User login
Parsimonious blood use and lower transfusion triggers: What is the evidence?
For decades, physicians believed in the benefit of prompt transfusion of blood to keep the hemoglobin level at arbitrary, optimum levels, ie, close to normal values, especially in the critically ill, the elderly, and those with coronary syndromes, stroke, or renal failure.
However, the evidence supporting arbitrary hemoglobin values as an indication for transfusion was weak or nonexistent. Also, blood transfusion can have complications and adverse effects, and blood is costly and scarce. These considerations prompted research into when blood transfusion should be considered, and recommendations that it should be used more sparingly than in the past.
This review offers a perspective on the evidence supporting restrictive blood use. First, we focus on hemodilution studies that demonstrated that humans can tolerate anemia. Then, we look at studies that compared a restrictive transfusion strategy with a liberal one in patients with critical illness and active bleeding. We conclude with current recommendations for blood transfusion.
EVIDENCE FROM HEMODILUTION STUDIES
Hemoglobin is essential for tissue oxygenation, but the serum hemoglobin concentration is just one of several factors involved.1–5 In anemia, the body can adapt not only by increasing production of red blood cells, but also by:
- Increasing cardiac output
- Increasing synthesis of 2,3-diphosphoglycerate (2,3-DPG), with a consequent shift in the oxyhemoglobin dissociation curve to the right, allowing enhanced release of oxygen at the tissue level
- Moving more carbon dioxide into the blood (the Bohr effect), which decreases pH and also shifts the dissociation curve to the right.
Just 20 years ago, physicians were using arbitrary cutoffs such as hemoglobin 10 g/dL or hematocrit 30% as indications for blood transfusion, without reasonable evidence to support these values. Not until acute normovolemic hemodilution studies were performed were we able to progressively appraise how well patients could tolerate lower levels of hemoglobin without significant adverse outcomes.
Acute normovolemic hemodilution involves withdrawing blood and replacing it with crystalloid or colloid solution to maintain the volume.6
Initial studies were done in animals and focused on the safety of acute anemia regarding splanchnic perfusion. Subsequently, studies proved that healthy, elderly, and stable cardiac patients can tolerate acute anemia with normal cardiovascular response. The targets in these studies were modest at first, but researchers aimed progressively for more aggressive hemodilution with lower hemoglobin targets and demonstrated that the body can tolerate and adapt to more severe anemia.6–8
Studies in healthy patients
Weiskopf et al9 assessed the effect of severe anemia in 32 conscious healthy patients (11 presurgical patients and 21 volunteers not undergoing surgery) by performing acute normovolemic hemodilution with 5% human albumin, autologous plasma, or both, with a target hemoglobin level of 5 g/dL. The process was done gradually, obtaining aliquots of blood of 500 to 900 mL. Cardiac index increased, along with a mild increase in oxygen consumption with no increase in plasma lactate levels, suggesting that in conscious healthy patients, tissue oxygenation remains adequate even in severe anemia.
Leung et al10 addressed the electrocardiographic changes that occur with severe anemia (hemoglobin 5 g/dL) in 55 healthy volunteers. Three developed transient, reversible ST-segment depression, which was associated with a higher heart rate than in the volunteers with no electrocardiographic changes; however, the changes were reversible and asymptomatic, and thus were considered physiologic and benign.
Hemodilution in healthy elderly patients
Spahn et al11 performed 6 and 12 mL/kg isovolemic exchange of blood for 6% hydroxyethyl starch in 20 patients older than 65 years (mean age 76, range 65–88) without underlying coronary disease.
The patients’ mean hemoglobin level decreased from 11.6 g/dL to 8.8 g/dL. Their cardiac index and oxygen extraction values increased adequately, with stable oxygen consumption during hemodilution. There were no electrocardiographic signs of ischemia.
Hemodilution in coronary artery disease
Spahn et al12 performed hemodilution studies in 60 patients (ages 35–81) with coronary artery disease managed chronically with beta-blockers who were scheduled for coronary artery bypass graft surgery. Hemodilution was performed with 6- and 12-mL/kg isovolemic exchange of blood for 6% hydroxyethyl starch maintaining normovolemia and stable filling pressures. Hemoglobin levels decreased from 12.6 g/dL to 9.9 g/dL. The hemodilution process was done before the revascularization. The authors monitored hemodynamic variables, ST-segment deviation, and oxygen consumption before and after each hemodilution.
There was a compensatory increase in cardiac index and oxygen extraction with consequent stable oxygen consumption. These changes were independent of patient age or left ventricular function. In addition, there were no electrocardiographic signs of ischemia.
Licker et al13 studied the hemodynamic effect of preoperative hemodilution in 50 patients with coronary artery disease undergoing coronary artery bypass graft surgery, performing transesophageal echocardiography before and after hemodilution. The patients underwent isovolemic exchange with iso-oncotic starch to target a hematocrit of 28%.
Acute normovolemic hemodilution triggered an increase in cardiac stroke volume, which had a direct correlation with an increase in the central venous pressure and the left ventricular end-diastolic area. No signs of ischemia were seen in these patients on electrocardiography or echocardiography (eg, left ventricular wall-motion abnormalities).
Hemodilution in mitral regurgitation
Spahn et al14 performed acute isovolemic hemodilution with 6% hydroxyethyl starch in 20 patients with mitral regurgitation. The cardiac filling pressures were stable before and after hemodilution; the mean hemoglobin value decreased from 13 to 10.3 g/dL. The cardiac index and oxygen extraction increased proportionally, with stable oxygen consumption; these findings were the same regardless of whether the patient was in normal sinus rhythm or atrial fibrillation.
Effect of hemodilution on cognition
Weiskopf et al15 assessed the effect of anemia on executive and memory function by inducing progressive acute isovolemic anemia in 90 healthy volunteers (age 29 ± 5), reducing their hemoglobin values to 7, 6, and 5 g/dL and performing repetitive neuropsychological and memory testing before and after the hemodilution, as well as after autologous blood transfusion to return their hemoglobin level to 7 g/dL.
There were no changes in reaction time or error rate at a hemoglobin concentration of 7 g/dL compared with the performance at a baseline hemoglobin concentration of 14 g/dL. The volunteers got slower on a mathematics test at hemoglobin levels of 6 g/dL and 5 g/dL, but their error rate did not increase. Immediate and delayed memory were significantly impaired at hemoglobin of 5 g/dL but not at 6 g/dL. All tests normalized with blood transfusion once the hemoglobin level reached 7 g/dL.15
Weiskopf et al16 subsequently investigated whether giving supplemental oxygen to raise the arterial partial pressure of oxygen (Pao2) to 350 mm Hg or greater would overcome the neurocognitive effects of severe acute anemia. They followed a protocol similar to the one in the earlier study15 and induced anemia in 31 healthy volunteers, age 28 ± 4 years, with a mean baseline hemoglobin concentration of 12.7 g/dL.
When the volunteers reached a hemoglobin concentration of 5.7 ± 0.3 g/dL, they were significantly slower on the mathematics test, and their delayed memory was significantly impaired. Then, in a double-blind fashion, they were given either room air or oxygen. Oxygen increased the Pao2 to 406 mm Hg and normalized neurocognitive performance.
Hemodilution studies in surgical patients
A 2015 meta-analysis17 of 63 studies involving 3,819 surgical patients compared the risk of perioperative allogeneic blood transfusion as well as the overall volume of transfused blood in patients undergoing preoperative acute normovolemic hemodilution vs a control group. Though the overall data showed that the patients who underwent acute normovolemic hemodilution needed fewer transfusions and less blood (relative risk [RR] 0.74, 95% confidence interval [CI] 0.63–0.88, P = .0006), the authors noted significant heterogeneity and publication bias.
However, the hemodilution studies paved the way for justifying a more conservative and restrictive transfusion strategy, with a hemoglobin cutoff value of 7 g/dL, and in acute anemia, using oxygen to overcome acute neurocognitive effects while searching for and correcting the cause of the anemia.
STUDIES OF RESTRICTIVE VS LIBERAL TRANSFUSION STRATEGIES
Studies in critical care and high-risk patients
Hébert et al18 randomized 418 critical care patients to a restrictive transfusion approach (in which they were given red blood cells if their hemoglobin concentration dropped below 7.0 g/dL) and 420 patients to a liberal strategy (given red blood cells if their hemoglobin concentration dropped below 10.0 g/dL). Mortality rates (restrictive vs liberal strategy) were as follows:
- Overall at 30 days 18.7% vs 23.3%, P = .11
- In the subgroup with less-severe disease (Acute Physiology and Chronic Health Evaluation II [APACHE II] score < 20), 8.7% vs 16.1%, P = .03
- In the subgroup under age 55, 5.7% vs 13%, P = .02
- In the subgroup with clinically significant cardiac disease, 20.5% vs 22.9%, P = .69
- In the hospital, 22.2% vs 28.1%; P = .05.
This study demonstrated that parsimonious blood use did not worsen clinical outcomes in critical care patients.
Carson et al19 evaluated 2,016 patients age 50 and older who had a history of or risk factors for cardiovascular disease and a baseline hemoglobin level below 10 g/dL who underwent surgery for hip fracture. Patients were randomized to two transfusion strategies based on threshold hemoglobin level: restrictive (< 8 g/dL) or liberal (< 10 g/dL). The primary outcome was death or inability to walk without assistance at 60-day follow-up. The median number of units of blood used was 2 in the liberal group and 0 in the restrictive group.
There was no significant difference in the rates of the primary outcome (odds ratio [OR] 1.01, 95% CI 0.84–1.22), infection, venous thromboembolism, or reoperation. This study demonstrated that a liberal transfusion strategy offered no benefit over a restrictive one.
Rao et al20 analyzed the impact of blood transfusion in 24,112 patients with acute coronary syndromes enrolled in three large trials. Ten percent of the patients received at least 1 blood transfusion during their hospitalization, and they were older and had more complex comorbidity.
At 30 days, the group that had received blood had higher rates of death (adjusted hazard ratio [HR] 3.94, 95% CI 3.26–4.75) and the combined outcome of death or myocardial infarction (HR 2.92, 95% CI 2.55–3.35). Transfusion in patients whose nadir hematocrit was higher than 25% was associated with worse outcomes.
This study suggests being cautious about routinely transfusing blood in stable patients with ischemic heart disease solely on the basis of arbitrary hematocrit levels.
Carson et al,21 however, in a later trial, found a trend toward worse outcomes with a restrictive strategy than with a liberal one. Here, 110 patients with acute coronary syndrome or stable angina undergoing cardiac catheterization were randomized to a target hemoglobin level of either at least 8 mg/dL or at least 10 g/dL. The primary outcome (a composite of death, myocardial infarction, or unscheduled revascularization 30 days after randomization) occurred in 14 patients (25.5%) in the restrictive group and 6 patients (10.9%) in the liberal group (P = .054), and 7 (13.0%) vs 1 (1.8%) of the patients died (P = .032).
Murphy et al22 similarly found trends toward worse outcomes with a restrictive strategy in cardiac patients. The investigators randomized 2,007 elective cardiac surgery patients with a postoperative hemoglobin level lower than 9 g/dL to a hemoglobin transfusion threshold of either 7.5 or 9 g/dL. Outcomes (restrictive vs liberal strategies):
- Transfusion rates 53.4% vs 92.2%
- Rates of the primary outcome (a serious infection [sepsis or wound infection] or ischemic event [stroke, myocardial infarction, mesenteric ischemia, or acute kidney injury] within 3 months):
35.1% vs 33.0%, OR 1.11, 95% CI 0.91–1.34, P = .30) - Mortality rates 4.2% vs 2.6%, HR 1.64, 95% CI 1.00–2.67, P = .045
- Total costs did not differ significantly between the groups.
These studies21,22 suggest the need for more definitive trials in patients with active coronary disease and in cardiac surgery patients.
Holst et al23 randomized 998 intensive care patients in septic shock to hemoglobin thresholds for transfusion of 7 vs 9 g/dL. Mortality rates at 90 days (the primary outcome) were 43.0% vs 45.0%, RR 0.94, 95% CI 0.78–1.09, P = .44.
This study suggests that even in septic shock, a liberal transfusion strategy has no advantage over a parsimonious one.
Active bleeding, especially active gastrointestinal bleeding, poses a significant stress that may trigger empirical transfusion even without evidence of the real hemoglobin level.
Villanueva et al24 randomized 921 patients with severe acute upper-gastrointestinal bleeding to two groups, with hemoglobin transfusion triggers of 7 vs 9 g/dL. The findings were impressive:
- Freedom from transfusion 51% vs 14% (P < .001)
- Survival rates at 6 weeks 95% vs 91% (HR 0.55, 95% CI 0.33–0.92, P = .02)
- Rebleeding 10% vs 16% (P = .01).
Patients with peptic ulcer disease as well as those with cirrhosis stage Child-Pugh class A or B had higher survival rates with a restrictive transfusion strategy.
The RELIEVE trial25 compared the effect of a restrictive transfusion strategy in elderly patients on mechanical ventilation in 6 intensive care units in the United Kingdom. Transfusion triggers were hemoglobin 7 vs 9 g/dL, and the mortality rate at 180 days was 55% vs 37%, RR 0.68, 95% CI 0.44–1.05, P = .073.
Meta-analyses and observational studies
Rohde et al26 performed a systematic review and meta-analysis of 17 trials with 7,456 patients, which revealed that a restrictive strategy is associated with a lower risk of nosocomial infection, including pneumonia, wound infection, and sepsis.
The pooled risk of all serious infections was 10.6% in the restrictive group and 12.7% in the liberal group. Even after adjusting for the use of leukocyte reduction, the risk of infection was lower in the restrictive strategy group (RR 0.83, 95% CI 0.69–0.99). With a hemoglobin threshold of less than 7.0 g/dL, the risk of serious infection was 14% lower. Although this was not statistically significant overall (RR 0.86, 95% CI 0.72–1.02), the difference was statistically significant in the subgroup undergoing orthopedic surgery (RR 0.72, 95% CI 0.53–0.97) and the subgroup presenting with sepsis (RR 0.51, 95% CI 0.28–0.95).
Salpeter et al27 performed a meta-analysis and systematic review of three randomized trials (N = 2,364) comparing a restrictive hemoglobin transfusion trigger (hemoglobin < 7 g/dL) vs a more liberal trigger. The groups with restrictive transfusion triggers had lower rates of:
- In-hospital mortality (RR 0.74, 95% CI 0.60–0.92)
- Total mortality (RR 0.80, 95% CI 0.65–0.98)
- Rebleeding (RR 0.64, 95% CI 0.45–0.90)
- Acute coronary syndrome (RR 0.44, 95% CI 0.22–0.89)
- Pulmonary edema (RR 0.48, 95% CI 0.33–0.72)
- Bacterial infections (RR 0.86, 95% CI 0.73–1.00).
Wang et al28 performed a meta-analysis of 4 randomized controlled trials in patients with upper-gastrointestinal bleeding comparing restrictive (hemoglobin < 7 g/dL) vs liberal transfusion strategies. The primary outcomes were death and rebleeding. The restrictive strategy was associated with:
- A lower mortality rate (OR 0.52, 95% CI 0.31–0.87, P = .01)
- A lower rebleeding rate (OR 0.26, 95% CI 0.03–2.10, P = .21)
- Shorter hospitalizations (P = .009)
- Less blood transfused (P = .0005).
Vincent et al,29 in a prospective observational study of 3,534 patients in intensive care units in 146 facilities in Western Europe, found a correlation between transfusion and mortality. Transfusion was done most often in elderly patients and those with a longer stay in the intensive care unit. The 28-day mortality rate was 22.7% in patients who received a transfusion and 17.1% in those who did not (P = .02). The more units of blood the patients received, the more likely they were to die, and receiving more than 4 units was associated with worse outcomes (P = .01).
Dunne et al30 performed a study of 6,301 noncardiac surgical patients in the Veterans Affairs Maryland Healthcare System from the National Veterans Administration Surgical Quality Improvement Program from 1995 to 2000. Multiple logistic regression analysis revealed that the composite of low hematocrit before and after surgery and high transfusion rates (> 4 units per hospitalization) were associated with higher rates of death (P < .01) and postoperative pneumonia (P ≤ .05) and longer hospitalizations (P < .05). The risk of pneumonia increased proportionally with the decrease in hematocrit.
These findings support pharmacologic optimization of anemia with hematinic supplementation before surgery to decrease the risk of needing a transfusion, often with parenteral iron. The fact that the patient’s hemoglobin can be optimized preoperatively by nontransfusional means may decrease the likelihood of blood transfusion, as the hemoglobin will potentially remain above the transfusion threshold. For example, if a patient has a preoperative hemoglobin level of 10 g/dL, and it is optimized up to 12, then if postoperatively the hemoglobin level drops 3 g/dL instead of reaching the threshold of 7 g/dL, the nadir will be just 9 g/dL, far above that transfusion threshold.
Brunskill et al,31 in a Cochrane review of 6 trials with 2,722 patients undergoing surgery for hip fracture, found no difference in rates of mortality, functional recovery or postoperative morbidity with a restrictive transfusion strategy (hemoglobin target > 8 g/dL vs a liberal one (> 10 g/dL). However, the quality of evidence was rated as low. The authors concluded that there is no justification for liberal red blood cell transfusion thresholds (10 g/dL), and a more restrictive transfusion threshold is preferable.
Weinberg et al32 found that, in trauma patients, receiving more than 6 units of blood was associated with poor prognosis, and outcomes were worse when the blood was older than 2 weeks. However, the effect of blood age is not significant when using smaller transfusion volumes (1 to 2 units of red blood cells).
Studies in sickle cell disease
Sickle cell disease patients have high levels of hemoglobin S, which causes erythrocyte sickling and increases blood viscosity. Transfusion with normal erythrocytes increases the amount of hemoglobin A (the normal variant).33,34
In trials in surgical patients,35,36 conservative strategies for preoperative blood transfusion aiming at a hemoglobin level of 10 g/dL were as effective in preventing postoperative complications as decreasing the hemoglobin S levels to 30% by aggressive exchange transfusion.35
In nonsurgical patients, blood transfusion should be based on formal risk-benefit assessments. Therefore, the expert panel report on sickle cell management advises against blood transfusion in sickle cell patients with uncomplicated vaso-occlusive crises, priapism, asymptomatic anemia, or acute kidney injury in the absence of multisystem organ failure.34
Is hemoglobin the most relevant marker?
Most studies that compared restrictive and liberal transfusion strategies focused on using a lower hemoglobin threshold as the transfusion trigger, not on using fewer units of blood. Is the amount of blood transfused more important than the hemoglobin threshold? Perhaps a study focused both on a restrictive vs liberal strategy and also on the minimum amount of blood that each patient may benefit from would help to answer this question.
We should beware of routinely using the hemoglobin concentration as a threshold for transfusion and a surrogate marker of transfusion benefit because changes in hemoglobin concentration may not reflect changes in absolute red cell mass.37 Changes in plasma volume (an increase or decrease) affect the hematocrit concentration without necessarily affecting the total red cell mass. Unfortunately, red cell mass is very difficult to measure; hence, the hemoglobin and hematocrit values are used instead. Studies addressing changes in red cell mass may be needed, perhaps even to validate using the hemoglobin concentration as the sole indicator for transfusion.
Is fresh blood better than old blood?
Using blood that is more than 14 days old may be associated with poor outcomes, for several possible reasons. Red blood cells age rapidly in refrigeration, and usually just 75% may remain viable 24 hours after phlebotomy. Adenosine triphosphate and 2,3-DPG levels steadily decrease, with a consequent decrease in capacity for appropriate tissue oxygen delivery. In addition, loss of membrane phospholipids causes progressive rigidity of the red cell membrane with consequent formation of echynocytes after 14 to 21 days.38,39
The use of blood more than 14 days old in cardiac surgery patients has been associated with worse outcomes, including higher rates of death, prolonged intubation, acute renal failure, and sepsis.40 Similar poor outcomes have been seen in trauma patients.32
Lacroix et al,41 in a multicenter, randomized trial in critically ill adults, compared the outcomes of transfusion of fresh packed red cells (stored < 8 days) or old blood (stored for a mean of 22 days). The primary outcome was the mortality rate at 90 days: 37.0% in the fresh-blood group vs 35.3% in the old-blood group (HR 1.1, 95% CI 0.9–1.2, P = .38).
The authors concluded that using fresh blood compared with old blood was not associated with a lower 90-day mortality rate in critically ill adults.
RISKS ASSOCIATED WITH TRANSFUSION
Infections
The risk of infection from blood transfusion is small. Human immunodeficiency virus (HIV) is transmitted in 1 in 1.5 million transfused blood components, and hepatitis C virus in 1 in 1.1 million; these odds are similar to those of having a fatal airplane accident (1 in 1.7 million per flight). Hepatitis B virus infection is more common, the reported incidence being 1 in 357,000.42
Noninfectious complications
Transfusion-associated circulatory overload occurs in 4% to 6% of patients who receive a transfusion. Therefore, circulatory overload is a greater danger from transfusion than infection is.42
Febrile nonhemolytic transfusion reactions occur in 1.1% of patients with prestorage leukoreduction.
Transfusion-associated acute lung injury occurs in 0.8 per 10,000 blood components transfused.
Errors associated with blood transfusion include, in decreasing order of frequency, transfusion of the wrong blood component, handling and storage errors, inappropriate administration of anti-D immunoglobulin, and avoidable, delayed, or insufficient transfusions.43
Surgery and condition-specific complications of red blood cell transfusion
Cardiovascular surgery. Transfusion is associated with a higher risk of postoperative stroke, respiratory failure, acute respiratory distress syndrome, prolonged intubation time, reintubation, in-hospital death, sepsis, and longer postoperative length of stay.44
Malignancy. The use of blood in this setting has been found to be an independent predictor of recurrence, decreased survival, and increased risk of lymphoplasmacytic and marginal-zone lymphomas.44–47
Vascular, orthopedic, and other surgeries. Transfusion is associated with a higher risk of death, thromboembolic events, acute kidney injury, death, composite morbidity, reoperation, sepsis, and pulmonary complications.44
ST-segment elevation myocardial infarction, sepsis, and intensive care unit admissions. Transfusion is associated with an increased risk of rebleeding, death, and secondary infections.44
COST OF RED BLOOD CELL TRANSFUSION
Up to 85 million units of red blood cells are transfused per year worldwide, 15 million of them in the United States.42 At our hospital in 2013, 1 unit of leukocyte-reduced red blood cells cost $957.27, which included the costs of acquisition, processing, banking, patient testing, administration, and monitoring.
The Premier Healthcare Alliance48 analyzed data from 7.4 million discharges from 464 hospitals between April 2011 and March 2012. Blood use varied significantly among hospitals, and the hospitals in the lowest quartile of blood use had better patient outcomes. If all the hospitals used as little blood as those in the lowest quartile and had outcomes as good, blood product use would be reduced by 802,716 units, with savings of up to $165 million annually.
In addition to the economic cost of blood transfusion, the clinician must be aware of the cost in terms of comorbidities caused by unnecessary blood transfusion.49,50
RECOMMENDATIONS FROM THE AABB
In view of all the current compelling evidence, a restrictive approach to transfusion is the single best strategy to minimize adverse outcomes.51 Below, we outline the current recommendations from the AABB (formerly the American Association of Blood Banks),42 which are similar to the national clinical guideline on blood transfusion in the United Kingdom,52 and have recently been updated, confirming the initial recommendations.53
In critical care patients, transfusion should be considered if the hemoglobin concentration is 7 g/dL or less.
In postoperative patients and hospitalized patients with preexisting cardiovascular disease, transfusion should be considered if the hemoglobin concentration is 8 g/dL or less or if the patient has signs or symptoms of anemia such as chest pain, orthostatic hypotension, or tachycardia unresponsive to fluid resuscitation, or heart failure.
In hemodynamically stable patients with acute coronary syndrome, there is not enough evidence to allow a formal recommendation for or against a liberal or restrictive transfusion threshold.
Consider both the hemoglobin concentration and the symptoms when deciding whether to give a transfusion. This recommendation is shared by a National Institutes of Health consensus conference,54 which indicates that multiple factors related to the patient’s clinical status and oxygen delivery should be considered before deciding to transfuse red blood cells.
The Society of Hospital Medicine55 and the American Society of Hematology56 concur with a parsimonious approach to blood use in their Choosing Wisely campaigns. The American Society of Hematology recommends that if transfusion of red blood cells is necessary, the minimum number of units should be given that relieve the symptoms of anemia or achieve a safe hemoglobin range (7–8 g/dL in stable noncardiac inpatients).57
New electronic tools can monitor the ordering and use of blood products in real time and can identify the hemoglobin level used as the trigger for transfusion. They also provide data on blood use by physician, hospital, and department. These tools can reveal current practice at a glance and allow sharing of best practices among peers and institutions.52
CONSIDER TRANSFUSION FOR HEMOGLOBIN BELOW 7 G/DL
The routine use of blood has come under scrutiny, given its association with increased healthcare costs and morbidity. The accepted practice in stable medical patients is a restrictive threshold approach for blood transfusion, which is to consider (not necessarily give) a single unit of packed red blood cells for a hemoglobin less than 7 g/dL.
However, studies in acute coronary syndrome patients and postoperative cardiac surgery patients have not shown the restrictive threshold to be superior to a liberal threshold in terms of outcomes and costs. This variability suggests the need for further studies to determine the best course of action in different patient subpopulations (eg, surgical, oncologic, trauma, critical illness).
Also, a limitation of most of the clinical studies was that only the hemoglobin concentration was used as a marker of anemia, with no strict assessment of changes in red cell mass with transfusion.
Despite the variability in certain populations, the overall weight of current evidence favors a restrictive approach to blood transfusion (hemoglobin < 7 g/dL), although perhaps in patients who have active coronary disease or are undergoing cardiac surgery, a more lenient threshold (< 8 g/dL) for transfusion should be considered.
- Shander A, Gross I, Hill S, Javidroozi M, Sledge S; College of American Pathologists; American Society of Anesthesiologists; Society of Thoracic Surgeons and Society of Cardiovascular Anesthesiologists; Society of Critical Care Medicine; Italian Society of Transfusion Medicine and Immunohaematology; American Association of Blood Banks. A new perspective on best transfusion practices. Blood Transfus 2013; 11:193–202.
- Madjdpour C, Spahn DR. Allogeneic red blood cell transfusion: physiology of oxygen transport. Best Pract Res Clin Anaesthesiol 2007; 21:163–171.
- Tánczos K, Molnár Z. The oxygen supply-demand balance: a monitoring challenge. Best Pract Res Clin Anaesthesiol 2013; 27:201–207.
- Hebert PC, Van der Linden P, Biro G, Hu LQ. Physiologic aspects of anemia. Crit Care Clin 2004; 20:187–212.
- Spinelli E, Bartlett RH. Anemia and transfusion in critical care: physiology and management. J Intensive Care Med 2016; 31:295–306.
- Jamnicki M, Kocian R, Van Der Linden P, Zaugg M, Spahn DR. Acute normovolemic hemodilution: physiology, limitations, and clinical use. J Cardiothorac Vasc Anesth 2003; 17:747–754.
- Monk TG. Acute normovolemic hemodilution. Anesthesiol Clin North America 2005; 23:271–281.
- Shander A, Rijhwani TS. Acute normovolemic hemodilution. Transfusion 2004; 44(suppl 2):26S–34S.
- Weiskopf RB, Viele MK, Feiner J, et al. Human cardiovascular and metabolic response to acute, severe isovolemic anemia. JAMA 1998; 279:217–221.
- Leung JM, Weiskopf RB, Feiner J, et al. Electrocardiographic ST-segment changes during acute, severe isovolemic hemodilution in humans. Anesthesiology 2000; 93:1004–1010.
- Spahn DR, Zollinger A, Schlumpf RB, et al. Hemodilution tolerance in elderly patients without known cardiac disease. Anesth Analg 1996; 82:681–686.
- Spahn DR, Schmid ER, Seifert B, Pasch T. Hemodilution tolerance in patients with coronary artery disease who are receiving chronic beta-adrenergic blocker therapy. Anesth Analg 1996; 82:687–694.
- Licker M, Ellenberger C, Sierra J, Christenson J, Diaper J, Morel D. Cardiovascular response to acute normovolemic hemodilution in patients with coronary artery diseases: assessment with transesophageal echocardiography. Crit Care Med 2005; 33:591–597.
- Spahn DR, Seifert B, Pasch T, Schmid ER. Haemodilution tolerance in patients with mitral regurgitation. Anaesthesia 1998; 53:20–24.
- Weiskopf RB, Kramer JH, Viele M, et al. Acute severe isovolemic anemia impairs cognitive function and memory in humans. Anesthesiology 2000; 92:1646–1652.
- Weiskopf RB, Feiner J, Hopf HW, et al. Oxygen reverses deficits of cognitive function and memory and increased heart rate induced by acute severe isovolemic anemia. Anesthesiology 2002; 96:871–877.
- Zhou X, Zhang C, Wang Y, Yu L, Yan M. Preoperative acute normovolemic hemodilution for minimizing allogeneic blood transfusion: a meta-analysis. Anesth Analg 2015; 121:1443–1455.
- Hébert P, Wells G, Blajchman M, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med 1999: 340:409–417.
- Carson JL, Terrin ML, Noveck H, et al; FOCUS Investigators. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med 2011; 365:2453–2462.
- Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004; 292:1555–1562.
- Carson JL, Brooks MM, Abbott JD, et al. Liberal versus restrictive transfusion thresholds for patients with symptomatic coronary artery disease. Am Heart J 2013; 165:964.e1–971.e1.
- Murphy GJ, Pike K, Rogers CA, et al; TITRe2 Investigators. Liberal or restrictive transfusion after cardiac surgery. N Engl J Med 2015; 372:997–1008.
- Holst LB, Haase N, Wetterslev J, et al; TRISS Trial Group; Scandinavian Critical Care Trials Group. Lower versus higher hemoglobin threshold for transfusion in septic shock. N Engl J Med 2014; 371:1381–1391.
- Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med 2013; 368:11–21.
- Walsh TS, Boyd JA, Watson D, et al; RELIEVE Investigators. Restrictive versus liberal transfusion strategies for older mechanically ventilated critically ill patients: a randomized pilot trial. Crit Care Med 2013; 41:2354–2363.
- Rohde JM, Dimcheff DE, Blumberg N, et al. Health care–associated infection after red blood cell transfusion. JAMA 2014; 311:1317–1326.
- Salpeter SR, Buckley JS, Chatterjee S. Impact of more restrictive blood transfusion strategies on clinical outcomes: a meta-analysis and systematic review. Am J Med 2014; 127:124.e3–131.e3.
- Wang J, Bao YX, Bai M, Zhang YG, Xu WD, Qi XS. Restrictive vs liberal transfusion for upper gastrointestinal bleeding: a meta-analysis of randomized controlled trials. World J Gastroenterol 2013; 19:6919–6927.
- Vincent JL, Baron JF, Reinhart K, et al; ABC (Anemia and Blood Transfusion in Critical Care) Investigators. Anemia and blood transfusion in critically ill patients. JAMA 2002; 288:1499–1507.
- Dunne JR, Malone D, Tracy JK, Gannon C, Napolitano LM. Perioperative anemia: an independent risk factor for infection, mortality, and resource utilization in surgery. J Surg Res 2002; 102:237–244.
- Brunskill SJ, Millette SL, Shokoohi A, et al. Red blood cell transfusion for people undergoing hip fracture surgery. Cochrane Database Syst Rev 2015; 4:CD009699.
- Weinberg JA, McGwin G Jr, Griffin RL, et al. Age of transfused blood: an independent predictor of mortality despite universal leukoreduction. J Trauma 2008; 65:279–284.
- Steinberg M. Management of sickle cell disease. N Engl J Med 1999; 340:1021–1030.
- Yawn BP, Buchanan GR, Afenyi-Annan AN, et al. Management of sickle cell disease. JAMA 2014; 312:1033–1048.
- Vichinsky EP, Haberkern CM, Neumayr L, et al. A comparison of conservative and aggressive transfusion regimens in the perioperative management of sickle cell disease. The Preoperative Transfusion in Sickle Cell Disease Study Group. N Engl J Med 1995; 333:206–213.
- Howard J, Malfroy M, Llewelyn C, et al. The Transfusion Alternatives Preoperatively in Sickle Cell Disease (TAPS) study: a randomised, controlled, multicentre clinical trial. Lancet 2013; 381:930–938.
- Goodnough LT, Levy JH, Murphy MF. Concepts of blood transfusion in adults. Lancet 2013; 381:1845–1854.
- Holme S. Current issues related to the quality of stored RBCs. Transfus Apher Sci 2005; 33:55–61.
- Hovav T, Yedgar S, Manny N, Barshtein G. Alteration of red cell aggregability and shape during blood storage. Transfusion 1999; 39:277–281.
- Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med 2008; 358:1229–1239.
- Lacroix J, Hebert PC, Fergusson DA, et al. Age of transfused blood in critically ill adults. N Engl J Med 2015; 372:1410–1418.
- Carson JL, Grossman BJ, Kleinman S, et al; Clinical Transfusion Medicine Committee of the AABB. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med 2012; 157:49–58.
- Bolton-Maggs P, Watt A, Poles D, et al, on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2015 Annual SHOT Report. www.shotuk.org/wp-content/uploads/SHOT-2015-Annual-Report-Web-Edition-Final-bookmarked.pdf. Accessed November 30, 2016.
- Shander A, Javidroozi M, Ozawa S, Hare GMT. What is really dangerous: anaemia or transfusion? Br J Anaesth 2011; 107(suppl 1):i41–i59.
- Reeh M, Ghadban T, Dedow J, et al. Allogenic blood transfusion is associated with poor perioperative and long-term outcome in esophageal cancer. World J Surg 2016 Oct 11. [Epub ahead of print]
- Elmi M, Mahar A, Kagedan D, et al. The impact of blood transfusion on perioperative outcomes following gastric cancer resection: an analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Can J Surg 2016; 59:322–329.
- Aquina CT, Blumberg N, Becerra AZ, et al. Association among blood transfusion, sepsis, and decreased long-term survival after colon cancer resection. Ann Surg 2016; Sep 14. [Epub ahead of print] PubMed PMID: 27631770.
- Premiere Analysis. Standardization of blood utilization practices could provide opportunity for improved outcomes, reduced costs. A Premiere Healthcare Alliance Analysis. 2012.
- Simeone F, Franchi F, Cevenini G, et al. A simple clinical model for planning transfusion quantities in heart surgery. BMC Med Inform Decis Mak 2011; 11:44.
- Spahn DR, Goodnough LT. Alternatives to blood transfusion. Lancet 2013; 381:1855–1865.
- Holst LB, Petersen MW, Haase N, Perner A, Wetterslev J. Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis. BMJ 2015; 350:h1354.
- National Institute for Health and Care Excellence: Clinical Guidelines. London: National Institute for Health and Care Excellence (UK). www.ncbi.nlm.nih.gov/books/NBK11822/.
- Carson JL, Guyatt G, Heddle NM, et al. Clinical practice guidelines from the AABB: red blood cell transfusion thresholds and storage. JAMA 2016 Oct 12. doi: 10.1001/jama.2016.9185. [Epub ahead of print]
- Consensus conference. Perioperative red blood cell transfusion. JAMA 1988; 260:2700–2703.
- Bulger J, Nickel W, Messler J, et al. Choosing wisely in adult hospital medicine: five opportunities for improved healthcare value. J Hosp Med 2013; 8:486–492.
- Hicks LK, Bering H, Carson KR, et al. The ASH Choosing Wisely® campaign: five hematologic tests and treatments to question. Blood 2013; 122:3879–3883.
- Haemonetics IMPACT Online. The Blood Management Company. www.haemonetics.com/Products/Services/Consulting Services/IMPACT Online.aspx. Accessed November 30, 2016.
For decades, physicians believed in the benefit of prompt transfusion of blood to keep the hemoglobin level at arbitrary, optimum levels, ie, close to normal values, especially in the critically ill, the elderly, and those with coronary syndromes, stroke, or renal failure.
However, the evidence supporting arbitrary hemoglobin values as an indication for transfusion was weak or nonexistent. Also, blood transfusion can have complications and adverse effects, and blood is costly and scarce. These considerations prompted research into when blood transfusion should be considered, and recommendations that it should be used more sparingly than in the past.
This review offers a perspective on the evidence supporting restrictive blood use. First, we focus on hemodilution studies that demonstrated that humans can tolerate anemia. Then, we look at studies that compared a restrictive transfusion strategy with a liberal one in patients with critical illness and active bleeding. We conclude with current recommendations for blood transfusion.
EVIDENCE FROM HEMODILUTION STUDIES
Hemoglobin is essential for tissue oxygenation, but the serum hemoglobin concentration is just one of several factors involved.1–5 In anemia, the body can adapt not only by increasing production of red blood cells, but also by:
- Increasing cardiac output
- Increasing synthesis of 2,3-diphosphoglycerate (2,3-DPG), with a consequent shift in the oxyhemoglobin dissociation curve to the right, allowing enhanced release of oxygen at the tissue level
- Moving more carbon dioxide into the blood (the Bohr effect), which decreases pH and also shifts the dissociation curve to the right.
Just 20 years ago, physicians were using arbitrary cutoffs such as hemoglobin 10 g/dL or hematocrit 30% as indications for blood transfusion, without reasonable evidence to support these values. Not until acute normovolemic hemodilution studies were performed were we able to progressively appraise how well patients could tolerate lower levels of hemoglobin without significant adverse outcomes.
Acute normovolemic hemodilution involves withdrawing blood and replacing it with crystalloid or colloid solution to maintain the volume.6
Initial studies were done in animals and focused on the safety of acute anemia regarding splanchnic perfusion. Subsequently, studies proved that healthy, elderly, and stable cardiac patients can tolerate acute anemia with normal cardiovascular response. The targets in these studies were modest at first, but researchers aimed progressively for more aggressive hemodilution with lower hemoglobin targets and demonstrated that the body can tolerate and adapt to more severe anemia.6–8
Studies in healthy patients
Weiskopf et al9 assessed the effect of severe anemia in 32 conscious healthy patients (11 presurgical patients and 21 volunteers not undergoing surgery) by performing acute normovolemic hemodilution with 5% human albumin, autologous plasma, or both, with a target hemoglobin level of 5 g/dL. The process was done gradually, obtaining aliquots of blood of 500 to 900 mL. Cardiac index increased, along with a mild increase in oxygen consumption with no increase in plasma lactate levels, suggesting that in conscious healthy patients, tissue oxygenation remains adequate even in severe anemia.
Leung et al10 addressed the electrocardiographic changes that occur with severe anemia (hemoglobin 5 g/dL) in 55 healthy volunteers. Three developed transient, reversible ST-segment depression, which was associated with a higher heart rate than in the volunteers with no electrocardiographic changes; however, the changes were reversible and asymptomatic, and thus were considered physiologic and benign.
Hemodilution in healthy elderly patients
Spahn et al11 performed 6 and 12 mL/kg isovolemic exchange of blood for 6% hydroxyethyl starch in 20 patients older than 65 years (mean age 76, range 65–88) without underlying coronary disease.
The patients’ mean hemoglobin level decreased from 11.6 g/dL to 8.8 g/dL. Their cardiac index and oxygen extraction values increased adequately, with stable oxygen consumption during hemodilution. There were no electrocardiographic signs of ischemia.
Hemodilution in coronary artery disease
Spahn et al12 performed hemodilution studies in 60 patients (ages 35–81) with coronary artery disease managed chronically with beta-blockers who were scheduled for coronary artery bypass graft surgery. Hemodilution was performed with 6- and 12-mL/kg isovolemic exchange of blood for 6% hydroxyethyl starch maintaining normovolemia and stable filling pressures. Hemoglobin levels decreased from 12.6 g/dL to 9.9 g/dL. The hemodilution process was done before the revascularization. The authors monitored hemodynamic variables, ST-segment deviation, and oxygen consumption before and after each hemodilution.
There was a compensatory increase in cardiac index and oxygen extraction with consequent stable oxygen consumption. These changes were independent of patient age or left ventricular function. In addition, there were no electrocardiographic signs of ischemia.
Licker et al13 studied the hemodynamic effect of preoperative hemodilution in 50 patients with coronary artery disease undergoing coronary artery bypass graft surgery, performing transesophageal echocardiography before and after hemodilution. The patients underwent isovolemic exchange with iso-oncotic starch to target a hematocrit of 28%.
Acute normovolemic hemodilution triggered an increase in cardiac stroke volume, which had a direct correlation with an increase in the central venous pressure and the left ventricular end-diastolic area. No signs of ischemia were seen in these patients on electrocardiography or echocardiography (eg, left ventricular wall-motion abnormalities).
Hemodilution in mitral regurgitation
Spahn et al14 performed acute isovolemic hemodilution with 6% hydroxyethyl starch in 20 patients with mitral regurgitation. The cardiac filling pressures were stable before and after hemodilution; the mean hemoglobin value decreased from 13 to 10.3 g/dL. The cardiac index and oxygen extraction increased proportionally, with stable oxygen consumption; these findings were the same regardless of whether the patient was in normal sinus rhythm or atrial fibrillation.
Effect of hemodilution on cognition
Weiskopf et al15 assessed the effect of anemia on executive and memory function by inducing progressive acute isovolemic anemia in 90 healthy volunteers (age 29 ± 5), reducing their hemoglobin values to 7, 6, and 5 g/dL and performing repetitive neuropsychological and memory testing before and after the hemodilution, as well as after autologous blood transfusion to return their hemoglobin level to 7 g/dL.
There were no changes in reaction time or error rate at a hemoglobin concentration of 7 g/dL compared with the performance at a baseline hemoglobin concentration of 14 g/dL. The volunteers got slower on a mathematics test at hemoglobin levels of 6 g/dL and 5 g/dL, but their error rate did not increase. Immediate and delayed memory were significantly impaired at hemoglobin of 5 g/dL but not at 6 g/dL. All tests normalized with blood transfusion once the hemoglobin level reached 7 g/dL.15
Weiskopf et al16 subsequently investigated whether giving supplemental oxygen to raise the arterial partial pressure of oxygen (Pao2) to 350 mm Hg or greater would overcome the neurocognitive effects of severe acute anemia. They followed a protocol similar to the one in the earlier study15 and induced anemia in 31 healthy volunteers, age 28 ± 4 years, with a mean baseline hemoglobin concentration of 12.7 g/dL.
When the volunteers reached a hemoglobin concentration of 5.7 ± 0.3 g/dL, they were significantly slower on the mathematics test, and their delayed memory was significantly impaired. Then, in a double-blind fashion, they were given either room air or oxygen. Oxygen increased the Pao2 to 406 mm Hg and normalized neurocognitive performance.
Hemodilution studies in surgical patients
A 2015 meta-analysis17 of 63 studies involving 3,819 surgical patients compared the risk of perioperative allogeneic blood transfusion as well as the overall volume of transfused blood in patients undergoing preoperative acute normovolemic hemodilution vs a control group. Though the overall data showed that the patients who underwent acute normovolemic hemodilution needed fewer transfusions and less blood (relative risk [RR] 0.74, 95% confidence interval [CI] 0.63–0.88, P = .0006), the authors noted significant heterogeneity and publication bias.
However, the hemodilution studies paved the way for justifying a more conservative and restrictive transfusion strategy, with a hemoglobin cutoff value of 7 g/dL, and in acute anemia, using oxygen to overcome acute neurocognitive effects while searching for and correcting the cause of the anemia.
STUDIES OF RESTRICTIVE VS LIBERAL TRANSFUSION STRATEGIES
Studies in critical care and high-risk patients
Hébert et al18 randomized 418 critical care patients to a restrictive transfusion approach (in which they were given red blood cells if their hemoglobin concentration dropped below 7.0 g/dL) and 420 patients to a liberal strategy (given red blood cells if their hemoglobin concentration dropped below 10.0 g/dL). Mortality rates (restrictive vs liberal strategy) were as follows:
- Overall at 30 days 18.7% vs 23.3%, P = .11
- In the subgroup with less-severe disease (Acute Physiology and Chronic Health Evaluation II [APACHE II] score < 20), 8.7% vs 16.1%, P = .03
- In the subgroup under age 55, 5.7% vs 13%, P = .02
- In the subgroup with clinically significant cardiac disease, 20.5% vs 22.9%, P = .69
- In the hospital, 22.2% vs 28.1%; P = .05.
This study demonstrated that parsimonious blood use did not worsen clinical outcomes in critical care patients.
Carson et al19 evaluated 2,016 patients age 50 and older who had a history of or risk factors for cardiovascular disease and a baseline hemoglobin level below 10 g/dL who underwent surgery for hip fracture. Patients were randomized to two transfusion strategies based on threshold hemoglobin level: restrictive (< 8 g/dL) or liberal (< 10 g/dL). The primary outcome was death or inability to walk without assistance at 60-day follow-up. The median number of units of blood used was 2 in the liberal group and 0 in the restrictive group.
There was no significant difference in the rates of the primary outcome (odds ratio [OR] 1.01, 95% CI 0.84–1.22), infection, venous thromboembolism, or reoperation. This study demonstrated that a liberal transfusion strategy offered no benefit over a restrictive one.
Rao et al20 analyzed the impact of blood transfusion in 24,112 patients with acute coronary syndromes enrolled in three large trials. Ten percent of the patients received at least 1 blood transfusion during their hospitalization, and they were older and had more complex comorbidity.
At 30 days, the group that had received blood had higher rates of death (adjusted hazard ratio [HR] 3.94, 95% CI 3.26–4.75) and the combined outcome of death or myocardial infarction (HR 2.92, 95% CI 2.55–3.35). Transfusion in patients whose nadir hematocrit was higher than 25% was associated with worse outcomes.
This study suggests being cautious about routinely transfusing blood in stable patients with ischemic heart disease solely on the basis of arbitrary hematocrit levels.
Carson et al,21 however, in a later trial, found a trend toward worse outcomes with a restrictive strategy than with a liberal one. Here, 110 patients with acute coronary syndrome or stable angina undergoing cardiac catheterization were randomized to a target hemoglobin level of either at least 8 mg/dL or at least 10 g/dL. The primary outcome (a composite of death, myocardial infarction, or unscheduled revascularization 30 days after randomization) occurred in 14 patients (25.5%) in the restrictive group and 6 patients (10.9%) in the liberal group (P = .054), and 7 (13.0%) vs 1 (1.8%) of the patients died (P = .032).
Murphy et al22 similarly found trends toward worse outcomes with a restrictive strategy in cardiac patients. The investigators randomized 2,007 elective cardiac surgery patients with a postoperative hemoglobin level lower than 9 g/dL to a hemoglobin transfusion threshold of either 7.5 or 9 g/dL. Outcomes (restrictive vs liberal strategies):
- Transfusion rates 53.4% vs 92.2%
- Rates of the primary outcome (a serious infection [sepsis or wound infection] or ischemic event [stroke, myocardial infarction, mesenteric ischemia, or acute kidney injury] within 3 months):
35.1% vs 33.0%, OR 1.11, 95% CI 0.91–1.34, P = .30) - Mortality rates 4.2% vs 2.6%, HR 1.64, 95% CI 1.00–2.67, P = .045
- Total costs did not differ significantly between the groups.
These studies21,22 suggest the need for more definitive trials in patients with active coronary disease and in cardiac surgery patients.
Holst et al23 randomized 998 intensive care patients in septic shock to hemoglobin thresholds for transfusion of 7 vs 9 g/dL. Mortality rates at 90 days (the primary outcome) were 43.0% vs 45.0%, RR 0.94, 95% CI 0.78–1.09, P = .44.
This study suggests that even in septic shock, a liberal transfusion strategy has no advantage over a parsimonious one.
Active bleeding, especially active gastrointestinal bleeding, poses a significant stress that may trigger empirical transfusion even without evidence of the real hemoglobin level.
Villanueva et al24 randomized 921 patients with severe acute upper-gastrointestinal bleeding to two groups, with hemoglobin transfusion triggers of 7 vs 9 g/dL. The findings were impressive:
- Freedom from transfusion 51% vs 14% (P < .001)
- Survival rates at 6 weeks 95% vs 91% (HR 0.55, 95% CI 0.33–0.92, P = .02)
- Rebleeding 10% vs 16% (P = .01).
Patients with peptic ulcer disease as well as those with cirrhosis stage Child-Pugh class A or B had higher survival rates with a restrictive transfusion strategy.
The RELIEVE trial25 compared the effect of a restrictive transfusion strategy in elderly patients on mechanical ventilation in 6 intensive care units in the United Kingdom. Transfusion triggers were hemoglobin 7 vs 9 g/dL, and the mortality rate at 180 days was 55% vs 37%, RR 0.68, 95% CI 0.44–1.05, P = .073.
Meta-analyses and observational studies
Rohde et al26 performed a systematic review and meta-analysis of 17 trials with 7,456 patients, which revealed that a restrictive strategy is associated with a lower risk of nosocomial infection, including pneumonia, wound infection, and sepsis.
The pooled risk of all serious infections was 10.6% in the restrictive group and 12.7% in the liberal group. Even after adjusting for the use of leukocyte reduction, the risk of infection was lower in the restrictive strategy group (RR 0.83, 95% CI 0.69–0.99). With a hemoglobin threshold of less than 7.0 g/dL, the risk of serious infection was 14% lower. Although this was not statistically significant overall (RR 0.86, 95% CI 0.72–1.02), the difference was statistically significant in the subgroup undergoing orthopedic surgery (RR 0.72, 95% CI 0.53–0.97) and the subgroup presenting with sepsis (RR 0.51, 95% CI 0.28–0.95).
Salpeter et al27 performed a meta-analysis and systematic review of three randomized trials (N = 2,364) comparing a restrictive hemoglobin transfusion trigger (hemoglobin < 7 g/dL) vs a more liberal trigger. The groups with restrictive transfusion triggers had lower rates of:
- In-hospital mortality (RR 0.74, 95% CI 0.60–0.92)
- Total mortality (RR 0.80, 95% CI 0.65–0.98)
- Rebleeding (RR 0.64, 95% CI 0.45–0.90)
- Acute coronary syndrome (RR 0.44, 95% CI 0.22–0.89)
- Pulmonary edema (RR 0.48, 95% CI 0.33–0.72)
- Bacterial infections (RR 0.86, 95% CI 0.73–1.00).
Wang et al28 performed a meta-analysis of 4 randomized controlled trials in patients with upper-gastrointestinal bleeding comparing restrictive (hemoglobin < 7 g/dL) vs liberal transfusion strategies. The primary outcomes were death and rebleeding. The restrictive strategy was associated with:
- A lower mortality rate (OR 0.52, 95% CI 0.31–0.87, P = .01)
- A lower rebleeding rate (OR 0.26, 95% CI 0.03–2.10, P = .21)
- Shorter hospitalizations (P = .009)
- Less blood transfused (P = .0005).
Vincent et al,29 in a prospective observational study of 3,534 patients in intensive care units in 146 facilities in Western Europe, found a correlation between transfusion and mortality. Transfusion was done most often in elderly patients and those with a longer stay in the intensive care unit. The 28-day mortality rate was 22.7% in patients who received a transfusion and 17.1% in those who did not (P = .02). The more units of blood the patients received, the more likely they were to die, and receiving more than 4 units was associated with worse outcomes (P = .01).
Dunne et al30 performed a study of 6,301 noncardiac surgical patients in the Veterans Affairs Maryland Healthcare System from the National Veterans Administration Surgical Quality Improvement Program from 1995 to 2000. Multiple logistic regression analysis revealed that the composite of low hematocrit before and after surgery and high transfusion rates (> 4 units per hospitalization) were associated with higher rates of death (P < .01) and postoperative pneumonia (P ≤ .05) and longer hospitalizations (P < .05). The risk of pneumonia increased proportionally with the decrease in hematocrit.
These findings support pharmacologic optimization of anemia with hematinic supplementation before surgery to decrease the risk of needing a transfusion, often with parenteral iron. The fact that the patient’s hemoglobin can be optimized preoperatively by nontransfusional means may decrease the likelihood of blood transfusion, as the hemoglobin will potentially remain above the transfusion threshold. For example, if a patient has a preoperative hemoglobin level of 10 g/dL, and it is optimized up to 12, then if postoperatively the hemoglobin level drops 3 g/dL instead of reaching the threshold of 7 g/dL, the nadir will be just 9 g/dL, far above that transfusion threshold.
Brunskill et al,31 in a Cochrane review of 6 trials with 2,722 patients undergoing surgery for hip fracture, found no difference in rates of mortality, functional recovery or postoperative morbidity with a restrictive transfusion strategy (hemoglobin target > 8 g/dL vs a liberal one (> 10 g/dL). However, the quality of evidence was rated as low. The authors concluded that there is no justification for liberal red blood cell transfusion thresholds (10 g/dL), and a more restrictive transfusion threshold is preferable.
Weinberg et al32 found that, in trauma patients, receiving more than 6 units of blood was associated with poor prognosis, and outcomes were worse when the blood was older than 2 weeks. However, the effect of blood age is not significant when using smaller transfusion volumes (1 to 2 units of red blood cells).
Studies in sickle cell disease
Sickle cell disease patients have high levels of hemoglobin S, which causes erythrocyte sickling and increases blood viscosity. Transfusion with normal erythrocytes increases the amount of hemoglobin A (the normal variant).33,34
In trials in surgical patients,35,36 conservative strategies for preoperative blood transfusion aiming at a hemoglobin level of 10 g/dL were as effective in preventing postoperative complications as decreasing the hemoglobin S levels to 30% by aggressive exchange transfusion.35
In nonsurgical patients, blood transfusion should be based on formal risk-benefit assessments. Therefore, the expert panel report on sickle cell management advises against blood transfusion in sickle cell patients with uncomplicated vaso-occlusive crises, priapism, asymptomatic anemia, or acute kidney injury in the absence of multisystem organ failure.34
Is hemoglobin the most relevant marker?
Most studies that compared restrictive and liberal transfusion strategies focused on using a lower hemoglobin threshold as the transfusion trigger, not on using fewer units of blood. Is the amount of blood transfused more important than the hemoglobin threshold? Perhaps a study focused both on a restrictive vs liberal strategy and also on the minimum amount of blood that each patient may benefit from would help to answer this question.
We should beware of routinely using the hemoglobin concentration as a threshold for transfusion and a surrogate marker of transfusion benefit because changes in hemoglobin concentration may not reflect changes in absolute red cell mass.37 Changes in plasma volume (an increase or decrease) affect the hematocrit concentration without necessarily affecting the total red cell mass. Unfortunately, red cell mass is very difficult to measure; hence, the hemoglobin and hematocrit values are used instead. Studies addressing changes in red cell mass may be needed, perhaps even to validate using the hemoglobin concentration as the sole indicator for transfusion.
Is fresh blood better than old blood?
Using blood that is more than 14 days old may be associated with poor outcomes, for several possible reasons. Red blood cells age rapidly in refrigeration, and usually just 75% may remain viable 24 hours after phlebotomy. Adenosine triphosphate and 2,3-DPG levels steadily decrease, with a consequent decrease in capacity for appropriate tissue oxygen delivery. In addition, loss of membrane phospholipids causes progressive rigidity of the red cell membrane with consequent formation of echynocytes after 14 to 21 days.38,39
The use of blood more than 14 days old in cardiac surgery patients has been associated with worse outcomes, including higher rates of death, prolonged intubation, acute renal failure, and sepsis.40 Similar poor outcomes have been seen in trauma patients.32
Lacroix et al,41 in a multicenter, randomized trial in critically ill adults, compared the outcomes of transfusion of fresh packed red cells (stored < 8 days) or old blood (stored for a mean of 22 days). The primary outcome was the mortality rate at 90 days: 37.0% in the fresh-blood group vs 35.3% in the old-blood group (HR 1.1, 95% CI 0.9–1.2, P = .38).
The authors concluded that using fresh blood compared with old blood was not associated with a lower 90-day mortality rate in critically ill adults.
RISKS ASSOCIATED WITH TRANSFUSION
Infections
The risk of infection from blood transfusion is small. Human immunodeficiency virus (HIV) is transmitted in 1 in 1.5 million transfused blood components, and hepatitis C virus in 1 in 1.1 million; these odds are similar to those of having a fatal airplane accident (1 in 1.7 million per flight). Hepatitis B virus infection is more common, the reported incidence being 1 in 357,000.42
Noninfectious complications
Transfusion-associated circulatory overload occurs in 4% to 6% of patients who receive a transfusion. Therefore, circulatory overload is a greater danger from transfusion than infection is.42
Febrile nonhemolytic transfusion reactions occur in 1.1% of patients with prestorage leukoreduction.
Transfusion-associated acute lung injury occurs in 0.8 per 10,000 blood components transfused.
Errors associated with blood transfusion include, in decreasing order of frequency, transfusion of the wrong blood component, handling and storage errors, inappropriate administration of anti-D immunoglobulin, and avoidable, delayed, or insufficient transfusions.43
Surgery and condition-specific complications of red blood cell transfusion
Cardiovascular surgery. Transfusion is associated with a higher risk of postoperative stroke, respiratory failure, acute respiratory distress syndrome, prolonged intubation time, reintubation, in-hospital death, sepsis, and longer postoperative length of stay.44
Malignancy. The use of blood in this setting has been found to be an independent predictor of recurrence, decreased survival, and increased risk of lymphoplasmacytic and marginal-zone lymphomas.44–47
Vascular, orthopedic, and other surgeries. Transfusion is associated with a higher risk of death, thromboembolic events, acute kidney injury, death, composite morbidity, reoperation, sepsis, and pulmonary complications.44
ST-segment elevation myocardial infarction, sepsis, and intensive care unit admissions. Transfusion is associated with an increased risk of rebleeding, death, and secondary infections.44
COST OF RED BLOOD CELL TRANSFUSION
Up to 85 million units of red blood cells are transfused per year worldwide, 15 million of them in the United States.42 At our hospital in 2013, 1 unit of leukocyte-reduced red blood cells cost $957.27, which included the costs of acquisition, processing, banking, patient testing, administration, and monitoring.
The Premier Healthcare Alliance48 analyzed data from 7.4 million discharges from 464 hospitals between April 2011 and March 2012. Blood use varied significantly among hospitals, and the hospitals in the lowest quartile of blood use had better patient outcomes. If all the hospitals used as little blood as those in the lowest quartile and had outcomes as good, blood product use would be reduced by 802,716 units, with savings of up to $165 million annually.
In addition to the economic cost of blood transfusion, the clinician must be aware of the cost in terms of comorbidities caused by unnecessary blood transfusion.49,50
RECOMMENDATIONS FROM THE AABB
In view of all the current compelling evidence, a restrictive approach to transfusion is the single best strategy to minimize adverse outcomes.51 Below, we outline the current recommendations from the AABB (formerly the American Association of Blood Banks),42 which are similar to the national clinical guideline on blood transfusion in the United Kingdom,52 and have recently been updated, confirming the initial recommendations.53
In critical care patients, transfusion should be considered if the hemoglobin concentration is 7 g/dL or less.
In postoperative patients and hospitalized patients with preexisting cardiovascular disease, transfusion should be considered if the hemoglobin concentration is 8 g/dL or less or if the patient has signs or symptoms of anemia such as chest pain, orthostatic hypotension, or tachycardia unresponsive to fluid resuscitation, or heart failure.
In hemodynamically stable patients with acute coronary syndrome, there is not enough evidence to allow a formal recommendation for or against a liberal or restrictive transfusion threshold.
Consider both the hemoglobin concentration and the symptoms when deciding whether to give a transfusion. This recommendation is shared by a National Institutes of Health consensus conference,54 which indicates that multiple factors related to the patient’s clinical status and oxygen delivery should be considered before deciding to transfuse red blood cells.
The Society of Hospital Medicine55 and the American Society of Hematology56 concur with a parsimonious approach to blood use in their Choosing Wisely campaigns. The American Society of Hematology recommends that if transfusion of red blood cells is necessary, the minimum number of units should be given that relieve the symptoms of anemia or achieve a safe hemoglobin range (7–8 g/dL in stable noncardiac inpatients).57
New electronic tools can monitor the ordering and use of blood products in real time and can identify the hemoglobin level used as the trigger for transfusion. They also provide data on blood use by physician, hospital, and department. These tools can reveal current practice at a glance and allow sharing of best practices among peers and institutions.52
CONSIDER TRANSFUSION FOR HEMOGLOBIN BELOW 7 G/DL
The routine use of blood has come under scrutiny, given its association with increased healthcare costs and morbidity. The accepted practice in stable medical patients is a restrictive threshold approach for blood transfusion, which is to consider (not necessarily give) a single unit of packed red blood cells for a hemoglobin less than 7 g/dL.
However, studies in acute coronary syndrome patients and postoperative cardiac surgery patients have not shown the restrictive threshold to be superior to a liberal threshold in terms of outcomes and costs. This variability suggests the need for further studies to determine the best course of action in different patient subpopulations (eg, surgical, oncologic, trauma, critical illness).
Also, a limitation of most of the clinical studies was that only the hemoglobin concentration was used as a marker of anemia, with no strict assessment of changes in red cell mass with transfusion.
Despite the variability in certain populations, the overall weight of current evidence favors a restrictive approach to blood transfusion (hemoglobin < 7 g/dL), although perhaps in patients who have active coronary disease or are undergoing cardiac surgery, a more lenient threshold (< 8 g/dL) for transfusion should be considered.
For decades, physicians believed in the benefit of prompt transfusion of blood to keep the hemoglobin level at arbitrary, optimum levels, ie, close to normal values, especially in the critically ill, the elderly, and those with coronary syndromes, stroke, or renal failure.
However, the evidence supporting arbitrary hemoglobin values as an indication for transfusion was weak or nonexistent. Also, blood transfusion can have complications and adverse effects, and blood is costly and scarce. These considerations prompted research into when blood transfusion should be considered, and recommendations that it should be used more sparingly than in the past.
This review offers a perspective on the evidence supporting restrictive blood use. First, we focus on hemodilution studies that demonstrated that humans can tolerate anemia. Then, we look at studies that compared a restrictive transfusion strategy with a liberal one in patients with critical illness and active bleeding. We conclude with current recommendations for blood transfusion.
EVIDENCE FROM HEMODILUTION STUDIES
Hemoglobin is essential for tissue oxygenation, but the serum hemoglobin concentration is just one of several factors involved.1–5 In anemia, the body can adapt not only by increasing production of red blood cells, but also by:
- Increasing cardiac output
- Increasing synthesis of 2,3-diphosphoglycerate (2,3-DPG), with a consequent shift in the oxyhemoglobin dissociation curve to the right, allowing enhanced release of oxygen at the tissue level
- Moving more carbon dioxide into the blood (the Bohr effect), which decreases pH and also shifts the dissociation curve to the right.
Just 20 years ago, physicians were using arbitrary cutoffs such as hemoglobin 10 g/dL or hematocrit 30% as indications for blood transfusion, without reasonable evidence to support these values. Not until acute normovolemic hemodilution studies were performed were we able to progressively appraise how well patients could tolerate lower levels of hemoglobin without significant adverse outcomes.
Acute normovolemic hemodilution involves withdrawing blood and replacing it with crystalloid or colloid solution to maintain the volume.6
Initial studies were done in animals and focused on the safety of acute anemia regarding splanchnic perfusion. Subsequently, studies proved that healthy, elderly, and stable cardiac patients can tolerate acute anemia with normal cardiovascular response. The targets in these studies were modest at first, but researchers aimed progressively for more aggressive hemodilution with lower hemoglobin targets and demonstrated that the body can tolerate and adapt to more severe anemia.6–8
Studies in healthy patients
Weiskopf et al9 assessed the effect of severe anemia in 32 conscious healthy patients (11 presurgical patients and 21 volunteers not undergoing surgery) by performing acute normovolemic hemodilution with 5% human albumin, autologous plasma, or both, with a target hemoglobin level of 5 g/dL. The process was done gradually, obtaining aliquots of blood of 500 to 900 mL. Cardiac index increased, along with a mild increase in oxygen consumption with no increase in plasma lactate levels, suggesting that in conscious healthy patients, tissue oxygenation remains adequate even in severe anemia.
Leung et al10 addressed the electrocardiographic changes that occur with severe anemia (hemoglobin 5 g/dL) in 55 healthy volunteers. Three developed transient, reversible ST-segment depression, which was associated with a higher heart rate than in the volunteers with no electrocardiographic changes; however, the changes were reversible and asymptomatic, and thus were considered physiologic and benign.
Hemodilution in healthy elderly patients
Spahn et al11 performed 6 and 12 mL/kg isovolemic exchange of blood for 6% hydroxyethyl starch in 20 patients older than 65 years (mean age 76, range 65–88) without underlying coronary disease.
The patients’ mean hemoglobin level decreased from 11.6 g/dL to 8.8 g/dL. Their cardiac index and oxygen extraction values increased adequately, with stable oxygen consumption during hemodilution. There were no electrocardiographic signs of ischemia.
Hemodilution in coronary artery disease
Spahn et al12 performed hemodilution studies in 60 patients (ages 35–81) with coronary artery disease managed chronically with beta-blockers who were scheduled for coronary artery bypass graft surgery. Hemodilution was performed with 6- and 12-mL/kg isovolemic exchange of blood for 6% hydroxyethyl starch maintaining normovolemia and stable filling pressures. Hemoglobin levels decreased from 12.6 g/dL to 9.9 g/dL. The hemodilution process was done before the revascularization. The authors monitored hemodynamic variables, ST-segment deviation, and oxygen consumption before and after each hemodilution.
There was a compensatory increase in cardiac index and oxygen extraction with consequent stable oxygen consumption. These changes were independent of patient age or left ventricular function. In addition, there were no electrocardiographic signs of ischemia.
Licker et al13 studied the hemodynamic effect of preoperative hemodilution in 50 patients with coronary artery disease undergoing coronary artery bypass graft surgery, performing transesophageal echocardiography before and after hemodilution. The patients underwent isovolemic exchange with iso-oncotic starch to target a hematocrit of 28%.
Acute normovolemic hemodilution triggered an increase in cardiac stroke volume, which had a direct correlation with an increase in the central venous pressure and the left ventricular end-diastolic area. No signs of ischemia were seen in these patients on electrocardiography or echocardiography (eg, left ventricular wall-motion abnormalities).
Hemodilution in mitral regurgitation
Spahn et al14 performed acute isovolemic hemodilution with 6% hydroxyethyl starch in 20 patients with mitral regurgitation. The cardiac filling pressures were stable before and after hemodilution; the mean hemoglobin value decreased from 13 to 10.3 g/dL. The cardiac index and oxygen extraction increased proportionally, with stable oxygen consumption; these findings were the same regardless of whether the patient was in normal sinus rhythm or atrial fibrillation.
Effect of hemodilution on cognition
Weiskopf et al15 assessed the effect of anemia on executive and memory function by inducing progressive acute isovolemic anemia in 90 healthy volunteers (age 29 ± 5), reducing their hemoglobin values to 7, 6, and 5 g/dL and performing repetitive neuropsychological and memory testing before and after the hemodilution, as well as after autologous blood transfusion to return their hemoglobin level to 7 g/dL.
There were no changes in reaction time or error rate at a hemoglobin concentration of 7 g/dL compared with the performance at a baseline hemoglobin concentration of 14 g/dL. The volunteers got slower on a mathematics test at hemoglobin levels of 6 g/dL and 5 g/dL, but their error rate did not increase. Immediate and delayed memory were significantly impaired at hemoglobin of 5 g/dL but not at 6 g/dL. All tests normalized with blood transfusion once the hemoglobin level reached 7 g/dL.15
Weiskopf et al16 subsequently investigated whether giving supplemental oxygen to raise the arterial partial pressure of oxygen (Pao2) to 350 mm Hg or greater would overcome the neurocognitive effects of severe acute anemia. They followed a protocol similar to the one in the earlier study15 and induced anemia in 31 healthy volunteers, age 28 ± 4 years, with a mean baseline hemoglobin concentration of 12.7 g/dL.
When the volunteers reached a hemoglobin concentration of 5.7 ± 0.3 g/dL, they were significantly slower on the mathematics test, and their delayed memory was significantly impaired. Then, in a double-blind fashion, they were given either room air or oxygen. Oxygen increased the Pao2 to 406 mm Hg and normalized neurocognitive performance.
Hemodilution studies in surgical patients
A 2015 meta-analysis17 of 63 studies involving 3,819 surgical patients compared the risk of perioperative allogeneic blood transfusion as well as the overall volume of transfused blood in patients undergoing preoperative acute normovolemic hemodilution vs a control group. Though the overall data showed that the patients who underwent acute normovolemic hemodilution needed fewer transfusions and less blood (relative risk [RR] 0.74, 95% confidence interval [CI] 0.63–0.88, P = .0006), the authors noted significant heterogeneity and publication bias.
However, the hemodilution studies paved the way for justifying a more conservative and restrictive transfusion strategy, with a hemoglobin cutoff value of 7 g/dL, and in acute anemia, using oxygen to overcome acute neurocognitive effects while searching for and correcting the cause of the anemia.
STUDIES OF RESTRICTIVE VS LIBERAL TRANSFUSION STRATEGIES
Studies in critical care and high-risk patients
Hébert et al18 randomized 418 critical care patients to a restrictive transfusion approach (in which they were given red blood cells if their hemoglobin concentration dropped below 7.0 g/dL) and 420 patients to a liberal strategy (given red blood cells if their hemoglobin concentration dropped below 10.0 g/dL). Mortality rates (restrictive vs liberal strategy) were as follows:
- Overall at 30 days 18.7% vs 23.3%, P = .11
- In the subgroup with less-severe disease (Acute Physiology and Chronic Health Evaluation II [APACHE II] score < 20), 8.7% vs 16.1%, P = .03
- In the subgroup under age 55, 5.7% vs 13%, P = .02
- In the subgroup with clinically significant cardiac disease, 20.5% vs 22.9%, P = .69
- In the hospital, 22.2% vs 28.1%; P = .05.
This study demonstrated that parsimonious blood use did not worsen clinical outcomes in critical care patients.
Carson et al19 evaluated 2,016 patients age 50 and older who had a history of or risk factors for cardiovascular disease and a baseline hemoglobin level below 10 g/dL who underwent surgery for hip fracture. Patients were randomized to two transfusion strategies based on threshold hemoglobin level: restrictive (< 8 g/dL) or liberal (< 10 g/dL). The primary outcome was death or inability to walk without assistance at 60-day follow-up. The median number of units of blood used was 2 in the liberal group and 0 in the restrictive group.
There was no significant difference in the rates of the primary outcome (odds ratio [OR] 1.01, 95% CI 0.84–1.22), infection, venous thromboembolism, or reoperation. This study demonstrated that a liberal transfusion strategy offered no benefit over a restrictive one.
Rao et al20 analyzed the impact of blood transfusion in 24,112 patients with acute coronary syndromes enrolled in three large trials. Ten percent of the patients received at least 1 blood transfusion during their hospitalization, and they were older and had more complex comorbidity.
At 30 days, the group that had received blood had higher rates of death (adjusted hazard ratio [HR] 3.94, 95% CI 3.26–4.75) and the combined outcome of death or myocardial infarction (HR 2.92, 95% CI 2.55–3.35). Transfusion in patients whose nadir hematocrit was higher than 25% was associated with worse outcomes.
This study suggests being cautious about routinely transfusing blood in stable patients with ischemic heart disease solely on the basis of arbitrary hematocrit levels.
Carson et al,21 however, in a later trial, found a trend toward worse outcomes with a restrictive strategy than with a liberal one. Here, 110 patients with acute coronary syndrome or stable angina undergoing cardiac catheterization were randomized to a target hemoglobin level of either at least 8 mg/dL or at least 10 g/dL. The primary outcome (a composite of death, myocardial infarction, or unscheduled revascularization 30 days after randomization) occurred in 14 patients (25.5%) in the restrictive group and 6 patients (10.9%) in the liberal group (P = .054), and 7 (13.0%) vs 1 (1.8%) of the patients died (P = .032).
Murphy et al22 similarly found trends toward worse outcomes with a restrictive strategy in cardiac patients. The investigators randomized 2,007 elective cardiac surgery patients with a postoperative hemoglobin level lower than 9 g/dL to a hemoglobin transfusion threshold of either 7.5 or 9 g/dL. Outcomes (restrictive vs liberal strategies):
- Transfusion rates 53.4% vs 92.2%
- Rates of the primary outcome (a serious infection [sepsis or wound infection] or ischemic event [stroke, myocardial infarction, mesenteric ischemia, or acute kidney injury] within 3 months):
35.1% vs 33.0%, OR 1.11, 95% CI 0.91–1.34, P = .30) - Mortality rates 4.2% vs 2.6%, HR 1.64, 95% CI 1.00–2.67, P = .045
- Total costs did not differ significantly between the groups.
These studies21,22 suggest the need for more definitive trials in patients with active coronary disease and in cardiac surgery patients.
Holst et al23 randomized 998 intensive care patients in septic shock to hemoglobin thresholds for transfusion of 7 vs 9 g/dL. Mortality rates at 90 days (the primary outcome) were 43.0% vs 45.0%, RR 0.94, 95% CI 0.78–1.09, P = .44.
This study suggests that even in septic shock, a liberal transfusion strategy has no advantage over a parsimonious one.
Active bleeding, especially active gastrointestinal bleeding, poses a significant stress that may trigger empirical transfusion even without evidence of the real hemoglobin level.
Villanueva et al24 randomized 921 patients with severe acute upper-gastrointestinal bleeding to two groups, with hemoglobin transfusion triggers of 7 vs 9 g/dL. The findings were impressive:
- Freedom from transfusion 51% vs 14% (P < .001)
- Survival rates at 6 weeks 95% vs 91% (HR 0.55, 95% CI 0.33–0.92, P = .02)
- Rebleeding 10% vs 16% (P = .01).
Patients with peptic ulcer disease as well as those with cirrhosis stage Child-Pugh class A or B had higher survival rates with a restrictive transfusion strategy.
The RELIEVE trial25 compared the effect of a restrictive transfusion strategy in elderly patients on mechanical ventilation in 6 intensive care units in the United Kingdom. Transfusion triggers were hemoglobin 7 vs 9 g/dL, and the mortality rate at 180 days was 55% vs 37%, RR 0.68, 95% CI 0.44–1.05, P = .073.
Meta-analyses and observational studies
Rohde et al26 performed a systematic review and meta-analysis of 17 trials with 7,456 patients, which revealed that a restrictive strategy is associated with a lower risk of nosocomial infection, including pneumonia, wound infection, and sepsis.
The pooled risk of all serious infections was 10.6% in the restrictive group and 12.7% in the liberal group. Even after adjusting for the use of leukocyte reduction, the risk of infection was lower in the restrictive strategy group (RR 0.83, 95% CI 0.69–0.99). With a hemoglobin threshold of less than 7.0 g/dL, the risk of serious infection was 14% lower. Although this was not statistically significant overall (RR 0.86, 95% CI 0.72–1.02), the difference was statistically significant in the subgroup undergoing orthopedic surgery (RR 0.72, 95% CI 0.53–0.97) and the subgroup presenting with sepsis (RR 0.51, 95% CI 0.28–0.95).
Salpeter et al27 performed a meta-analysis and systematic review of three randomized trials (N = 2,364) comparing a restrictive hemoglobin transfusion trigger (hemoglobin < 7 g/dL) vs a more liberal trigger. The groups with restrictive transfusion triggers had lower rates of:
- In-hospital mortality (RR 0.74, 95% CI 0.60–0.92)
- Total mortality (RR 0.80, 95% CI 0.65–0.98)
- Rebleeding (RR 0.64, 95% CI 0.45–0.90)
- Acute coronary syndrome (RR 0.44, 95% CI 0.22–0.89)
- Pulmonary edema (RR 0.48, 95% CI 0.33–0.72)
- Bacterial infections (RR 0.86, 95% CI 0.73–1.00).
Wang et al28 performed a meta-analysis of 4 randomized controlled trials in patients with upper-gastrointestinal bleeding comparing restrictive (hemoglobin < 7 g/dL) vs liberal transfusion strategies. The primary outcomes were death and rebleeding. The restrictive strategy was associated with:
- A lower mortality rate (OR 0.52, 95% CI 0.31–0.87, P = .01)
- A lower rebleeding rate (OR 0.26, 95% CI 0.03–2.10, P = .21)
- Shorter hospitalizations (P = .009)
- Less blood transfused (P = .0005).
Vincent et al,29 in a prospective observational study of 3,534 patients in intensive care units in 146 facilities in Western Europe, found a correlation between transfusion and mortality. Transfusion was done most often in elderly patients and those with a longer stay in the intensive care unit. The 28-day mortality rate was 22.7% in patients who received a transfusion and 17.1% in those who did not (P = .02). The more units of blood the patients received, the more likely they were to die, and receiving more than 4 units was associated with worse outcomes (P = .01).
Dunne et al30 performed a study of 6,301 noncardiac surgical patients in the Veterans Affairs Maryland Healthcare System from the National Veterans Administration Surgical Quality Improvement Program from 1995 to 2000. Multiple logistic regression analysis revealed that the composite of low hematocrit before and after surgery and high transfusion rates (> 4 units per hospitalization) were associated with higher rates of death (P < .01) and postoperative pneumonia (P ≤ .05) and longer hospitalizations (P < .05). The risk of pneumonia increased proportionally with the decrease in hematocrit.
These findings support pharmacologic optimization of anemia with hematinic supplementation before surgery to decrease the risk of needing a transfusion, often with parenteral iron. The fact that the patient’s hemoglobin can be optimized preoperatively by nontransfusional means may decrease the likelihood of blood transfusion, as the hemoglobin will potentially remain above the transfusion threshold. For example, if a patient has a preoperative hemoglobin level of 10 g/dL, and it is optimized up to 12, then if postoperatively the hemoglobin level drops 3 g/dL instead of reaching the threshold of 7 g/dL, the nadir will be just 9 g/dL, far above that transfusion threshold.
Brunskill et al,31 in a Cochrane review of 6 trials with 2,722 patients undergoing surgery for hip fracture, found no difference in rates of mortality, functional recovery or postoperative morbidity with a restrictive transfusion strategy (hemoglobin target > 8 g/dL vs a liberal one (> 10 g/dL). However, the quality of evidence was rated as low. The authors concluded that there is no justification for liberal red blood cell transfusion thresholds (10 g/dL), and a more restrictive transfusion threshold is preferable.
Weinberg et al32 found that, in trauma patients, receiving more than 6 units of blood was associated with poor prognosis, and outcomes were worse when the blood was older than 2 weeks. However, the effect of blood age is not significant when using smaller transfusion volumes (1 to 2 units of red blood cells).
Studies in sickle cell disease
Sickle cell disease patients have high levels of hemoglobin S, which causes erythrocyte sickling and increases blood viscosity. Transfusion with normal erythrocytes increases the amount of hemoglobin A (the normal variant).33,34
In trials in surgical patients,35,36 conservative strategies for preoperative blood transfusion aiming at a hemoglobin level of 10 g/dL were as effective in preventing postoperative complications as decreasing the hemoglobin S levels to 30% by aggressive exchange transfusion.35
In nonsurgical patients, blood transfusion should be based on formal risk-benefit assessments. Therefore, the expert panel report on sickle cell management advises against blood transfusion in sickle cell patients with uncomplicated vaso-occlusive crises, priapism, asymptomatic anemia, or acute kidney injury in the absence of multisystem organ failure.34
Is hemoglobin the most relevant marker?
Most studies that compared restrictive and liberal transfusion strategies focused on using a lower hemoglobin threshold as the transfusion trigger, not on using fewer units of blood. Is the amount of blood transfused more important than the hemoglobin threshold? Perhaps a study focused both on a restrictive vs liberal strategy and also on the minimum amount of blood that each patient may benefit from would help to answer this question.
We should beware of routinely using the hemoglobin concentration as a threshold for transfusion and a surrogate marker of transfusion benefit because changes in hemoglobin concentration may not reflect changes in absolute red cell mass.37 Changes in plasma volume (an increase or decrease) affect the hematocrit concentration without necessarily affecting the total red cell mass. Unfortunately, red cell mass is very difficult to measure; hence, the hemoglobin and hematocrit values are used instead. Studies addressing changes in red cell mass may be needed, perhaps even to validate using the hemoglobin concentration as the sole indicator for transfusion.
Is fresh blood better than old blood?
Using blood that is more than 14 days old may be associated with poor outcomes, for several possible reasons. Red blood cells age rapidly in refrigeration, and usually just 75% may remain viable 24 hours after phlebotomy. Adenosine triphosphate and 2,3-DPG levels steadily decrease, with a consequent decrease in capacity for appropriate tissue oxygen delivery. In addition, loss of membrane phospholipids causes progressive rigidity of the red cell membrane with consequent formation of echynocytes after 14 to 21 days.38,39
The use of blood more than 14 days old in cardiac surgery patients has been associated with worse outcomes, including higher rates of death, prolonged intubation, acute renal failure, and sepsis.40 Similar poor outcomes have been seen in trauma patients.32
Lacroix et al,41 in a multicenter, randomized trial in critically ill adults, compared the outcomes of transfusion of fresh packed red cells (stored < 8 days) or old blood (stored for a mean of 22 days). The primary outcome was the mortality rate at 90 days: 37.0% in the fresh-blood group vs 35.3% in the old-blood group (HR 1.1, 95% CI 0.9–1.2, P = .38).
The authors concluded that using fresh blood compared with old blood was not associated with a lower 90-day mortality rate in critically ill adults.
RISKS ASSOCIATED WITH TRANSFUSION
Infections
The risk of infection from blood transfusion is small. Human immunodeficiency virus (HIV) is transmitted in 1 in 1.5 million transfused blood components, and hepatitis C virus in 1 in 1.1 million; these odds are similar to those of having a fatal airplane accident (1 in 1.7 million per flight). Hepatitis B virus infection is more common, the reported incidence being 1 in 357,000.42
Noninfectious complications
Transfusion-associated circulatory overload occurs in 4% to 6% of patients who receive a transfusion. Therefore, circulatory overload is a greater danger from transfusion than infection is.42
Febrile nonhemolytic transfusion reactions occur in 1.1% of patients with prestorage leukoreduction.
Transfusion-associated acute lung injury occurs in 0.8 per 10,000 blood components transfused.
Errors associated with blood transfusion include, in decreasing order of frequency, transfusion of the wrong blood component, handling and storage errors, inappropriate administration of anti-D immunoglobulin, and avoidable, delayed, or insufficient transfusions.43
Surgery and condition-specific complications of red blood cell transfusion
Cardiovascular surgery. Transfusion is associated with a higher risk of postoperative stroke, respiratory failure, acute respiratory distress syndrome, prolonged intubation time, reintubation, in-hospital death, sepsis, and longer postoperative length of stay.44
Malignancy. The use of blood in this setting has been found to be an independent predictor of recurrence, decreased survival, and increased risk of lymphoplasmacytic and marginal-zone lymphomas.44–47
Vascular, orthopedic, and other surgeries. Transfusion is associated with a higher risk of death, thromboembolic events, acute kidney injury, death, composite morbidity, reoperation, sepsis, and pulmonary complications.44
ST-segment elevation myocardial infarction, sepsis, and intensive care unit admissions. Transfusion is associated with an increased risk of rebleeding, death, and secondary infections.44
COST OF RED BLOOD CELL TRANSFUSION
Up to 85 million units of red blood cells are transfused per year worldwide, 15 million of them in the United States.42 At our hospital in 2013, 1 unit of leukocyte-reduced red blood cells cost $957.27, which included the costs of acquisition, processing, banking, patient testing, administration, and monitoring.
The Premier Healthcare Alliance48 analyzed data from 7.4 million discharges from 464 hospitals between April 2011 and March 2012. Blood use varied significantly among hospitals, and the hospitals in the lowest quartile of blood use had better patient outcomes. If all the hospitals used as little blood as those in the lowest quartile and had outcomes as good, blood product use would be reduced by 802,716 units, with savings of up to $165 million annually.
In addition to the economic cost of blood transfusion, the clinician must be aware of the cost in terms of comorbidities caused by unnecessary blood transfusion.49,50
RECOMMENDATIONS FROM THE AABB
In view of all the current compelling evidence, a restrictive approach to transfusion is the single best strategy to minimize adverse outcomes.51 Below, we outline the current recommendations from the AABB (formerly the American Association of Blood Banks),42 which are similar to the national clinical guideline on blood transfusion in the United Kingdom,52 and have recently been updated, confirming the initial recommendations.53
In critical care patients, transfusion should be considered if the hemoglobin concentration is 7 g/dL or less.
In postoperative patients and hospitalized patients with preexisting cardiovascular disease, transfusion should be considered if the hemoglobin concentration is 8 g/dL or less or if the patient has signs or symptoms of anemia such as chest pain, orthostatic hypotension, or tachycardia unresponsive to fluid resuscitation, or heart failure.
In hemodynamically stable patients with acute coronary syndrome, there is not enough evidence to allow a formal recommendation for or against a liberal or restrictive transfusion threshold.
Consider both the hemoglobin concentration and the symptoms when deciding whether to give a transfusion. This recommendation is shared by a National Institutes of Health consensus conference,54 which indicates that multiple factors related to the patient’s clinical status and oxygen delivery should be considered before deciding to transfuse red blood cells.
The Society of Hospital Medicine55 and the American Society of Hematology56 concur with a parsimonious approach to blood use in their Choosing Wisely campaigns. The American Society of Hematology recommends that if transfusion of red blood cells is necessary, the minimum number of units should be given that relieve the symptoms of anemia or achieve a safe hemoglobin range (7–8 g/dL in stable noncardiac inpatients).57
New electronic tools can monitor the ordering and use of blood products in real time and can identify the hemoglobin level used as the trigger for transfusion. They also provide data on blood use by physician, hospital, and department. These tools can reveal current practice at a glance and allow sharing of best practices among peers and institutions.52
CONSIDER TRANSFUSION FOR HEMOGLOBIN BELOW 7 G/DL
The routine use of blood has come under scrutiny, given its association with increased healthcare costs and morbidity. The accepted practice in stable medical patients is a restrictive threshold approach for blood transfusion, which is to consider (not necessarily give) a single unit of packed red blood cells for a hemoglobin less than 7 g/dL.
However, studies in acute coronary syndrome patients and postoperative cardiac surgery patients have not shown the restrictive threshold to be superior to a liberal threshold in terms of outcomes and costs. This variability suggests the need for further studies to determine the best course of action in different patient subpopulations (eg, surgical, oncologic, trauma, critical illness).
Also, a limitation of most of the clinical studies was that only the hemoglobin concentration was used as a marker of anemia, with no strict assessment of changes in red cell mass with transfusion.
Despite the variability in certain populations, the overall weight of current evidence favors a restrictive approach to blood transfusion (hemoglobin < 7 g/dL), although perhaps in patients who have active coronary disease or are undergoing cardiac surgery, a more lenient threshold (< 8 g/dL) for transfusion should be considered.
- Shander A, Gross I, Hill S, Javidroozi M, Sledge S; College of American Pathologists; American Society of Anesthesiologists; Society of Thoracic Surgeons and Society of Cardiovascular Anesthesiologists; Society of Critical Care Medicine; Italian Society of Transfusion Medicine and Immunohaematology; American Association of Blood Banks. A new perspective on best transfusion practices. Blood Transfus 2013; 11:193–202.
- Madjdpour C, Spahn DR. Allogeneic red blood cell transfusion: physiology of oxygen transport. Best Pract Res Clin Anaesthesiol 2007; 21:163–171.
- Tánczos K, Molnár Z. The oxygen supply-demand balance: a monitoring challenge. Best Pract Res Clin Anaesthesiol 2013; 27:201–207.
- Hebert PC, Van der Linden P, Biro G, Hu LQ. Physiologic aspects of anemia. Crit Care Clin 2004; 20:187–212.
- Spinelli E, Bartlett RH. Anemia and transfusion in critical care: physiology and management. J Intensive Care Med 2016; 31:295–306.
- Jamnicki M, Kocian R, Van Der Linden P, Zaugg M, Spahn DR. Acute normovolemic hemodilution: physiology, limitations, and clinical use. J Cardiothorac Vasc Anesth 2003; 17:747–754.
- Monk TG. Acute normovolemic hemodilution. Anesthesiol Clin North America 2005; 23:271–281.
- Shander A, Rijhwani TS. Acute normovolemic hemodilution. Transfusion 2004; 44(suppl 2):26S–34S.
- Weiskopf RB, Viele MK, Feiner J, et al. Human cardiovascular and metabolic response to acute, severe isovolemic anemia. JAMA 1998; 279:217–221.
- Leung JM, Weiskopf RB, Feiner J, et al. Electrocardiographic ST-segment changes during acute, severe isovolemic hemodilution in humans. Anesthesiology 2000; 93:1004–1010.
- Spahn DR, Zollinger A, Schlumpf RB, et al. Hemodilution tolerance in elderly patients without known cardiac disease. Anesth Analg 1996; 82:681–686.
- Spahn DR, Schmid ER, Seifert B, Pasch T. Hemodilution tolerance in patients with coronary artery disease who are receiving chronic beta-adrenergic blocker therapy. Anesth Analg 1996; 82:687–694.
- Licker M, Ellenberger C, Sierra J, Christenson J, Diaper J, Morel D. Cardiovascular response to acute normovolemic hemodilution in patients with coronary artery diseases: assessment with transesophageal echocardiography. Crit Care Med 2005; 33:591–597.
- Spahn DR, Seifert B, Pasch T, Schmid ER. Haemodilution tolerance in patients with mitral regurgitation. Anaesthesia 1998; 53:20–24.
- Weiskopf RB, Kramer JH, Viele M, et al. Acute severe isovolemic anemia impairs cognitive function and memory in humans. Anesthesiology 2000; 92:1646–1652.
- Weiskopf RB, Feiner J, Hopf HW, et al. Oxygen reverses deficits of cognitive function and memory and increased heart rate induced by acute severe isovolemic anemia. Anesthesiology 2002; 96:871–877.
- Zhou X, Zhang C, Wang Y, Yu L, Yan M. Preoperative acute normovolemic hemodilution for minimizing allogeneic blood transfusion: a meta-analysis. Anesth Analg 2015; 121:1443–1455.
- Hébert P, Wells G, Blajchman M, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med 1999: 340:409–417.
- Carson JL, Terrin ML, Noveck H, et al; FOCUS Investigators. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med 2011; 365:2453–2462.
- Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004; 292:1555–1562.
- Carson JL, Brooks MM, Abbott JD, et al. Liberal versus restrictive transfusion thresholds for patients with symptomatic coronary artery disease. Am Heart J 2013; 165:964.e1–971.e1.
- Murphy GJ, Pike K, Rogers CA, et al; TITRe2 Investigators. Liberal or restrictive transfusion after cardiac surgery. N Engl J Med 2015; 372:997–1008.
- Holst LB, Haase N, Wetterslev J, et al; TRISS Trial Group; Scandinavian Critical Care Trials Group. Lower versus higher hemoglobin threshold for transfusion in septic shock. N Engl J Med 2014; 371:1381–1391.
- Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med 2013; 368:11–21.
- Walsh TS, Boyd JA, Watson D, et al; RELIEVE Investigators. Restrictive versus liberal transfusion strategies for older mechanically ventilated critically ill patients: a randomized pilot trial. Crit Care Med 2013; 41:2354–2363.
- Rohde JM, Dimcheff DE, Blumberg N, et al. Health care–associated infection after red blood cell transfusion. JAMA 2014; 311:1317–1326.
- Salpeter SR, Buckley JS, Chatterjee S. Impact of more restrictive blood transfusion strategies on clinical outcomes: a meta-analysis and systematic review. Am J Med 2014; 127:124.e3–131.e3.
- Wang J, Bao YX, Bai M, Zhang YG, Xu WD, Qi XS. Restrictive vs liberal transfusion for upper gastrointestinal bleeding: a meta-analysis of randomized controlled trials. World J Gastroenterol 2013; 19:6919–6927.
- Vincent JL, Baron JF, Reinhart K, et al; ABC (Anemia and Blood Transfusion in Critical Care) Investigators. Anemia and blood transfusion in critically ill patients. JAMA 2002; 288:1499–1507.
- Dunne JR, Malone D, Tracy JK, Gannon C, Napolitano LM. Perioperative anemia: an independent risk factor for infection, mortality, and resource utilization in surgery. J Surg Res 2002; 102:237–244.
- Brunskill SJ, Millette SL, Shokoohi A, et al. Red blood cell transfusion for people undergoing hip fracture surgery. Cochrane Database Syst Rev 2015; 4:CD009699.
- Weinberg JA, McGwin G Jr, Griffin RL, et al. Age of transfused blood: an independent predictor of mortality despite universal leukoreduction. J Trauma 2008; 65:279–284.
- Steinberg M. Management of sickle cell disease. N Engl J Med 1999; 340:1021–1030.
- Yawn BP, Buchanan GR, Afenyi-Annan AN, et al. Management of sickle cell disease. JAMA 2014; 312:1033–1048.
- Vichinsky EP, Haberkern CM, Neumayr L, et al. A comparison of conservative and aggressive transfusion regimens in the perioperative management of sickle cell disease. The Preoperative Transfusion in Sickle Cell Disease Study Group. N Engl J Med 1995; 333:206–213.
- Howard J, Malfroy M, Llewelyn C, et al. The Transfusion Alternatives Preoperatively in Sickle Cell Disease (TAPS) study: a randomised, controlled, multicentre clinical trial. Lancet 2013; 381:930–938.
- Goodnough LT, Levy JH, Murphy MF. Concepts of blood transfusion in adults. Lancet 2013; 381:1845–1854.
- Holme S. Current issues related to the quality of stored RBCs. Transfus Apher Sci 2005; 33:55–61.
- Hovav T, Yedgar S, Manny N, Barshtein G. Alteration of red cell aggregability and shape during blood storage. Transfusion 1999; 39:277–281.
- Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med 2008; 358:1229–1239.
- Lacroix J, Hebert PC, Fergusson DA, et al. Age of transfused blood in critically ill adults. N Engl J Med 2015; 372:1410–1418.
- Carson JL, Grossman BJ, Kleinman S, et al; Clinical Transfusion Medicine Committee of the AABB. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med 2012; 157:49–58.
- Bolton-Maggs P, Watt A, Poles D, et al, on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2015 Annual SHOT Report. www.shotuk.org/wp-content/uploads/SHOT-2015-Annual-Report-Web-Edition-Final-bookmarked.pdf. Accessed November 30, 2016.
- Shander A, Javidroozi M, Ozawa S, Hare GMT. What is really dangerous: anaemia or transfusion? Br J Anaesth 2011; 107(suppl 1):i41–i59.
- Reeh M, Ghadban T, Dedow J, et al. Allogenic blood transfusion is associated with poor perioperative and long-term outcome in esophageal cancer. World J Surg 2016 Oct 11. [Epub ahead of print]
- Elmi M, Mahar A, Kagedan D, et al. The impact of blood transfusion on perioperative outcomes following gastric cancer resection: an analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Can J Surg 2016; 59:322–329.
- Aquina CT, Blumberg N, Becerra AZ, et al. Association among blood transfusion, sepsis, and decreased long-term survival after colon cancer resection. Ann Surg 2016; Sep 14. [Epub ahead of print] PubMed PMID: 27631770.
- Premiere Analysis. Standardization of blood utilization practices could provide opportunity for improved outcomes, reduced costs. A Premiere Healthcare Alliance Analysis. 2012.
- Simeone F, Franchi F, Cevenini G, et al. A simple clinical model for planning transfusion quantities in heart surgery. BMC Med Inform Decis Mak 2011; 11:44.
- Spahn DR, Goodnough LT. Alternatives to blood transfusion. Lancet 2013; 381:1855–1865.
- Holst LB, Petersen MW, Haase N, Perner A, Wetterslev J. Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis. BMJ 2015; 350:h1354.
- National Institute for Health and Care Excellence: Clinical Guidelines. London: National Institute for Health and Care Excellence (UK). www.ncbi.nlm.nih.gov/books/NBK11822/.
- Carson JL, Guyatt G, Heddle NM, et al. Clinical practice guidelines from the AABB: red blood cell transfusion thresholds and storage. JAMA 2016 Oct 12. doi: 10.1001/jama.2016.9185. [Epub ahead of print]
- Consensus conference. Perioperative red blood cell transfusion. JAMA 1988; 260:2700–2703.
- Bulger J, Nickel W, Messler J, et al. Choosing wisely in adult hospital medicine: five opportunities for improved healthcare value. J Hosp Med 2013; 8:486–492.
- Hicks LK, Bering H, Carson KR, et al. The ASH Choosing Wisely® campaign: five hematologic tests and treatments to question. Blood 2013; 122:3879–3883.
- Haemonetics IMPACT Online. The Blood Management Company. www.haemonetics.com/Products/Services/Consulting Services/IMPACT Online.aspx. Accessed November 30, 2016.
- Shander A, Gross I, Hill S, Javidroozi M, Sledge S; College of American Pathologists; American Society of Anesthesiologists; Society of Thoracic Surgeons and Society of Cardiovascular Anesthesiologists; Society of Critical Care Medicine; Italian Society of Transfusion Medicine and Immunohaematology; American Association of Blood Banks. A new perspective on best transfusion practices. Blood Transfus 2013; 11:193–202.
- Madjdpour C, Spahn DR. Allogeneic red blood cell transfusion: physiology of oxygen transport. Best Pract Res Clin Anaesthesiol 2007; 21:163–171.
- Tánczos K, Molnár Z. The oxygen supply-demand balance: a monitoring challenge. Best Pract Res Clin Anaesthesiol 2013; 27:201–207.
- Hebert PC, Van der Linden P, Biro G, Hu LQ. Physiologic aspects of anemia. Crit Care Clin 2004; 20:187–212.
- Spinelli E, Bartlett RH. Anemia and transfusion in critical care: physiology and management. J Intensive Care Med 2016; 31:295–306.
- Jamnicki M, Kocian R, Van Der Linden P, Zaugg M, Spahn DR. Acute normovolemic hemodilution: physiology, limitations, and clinical use. J Cardiothorac Vasc Anesth 2003; 17:747–754.
- Monk TG. Acute normovolemic hemodilution. Anesthesiol Clin North America 2005; 23:271–281.
- Shander A, Rijhwani TS. Acute normovolemic hemodilution. Transfusion 2004; 44(suppl 2):26S–34S.
- Weiskopf RB, Viele MK, Feiner J, et al. Human cardiovascular and metabolic response to acute, severe isovolemic anemia. JAMA 1998; 279:217–221.
- Leung JM, Weiskopf RB, Feiner J, et al. Electrocardiographic ST-segment changes during acute, severe isovolemic hemodilution in humans. Anesthesiology 2000; 93:1004–1010.
- Spahn DR, Zollinger A, Schlumpf RB, et al. Hemodilution tolerance in elderly patients without known cardiac disease. Anesth Analg 1996; 82:681–686.
- Spahn DR, Schmid ER, Seifert B, Pasch T. Hemodilution tolerance in patients with coronary artery disease who are receiving chronic beta-adrenergic blocker therapy. Anesth Analg 1996; 82:687–694.
- Licker M, Ellenberger C, Sierra J, Christenson J, Diaper J, Morel D. Cardiovascular response to acute normovolemic hemodilution in patients with coronary artery diseases: assessment with transesophageal echocardiography. Crit Care Med 2005; 33:591–597.
- Spahn DR, Seifert B, Pasch T, Schmid ER. Haemodilution tolerance in patients with mitral regurgitation. Anaesthesia 1998; 53:20–24.
- Weiskopf RB, Kramer JH, Viele M, et al. Acute severe isovolemic anemia impairs cognitive function and memory in humans. Anesthesiology 2000; 92:1646–1652.
- Weiskopf RB, Feiner J, Hopf HW, et al. Oxygen reverses deficits of cognitive function and memory and increased heart rate induced by acute severe isovolemic anemia. Anesthesiology 2002; 96:871–877.
- Zhou X, Zhang C, Wang Y, Yu L, Yan M. Preoperative acute normovolemic hemodilution for minimizing allogeneic blood transfusion: a meta-analysis. Anesth Analg 2015; 121:1443–1455.
- Hébert P, Wells G, Blajchman M, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med 1999: 340:409–417.
- Carson JL, Terrin ML, Noveck H, et al; FOCUS Investigators. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med 2011; 365:2453–2462.
- Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004; 292:1555–1562.
- Carson JL, Brooks MM, Abbott JD, et al. Liberal versus restrictive transfusion thresholds for patients with symptomatic coronary artery disease. Am Heart J 2013; 165:964.e1–971.e1.
- Murphy GJ, Pike K, Rogers CA, et al; TITRe2 Investigators. Liberal or restrictive transfusion after cardiac surgery. N Engl J Med 2015; 372:997–1008.
- Holst LB, Haase N, Wetterslev J, et al; TRISS Trial Group; Scandinavian Critical Care Trials Group. Lower versus higher hemoglobin threshold for transfusion in septic shock. N Engl J Med 2014; 371:1381–1391.
- Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med 2013; 368:11–21.
- Walsh TS, Boyd JA, Watson D, et al; RELIEVE Investigators. Restrictive versus liberal transfusion strategies for older mechanically ventilated critically ill patients: a randomized pilot trial. Crit Care Med 2013; 41:2354–2363.
- Rohde JM, Dimcheff DE, Blumberg N, et al. Health care–associated infection after red blood cell transfusion. JAMA 2014; 311:1317–1326.
- Salpeter SR, Buckley JS, Chatterjee S. Impact of more restrictive blood transfusion strategies on clinical outcomes: a meta-analysis and systematic review. Am J Med 2014; 127:124.e3–131.e3.
- Wang J, Bao YX, Bai M, Zhang YG, Xu WD, Qi XS. Restrictive vs liberal transfusion for upper gastrointestinal bleeding: a meta-analysis of randomized controlled trials. World J Gastroenterol 2013; 19:6919–6927.
- Vincent JL, Baron JF, Reinhart K, et al; ABC (Anemia and Blood Transfusion in Critical Care) Investigators. Anemia and blood transfusion in critically ill patients. JAMA 2002; 288:1499–1507.
- Dunne JR, Malone D, Tracy JK, Gannon C, Napolitano LM. Perioperative anemia: an independent risk factor for infection, mortality, and resource utilization in surgery. J Surg Res 2002; 102:237–244.
- Brunskill SJ, Millette SL, Shokoohi A, et al. Red blood cell transfusion for people undergoing hip fracture surgery. Cochrane Database Syst Rev 2015; 4:CD009699.
- Weinberg JA, McGwin G Jr, Griffin RL, et al. Age of transfused blood: an independent predictor of mortality despite universal leukoreduction. J Trauma 2008; 65:279–284.
- Steinberg M. Management of sickle cell disease. N Engl J Med 1999; 340:1021–1030.
- Yawn BP, Buchanan GR, Afenyi-Annan AN, et al. Management of sickle cell disease. JAMA 2014; 312:1033–1048.
- Vichinsky EP, Haberkern CM, Neumayr L, et al. A comparison of conservative and aggressive transfusion regimens in the perioperative management of sickle cell disease. The Preoperative Transfusion in Sickle Cell Disease Study Group. N Engl J Med 1995; 333:206–213.
- Howard J, Malfroy M, Llewelyn C, et al. The Transfusion Alternatives Preoperatively in Sickle Cell Disease (TAPS) study: a randomised, controlled, multicentre clinical trial. Lancet 2013; 381:930–938.
- Goodnough LT, Levy JH, Murphy MF. Concepts of blood transfusion in adults. Lancet 2013; 381:1845–1854.
- Holme S. Current issues related to the quality of stored RBCs. Transfus Apher Sci 2005; 33:55–61.
- Hovav T, Yedgar S, Manny N, Barshtein G. Alteration of red cell aggregability and shape during blood storage. Transfusion 1999; 39:277–281.
- Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med 2008; 358:1229–1239.
- Lacroix J, Hebert PC, Fergusson DA, et al. Age of transfused blood in critically ill adults. N Engl J Med 2015; 372:1410–1418.
- Carson JL, Grossman BJ, Kleinman S, et al; Clinical Transfusion Medicine Committee of the AABB. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med 2012; 157:49–58.
- Bolton-Maggs P, Watt A, Poles D, et al, on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2015 Annual SHOT Report. www.shotuk.org/wp-content/uploads/SHOT-2015-Annual-Report-Web-Edition-Final-bookmarked.pdf. Accessed November 30, 2016.
- Shander A, Javidroozi M, Ozawa S, Hare GMT. What is really dangerous: anaemia or transfusion? Br J Anaesth 2011; 107(suppl 1):i41–i59.
- Reeh M, Ghadban T, Dedow J, et al. Allogenic blood transfusion is associated with poor perioperative and long-term outcome in esophageal cancer. World J Surg 2016 Oct 11. [Epub ahead of print]
- Elmi M, Mahar A, Kagedan D, et al. The impact of blood transfusion on perioperative outcomes following gastric cancer resection: an analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Can J Surg 2016; 59:322–329.
- Aquina CT, Blumberg N, Becerra AZ, et al. Association among blood transfusion, sepsis, and decreased long-term survival after colon cancer resection. Ann Surg 2016; Sep 14. [Epub ahead of print] PubMed PMID: 27631770.
- Premiere Analysis. Standardization of blood utilization practices could provide opportunity for improved outcomes, reduced costs. A Premiere Healthcare Alliance Analysis. 2012.
- Simeone F, Franchi F, Cevenini G, et al. A simple clinical model for planning transfusion quantities in heart surgery. BMC Med Inform Decis Mak 2011; 11:44.
- Spahn DR, Goodnough LT. Alternatives to blood transfusion. Lancet 2013; 381:1855–1865.
- Holst LB, Petersen MW, Haase N, Perner A, Wetterslev J. Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis. BMJ 2015; 350:h1354.
- National Institute for Health and Care Excellence: Clinical Guidelines. London: National Institute for Health and Care Excellence (UK). www.ncbi.nlm.nih.gov/books/NBK11822/.
- Carson JL, Guyatt G, Heddle NM, et al. Clinical practice guidelines from the AABB: red blood cell transfusion thresholds and storage. JAMA 2016 Oct 12. doi: 10.1001/jama.2016.9185. [Epub ahead of print]
- Consensus conference. Perioperative red blood cell transfusion. JAMA 1988; 260:2700–2703.
- Bulger J, Nickel W, Messler J, et al. Choosing wisely in adult hospital medicine: five opportunities for improved healthcare value. J Hosp Med 2013; 8:486–492.
- Hicks LK, Bering H, Carson KR, et al. The ASH Choosing Wisely® campaign: five hematologic tests and treatments to question. Blood 2013; 122:3879–3883.
- Haemonetics IMPACT Online. The Blood Management Company. www.haemonetics.com/Products/Services/Consulting Services/IMPACT Online.aspx. Accessed November 30, 2016.
KEY POINTS
- In critical care patients, transfusion should be considered when the hemoglobin concentration reaches 7 g/dL or less.
- In postoperative patients and hospitalized patients with preexisting cardiovascular disease, transfusion should be considered at a hemoglobin concentration of 8 g/dL or less or for symptoms such as chest pain, orthostatic hypotension, or tachycardia unresponsive to fluid resuscitation, or heart failure.
- Consider both the hemoglobin concentration and the symptoms when deciding whether to give a patient a transfusion.

Should we stop the oral selective estrogen receptor modulator raloxifene prior to surgery?
Should mesalamine be stopped prior to noncardiac surgery to avoid bleeding complications?
Nuts and bolts of preoperative clinics: The view from three institutions
Weiner Center for Preoperative Evaluation at Brigham and Women’s Hospital
By Angela M. Bader, MD, MPH
When organizing our preoperative clinic at Brigham and Women’s Hospital, we had several goals. Overall, we wanted a standardized process to help us achieve a high level of excellence. We hoped that creating a new system would eliminate ambiguity about who was responsible for following up on a patient’s abnormal laboratory test result—the surgeon, anesthesiologist, or primary care physician. We also wanted to better coordinate the various care teams involved throughout the perioperative period.
STANDARDIZATION HELPS MEET MANY GOALS
Standardization can occur at many levels:
- Performance of assessments and testing
- Organization of the patient chart and medical records
- Systems checks throughout the process to ensure that nothing is missed
- Team-to-team communication.
Documentation requirements apply regardless of institutional structure
When considering any system of preoperative assessment, keep in mind that the hospital must meet and appropriately document compliance with all regulatory, accreditation, and payer requirements and guidelines, such as those of the Joint Commission, the Centers for Medicare and Medicaid Services (CMS), and the National Surgical Quality Improvement Program. For example, the Joint Commission requires that a surgical history and physical examination be done within 30 days of a procedure. An anesthesiology assessment and a nursing assessment are also required. All of these assessments have mandatory elements, including documenting “never events” and ordering appropriate laboratory tests, electrocardiograms (ECGs), and radiographs.
Sometimes administrators of other hospitals say to me, “We can’t afford a preoperative clinic, and we don’t need one.” My response is that regardless of whether a hospital has a preoperative clinic, the regulatory requirements and guidelines must be met: it is not an issue of avoiding certain steps. Having a dedicated preoperative clinic simply shifts the work to a standardized, centralized system and avoids delaying these required steps until the day of surgery, when taking care of a problem involves the most inefficient use of resources.
Tailor system to institutional needs and characteristics
Within the regulatory framework, the organizational scheme of every institution must address issues of volume and acuity, the types of surgery performed, and the time frames required. A system must be able to deal with the preoperative needs of patients undergoing operations that are booked weeks in advance (often the case for orthopedic surgery) as well as those that may not be booked until a day before the procedure (eg, cancer surgery).
Our plan was developed for our very high-volume, tertiary care institution. In 2008, 24,000 patients used our clinic (roughly 100 patients per day).
DESIGN OF THE PREOPERATIVE CLINIC
A nurse practitioner–based model for ‘one-stop shopping’
We decided that the clinic should offer all elements of the preoperative assessment and thereby give patients “one-stop shopping.” Each patient sees a nurse practitioner, who performs the surgical history and physical examination as well as the anesthesiology and nursing assessments. The result is a multidisciplinary approach with a single assessment output. We shifted employees who had been responsible for preoperative assessment in the offices of various surgeons to a central clinic so that all assessments could be standardized, and we provided additional training to enable them to perform various assessments. The nurse practitioners are supervised by an on-site attending physician, as detailed below.
This model offers a number of advantages:
- Patients see a single provider.
- Assessment is facilitated for our surgeons, who may not be completely up-to-date on perioperative risk assessment and management.
- We have a central location for standardized education programs for our physicians, nurses, and residents.
- The clinic’s standardized records and processes facilitate data generation for research and clinical practice improvement.
Independent budgetary and staffing structure
The preoperative clinic is a separate cost center under the leadership of the department of anesthesiology. Resources were shifted to a central location so that as volume increases, we can add resources to meet the additional volume. We contracted with the hospital administration to provide payment for two full-time-equivalent anesthesiologists per day, who serve as on-site attending physicians. The hospital is willing to do this because not only do these attending physicians supervise the anesthesiology assessment, they are the collaborating physicians for the entire perioperative assessment. They review every patient, order tests and write prescriptions as needed, and discuss issues with the primary care physicians and referring specialists.
The preoperative clinic has an anesthesiologist director (me) who reports directly to the hospital’s vice president for surgical services on budget and staffing issues. I also report to the chairman of the department of anesthesiology, though he is not involved in budgetary functions (the hospital contracts with him to provide the anesthesiology staffing). The clerical and nursing staff work directly for the clinic.
The clinic is run in a self-contained area with a central waiting room and space for doing all the assessments and laboratory work internally, including 16 examination rooms and a room for chart organization.
MORE BENEFITS OF STANDARDIZATION
Standardized scheduling ensures reliability
The secretaries in each surgeon’s office schedule appointments through a central computer system after registration and insurance precertification. Our computer system does not allow an operation to be scheduled without an evaluation also being scheduled. The evaluation can involve either a visit or a telephone screen; we provide algorithms so that the surgeons’ secretaries know which is required. This system has substantially reduced the number of walk-ins, allowing for a more even distribution of patients and ensuring that medical records will be available when a patient is seen.
We watch our schedule carefully. Our computer system monitors the time that each patient is in our clinic to determine his or her waiting time and assessment time. It takes about 75 minutes to go through the whole process, including the time for a nurse practitioner to do the surgical history and physical examination and the anesthesiology and nursing assessments, a laboratory technician to do an ECG and laboratory tests if indicated, and completion of all required documentation. Accordingly, patients are scheduled in 75-minute blocks between 7:00 am and 6:30 pm. We do not have evening or weekend hours because of the difficulty of contacting surgeons and primary care physicians when questions arise. It is simply not cost-effective to have to do that type of follow-up on a case after the patient leaves.
Only about 10% of our patients are screened by telephone, since most of our operations are complicated and require in-person assessment (most low-acuity procedures are done at other hospitals). Of the patients who visit the preoperative clinic, about 75% undergo the single assessment model for surgery, anesthesiology, and nursing as described above. The remaining 25% of patients have their history and physical exam completed outside Brigham and Women’s Hospital for insurance reasons; the remainder of their assessment is conducted in our preoperative clinic by a registered nurse and an anesthesiology resident.
Multiple systems checks
Our model also incorporates standardization in the form of multiple systems checks:
- Case presentation. Every case is presented to an attending anesthesiologist, who reviews the ECG (if ordered) before the patient leaves the clinic.
- Post-visit chart check. A registered nurse or nurse practitioner signs off on each chart after the visit, confirming test results and resolution of all paperwork issues.
- Surgical checklist. The end result is a checklist that serves as the front sheet of the operating room chart.
Our ability to use this system of checks to get the chart completed comprehensively and reliably and deliver it to the operating room when needed was key to securing institutional support and funding for the preoperative clinic.
ROLE OF THE ATTENDING ANESTHESIOLOGISTS
Two full-time attending anesthesiologists are present in the preoperative clinic each day. One is responsible largely for supervising the nurse practitioner assessments and reviewing case presentations, while the other also oversees the education and supervision of residents. Residents rotate through the clinic for 2 weeks (one or two at a time) and have a designated curriculum consisting of daily lectures and competencies in preoperative evaluation.
Because our anesthesiologists are expert in preoperative assessment, we require very few outside consults. We can communicate directly with the cardiologists and other physicians and order tests when indicated. We have a clerical assistant who obtains all necessary paperwork and prior testing from outside providers so that the clinicians need not waste time on this.
A GROWING CHALLENGE: ASSESSMENT FOR PROCEDURES IN AMBULATORY SETTINGS
Looking forward, a rapidly growing challenge facing our clinic stems from the tremendous growth in patients who require anesthesia for procedures performed outside the operating room. In these situations, the proceduralists need a system for deciding whether an anesthesiologist must be present for any given case.
We have started to develop appropriate screening processes to ensure that the proceduralists in multiple departments know which patients to refer for preprocedure assessment. We hope to soon develop protocols for high-risk patients and for various procedures such as implanting a pacemaker or defibrillator, catheter procedures, interventional radiology, and endoscopy.
Anesthesia Perioperative Medicine Clinic at University of Chicago
By BobbieJean Sweitzer, MD
Detsky and Naglie have argued that the costs and clinical outcomes associated with any intervention must be compared with those of alternate strategies for treating the same patients,1 and I believe their point applies well to preoperative clinics. Although certain requirements of the Joint Commission and CMS must be met, as noted by Dr. Bader, they can be met in various ways. I will preface my comments by emphasizing that one size does not fit all: every institution must decide the best approach to preoperative assessment based on its patient population, the types of procedures it performs, and the volume it handles.
TRIAGE STREAMLINES THE PROCESS
Our preoperative clinic at the University of Chicago emphasizes triage. Not every patient should have to go to the trouble of coming in to see a provider. In the future, we will likely see more “virtual” preoperative assessments using devices in development, such as handheld ultrasonography machines. Just as patients can have their pacemakers and implantable cardiac defibrillators remotely checked via phone contact, more tools will one day be available for remote assessment.
Although not every surgical patient needs to come in to the preoperative clinic, every patient must have a physical examination. All patients will be seen on the day of surgery, so in some cases the physical exam may be able to wait until then. For example, an airway assessment need not be done ahead of time. Most anesthesiologists are prepared to manage airways on very short notice, so extensive advance planning is not always necessary.
Obtain basic info by questionnaire to save staff time
Information about the patient is key to triage, and it may be either paper- or computer-based. An initial priority should be to develop some mechanism for getting information from patients before the day of their procedure without a visit to the hospital or ambulatory surgery center.
We use a two-page paper questionnaire to obtain basic information from patients, including (among other pertinent questions) age, planned operation, names of the surgeon and primary doctor, past operations and medical history, allergies, a list of medications, social history (drug, alcohol, tobacco use), whether they have ever taken steroids, whether they have high blood pressure, and whether they can comfortably walk up a flight of stairs. We provide the primary care physicians and surgeons with blank questionnaires, which their patients can fill out in their waiting rooms or take home and fax to us (or drop off) later. The questionnaire gives us a good deal of essential information without using staff time.
Various computer-based and Web-based systems are also available for collecting basic patient information. Smaller institutions need not purchase an entire electronic medical record system, which can be very expensive. Some Web-based tools operate on a pay-per-use basis and can be very helpful.
Review the information to guide triage
We then review the patient information to determine the extent of preoperative evaluation required. Some patients, especially those scheduled at an ambulatory surgery center, are healthy enough that they can just come in on the day of surgery for an examination and an update of their information. Others will need an appointment at the clinic before the day of surgery for more extensive preoperative evaluation. For other patients, review of their questionnaire responses may prompt a phone call or e-mail from the clinic for more information to determine whether a day-of-surgery exam will suffice or whether evaluation in advance is needed. When in doubt, concerns raised by the questionnaire should be explored before the day of surgery to avoid surprises and allow sufficient time for a consultation, if needed.
STANDARDIZED GUIDELINES KEEP CARE CONSISTENT
We encourage our staff to minimize preoperative testing and ECGs. A majority of diagnoses are made based on the history and physical exam.2 Generally, a test should confirm what is already suspected and merely provide objective evidence when needed. Testing in this setting should not be done to “find out what is wrong” with a patient.
It is helpful to develop standardized guidelines for preoperative assessment and make them available to everyone in the institution via the Web. The guidelines should address recommended preoperative tests and management practices according to specific patient conditions or surgical procedures. The clear objective is to avoid disagreement about what a patient needs between the provider who evaluated the patient in advance and the surgeon or anesthesiologist who evaluates the patient on the day of surgery.
Our guidelines at the University of Chicago include recommendations for patients on long-term anticoagulant therapy, for patients with coronary stents, for medications that should be discontinued (and those that may be continued) on the day of surgery, and for numerous other conditions and issues. Our testing guidelines list indicated tests for various medical problems, which in turn link to other guidelines. Other links are based on the medications a patient is using or the type of operation that is planned.
We collaborated with our electrophysiology department to create guidelines for managing patients with pacemakers and defibrillators. Almost every patient with one of these devices has a little card associated with the device, and we ask the surgeons to copy the card and send it to the clinic if we will not be directly seeing the patient. Using a national database, the electrophysiology department can determine from the card the type of pacemaker or defibrillator a patient has, and they fax or e-mail us back a page of instructions to let us know whether the device requires special consideration during surgery, whether it should be checked preoperatively, and whether its battery needs replacing. With this system, we have markedly reduced problems on the day of surgery.
CONSULTS HAVE AN IMPORTANT ROLE
Consults should never be requested in order to “clear a patient for surgery.” Consult requests should rather address specific issues, such as, “Is this patient medically optimized?” or “Please address this patient’s hypertension.” In turn, consult notes should provide meaningful information that can be used in a specific way. A clearance letter or simple risk assessment is not helpful.
If a patient has not seen a primary care doctor in a long time, a consult request should (in addition to requesting a global risk assessment) specify any particular concerns, such as, “The patient reports snoring; please address sleep apnea and cardiac risk.”
Case study: Beware consult notes with no specifics
Consider a case we encountered of a 54-year-old man who had a preoperative cardiac risk assessment. The cardiology consultant completed a short form consisting of a multiple-choice check-off list indicating low, moderate, or high cardiac risk. The consultant checked that the patient had low cardiac risk but provided no other instructions or information other than his own contact information.
When we reviewed the patient’s questionnaire, we saw that his medications included metoprolol, clopidogrel, and aspirin even though the patient did not mention that he had coronary artery disease. On this basis, we requested details about his cardiac evaluation from his cardiologist. It turned out that the patient had a history of four catheterizations with several cardiac stents placed. The most recent stent was implanted to overlap a previous stent that had been found “floating” in the blood vessel; this last stent was placed just 6 months before the cardiologist issued the consult note indicating “low cardiac risk.”
The moral is to approach consult notes with caution, especially if they offer no specifics. It actually makes me nervous when a note states “low risk” because if something unexpectedly goes wrong in surgery, it appears that the perioperative team took poor care of the patient even if the complication actually may have stemmed from higher-than-recognized underlying patient risk.
PROVIDE, AND REINFORCE, CLEAR INSTRUCTIONS
We give patients written preoperative instructions that become part of our computerized records. We first verbally give explicit instructions for each medication—ie, whether it can be taken as usual or when it needs to be stopped before surgery (and why). Then we provide the same information in writing, after which we try to have the patient repeat the instructions back to the clinician. We include a phone number that patients can call if they need help understanding their preoperative instructions.
Web-based programs also can provide patients online instructions about their medications. Some services even customize information by providing, for example, lists of local surgeons who are willing to allow a patient to continue on aspirin therapy until the day of surgery.
USE THE RIGHT RESOURCES
Staffing
Our model at the University of Chicago relies mainly on residents in training and physician assistants, but advanced nurse practitioners are well suited to a preoperative clinic as well. These types of providers have background training in history-taking, physical examination, diagnostic testing, and disease management. Registered nurses have more limited abilities, although they may be appropriate for a clinic that deals primarily with healthy patients for whom only history taking and a list of medications is needed. Additionally, our clinic is staffed by one attending anesthesiologist at all times (from among a group of rotating anesthesiologists) as well as medical assistants and clerical staff.
Some clinics perform the surgical history and physical exam at the same time as the anesthesia assessment. I would urge caution with this practice. Just as primary care doctors should not be conducting the anesthesia assessment, nonsurgeons should not be conducting the surgical assessment; doing so puts them out on a limb from a medicolegal standpoint. Advanced nurse practitioners and physician assistants may do surgical assessments under the supervision of a surgeon, but only surgeons should ultimately decide—and document—whether an operation is necessary and what degree of examination is required in advance.
Computer technology for records, messaging, billing
Using electronic medical records and corresponding with colleagues by e-mail make preoperative care much more efficient. We have standardized computer forms for ordering tests and documenting the physical exam. Patients usually understand that electronic medical records are safe and more efficient, and they are often more accepting of their use than practitioners are. Many patients want e-mail access to doctors, to schedule appointments online, and to receive appointment reminders by e-mail.3
Electronic medical records also avoid redundancy. If a patient has been seen in our preoperative clinic and is later scheduled for another surgery (even if a different surgeon is involved), a return visit to our clinic may not be necessary. In some cases, we can send the old work-up stamped “For information only,” which can then be updated by the anesthesiologist on the day of surgery.
A central, standardized process also makes billing more efficient and helps to ensure that payment is received for all services provided. Standardized documentation makes it easier for coders to enter the correct evaluation and management codes and ensures that all required criteria are met.
THE PAYOFF: LIVES AND DOLLARS SAVED
A thorough and efficient preoperative assessment system is cost-effective. Every minute of operating room time is worth $10 to $15,4,5 so delays should be avoided. Everything that is done ahead of time saves money for the whole enterprise by reducing unnecessary case setups and reducing “down time” due to lack of patient, equipment, or staff readiness. We routinely bill for preoperative evaluations when this service goes beyond a routine preoperative assessment based on CMS (and other insurance) requirements. However, a preoperative evaluation is required by CMS and most payers if one wants to be paid for any anesthesia-provided service. As a result, a cost is incurred without offsetting revenue if a case is cancelled on the day of surgery after one performs the anesthesia evaluation.
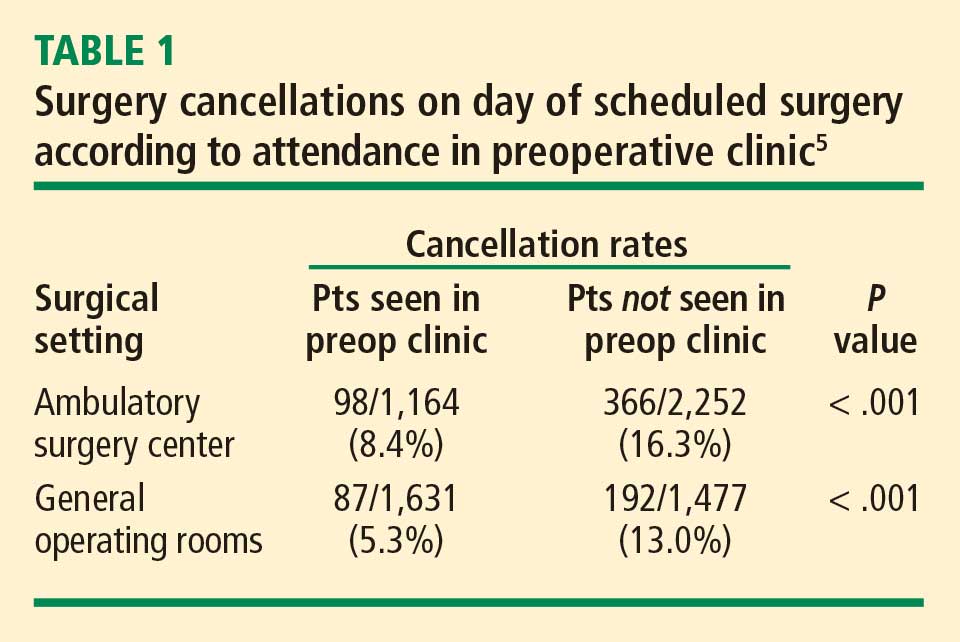
Yesterday I heard someone ask, “Do we really need all this preoperative evaluation? Does it really improve outcomes?” There is some evidence that it does. A study from 2000 based on data from the Australian Incident Monitoring Study found that 11% of the 6,271 critical incidents that occurred following operations were attributable to inadequate preoperative evaluation and that 3% were unequivocally related to problems with preoperative assessment or preparation. More than half of the incidents were deemed preventable.6
Preoperative clinics are good for patients and make good sense economically. We just need to demonstrate to our administrators and to payers that we are offering an excellent service.
Cleveland Clinic IMPACT Center
By Ajay Kumar, MD
Cleveland Clinic is structured differently from most other institutions in that its surgeons, anesthesiologists, and hospitalists are all direct employees of the institution. Despite this unique structure, many aspects of our preoperative clinic—known as the Internal Medicine Preoperative Assessment, Consultation and Treatment (IMPACT) Center—are applicable to other institutions.
Cleveland Clinic is a busy surgical hospital whose preoperative optimization system is designed to provide high-quality care. The IMPACT Center is consulted for most complicated noncardiac surgery patients, and its referral sources include most of the institution’s surgical specialties.
QUEST FOR A BETTER PATIENT EXPERIENCE
When the IMPACT Center was created in 1997, the aim was to focus on the same objectives highlighted by Drs. Bader and Sweitzer: safety, a positive patient experience, enhanced communication, better continuity of care, effective use of resources, and improving throughput by standardizing care.
A prime motivator was the desire to move away from the tendency for presurgical consults to simply “clear the patient for surgery,” and we have indeed evolved considerably from that point. The focus of our perioperative care program today is to comprehensively evaluate risk by taking into account patient-, procedure-, and anesthesia-related factors.
We offer “one-stop shopping,” and our priority is for efficient throughput. We are located in a 12-story building that includes outpatient, preoperative, and surgical clinics and offices. The IMPACT Center is on the first floor along with the preoperative anesthesia consultation and evaluation (PACE) clinic, the laboratory, and ECG and stress-test labs. Patients can undergo radiographic studies on the second floor.
The patient experience counts for a lot. Many of our patients are from another state or country, so efficiency and convenience are especially important. Patients can usually get all assessment and testing done in a single day.
A TIGHTLY MANAGED PROCESS
A ‘smart’ questionnaire starts the process
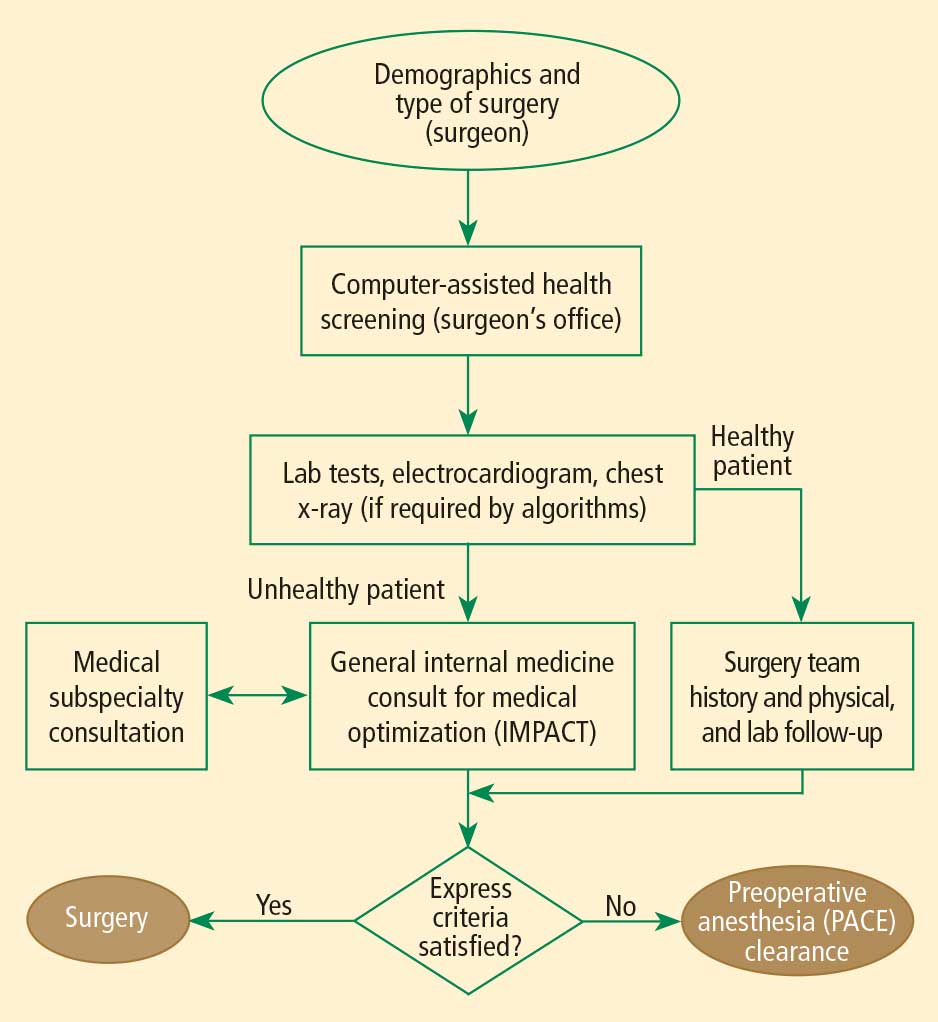
A computerized report based on the questionnaire guides the surgical office in scheduling the patient to specific areas according to algorithms. Based on case complexity and clinical needs, patients are scheduled for the IMPACT Center along with the PACE clinic; if needed (based on the algorithms), patients also are scheduled for laboratory tests or imaging. This standardized approach helps create a safe passage for patients through the preoperative process with less confusion.
Patient is given a personalized binder
Once all appointments and tests are scheduled, the patient is given a binder containing specific information about the procedure and preoperative instructions. The medical appointment at the IMPACT Center is usually scheduled before the PACE clinic appointment. Patients receive an itinerary for all preoperative appointments and surgical office appointments before the planned surgery. The itinerary is planned so that if additional testing is requested, it can be accommodated on the same day.
At the end of the preoperative assessment, the patient receives printed information with specific preoperative instructions, including which medications to continue or stop.
Standardized, computer-based medical records
Our systems and processes have undergone a good deal of evolution. We have integrated our medical records and use a standard outside medical record retrieval process. The template for the history and physical exam is standard for all Cleveland Clinic patients and is used for all presurgical assessments before all noncardiac surgeries. The template is comprehensive, including the history of the present illness, the review of systems, the physical exam, and anesthesia-related issues. All outside documents are scanned into our electronic medical record system and are available for viewing prior to surgery from any computer connected to the system.
Our preoperative assessment guidelines are also kept updated at a central online location so that all providers have access to them.
Staff keeps process running efficiently
The IMPACT Center is managed by the department of hospital medicine and supported by at least 5.5 full-time physicians every day. We also have two registered nurses, two assistants who help with scheduling and testing, and three secretaries who support the doctors, obtain records, and make arrangements with outside doctors for testing if a patient wants to return home before our testing can be completed.
A secretary also keeps a log for each patient seen in the clinic, tracking all pending issues. The day before surgery, the secretary contacts the appropriate office for anything that is still pending. If she gets no response, the matter is transferred to one of our doctors so that the problem can be resolved at once. This strategy allows us to achieve a nearly 0% rate of surgery delay or cancellation attributable to unavailable test results.
Our patient volumes have increased significantly since we started in 1997. Last year more than 15,000 patients visited the IMPACT Center and now we have expanded our services to regional hospitals within the Cleveland Clinic Health System.
INTERDEPARTMENTAL COMMUNICATION IS CRITICAL
Interdepartmental communication is a must for patient safety, so we encourage a culture of communication between the hospitalist and the surgical team. The location of most of our surgical clinics within the same building as the IMPACT Center further facilitates communication, as does the proximity of the PACE clinic. Additionally, one of our IMPACT Center physicians is accessible around the clock to answer to our surgeon or anesthesiologist colleagues as needed.
We regularly assess our process and seek feedback from surgeons and anesthesiologists. We also conduct yearly patient experience surveys to make sure we are providing patients with the highest quality of care.
Discussion
Question from the audience: Our anesthesia assessment department was approached by our surgeons to do both the anesthesia and surgical assessments, but we felt that would put us in a potential legal conflict if a patient who was assessed that way developed problems. Can you comment?
Dr. Bader: Although we do surgical assessments at our preoperative clinic, we don’t make any decisions about whether or not to proceed with an operation. We get an office note from the surgeon that is directed specifically toward the need for surgery, indications for surgery, and surgical consent. We perform the surgical history and physical examination. Our process is essentially the same as when surgeons have a physician assistant do the history and physical examination in their office. Our practitioners are employed by the hospital, so there is no conflict of interest there.
Comment from the audience: I’m a strong believer in hands-on patient contact. Over my 15 years of practice, we have encountered a lot of unexpected problems during the preoperative exam—aortic stenoses, infections, ventricular septal defects—all of which would never have been detected from a screening form.
Dr. Sweitzer: I agree that we pick up many things by seeing the patient in person. I’ve picked up more cases of aortic stenosis as an anesthesiologist in the preoperative clinic than I ever did as an internist, because the population is high-risk. But patients who have such problems tend to have risk factors and be in certain age groups. Studies indicate that the history is more important than the physical exam: the history suggests about 75% of conditions that are present. The physical exam adds only a little more—perhaps another 15%. Our recommendations are very much consistent with the American College of Cardiology and American Heart Association guidelines on preoperative cardiac evaluation.7 It is more important to identify whether a patient has risk factors for coronary artery disease than to find out whether a stress test or ECG is normal. One needs to do a really good history, but it can be done remotely. Based on certain risk factors identified, high-risk patients can be selected who need to come in and have a physical exam.
Question from the audience: Could you elaborate on the electronic medical record system used at the University of Chicago? I’ve heard there’s a steep learning curve when implementing these kinds of systems. They also are very expensive—I’ve heard that some cost $40 to $80 million. Has enhanced revenue flow offset the costs?
Dr. Sweitzer: We have a home-grown system developed with FileMaker Pro by a computer programmer at our institution. It was a lot easier to develop than people tend to think. There are many savvy computer programmers out there; I’ve had medical students assist me with updating it. We’re now considering developing it as a commercial system. Many systems are available for purchase, including Epic, Pyxis, one from General Electric, and many others. They are very expensive, so smaller institutions might want to use a pay-for-service system.
There definitely is a learning curve to switching to electronic medical records, but it is not nearly as steep as many believe. The extra time it takes a clinician to initially make a computer entry rather than write on paper is vastly recouped downstream: the electronic medical record is legible and organized, and it doesn’t get lost or need to be redone. You can bring up a patient record from 6 months before and reuse it as a template.
Dr. Bader: The discussion of cost savings from preoperative clinics usually focuses on savings from avoiding surgery cancellations and delays and from more efficient laboratory testing, but the biggest savings for an institution is better reimbursement through better diagnosis-related groups (DRG) coding. That’s an important reason our institution is funding our clinic. Electronic medical records allow standardization of information so that coders know exactly where to look for the comorbidities and other pertinent information. This increases payments for DRGs, which can be documented for the hospital. This literally runs into millions of dollars a year and more than offsets the costs of the system.
Question from the audience: Dr. Bader, I’m impressed with the number of patients going through your preoperative clinic. How many patients are seen per nurse practitioner in your clinic?
Dr. Bader: The nurse practitioners have 10-hour shifts and see one patient every 75 minutes. The process of seeing a patient takes a lot less time now than with the old system, in which patients saw an anesthesiologist plus a nurse. Our current system eliminates redundancy: questions need to be asked only once.
Question from the audience: My compliance office says that preoperative assessments for early-morning admission patients are good for only 7 days. Is that true?
Dr. Bader: There are sometimes differences between Joint Commission requirements and those of certain insurance companies. That kind of issue needs to be discussed with your hospital compliance office. We program rules into our scheduling system to accommodate different insurance policies and other requirements so that a patient is not scheduled beyond the allowable period.
- Detsky AS, Naglie IG. A clinician’s guide to cost-effectiveness analysis. Ann Intern Med 1990; 113:147–154.
- Sandler G. The importance of the history in the medical clinic and the cost of unnecessary tests. Am Heart J 1980; 100:928–931.
- Blumenthal D, Glaser JP. Information technology comes to medicine. N Engl J Med 2007; 356:2527–2534.
- Strum DP, Vargas LG, May JH. Surgical subspecialty block utilization and capacity planning: a minimal cost analysis model. Anesthesiology 1999; 90:1176–1185.
- Ferschl MB, Tung A, Sweitzer B, Huo D, Glick DB. Preoperative clinic visits reduce operating room cancellations and delays. Anesthesiology 2005; 103:855–859.
- Kluger MT, Tham EJ, Coleman NA, et al. Inadequate preoperative evaluation and preparation: a review of 197 reports from the Australian incident monitoring study. Anaesthesia 2000; 55:1173–1178.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2007; 50:1707–1732.
Weiner Center for Preoperative Evaluation at Brigham and Women’s Hospital
By Angela M. Bader, MD, MPH
When organizing our preoperative clinic at Brigham and Women’s Hospital, we had several goals. Overall, we wanted a standardized process to help us achieve a high level of excellence. We hoped that creating a new system would eliminate ambiguity about who was responsible for following up on a patient’s abnormal laboratory test result—the surgeon, anesthesiologist, or primary care physician. We also wanted to better coordinate the various care teams involved throughout the perioperative period.
STANDARDIZATION HELPS MEET MANY GOALS
Standardization can occur at many levels:
- Performance of assessments and testing
- Organization of the patient chart and medical records
- Systems checks throughout the process to ensure that nothing is missed
- Team-to-team communication.
Documentation requirements apply regardless of institutional structure
When considering any system of preoperative assessment, keep in mind that the hospital must meet and appropriately document compliance with all regulatory, accreditation, and payer requirements and guidelines, such as those of the Joint Commission, the Centers for Medicare and Medicaid Services (CMS), and the National Surgical Quality Improvement Program. For example, the Joint Commission requires that a surgical history and physical examination be done within 30 days of a procedure. An anesthesiology assessment and a nursing assessment are also required. All of these assessments have mandatory elements, including documenting “never events” and ordering appropriate laboratory tests, electrocardiograms (ECGs), and radiographs.
Sometimes administrators of other hospitals say to me, “We can’t afford a preoperative clinic, and we don’t need one.” My response is that regardless of whether a hospital has a preoperative clinic, the regulatory requirements and guidelines must be met: it is not an issue of avoiding certain steps. Having a dedicated preoperative clinic simply shifts the work to a standardized, centralized system and avoids delaying these required steps until the day of surgery, when taking care of a problem involves the most inefficient use of resources.
Tailor system to institutional needs and characteristics
Within the regulatory framework, the organizational scheme of every institution must address issues of volume and acuity, the types of surgery performed, and the time frames required. A system must be able to deal with the preoperative needs of patients undergoing operations that are booked weeks in advance (often the case for orthopedic surgery) as well as those that may not be booked until a day before the procedure (eg, cancer surgery).
Our plan was developed for our very high-volume, tertiary care institution. In 2008, 24,000 patients used our clinic (roughly 100 patients per day).
DESIGN OF THE PREOPERATIVE CLINIC
A nurse practitioner–based model for ‘one-stop shopping’
We decided that the clinic should offer all elements of the preoperative assessment and thereby give patients “one-stop shopping.” Each patient sees a nurse practitioner, who performs the surgical history and physical examination as well as the anesthesiology and nursing assessments. The result is a multidisciplinary approach with a single assessment output. We shifted employees who had been responsible for preoperative assessment in the offices of various surgeons to a central clinic so that all assessments could be standardized, and we provided additional training to enable them to perform various assessments. The nurse practitioners are supervised by an on-site attending physician, as detailed below.
This model offers a number of advantages:
- Patients see a single provider.
- Assessment is facilitated for our surgeons, who may not be completely up-to-date on perioperative risk assessment and management.
- We have a central location for standardized education programs for our physicians, nurses, and residents.
- The clinic’s standardized records and processes facilitate data generation for research and clinical practice improvement.
Independent budgetary and staffing structure
The preoperative clinic is a separate cost center under the leadership of the department of anesthesiology. Resources were shifted to a central location so that as volume increases, we can add resources to meet the additional volume. We contracted with the hospital administration to provide payment for two full-time-equivalent anesthesiologists per day, who serve as on-site attending physicians. The hospital is willing to do this because not only do these attending physicians supervise the anesthesiology assessment, they are the collaborating physicians for the entire perioperative assessment. They review every patient, order tests and write prescriptions as needed, and discuss issues with the primary care physicians and referring specialists.
The preoperative clinic has an anesthesiologist director (me) who reports directly to the hospital’s vice president for surgical services on budget and staffing issues. I also report to the chairman of the department of anesthesiology, though he is not involved in budgetary functions (the hospital contracts with him to provide the anesthesiology staffing). The clerical and nursing staff work directly for the clinic.
The clinic is run in a self-contained area with a central waiting room and space for doing all the assessments and laboratory work internally, including 16 examination rooms and a room for chart organization.
MORE BENEFITS OF STANDARDIZATION
Standardized scheduling ensures reliability
The secretaries in each surgeon’s office schedule appointments through a central computer system after registration and insurance precertification. Our computer system does not allow an operation to be scheduled without an evaluation also being scheduled. The evaluation can involve either a visit or a telephone screen; we provide algorithms so that the surgeons’ secretaries know which is required. This system has substantially reduced the number of walk-ins, allowing for a more even distribution of patients and ensuring that medical records will be available when a patient is seen.
We watch our schedule carefully. Our computer system monitors the time that each patient is in our clinic to determine his or her waiting time and assessment time. It takes about 75 minutes to go through the whole process, including the time for a nurse practitioner to do the surgical history and physical examination and the anesthesiology and nursing assessments, a laboratory technician to do an ECG and laboratory tests if indicated, and completion of all required documentation. Accordingly, patients are scheduled in 75-minute blocks between 7:00 am and 6:30 pm. We do not have evening or weekend hours because of the difficulty of contacting surgeons and primary care physicians when questions arise. It is simply not cost-effective to have to do that type of follow-up on a case after the patient leaves.
Only about 10% of our patients are screened by telephone, since most of our operations are complicated and require in-person assessment (most low-acuity procedures are done at other hospitals). Of the patients who visit the preoperative clinic, about 75% undergo the single assessment model for surgery, anesthesiology, and nursing as described above. The remaining 25% of patients have their history and physical exam completed outside Brigham and Women’s Hospital for insurance reasons; the remainder of their assessment is conducted in our preoperative clinic by a registered nurse and an anesthesiology resident.
Multiple systems checks
Our model also incorporates standardization in the form of multiple systems checks:
- Case presentation. Every case is presented to an attending anesthesiologist, who reviews the ECG (if ordered) before the patient leaves the clinic.
- Post-visit chart check. A registered nurse or nurse practitioner signs off on each chart after the visit, confirming test results and resolution of all paperwork issues.
- Surgical checklist. The end result is a checklist that serves as the front sheet of the operating room chart.
Our ability to use this system of checks to get the chart completed comprehensively and reliably and deliver it to the operating room when needed was key to securing institutional support and funding for the preoperative clinic.
ROLE OF THE ATTENDING ANESTHESIOLOGISTS
Two full-time attending anesthesiologists are present in the preoperative clinic each day. One is responsible largely for supervising the nurse practitioner assessments and reviewing case presentations, while the other also oversees the education and supervision of residents. Residents rotate through the clinic for 2 weeks (one or two at a time) and have a designated curriculum consisting of daily lectures and competencies in preoperative evaluation.
Because our anesthesiologists are expert in preoperative assessment, we require very few outside consults. We can communicate directly with the cardiologists and other physicians and order tests when indicated. We have a clerical assistant who obtains all necessary paperwork and prior testing from outside providers so that the clinicians need not waste time on this.
A GROWING CHALLENGE: ASSESSMENT FOR PROCEDURES IN AMBULATORY SETTINGS
Looking forward, a rapidly growing challenge facing our clinic stems from the tremendous growth in patients who require anesthesia for procedures performed outside the operating room. In these situations, the proceduralists need a system for deciding whether an anesthesiologist must be present for any given case.
We have started to develop appropriate screening processes to ensure that the proceduralists in multiple departments know which patients to refer for preprocedure assessment. We hope to soon develop protocols for high-risk patients and for various procedures such as implanting a pacemaker or defibrillator, catheter procedures, interventional radiology, and endoscopy.
Anesthesia Perioperative Medicine Clinic at University of Chicago
By BobbieJean Sweitzer, MD
Detsky and Naglie have argued that the costs and clinical outcomes associated with any intervention must be compared with those of alternate strategies for treating the same patients,1 and I believe their point applies well to preoperative clinics. Although certain requirements of the Joint Commission and CMS must be met, as noted by Dr. Bader, they can be met in various ways. I will preface my comments by emphasizing that one size does not fit all: every institution must decide the best approach to preoperative assessment based on its patient population, the types of procedures it performs, and the volume it handles.
TRIAGE STREAMLINES THE PROCESS
Our preoperative clinic at the University of Chicago emphasizes triage. Not every patient should have to go to the trouble of coming in to see a provider. In the future, we will likely see more “virtual” preoperative assessments using devices in development, such as handheld ultrasonography machines. Just as patients can have their pacemakers and implantable cardiac defibrillators remotely checked via phone contact, more tools will one day be available for remote assessment.
Although not every surgical patient needs to come in to the preoperative clinic, every patient must have a physical examination. All patients will be seen on the day of surgery, so in some cases the physical exam may be able to wait until then. For example, an airway assessment need not be done ahead of time. Most anesthesiologists are prepared to manage airways on very short notice, so extensive advance planning is not always necessary.
Obtain basic info by questionnaire to save staff time
Information about the patient is key to triage, and it may be either paper- or computer-based. An initial priority should be to develop some mechanism for getting information from patients before the day of their procedure without a visit to the hospital or ambulatory surgery center.
We use a two-page paper questionnaire to obtain basic information from patients, including (among other pertinent questions) age, planned operation, names of the surgeon and primary doctor, past operations and medical history, allergies, a list of medications, social history (drug, alcohol, tobacco use), whether they have ever taken steroids, whether they have high blood pressure, and whether they can comfortably walk up a flight of stairs. We provide the primary care physicians and surgeons with blank questionnaires, which their patients can fill out in their waiting rooms or take home and fax to us (or drop off) later. The questionnaire gives us a good deal of essential information without using staff time.
Various computer-based and Web-based systems are also available for collecting basic patient information. Smaller institutions need not purchase an entire electronic medical record system, which can be very expensive. Some Web-based tools operate on a pay-per-use basis and can be very helpful.
Review the information to guide triage
We then review the patient information to determine the extent of preoperative evaluation required. Some patients, especially those scheduled at an ambulatory surgery center, are healthy enough that they can just come in on the day of surgery for an examination and an update of their information. Others will need an appointment at the clinic before the day of surgery for more extensive preoperative evaluation. For other patients, review of their questionnaire responses may prompt a phone call or e-mail from the clinic for more information to determine whether a day-of-surgery exam will suffice or whether evaluation in advance is needed. When in doubt, concerns raised by the questionnaire should be explored before the day of surgery to avoid surprises and allow sufficient time for a consultation, if needed.
STANDARDIZED GUIDELINES KEEP CARE CONSISTENT
We encourage our staff to minimize preoperative testing and ECGs. A majority of diagnoses are made based on the history and physical exam.2 Generally, a test should confirm what is already suspected and merely provide objective evidence when needed. Testing in this setting should not be done to “find out what is wrong” with a patient.
It is helpful to develop standardized guidelines for preoperative assessment and make them available to everyone in the institution via the Web. The guidelines should address recommended preoperative tests and management practices according to specific patient conditions or surgical procedures. The clear objective is to avoid disagreement about what a patient needs between the provider who evaluated the patient in advance and the surgeon or anesthesiologist who evaluates the patient on the day of surgery.
Our guidelines at the University of Chicago include recommendations for patients on long-term anticoagulant therapy, for patients with coronary stents, for medications that should be discontinued (and those that may be continued) on the day of surgery, and for numerous other conditions and issues. Our testing guidelines list indicated tests for various medical problems, which in turn link to other guidelines. Other links are based on the medications a patient is using or the type of operation that is planned.
We collaborated with our electrophysiology department to create guidelines for managing patients with pacemakers and defibrillators. Almost every patient with one of these devices has a little card associated with the device, and we ask the surgeons to copy the card and send it to the clinic if we will not be directly seeing the patient. Using a national database, the electrophysiology department can determine from the card the type of pacemaker or defibrillator a patient has, and they fax or e-mail us back a page of instructions to let us know whether the device requires special consideration during surgery, whether it should be checked preoperatively, and whether its battery needs replacing. With this system, we have markedly reduced problems on the day of surgery.
CONSULTS HAVE AN IMPORTANT ROLE
Consults should never be requested in order to “clear a patient for surgery.” Consult requests should rather address specific issues, such as, “Is this patient medically optimized?” or “Please address this patient’s hypertension.” In turn, consult notes should provide meaningful information that can be used in a specific way. A clearance letter or simple risk assessment is not helpful.
If a patient has not seen a primary care doctor in a long time, a consult request should (in addition to requesting a global risk assessment) specify any particular concerns, such as, “The patient reports snoring; please address sleep apnea and cardiac risk.”
Case study: Beware consult notes with no specifics
Consider a case we encountered of a 54-year-old man who had a preoperative cardiac risk assessment. The cardiology consultant completed a short form consisting of a multiple-choice check-off list indicating low, moderate, or high cardiac risk. The consultant checked that the patient had low cardiac risk but provided no other instructions or information other than his own contact information.
When we reviewed the patient’s questionnaire, we saw that his medications included metoprolol, clopidogrel, and aspirin even though the patient did not mention that he had coronary artery disease. On this basis, we requested details about his cardiac evaluation from his cardiologist. It turned out that the patient had a history of four catheterizations with several cardiac stents placed. The most recent stent was implanted to overlap a previous stent that had been found “floating” in the blood vessel; this last stent was placed just 6 months before the cardiologist issued the consult note indicating “low cardiac risk.”
The moral is to approach consult notes with caution, especially if they offer no specifics. It actually makes me nervous when a note states “low risk” because if something unexpectedly goes wrong in surgery, it appears that the perioperative team took poor care of the patient even if the complication actually may have stemmed from higher-than-recognized underlying patient risk.
PROVIDE, AND REINFORCE, CLEAR INSTRUCTIONS
We give patients written preoperative instructions that become part of our computerized records. We first verbally give explicit instructions for each medication—ie, whether it can be taken as usual or when it needs to be stopped before surgery (and why). Then we provide the same information in writing, after which we try to have the patient repeat the instructions back to the clinician. We include a phone number that patients can call if they need help understanding their preoperative instructions.
Web-based programs also can provide patients online instructions about their medications. Some services even customize information by providing, for example, lists of local surgeons who are willing to allow a patient to continue on aspirin therapy until the day of surgery.
USE THE RIGHT RESOURCES
Staffing
Our model at the University of Chicago relies mainly on residents in training and physician assistants, but advanced nurse practitioners are well suited to a preoperative clinic as well. These types of providers have background training in history-taking, physical examination, diagnostic testing, and disease management. Registered nurses have more limited abilities, although they may be appropriate for a clinic that deals primarily with healthy patients for whom only history taking and a list of medications is needed. Additionally, our clinic is staffed by one attending anesthesiologist at all times (from among a group of rotating anesthesiologists) as well as medical assistants and clerical staff.
Some clinics perform the surgical history and physical exam at the same time as the anesthesia assessment. I would urge caution with this practice. Just as primary care doctors should not be conducting the anesthesia assessment, nonsurgeons should not be conducting the surgical assessment; doing so puts them out on a limb from a medicolegal standpoint. Advanced nurse practitioners and physician assistants may do surgical assessments under the supervision of a surgeon, but only surgeons should ultimately decide—and document—whether an operation is necessary and what degree of examination is required in advance.
Computer technology for records, messaging, billing
Using electronic medical records and corresponding with colleagues by e-mail make preoperative care much more efficient. We have standardized computer forms for ordering tests and documenting the physical exam. Patients usually understand that electronic medical records are safe and more efficient, and they are often more accepting of their use than practitioners are. Many patients want e-mail access to doctors, to schedule appointments online, and to receive appointment reminders by e-mail.3
Electronic medical records also avoid redundancy. If a patient has been seen in our preoperative clinic and is later scheduled for another surgery (even if a different surgeon is involved), a return visit to our clinic may not be necessary. In some cases, we can send the old work-up stamped “For information only,” which can then be updated by the anesthesiologist on the day of surgery.
A central, standardized process also makes billing more efficient and helps to ensure that payment is received for all services provided. Standardized documentation makes it easier for coders to enter the correct evaluation and management codes and ensures that all required criteria are met.
THE PAYOFF: LIVES AND DOLLARS SAVED
A thorough and efficient preoperative assessment system is cost-effective. Every minute of operating room time is worth $10 to $15,4,5 so delays should be avoided. Everything that is done ahead of time saves money for the whole enterprise by reducing unnecessary case setups and reducing “down time” due to lack of patient, equipment, or staff readiness. We routinely bill for preoperative evaluations when this service goes beyond a routine preoperative assessment based on CMS (and other insurance) requirements. However, a preoperative evaluation is required by CMS and most payers if one wants to be paid for any anesthesia-provided service. As a result, a cost is incurred without offsetting revenue if a case is cancelled on the day of surgery after one performs the anesthesia evaluation.
Yesterday I heard someone ask, “Do we really need all this preoperative evaluation? Does it really improve outcomes?” There is some evidence that it does. A study from 2000 based on data from the Australian Incident Monitoring Study found that 11% of the 6,271 critical incidents that occurred following operations were attributable to inadequate preoperative evaluation and that 3% were unequivocally related to problems with preoperative assessment or preparation. More than half of the incidents were deemed preventable.6
Preoperative clinics are good for patients and make good sense economically. We just need to demonstrate to our administrators and to payers that we are offering an excellent service.
Cleveland Clinic IMPACT Center
By Ajay Kumar, MD
Cleveland Clinic is structured differently from most other institutions in that its surgeons, anesthesiologists, and hospitalists are all direct employees of the institution. Despite this unique structure, many aspects of our preoperative clinic—known as the Internal Medicine Preoperative Assessment, Consultation and Treatment (IMPACT) Center—are applicable to other institutions.
Cleveland Clinic is a busy surgical hospital whose preoperative optimization system is designed to provide high-quality care. The IMPACT Center is consulted for most complicated noncardiac surgery patients, and its referral sources include most of the institution’s surgical specialties.
QUEST FOR A BETTER PATIENT EXPERIENCE
When the IMPACT Center was created in 1997, the aim was to focus on the same objectives highlighted by Drs. Bader and Sweitzer: safety, a positive patient experience, enhanced communication, better continuity of care, effective use of resources, and improving throughput by standardizing care.
A prime motivator was the desire to move away from the tendency for presurgical consults to simply “clear the patient for surgery,” and we have indeed evolved considerably from that point. The focus of our perioperative care program today is to comprehensively evaluate risk by taking into account patient-, procedure-, and anesthesia-related factors.
We offer “one-stop shopping,” and our priority is for efficient throughput. We are located in a 12-story building that includes outpatient, preoperative, and surgical clinics and offices. The IMPACT Center is on the first floor along with the preoperative anesthesia consultation and evaluation (PACE) clinic, the laboratory, and ECG and stress-test labs. Patients can undergo radiographic studies on the second floor.
The patient experience counts for a lot. Many of our patients are from another state or country, so efficiency and convenience are especially important. Patients can usually get all assessment and testing done in a single day.
A TIGHTLY MANAGED PROCESS
A ‘smart’ questionnaire starts the process
A computerized report based on the questionnaire guides the surgical office in scheduling the patient to specific areas according to algorithms. Based on case complexity and clinical needs, patients are scheduled for the IMPACT Center along with the PACE clinic; if needed (based on the algorithms), patients also are scheduled for laboratory tests or imaging. This standardized approach helps create a safe passage for patients through the preoperative process with less confusion.
Patient is given a personalized binder
Once all appointments and tests are scheduled, the patient is given a binder containing specific information about the procedure and preoperative instructions. The medical appointment at the IMPACT Center is usually scheduled before the PACE clinic appointment. Patients receive an itinerary for all preoperative appointments and surgical office appointments before the planned surgery. The itinerary is planned so that if additional testing is requested, it can be accommodated on the same day.
At the end of the preoperative assessment, the patient receives printed information with specific preoperative instructions, including which medications to continue or stop.
Standardized, computer-based medical records
Our systems and processes have undergone a good deal of evolution. We have integrated our medical records and use a standard outside medical record retrieval process. The template for the history and physical exam is standard for all Cleveland Clinic patients and is used for all presurgical assessments before all noncardiac surgeries. The template is comprehensive, including the history of the present illness, the review of systems, the physical exam, and anesthesia-related issues. All outside documents are scanned into our electronic medical record system and are available for viewing prior to surgery from any computer connected to the system.
Our preoperative assessment guidelines are also kept updated at a central online location so that all providers have access to them.
Staff keeps process running efficiently
The IMPACT Center is managed by the department of hospital medicine and supported by at least 5.5 full-time physicians every day. We also have two registered nurses, two assistants who help with scheduling and testing, and three secretaries who support the doctors, obtain records, and make arrangements with outside doctors for testing if a patient wants to return home before our testing can be completed.
A secretary also keeps a log for each patient seen in the clinic, tracking all pending issues. The day before surgery, the secretary contacts the appropriate office for anything that is still pending. If she gets no response, the matter is transferred to one of our doctors so that the problem can be resolved at once. This strategy allows us to achieve a nearly 0% rate of surgery delay or cancellation attributable to unavailable test results.
Our patient volumes have increased significantly since we started in 1997. Last year more than 15,000 patients visited the IMPACT Center and now we have expanded our services to regional hospitals within the Cleveland Clinic Health System.
INTERDEPARTMENTAL COMMUNICATION IS CRITICAL
Interdepartmental communication is a must for patient safety, so we encourage a culture of communication between the hospitalist and the surgical team. The location of most of our surgical clinics within the same building as the IMPACT Center further facilitates communication, as does the proximity of the PACE clinic. Additionally, one of our IMPACT Center physicians is accessible around the clock to answer to our surgeon or anesthesiologist colleagues as needed.
We regularly assess our process and seek feedback from surgeons and anesthesiologists. We also conduct yearly patient experience surveys to make sure we are providing patients with the highest quality of care.
Discussion
Question from the audience: Our anesthesia assessment department was approached by our surgeons to do both the anesthesia and surgical assessments, but we felt that would put us in a potential legal conflict if a patient who was assessed that way developed problems. Can you comment?
Dr. Bader: Although we do surgical assessments at our preoperative clinic, we don’t make any decisions about whether or not to proceed with an operation. We get an office note from the surgeon that is directed specifically toward the need for surgery, indications for surgery, and surgical consent. We perform the surgical history and physical examination. Our process is essentially the same as when surgeons have a physician assistant do the history and physical examination in their office. Our practitioners are employed by the hospital, so there is no conflict of interest there.
Comment from the audience: I’m a strong believer in hands-on patient contact. Over my 15 years of practice, we have encountered a lot of unexpected problems during the preoperative exam—aortic stenoses, infections, ventricular septal defects—all of which would never have been detected from a screening form.
Dr. Sweitzer: I agree that we pick up many things by seeing the patient in person. I’ve picked up more cases of aortic stenosis as an anesthesiologist in the preoperative clinic than I ever did as an internist, because the population is high-risk. But patients who have such problems tend to have risk factors and be in certain age groups. Studies indicate that the history is more important than the physical exam: the history suggests about 75% of conditions that are present. The physical exam adds only a little more—perhaps another 15%. Our recommendations are very much consistent with the American College of Cardiology and American Heart Association guidelines on preoperative cardiac evaluation.7 It is more important to identify whether a patient has risk factors for coronary artery disease than to find out whether a stress test or ECG is normal. One needs to do a really good history, but it can be done remotely. Based on certain risk factors identified, high-risk patients can be selected who need to come in and have a physical exam.
Question from the audience: Could you elaborate on the electronic medical record system used at the University of Chicago? I’ve heard there’s a steep learning curve when implementing these kinds of systems. They also are very expensive—I’ve heard that some cost $40 to $80 million. Has enhanced revenue flow offset the costs?
Dr. Sweitzer: We have a home-grown system developed with FileMaker Pro by a computer programmer at our institution. It was a lot easier to develop than people tend to think. There are many savvy computer programmers out there; I’ve had medical students assist me with updating it. We’re now considering developing it as a commercial system. Many systems are available for purchase, including Epic, Pyxis, one from General Electric, and many others. They are very expensive, so smaller institutions might want to use a pay-for-service system.
There definitely is a learning curve to switching to electronic medical records, but it is not nearly as steep as many believe. The extra time it takes a clinician to initially make a computer entry rather than write on paper is vastly recouped downstream: the electronic medical record is legible and organized, and it doesn’t get lost or need to be redone. You can bring up a patient record from 6 months before and reuse it as a template.
Dr. Bader: The discussion of cost savings from preoperative clinics usually focuses on savings from avoiding surgery cancellations and delays and from more efficient laboratory testing, but the biggest savings for an institution is better reimbursement through better diagnosis-related groups (DRG) coding. That’s an important reason our institution is funding our clinic. Electronic medical records allow standardization of information so that coders know exactly where to look for the comorbidities and other pertinent information. This increases payments for DRGs, which can be documented for the hospital. This literally runs into millions of dollars a year and more than offsets the costs of the system.
Question from the audience: Dr. Bader, I’m impressed with the number of patients going through your preoperative clinic. How many patients are seen per nurse practitioner in your clinic?
Dr. Bader: The nurse practitioners have 10-hour shifts and see one patient every 75 minutes. The process of seeing a patient takes a lot less time now than with the old system, in which patients saw an anesthesiologist plus a nurse. Our current system eliminates redundancy: questions need to be asked only once.
Question from the audience: My compliance office says that preoperative assessments for early-morning admission patients are good for only 7 days. Is that true?
Dr. Bader: There are sometimes differences between Joint Commission requirements and those of certain insurance companies. That kind of issue needs to be discussed with your hospital compliance office. We program rules into our scheduling system to accommodate different insurance policies and other requirements so that a patient is not scheduled beyond the allowable period.
Weiner Center for Preoperative Evaluation at Brigham and Women’s Hospital
By Angela M. Bader, MD, MPH
When organizing our preoperative clinic at Brigham and Women’s Hospital, we had several goals. Overall, we wanted a standardized process to help us achieve a high level of excellence. We hoped that creating a new system would eliminate ambiguity about who was responsible for following up on a patient’s abnormal laboratory test result—the surgeon, anesthesiologist, or primary care physician. We also wanted to better coordinate the various care teams involved throughout the perioperative period.
STANDARDIZATION HELPS MEET MANY GOALS
Standardization can occur at many levels:
- Performance of assessments and testing
- Organization of the patient chart and medical records
- Systems checks throughout the process to ensure that nothing is missed
- Team-to-team communication.
Documentation requirements apply regardless of institutional structure
When considering any system of preoperative assessment, keep in mind that the hospital must meet and appropriately document compliance with all regulatory, accreditation, and payer requirements and guidelines, such as those of the Joint Commission, the Centers for Medicare and Medicaid Services (CMS), and the National Surgical Quality Improvement Program. For example, the Joint Commission requires that a surgical history and physical examination be done within 30 days of a procedure. An anesthesiology assessment and a nursing assessment are also required. All of these assessments have mandatory elements, including documenting “never events” and ordering appropriate laboratory tests, electrocardiograms (ECGs), and radiographs.
Sometimes administrators of other hospitals say to me, “We can’t afford a preoperative clinic, and we don’t need one.” My response is that regardless of whether a hospital has a preoperative clinic, the regulatory requirements and guidelines must be met: it is not an issue of avoiding certain steps. Having a dedicated preoperative clinic simply shifts the work to a standardized, centralized system and avoids delaying these required steps until the day of surgery, when taking care of a problem involves the most inefficient use of resources.
Tailor system to institutional needs and characteristics
Within the regulatory framework, the organizational scheme of every institution must address issues of volume and acuity, the types of surgery performed, and the time frames required. A system must be able to deal with the preoperative needs of patients undergoing operations that are booked weeks in advance (often the case for orthopedic surgery) as well as those that may not be booked until a day before the procedure (eg, cancer surgery).
Our plan was developed for our very high-volume, tertiary care institution. In 2008, 24,000 patients used our clinic (roughly 100 patients per day).
DESIGN OF THE PREOPERATIVE CLINIC
A nurse practitioner–based model for ‘one-stop shopping’
We decided that the clinic should offer all elements of the preoperative assessment and thereby give patients “one-stop shopping.” Each patient sees a nurse practitioner, who performs the surgical history and physical examination as well as the anesthesiology and nursing assessments. The result is a multidisciplinary approach with a single assessment output. We shifted employees who had been responsible for preoperative assessment in the offices of various surgeons to a central clinic so that all assessments could be standardized, and we provided additional training to enable them to perform various assessments. The nurse practitioners are supervised by an on-site attending physician, as detailed below.
This model offers a number of advantages:
- Patients see a single provider.
- Assessment is facilitated for our surgeons, who may not be completely up-to-date on perioperative risk assessment and management.
- We have a central location for standardized education programs for our physicians, nurses, and residents.
- The clinic’s standardized records and processes facilitate data generation for research and clinical practice improvement.
Independent budgetary and staffing structure
The preoperative clinic is a separate cost center under the leadership of the department of anesthesiology. Resources were shifted to a central location so that as volume increases, we can add resources to meet the additional volume. We contracted with the hospital administration to provide payment for two full-time-equivalent anesthesiologists per day, who serve as on-site attending physicians. The hospital is willing to do this because not only do these attending physicians supervise the anesthesiology assessment, they are the collaborating physicians for the entire perioperative assessment. They review every patient, order tests and write prescriptions as needed, and discuss issues with the primary care physicians and referring specialists.
The preoperative clinic has an anesthesiologist director (me) who reports directly to the hospital’s vice president for surgical services on budget and staffing issues. I also report to the chairman of the department of anesthesiology, though he is not involved in budgetary functions (the hospital contracts with him to provide the anesthesiology staffing). The clerical and nursing staff work directly for the clinic.
The clinic is run in a self-contained area with a central waiting room and space for doing all the assessments and laboratory work internally, including 16 examination rooms and a room for chart organization.
MORE BENEFITS OF STANDARDIZATION
Standardized scheduling ensures reliability
The secretaries in each surgeon’s office schedule appointments through a central computer system after registration and insurance precertification. Our computer system does not allow an operation to be scheduled without an evaluation also being scheduled. The evaluation can involve either a visit or a telephone screen; we provide algorithms so that the surgeons’ secretaries know which is required. This system has substantially reduced the number of walk-ins, allowing for a more even distribution of patients and ensuring that medical records will be available when a patient is seen.
We watch our schedule carefully. Our computer system monitors the time that each patient is in our clinic to determine his or her waiting time and assessment time. It takes about 75 minutes to go through the whole process, including the time for a nurse practitioner to do the surgical history and physical examination and the anesthesiology and nursing assessments, a laboratory technician to do an ECG and laboratory tests if indicated, and completion of all required documentation. Accordingly, patients are scheduled in 75-minute blocks between 7:00 am and 6:30 pm. We do not have evening or weekend hours because of the difficulty of contacting surgeons and primary care physicians when questions arise. It is simply not cost-effective to have to do that type of follow-up on a case after the patient leaves.
Only about 10% of our patients are screened by telephone, since most of our operations are complicated and require in-person assessment (most low-acuity procedures are done at other hospitals). Of the patients who visit the preoperative clinic, about 75% undergo the single assessment model for surgery, anesthesiology, and nursing as described above. The remaining 25% of patients have their history and physical exam completed outside Brigham and Women’s Hospital for insurance reasons; the remainder of their assessment is conducted in our preoperative clinic by a registered nurse and an anesthesiology resident.
Multiple systems checks
Our model also incorporates standardization in the form of multiple systems checks:
- Case presentation. Every case is presented to an attending anesthesiologist, who reviews the ECG (if ordered) before the patient leaves the clinic.
- Post-visit chart check. A registered nurse or nurse practitioner signs off on each chart after the visit, confirming test results and resolution of all paperwork issues.
- Surgical checklist. The end result is a checklist that serves as the front sheet of the operating room chart.
Our ability to use this system of checks to get the chart completed comprehensively and reliably and deliver it to the operating room when needed was key to securing institutional support and funding for the preoperative clinic.
ROLE OF THE ATTENDING ANESTHESIOLOGISTS
Two full-time attending anesthesiologists are present in the preoperative clinic each day. One is responsible largely for supervising the nurse practitioner assessments and reviewing case presentations, while the other also oversees the education and supervision of residents. Residents rotate through the clinic for 2 weeks (one or two at a time) and have a designated curriculum consisting of daily lectures and competencies in preoperative evaluation.
Because our anesthesiologists are expert in preoperative assessment, we require very few outside consults. We can communicate directly with the cardiologists and other physicians and order tests when indicated. We have a clerical assistant who obtains all necessary paperwork and prior testing from outside providers so that the clinicians need not waste time on this.
A GROWING CHALLENGE: ASSESSMENT FOR PROCEDURES IN AMBULATORY SETTINGS
Looking forward, a rapidly growing challenge facing our clinic stems from the tremendous growth in patients who require anesthesia for procedures performed outside the operating room. In these situations, the proceduralists need a system for deciding whether an anesthesiologist must be present for any given case.
We have started to develop appropriate screening processes to ensure that the proceduralists in multiple departments know which patients to refer for preprocedure assessment. We hope to soon develop protocols for high-risk patients and for various procedures such as implanting a pacemaker or defibrillator, catheter procedures, interventional radiology, and endoscopy.
Anesthesia Perioperative Medicine Clinic at University of Chicago
By BobbieJean Sweitzer, MD
Detsky and Naglie have argued that the costs and clinical outcomes associated with any intervention must be compared with those of alternate strategies for treating the same patients,1 and I believe their point applies well to preoperative clinics. Although certain requirements of the Joint Commission and CMS must be met, as noted by Dr. Bader, they can be met in various ways. I will preface my comments by emphasizing that one size does not fit all: every institution must decide the best approach to preoperative assessment based on its patient population, the types of procedures it performs, and the volume it handles.
TRIAGE STREAMLINES THE PROCESS
Our preoperative clinic at the University of Chicago emphasizes triage. Not every patient should have to go to the trouble of coming in to see a provider. In the future, we will likely see more “virtual” preoperative assessments using devices in development, such as handheld ultrasonography machines. Just as patients can have their pacemakers and implantable cardiac defibrillators remotely checked via phone contact, more tools will one day be available for remote assessment.
Although not every surgical patient needs to come in to the preoperative clinic, every patient must have a physical examination. All patients will be seen on the day of surgery, so in some cases the physical exam may be able to wait until then. For example, an airway assessment need not be done ahead of time. Most anesthesiologists are prepared to manage airways on very short notice, so extensive advance planning is not always necessary.
Obtain basic info by questionnaire to save staff time
Information about the patient is key to triage, and it may be either paper- or computer-based. An initial priority should be to develop some mechanism for getting information from patients before the day of their procedure without a visit to the hospital or ambulatory surgery center.
We use a two-page paper questionnaire to obtain basic information from patients, including (among other pertinent questions) age, planned operation, names of the surgeon and primary doctor, past operations and medical history, allergies, a list of medications, social history (drug, alcohol, tobacco use), whether they have ever taken steroids, whether they have high blood pressure, and whether they can comfortably walk up a flight of stairs. We provide the primary care physicians and surgeons with blank questionnaires, which their patients can fill out in their waiting rooms or take home and fax to us (or drop off) later. The questionnaire gives us a good deal of essential information without using staff time.
Various computer-based and Web-based systems are also available for collecting basic patient information. Smaller institutions need not purchase an entire electronic medical record system, which can be very expensive. Some Web-based tools operate on a pay-per-use basis and can be very helpful.
Review the information to guide triage
We then review the patient information to determine the extent of preoperative evaluation required. Some patients, especially those scheduled at an ambulatory surgery center, are healthy enough that they can just come in on the day of surgery for an examination and an update of their information. Others will need an appointment at the clinic before the day of surgery for more extensive preoperative evaluation. For other patients, review of their questionnaire responses may prompt a phone call or e-mail from the clinic for more information to determine whether a day-of-surgery exam will suffice or whether evaluation in advance is needed. When in doubt, concerns raised by the questionnaire should be explored before the day of surgery to avoid surprises and allow sufficient time for a consultation, if needed.
STANDARDIZED GUIDELINES KEEP CARE CONSISTENT
We encourage our staff to minimize preoperative testing and ECGs. A majority of diagnoses are made based on the history and physical exam.2 Generally, a test should confirm what is already suspected and merely provide objective evidence when needed. Testing in this setting should not be done to “find out what is wrong” with a patient.
It is helpful to develop standardized guidelines for preoperative assessment and make them available to everyone in the institution via the Web. The guidelines should address recommended preoperative tests and management practices according to specific patient conditions or surgical procedures. The clear objective is to avoid disagreement about what a patient needs between the provider who evaluated the patient in advance and the surgeon or anesthesiologist who evaluates the patient on the day of surgery.
Our guidelines at the University of Chicago include recommendations for patients on long-term anticoagulant therapy, for patients with coronary stents, for medications that should be discontinued (and those that may be continued) on the day of surgery, and for numerous other conditions and issues. Our testing guidelines list indicated tests for various medical problems, which in turn link to other guidelines. Other links are based on the medications a patient is using or the type of operation that is planned.
We collaborated with our electrophysiology department to create guidelines for managing patients with pacemakers and defibrillators. Almost every patient with one of these devices has a little card associated with the device, and we ask the surgeons to copy the card and send it to the clinic if we will not be directly seeing the patient. Using a national database, the electrophysiology department can determine from the card the type of pacemaker or defibrillator a patient has, and they fax or e-mail us back a page of instructions to let us know whether the device requires special consideration during surgery, whether it should be checked preoperatively, and whether its battery needs replacing. With this system, we have markedly reduced problems on the day of surgery.
CONSULTS HAVE AN IMPORTANT ROLE
Consults should never be requested in order to “clear a patient for surgery.” Consult requests should rather address specific issues, such as, “Is this patient medically optimized?” or “Please address this patient’s hypertension.” In turn, consult notes should provide meaningful information that can be used in a specific way. A clearance letter or simple risk assessment is not helpful.
If a patient has not seen a primary care doctor in a long time, a consult request should (in addition to requesting a global risk assessment) specify any particular concerns, such as, “The patient reports snoring; please address sleep apnea and cardiac risk.”
Case study: Beware consult notes with no specifics
Consider a case we encountered of a 54-year-old man who had a preoperative cardiac risk assessment. The cardiology consultant completed a short form consisting of a multiple-choice check-off list indicating low, moderate, or high cardiac risk. The consultant checked that the patient had low cardiac risk but provided no other instructions or information other than his own contact information.
When we reviewed the patient’s questionnaire, we saw that his medications included metoprolol, clopidogrel, and aspirin even though the patient did not mention that he had coronary artery disease. On this basis, we requested details about his cardiac evaluation from his cardiologist. It turned out that the patient had a history of four catheterizations with several cardiac stents placed. The most recent stent was implanted to overlap a previous stent that had been found “floating” in the blood vessel; this last stent was placed just 6 months before the cardiologist issued the consult note indicating “low cardiac risk.”
The moral is to approach consult notes with caution, especially if they offer no specifics. It actually makes me nervous when a note states “low risk” because if something unexpectedly goes wrong in surgery, it appears that the perioperative team took poor care of the patient even if the complication actually may have stemmed from higher-than-recognized underlying patient risk.
PROVIDE, AND REINFORCE, CLEAR INSTRUCTIONS
We give patients written preoperative instructions that become part of our computerized records. We first verbally give explicit instructions for each medication—ie, whether it can be taken as usual or when it needs to be stopped before surgery (and why). Then we provide the same information in writing, after which we try to have the patient repeat the instructions back to the clinician. We include a phone number that patients can call if they need help understanding their preoperative instructions.
Web-based programs also can provide patients online instructions about their medications. Some services even customize information by providing, for example, lists of local surgeons who are willing to allow a patient to continue on aspirin therapy until the day of surgery.
USE THE RIGHT RESOURCES
Staffing
Our model at the University of Chicago relies mainly on residents in training and physician assistants, but advanced nurse practitioners are well suited to a preoperative clinic as well. These types of providers have background training in history-taking, physical examination, diagnostic testing, and disease management. Registered nurses have more limited abilities, although they may be appropriate for a clinic that deals primarily with healthy patients for whom only history taking and a list of medications is needed. Additionally, our clinic is staffed by one attending anesthesiologist at all times (from among a group of rotating anesthesiologists) as well as medical assistants and clerical staff.
Some clinics perform the surgical history and physical exam at the same time as the anesthesia assessment. I would urge caution with this practice. Just as primary care doctors should not be conducting the anesthesia assessment, nonsurgeons should not be conducting the surgical assessment; doing so puts them out on a limb from a medicolegal standpoint. Advanced nurse practitioners and physician assistants may do surgical assessments under the supervision of a surgeon, but only surgeons should ultimately decide—and document—whether an operation is necessary and what degree of examination is required in advance.
Computer technology for records, messaging, billing
Using electronic medical records and corresponding with colleagues by e-mail make preoperative care much more efficient. We have standardized computer forms for ordering tests and documenting the physical exam. Patients usually understand that electronic medical records are safe and more efficient, and they are often more accepting of their use than practitioners are. Many patients want e-mail access to doctors, to schedule appointments online, and to receive appointment reminders by e-mail.3
Electronic medical records also avoid redundancy. If a patient has been seen in our preoperative clinic and is later scheduled for another surgery (even if a different surgeon is involved), a return visit to our clinic may not be necessary. In some cases, we can send the old work-up stamped “For information only,” which can then be updated by the anesthesiologist on the day of surgery.
A central, standardized process also makes billing more efficient and helps to ensure that payment is received for all services provided. Standardized documentation makes it easier for coders to enter the correct evaluation and management codes and ensures that all required criteria are met.
THE PAYOFF: LIVES AND DOLLARS SAVED
A thorough and efficient preoperative assessment system is cost-effective. Every minute of operating room time is worth $10 to $15,4,5 so delays should be avoided. Everything that is done ahead of time saves money for the whole enterprise by reducing unnecessary case setups and reducing “down time” due to lack of patient, equipment, or staff readiness. We routinely bill for preoperative evaluations when this service goes beyond a routine preoperative assessment based on CMS (and other insurance) requirements. However, a preoperative evaluation is required by CMS and most payers if one wants to be paid for any anesthesia-provided service. As a result, a cost is incurred without offsetting revenue if a case is cancelled on the day of surgery after one performs the anesthesia evaluation.
Yesterday I heard someone ask, “Do we really need all this preoperative evaluation? Does it really improve outcomes?” There is some evidence that it does. A study from 2000 based on data from the Australian Incident Monitoring Study found that 11% of the 6,271 critical incidents that occurred following operations were attributable to inadequate preoperative evaluation and that 3% were unequivocally related to problems with preoperative assessment or preparation. More than half of the incidents were deemed preventable.6
Preoperative clinics are good for patients and make good sense economically. We just need to demonstrate to our administrators and to payers that we are offering an excellent service.
Cleveland Clinic IMPACT Center
By Ajay Kumar, MD
Cleveland Clinic is structured differently from most other institutions in that its surgeons, anesthesiologists, and hospitalists are all direct employees of the institution. Despite this unique structure, many aspects of our preoperative clinic—known as the Internal Medicine Preoperative Assessment, Consultation and Treatment (IMPACT) Center—are applicable to other institutions.
Cleveland Clinic is a busy surgical hospital whose preoperative optimization system is designed to provide high-quality care. The IMPACT Center is consulted for most complicated noncardiac surgery patients, and its referral sources include most of the institution’s surgical specialties.
QUEST FOR A BETTER PATIENT EXPERIENCE
When the IMPACT Center was created in 1997, the aim was to focus on the same objectives highlighted by Drs. Bader and Sweitzer: safety, a positive patient experience, enhanced communication, better continuity of care, effective use of resources, and improving throughput by standardizing care.
A prime motivator was the desire to move away from the tendency for presurgical consults to simply “clear the patient for surgery,” and we have indeed evolved considerably from that point. The focus of our perioperative care program today is to comprehensively evaluate risk by taking into account patient-, procedure-, and anesthesia-related factors.
We offer “one-stop shopping,” and our priority is for efficient throughput. We are located in a 12-story building that includes outpatient, preoperative, and surgical clinics and offices. The IMPACT Center is on the first floor along with the preoperative anesthesia consultation and evaluation (PACE) clinic, the laboratory, and ECG and stress-test labs. Patients can undergo radiographic studies on the second floor.
The patient experience counts for a lot. Many of our patients are from another state or country, so efficiency and convenience are especially important. Patients can usually get all assessment and testing done in a single day.
A TIGHTLY MANAGED PROCESS
A ‘smart’ questionnaire starts the process
A computerized report based on the questionnaire guides the surgical office in scheduling the patient to specific areas according to algorithms. Based on case complexity and clinical needs, patients are scheduled for the IMPACT Center along with the PACE clinic; if needed (based on the algorithms), patients also are scheduled for laboratory tests or imaging. This standardized approach helps create a safe passage for patients through the preoperative process with less confusion.
Patient is given a personalized binder
Once all appointments and tests are scheduled, the patient is given a binder containing specific information about the procedure and preoperative instructions. The medical appointment at the IMPACT Center is usually scheduled before the PACE clinic appointment. Patients receive an itinerary for all preoperative appointments and surgical office appointments before the planned surgery. The itinerary is planned so that if additional testing is requested, it can be accommodated on the same day.
At the end of the preoperative assessment, the patient receives printed information with specific preoperative instructions, including which medications to continue or stop.
Standardized, computer-based medical records
Our systems and processes have undergone a good deal of evolution. We have integrated our medical records and use a standard outside medical record retrieval process. The template for the history and physical exam is standard for all Cleveland Clinic patients and is used for all presurgical assessments before all noncardiac surgeries. The template is comprehensive, including the history of the present illness, the review of systems, the physical exam, and anesthesia-related issues. All outside documents are scanned into our electronic medical record system and are available for viewing prior to surgery from any computer connected to the system.
Our preoperative assessment guidelines are also kept updated at a central online location so that all providers have access to them.
Staff keeps process running efficiently
The IMPACT Center is managed by the department of hospital medicine and supported by at least 5.5 full-time physicians every day. We also have two registered nurses, two assistants who help with scheduling and testing, and three secretaries who support the doctors, obtain records, and make arrangements with outside doctors for testing if a patient wants to return home before our testing can be completed.
A secretary also keeps a log for each patient seen in the clinic, tracking all pending issues. The day before surgery, the secretary contacts the appropriate office for anything that is still pending. If she gets no response, the matter is transferred to one of our doctors so that the problem can be resolved at once. This strategy allows us to achieve a nearly 0% rate of surgery delay or cancellation attributable to unavailable test results.
Our patient volumes have increased significantly since we started in 1997. Last year more than 15,000 patients visited the IMPACT Center and now we have expanded our services to regional hospitals within the Cleveland Clinic Health System.
INTERDEPARTMENTAL COMMUNICATION IS CRITICAL
Interdepartmental communication is a must for patient safety, so we encourage a culture of communication between the hospitalist and the surgical team. The location of most of our surgical clinics within the same building as the IMPACT Center further facilitates communication, as does the proximity of the PACE clinic. Additionally, one of our IMPACT Center physicians is accessible around the clock to answer to our surgeon or anesthesiologist colleagues as needed.
We regularly assess our process and seek feedback from surgeons and anesthesiologists. We also conduct yearly patient experience surveys to make sure we are providing patients with the highest quality of care.
Discussion
Question from the audience: Our anesthesia assessment department was approached by our surgeons to do both the anesthesia and surgical assessments, but we felt that would put us in a potential legal conflict if a patient who was assessed that way developed problems. Can you comment?
Dr. Bader: Although we do surgical assessments at our preoperative clinic, we don’t make any decisions about whether or not to proceed with an operation. We get an office note from the surgeon that is directed specifically toward the need for surgery, indications for surgery, and surgical consent. We perform the surgical history and physical examination. Our process is essentially the same as when surgeons have a physician assistant do the history and physical examination in their office. Our practitioners are employed by the hospital, so there is no conflict of interest there.
Comment from the audience: I’m a strong believer in hands-on patient contact. Over my 15 years of practice, we have encountered a lot of unexpected problems during the preoperative exam—aortic stenoses, infections, ventricular septal defects—all of which would never have been detected from a screening form.
Dr. Sweitzer: I agree that we pick up many things by seeing the patient in person. I’ve picked up more cases of aortic stenosis as an anesthesiologist in the preoperative clinic than I ever did as an internist, because the population is high-risk. But patients who have such problems tend to have risk factors and be in certain age groups. Studies indicate that the history is more important than the physical exam: the history suggests about 75% of conditions that are present. The physical exam adds only a little more—perhaps another 15%. Our recommendations are very much consistent with the American College of Cardiology and American Heart Association guidelines on preoperative cardiac evaluation.7 It is more important to identify whether a patient has risk factors for coronary artery disease than to find out whether a stress test or ECG is normal. One needs to do a really good history, but it can be done remotely. Based on certain risk factors identified, high-risk patients can be selected who need to come in and have a physical exam.
Question from the audience: Could you elaborate on the electronic medical record system used at the University of Chicago? I’ve heard there’s a steep learning curve when implementing these kinds of systems. They also are very expensive—I’ve heard that some cost $40 to $80 million. Has enhanced revenue flow offset the costs?
Dr. Sweitzer: We have a home-grown system developed with FileMaker Pro by a computer programmer at our institution. It was a lot easier to develop than people tend to think. There are many savvy computer programmers out there; I’ve had medical students assist me with updating it. We’re now considering developing it as a commercial system. Many systems are available for purchase, including Epic, Pyxis, one from General Electric, and many others. They are very expensive, so smaller institutions might want to use a pay-for-service system.
There definitely is a learning curve to switching to electronic medical records, but it is not nearly as steep as many believe. The extra time it takes a clinician to initially make a computer entry rather than write on paper is vastly recouped downstream: the electronic medical record is legible and organized, and it doesn’t get lost or need to be redone. You can bring up a patient record from 6 months before and reuse it as a template.
Dr. Bader: The discussion of cost savings from preoperative clinics usually focuses on savings from avoiding surgery cancellations and delays and from more efficient laboratory testing, but the biggest savings for an institution is better reimbursement through better diagnosis-related groups (DRG) coding. That’s an important reason our institution is funding our clinic. Electronic medical records allow standardization of information so that coders know exactly where to look for the comorbidities and other pertinent information. This increases payments for DRGs, which can be documented for the hospital. This literally runs into millions of dollars a year and more than offsets the costs of the system.
Question from the audience: Dr. Bader, I’m impressed with the number of patients going through your preoperative clinic. How many patients are seen per nurse practitioner in your clinic?
Dr. Bader: The nurse practitioners have 10-hour shifts and see one patient every 75 minutes. The process of seeing a patient takes a lot less time now than with the old system, in which patients saw an anesthesiologist plus a nurse. Our current system eliminates redundancy: questions need to be asked only once.
Question from the audience: My compliance office says that preoperative assessments for early-morning admission patients are good for only 7 days. Is that true?
Dr. Bader: There are sometimes differences between Joint Commission requirements and those of certain insurance companies. That kind of issue needs to be discussed with your hospital compliance office. We program rules into our scheduling system to accommodate different insurance policies and other requirements so that a patient is not scheduled beyond the allowable period.
- Detsky AS, Naglie IG. A clinician’s guide to cost-effectiveness analysis. Ann Intern Med 1990; 113:147–154.
- Sandler G. The importance of the history in the medical clinic and the cost of unnecessary tests. Am Heart J 1980; 100:928–931.
- Blumenthal D, Glaser JP. Information technology comes to medicine. N Engl J Med 2007; 356:2527–2534.
- Strum DP, Vargas LG, May JH. Surgical subspecialty block utilization and capacity planning: a minimal cost analysis model. Anesthesiology 1999; 90:1176–1185.
- Ferschl MB, Tung A, Sweitzer B, Huo D, Glick DB. Preoperative clinic visits reduce operating room cancellations and delays. Anesthesiology 2005; 103:855–859.
- Kluger MT, Tham EJ, Coleman NA, et al. Inadequate preoperative evaluation and preparation: a review of 197 reports from the Australian incident monitoring study. Anaesthesia 2000; 55:1173–1178.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2007; 50:1707–1732.
- Detsky AS, Naglie IG. A clinician’s guide to cost-effectiveness analysis. Ann Intern Med 1990; 113:147–154.
- Sandler G. The importance of the history in the medical clinic and the cost of unnecessary tests. Am Heart J 1980; 100:928–931.
- Blumenthal D, Glaser JP. Information technology comes to medicine. N Engl J Med 2007; 356:2527–2534.
- Strum DP, Vargas LG, May JH. Surgical subspecialty block utilization and capacity planning: a minimal cost analysis model. Anesthesiology 1999; 90:1176–1185.
- Ferschl MB, Tung A, Sweitzer B, Huo D, Glick DB. Preoperative clinic visits reduce operating room cancellations and delays. Anesthesiology 2005; 103:855–859.
- Kluger MT, Tham EJ, Coleman NA, et al. Inadequate preoperative evaluation and preparation: a review of 197 reports from the Australian incident monitoring study. Anaesthesia 2000; 55:1173–1178.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2007; 50:1707–1732.
KEY POINTS
- Standardizing the preoperative assessment process helps ensure that regulatory, accreditation, and payer requirements and guidelines are met.
- Careful triage based on a patient’s history can help avoid unnecessary assessment of low-risk patients and ensure that necessary assessments for higher-risk patients are completed before the day of surgery.
- Perioperative assessment and management guidelines for various types of surgery and patient risk factors should be developed, continuously updated, and made available online to all providers within the institution.
- Electronic medical records allow standardization of patient information, avoid redundancy, and provide a database for research.
Perioperative management of anemia: Limits of blood transfusion and alternatives to it
Anemia is a potent risk factor for mortality and morbidity in surgical patients, and its management has begun to shift away from allogeneic blood transfusion in recent years. This article reviews the clinical importance of perioperative anemia, the role and shortcomings of blood transfusion, and the pros and cons of alternative approaches to managing perioperative anemia. I conclude with an overview of a program for perioperative blood product use at my institution, Cleveland Clinic.
SIGNIFICANCE OF PERIOPERATIVE ANEMIA
Prevalence depends on many factors
The reported prevalence of anemia in surgical patients varies widely—from 5% to 76%1—and depends on the patient’s disease and comorbidities, the surgical procedure and associated blood loss, and the definition of anemia used. The prevalence of preoperative anemia increases with patient age and is higher in women than in men.2
A multiplier of risk
Anemia is an important multiplier of mortality risk. For example, the presence of anemia raises the relative risk of 2-year mortality from 2.05 to 3.37 in patients with chronic kidney disease, from 2.86 to 3.78 in patients with heart failure, and from 4.86 to 6.07 in patients with concomitant heart failure and chronic kidney disease.3
Adverse effects of anemia have been demonstrated specifically in the perioperative setting as well. A large retrospective cohort study showed that a preoperative hemoglobin concentration of less than 6 g/dL increases the risk of death 30 days after surgery by a factor of 26 relative to a concentration of 12 g/dL or greater in surgical patients who declined blood transfusion for religious reasons.4 The anemia-associated mortality risk was especially pronounced among patients with cardiovascular disease.4 Other studies have demonstrated perioperative anemia to be associated with increases in the risk of death,5 cardiac events,6 pneumonia,7 and postoperative delirium.8
IS BLOOD TRANSFUSION THE ANSWER
The use of allogeneic blood transfusion to manage anemia and blood loss is a concept that originated several centuries ago and has changed little over the years.
Blood supply challenges
Blood collection has historically lagged demand, resulting in a blood supply insufficient to meet transfusion needs. According to the federal government’s 2007 National Blood Collection and Utilization Survey Report, 6.89% of US hospitals reported that they cancelled elective surgery on 1 or more days in the prior year because of a lack of blood availability, and 13.5% experienced at least 1 day in which nonsurgical blood needs could not be met.9 Unless practices are changed to increase blood donation, these unmet tranfusion needs may grow.
Joint Commission set to measure blood management
In response to this challenge, an advisory panel formed by the Joint Commission has identified 17 performance measures related to blood conservation and appropriate transfusion.10 These measures are currently in development, and we expect to see some types of metrics in the near future. Such metrics are likely to further prioritize blood management for US hospitals.
Safety of the blood supply: Viral transmission down, TRALI risk persists
The safety of the blood supply has improved markedly. Sophisticated testing and public demand have led to a dramatic decline in the risk of transfusion-related transmission of HIV, hepatitis C virus, and hepatitis B virus.11
Despite this progress, the risk of transfusion-related acute lung injury (TRALI) has persisted in recent years. TRALI is characterized by acute onset of noncardiogenic pulmonary edema within 6 hours of blood product transfusion. Believed to be immune-mediated, TRALI is thought to occur as antibodies to human leukocyte antigens develop, inducing capillary leak syndrome.12 The patients most commonly affected are those who receive plasma from multiparous female donors. A recent evaluation of transfusion-related fatalities reported to the US Food and Drug Administration (FDA) revealed a continual rise in fatal TRALI cases in the United States from 2001 to 2006.13–15 TRALI was implicated in more than half of all transfusion-related fatalities reported to the FDA in 2006, a higher number than for any other single cause.13
At the same time, there is evidence that hemovigilance can reduce TRALI risk. In the United Kingdom, the Serious Hazards of Transfusion Steering Group introduced in late 2003 a policy of using plasma from male donors as much as possible, in view of the association of TRALI with plasma from multiparous female donors. The effort appeared to pay off: whereas TRALI accounted for 6.8% of all transfusion-related adverse events reported in the United Kingdom during the period 1996–2003,16 this proportion declined to just 1.9% in 2006.17
Finally, despite the progress in screening blood for more established infections like HIV and the hepatitis viruses, some additional infections now must be considered when assessing blood supply safety. These include diseases newly recognized as being transmissible by blood, or for which blood donor screening is not currently available, or that are newly emergent infections for which the potential for spread by transfusion is unknown. For such diseases—which include malaria and West Nile virus—the risk of transmission through transfusion is low, as they are much more likely to be acquired by other means.
Transfusion and outcomes: Not a strong record
Transfusion has never undergone safety and efficacy evaluation by the FDA. Given the challenges of conducting a randomized study of transfusion in the perioperative setting, we may never have high-quality data to assess transfusion in this setting.
A few studies merit mention, however. The Transfusion Requirement in Critical Care (TRICC) trial was conducted in 838 critically ill patients in the intensive care setting.18 Patients were randomized to a strategy of either liberal transfusion (begun when hemoglobin fell below 10 g/dL) or restrictive transfusion (begun when hemoglobin fell below 7 g/dL). Thirty-day mortality was similar between patients in the two strategy groups, but the restrictive strategy was associated with significantly lower mortality in at least two subgroups: patients with myocardial infarction and patients with pulmonary edema. Further subgroup analysis found no benefit of early or aggressive transfusion in patients with coronary artery disease or in those requiring mechanical ventilation.
Rao et al performed a meta-analysis of three large international trials of patients with acute coronary syndromes to determine whether blood transfusion to correct anemia in this setting was associated with improved survival.19 They found significantly higher mortality among patients who underwent transfusion compared with those who did not, prompting them to urge caution in the use of transfusion to maintain arbitrary hematocrit levels in stable patients with ischemic heart disease.
Similarly, a risk-adjusted, propensity-matched analysis of 6,301 patients undergoing noncardiac surgery found that receipt of 4 U of blood or more was a predictor of greater mortality, higher risk of infection, and longer hospital stay.20 Moreover, in an observational cohort study of 11,963 patients who underwent isolated coronary artery bypass graft surgery, each unit of red blood cells transfused was associated with an incrementally increased risk of adverse outcome (eg, mortality, renal injury, need for ventilator support, lengthened hospital stay, infection).21 The latter study found that transfusion was the single factor most reliably associated with increased risk of postoperative morbidity.
Additional studies have echoed these findings—ie, that perioperative blood transfusion has been associated with a host of adverse outcomes, including increased morbidity and length of stay, increased rates of postoperative infection, as well as immunosuppression, viral transmission, and acute transfusion reactions.5,22,23
Outcomes and duration of blood storage
An interesting factor in the relation between transfusion and outcomes is the shelf life of the blood being transfused. The FDA currently allows storage of blood for a maximum of 42 days, but a recent study of patients who received red blood cell transfusions during cardiac surgery found that those who received “older blood” (stored for > 14 days) had significantly higher rates of sepsis, prolonged intubation, renal failure, in-hospital mortality, and 1-year mortality compared with those who received “newer blood” (stored for ≤ 14 days).24
These differing outcomes are generally attributed to the so-called storage defect: as blood gets older, it loses components such as 2,3-DPG and adenosine disphosphate, its red cells lose deformability, and it undergoes buildup of cytokines and free hemoglobin. Increased demand for newer blood in light of the storage defect could further intensify pressures on the blood supply.
MANAGEMENT OF PERIOPERATIVE ANEMIA
In light of these shortcomings of blood transfusion, how should anemia be managed perioperatively to reduce or avoid the need for transfusion?
Preoperative evaluation
Vigilance for anemia and related issues in the preoperative evaluation is fundamental. The evaluation should elicit a history of bleeding tendencies, previous transfusions, and symptoms of anemia. Medications should be reviewed with an eye toward any that may predispose to perioperative bleeding and anemia, such as aspirin, clopidogrel, and anticoagulants. During the physical examination, alertness for pallor and petechiae is key, as is attentiveness to symptoms of anemia such as shortness of breath and fatigue.
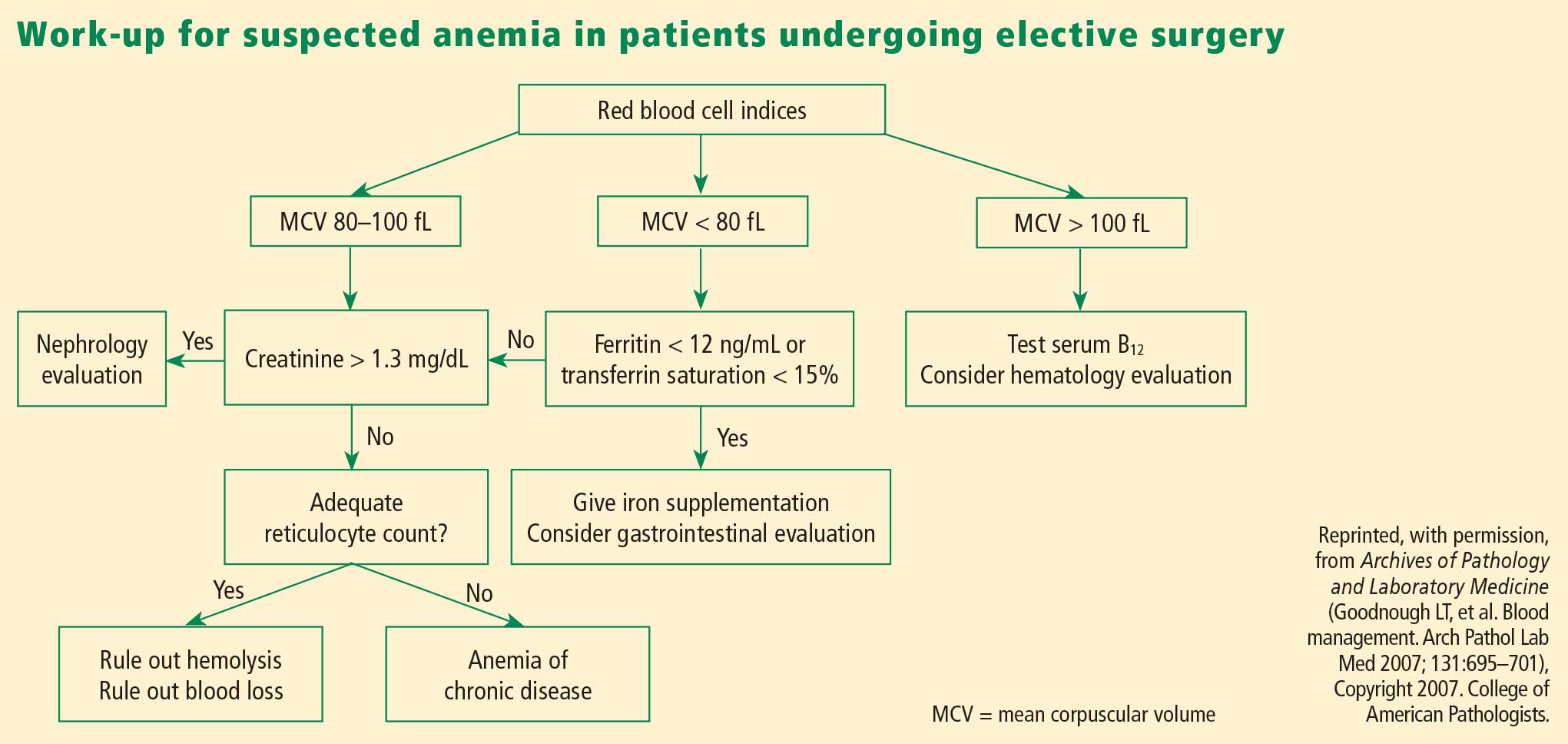
Overview of management options
Once the cause of anemia is identified, the choice for optimal medical management can be made. Choices broadly consist of pharmacologic and technological options. The former include iron supplements and erythropoiesis-stimulating agents. Among other pharmacologic options are thrombin, collagen, fibrin glue, tranexamic acid, and aminocaproic acid, but these agents are less well studied and will not be discussed here. Technological options include preoperative autologous blood donation, cell salvage, and acute normovolemic hemodilution.
In addition to these options, careful management of anticoagulant and antiplatelet medications should be provided, including discontinuation or substitution of drugs that could hamper clotting perioperatively.
PHARMACOLOGIC OPTIONS
Iron supplementation
Oral iron is available in four preparations: ferrous sulfate, ferrous gluconate, ferrous fumarate, and iron polysaccharide. Gastrointestinal side effects may limit these preparations’ tolerability. Iron supplements with a high elemental value will require fewer pills and fewer doses, reducing the risk or frequency of side effects.
Intravenous (IV) iron preparations are much safer now than they were years ago, when anaphylactic reactions were a concern. The ones generally used in the perioperative setting are iron sucrose and iron gluconate. Unlike the older IV preparations, the use of iron sucrose and iron gluconate often requires a second dose. The effect on hemoglobin levels usually occurs starting at 1 week, with the maximum effect achieved at 2 weeks. Hypotension, arthralgia, abdominal discomfort, and back pain are potential side effects of IV iron.
Efficacy and safety of iron supplementation. Evidence of the efficacy of preoperative iron supplementation is mounting. A study of 569 patients undergoing colorectal cancer surgery found that among the 116 patients who were anemic, intraoperative transfusion was needed in a significantly lower proportion of those who received 2 weeks of preoperative oral iron supplementation (200 mg) compared with those who received no iron therapy (9.4% vs 27.4%; P < .05).26 Similarly, in an uncontrolled study, 10 days of IV iron sucrose starting 4 weeks preoperatively significantly increased hemoglobin levels in 20 patients with iron-deficiency anemia prior to elective orthopedic surgery.27
Risks of infection and cancer progression have been concerns with IV iron therapy. However, no significant association between IV iron therapy and bacteremia was identified in a prospective study of 985 patients receiving chronic hemodialysis.28 The effect of IV iron administration on tumor progression has not been prospectively studied.
In general, IV iron, especially the newer forms, is a safer alternative to blood transfusion. Death occurs at a much lower rate with iron than with blood transfusion (0.4 per million vs 4 per million, respectively), as do life-threatening adverse events (4 per million vs 10 per million, respectively), according to a systematic review by the Network for Advancement of Transfusion Alternatives.29
Erythropoiesis-stimulating agents
Erythropoiesis-stimulating agents (ESAs) include epoetin alfa (erythropoietin), first approved by the FDA in 1989, and the more recently introduced darbepoetin alfa. They are approved to treat anemia in several patient populations, but only epoetin alfa is approved by the FDA explicitly for use in patients undergoing major surgery (to reduce the need for blood transfusions). The ESAs have come under intense scrutiny in recent years over their risk-to-benefit ratio, as detailed below.
The preoperative dosing schedule for epoetin alfa is usually three weekly doses (plus a fourth dose on the day of surgery) if the surgery is scheduled 3 or more weeks in advance. However, daily dosing can be used effectively if the preoperative period is less than 3 weeks, provided that it is continued until 4 days after surgery. Oral iron is necessary throughout the course of epoetin alfa therapy.
Efficacy in reducing transfusions. In a systematic review published in 1998, epoetin alfa was shown to minimize perioperative exposure to allogeneic blood transfusion in patients undergoing orthopedic or cardiac surgery.30 Its benefit was greatest in patients at the highest risk of requiring transfusion. It was effective whether given daily or weekly, and did not significantly increase the risk of thrombotic events when used in surgical patients, although some studies did find an excess of thrombotic events with its use.
In three randomized trials conducted in patients undergoing joint arthroplasty (hip or knee), epoetin alfa was associated with substantial and significant reductions in perioperative blood transfusion compared with placebo or preoperative autologous blood donation.31–33 Rates of deep vein thrombosis (DVT) did not differ significantly between the epoetin alfa and placebo groups.
Concerns over perioperative thromboembolic risk. In early 2007, the FDA was made aware of preliminary results of an open-label study in which 681 patients undergoing elective spinal surgery who did not receive prophylactic anticoagulation were randomized to epoetin alfa plus standard-of-care therapy (pneumatic compression) or standard-of-care therapy alone.34,35 The incidence of DVT was 4.7% in patients treated with epoetin alfa compared with 2.1% in those not receiving epoetin alfa. It is important to note that the available ESAs are prothrombotic and increase thrombotic risk significantly, especially in populations like this one in which pharmacologic DVT prophylaxis is not routinely used.
Based in part on this study, the FDA in 2007 required a boxed warning to be added to the ESAs’ package inserts to specify the increased risk of DVT with their use in surgical patients not receiving prophylactic anticoagulation. The warning urges consideration of the use of DVT prophylaxis in surgical patients receiving an ESA.34,35
TECHNOLOGICAL OPTIONS AND OTHER STRATEGIES
Autologous blood donation: A practice in decline
In cases of elective surgery, autologous blood donation can be used to protect against disease transmission and overcome the challenge of blood type compatibility. Preoperative autologous donation of blood has been a prevalent practice, but its use is declining. One reason is that waste is high (approximately 50% at Cleveland Clinic), which makes this practice more costly than is often realized. Also, autologous blood donation increases the likelihood that the patient will be anemic on the day of surgery, so that he or she may still need allogeneic blood after all, defeating the initial purpose. Despite these limitations, preoperative autologous blood donation remains a useful option for a subset of patients with multiple antibodies for whom donor blood may be difficult to obtain.
Cell salvage
Cell salvage is an innovative technology that recovers the patient’s own blood (after being shed from the surgical incision) for transfusion after filtering and washing. It is particularly well suited to procedures that involve massive blood loss. Cell savage requires technical expertise, however, and involves costs associated with both the machine and disposables.
Restricted postoperative phlebotomy
Phlebotomy accounts for a significant amount of blood loss, especially in intensive care patients with arterial lines. The equivalent of 30% of total blood transfused has been reported to be lost to phlebotomy during an intensive care unit stay.36 Triggers for transfusion cannot be assigned universally based on blood loss from phlebotomy but must consider the patient’s hemodynamic status, cardiac reserve, and other clinical characteristics.
PROMOTING RESPONSIBLE BLOOD PRODUCT USE
Blood is expensive, and in recent years hospitals have experienced increases in the cost of blood and blood products. To promote responsible blood use, we have developed a multipronged approach to blood management at Cleveland Clinic. The program’s cornerstone is increased awareness of the risks associated with blood transfusions. The emphasis is on educating staff physicians and other caregivers about the appropriate use of blood products. We also have implemented a new policy requiring staff authorization for all blood requested in nonemergency situations. Additionally, requests for blood components require adherence to an indication-based ordering process. Finally, data about blood use are shared transparently among physicians, encouraging good clinical practice.
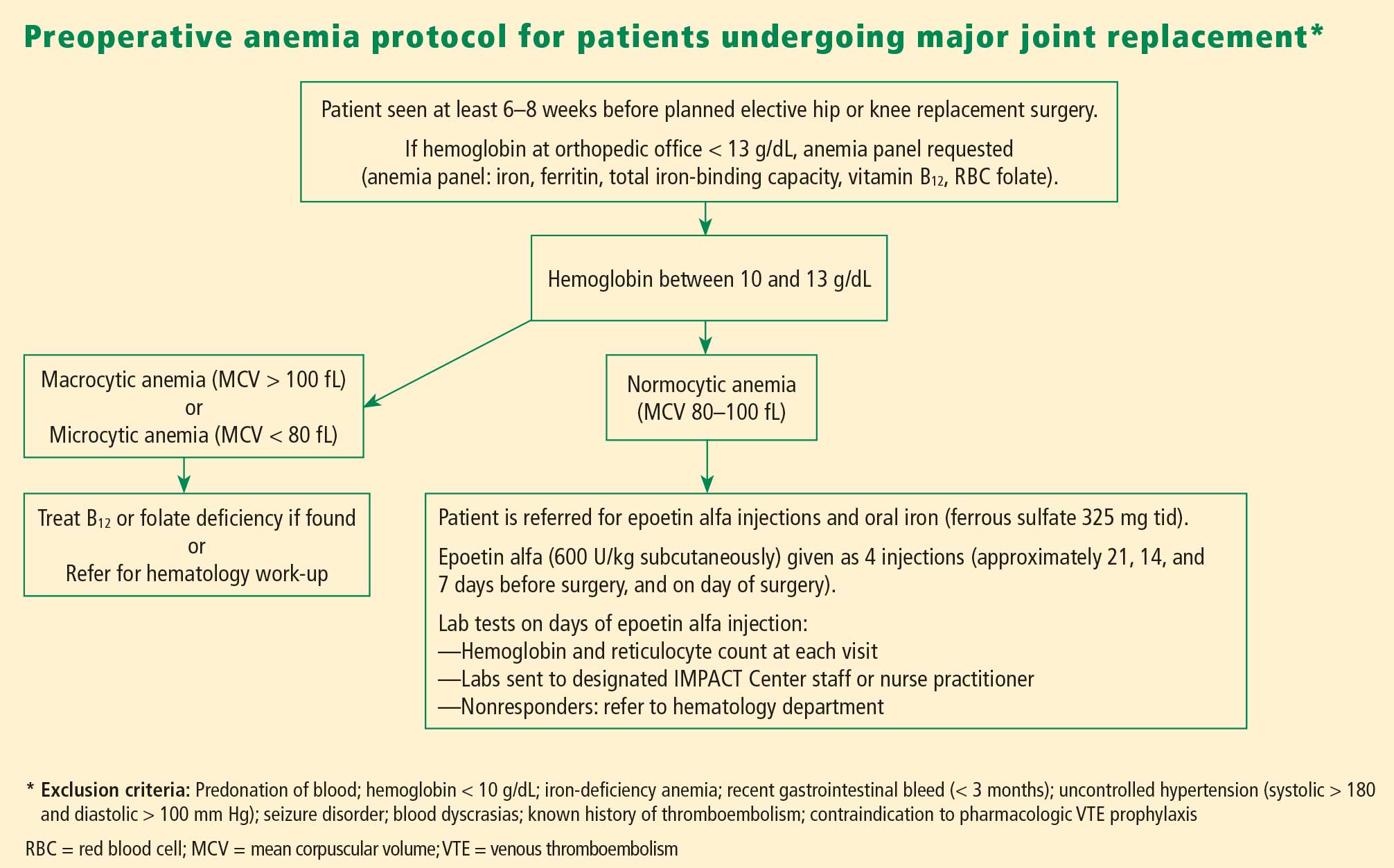
In the first 7 months of the program, we observed decreased utilization of blood products in the inpatient setting. Notably, the reduction in blood use was significantly greater in the surgical population than in the medical population.
CONCULSIONS
Anemia is associated with increased morbidity and mortality in the perioperative setting. Perioperative blood transfusion is one method of raising hemoglobin levels in anemic surgical patients, but it increases perioperative morbidity in the form of acute transfusion reactions, immunosuppression, postoperative infection, and longer hospital stays. Moreover, blood collection continues to lag blood demand. For these reasons, most relevant major medical organizations—including the Association of Blood Banks, the American Red Cross, and the FDA—advise that red blood cell–containing components should not be used to treat anemias that can be corrected with medications. These medical alternatives—all of which can be used in the perioperative setting—include iron supplementation, vitamin B12, and ESAs in select patient groups.
DISCUSSION
Question from the audience: Are there risks involved with autologous blood donation? Are different hemoglobin thresholds used when a patient’s own blood is used?
Dr. Kumar: As I mentioned, preoperative autologous donation is a technique that is less frequently used in our hospital. Autologous transfusion is considered safe only for patients who come to the clinic with normal hemoglobin values. Some patients may not have recovered from their blood loss by the time they come to surgery, so you end up needing to give them more blood because they started out anemic.
Question from the audience: Is there risk to giving patients back their own blood? Do you have to worry about transfusion-induced lung injury, sepsis, or other complications?
Dr. Kumar: As with allogeneic blood, the risk of clerical or clinical error exists with autologous blood: it too needs to be kept on the shelf, taken out, and infused, and the risk of sepsis remains the same.
- Shander A, Knight K, Thurer R, Adamson J, Spence R. Prevalence and outcomes of anemia in surgery: a systematic review of the literature. Am J Med 2004; 116(suppl 7A):58S–69S.
- Kulier A, Gombotz H. Perioperative anemia [in German]. Anaesthesist 2001; 50:73–86.
- Herzog CA, Muster HA, Li S, Collins AJ. Impact of congestive heart failure, chronic kidney disease, and anemia on survival in the Medicare population. J Card Fail 2004; 10:467–472.
- Carson JL, Duff A, Poses RM, et al. Effect of anaemia and cardiovascular disease on surgical mortality and morbidity. Lancet 1996; 348:1055–1060.
- Gruson KI, Aharonoff GB, Egol KA, Zuckerman JD, Koval KJ. The relationship between admission hemoglobin level and outcome after hip fracture. J Orthop Trauma 2002; 16:39–44.
- Nelson AH, Fleisher LA, Rosenbaum SH. Relationship between postoperative anemia and cardiac morbidity in high-risk vascular patients in the intensive care unit. Crit Care Med 1993; 21:860–866.
- Faris PM, Spence RK, Larholt KM, Sampson AR, Frei D. The predictive power of baseline hemoglobin for transfusion risk in surgery patients. Orthopedics 1999; 22(suppl 1):s135–s140.
- Marcantonio ER, Goldman L, Orav EJ, Cook EF, Lee TH. The association of intraoperative factors with the development of postoperative delirium. Am J Med 1998; 105:380–384.
- US Department of Health and Human Services. The 2007 National Blood Collection and Utilization Survey. Available at: http://www.aabb.org/Documents/Programs_and_Services/Data_Center/07nbcusrpt.pdf. Accessed March 9, 2009.
- The Joint Commission. Performance measurement initiatives. Available at http://www.jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/Blood+Management+-+Utilization.htm.
- Busch MP, Kleinman SH, Nemo GJ. Current and emerging infectious risks of blood transfusions. JAMA 2003; 289:959–962.
- Silliman CC, Ambruso DR, Boshkov LK. Transfusion-related acute lung injury. Blood 2005; 105:2266–2273.
- Benjamin RJ. Transfusion and transplantation safety: American Red Cross concerns. PowerPoint slides presented at Department of Health and Human Services Advisory Committee on Blood Safety and Availability meeting, May 10–11, 2007. Available at: http://www.hhs.gov/ophs/bloodsafety/presentations/Benjamin0507.pdf. Accessed March 9, 2009.
- Holness L. Transfusion related acute lung injury (TRALI): the FDA current view. PowerPoint slides presented at FDA Blood Products Advisory Committee meeting, July 22–23, 2004. Available at: http://www.fda.gov/OHRMS/DOCKETS/ac/04/briefing/2004-4057b1_01.pdf. Accessed March 9, 2009.
- Williams AE. Transfusion related acute lung injury (TRALI). PowerPoint slides presented at FDA Blood Products Advisory Committee meeting, April 27, 2007. Available at: http://www.fda.gov/ohrms/dockets/ac/07/slides/2007-4300S2-05.ppt. Accessed March 9, 2009.
- Stainsby D, Cohen H, Jones H, et al. Serious Hazards of Transfusion—Annual Report 2003. Published July 5, 2004. Available at: http://www.shotuk.org/SHOT%20Report%202003.pdf. Accessed April 29, 2009.
- Taylor C, Cohen H, Stainsby D, et al. Serious Hazards of Transfusion—Annual Report 2006. Published November 20, 2007. Available at: http://www.shotuk.org/SHOT_report_2006.pdf. Accessed April 29, 2009.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999; 340:409–417.
- Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004; 292:1555–1562.
- Dunne JR, Malone D, Tracy JK, et al. Perioperative anemia: an independent risk factor for infection, mortality, and resource utilization in surgery. J Surg Res 2002; 102:237–244.
- Koch CG, Li L, Duncan AI, et al. Morbidity and mortality risk associated with red blood cell and blood-component transfusion in isolated coronary artery bypass grafting. Crit Care Med 2006; 34:1608–1616.
- Rady MY, Ryan T, Starr NJ. Perioperative determinants of morbidity and mortality in elderly patients undergoing cardiac surgery. Crit Care Med 1998; 26:225–235.
- Goodnough LT, Brecher ME, Kanter MH, AuBuchon JP. Transfusion medicine. First of two parts—blood transfusion. N Engl J Med 1999; 340:438–447.
- Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med 2008; 358:1229–1239.
- Goodnough LT, Shander A. Blood management. Arch Pathol Lab Med 2007; 131:695–701.
- Okuyama M, Ikeda K, Shibata T, et al. Preoperative iron supplementation and intraoperative transfusion during colorectal cancer surgery. Surg Today 2005; 35:36–40.
- Theusinger OM, Leyvraz PF, Schanz U, et al. Treatment of iron deficiency anemia in orthopedic surgery with intravenous iron: efficacy and limits: a prospective study. Anesthesiology 2007; 107:923–927.
- Hoen B, Paul-Dauphin A, Kessler M. Intravenous iron administration does not significantly increase the risk of bacteremia in chronic hemodialysis patients. Clin Nephrol 2002; 57:457–461.
- Beris P, Muñoz M, García-Erce JA, et al. Perioperative anaemia management: consensus statement on the role of intravenous iron. Br J Anaesth 2008; 100:599–604.
- Laupacis A, Fergusson D. Erythropoietin to minimize perioperative blood transfusion: a systematic review of randomized trials: The International Study of Perioperative Transfusion (ISPOT) Investigators. Transfus Med 1998; 8:309–317.
- Feagan BG, Wong CJ, Kirkley A, et al. Erythropoietin with iron supplementation to prevent allogeneic blood transfusion in total hip joint arthroplasty: a randomized, controlled trial. Ann Intern Med 2000; 133:845–854.
- Stowell CP, Chandler H, Jové M, et al. An open-label, randomized study to compare the safety and efficacy of perioperative epoetin alfa with preoperative autologous blood donation in total joint arthroplasty. Orthopedics 1999; 22(suppl 1):s105–s112.
- de Andrade JR, Jové M, Landon G, et al. Baseline hemoglobin as a predictor of risk of transfusion and response to Epoetin alfa in orthopedic surgery patients. Am J Orthop 1996; 25:533–542.
- Procrit [package insert]. Raritan, NJ: Ortho Biotech Products LP; 2009.
- Epogen [package insert]. Thousand Oaks, CA: Amgen Inc.; 2009.
- Smoller BR, Kuskall MS. Phlebotomy for diagnostic laboratory tests in adults: pattern of use and effect on transfusion requirements. N Engl J Med 1986; 314:1233–1235.
Anemia is a potent risk factor for mortality and morbidity in surgical patients, and its management has begun to shift away from allogeneic blood transfusion in recent years. This article reviews the clinical importance of perioperative anemia, the role and shortcomings of blood transfusion, and the pros and cons of alternative approaches to managing perioperative anemia. I conclude with an overview of a program for perioperative blood product use at my institution, Cleveland Clinic.
SIGNIFICANCE OF PERIOPERATIVE ANEMIA
Prevalence depends on many factors
The reported prevalence of anemia in surgical patients varies widely—from 5% to 76%1—and depends on the patient’s disease and comorbidities, the surgical procedure and associated blood loss, and the definition of anemia used. The prevalence of preoperative anemia increases with patient age and is higher in women than in men.2
A multiplier of risk
Anemia is an important multiplier of mortality risk. For example, the presence of anemia raises the relative risk of 2-year mortality from 2.05 to 3.37 in patients with chronic kidney disease, from 2.86 to 3.78 in patients with heart failure, and from 4.86 to 6.07 in patients with concomitant heart failure and chronic kidney disease.3
Adverse effects of anemia have been demonstrated specifically in the perioperative setting as well. A large retrospective cohort study showed that a preoperative hemoglobin concentration of less than 6 g/dL increases the risk of death 30 days after surgery by a factor of 26 relative to a concentration of 12 g/dL or greater in surgical patients who declined blood transfusion for religious reasons.4 The anemia-associated mortality risk was especially pronounced among patients with cardiovascular disease.4 Other studies have demonstrated perioperative anemia to be associated with increases in the risk of death,5 cardiac events,6 pneumonia,7 and postoperative delirium.8
IS BLOOD TRANSFUSION THE ANSWER
The use of allogeneic blood transfusion to manage anemia and blood loss is a concept that originated several centuries ago and has changed little over the years.
Blood supply challenges
Blood collection has historically lagged demand, resulting in a blood supply insufficient to meet transfusion needs. According to the federal government’s 2007 National Blood Collection and Utilization Survey Report, 6.89% of US hospitals reported that they cancelled elective surgery on 1 or more days in the prior year because of a lack of blood availability, and 13.5% experienced at least 1 day in which nonsurgical blood needs could not be met.9 Unless practices are changed to increase blood donation, these unmet tranfusion needs may grow.
Joint Commission set to measure blood management
In response to this challenge, an advisory panel formed by the Joint Commission has identified 17 performance measures related to blood conservation and appropriate transfusion.10 These measures are currently in development, and we expect to see some types of metrics in the near future. Such metrics are likely to further prioritize blood management for US hospitals.
Safety of the blood supply: Viral transmission down, TRALI risk persists
The safety of the blood supply has improved markedly. Sophisticated testing and public demand have led to a dramatic decline in the risk of transfusion-related transmission of HIV, hepatitis C virus, and hepatitis B virus.11
Despite this progress, the risk of transfusion-related acute lung injury (TRALI) has persisted in recent years. TRALI is characterized by acute onset of noncardiogenic pulmonary edema within 6 hours of blood product transfusion. Believed to be immune-mediated, TRALI is thought to occur as antibodies to human leukocyte antigens develop, inducing capillary leak syndrome.12 The patients most commonly affected are those who receive plasma from multiparous female donors. A recent evaluation of transfusion-related fatalities reported to the US Food and Drug Administration (FDA) revealed a continual rise in fatal TRALI cases in the United States from 2001 to 2006.13–15 TRALI was implicated in more than half of all transfusion-related fatalities reported to the FDA in 2006, a higher number than for any other single cause.13
At the same time, there is evidence that hemovigilance can reduce TRALI risk. In the United Kingdom, the Serious Hazards of Transfusion Steering Group introduced in late 2003 a policy of using plasma from male donors as much as possible, in view of the association of TRALI with plasma from multiparous female donors. The effort appeared to pay off: whereas TRALI accounted for 6.8% of all transfusion-related adverse events reported in the United Kingdom during the period 1996–2003,16 this proportion declined to just 1.9% in 2006.17
Finally, despite the progress in screening blood for more established infections like HIV and the hepatitis viruses, some additional infections now must be considered when assessing blood supply safety. These include diseases newly recognized as being transmissible by blood, or for which blood donor screening is not currently available, or that are newly emergent infections for which the potential for spread by transfusion is unknown. For such diseases—which include malaria and West Nile virus—the risk of transmission through transfusion is low, as they are much more likely to be acquired by other means.
Transfusion and outcomes: Not a strong record
Transfusion has never undergone safety and efficacy evaluation by the FDA. Given the challenges of conducting a randomized study of transfusion in the perioperative setting, we may never have high-quality data to assess transfusion in this setting.
A few studies merit mention, however. The Transfusion Requirement in Critical Care (TRICC) trial was conducted in 838 critically ill patients in the intensive care setting.18 Patients were randomized to a strategy of either liberal transfusion (begun when hemoglobin fell below 10 g/dL) or restrictive transfusion (begun when hemoglobin fell below 7 g/dL). Thirty-day mortality was similar between patients in the two strategy groups, but the restrictive strategy was associated with significantly lower mortality in at least two subgroups: patients with myocardial infarction and patients with pulmonary edema. Further subgroup analysis found no benefit of early or aggressive transfusion in patients with coronary artery disease or in those requiring mechanical ventilation.
Rao et al performed a meta-analysis of three large international trials of patients with acute coronary syndromes to determine whether blood transfusion to correct anemia in this setting was associated with improved survival.19 They found significantly higher mortality among patients who underwent transfusion compared with those who did not, prompting them to urge caution in the use of transfusion to maintain arbitrary hematocrit levels in stable patients with ischemic heart disease.
Similarly, a risk-adjusted, propensity-matched analysis of 6,301 patients undergoing noncardiac surgery found that receipt of 4 U of blood or more was a predictor of greater mortality, higher risk of infection, and longer hospital stay.20 Moreover, in an observational cohort study of 11,963 patients who underwent isolated coronary artery bypass graft surgery, each unit of red blood cells transfused was associated with an incrementally increased risk of adverse outcome (eg, mortality, renal injury, need for ventilator support, lengthened hospital stay, infection).21 The latter study found that transfusion was the single factor most reliably associated with increased risk of postoperative morbidity.
Additional studies have echoed these findings—ie, that perioperative blood transfusion has been associated with a host of adverse outcomes, including increased morbidity and length of stay, increased rates of postoperative infection, as well as immunosuppression, viral transmission, and acute transfusion reactions.5,22,23
Outcomes and duration of blood storage
An interesting factor in the relation between transfusion and outcomes is the shelf life of the blood being transfused. The FDA currently allows storage of blood for a maximum of 42 days, but a recent study of patients who received red blood cell transfusions during cardiac surgery found that those who received “older blood” (stored for > 14 days) had significantly higher rates of sepsis, prolonged intubation, renal failure, in-hospital mortality, and 1-year mortality compared with those who received “newer blood” (stored for ≤ 14 days).24
These differing outcomes are generally attributed to the so-called storage defect: as blood gets older, it loses components such as 2,3-DPG and adenosine disphosphate, its red cells lose deformability, and it undergoes buildup of cytokines and free hemoglobin. Increased demand for newer blood in light of the storage defect could further intensify pressures on the blood supply.
MANAGEMENT OF PERIOPERATIVE ANEMIA
In light of these shortcomings of blood transfusion, how should anemia be managed perioperatively to reduce or avoid the need for transfusion?
Preoperative evaluation
Vigilance for anemia and related issues in the preoperative evaluation is fundamental. The evaluation should elicit a history of bleeding tendencies, previous transfusions, and symptoms of anemia. Medications should be reviewed with an eye toward any that may predispose to perioperative bleeding and anemia, such as aspirin, clopidogrel, and anticoagulants. During the physical examination, alertness for pallor and petechiae is key, as is attentiveness to symptoms of anemia such as shortness of breath and fatigue.
Overview of management options
Once the cause of anemia is identified, the choice for optimal medical management can be made. Choices broadly consist of pharmacologic and technological options. The former include iron supplements and erythropoiesis-stimulating agents. Among other pharmacologic options are thrombin, collagen, fibrin glue, tranexamic acid, and aminocaproic acid, but these agents are less well studied and will not be discussed here. Technological options include preoperative autologous blood donation, cell salvage, and acute normovolemic hemodilution.
In addition to these options, careful management of anticoagulant and antiplatelet medications should be provided, including discontinuation or substitution of drugs that could hamper clotting perioperatively.
PHARMACOLOGIC OPTIONS
Iron supplementation
Oral iron is available in four preparations: ferrous sulfate, ferrous gluconate, ferrous fumarate, and iron polysaccharide. Gastrointestinal side effects may limit these preparations’ tolerability. Iron supplements with a high elemental value will require fewer pills and fewer doses, reducing the risk or frequency of side effects.
Intravenous (IV) iron preparations are much safer now than they were years ago, when anaphylactic reactions were a concern. The ones generally used in the perioperative setting are iron sucrose and iron gluconate. Unlike the older IV preparations, the use of iron sucrose and iron gluconate often requires a second dose. The effect on hemoglobin levels usually occurs starting at 1 week, with the maximum effect achieved at 2 weeks. Hypotension, arthralgia, abdominal discomfort, and back pain are potential side effects of IV iron.
Efficacy and safety of iron supplementation. Evidence of the efficacy of preoperative iron supplementation is mounting. A study of 569 patients undergoing colorectal cancer surgery found that among the 116 patients who were anemic, intraoperative transfusion was needed in a significantly lower proportion of those who received 2 weeks of preoperative oral iron supplementation (200 mg) compared with those who received no iron therapy (9.4% vs 27.4%; P < .05).26 Similarly, in an uncontrolled study, 10 days of IV iron sucrose starting 4 weeks preoperatively significantly increased hemoglobin levels in 20 patients with iron-deficiency anemia prior to elective orthopedic surgery.27
Risks of infection and cancer progression have been concerns with IV iron therapy. However, no significant association between IV iron therapy and bacteremia was identified in a prospective study of 985 patients receiving chronic hemodialysis.28 The effect of IV iron administration on tumor progression has not been prospectively studied.
In general, IV iron, especially the newer forms, is a safer alternative to blood transfusion. Death occurs at a much lower rate with iron than with blood transfusion (0.4 per million vs 4 per million, respectively), as do life-threatening adverse events (4 per million vs 10 per million, respectively), according to a systematic review by the Network for Advancement of Transfusion Alternatives.29
Erythropoiesis-stimulating agents
Erythropoiesis-stimulating agents (ESAs) include epoetin alfa (erythropoietin), first approved by the FDA in 1989, and the more recently introduced darbepoetin alfa. They are approved to treat anemia in several patient populations, but only epoetin alfa is approved by the FDA explicitly for use in patients undergoing major surgery (to reduce the need for blood transfusions). The ESAs have come under intense scrutiny in recent years over their risk-to-benefit ratio, as detailed below.
The preoperative dosing schedule for epoetin alfa is usually three weekly doses (plus a fourth dose on the day of surgery) if the surgery is scheduled 3 or more weeks in advance. However, daily dosing can be used effectively if the preoperative period is less than 3 weeks, provided that it is continued until 4 days after surgery. Oral iron is necessary throughout the course of epoetin alfa therapy.
Efficacy in reducing transfusions. In a systematic review published in 1998, epoetin alfa was shown to minimize perioperative exposure to allogeneic blood transfusion in patients undergoing orthopedic or cardiac surgery.30 Its benefit was greatest in patients at the highest risk of requiring transfusion. It was effective whether given daily or weekly, and did not significantly increase the risk of thrombotic events when used in surgical patients, although some studies did find an excess of thrombotic events with its use.
In three randomized trials conducted in patients undergoing joint arthroplasty (hip or knee), epoetin alfa was associated with substantial and significant reductions in perioperative blood transfusion compared with placebo or preoperative autologous blood donation.31–33 Rates of deep vein thrombosis (DVT) did not differ significantly between the epoetin alfa and placebo groups.
Concerns over perioperative thromboembolic risk. In early 2007, the FDA was made aware of preliminary results of an open-label study in which 681 patients undergoing elective spinal surgery who did not receive prophylactic anticoagulation were randomized to epoetin alfa plus standard-of-care therapy (pneumatic compression) or standard-of-care therapy alone.34,35 The incidence of DVT was 4.7% in patients treated with epoetin alfa compared with 2.1% in those not receiving epoetin alfa. It is important to note that the available ESAs are prothrombotic and increase thrombotic risk significantly, especially in populations like this one in which pharmacologic DVT prophylaxis is not routinely used.
Based in part on this study, the FDA in 2007 required a boxed warning to be added to the ESAs’ package inserts to specify the increased risk of DVT with their use in surgical patients not receiving prophylactic anticoagulation. The warning urges consideration of the use of DVT prophylaxis in surgical patients receiving an ESA.34,35
TECHNOLOGICAL OPTIONS AND OTHER STRATEGIES
Autologous blood donation: A practice in decline
In cases of elective surgery, autologous blood donation can be used to protect against disease transmission and overcome the challenge of blood type compatibility. Preoperative autologous donation of blood has been a prevalent practice, but its use is declining. One reason is that waste is high (approximately 50% at Cleveland Clinic), which makes this practice more costly than is often realized. Also, autologous blood donation increases the likelihood that the patient will be anemic on the day of surgery, so that he or she may still need allogeneic blood after all, defeating the initial purpose. Despite these limitations, preoperative autologous blood donation remains a useful option for a subset of patients with multiple antibodies for whom donor blood may be difficult to obtain.
Cell salvage
Cell salvage is an innovative technology that recovers the patient’s own blood (after being shed from the surgical incision) for transfusion after filtering and washing. It is particularly well suited to procedures that involve massive blood loss. Cell savage requires technical expertise, however, and involves costs associated with both the machine and disposables.
Restricted postoperative phlebotomy
Phlebotomy accounts for a significant amount of blood loss, especially in intensive care patients with arterial lines. The equivalent of 30% of total blood transfused has been reported to be lost to phlebotomy during an intensive care unit stay.36 Triggers for transfusion cannot be assigned universally based on blood loss from phlebotomy but must consider the patient’s hemodynamic status, cardiac reserve, and other clinical characteristics.
PROMOTING RESPONSIBLE BLOOD PRODUCT USE
Blood is expensive, and in recent years hospitals have experienced increases in the cost of blood and blood products. To promote responsible blood use, we have developed a multipronged approach to blood management at Cleveland Clinic. The program’s cornerstone is increased awareness of the risks associated with blood transfusions. The emphasis is on educating staff physicians and other caregivers about the appropriate use of blood products. We also have implemented a new policy requiring staff authorization for all blood requested in nonemergency situations. Additionally, requests for blood components require adherence to an indication-based ordering process. Finally, data about blood use are shared transparently among physicians, encouraging good clinical practice.
In the first 7 months of the program, we observed decreased utilization of blood products in the inpatient setting. Notably, the reduction in blood use was significantly greater in the surgical population than in the medical population.
CONCULSIONS
Anemia is associated with increased morbidity and mortality in the perioperative setting. Perioperative blood transfusion is one method of raising hemoglobin levels in anemic surgical patients, but it increases perioperative morbidity in the form of acute transfusion reactions, immunosuppression, postoperative infection, and longer hospital stays. Moreover, blood collection continues to lag blood demand. For these reasons, most relevant major medical organizations—including the Association of Blood Banks, the American Red Cross, and the FDA—advise that red blood cell–containing components should not be used to treat anemias that can be corrected with medications. These medical alternatives—all of which can be used in the perioperative setting—include iron supplementation, vitamin B12, and ESAs in select patient groups.
DISCUSSION
Question from the audience: Are there risks involved with autologous blood donation? Are different hemoglobin thresholds used when a patient’s own blood is used?
Dr. Kumar: As I mentioned, preoperative autologous donation is a technique that is less frequently used in our hospital. Autologous transfusion is considered safe only for patients who come to the clinic with normal hemoglobin values. Some patients may not have recovered from their blood loss by the time they come to surgery, so you end up needing to give them more blood because they started out anemic.
Question from the audience: Is there risk to giving patients back their own blood? Do you have to worry about transfusion-induced lung injury, sepsis, or other complications?
Dr. Kumar: As with allogeneic blood, the risk of clerical or clinical error exists with autologous blood: it too needs to be kept on the shelf, taken out, and infused, and the risk of sepsis remains the same.
Anemia is a potent risk factor for mortality and morbidity in surgical patients, and its management has begun to shift away from allogeneic blood transfusion in recent years. This article reviews the clinical importance of perioperative anemia, the role and shortcomings of blood transfusion, and the pros and cons of alternative approaches to managing perioperative anemia. I conclude with an overview of a program for perioperative blood product use at my institution, Cleveland Clinic.
SIGNIFICANCE OF PERIOPERATIVE ANEMIA
Prevalence depends on many factors
The reported prevalence of anemia in surgical patients varies widely—from 5% to 76%1—and depends on the patient’s disease and comorbidities, the surgical procedure and associated blood loss, and the definition of anemia used. The prevalence of preoperative anemia increases with patient age and is higher in women than in men.2
A multiplier of risk
Anemia is an important multiplier of mortality risk. For example, the presence of anemia raises the relative risk of 2-year mortality from 2.05 to 3.37 in patients with chronic kidney disease, from 2.86 to 3.78 in patients with heart failure, and from 4.86 to 6.07 in patients with concomitant heart failure and chronic kidney disease.3
Adverse effects of anemia have been demonstrated specifically in the perioperative setting as well. A large retrospective cohort study showed that a preoperative hemoglobin concentration of less than 6 g/dL increases the risk of death 30 days after surgery by a factor of 26 relative to a concentration of 12 g/dL or greater in surgical patients who declined blood transfusion for religious reasons.4 The anemia-associated mortality risk was especially pronounced among patients with cardiovascular disease.4 Other studies have demonstrated perioperative anemia to be associated with increases in the risk of death,5 cardiac events,6 pneumonia,7 and postoperative delirium.8
IS BLOOD TRANSFUSION THE ANSWER
The use of allogeneic blood transfusion to manage anemia and blood loss is a concept that originated several centuries ago and has changed little over the years.
Blood supply challenges
Blood collection has historically lagged demand, resulting in a blood supply insufficient to meet transfusion needs. According to the federal government’s 2007 National Blood Collection and Utilization Survey Report, 6.89% of US hospitals reported that they cancelled elective surgery on 1 or more days in the prior year because of a lack of blood availability, and 13.5% experienced at least 1 day in which nonsurgical blood needs could not be met.9 Unless practices are changed to increase blood donation, these unmet tranfusion needs may grow.
Joint Commission set to measure blood management
In response to this challenge, an advisory panel formed by the Joint Commission has identified 17 performance measures related to blood conservation and appropriate transfusion.10 These measures are currently in development, and we expect to see some types of metrics in the near future. Such metrics are likely to further prioritize blood management for US hospitals.
Safety of the blood supply: Viral transmission down, TRALI risk persists
The safety of the blood supply has improved markedly. Sophisticated testing and public demand have led to a dramatic decline in the risk of transfusion-related transmission of HIV, hepatitis C virus, and hepatitis B virus.11
Despite this progress, the risk of transfusion-related acute lung injury (TRALI) has persisted in recent years. TRALI is characterized by acute onset of noncardiogenic pulmonary edema within 6 hours of blood product transfusion. Believed to be immune-mediated, TRALI is thought to occur as antibodies to human leukocyte antigens develop, inducing capillary leak syndrome.12 The patients most commonly affected are those who receive plasma from multiparous female donors. A recent evaluation of transfusion-related fatalities reported to the US Food and Drug Administration (FDA) revealed a continual rise in fatal TRALI cases in the United States from 2001 to 2006.13–15 TRALI was implicated in more than half of all transfusion-related fatalities reported to the FDA in 2006, a higher number than for any other single cause.13
At the same time, there is evidence that hemovigilance can reduce TRALI risk. In the United Kingdom, the Serious Hazards of Transfusion Steering Group introduced in late 2003 a policy of using plasma from male donors as much as possible, in view of the association of TRALI with plasma from multiparous female donors. The effort appeared to pay off: whereas TRALI accounted for 6.8% of all transfusion-related adverse events reported in the United Kingdom during the period 1996–2003,16 this proportion declined to just 1.9% in 2006.17
Finally, despite the progress in screening blood for more established infections like HIV and the hepatitis viruses, some additional infections now must be considered when assessing blood supply safety. These include diseases newly recognized as being transmissible by blood, or for which blood donor screening is not currently available, or that are newly emergent infections for which the potential for spread by transfusion is unknown. For such diseases—which include malaria and West Nile virus—the risk of transmission through transfusion is low, as they are much more likely to be acquired by other means.
Transfusion and outcomes: Not a strong record
Transfusion has never undergone safety and efficacy evaluation by the FDA. Given the challenges of conducting a randomized study of transfusion in the perioperative setting, we may never have high-quality data to assess transfusion in this setting.
A few studies merit mention, however. The Transfusion Requirement in Critical Care (TRICC) trial was conducted in 838 critically ill patients in the intensive care setting.18 Patients were randomized to a strategy of either liberal transfusion (begun when hemoglobin fell below 10 g/dL) or restrictive transfusion (begun when hemoglobin fell below 7 g/dL). Thirty-day mortality was similar between patients in the two strategy groups, but the restrictive strategy was associated with significantly lower mortality in at least two subgroups: patients with myocardial infarction and patients with pulmonary edema. Further subgroup analysis found no benefit of early or aggressive transfusion in patients with coronary artery disease or in those requiring mechanical ventilation.
Rao et al performed a meta-analysis of three large international trials of patients with acute coronary syndromes to determine whether blood transfusion to correct anemia in this setting was associated with improved survival.19 They found significantly higher mortality among patients who underwent transfusion compared with those who did not, prompting them to urge caution in the use of transfusion to maintain arbitrary hematocrit levels in stable patients with ischemic heart disease.
Similarly, a risk-adjusted, propensity-matched analysis of 6,301 patients undergoing noncardiac surgery found that receipt of 4 U of blood or more was a predictor of greater mortality, higher risk of infection, and longer hospital stay.20 Moreover, in an observational cohort study of 11,963 patients who underwent isolated coronary artery bypass graft surgery, each unit of red blood cells transfused was associated with an incrementally increased risk of adverse outcome (eg, mortality, renal injury, need for ventilator support, lengthened hospital stay, infection).21 The latter study found that transfusion was the single factor most reliably associated with increased risk of postoperative morbidity.
Additional studies have echoed these findings—ie, that perioperative blood transfusion has been associated with a host of adverse outcomes, including increased morbidity and length of stay, increased rates of postoperative infection, as well as immunosuppression, viral transmission, and acute transfusion reactions.5,22,23
Outcomes and duration of blood storage
An interesting factor in the relation between transfusion and outcomes is the shelf life of the blood being transfused. The FDA currently allows storage of blood for a maximum of 42 days, but a recent study of patients who received red blood cell transfusions during cardiac surgery found that those who received “older blood” (stored for > 14 days) had significantly higher rates of sepsis, prolonged intubation, renal failure, in-hospital mortality, and 1-year mortality compared with those who received “newer blood” (stored for ≤ 14 days).24
These differing outcomes are generally attributed to the so-called storage defect: as blood gets older, it loses components such as 2,3-DPG and adenosine disphosphate, its red cells lose deformability, and it undergoes buildup of cytokines and free hemoglobin. Increased demand for newer blood in light of the storage defect could further intensify pressures on the blood supply.
MANAGEMENT OF PERIOPERATIVE ANEMIA
In light of these shortcomings of blood transfusion, how should anemia be managed perioperatively to reduce or avoid the need for transfusion?
Preoperative evaluation
Vigilance for anemia and related issues in the preoperative evaluation is fundamental. The evaluation should elicit a history of bleeding tendencies, previous transfusions, and symptoms of anemia. Medications should be reviewed with an eye toward any that may predispose to perioperative bleeding and anemia, such as aspirin, clopidogrel, and anticoagulants. During the physical examination, alertness for pallor and petechiae is key, as is attentiveness to symptoms of anemia such as shortness of breath and fatigue.
Overview of management options
Once the cause of anemia is identified, the choice for optimal medical management can be made. Choices broadly consist of pharmacologic and technological options. The former include iron supplements and erythropoiesis-stimulating agents. Among other pharmacologic options are thrombin, collagen, fibrin glue, tranexamic acid, and aminocaproic acid, but these agents are less well studied and will not be discussed here. Technological options include preoperative autologous blood donation, cell salvage, and acute normovolemic hemodilution.
In addition to these options, careful management of anticoagulant and antiplatelet medications should be provided, including discontinuation or substitution of drugs that could hamper clotting perioperatively.
PHARMACOLOGIC OPTIONS
Iron supplementation
Oral iron is available in four preparations: ferrous sulfate, ferrous gluconate, ferrous fumarate, and iron polysaccharide. Gastrointestinal side effects may limit these preparations’ tolerability. Iron supplements with a high elemental value will require fewer pills and fewer doses, reducing the risk or frequency of side effects.
Intravenous (IV) iron preparations are much safer now than they were years ago, when anaphylactic reactions were a concern. The ones generally used in the perioperative setting are iron sucrose and iron gluconate. Unlike the older IV preparations, the use of iron sucrose and iron gluconate often requires a second dose. The effect on hemoglobin levels usually occurs starting at 1 week, with the maximum effect achieved at 2 weeks. Hypotension, arthralgia, abdominal discomfort, and back pain are potential side effects of IV iron.
Efficacy and safety of iron supplementation. Evidence of the efficacy of preoperative iron supplementation is mounting. A study of 569 patients undergoing colorectal cancer surgery found that among the 116 patients who were anemic, intraoperative transfusion was needed in a significantly lower proportion of those who received 2 weeks of preoperative oral iron supplementation (200 mg) compared with those who received no iron therapy (9.4% vs 27.4%; P < .05).26 Similarly, in an uncontrolled study, 10 days of IV iron sucrose starting 4 weeks preoperatively significantly increased hemoglobin levels in 20 patients with iron-deficiency anemia prior to elective orthopedic surgery.27
Risks of infection and cancer progression have been concerns with IV iron therapy. However, no significant association between IV iron therapy and bacteremia was identified in a prospective study of 985 patients receiving chronic hemodialysis.28 The effect of IV iron administration on tumor progression has not been prospectively studied.
In general, IV iron, especially the newer forms, is a safer alternative to blood transfusion. Death occurs at a much lower rate with iron than with blood transfusion (0.4 per million vs 4 per million, respectively), as do life-threatening adverse events (4 per million vs 10 per million, respectively), according to a systematic review by the Network for Advancement of Transfusion Alternatives.29
Erythropoiesis-stimulating agents
Erythropoiesis-stimulating agents (ESAs) include epoetin alfa (erythropoietin), first approved by the FDA in 1989, and the more recently introduced darbepoetin alfa. They are approved to treat anemia in several patient populations, but only epoetin alfa is approved by the FDA explicitly for use in patients undergoing major surgery (to reduce the need for blood transfusions). The ESAs have come under intense scrutiny in recent years over their risk-to-benefit ratio, as detailed below.
The preoperative dosing schedule for epoetin alfa is usually three weekly doses (plus a fourth dose on the day of surgery) if the surgery is scheduled 3 or more weeks in advance. However, daily dosing can be used effectively if the preoperative period is less than 3 weeks, provided that it is continued until 4 days after surgery. Oral iron is necessary throughout the course of epoetin alfa therapy.
Efficacy in reducing transfusions. In a systematic review published in 1998, epoetin alfa was shown to minimize perioperative exposure to allogeneic blood transfusion in patients undergoing orthopedic or cardiac surgery.30 Its benefit was greatest in patients at the highest risk of requiring transfusion. It was effective whether given daily or weekly, and did not significantly increase the risk of thrombotic events when used in surgical patients, although some studies did find an excess of thrombotic events with its use.
In three randomized trials conducted in patients undergoing joint arthroplasty (hip or knee), epoetin alfa was associated with substantial and significant reductions in perioperative blood transfusion compared with placebo or preoperative autologous blood donation.31–33 Rates of deep vein thrombosis (DVT) did not differ significantly between the epoetin alfa and placebo groups.
Concerns over perioperative thromboembolic risk. In early 2007, the FDA was made aware of preliminary results of an open-label study in which 681 patients undergoing elective spinal surgery who did not receive prophylactic anticoagulation were randomized to epoetin alfa plus standard-of-care therapy (pneumatic compression) or standard-of-care therapy alone.34,35 The incidence of DVT was 4.7% in patients treated with epoetin alfa compared with 2.1% in those not receiving epoetin alfa. It is important to note that the available ESAs are prothrombotic and increase thrombotic risk significantly, especially in populations like this one in which pharmacologic DVT prophylaxis is not routinely used.
Based in part on this study, the FDA in 2007 required a boxed warning to be added to the ESAs’ package inserts to specify the increased risk of DVT with their use in surgical patients not receiving prophylactic anticoagulation. The warning urges consideration of the use of DVT prophylaxis in surgical patients receiving an ESA.34,35
TECHNOLOGICAL OPTIONS AND OTHER STRATEGIES
Autologous blood donation: A practice in decline
In cases of elective surgery, autologous blood donation can be used to protect against disease transmission and overcome the challenge of blood type compatibility. Preoperative autologous donation of blood has been a prevalent practice, but its use is declining. One reason is that waste is high (approximately 50% at Cleveland Clinic), which makes this practice more costly than is often realized. Also, autologous blood donation increases the likelihood that the patient will be anemic on the day of surgery, so that he or she may still need allogeneic blood after all, defeating the initial purpose. Despite these limitations, preoperative autologous blood donation remains a useful option for a subset of patients with multiple antibodies for whom donor blood may be difficult to obtain.
Cell salvage
Cell salvage is an innovative technology that recovers the patient’s own blood (after being shed from the surgical incision) for transfusion after filtering and washing. It is particularly well suited to procedures that involve massive blood loss. Cell savage requires technical expertise, however, and involves costs associated with both the machine and disposables.
Restricted postoperative phlebotomy
Phlebotomy accounts for a significant amount of blood loss, especially in intensive care patients with arterial lines. The equivalent of 30% of total blood transfused has been reported to be lost to phlebotomy during an intensive care unit stay.36 Triggers for transfusion cannot be assigned universally based on blood loss from phlebotomy but must consider the patient’s hemodynamic status, cardiac reserve, and other clinical characteristics.
PROMOTING RESPONSIBLE BLOOD PRODUCT USE
Blood is expensive, and in recent years hospitals have experienced increases in the cost of blood and blood products. To promote responsible blood use, we have developed a multipronged approach to blood management at Cleveland Clinic. The program’s cornerstone is increased awareness of the risks associated with blood transfusions. The emphasis is on educating staff physicians and other caregivers about the appropriate use of blood products. We also have implemented a new policy requiring staff authorization for all blood requested in nonemergency situations. Additionally, requests for blood components require adherence to an indication-based ordering process. Finally, data about blood use are shared transparently among physicians, encouraging good clinical practice.
In the first 7 months of the program, we observed decreased utilization of blood products in the inpatient setting. Notably, the reduction in blood use was significantly greater in the surgical population than in the medical population.
CONCULSIONS
Anemia is associated with increased morbidity and mortality in the perioperative setting. Perioperative blood transfusion is one method of raising hemoglobin levels in anemic surgical patients, but it increases perioperative morbidity in the form of acute transfusion reactions, immunosuppression, postoperative infection, and longer hospital stays. Moreover, blood collection continues to lag blood demand. For these reasons, most relevant major medical organizations—including the Association of Blood Banks, the American Red Cross, and the FDA—advise that red blood cell–containing components should not be used to treat anemias that can be corrected with medications. These medical alternatives—all of which can be used in the perioperative setting—include iron supplementation, vitamin B12, and ESAs in select patient groups.
DISCUSSION
Question from the audience: Are there risks involved with autologous blood donation? Are different hemoglobin thresholds used when a patient’s own blood is used?
Dr. Kumar: As I mentioned, preoperative autologous donation is a technique that is less frequently used in our hospital. Autologous transfusion is considered safe only for patients who come to the clinic with normal hemoglobin values. Some patients may not have recovered from their blood loss by the time they come to surgery, so you end up needing to give them more blood because they started out anemic.
Question from the audience: Is there risk to giving patients back their own blood? Do you have to worry about transfusion-induced lung injury, sepsis, or other complications?
Dr. Kumar: As with allogeneic blood, the risk of clerical or clinical error exists with autologous blood: it too needs to be kept on the shelf, taken out, and infused, and the risk of sepsis remains the same.
- Shander A, Knight K, Thurer R, Adamson J, Spence R. Prevalence and outcomes of anemia in surgery: a systematic review of the literature. Am J Med 2004; 116(suppl 7A):58S–69S.
- Kulier A, Gombotz H. Perioperative anemia [in German]. Anaesthesist 2001; 50:73–86.
- Herzog CA, Muster HA, Li S, Collins AJ. Impact of congestive heart failure, chronic kidney disease, and anemia on survival in the Medicare population. J Card Fail 2004; 10:467–472.
- Carson JL, Duff A, Poses RM, et al. Effect of anaemia and cardiovascular disease on surgical mortality and morbidity. Lancet 1996; 348:1055–1060.
- Gruson KI, Aharonoff GB, Egol KA, Zuckerman JD, Koval KJ. The relationship between admission hemoglobin level and outcome after hip fracture. J Orthop Trauma 2002; 16:39–44.
- Nelson AH, Fleisher LA, Rosenbaum SH. Relationship between postoperative anemia and cardiac morbidity in high-risk vascular patients in the intensive care unit. Crit Care Med 1993; 21:860–866.
- Faris PM, Spence RK, Larholt KM, Sampson AR, Frei D. The predictive power of baseline hemoglobin for transfusion risk in surgery patients. Orthopedics 1999; 22(suppl 1):s135–s140.
- Marcantonio ER, Goldman L, Orav EJ, Cook EF, Lee TH. The association of intraoperative factors with the development of postoperative delirium. Am J Med 1998; 105:380–384.
- US Department of Health and Human Services. The 2007 National Blood Collection and Utilization Survey. Available at: http://www.aabb.org/Documents/Programs_and_Services/Data_Center/07nbcusrpt.pdf. Accessed March 9, 2009.
- The Joint Commission. Performance measurement initiatives. Available at http://www.jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/Blood+Management+-+Utilization.htm.
- Busch MP, Kleinman SH, Nemo GJ. Current and emerging infectious risks of blood transfusions. JAMA 2003; 289:959–962.
- Silliman CC, Ambruso DR, Boshkov LK. Transfusion-related acute lung injury. Blood 2005; 105:2266–2273.
- Benjamin RJ. Transfusion and transplantation safety: American Red Cross concerns. PowerPoint slides presented at Department of Health and Human Services Advisory Committee on Blood Safety and Availability meeting, May 10–11, 2007. Available at: http://www.hhs.gov/ophs/bloodsafety/presentations/Benjamin0507.pdf. Accessed March 9, 2009.
- Holness L. Transfusion related acute lung injury (TRALI): the FDA current view. PowerPoint slides presented at FDA Blood Products Advisory Committee meeting, July 22–23, 2004. Available at: http://www.fda.gov/OHRMS/DOCKETS/ac/04/briefing/2004-4057b1_01.pdf. Accessed March 9, 2009.
- Williams AE. Transfusion related acute lung injury (TRALI). PowerPoint slides presented at FDA Blood Products Advisory Committee meeting, April 27, 2007. Available at: http://www.fda.gov/ohrms/dockets/ac/07/slides/2007-4300S2-05.ppt. Accessed March 9, 2009.
- Stainsby D, Cohen H, Jones H, et al. Serious Hazards of Transfusion—Annual Report 2003. Published July 5, 2004. Available at: http://www.shotuk.org/SHOT%20Report%202003.pdf. Accessed April 29, 2009.
- Taylor C, Cohen H, Stainsby D, et al. Serious Hazards of Transfusion—Annual Report 2006. Published November 20, 2007. Available at: http://www.shotuk.org/SHOT_report_2006.pdf. Accessed April 29, 2009.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999; 340:409–417.
- Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004; 292:1555–1562.
- Dunne JR, Malone D, Tracy JK, et al. Perioperative anemia: an independent risk factor for infection, mortality, and resource utilization in surgery. J Surg Res 2002; 102:237–244.
- Koch CG, Li L, Duncan AI, et al. Morbidity and mortality risk associated with red blood cell and blood-component transfusion in isolated coronary artery bypass grafting. Crit Care Med 2006; 34:1608–1616.
- Rady MY, Ryan T, Starr NJ. Perioperative determinants of morbidity and mortality in elderly patients undergoing cardiac surgery. Crit Care Med 1998; 26:225–235.
- Goodnough LT, Brecher ME, Kanter MH, AuBuchon JP. Transfusion medicine. First of two parts—blood transfusion. N Engl J Med 1999; 340:438–447.
- Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med 2008; 358:1229–1239.
- Goodnough LT, Shander A. Blood management. Arch Pathol Lab Med 2007; 131:695–701.
- Okuyama M, Ikeda K, Shibata T, et al. Preoperative iron supplementation and intraoperative transfusion during colorectal cancer surgery. Surg Today 2005; 35:36–40.
- Theusinger OM, Leyvraz PF, Schanz U, et al. Treatment of iron deficiency anemia in orthopedic surgery with intravenous iron: efficacy and limits: a prospective study. Anesthesiology 2007; 107:923–927.
- Hoen B, Paul-Dauphin A, Kessler M. Intravenous iron administration does not significantly increase the risk of bacteremia in chronic hemodialysis patients. Clin Nephrol 2002; 57:457–461.
- Beris P, Muñoz M, García-Erce JA, et al. Perioperative anaemia management: consensus statement on the role of intravenous iron. Br J Anaesth 2008; 100:599–604.
- Laupacis A, Fergusson D. Erythropoietin to minimize perioperative blood transfusion: a systematic review of randomized trials: The International Study of Perioperative Transfusion (ISPOT) Investigators. Transfus Med 1998; 8:309–317.
- Feagan BG, Wong CJ, Kirkley A, et al. Erythropoietin with iron supplementation to prevent allogeneic blood transfusion in total hip joint arthroplasty: a randomized, controlled trial. Ann Intern Med 2000; 133:845–854.
- Stowell CP, Chandler H, Jové M, et al. An open-label, randomized study to compare the safety and efficacy of perioperative epoetin alfa with preoperative autologous blood donation in total joint arthroplasty. Orthopedics 1999; 22(suppl 1):s105–s112.
- de Andrade JR, Jové M, Landon G, et al. Baseline hemoglobin as a predictor of risk of transfusion and response to Epoetin alfa in orthopedic surgery patients. Am J Orthop 1996; 25:533–542.
- Procrit [package insert]. Raritan, NJ: Ortho Biotech Products LP; 2009.
- Epogen [package insert]. Thousand Oaks, CA: Amgen Inc.; 2009.
- Smoller BR, Kuskall MS. Phlebotomy for diagnostic laboratory tests in adults: pattern of use and effect on transfusion requirements. N Engl J Med 1986; 314:1233–1235.
- Shander A, Knight K, Thurer R, Adamson J, Spence R. Prevalence and outcomes of anemia in surgery: a systematic review of the literature. Am J Med 2004; 116(suppl 7A):58S–69S.
- Kulier A, Gombotz H. Perioperative anemia [in German]. Anaesthesist 2001; 50:73–86.
- Herzog CA, Muster HA, Li S, Collins AJ. Impact of congestive heart failure, chronic kidney disease, and anemia on survival in the Medicare population. J Card Fail 2004; 10:467–472.
- Carson JL, Duff A, Poses RM, et al. Effect of anaemia and cardiovascular disease on surgical mortality and morbidity. Lancet 1996; 348:1055–1060.
- Gruson KI, Aharonoff GB, Egol KA, Zuckerman JD, Koval KJ. The relationship between admission hemoglobin level and outcome after hip fracture. J Orthop Trauma 2002; 16:39–44.
- Nelson AH, Fleisher LA, Rosenbaum SH. Relationship between postoperative anemia and cardiac morbidity in high-risk vascular patients in the intensive care unit. Crit Care Med 1993; 21:860–866.
- Faris PM, Spence RK, Larholt KM, Sampson AR, Frei D. The predictive power of baseline hemoglobin for transfusion risk in surgery patients. Orthopedics 1999; 22(suppl 1):s135–s140.
- Marcantonio ER, Goldman L, Orav EJ, Cook EF, Lee TH. The association of intraoperative factors with the development of postoperative delirium. Am J Med 1998; 105:380–384.
- US Department of Health and Human Services. The 2007 National Blood Collection and Utilization Survey. Available at: http://www.aabb.org/Documents/Programs_and_Services/Data_Center/07nbcusrpt.pdf. Accessed March 9, 2009.
- The Joint Commission. Performance measurement initiatives. Available at http://www.jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/Blood+Management+-+Utilization.htm.
- Busch MP, Kleinman SH, Nemo GJ. Current and emerging infectious risks of blood transfusions. JAMA 2003; 289:959–962.
- Silliman CC, Ambruso DR, Boshkov LK. Transfusion-related acute lung injury. Blood 2005; 105:2266–2273.
- Benjamin RJ. Transfusion and transplantation safety: American Red Cross concerns. PowerPoint slides presented at Department of Health and Human Services Advisory Committee on Blood Safety and Availability meeting, May 10–11, 2007. Available at: http://www.hhs.gov/ophs/bloodsafety/presentations/Benjamin0507.pdf. Accessed March 9, 2009.
- Holness L. Transfusion related acute lung injury (TRALI): the FDA current view. PowerPoint slides presented at FDA Blood Products Advisory Committee meeting, July 22–23, 2004. Available at: http://www.fda.gov/OHRMS/DOCKETS/ac/04/briefing/2004-4057b1_01.pdf. Accessed March 9, 2009.
- Williams AE. Transfusion related acute lung injury (TRALI). PowerPoint slides presented at FDA Blood Products Advisory Committee meeting, April 27, 2007. Available at: http://www.fda.gov/ohrms/dockets/ac/07/slides/2007-4300S2-05.ppt. Accessed March 9, 2009.
- Stainsby D, Cohen H, Jones H, et al. Serious Hazards of Transfusion—Annual Report 2003. Published July 5, 2004. Available at: http://www.shotuk.org/SHOT%20Report%202003.pdf. Accessed April 29, 2009.
- Taylor C, Cohen H, Stainsby D, et al. Serious Hazards of Transfusion—Annual Report 2006. Published November 20, 2007. Available at: http://www.shotuk.org/SHOT_report_2006.pdf. Accessed April 29, 2009.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999; 340:409–417.
- Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004; 292:1555–1562.
- Dunne JR, Malone D, Tracy JK, et al. Perioperative anemia: an independent risk factor for infection, mortality, and resource utilization in surgery. J Surg Res 2002; 102:237–244.
- Koch CG, Li L, Duncan AI, et al. Morbidity and mortality risk associated with red blood cell and blood-component transfusion in isolated coronary artery bypass grafting. Crit Care Med 2006; 34:1608–1616.
- Rady MY, Ryan T, Starr NJ. Perioperative determinants of morbidity and mortality in elderly patients undergoing cardiac surgery. Crit Care Med 1998; 26:225–235.
- Goodnough LT, Brecher ME, Kanter MH, AuBuchon JP. Transfusion medicine. First of two parts—blood transfusion. N Engl J Med 1999; 340:438–447.
- Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med 2008; 358:1229–1239.
- Goodnough LT, Shander A. Blood management. Arch Pathol Lab Med 2007; 131:695–701.
- Okuyama M, Ikeda K, Shibata T, et al. Preoperative iron supplementation and intraoperative transfusion during colorectal cancer surgery. Surg Today 2005; 35:36–40.
- Theusinger OM, Leyvraz PF, Schanz U, et al. Treatment of iron deficiency anemia in orthopedic surgery with intravenous iron: efficacy and limits: a prospective study. Anesthesiology 2007; 107:923–927.
- Hoen B, Paul-Dauphin A, Kessler M. Intravenous iron administration does not significantly increase the risk of bacteremia in chronic hemodialysis patients. Clin Nephrol 2002; 57:457–461.
- Beris P, Muñoz M, García-Erce JA, et al. Perioperative anaemia management: consensus statement on the role of intravenous iron. Br J Anaesth 2008; 100:599–604.
- Laupacis A, Fergusson D. Erythropoietin to minimize perioperative blood transfusion: a systematic review of randomized trials: The International Study of Perioperative Transfusion (ISPOT) Investigators. Transfus Med 1998; 8:309–317.
- Feagan BG, Wong CJ, Kirkley A, et al. Erythropoietin with iron supplementation to prevent allogeneic blood transfusion in total hip joint arthroplasty: a randomized, controlled trial. Ann Intern Med 2000; 133:845–854.
- Stowell CP, Chandler H, Jové M, et al. An open-label, randomized study to compare the safety and efficacy of perioperative epoetin alfa with preoperative autologous blood donation in total joint arthroplasty. Orthopedics 1999; 22(suppl 1):s105–s112.
- de Andrade JR, Jové M, Landon G, et al. Baseline hemoglobin as a predictor of risk of transfusion and response to Epoetin alfa in orthopedic surgery patients. Am J Orthop 1996; 25:533–542.
- Procrit [package insert]. Raritan, NJ: Ortho Biotech Products LP; 2009.
- Epogen [package insert]. Thousand Oaks, CA: Amgen Inc.; 2009.
- Smoller BR, Kuskall MS. Phlebotomy for diagnostic laboratory tests in adults: pattern of use and effect on transfusion requirements. N Engl J Med 1986; 314:1233–1235.
KEY POINTS
- Anemia is a potent multiplier of morbidity and mortality risk, including in the perioperative setting.
- The Joint Commission plans to implement a performance measure on blood management in the near future.
- While the safety of the blood supply has improved markedly from the standpoint of infection transmission, other risks from transfusion persist, including transfusion-related acute lung injury and emerging infections.
- The preoperative evaluation should elicit a history of bleeding tendencies, previous transfusions, and symptoms of anemia. Medications should be reviewed with an eye toward those that may need to be stopped to avoid a predisposition to bleeding (eg, antiplatelets, anticoagulants).
- Use of ESAs minimizes the need for blood transfusion in patients undergoing orthopedic and other surgeries, but they raise the risk of thromboembolism in the absence of prophylactic anticoagulation.