (odds ratio, 2.2). Disc height narrowing was not associated with low back pain in these patients (Osteoarthritis Cartilage 2013;21:1199-206).
The findings contrast with those from prior studies, likely because the cohort was older (mean age of 67 years vs. 30s to 50s), he said.
It may be that with age, back pain classified as "nonspecific" shifts from discogenic pain in younger adults to facetogenic pain in older adults, he suggested.
Findings with respect to disc pathology and low back pain in young and middle-aged adults seem to support this hypothesis, he noted.
For example, in a study of patients with a mean age of 49 years, low back pain was associated with a twofold increased likelihood of disc height loss and annular tears, and in a study of patients aged 18-50 years, moderate disc height loss was also associated with a twofold increased likelihood of low back pain. In another study of patients with a mean age of 50 years, advanced disc height loss was associated with a threefold increased likelihood of prevalent low back pain.
In another study, severe disc height narrowing was associated with a threefold increase in the odds of low back pain in those younger than age 60 years but not in those over age 60 years.
There are markers for symptomatic facet joint OA. Despite the known association between severe facet joint OA and low back pain, "the truth is there is still limited positive predictive value for that," he said.
"Many older adults with severe facet joint OA on imaging are relatively asymptomatic," he added.
There are some additional imaging makers, however. Symptomatic facet join OA is apparent on single-photon emission computed tomography/computed tomography (SPECT/CT) or fluid-sensitive, fat-suppressed MRI. Also, 64% of patients with suspected facet joint pain in one study had bone marrow lesions on short T1 inversion recovery (STIR) MRI, which were well correlated to the side of pain, he said.
There are no serum biomarkers for the condition at present, he noted.
In addition to older age and these findings on imaging, other risk factors and correlates for facet joint OA include sex (women are 1.5-1.9 times more likely than men to have facet joint OA), race (African Americans are about 60% less likely than white Americans to have facet joint OA), and high body mass index (those with BMI of 25-30 and 30-35 have a three- and fivefold increased risk of lumbar pain associated with facet joint OA, respectively, compared with those with BMI below 25).
Abdominal aortic calcifications and more sagittal orientation of the joints (vs. coronal orientation), also are associated with facet joint OA, Dr. Gellhorn said.
With additional research, these factors could be useful for "disambiguating nonspecific low back pain," he said.
"I think we’re getting closer. We’re not there yet, but we’re getting closer," he said.
Clinically, facet joint OA often presents as localized back or neck pain at C5-C6 with some radiation into the scapular region.
"It’s less clear in the lumbar spine, but almost always people will have pain in the lumbar region, and almost always they will have pain that radiates into the buttocks," he said, noting that pain radiating into the anterior or lateral thighs can be associated with facet joint OA, but pain that extends below the knees is more likely to be radicular.
There are no specific examination maneuvers that are pathognomonic – or even particularly helpful – for the condition, he added.
It is important to keep in mind that many patients will have associated conditions, including spondylolisthesis, disc degeneration, scoliosis, muscle atrophy, and spinal stenosis.
"It’s easy to get overwhelmed in the face of this, but I would urge you not to, and to still try to disentangle some of these concepts of low back pain without throwing up your hands," he said.
Although anesthetic blockade of the medial branches of the dorsal primary ramus (or "medial branch blocks,") are considered the gold standard for diagnosis, they are controversial, have an unacceptably high rate of false-positive results with a single block, and thus may require comparative blocks, which can result in numerous spinal injections.
This is problematic; there is no good way to make the diagnosis before doing more rational, conservative treatment, he said.
"I think that there are probably better things than doing 30 injections into someone’s spine to establish a diagnosis," he said.
In fact, treatment for facet joint OA generally involves physical activity.
"You don’t want to push these people to their limits, but certainly it is important to have them move and to have them keep the strength in their spine," he said.
In the absence of good studies evaluating noninterventional therapy for confirmed facet joint pain, treatment is generally based on findings in patients with chronic nonspecific low back pain and knee OA, and there is evidence in both of those settings that suggest exercise is helpful for increasing strength and decreasing pain and disability.
A Cochrane review showed that exercise therapy provides mild to moderate benefit. Additional studies have suggested that early referral to physical therapy results in modest improvement in function at 12 months in older adults, suggesting physical therapy provides longer-term results than many other interventions for low back pain, which tend to provide only short-term relief, he noted.
Furthermore, patients who have physical therapy tend to require fewer interventions. Dr. Gellhorn found in a recent study that physical therapy in a Medicare population with low back pain was associated with fewer lumbar injections, physician office visits, and lumbar surgeries.
"So it’s very reasonable to send your patients with facet joint OA to PT," he said.
Other treatments that may have some benefit if physical activity is inadequate include intra-articular steroid injections and radiofrequency denervation.
In studies that used SPECT for inclusion criteria, intra-articular injections were better than medial branch blocks at 3 months, and were more effective at 1 month and 3 months than were injections used in studies that did not use SPECT for inclusion, he said.
Injections were not useful in studies that used physical examination or diagnostic block for inclusion.
"So if you’re basing it on metabolic activity, you’re likely to have a good outcome from your injection," he said.
Radiofrequency denervation tends to work better in the cervical spine than in the lumbar spine, but it is difficult to justify in practice because it requires medial branch block, or double or even triple block to optimize success, and because it is associated with a number of potential complications, such as loss of innervation to the multifidus muscles.
In his practice he first screens for red flags in patients who present with low back pain. Next, he gets an X-ray to look for alignment issues, and he "heavily considers – if the clinical picture fits" – whether facet joint OA might be the cause of the pain.
"I’ll talk to them about it, and then almost always, I’ll send them for an empiric trial of physical therapy plus or minus some analgesics – Tylenol or NSAIDs," he said.
If patients experience improved function and a decrease in symptoms within 6-8 weeks, he recommends that they begin a more interesting (than their home physical therapy regimen) exercise program, such as yoga or Pilates to help them maintain those gains; if they remain symptomatic, he images them.
He starts with SPECT/CT rather than MRI if facet joint OA is high on his differential list for the patient, and if that’s positive, he will consider intra-articular steroid injections. If the injections are effective he recommends yoga and/or Pilates for maintaining the gains.
In rare cases a patient doesn’t respond to the injections, and then he will consider more aggressive treatment, such as medial branch block or radiofrequency denervation.
Understanding of facet joint OA has been slow to emerge, but progress is being made, Dr. Gellhorn said.
For example, the work with SPECT/CT and STIR MRI is very exciting, he said.
"I think this is going to give us a number of things to work with: first and foremost, it’s going to give us better criteria to diagnose patients and enroll them in treatment studies," he said.
Serum, urine, and genetic biomarkers, on the other hand, are interesting and on the horizon, "but we’re not really there yet," he added.
"But I think we will be able to at least use imaging studies to monitor some response to treatment," he said.
Additional study is also needed with respect to conservative treatments. Studies comparing different exercise programs, including studies comparing strength vs. flexibility and extension vs. flexion, are needed.
Regenerative treatments, such as platelet rich plasma and autologous stem cells are another area of interest, he said.
Dr. Gellhorn reported having no disclosures.
EXPERT ANALYSIS FROM CCR 14

Physical therapy failed to improve hip OA
Physical therapy incorporating manual therapy, exercise, patient education, and in some cases use of an assistive device for walking, failed to lessen pain or improve function in hip osteoarthritis beyond what was achieved with a sham therapy, according to a report published online May 20 in JAMA.
The multimodal active therapy, which was typical of those used in clinical practice, also was associated with significantly more adverse events than the sham treatment, including hip pain, hip stiffness, back pain, and pain in other bodily regions. "These results question the benefits of such a physical therapy program for this patient population," said Kim L. Bennell, Ph.D., foundation director and professor, centre for health, exercise and sports medicine, department of physiotherapy, Melbourne School of Health Sciences, the University of Melbourne, and her associates.

Very few clinical studies have assessed multimodal physical therapy (PT) for this indication, and those that have done so never compared it against a placebo. Studies that at least compared PT against usual care or no treatment have yielded conflicting results. Nevertheless, clinical guidelines recommend "conservative nonpharmacological physiotherapeutic treatments for hip osteoarthritis irrespective of disease severity, pain levels, and functional status," the investigators noted.
To test the efficacy of PT for hip OA, Dr. Bennell and her colleagues compared a 12-week course against 12 weeks of sham therapy in 102 patients aged 50 years and older who had moderate pain and moderate impairment of daily activities. Both interventions were delivered by experienced physical therapists at nine private clinics.
The PT included hip thrust manipulation, hip-lumbar spine mobilization, deep-tissue massage, and muscle stretches. Patients also were instructed to perform home exercises four times per week to strengthen the hip abductors and quadriceps, improve range of motion, and improve balance and gait, and they were given a walking stick if appropriate. The sham treatment comprised inactive ultrasound and the application of an inert gel to the hip region.
At 13- and 36-week follow-up, patients in both study groups reported lessening of pain and improvement in function. However, the changes were not significantly different between active and sham therapy on several instruments: a measure of hip pain intensity, the Hip Osteoarthritis Outcome Scale, a quality-of-life score, a global measure of body pain and function, the Arthritis Self-Efficacy Scale, the Pain Catastrophizing Scale, the Physical Activity Scale for the Elderly, a measure of hip range of motion, a measure of isometric strength of hip and thigh muscles, a stair-climbing test, a measure of walking velocity, and a balance test.
Nineteen of 46 patients (41%) who received active PT reported adverse events such as aggravated hip pain or back pain, compared with only 7 of 49 (14%) who received sham treatment, the investigators said (JAMA 2014 May 20 [doi:10.1001/jama.2014.4591]).
The "benefits" in both study groups, particularly in patient-reported pain and function, likely reflect the significant placebo effect that has been reported previously with hip OA. Both study groups participated in "10 individual sessions with an attentive therapist and treatment that involved skin stimulation and touch," which, together with patient confidence in their therapy, "are known to contribute to an effective placebo response," Dr. Bennell and her associates said.
This study was supported by Australia’s National Health and Medical Research Council. Dr. Bennell reported that she receives royalties for an educational DVD on knee OA and a commercially available shoe from Asics Oceania; no other investigator reported having potential conflicts of interest.
Physical therapy incorporating manual therapy, exercise, patient education, and in some cases use of an assistive device for walking, failed to lessen pain or improve function in hip osteoarthritis beyond what was achieved with a sham therapy, according to a report published online May 20 in JAMA.
The multimodal active therapy, which was typical of those used in clinical practice, also was associated with significantly more adverse events than the sham treatment, including hip pain, hip stiffness, back pain, and pain in other bodily regions. "These results question the benefits of such a physical therapy program for this patient population," said Kim L. Bennell, Ph.D., foundation director and professor, centre for health, exercise and sports medicine, department of physiotherapy, Melbourne School of Health Sciences, the University of Melbourne, and her associates.
Very few clinical studies have assessed multimodal physical therapy (PT) for this indication, and those that have done so never compared it against a placebo. Studies that at least compared PT against usual care or no treatment have yielded conflicting results. Nevertheless, clinical guidelines recommend "conservative nonpharmacological physiotherapeutic treatments for hip osteoarthritis irrespective of disease severity, pain levels, and functional status," the investigators noted.
To test the efficacy of PT for hip OA, Dr. Bennell and her colleagues compared a 12-week course against 12 weeks of sham therapy in 102 patients aged 50 years and older who had moderate pain and moderate impairment of daily activities. Both interventions were delivered by experienced physical therapists at nine private clinics.
The PT included hip thrust manipulation, hip-lumbar spine mobilization, deep-tissue massage, and muscle stretches. Patients also were instructed to perform home exercises four times per week to strengthen the hip abductors and quadriceps, improve range of motion, and improve balance and gait, and they were given a walking stick if appropriate. The sham treatment comprised inactive ultrasound and the application of an inert gel to the hip region.
At 13- and 36-week follow-up, patients in both study groups reported lessening of pain and improvement in function. However, the changes were not significantly different between active and sham therapy on several instruments: a measure of hip pain intensity, the Hip Osteoarthritis Outcome Scale, a quality-of-life score, a global measure of body pain and function, the Arthritis Self-Efficacy Scale, the Pain Catastrophizing Scale, the Physical Activity Scale for the Elderly, a measure of hip range of motion, a measure of isometric strength of hip and thigh muscles, a stair-climbing test, a measure of walking velocity, and a balance test.
Nineteen of 46 patients (41%) who received active PT reported adverse events such as aggravated hip pain or back pain, compared with only 7 of 49 (14%) who received sham treatment, the investigators said (JAMA 2014 May 20 [doi:10.1001/jama.2014.4591]).
The "benefits" in both study groups, particularly in patient-reported pain and function, likely reflect the significant placebo effect that has been reported previously with hip OA. Both study groups participated in "10 individual sessions with an attentive therapist and treatment that involved skin stimulation and touch," which, together with patient confidence in their therapy, "are known to contribute to an effective placebo response," Dr. Bennell and her associates said.
This study was supported by Australia’s National Health and Medical Research Council. Dr. Bennell reported that she receives royalties for an educational DVD on knee OA and a commercially available shoe from Asics Oceania; no other investigator reported having potential conflicts of interest.
Physical therapy incorporating manual therapy, exercise, patient education, and in some cases use of an assistive device for walking, failed to lessen pain or improve function in hip osteoarthritis beyond what was achieved with a sham therapy, according to a report published online May 20 in JAMA.
The multimodal active therapy, which was typical of those used in clinical practice, also was associated with significantly more adverse events than the sham treatment, including hip pain, hip stiffness, back pain, and pain in other bodily regions. "These results question the benefits of such a physical therapy program for this patient population," said Kim L. Bennell, Ph.D., foundation director and professor, centre for health, exercise and sports medicine, department of physiotherapy, Melbourne School of Health Sciences, the University of Melbourne, and her associates.
Very few clinical studies have assessed multimodal physical therapy (PT) for this indication, and those that have done so never compared it against a placebo. Studies that at least compared PT against usual care or no treatment have yielded conflicting results. Nevertheless, clinical guidelines recommend "conservative nonpharmacological physiotherapeutic treatments for hip osteoarthritis irrespective of disease severity, pain levels, and functional status," the investigators noted.
To test the efficacy of PT for hip OA, Dr. Bennell and her colleagues compared a 12-week course against 12 weeks of sham therapy in 102 patients aged 50 years and older who had moderate pain and moderate impairment of daily activities. Both interventions were delivered by experienced physical therapists at nine private clinics.
The PT included hip thrust manipulation, hip-lumbar spine mobilization, deep-tissue massage, and muscle stretches. Patients also were instructed to perform home exercises four times per week to strengthen the hip abductors and quadriceps, improve range of motion, and improve balance and gait, and they were given a walking stick if appropriate. The sham treatment comprised inactive ultrasound and the application of an inert gel to the hip region.
At 13- and 36-week follow-up, patients in both study groups reported lessening of pain and improvement in function. However, the changes were not significantly different between active and sham therapy on several instruments: a measure of hip pain intensity, the Hip Osteoarthritis Outcome Scale, a quality-of-life score, a global measure of body pain and function, the Arthritis Self-Efficacy Scale, the Pain Catastrophizing Scale, the Physical Activity Scale for the Elderly, a measure of hip range of motion, a measure of isometric strength of hip and thigh muscles, a stair-climbing test, a measure of walking velocity, and a balance test.
Nineteen of 46 patients (41%) who received active PT reported adverse events such as aggravated hip pain or back pain, compared with only 7 of 49 (14%) who received sham treatment, the investigators said (JAMA 2014 May 20 [doi:10.1001/jama.2014.4591]).
The "benefits" in both study groups, particularly in patient-reported pain and function, likely reflect the significant placebo effect that has been reported previously with hip OA. Both study groups participated in "10 individual sessions with an attentive therapist and treatment that involved skin stimulation and touch," which, together with patient confidence in their therapy, "are known to contribute to an effective placebo response," Dr. Bennell and her associates said.
This study was supported by Australia’s National Health and Medical Research Council. Dr. Bennell reported that she receives royalties for an educational DVD on knee OA and a commercially available shoe from Asics Oceania; no other investigator reported having potential conflicts of interest.
FROM JAMA
Key clinical point: Think twice before referring patients with hip OA for PT.
Major finding: Physical therapy offered no advantage over sham therapy at 13-week and 36-week follow-up, on numerous measures of hip pain, activities of daily living, quality of life, global body pain and function, pain catastrophizing, physical activity, hip range of motion, strength of hip and thigh muscles, stair-climbing ability, walking velocity, or balance.
Data source: A randomized, partially blinded clinical trial comparing pain and function outcomes between 49 knee OA patients given multimodal PT and 53 given a sham therapy for 12 weeks.
Disclosures: This study was supported by Australia’s National Health and Medical Research Council. Dr. Bennell reported that she receives royalties for an educational DVD on knee OA and a commercially available shoe from Asics Oceania; no other potential conflicts of interest were reported.

Inflammatory ultrasound changes track with hand OA progression
PARIS – Inflammatory ultrasound features in hand osteoarthritis may point clinicians toward patients at higher risk for radiographic progression, a longitudinal study suggests.
"We found inflammatory ultrasound features are independently associated with both progressive joint space narrowing and progression of osteophytes in hand osteoarthritis. This is especially true with persistent inflammation," Dr. Marion Kortekaas said at the World Congress on Osteoarthritis.

She presented data on 56 consecutive hand OA patients who underwent baseline and 2.3-year follow-up radiographic and ultrasound assessment of all first carpometacarpal, distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first interphalangeal joints.
Radiographs were scored for osteophytes and joint space narrowing using the OARSI Atlas grading system (0-3 scale). Ultrasound synovial thickening, effusion, and power Doppler signal (PDS) were scored on a validated 3-point scale, with 3 being severe. Progression was defined as at least one grade increase of either joint space narrowing or osteophytes, explained Dr. Kortekaas, a rheumatologist at Leiden (the Netherlands) University Medical Center.
Most patients were female (86%) and their average age was 61 years. Patients with rheumatic diseases, trauma/operation, and corticosteroid use were excluded.
Of 1,680 joints at baseline, 141 (8.4%) had synovial thickening, 332 (19.8%) effusion, and 146 (8.7%) PDS.
At follow-up, progression of osteophytes and joint space narrowing was present in 120 and 96 joints, respectively, she said.
PDS, synovial thickening, and effusion were "persistent," defined as present at baseline and follow-up, in 40, 118, and 232 joints, and were "fluctuating," or present only at baseline or follow-up, in 243, 641, and 636 joints, respectively.
Using generalized estimating equations analyses, progression was independently associated with ultrasound synovial thickening (odds ratio, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7) for grade 2-3 vs. grade 0, after adjustment for age, sex, body mass index, baseline osteophytes, and joint space narrowing scores, Dr. Kortekaas said.
Joint space narrowing was also independently associated with the ultrasound features of synovial thickening (OR, 3.4), effusion (OR, 3.3), and power Doppler signal (OR, 3.1), again after adjustment and comparing grade 2-3 vs. grade 0.
Persistent inflammation showed stronger associations with radiographic progression than did fluctuating inflammatory features in comparison with no inflammatory features at all, she said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, Dr. Kortekaas said inflammatory and synovial changes are loosely related to symptoms and pain, but that the group has yet to look at an association with C-reactive protein or inflammation in other joints.
Session comoderator Dr. Gillian Hawker, professor of medicine at the University of Toronto and physician in chief of medicine at Women’s College Hospital, Toronto, commented that until recently, ultrasound for hand OA has been far more common in clinical practice in Europe than in North America.
"I think that’s exactly where the radiology community is starting to go," she said in an interview. "Would we be doing a better job, picking things up earlier if we were ultrasounding? [There’s] definitely higher sensitivity. But, we haven’t quite gotten there yet. It’s going to cost money to get ultrasound machines into practices and train physicians."
Dr. Hawker observed that the American College of Radiology has added an ultrasound course and that residents at her institution are now going through ultrasound training as part of their residency.
Dr. Kortekaas and her coauthors reported no conflicting interests.
PARIS – Inflammatory ultrasound features in hand osteoarthritis may point clinicians toward patients at higher risk for radiographic progression, a longitudinal study suggests.
"We found inflammatory ultrasound features are independently associated with both progressive joint space narrowing and progression of osteophytes in hand osteoarthritis. This is especially true with persistent inflammation," Dr. Marion Kortekaas said at the World Congress on Osteoarthritis.
She presented data on 56 consecutive hand OA patients who underwent baseline and 2.3-year follow-up radiographic and ultrasound assessment of all first carpometacarpal, distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first interphalangeal joints.
Radiographs were scored for osteophytes and joint space narrowing using the OARSI Atlas grading system (0-3 scale). Ultrasound synovial thickening, effusion, and power Doppler signal (PDS) were scored on a validated 3-point scale, with 3 being severe. Progression was defined as at least one grade increase of either joint space narrowing or osteophytes, explained Dr. Kortekaas, a rheumatologist at Leiden (the Netherlands) University Medical Center.
Most patients were female (86%) and their average age was 61 years. Patients with rheumatic diseases, trauma/operation, and corticosteroid use were excluded.
Of 1,680 joints at baseline, 141 (8.4%) had synovial thickening, 332 (19.8%) effusion, and 146 (8.7%) PDS.
At follow-up, progression of osteophytes and joint space narrowing was present in 120 and 96 joints, respectively, she said.
PDS, synovial thickening, and effusion were "persistent," defined as present at baseline and follow-up, in 40, 118, and 232 joints, and were "fluctuating," or present only at baseline or follow-up, in 243, 641, and 636 joints, respectively.
Using generalized estimating equations analyses, progression was independently associated with ultrasound synovial thickening (odds ratio, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7) for grade 2-3 vs. grade 0, after adjustment for age, sex, body mass index, baseline osteophytes, and joint space narrowing scores, Dr. Kortekaas said.
Joint space narrowing was also independently associated with the ultrasound features of synovial thickening (OR, 3.4), effusion (OR, 3.3), and power Doppler signal (OR, 3.1), again after adjustment and comparing grade 2-3 vs. grade 0.
Persistent inflammation showed stronger associations with radiographic progression than did fluctuating inflammatory features in comparison with no inflammatory features at all, she said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, Dr. Kortekaas said inflammatory and synovial changes are loosely related to symptoms and pain, but that the group has yet to look at an association with C-reactive protein or inflammation in other joints.
Session comoderator Dr. Gillian Hawker, professor of medicine at the University of Toronto and physician in chief of medicine at Women’s College Hospital, Toronto, commented that until recently, ultrasound for hand OA has been far more common in clinical practice in Europe than in North America.
"I think that’s exactly where the radiology community is starting to go," she said in an interview. "Would we be doing a better job, picking things up earlier if we were ultrasounding? [There’s] definitely higher sensitivity. But, we haven’t quite gotten there yet. It’s going to cost money to get ultrasound machines into practices and train physicians."
Dr. Hawker observed that the American College of Radiology has added an ultrasound course and that residents at her institution are now going through ultrasound training as part of their residency.
Dr. Kortekaas and her coauthors reported no conflicting interests.
PARIS – Inflammatory ultrasound features in hand osteoarthritis may point clinicians toward patients at higher risk for radiographic progression, a longitudinal study suggests.
"We found inflammatory ultrasound features are independently associated with both progressive joint space narrowing and progression of osteophytes in hand osteoarthritis. This is especially true with persistent inflammation," Dr. Marion Kortekaas said at the World Congress on Osteoarthritis.
She presented data on 56 consecutive hand OA patients who underwent baseline and 2.3-year follow-up radiographic and ultrasound assessment of all first carpometacarpal, distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first interphalangeal joints.
Radiographs were scored for osteophytes and joint space narrowing using the OARSI Atlas grading system (0-3 scale). Ultrasound synovial thickening, effusion, and power Doppler signal (PDS) were scored on a validated 3-point scale, with 3 being severe. Progression was defined as at least one grade increase of either joint space narrowing or osteophytes, explained Dr. Kortekaas, a rheumatologist at Leiden (the Netherlands) University Medical Center.
Most patients were female (86%) and their average age was 61 years. Patients with rheumatic diseases, trauma/operation, and corticosteroid use were excluded.
Of 1,680 joints at baseline, 141 (8.4%) had synovial thickening, 332 (19.8%) effusion, and 146 (8.7%) PDS.
At follow-up, progression of osteophytes and joint space narrowing was present in 120 and 96 joints, respectively, she said.
PDS, synovial thickening, and effusion were "persistent," defined as present at baseline and follow-up, in 40, 118, and 232 joints, and were "fluctuating," or present only at baseline or follow-up, in 243, 641, and 636 joints, respectively.
Using generalized estimating equations analyses, progression was independently associated with ultrasound synovial thickening (odds ratio, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7) for grade 2-3 vs. grade 0, after adjustment for age, sex, body mass index, baseline osteophytes, and joint space narrowing scores, Dr. Kortekaas said.
Joint space narrowing was also independently associated with the ultrasound features of synovial thickening (OR, 3.4), effusion (OR, 3.3), and power Doppler signal (OR, 3.1), again after adjustment and comparing grade 2-3 vs. grade 0.
Persistent inflammation showed stronger associations with radiographic progression than did fluctuating inflammatory features in comparison with no inflammatory features at all, she said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, Dr. Kortekaas said inflammatory and synovial changes are loosely related to symptoms and pain, but that the group has yet to look at an association with C-reactive protein or inflammation in other joints.
Session comoderator Dr. Gillian Hawker, professor of medicine at the University of Toronto and physician in chief of medicine at Women’s College Hospital, Toronto, commented that until recently, ultrasound for hand OA has been far more common in clinical practice in Europe than in North America.
"I think that’s exactly where the radiology community is starting to go," she said in an interview. "Would we be doing a better job, picking things up earlier if we were ultrasounding? [There’s] definitely higher sensitivity. But, we haven’t quite gotten there yet. It’s going to cost money to get ultrasound machines into practices and train physicians."
Dr. Hawker observed that the American College of Radiology has added an ultrasound course and that residents at her institution are now going through ultrasound training as part of their residency.
Dr. Kortekaas and her coauthors reported no conflicting interests.
AT OARSI 2014
Key clinical point: Patients with inflammatory changes in hand OA on ultrasound during follow-up are at higher risk for radiographic progression.
Major finding: In adjusted analyses, hand OA progression was independently associated with ultrasound synovial thickening (OR, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7).
Data source: A longitudinal study in 56 consecutive hand OA patients.
Disclosures: Dr. Kortekaas and her coauthors reported no conflicting interests.

In obesity and knee OA, weight loss is a big win
PARIS – Weight loss of more than 5% produced clinically meaningful improvements in knee osteoarthritis, even when final body mass index remained high, a large, community-based study has shown.
For those patients who lost 10% body weight in the study, knee osteoarthritis symptoms improved by about 40%, consistent with the recent IDEA (Intensive Diet and Exercise for Arthritis) trial findings.
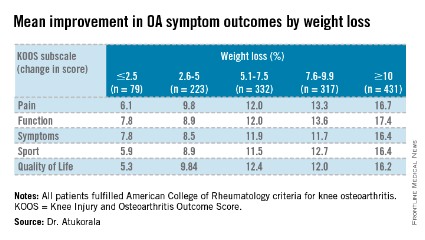
"There is a strong dose-response relationship between percentage weight loss and improvement in knee pain, function, symptoms, sport or recreation, and quality of life," Dr. Inoshi Atukorala said at the World Congress on Osteoarthritis.
Dr. Atukorala described the study as the first to examine the dose-response relationship between changes in body weight and knee osteoarthritis in a real-world, community setting.
The researchers evaluated 1,383 Australians who fulfilled the American College of Rheumatology criteria for knee osteoarthritis (OA) and were enrolled in the structured, remotely delivered "Healthy Weight for Life" knee and hip osteoarthritis management program. It integrates intensive weight loss as a component of tailored interventions, with the aim of achieving a 7%-10% body weight loss over 18 weeks, explained Dr. Atukorala, a consultant rheumatologist at the University of Colombo, Sri Lanka.
The program uses a partial very-low-calorie diet, portion management tools and devices, written healthy eating advice, and lifestyle education together with targeted telephone, e-mail, and text-message motivation and support. All participants were given the same strength, balance, and mobility exercise tools, instruction, and support.

At baseline, 81.7% of participants were obese, the average body mass index (BMI) was 34.3 kg/m2, and the mean Knee injury and Osteoarthritis Outcome Score (KOOS) pain and function subscale scores were 56.3 and 59.5. The cohort was 71% female and had an average age of 64 years.
At 18-weeks, there was a clear and significant incremental improvement in KOOS subscales across the weight-loss categories, with the greatest improvements in those losing at least 10% body weight, Dr. Atukorala said.
The weight-loss category cutoffs were chosen based on the IDEA trial (JAMA 2013;310:1263-73), as well as the weight-loss goal in the diet groups in the ADAPT study and the weight loss typically achieved in its exercise-only cohort of older adults with knee OA (Arthritis Rheum. 2004;50;1501-10), she explained.
Using repeated measures analysis of covariance, the investigators next examined the dose-response of weight loss, compared with differences in pain and function. For this analysis, the 2.5% or less weight-loss category was set as the reference.
The dose-relationship between weight loss and improvements in pain and function persisted, even after controlling for baseline age, gender, weight, height, and KOOS, Dr. Atukorala said at the meeting, sponsored by the Osteoarthritis Research Society International. The differences reached statistical significance on all KOOS subscales for the two highest weight-loss categories and on all but one subscale (KOOS sport) for those losing 5.1%-7.5% body weight.
"We are limited by the fact that the program did not assess the magnitude of exercise interventions in each weight-loss category, but it confirms the dose-response benefit of weight loss as a therapeutic intervention in knee osteoarthritis," Dr. Atukorala concluded. "And, it demonstrates the effectiveness of disseminating and implementing intensive weight-loss intervention in a community-based setting."
Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
PARIS – Weight loss of more than 5% produced clinically meaningful improvements in knee osteoarthritis, even when final body mass index remained high, a large, community-based study has shown.
For those patients who lost 10% body weight in the study, knee osteoarthritis symptoms improved by about 40%, consistent with the recent IDEA (Intensive Diet and Exercise for Arthritis) trial findings.
"There is a strong dose-response relationship between percentage weight loss and improvement in knee pain, function, symptoms, sport or recreation, and quality of life," Dr. Inoshi Atukorala said at the World Congress on Osteoarthritis.
Dr. Atukorala described the study as the first to examine the dose-response relationship between changes in body weight and knee osteoarthritis in a real-world, community setting.
The researchers evaluated 1,383 Australians who fulfilled the American College of Rheumatology criteria for knee osteoarthritis (OA) and were enrolled in the structured, remotely delivered "Healthy Weight for Life" knee and hip osteoarthritis management program. It integrates intensive weight loss as a component of tailored interventions, with the aim of achieving a 7%-10% body weight loss over 18 weeks, explained Dr. Atukorala, a consultant rheumatologist at the University of Colombo, Sri Lanka.
The program uses a partial very-low-calorie diet, portion management tools and devices, written healthy eating advice, and lifestyle education together with targeted telephone, e-mail, and text-message motivation and support. All participants were given the same strength, balance, and mobility exercise tools, instruction, and support.
At baseline, 81.7% of participants were obese, the average body mass index (BMI) was 34.3 kg/m2, and the mean Knee injury and Osteoarthritis Outcome Score (KOOS) pain and function subscale scores were 56.3 and 59.5. The cohort was 71% female and had an average age of 64 years.
At 18-weeks, there was a clear and significant incremental improvement in KOOS subscales across the weight-loss categories, with the greatest improvements in those losing at least 10% body weight, Dr. Atukorala said.
The weight-loss category cutoffs were chosen based on the IDEA trial (JAMA 2013;310:1263-73), as well as the weight-loss goal in the diet groups in the ADAPT study and the weight loss typically achieved in its exercise-only cohort of older adults with knee OA (Arthritis Rheum. 2004;50;1501-10), she explained.
Using repeated measures analysis of covariance, the investigators next examined the dose-response of weight loss, compared with differences in pain and function. For this analysis, the 2.5% or less weight-loss category was set as the reference.
The dose-relationship between weight loss and improvements in pain and function persisted, even after controlling for baseline age, gender, weight, height, and KOOS, Dr. Atukorala said at the meeting, sponsored by the Osteoarthritis Research Society International. The differences reached statistical significance on all KOOS subscales for the two highest weight-loss categories and on all but one subscale (KOOS sport) for those losing 5.1%-7.5% body weight.
"We are limited by the fact that the program did not assess the magnitude of exercise interventions in each weight-loss category, but it confirms the dose-response benefit of weight loss as a therapeutic intervention in knee osteoarthritis," Dr. Atukorala concluded. "And, it demonstrates the effectiveness of disseminating and implementing intensive weight-loss intervention in a community-based setting."
Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
PARIS – Weight loss of more than 5% produced clinically meaningful improvements in knee osteoarthritis, even when final body mass index remained high, a large, community-based study has shown.
For those patients who lost 10% body weight in the study, knee osteoarthritis symptoms improved by about 40%, consistent with the recent IDEA (Intensive Diet and Exercise for Arthritis) trial findings.
"There is a strong dose-response relationship between percentage weight loss and improvement in knee pain, function, symptoms, sport or recreation, and quality of life," Dr. Inoshi Atukorala said at the World Congress on Osteoarthritis.
Dr. Atukorala described the study as the first to examine the dose-response relationship between changes in body weight and knee osteoarthritis in a real-world, community setting.
The researchers evaluated 1,383 Australians who fulfilled the American College of Rheumatology criteria for knee osteoarthritis (OA) and were enrolled in the structured, remotely delivered "Healthy Weight for Life" knee and hip osteoarthritis management program. It integrates intensive weight loss as a component of tailored interventions, with the aim of achieving a 7%-10% body weight loss over 18 weeks, explained Dr. Atukorala, a consultant rheumatologist at the University of Colombo, Sri Lanka.
The program uses a partial very-low-calorie diet, portion management tools and devices, written healthy eating advice, and lifestyle education together with targeted telephone, e-mail, and text-message motivation and support. All participants were given the same strength, balance, and mobility exercise tools, instruction, and support.
At baseline, 81.7% of participants were obese, the average body mass index (BMI) was 34.3 kg/m2, and the mean Knee injury and Osteoarthritis Outcome Score (KOOS) pain and function subscale scores were 56.3 and 59.5. The cohort was 71% female and had an average age of 64 years.
At 18-weeks, there was a clear and significant incremental improvement in KOOS subscales across the weight-loss categories, with the greatest improvements in those losing at least 10% body weight, Dr. Atukorala said.
The weight-loss category cutoffs were chosen based on the IDEA trial (JAMA 2013;310:1263-73), as well as the weight-loss goal in the diet groups in the ADAPT study and the weight loss typically achieved in its exercise-only cohort of older adults with knee OA (Arthritis Rheum. 2004;50;1501-10), she explained.
Using repeated measures analysis of covariance, the investigators next examined the dose-response of weight loss, compared with differences in pain and function. For this analysis, the 2.5% or less weight-loss category was set as the reference.
The dose-relationship between weight loss and improvements in pain and function persisted, even after controlling for baseline age, gender, weight, height, and KOOS, Dr. Atukorala said at the meeting, sponsored by the Osteoarthritis Research Society International. The differences reached statistical significance on all KOOS subscales for the two highest weight-loss categories and on all but one subscale (KOOS sport) for those losing 5.1%-7.5% body weight.
"We are limited by the fact that the program did not assess the magnitude of exercise interventions in each weight-loss category, but it confirms the dose-response benefit of weight loss as a therapeutic intervention in knee osteoarthritis," Dr. Atukorala concluded. "And, it demonstrates the effectiveness of disseminating and implementing intensive weight-loss intervention in a community-based setting."
Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
AT OARSI 2014
Major finding: Participants who lost at least 10% body weight (mean 12.5%) had mean improvements on the KOOS pain, function, symptoms, sport, and quality of life subscales of 16.7, 17.4, 16.4, 16.4, and 16.2 points (P =.000).
Data source: Analysis of 1,383 consecutive knee OA participants in a knee and hip OA management program.
Disclosures: Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
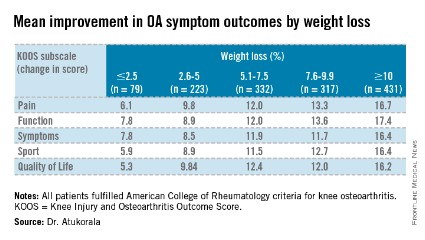
Poor vibratory sense contributes to OA knee instability
PARIS – Impaired vibratory sense and muscle strength may be important risk factors for knee instability in persons with or at risk for symptomatic knee osteoarthritis, according to an analysis of a large, longitudinal cohort.
"Buckling is commonly been thought of as a mechanical phenomenon, but no one really knows the risk factors," Dr. Najia Shakoor said in an interview at the World Congress on Osteoarthritis. "For many, sensory input may be important. If you have greater sensory input, in this case, greater vibratory sense, perhaps you can protect yourself from buckling."
Knee instability is common in persons with knee osteoarthritis (OA) and has been found in studies to be associated with muscle weakness. None have examined whether weakness predicts onset or worsening of knee instability, she said.

It is also unknown whether decreased vibratory sense, often seen in older adults with knee OA, may distort one’s sense of knee position and increase the risk of instability.
For the current analysis, unilateral knee extensor strength and bilateral vibratory perception thresholds (VPT) were evaluated in 2,212 participants with or at risk for knee OA in the Multicenter Osteoarthritis Study (MOST). VPT was measured using a biothesiometer, with the tip placed on the tibial tuberosity and the voltage increased by 1 volt/sec from 0 until the participant acknowledged sensation.
The mean age of study participants was 68 years, mean body mass index (BMI) was 31 kg/m2, and 60% were women.
At the 60-month visit, 17% of participants reported knee buckling in the past 3 months, 29% reported slipping or "shifting, slipping, or going to give way, but didn’t actually do so," and 37% reported instability (buckling and/or slipping), said Dr. Shakoor, a rheumatologist with Rush University Medical Center, Chicago.
During follow-up, 32% of patients developed incident instability, 20% incident buckling, 11% worsening instability, and 21% worsening buckling.
In Poisson regression person-based analyses, the risk of incident knee instability was significantly less in those with greater quadriceps strength (relative risk, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024), after adjustment for age, sex, BMI, race, clinic site, Kellgren-Lawrence OA grade, Western Ontario and McMaster Osteoarthritis Index knee pain, and both predictors.
Better vibratory sense also protected against worsening of both knee instability (RR, 0.42; P = .021) and buckling (RR, 0.67; P = .020), Dr. Shakoor reported in the poster presentation at the meeting, sponsored by the Osteoarthritis Research Society International.
Although it’s not known whether vibratory sense can be improved, muscle strength can be. "So these are potentially modifiable risk factors for a common problem," she said.
Prior work by the group has found that vibratory sense is impaired in hip as well as knee OA, compared with healthy controls.
The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
PARIS – Impaired vibratory sense and muscle strength may be important risk factors for knee instability in persons with or at risk for symptomatic knee osteoarthritis, according to an analysis of a large, longitudinal cohort.
"Buckling is commonly been thought of as a mechanical phenomenon, but no one really knows the risk factors," Dr. Najia Shakoor said in an interview at the World Congress on Osteoarthritis. "For many, sensory input may be important. If you have greater sensory input, in this case, greater vibratory sense, perhaps you can protect yourself from buckling."
Knee instability is common in persons with knee osteoarthritis (OA) and has been found in studies to be associated with muscle weakness. None have examined whether weakness predicts onset or worsening of knee instability, she said.
It is also unknown whether decreased vibratory sense, often seen in older adults with knee OA, may distort one’s sense of knee position and increase the risk of instability.
For the current analysis, unilateral knee extensor strength and bilateral vibratory perception thresholds (VPT) were evaluated in 2,212 participants with or at risk for knee OA in the Multicenter Osteoarthritis Study (MOST). VPT was measured using a biothesiometer, with the tip placed on the tibial tuberosity and the voltage increased by 1 volt/sec from 0 until the participant acknowledged sensation.
The mean age of study participants was 68 years, mean body mass index (BMI) was 31 kg/m2, and 60% were women.
At the 60-month visit, 17% of participants reported knee buckling in the past 3 months, 29% reported slipping or "shifting, slipping, or going to give way, but didn’t actually do so," and 37% reported instability (buckling and/or slipping), said Dr. Shakoor, a rheumatologist with Rush University Medical Center, Chicago.
During follow-up, 32% of patients developed incident instability, 20% incident buckling, 11% worsening instability, and 21% worsening buckling.
In Poisson regression person-based analyses, the risk of incident knee instability was significantly less in those with greater quadriceps strength (relative risk, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024), after adjustment for age, sex, BMI, race, clinic site, Kellgren-Lawrence OA grade, Western Ontario and McMaster Osteoarthritis Index knee pain, and both predictors.
Better vibratory sense also protected against worsening of both knee instability (RR, 0.42; P = .021) and buckling (RR, 0.67; P = .020), Dr. Shakoor reported in the poster presentation at the meeting, sponsored by the Osteoarthritis Research Society International.
Although it’s not known whether vibratory sense can be improved, muscle strength can be. "So these are potentially modifiable risk factors for a common problem," she said.
Prior work by the group has found that vibratory sense is impaired in hip as well as knee OA, compared with healthy controls.
The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
PARIS – Impaired vibratory sense and muscle strength may be important risk factors for knee instability in persons with or at risk for symptomatic knee osteoarthritis, according to an analysis of a large, longitudinal cohort.
"Buckling is commonly been thought of as a mechanical phenomenon, but no one really knows the risk factors," Dr. Najia Shakoor said in an interview at the World Congress on Osteoarthritis. "For many, sensory input may be important. If you have greater sensory input, in this case, greater vibratory sense, perhaps you can protect yourself from buckling."
Knee instability is common in persons with knee osteoarthritis (OA) and has been found in studies to be associated with muscle weakness. None have examined whether weakness predicts onset or worsening of knee instability, she said.
It is also unknown whether decreased vibratory sense, often seen in older adults with knee OA, may distort one’s sense of knee position and increase the risk of instability.
For the current analysis, unilateral knee extensor strength and bilateral vibratory perception thresholds (VPT) were evaluated in 2,212 participants with or at risk for knee OA in the Multicenter Osteoarthritis Study (MOST). VPT was measured using a biothesiometer, with the tip placed on the tibial tuberosity and the voltage increased by 1 volt/sec from 0 until the participant acknowledged sensation.
The mean age of study participants was 68 years, mean body mass index (BMI) was 31 kg/m2, and 60% were women.
At the 60-month visit, 17% of participants reported knee buckling in the past 3 months, 29% reported slipping or "shifting, slipping, or going to give way, but didn’t actually do so," and 37% reported instability (buckling and/or slipping), said Dr. Shakoor, a rheumatologist with Rush University Medical Center, Chicago.
During follow-up, 32% of patients developed incident instability, 20% incident buckling, 11% worsening instability, and 21% worsening buckling.
In Poisson regression person-based analyses, the risk of incident knee instability was significantly less in those with greater quadriceps strength (relative risk, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024), after adjustment for age, sex, BMI, race, clinic site, Kellgren-Lawrence OA grade, Western Ontario and McMaster Osteoarthritis Index knee pain, and both predictors.
Better vibratory sense also protected against worsening of both knee instability (RR, 0.42; P = .021) and buckling (RR, 0.67; P = .020), Dr. Shakoor reported in the poster presentation at the meeting, sponsored by the Osteoarthritis Research Society International.
Although it’s not known whether vibratory sense can be improved, muscle strength can be. "So these are potentially modifiable risk factors for a common problem," she said.
Prior work by the group has found that vibratory sense is impaired in hip as well as knee OA, compared with healthy controls.
The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
AT OARSI 2014
Key clinical point: Working to increase quadriceps strength may reduce knee instability in OA patients.
Major finding: The risk of incident knee instability was significantly less in those with greater quadriceps strength (RR, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024).
Data source: A longitudinal analysis of 2,212 patients with knee OA.
Disclosures: The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
