User login
Lead the Change
Modern medicine … certainly as it should be practiced by hospitalists, is the most information-intensive activity that human beings ever engaged in,” says Kenneth W. Kizer, MD, MPH, CEO and chairman of the board of Medsphere Systems Corporation in Aliso Viejo, Calif.
He should know. From his first healthcare-related position in 1969 as a hospital orderly at Stanford University Hospital, he rose to become the Under Secretary for Health in the Department of Veterans Affairs (VA)—the CEO of the largest healthcare system in the nation. He is widely credited as being the chief architect and driving force behind the successful transformation of VA healthcare in the 1990s.
The VA’s 154 hospitals and 875 clinics, which serve 5.4 million patients, have been rated “best in class” by a number of independent groups since it implemented the changes in the 1990s.1 In a study conducted by the Rand Corporation, the VA scored higher compared with the U.S. private sector hospitals in every category except acute care, in which “the numbers ran neck and neck,” says Dr. Kizer. “Where the VA has done much better [than private sector hospitals] is in managing chronic disease and integrating prevention and health maintenance into the acute care program.”
Differences between a VA facility and one in the private sector are mostly “cosmetic and in the financing,” says Dr. Kizer. “The VA takes care of a particular patient population—veterans of military service—but it is a civilian practice that happens to be run by the federal government.”
According to a July 17, 2006, article in BusinessWeek, “The Best Medical Care in the U.S.,” the VA system provides about two-thirds of the care protocols recommended by organizations such as the Agency for Healthcare Research and Quality, compared with 50% provided in private sector hospitals.1 Also, as many as 8% of the prescriptions filled in private sector hospitals contain errors, but the VA’s prescription-related accuracy is greater than 99.997%. In addition, the VA spends an average of $5,000 per patient compared with the national average of $6,300.
Dr. Kizer’s focus on quality improvement at the VA should not be surprising in view of his long-time focus on improving the quality of healthcare. In his mind, an essential element in improving the quality of American healthcare is the widespread adoption of electronic health records (EHR).
When he arrived at his post at the VA in 1994, Dr. Kizer was pleasantly surprised to find advanced automated information management in place. The VA had been working on developing an EHR since 1978. As part Kizer’s transformation of the VA, all of the VA’s information systems were integrated, and VistA (an acronym for Veterans Health Information Systems and Technology Architecture) was launched in 1997. VistA is often the first thing that VA-affiliated hospitalists mention when they are asked what distinguishes VA hospitals from non-VA hospitals.
Key Features and Benefits of the VA
Sanjay Saint, MD, knows a great deal about academically affiliated VAs. He was a resident (July 1993-June 1995) and then chief medical resident at the San Francisco VA (June 1995-June 1996), an affiliate of the University of California at San Francisco. He was also a fellow at the University of Washington-affiliated Seattle VA (July 1996-June 1998), and for more than eight years he has been on the faculty at the University of Michigan as a professor of internal medicine (1998-2006). Dr. Saint is currently a hospitalist at the University of Michigan-affiliated Ann Arbor VA Hospital. He was also recently the acting chief of medicine there for six months (Dec. 2005-May 2006) while the permanent chief was on sabbatical.
The instant availability of the EHR system is a key benefit of practicing in a VA hospital, says Dr. Saint. “It involves not only being able to get up-to-date, relevant patient information at our VA but also the information obtained if the patient has been seen at other VAs.”
“One of the reasons why [the VA’s EHR] is so good is that it is fully integrated,” says Dr. Kizer. “Everything was made to fit together to begin with—in contrast to essentially all commercial products, which have been melded together from pieces that come from a variety of origins. Being fully integrated certainly increases the speed and efficiency of operations. The second reason why VistA is so good is that it was developed by clinicians for clinicians … .”
A key feature operating as part of the EHR is the focus on computer-based provider order entry (CPOE). CPOE can help physicians make correct clinical decisions, says Dr. Saint. He cites the example of a pilot test he and co-workers conducted at the Seattle VA: After 72 hours of urinary catheterization in a patient, an alert reminded physicians to remove the catheter. From that simple type of quality improvement experiment, the data revealed that those patients for whom the reminder had been used had a significantly reduced rate of infection compared with those for whom it had not.
One particularly good, but perhaps underutilized, aspect of the computerized system is the use of care protocols or models that can be used across the VA, says Peter Kaboli, MD, MS, hospitalist at the Iowa City VA Hospital, an affiliate of the University of Iowa. “And we could probably … have more available electronically [that] could be modified for the local care environment,” he says, adding that insulin protocols come to mind first.
Another key EHR feature is an extensive adverse event reporting system, including registering near misses. About 96% of prescriptions and physician orders are entered with the system; in private sector hospitals, the rough estimate is 8%. There is also a bar-coding system for verification of medications and identification of patients. The VA “has done a great job of changing the culture to foster systems-based care and to address errors and adverse patient outcomes straightforward[ly] and deal with them up front.”
Another distinguishing feature of the VA, says Dr. Saint, is its heavy investment in quality improvement and health services research (HSR). The VA has large repositories of administrative and clinical data for performing research with hospitalized patients. Dr. Saint also points out that a lot of the academic centers benefit from having a VA as an affiliate. “The house staff, medical students, and physicians often will be at the VA [and can] see the state-of-the-art electronic medical records and CPOE system and inquire, ‘Why can’t we have that at the university hospital?’ ”
Discharge: Seamless Transition
Dr. Kaboli can point to another advantage for hospital medicine in the VA: a concerted interest in developing hospitalists. Two-thirds of VA medical centers (VAMCs) use hospitalists, and two-thirds of inpatients are cared for by hospitalists. In total, approximately 400 hospitalists are employed by the VA, making it the largest single employer of hospitalists in the United States. Within two years, 75% of VAMCs will use hospitalists.2
Dr. Kaboli has also become well versed on the advantages of the VA’s EHR in the area of patient discharge. The greatest benefit to hospitalists of having a fully integrated medical record with CPOE and all inpatient and outpatient notes available in all the VA facilities across the country, he says, “is the almost seamless transition of these records both from the clinic side to the hospital and from the hospital back to the clinic.”
One “great luxury” of having that integrated system, Dr. Kaboli adds, is that a hospitalist can hand patients their discharge summaries and advise them to pass the information on in the next doctor’s visit. “Even though you’re going to send it via e-mail, [in a] fax, or by mail, you have that as another option to translate that information to other docs,” he explains. Hospitalists can also “alert other providers by making them co-signers to notes so that when it comes into their inbox, they know that a patient was discharged, and they get the discharge summary immediately.”
There is no connection electronically with non-VA providers, however, which is the same situation that exists in any other non-VA healthcare system. “We know [that] a fairly large percentage of veterans receive care, both within and outside the VA, who are what we call co-managed,” says Dr. Kaboli. “If a patient doesn’t live near a VA hospital or clinic, he may have to travel an hour or two, so that person might as well have a local doctor. Without that [EHR system], if [the patient is] speaking to a primary care physician in a local community, [that physician is] up against the same challenges as [someone who works] outside the VA.”
Get on the EHR Bandwagon
“The federal government has a crucial leadership role in promoting a national health information infrastructure,” said Dr. Kizer in his June 17, 2004 testimony to Congress. When asked about that statement, Dr. Saint (who is also director of the VA/University of Michigan Patient Safety Enhancement Program) has one piece of advice for his hospitalist colleagues. “You don’t want perfect to become the enemy of the very good,” he says. “Rather than waiting until there is a national technology information infrastructure, which may be years—if not decades—away, you can at least advocate for change in your own hospital.”
Use the VA as a model, he says. “You don’t have to use the exact same system, but at least you can point to some of the quality advantages that electronic medical records and CPOE can provide. You can also point out some of the advantages that investment in quality improvement and health services research can bring to an organization and say, ‘We can adapt—not necessarily adopt—what the VA has done.’ ”
How can hospitalists best do that? Many publications in the peer-reviewed literature address the quality improvement focus of the VA. There is also a VA Web site that discusses the focus on HSR and development (www1. va.gov/health). A VA-sponsored national health services research and development (HSR&D) meeting, at which investigators from all over the country present their latest findings, is held annually in Washington, D.C., usually in February.
For the young hospitalist who wants to pursue additional training, Dr. Saint says, there are VA-funded fellowships, HSR&D, a quality scholars program, and other career development opportunities within the VA that promote leadership roles both in and outside the VA.
Dr. Kaboli suggests identifying networks of hospitalists within and outside of your own healthcare system that you can work with and learn from. Hospitalists can also collaborate in developing protocols that incorporate local modifications. Also, he suggests, “there are a lot of questions that come up in the day-to-day care of patients. If you have colleagues as interested as you are, as hospitalists, in the quality of care for hospitalized medical patients, you can tap into that passion. The SHM listservs are a great way to connect; one for VA hospitalists has just been organized.
Anyone interested in the OpenVista Electronic Health Record, Medsphere’s commercial product (which, Dr. Kizer says, “is VistA at the core” and is being marketed to hospitals and large clinics) can learn more at www.medsphere.com.
Dr. Kizer says hospitalists will need to understand the needs of future healthcare and help prepare for and welcome it. “For example, performance measurement is an absolute part of the future of healthcare,” he says. “I think, by and large, hospitalists understand that better and are more accepting of that than certainly most docs in private practice.”
He believes hospitalists “can help promote that understanding among their peers and their hospitals and keep moving things forward as opposed to resisting it.” This is just one aspect of the “openness and transparency that we want to see in so many areas,” says Dr. Kizer, and hospitalists can be “pushing for the tools to make it happen. The hospitalists, I would think, should be leading the charge for electronic health records.”
Now and Tomorrow
Dr. Kizer, who is one of nine experts on veterans’ issues named to the newly formed Commission on the Future for America’s Veterans and is board certified in six medical specialties, also has a personal view on the work of hospital medicine. Recently, his wife was hospitalized in the ICU at the University of California at Davis Medical Center for a number of months, and Dr. Kizer says that a succession of hospitalists have served as her principal providers. It’s given him a more intimate view of what matters, beyond strictly clinical care, to patients and their families.
“By and large, I’ve always supported the hospitalist notion,” he says, “because it … supports my view [that] keeping up to date on all the science and technology and running an office practice [at the same time] is just more than you can reasonably expect anyone to do.” What he has especially noticed now, as a family caregiver visiting a hospital, “is that there is tremendous variability in how much [hospitalists] communicate with the patient and his or her family and how they view the episode of care within the context of the family and their community.”
Dr. Kizer, who has studied communications for a long time and in myriad ways, notes that a lot of the hospitalists he has met during this recent experience “think they’re communicating, but they often don’t take the time to determine if they are actually connecting with the family or addressing the issues that are important to the patient and family.”
In the same vein, he agrees that the better the electronic communication systems of a healthcare system—including proficiency in identifying medical errors—the more minutes can be freed up for a physician to pull up a chair and talk with a patient. “It is also a powerful tool to educate and to help inform,” he says. “For example, when [a hospitalist] can just quickly graph out where the patient’s blood pressure … or blood sugars or … creatinine has been, you can use the display of data to quickly educate the patient and/or the family about what has happened and where you need to go. One picture can save you 10 minutes of explaining.”
Conclusion
The VA has taken a lead in addressing the issues that have been brought up over the years by organizations such as the Institute of Medicine and the Institute for Healthcare Improvement. Their integrated electronic health records system can serve as a model for non-VA hospitals. Until there is a national integration of computerized technology, hospitalists can become advocates for improving their own hospital technology systems. “Electronic health records and hospitalists should go hand in glove,” concludes Dr. Kizer. “It’s potentially a great marriage of technology and the human element.” TH
Andrea Sattinger is a regular contributor to The Hospitalist.
References
- Arnst C. The best medical care in the U.S.: How Veterans Affairs transformed itself—and what it means for the rest of us. BusinessWeek online. July 17, 2006. Available at www.businessweek.com/magazine/content/06_29/b3993061.htm?chan=top+news_top+news. Last accessed October 20, 2006.
- Kaboli PJ, Barrett T, Vazirani S, et al. Growth of hospitalists in the Veterans Administration (VA) healthcare system: 1997-2005. Hosp Med. Abstract. 2006;1(S2):1-30.
- Lurie JD, Merrens EJ, Lee J, et al. An approach to hospital quality improvement. Med Clin North Am. 2002 Jul;86(4):825-845.
A Hospitalist Revolutionizes UCSD’s Online Clinical Systems

Josh Lee, MD, is a hospitalist. But Dr. Lee is also a computer geek, and the combination has served him and patient care well.
As medical director of Information Services at the University of California at San Diego (UCSD), Dr. Lee has oversight over all online clinical systems, and that is no small task. With Dr. Lee’s guidance, UCSD is now a leader in the medical informatics movement. With the exception of physician documentation, the system has comprehensive electronic records; that is, some physicians still prefer to “wet-sign” their notes. Lab results at UCSD are 100% electronic, as is order entry for adult inpatients. “We have now completed what we call the entire order life cycle: physician orders, direct integrations through our pharmacy, pharmacy validation, and bar-coded administration at bedside,” he says.
As opposed to the VA’s homegrown EHR, UCSD did what many healthcare systems do: They bought an off-the-shelf product—this one was Invision from Siemens—but UCSD calls their product PCIS, for Patient Care Information Services.
“A lot of people are able to do cool stuff [with medical informatics],” says Dr. Lee, “but they have done it with a proprietary product, so it’s different than VA, where they are using something they have total control over.”
He says many people are now focused on order entry, “but I think the newest area of research and integration [involves the question], how do we communicate key clinical issues and follow-up for discharge?” (See Figure 1, above.) At UCSD Medical Center, these screens can be printed and the pages given directly to the patient upon discharge.) “We have leveraged our electronic system to ensure that, at the moment of discharge, not only is the patient informed about [his or her] care, but it is clear to anybody on our side, or from the side of the receiving physician, what is supposed to happen next.”
As any hospitalist knows, there can be a huge “voltage drop” in this area, as Robert Wachter, MD, professor and associate chairman at UCSF’s Department of Medicine, San Francisco, refers to it. Dr. Wachter is
And the great advantages of the VA’s electronic products are not available to the “99% of American hospitalists who don’t practice in closed systems,” says Dr. Lee.
Because most hospitalists don’t have that advantage, careful and complete discharge communications are imperative. That’s why UCSD built screens that can accommodate the specific information patients need, he says. “It’s different from the classic discharge summary, which is usually a lengthy, unwieldy, dictated document that is mostly [composed] after the patient leaves the hospital. This is done in real time … and these print-outs are immediately available for the patient.”
Before Dr. Lee came to UCSD, he worked with Drs. Jon Lurie, Mark Splaine, and Ed Merrens, all members of the general internal medicine division at Dartmouth-Hitchcock Medical Center in Hanover, N.H.3 As part of the team’s exploration of quality improvement and medical informatics, they particularly looked at how to adapt products to be workflow sensitive.
And one of the most important things Dr. Lee says he would tell his counterparts at other institutions is “to ensure that computerized solutions for safety and documentation are appropriately matched to the work flow.” He thinks that when these initiatives fail it is often due to an underappreciation of the impact that these changes and enhancements have on actual provision of care. “Do those things that are [the] most highly successful, leverage moments that you’re going to do anyway, but then automate it, make it safer, make it more comprehensive,” he says. “That’s my challenge to my colleagues.”—AS
Modern medicine … certainly as it should be practiced by hospitalists, is the most information-intensive activity that human beings ever engaged in,” says Kenneth W. Kizer, MD, MPH, CEO and chairman of the board of Medsphere Systems Corporation in Aliso Viejo, Calif.
He should know. From his first healthcare-related position in 1969 as a hospital orderly at Stanford University Hospital, he rose to become the Under Secretary for Health in the Department of Veterans Affairs (VA)—the CEO of the largest healthcare system in the nation. He is widely credited as being the chief architect and driving force behind the successful transformation of VA healthcare in the 1990s.
The VA’s 154 hospitals and 875 clinics, which serve 5.4 million patients, have been rated “best in class” by a number of independent groups since it implemented the changes in the 1990s.1 In a study conducted by the Rand Corporation, the VA scored higher compared with the U.S. private sector hospitals in every category except acute care, in which “the numbers ran neck and neck,” says Dr. Kizer. “Where the VA has done much better [than private sector hospitals] is in managing chronic disease and integrating prevention and health maintenance into the acute care program.”
Differences between a VA facility and one in the private sector are mostly “cosmetic and in the financing,” says Dr. Kizer. “The VA takes care of a particular patient population—veterans of military service—but it is a civilian practice that happens to be run by the federal government.”
According to a July 17, 2006, article in BusinessWeek, “The Best Medical Care in the U.S.,” the VA system provides about two-thirds of the care protocols recommended by organizations such as the Agency for Healthcare Research and Quality, compared with 50% provided in private sector hospitals.1 Also, as many as 8% of the prescriptions filled in private sector hospitals contain errors, but the VA’s prescription-related accuracy is greater than 99.997%. In addition, the VA spends an average of $5,000 per patient compared with the national average of $6,300.
Dr. Kizer’s focus on quality improvement at the VA should not be surprising in view of his long-time focus on improving the quality of healthcare. In his mind, an essential element in improving the quality of American healthcare is the widespread adoption of electronic health records (EHR).
When he arrived at his post at the VA in 1994, Dr. Kizer was pleasantly surprised to find advanced automated information management in place. The VA had been working on developing an EHR since 1978. As part Kizer’s transformation of the VA, all of the VA’s information systems were integrated, and VistA (an acronym for Veterans Health Information Systems and Technology Architecture) was launched in 1997. VistA is often the first thing that VA-affiliated hospitalists mention when they are asked what distinguishes VA hospitals from non-VA hospitals.
Key Features and Benefits of the VA
Sanjay Saint, MD, knows a great deal about academically affiliated VAs. He was a resident (July 1993-June 1995) and then chief medical resident at the San Francisco VA (June 1995-June 1996), an affiliate of the University of California at San Francisco. He was also a fellow at the University of Washington-affiliated Seattle VA (July 1996-June 1998), and for more than eight years he has been on the faculty at the University of Michigan as a professor of internal medicine (1998-2006). Dr. Saint is currently a hospitalist at the University of Michigan-affiliated Ann Arbor VA Hospital. He was also recently the acting chief of medicine there for six months (Dec. 2005-May 2006) while the permanent chief was on sabbatical.
The instant availability of the EHR system is a key benefit of practicing in a VA hospital, says Dr. Saint. “It involves not only being able to get up-to-date, relevant patient information at our VA but also the information obtained if the patient has been seen at other VAs.”
“One of the reasons why [the VA’s EHR] is so good is that it is fully integrated,” says Dr. Kizer. “Everything was made to fit together to begin with—in contrast to essentially all commercial products, which have been melded together from pieces that come from a variety of origins. Being fully integrated certainly increases the speed and efficiency of operations. The second reason why VistA is so good is that it was developed by clinicians for clinicians … .”
A key feature operating as part of the EHR is the focus on computer-based provider order entry (CPOE). CPOE can help physicians make correct clinical decisions, says Dr. Saint. He cites the example of a pilot test he and co-workers conducted at the Seattle VA: After 72 hours of urinary catheterization in a patient, an alert reminded physicians to remove the catheter. From that simple type of quality improvement experiment, the data revealed that those patients for whom the reminder had been used had a significantly reduced rate of infection compared with those for whom it had not.
One particularly good, but perhaps underutilized, aspect of the computerized system is the use of care protocols or models that can be used across the VA, says Peter Kaboli, MD, MS, hospitalist at the Iowa City VA Hospital, an affiliate of the University of Iowa. “And we could probably … have more available electronically [that] could be modified for the local care environment,” he says, adding that insulin protocols come to mind first.
Another key EHR feature is an extensive adverse event reporting system, including registering near misses. About 96% of prescriptions and physician orders are entered with the system; in private sector hospitals, the rough estimate is 8%. There is also a bar-coding system for verification of medications and identification of patients. The VA “has done a great job of changing the culture to foster systems-based care and to address errors and adverse patient outcomes straightforward[ly] and deal with them up front.”
Another distinguishing feature of the VA, says Dr. Saint, is its heavy investment in quality improvement and health services research (HSR). The VA has large repositories of administrative and clinical data for performing research with hospitalized patients. Dr. Saint also points out that a lot of the academic centers benefit from having a VA as an affiliate. “The house staff, medical students, and physicians often will be at the VA [and can] see the state-of-the-art electronic medical records and CPOE system and inquire, ‘Why can’t we have that at the university hospital?’ ”
Discharge: Seamless Transition
Dr. Kaboli can point to another advantage for hospital medicine in the VA: a concerted interest in developing hospitalists. Two-thirds of VA medical centers (VAMCs) use hospitalists, and two-thirds of inpatients are cared for by hospitalists. In total, approximately 400 hospitalists are employed by the VA, making it the largest single employer of hospitalists in the United States. Within two years, 75% of VAMCs will use hospitalists.2
Dr. Kaboli has also become well versed on the advantages of the VA’s EHR in the area of patient discharge. The greatest benefit to hospitalists of having a fully integrated medical record with CPOE and all inpatient and outpatient notes available in all the VA facilities across the country, he says, “is the almost seamless transition of these records both from the clinic side to the hospital and from the hospital back to the clinic.”
One “great luxury” of having that integrated system, Dr. Kaboli adds, is that a hospitalist can hand patients their discharge summaries and advise them to pass the information on in the next doctor’s visit. “Even though you’re going to send it via e-mail, [in a] fax, or by mail, you have that as another option to translate that information to other docs,” he explains. Hospitalists can also “alert other providers by making them co-signers to notes so that when it comes into their inbox, they know that a patient was discharged, and they get the discharge summary immediately.”
There is no connection electronically with non-VA providers, however, which is the same situation that exists in any other non-VA healthcare system. “We know [that] a fairly large percentage of veterans receive care, both within and outside the VA, who are what we call co-managed,” says Dr. Kaboli. “If a patient doesn’t live near a VA hospital or clinic, he may have to travel an hour or two, so that person might as well have a local doctor. Without that [EHR system], if [the patient is] speaking to a primary care physician in a local community, [that physician is] up against the same challenges as [someone who works] outside the VA.”
Get on the EHR Bandwagon
“The federal government has a crucial leadership role in promoting a national health information infrastructure,” said Dr. Kizer in his June 17, 2004 testimony to Congress. When asked about that statement, Dr. Saint (who is also director of the VA/University of Michigan Patient Safety Enhancement Program) has one piece of advice for his hospitalist colleagues. “You don’t want perfect to become the enemy of the very good,” he says. “Rather than waiting until there is a national technology information infrastructure, which may be years—if not decades—away, you can at least advocate for change in your own hospital.”
Use the VA as a model, he says. “You don’t have to use the exact same system, but at least you can point to some of the quality advantages that electronic medical records and CPOE can provide. You can also point out some of the advantages that investment in quality improvement and health services research can bring to an organization and say, ‘We can adapt—not necessarily adopt—what the VA has done.’ ”
How can hospitalists best do that? Many publications in the peer-reviewed literature address the quality improvement focus of the VA. There is also a VA Web site that discusses the focus on HSR and development (www1. va.gov/health). A VA-sponsored national health services research and development (HSR&D) meeting, at which investigators from all over the country present their latest findings, is held annually in Washington, D.C., usually in February.
For the young hospitalist who wants to pursue additional training, Dr. Saint says, there are VA-funded fellowships, HSR&D, a quality scholars program, and other career development opportunities within the VA that promote leadership roles both in and outside the VA.
Dr. Kaboli suggests identifying networks of hospitalists within and outside of your own healthcare system that you can work with and learn from. Hospitalists can also collaborate in developing protocols that incorporate local modifications. Also, he suggests, “there are a lot of questions that come up in the day-to-day care of patients. If you have colleagues as interested as you are, as hospitalists, in the quality of care for hospitalized medical patients, you can tap into that passion. The SHM listservs are a great way to connect; one for VA hospitalists has just been organized.
Anyone interested in the OpenVista Electronic Health Record, Medsphere’s commercial product (which, Dr. Kizer says, “is VistA at the core” and is being marketed to hospitals and large clinics) can learn more at www.medsphere.com.
Dr. Kizer says hospitalists will need to understand the needs of future healthcare and help prepare for and welcome it. “For example, performance measurement is an absolute part of the future of healthcare,” he says. “I think, by and large, hospitalists understand that better and are more accepting of that than certainly most docs in private practice.”
He believes hospitalists “can help promote that understanding among their peers and their hospitals and keep moving things forward as opposed to resisting it.” This is just one aspect of the “openness and transparency that we want to see in so many areas,” says Dr. Kizer, and hospitalists can be “pushing for the tools to make it happen. The hospitalists, I would think, should be leading the charge for electronic health records.”
Now and Tomorrow
Dr. Kizer, who is one of nine experts on veterans’ issues named to the newly formed Commission on the Future for America’s Veterans and is board certified in six medical specialties, also has a personal view on the work of hospital medicine. Recently, his wife was hospitalized in the ICU at the University of California at Davis Medical Center for a number of months, and Dr. Kizer says that a succession of hospitalists have served as her principal providers. It’s given him a more intimate view of what matters, beyond strictly clinical care, to patients and their families.
“By and large, I’ve always supported the hospitalist notion,” he says, “because it … supports my view [that] keeping up to date on all the science and technology and running an office practice [at the same time] is just more than you can reasonably expect anyone to do.” What he has especially noticed now, as a family caregiver visiting a hospital, “is that there is tremendous variability in how much [hospitalists] communicate with the patient and his or her family and how they view the episode of care within the context of the family and their community.”
Dr. Kizer, who has studied communications for a long time and in myriad ways, notes that a lot of the hospitalists he has met during this recent experience “think they’re communicating, but they often don’t take the time to determine if they are actually connecting with the family or addressing the issues that are important to the patient and family.”
In the same vein, he agrees that the better the electronic communication systems of a healthcare system—including proficiency in identifying medical errors—the more minutes can be freed up for a physician to pull up a chair and talk with a patient. “It is also a powerful tool to educate and to help inform,” he says. “For example, when [a hospitalist] can just quickly graph out where the patient’s blood pressure … or blood sugars or … creatinine has been, you can use the display of data to quickly educate the patient and/or the family about what has happened and where you need to go. One picture can save you 10 minutes of explaining.”
Conclusion
The VA has taken a lead in addressing the issues that have been brought up over the years by organizations such as the Institute of Medicine and the Institute for Healthcare Improvement. Their integrated electronic health records system can serve as a model for non-VA hospitals. Until there is a national integration of computerized technology, hospitalists can become advocates for improving their own hospital technology systems. “Electronic health records and hospitalists should go hand in glove,” concludes Dr. Kizer. “It’s potentially a great marriage of technology and the human element.” TH
Andrea Sattinger is a regular contributor to The Hospitalist.
References
- Arnst C. The best medical care in the U.S.: How Veterans Affairs transformed itself—and what it means for the rest of us. BusinessWeek online. July 17, 2006. Available at www.businessweek.com/magazine/content/06_29/b3993061.htm?chan=top+news_top+news. Last accessed October 20, 2006.
- Kaboli PJ, Barrett T, Vazirani S, et al. Growth of hospitalists in the Veterans Administration (VA) healthcare system: 1997-2005. Hosp Med. Abstract. 2006;1(S2):1-30.
- Lurie JD, Merrens EJ, Lee J, et al. An approach to hospital quality improvement. Med Clin North Am. 2002 Jul;86(4):825-845.
A Hospitalist Revolutionizes UCSD’s Online Clinical Systems
Josh Lee, MD, is a hospitalist. But Dr. Lee is also a computer geek, and the combination has served him and patient care well.
As medical director of Information Services at the University of California at San Diego (UCSD), Dr. Lee has oversight over all online clinical systems, and that is no small task. With Dr. Lee’s guidance, UCSD is now a leader in the medical informatics movement. With the exception of physician documentation, the system has comprehensive electronic records; that is, some physicians still prefer to “wet-sign” their notes. Lab results at UCSD are 100% electronic, as is order entry for adult inpatients. “We have now completed what we call the entire order life cycle: physician orders, direct integrations through our pharmacy, pharmacy validation, and bar-coded administration at bedside,” he says.
As opposed to the VA’s homegrown EHR, UCSD did what many healthcare systems do: They bought an off-the-shelf product—this one was Invision from Siemens—but UCSD calls their product PCIS, for Patient Care Information Services.
“A lot of people are able to do cool stuff [with medical informatics],” says Dr. Lee, “but they have done it with a proprietary product, so it’s different than VA, where they are using something they have total control over.”
He says many people are now focused on order entry, “but I think the newest area of research and integration [involves the question], how do we communicate key clinical issues and follow-up for discharge?” (See Figure 1, above.) At UCSD Medical Center, these screens can be printed and the pages given directly to the patient upon discharge.) “We have leveraged our electronic system to ensure that, at the moment of discharge, not only is the patient informed about [his or her] care, but it is clear to anybody on our side, or from the side of the receiving physician, what is supposed to happen next.”
As any hospitalist knows, there can be a huge “voltage drop” in this area, as Robert Wachter, MD, professor and associate chairman at UCSF’s Department of Medicine, San Francisco, refers to it. Dr. Wachter is
And the great advantages of the VA’s electronic products are not available to the “99% of American hospitalists who don’t practice in closed systems,” says Dr. Lee.
Because most hospitalists don’t have that advantage, careful and complete discharge communications are imperative. That’s why UCSD built screens that can accommodate the specific information patients need, he says. “It’s different from the classic discharge summary, which is usually a lengthy, unwieldy, dictated document that is mostly [composed] after the patient leaves the hospital. This is done in real time … and these print-outs are immediately available for the patient.”
Before Dr. Lee came to UCSD, he worked with Drs. Jon Lurie, Mark Splaine, and Ed Merrens, all members of the general internal medicine division at Dartmouth-Hitchcock Medical Center in Hanover, N.H.3 As part of the team’s exploration of quality improvement and medical informatics, they particularly looked at how to adapt products to be workflow sensitive.
And one of the most important things Dr. Lee says he would tell his counterparts at other institutions is “to ensure that computerized solutions for safety and documentation are appropriately matched to the work flow.” He thinks that when these initiatives fail it is often due to an underappreciation of the impact that these changes and enhancements have on actual provision of care. “Do those things that are [the] most highly successful, leverage moments that you’re going to do anyway, but then automate it, make it safer, make it more comprehensive,” he says. “That’s my challenge to my colleagues.”—AS
Modern medicine … certainly as it should be practiced by hospitalists, is the most information-intensive activity that human beings ever engaged in,” says Kenneth W. Kizer, MD, MPH, CEO and chairman of the board of Medsphere Systems Corporation in Aliso Viejo, Calif.
He should know. From his first healthcare-related position in 1969 as a hospital orderly at Stanford University Hospital, he rose to become the Under Secretary for Health in the Department of Veterans Affairs (VA)—the CEO of the largest healthcare system in the nation. He is widely credited as being the chief architect and driving force behind the successful transformation of VA healthcare in the 1990s.
The VA’s 154 hospitals and 875 clinics, which serve 5.4 million patients, have been rated “best in class” by a number of independent groups since it implemented the changes in the 1990s.1 In a study conducted by the Rand Corporation, the VA scored higher compared with the U.S. private sector hospitals in every category except acute care, in which “the numbers ran neck and neck,” says Dr. Kizer. “Where the VA has done much better [than private sector hospitals] is in managing chronic disease and integrating prevention and health maintenance into the acute care program.”
Differences between a VA facility and one in the private sector are mostly “cosmetic and in the financing,” says Dr. Kizer. “The VA takes care of a particular patient population—veterans of military service—but it is a civilian practice that happens to be run by the federal government.”
According to a July 17, 2006, article in BusinessWeek, “The Best Medical Care in the U.S.,” the VA system provides about two-thirds of the care protocols recommended by organizations such as the Agency for Healthcare Research and Quality, compared with 50% provided in private sector hospitals.1 Also, as many as 8% of the prescriptions filled in private sector hospitals contain errors, but the VA’s prescription-related accuracy is greater than 99.997%. In addition, the VA spends an average of $5,000 per patient compared with the national average of $6,300.
Dr. Kizer’s focus on quality improvement at the VA should not be surprising in view of his long-time focus on improving the quality of healthcare. In his mind, an essential element in improving the quality of American healthcare is the widespread adoption of electronic health records (EHR).
When he arrived at his post at the VA in 1994, Dr. Kizer was pleasantly surprised to find advanced automated information management in place. The VA had been working on developing an EHR since 1978. As part Kizer’s transformation of the VA, all of the VA’s information systems were integrated, and VistA (an acronym for Veterans Health Information Systems and Technology Architecture) was launched in 1997. VistA is often the first thing that VA-affiliated hospitalists mention when they are asked what distinguishes VA hospitals from non-VA hospitals.
Key Features and Benefits of the VA
Sanjay Saint, MD, knows a great deal about academically affiliated VAs. He was a resident (July 1993-June 1995) and then chief medical resident at the San Francisco VA (June 1995-June 1996), an affiliate of the University of California at San Francisco. He was also a fellow at the University of Washington-affiliated Seattle VA (July 1996-June 1998), and for more than eight years he has been on the faculty at the University of Michigan as a professor of internal medicine (1998-2006). Dr. Saint is currently a hospitalist at the University of Michigan-affiliated Ann Arbor VA Hospital. He was also recently the acting chief of medicine there for six months (Dec. 2005-May 2006) while the permanent chief was on sabbatical.
The instant availability of the EHR system is a key benefit of practicing in a VA hospital, says Dr. Saint. “It involves not only being able to get up-to-date, relevant patient information at our VA but also the information obtained if the patient has been seen at other VAs.”
“One of the reasons why [the VA’s EHR] is so good is that it is fully integrated,” says Dr. Kizer. “Everything was made to fit together to begin with—in contrast to essentially all commercial products, which have been melded together from pieces that come from a variety of origins. Being fully integrated certainly increases the speed and efficiency of operations. The second reason why VistA is so good is that it was developed by clinicians for clinicians … .”
A key feature operating as part of the EHR is the focus on computer-based provider order entry (CPOE). CPOE can help physicians make correct clinical decisions, says Dr. Saint. He cites the example of a pilot test he and co-workers conducted at the Seattle VA: After 72 hours of urinary catheterization in a patient, an alert reminded physicians to remove the catheter. From that simple type of quality improvement experiment, the data revealed that those patients for whom the reminder had been used had a significantly reduced rate of infection compared with those for whom it had not.
One particularly good, but perhaps underutilized, aspect of the computerized system is the use of care protocols or models that can be used across the VA, says Peter Kaboli, MD, MS, hospitalist at the Iowa City VA Hospital, an affiliate of the University of Iowa. “And we could probably … have more available electronically [that] could be modified for the local care environment,” he says, adding that insulin protocols come to mind first.
Another key EHR feature is an extensive adverse event reporting system, including registering near misses. About 96% of prescriptions and physician orders are entered with the system; in private sector hospitals, the rough estimate is 8%. There is also a bar-coding system for verification of medications and identification of patients. The VA “has done a great job of changing the culture to foster systems-based care and to address errors and adverse patient outcomes straightforward[ly] and deal with them up front.”
Another distinguishing feature of the VA, says Dr. Saint, is its heavy investment in quality improvement and health services research (HSR). The VA has large repositories of administrative and clinical data for performing research with hospitalized patients. Dr. Saint also points out that a lot of the academic centers benefit from having a VA as an affiliate. “The house staff, medical students, and physicians often will be at the VA [and can] see the state-of-the-art electronic medical records and CPOE system and inquire, ‘Why can’t we have that at the university hospital?’ ”
Discharge: Seamless Transition
Dr. Kaboli can point to another advantage for hospital medicine in the VA: a concerted interest in developing hospitalists. Two-thirds of VA medical centers (VAMCs) use hospitalists, and two-thirds of inpatients are cared for by hospitalists. In total, approximately 400 hospitalists are employed by the VA, making it the largest single employer of hospitalists in the United States. Within two years, 75% of VAMCs will use hospitalists.2
Dr. Kaboli has also become well versed on the advantages of the VA’s EHR in the area of patient discharge. The greatest benefit to hospitalists of having a fully integrated medical record with CPOE and all inpatient and outpatient notes available in all the VA facilities across the country, he says, “is the almost seamless transition of these records both from the clinic side to the hospital and from the hospital back to the clinic.”
One “great luxury” of having that integrated system, Dr. Kaboli adds, is that a hospitalist can hand patients their discharge summaries and advise them to pass the information on in the next doctor’s visit. “Even though you’re going to send it via e-mail, [in a] fax, or by mail, you have that as another option to translate that information to other docs,” he explains. Hospitalists can also “alert other providers by making them co-signers to notes so that when it comes into their inbox, they know that a patient was discharged, and they get the discharge summary immediately.”
There is no connection electronically with non-VA providers, however, which is the same situation that exists in any other non-VA healthcare system. “We know [that] a fairly large percentage of veterans receive care, both within and outside the VA, who are what we call co-managed,” says Dr. Kaboli. “If a patient doesn’t live near a VA hospital or clinic, he may have to travel an hour or two, so that person might as well have a local doctor. Without that [EHR system], if [the patient is] speaking to a primary care physician in a local community, [that physician is] up against the same challenges as [someone who works] outside the VA.”
Get on the EHR Bandwagon
“The federal government has a crucial leadership role in promoting a national health information infrastructure,” said Dr. Kizer in his June 17, 2004 testimony to Congress. When asked about that statement, Dr. Saint (who is also director of the VA/University of Michigan Patient Safety Enhancement Program) has one piece of advice for his hospitalist colleagues. “You don’t want perfect to become the enemy of the very good,” he says. “Rather than waiting until there is a national technology information infrastructure, which may be years—if not decades—away, you can at least advocate for change in your own hospital.”
Use the VA as a model, he says. “You don’t have to use the exact same system, but at least you can point to some of the quality advantages that electronic medical records and CPOE can provide. You can also point out some of the advantages that investment in quality improvement and health services research can bring to an organization and say, ‘We can adapt—not necessarily adopt—what the VA has done.’ ”
How can hospitalists best do that? Many publications in the peer-reviewed literature address the quality improvement focus of the VA. There is also a VA Web site that discusses the focus on HSR and development (www1. va.gov/health). A VA-sponsored national health services research and development (HSR&D) meeting, at which investigators from all over the country present their latest findings, is held annually in Washington, D.C., usually in February.
For the young hospitalist who wants to pursue additional training, Dr. Saint says, there are VA-funded fellowships, HSR&D, a quality scholars program, and other career development opportunities within the VA that promote leadership roles both in and outside the VA.
Dr. Kaboli suggests identifying networks of hospitalists within and outside of your own healthcare system that you can work with and learn from. Hospitalists can also collaborate in developing protocols that incorporate local modifications. Also, he suggests, “there are a lot of questions that come up in the day-to-day care of patients. If you have colleagues as interested as you are, as hospitalists, in the quality of care for hospitalized medical patients, you can tap into that passion. The SHM listservs are a great way to connect; one for VA hospitalists has just been organized.
Anyone interested in the OpenVista Electronic Health Record, Medsphere’s commercial product (which, Dr. Kizer says, “is VistA at the core” and is being marketed to hospitals and large clinics) can learn more at www.medsphere.com.
Dr. Kizer says hospitalists will need to understand the needs of future healthcare and help prepare for and welcome it. “For example, performance measurement is an absolute part of the future of healthcare,” he says. “I think, by and large, hospitalists understand that better and are more accepting of that than certainly most docs in private practice.”
He believes hospitalists “can help promote that understanding among their peers and their hospitals and keep moving things forward as opposed to resisting it.” This is just one aspect of the “openness and transparency that we want to see in so many areas,” says Dr. Kizer, and hospitalists can be “pushing for the tools to make it happen. The hospitalists, I would think, should be leading the charge for electronic health records.”
Now and Tomorrow
Dr. Kizer, who is one of nine experts on veterans’ issues named to the newly formed Commission on the Future for America’s Veterans and is board certified in six medical specialties, also has a personal view on the work of hospital medicine. Recently, his wife was hospitalized in the ICU at the University of California at Davis Medical Center for a number of months, and Dr. Kizer says that a succession of hospitalists have served as her principal providers. It’s given him a more intimate view of what matters, beyond strictly clinical care, to patients and their families.
“By and large, I’ve always supported the hospitalist notion,” he says, “because it … supports my view [that] keeping up to date on all the science and technology and running an office practice [at the same time] is just more than you can reasonably expect anyone to do.” What he has especially noticed now, as a family caregiver visiting a hospital, “is that there is tremendous variability in how much [hospitalists] communicate with the patient and his or her family and how they view the episode of care within the context of the family and their community.”
Dr. Kizer, who has studied communications for a long time and in myriad ways, notes that a lot of the hospitalists he has met during this recent experience “think they’re communicating, but they often don’t take the time to determine if they are actually connecting with the family or addressing the issues that are important to the patient and family.”
In the same vein, he agrees that the better the electronic communication systems of a healthcare system—including proficiency in identifying medical errors—the more minutes can be freed up for a physician to pull up a chair and talk with a patient. “It is also a powerful tool to educate and to help inform,” he says. “For example, when [a hospitalist] can just quickly graph out where the patient’s blood pressure … or blood sugars or … creatinine has been, you can use the display of data to quickly educate the patient and/or the family about what has happened and where you need to go. One picture can save you 10 minutes of explaining.”
Conclusion
The VA has taken a lead in addressing the issues that have been brought up over the years by organizations such as the Institute of Medicine and the Institute for Healthcare Improvement. Their integrated electronic health records system can serve as a model for non-VA hospitals. Until there is a national integration of computerized technology, hospitalists can become advocates for improving their own hospital technology systems. “Electronic health records and hospitalists should go hand in glove,” concludes Dr. Kizer. “It’s potentially a great marriage of technology and the human element.” TH
Andrea Sattinger is a regular contributor to The Hospitalist.
References
- Arnst C. The best medical care in the U.S.: How Veterans Affairs transformed itself—and what it means for the rest of us. BusinessWeek online. July 17, 2006. Available at www.businessweek.com/magazine/content/06_29/b3993061.htm?chan=top+news_top+news. Last accessed October 20, 2006.
- Kaboli PJ, Barrett T, Vazirani S, et al. Growth of hospitalists in the Veterans Administration (VA) healthcare system: 1997-2005. Hosp Med. Abstract. 2006;1(S2):1-30.
- Lurie JD, Merrens EJ, Lee J, et al. An approach to hospital quality improvement. Med Clin North Am. 2002 Jul;86(4):825-845.
A Hospitalist Revolutionizes UCSD’s Online Clinical Systems
Josh Lee, MD, is a hospitalist. But Dr. Lee is also a computer geek, and the combination has served him and patient care well.
As medical director of Information Services at the University of California at San Diego (UCSD), Dr. Lee has oversight over all online clinical systems, and that is no small task. With Dr. Lee’s guidance, UCSD is now a leader in the medical informatics movement. With the exception of physician documentation, the system has comprehensive electronic records; that is, some physicians still prefer to “wet-sign” their notes. Lab results at UCSD are 100% electronic, as is order entry for adult inpatients. “We have now completed what we call the entire order life cycle: physician orders, direct integrations through our pharmacy, pharmacy validation, and bar-coded administration at bedside,” he says.
As opposed to the VA’s homegrown EHR, UCSD did what many healthcare systems do: They bought an off-the-shelf product—this one was Invision from Siemens—but UCSD calls their product PCIS, for Patient Care Information Services.
“A lot of people are able to do cool stuff [with medical informatics],” says Dr. Lee, “but they have done it with a proprietary product, so it’s different than VA, where they are using something they have total control over.”
He says many people are now focused on order entry, “but I think the newest area of research and integration [involves the question], how do we communicate key clinical issues and follow-up for discharge?” (See Figure 1, above.) At UCSD Medical Center, these screens can be printed and the pages given directly to the patient upon discharge.) “We have leveraged our electronic system to ensure that, at the moment of discharge, not only is the patient informed about [his or her] care, but it is clear to anybody on our side, or from the side of the receiving physician, what is supposed to happen next.”
As any hospitalist knows, there can be a huge “voltage drop” in this area, as Robert Wachter, MD, professor and associate chairman at UCSF’s Department of Medicine, San Francisco, refers to it. Dr. Wachter is
And the great advantages of the VA’s electronic products are not available to the “99% of American hospitalists who don’t practice in closed systems,” says Dr. Lee.
Because most hospitalists don’t have that advantage, careful and complete discharge communications are imperative. That’s why UCSD built screens that can accommodate the specific information patients need, he says. “It’s different from the classic discharge summary, which is usually a lengthy, unwieldy, dictated document that is mostly [composed] after the patient leaves the hospital. This is done in real time … and these print-outs are immediately available for the patient.”
Before Dr. Lee came to UCSD, he worked with Drs. Jon Lurie, Mark Splaine, and Ed Merrens, all members of the general internal medicine division at Dartmouth-Hitchcock Medical Center in Hanover, N.H.3 As part of the team’s exploration of quality improvement and medical informatics, they particularly looked at how to adapt products to be workflow sensitive.
And one of the most important things Dr. Lee says he would tell his counterparts at other institutions is “to ensure that computerized solutions for safety and documentation are appropriately matched to the work flow.” He thinks that when these initiatives fail it is often due to an underappreciation of the impact that these changes and enhancements have on actual provision of care. “Do those things that are [the] most highly successful, leverage moments that you’re going to do anyway, but then automate it, make it safer, make it more comprehensive,” he says. “That’s my challenge to my colleagues.”—AS
In the Know

Since the late 1960s, a growing body of evidence has suggested the chances that patients truly understand what they are consenting to in informed consent documents are not only unlikely but “remote.”1 A review of 70 studies conducted in a variety of clinical settings demonstrated that, although consent and refusals were legally and institutionally valid, they failed to result in “genuinely autonomous decision making.”
Factors associated with such outcomes included low socioeconomic status, poor education, old age, lengthy hospital stay, stress, language barriers, and misinterpretation of probabilistic data. Accompanying disclosure practices were also found inadequate, though perfectly legal.
Research by the National Quality Forum (NQF) revealed that, despite having signed a consent form, 18% to 45% of patients are unable to recall even the major risks associated with their surgeries. Many cannot answer basic questions about the services or procedures they agreed to receive, while 44% do not know the exact nature of their operation, and most (60% to 69%) do not understand or read the information contained in generic hospital consent forms.2 Treating patients such as these can lead to compromised care and safety and increased medical malpractice risk.
Many bioethicists endorse the position that “striving for fully informed consent is generally unfeasible and perhaps even undesirable.”-- Others argue that the concept of fully informed consent should at least serve as an ideal. For that to be achieved, patients would need to understand fully their conditions and treatment. At a minimum, then, and as law, patients have the right to be given information that will optimize their autonomy.3-6 That information includes:
- The nature of the procedure or treatment being offered, including whether it is diagnostic or therapeutic;
- The risks and potential complications of a procedure or medical treatment;
- The benefits of the procedure; and
- Treatment alternatives, along with their risks and benefits.7
The ideal is far from reality. Frequently cited factors interfering with full comprehension, in addition to those already mentioned, include personal or cultural beliefs and low health literacy rates.1,2 Providers’ inability to communicate clearly in a rushed environment is also a factor, as is a tendency for providers who see the act of acquiring informed consent as a legal formality to delegate to a junior colleague.
But “the patient’s consent happens during the process of dialogue with the surgeon,” wrote Bernat and Peterson in the January 2006 Archives of Surgery:8 “The signature on a surgical consent form is merely the culmination and formalization of this preceding consent discussion and agreement.”
A signed consent form represents evidence of the patient’s consent—not of his or her understanding. That signed form may not be sufficient to protect providers in cases of liability. According to Jury Verdict Research, informed consent issues are among the top 10 most common reasons patients file malpractice claims.2
The low health literacy of almost half of adults in the United States limits their ability to understand the basic health information and services that are needed to make appropriate health decisions. In fact, articles in two of the July 2006 issues of the New England Journal of Medicine, as well as the entire August 2006 issue of the Journal of General Internal Medicine, are devoted to the subject of health literacy.9-11
Given that surgeons and other specialists are often responsible for securing informed consent, what are the areas of informed consent to which hospitalists should be attuned?
Key Considerations for the Hospitalist
Ordinarily, the person whose name is at the top of the patient’s chart has full responsibility for informed consent, although sometimes a subspecialty consultant, such as a cardiologist asking for a particular study, might help. A hospitalist might be named as the responsible provider in an area in which he or she is active.
Ben Rich, JD, PhD, a professor of bioethics at the University of California-Davis School (UCD) of Medicine in Sacramento, Calif., has considered the critical problems or distinctions that the hospitalist, as opposed to other physicians, may have in the area of informed consent. One area that strikes him as potentially risky is that of advance directives. Dr. Rich, who teaches a course on medicine and law at UCD, says that for decades experts have urged primary care physicians (PCPs) to discuss advance directives with patients as part of routine care. Even so, he acknowledges, if a patient is in critical condition and is hospitalized, “it is entirely possible that their personal physician won’t even know about it. So here is the person who is supposed to have apprised herself of the patient’s values and priorities in circumstances like that, and they’re out of the picture. And the person who is trying to interpret advance directives, if there is one, is the hospitalist.”
It might be difficult for the hospitalist to interpret any ambiguities. If the hospitalist believes it is impossible to know what the patient understood at the time they drafted the directive about the circumstances they are now facing, he or she may be more likely to dismiss it as invalid and simply make a decision as to what is medically appropriate, says Dr. Rich.
The discontinuity of care imposed by the hospitalist systems raises several ethical concerns, wrote Steven Pantilat, MD, in JAMA.12 The primary care physician and patient have previously negotiated, through the process of medical decision-making, the patient’s goals and values regarding medical interventions. “Because hospitalist systems leave no formal inpatient role for the PCP,” wrote Dr. Pantilat, “ … patients can no longer rely on agreements reached in the office following them to the hospital. Nonetheless, the hospitalist shares the PCP’s obligations to respect the ethical principles that agreements about preferences for care or individual values often represent.”
Another important but somewhat controversial issue involves whether a consent discussion held preoperatively also encompasses the management of post-procedure complications.8 Although it is impossible to mention all possible serious complications beforehand, it is prudent to reference the patient’s goals and general treatment preferences and to ensure that a family member (if not the designated surrogate) is present during this conversation. Just the same, each new intervention or procedure requires a new conversation and, in some cases, a new signed form. “Because at the end of the day,” says Patrick O’Rourke, JD, an attorney in Denver who regularly represents physicians in medical malpractice cases, “physicians are the people who have the obligation to obtain informed consent; the hospital as an institution does not, because hospitals don’t practice medicine; physicians do.”
Particularly with patients who face serious illness and those confronting what may be a chronic condition going forward, says Dr. Rich, “there’s a school of thought [that maintains] that part of the informed consent process is obsessively focused on procedures and pays woefully inadequate attention to the reasonable goals of care. This is nowhere more obvious than in the ICU setting.”
Continuums of Care and Consent
Indeed, any expert on medical law will tell you that informed consent is a process—not an event.8 Though a hospitalist may not have secured the signature on a consent form, a hospitalist’s practice is as much a part of a patient’s ongoing process of “consent” as is that of the surgeon who performed the patient’s operation.
The American Academy of Family Physicians has adopted the following guideline: “During the period of hospitalization, decisions regarding care, consultation, admission, transfer, and discharge should be the sole responsibility of the inpatient care physician in consultation with the patient and, as appropriate, the patient’s family physician and/or family members.”13 The times when patients actually sign informed consent documents are junctures in the continuum of consent that covers a lifetime healthcare experience. Hospitalists, then, are involved in informed consent from patient assignment to patient discharge.
“And the manner in which the process is conducted is at least as important as substantive information given,” says Dr. Rich. “A skilled and experienced physician can give any patient two descriptions of the procedure that they’re recommending,” he says. “[After o]ne, couched in a certain way, but not inaccurate, the patient would say, ‘Well, of course, I want that.’ And if the physician gives it in the other way, still accurate, the patient would say, Well, who would want that? And it all has to do with the terms you use, your tone of voice, your body language, the setting in which you provide it. … All that can profoundly shape the informed consent process. And it is not something that physicians are routinely taught.”
Because the process of informed consent is ongoing, discussions may continue for several sessions over a length of time before a patient decides to undergo a treatment. This gives patients more time to think of questions or concerns they may have. Addressing those concerns is a crucial part of the process.
“The reason that’s important is that you always want to offer and document that you have an opportunity to address what the patient’s questions were so the consent is truly informed,” says O’Rourke. One-way delivery of information is not equivalent to the dialogue implied by the term “informed consent.” “It is vitally important to ask, ‘What other information can I give you?’” he explains, especially because informed consent cases often deal with complications that develop after surgery.
Community Standard
The risks of procedures mentioned in informed consent discussions comprise a special category, says O’Rourke, “because there are some things that are not easily foreseen.” Some complications are not within the range generally anticipated after a procedure. “And the way the law works is that you don’t have to imagine the million-to-one shot [complication]; you would review the risks in terms of what a physician should disclose … in terms of significance.”
Physicians are judged by how well they informed patients of the risks as assessed by a community standard of what reasonable practitioners in the community say the risks are, he says. Physicians need to be knowledgeable about the risks of the procedure based on the medical literature, their training, and their discussions with colleagues.14
“Oftentimes, in order to give and get full informed consent, we use the knowledge from our subspecialty consultants,” says Dennis Manning, MD, FACP, FACC, a hospitalist and director of quality in the Department of Medicine and an assistant professor at the Mayo Clinic College of Medicine, Rochester, Minn. “We ask them, ‘What do you think the risks are?’ We might have to pick their brains in order to become fully aware of the hazards in a particular patient.”
“Risk is the category where litigation pops up and where you see the most challenges,” says O’Rourke, because the patient filing a claim may say, “ ‘Well, the doctor didn’t tell me about this risk and had I known this occurred, I would have elected to forego this procedure; I would have chosen one of the other alternatives.’ ”
If a patient develops a complication and the hospitalist must initiate a new intervention, then it’s the hospitalist’s duty to get informed consent for that next intervention. “Every time a physician undertakes a particular intervention, the patient has to be informed in why that intervention is being taken and what the risks, benefits, and alternatives are,” says O’Rourke.
If a patient is incapable of giving consent, then consider whether there is a significant risk in waiting until the patient is capable of giving informed consent. If the answer is “no,” then consider whether or not to delay the intervention. “If there’s no potential harm caused by waiting until the patient hits a higher level of consciousness,” says O’Rourke, “then that’s perfectly appropriate.”
In an emergency situation, a surrogate may need to make the decision. If neither one of those alternatives is available, “the law presumes that the patient is going to do what is reasonable and necessary in order to preserve his or her health, unless there’s been some instruction otherwise,” notes O’Rourke.
Teach Back
Studies show that when patients are asked to repeat what they understood from their informed consent discussions, they have greater recall and comprehension of the risks and benefits of surgical procedures.2,15 “Teach back” is an especially valuable technique to use with low literacy patients. The NQF discovered that the providers and departments using teach back were widely recognized by their peers as having the most well-informed patients compared with departments that did not use this method.2 (See “Teach Back in Action,” above right.) A number of studies have found that when a provider asks a patient to restate information or instructions, the benefits include providing a check for lapses of recall and understanding, revealing health beliefs, reinforcing and individualizing health messages, and motivating patients by activating dialogue.15
In May 2003, the NQF published Safe Practices for Better Healthcare, which endorsed a set of consensus standards for 30 healthcare practices, one of which (Safe Practice 10) recommends that all healthcare professionals ask patients to teach back what they have been told by their providers during their informed consent discussions.2
In its 2001 report, Making Health Care Safer: A Critical Analysis of Patient Safety Practices (project director, Robert M. Wachter, MD), the Agency for Healthcare Research and Quality suggested that special attention be paid to implementing 11 particular practices, one of which was “asking that patients recall and restate what they have been told during the informed consent process.”16
Even if you are not asking for a signed form, physicians, nurses, interpreters, and any professional who communicates with patients regarding their healthcare decisions is involved in the informed consent process and should use teach back—especially with those patients who find even basic health information difficult to understand. Although the NQF found that physicians were reluctant to incorporate this technique into their communications, the providers reported anecdotally that teach back takes less than a minute to complete; research backs up the claim that the more the technique is practiced, the speedier it gets.2
The provision of this “interactive communication loop,” as it has been called,15 has also been shown to affect clinical outcomes. In a study by Schillinger and colleagues conducted at an outpatient general internal medicine clinic and at San Francisco General Hospital, physicians assessed recall and comprehension of any new concept in 12 (20%) of 61 outpatient visits by diabetic patients for 15 (12%) of 124 concepts.15 The patients whose physicians assessed their recall by means of teach back were more likely to have hemoglobin A1c levels below the mean compared with patients whose doctors did not. The two variables found to be independently associated with good glycemic control were higher health literacy levels and physicians’ application of the teach-back strategy.
Consent Forms
The informed consent process is intended to protect patients and physicians both.7 Legal doctrine, including hospital accreditation standards, ethical theories, and perspectives on the physician-patient relationship, emphasizes the importance of full patient comprehension regarding treatment. But many hospitals do not use forms that contribute to that objective. In a study by Bottrell and colleagues of 540 forms from 157 hospitals nationwide, 96% indicated the nature of the procedure for the patient; however, only 26% of forms included all four elements of informed consent: procedure, risks, benefits, and alternative treatment options. Thirty-five percent included three of four elements, 23% provided two of four elements, 14% listed only one element, and 2% contained none of the elements.
In general, the investigators concluded, the forms appear to be designed to authorize treatment or protect hospitals and caregivers from liability rather than to help patients clarify information or make decisions. Even hospitals in states that have statutes requiring institutions to include all four elements on their forms were no more likely to do so than those in other states. Fewer than 40% of forms were found to support models of shared decision making, the basis of patient autonomy and the overarching intention for informed consent.
“Generally … informed consent forms are seen as mere documentation vehicles, and perhaps as legal protection, regardless of whether the process of informed consent was successfully accomplished or of minimal quality,” this study’s authors wrote, and because patients are not blind to the intentions of these forms, this may add to their discomfort.7 Most forms, the authors concluded, are insufficient because the language used does not accommodate low health literacy or because there are no graphic features.
On the other hand, “informed consent can sometimes get very awkward and cumbersome,” says William Jacott, MD, special advisor for professional relations at the Joint Commission on Accreditation of Healthcare Organizations, St. Paul, Minn., for the past five years and liaison to SHM for the past two. Some institutions or organizations interpret Joint Commission and other legal standards excessively, he says, “and I’ve seen 10-page consent forms, which just overwhelms the patient, let alone the doctor. So an over-interpretation and overkill need to be avoided.”
Conclusion: Communication and Documentation
The ways in which hospitalists can avoid the pitfalls of faulty informed consent conversations include close communication with surgeons as well as other colleagues.
“We have a great tendency to communicate via the medical record,” says Dr. Jacott, and if a patient’s co-managers (the hospitalist and subspecialist) don’t communicate, “one might assume the other has already done [informed consent], and nobody does it.”
He has also seen instances in teaching hospitals in which both the surgeon and the hospitalist incorrectly assume that the house staff has acquired informed consent.
Nurses can also help hospitalists ensure that patients are comfortable with their treatment choices. “Nurses often have more firsthand information about when patients are confused or scared or dubious or are somehow being coerced or manipulated into consenting to something,” says Dr. Rich.
Hospitalists should also avoid making assumptions about the completeness of their colleagues’ discussions with patients and should look for clear documentation as well as record their own. “Some subspecialists play fast and loose with informed consent,” Dr. Rich says, “and [may] resent a medical staff colleague who takes it seriously and attempts to hold them accountable for really doing it right. And for the hospitalist, that’s where it is critical that their institution stand behind them.”
A hospitalist’s responsibilities with regard to informed consent also include ensuring that the patient’s consent is truly informed. Using the teach back method, allowing time for the patient to ask questions and voice concerns, and including all four elements of informed consent on the patient’s consent form are just some of the ways the hospitalist can play an essential role in the continuum that is informed consent.
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Epstein M. Why effective consent presupposes autonomous authorisation: a counterorthodox argument. J Med Ethics. 2006;32:342-345.
- National Quality Forum. Implementing a national voluntary consensus standard for informed consent: a user’s guide for healthcare professionals. September 2005. Available at: www.qualityforum.org/publications.html. Accessed September 5, 2006.
- Rizzo v Schiller, 445 SE2d 153 (Va. 1994). Available at: www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=10184327&dopt=Abstract. Accessed September 11, 2006.
- Gorab v Zook, 943 P2d 423 (Colo. 1997). Available at: http://caselaw.lp.findlaw.com/scripts/getcase.pl?court=co&vol=2003app%5C3477&invol=1. Accessed September 11, 2006.
- Schuck PH. Rethinking informed consent. Yale Law J. 1994;103:899-959.
- Culbertson v Mernitz, 602 NE2d 98 (Ind. 1992).
- Bottrell MM, Alpert H, Fischbach RL, et al. Hospital informed consent for procedure forms: facilitating quality patient-physician interaction. Arch Surg. 2000 Jan;135(1):26-33.
- Bernat JL, Peterson LM. Patient-centered informed consent in surgical practice. Arch Surg. 2006 Jan;141(7):86-92.
- Marcus EN. The silent epidemic—the health effects of illiteracy. N Engl J Med. 2006;355:339-341.
- Flores G. Language barriers to health care in the United States. N Engl J Med. 2006 Jul;355:229-231.
- Carmona RH. Health literacy: a national priority. J Gen Intern Med. 2006;21:803.
- Pantilat SZ, Alpers A, Wachter RM. A new doctor in the house: ethical issues in hospitalist systems. JAMA. 1999 Jul 14;282:171-174.
- Henry LA. What the hospitalist movement means to family physicians. Fam Pract Manag. 1998 Nov-Dec;5(10):54-62.
- Rajput V, Bekes CE. Ethical issues in hospital medicine. Med Clin North Am. 2002 Jul;86(4):869-886.
- Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003 Jan 13;163(1):83-90.
- University of California at San Francisco (UCSF)-Stanford University Evidence-based Practice Center. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment: Number 43. AHRQ Publication No. 01-E058, July 2001. Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/clinic/ptsafety/. Accessed September 5, 2006.
- Baum N. Comprehension is the key: the challenge hospitals face is that many patients do not understand the fundamental information regarding their treatment plans. Patient Safety Quality Healthcare. May/June 2006:35-38.
Since the late 1960s, a growing body of evidence has suggested the chances that patients truly understand what they are consenting to in informed consent documents are not only unlikely but “remote.”1 A review of 70 studies conducted in a variety of clinical settings demonstrated that, although consent and refusals were legally and institutionally valid, they failed to result in “genuinely autonomous decision making.”
Factors associated with such outcomes included low socioeconomic status, poor education, old age, lengthy hospital stay, stress, language barriers, and misinterpretation of probabilistic data. Accompanying disclosure practices were also found inadequate, though perfectly legal.
Research by the National Quality Forum (NQF) revealed that, despite having signed a consent form, 18% to 45% of patients are unable to recall even the major risks associated with their surgeries. Many cannot answer basic questions about the services or procedures they agreed to receive, while 44% do not know the exact nature of their operation, and most (60% to 69%) do not understand or read the information contained in generic hospital consent forms.2 Treating patients such as these can lead to compromised care and safety and increased medical malpractice risk.
Many bioethicists endorse the position that “striving for fully informed consent is generally unfeasible and perhaps even undesirable.”-- Others argue that the concept of fully informed consent should at least serve as an ideal. For that to be achieved, patients would need to understand fully their conditions and treatment. At a minimum, then, and as law, patients have the right to be given information that will optimize their autonomy.3-6 That information includes:
- The nature of the procedure or treatment being offered, including whether it is diagnostic or therapeutic;
- The risks and potential complications of a procedure or medical treatment;
- The benefits of the procedure; and
- Treatment alternatives, along with their risks and benefits.7
The ideal is far from reality. Frequently cited factors interfering with full comprehension, in addition to those already mentioned, include personal or cultural beliefs and low health literacy rates.1,2 Providers’ inability to communicate clearly in a rushed environment is also a factor, as is a tendency for providers who see the act of acquiring informed consent as a legal formality to delegate to a junior colleague.
But “the patient’s consent happens during the process of dialogue with the surgeon,” wrote Bernat and Peterson in the January 2006 Archives of Surgery:8 “The signature on a surgical consent form is merely the culmination and formalization of this preceding consent discussion and agreement.”
A signed consent form represents evidence of the patient’s consent—not of his or her understanding. That signed form may not be sufficient to protect providers in cases of liability. According to Jury Verdict Research, informed consent issues are among the top 10 most common reasons patients file malpractice claims.2
The low health literacy of almost half of adults in the United States limits their ability to understand the basic health information and services that are needed to make appropriate health decisions. In fact, articles in two of the July 2006 issues of the New England Journal of Medicine, as well as the entire August 2006 issue of the Journal of General Internal Medicine, are devoted to the subject of health literacy.9-11
Given that surgeons and other specialists are often responsible for securing informed consent, what are the areas of informed consent to which hospitalists should be attuned?
Key Considerations for the Hospitalist
Ordinarily, the person whose name is at the top of the patient’s chart has full responsibility for informed consent, although sometimes a subspecialty consultant, such as a cardiologist asking for a particular study, might help. A hospitalist might be named as the responsible provider in an area in which he or she is active.
Ben Rich, JD, PhD, a professor of bioethics at the University of California-Davis School (UCD) of Medicine in Sacramento, Calif., has considered the critical problems or distinctions that the hospitalist, as opposed to other physicians, may have in the area of informed consent. One area that strikes him as potentially risky is that of advance directives. Dr. Rich, who teaches a course on medicine and law at UCD, says that for decades experts have urged primary care physicians (PCPs) to discuss advance directives with patients as part of routine care. Even so, he acknowledges, if a patient is in critical condition and is hospitalized, “it is entirely possible that their personal physician won’t even know about it. So here is the person who is supposed to have apprised herself of the patient’s values and priorities in circumstances like that, and they’re out of the picture. And the person who is trying to interpret advance directives, if there is one, is the hospitalist.”
It might be difficult for the hospitalist to interpret any ambiguities. If the hospitalist believes it is impossible to know what the patient understood at the time they drafted the directive about the circumstances they are now facing, he or she may be more likely to dismiss it as invalid and simply make a decision as to what is medically appropriate, says Dr. Rich.
The discontinuity of care imposed by the hospitalist systems raises several ethical concerns, wrote Steven Pantilat, MD, in JAMA.12 The primary care physician and patient have previously negotiated, through the process of medical decision-making, the patient’s goals and values regarding medical interventions. “Because hospitalist systems leave no formal inpatient role for the PCP,” wrote Dr. Pantilat, “ … patients can no longer rely on agreements reached in the office following them to the hospital. Nonetheless, the hospitalist shares the PCP’s obligations to respect the ethical principles that agreements about preferences for care or individual values often represent.”
Another important but somewhat controversial issue involves whether a consent discussion held preoperatively also encompasses the management of post-procedure complications.8 Although it is impossible to mention all possible serious complications beforehand, it is prudent to reference the patient’s goals and general treatment preferences and to ensure that a family member (if not the designated surrogate) is present during this conversation. Just the same, each new intervention or procedure requires a new conversation and, in some cases, a new signed form. “Because at the end of the day,” says Patrick O’Rourke, JD, an attorney in Denver who regularly represents physicians in medical malpractice cases, “physicians are the people who have the obligation to obtain informed consent; the hospital as an institution does not, because hospitals don’t practice medicine; physicians do.”
Particularly with patients who face serious illness and those confronting what may be a chronic condition going forward, says Dr. Rich, “there’s a school of thought [that maintains] that part of the informed consent process is obsessively focused on procedures and pays woefully inadequate attention to the reasonable goals of care. This is nowhere more obvious than in the ICU setting.”
Continuums of Care and Consent
Indeed, any expert on medical law will tell you that informed consent is a process—not an event.8 Though a hospitalist may not have secured the signature on a consent form, a hospitalist’s practice is as much a part of a patient’s ongoing process of “consent” as is that of the surgeon who performed the patient’s operation.
The American Academy of Family Physicians has adopted the following guideline: “During the period of hospitalization, decisions regarding care, consultation, admission, transfer, and discharge should be the sole responsibility of the inpatient care physician in consultation with the patient and, as appropriate, the patient’s family physician and/or family members.”13 The times when patients actually sign informed consent documents are junctures in the continuum of consent that covers a lifetime healthcare experience. Hospitalists, then, are involved in informed consent from patient assignment to patient discharge.
“And the manner in which the process is conducted is at least as important as substantive information given,” says Dr. Rich. “A skilled and experienced physician can give any patient two descriptions of the procedure that they’re recommending,” he says. “[After o]ne, couched in a certain way, but not inaccurate, the patient would say, ‘Well, of course, I want that.’ And if the physician gives it in the other way, still accurate, the patient would say, Well, who would want that? And it all has to do with the terms you use, your tone of voice, your body language, the setting in which you provide it. … All that can profoundly shape the informed consent process. And it is not something that physicians are routinely taught.”
Because the process of informed consent is ongoing, discussions may continue for several sessions over a length of time before a patient decides to undergo a treatment. This gives patients more time to think of questions or concerns they may have. Addressing those concerns is a crucial part of the process.
“The reason that’s important is that you always want to offer and document that you have an opportunity to address what the patient’s questions were so the consent is truly informed,” says O’Rourke. One-way delivery of information is not equivalent to the dialogue implied by the term “informed consent.” “It is vitally important to ask, ‘What other information can I give you?’” he explains, especially because informed consent cases often deal with complications that develop after surgery.
Community Standard
The risks of procedures mentioned in informed consent discussions comprise a special category, says O’Rourke, “because there are some things that are not easily foreseen.” Some complications are not within the range generally anticipated after a procedure. “And the way the law works is that you don’t have to imagine the million-to-one shot [complication]; you would review the risks in terms of what a physician should disclose … in terms of significance.”
Physicians are judged by how well they informed patients of the risks as assessed by a community standard of what reasonable practitioners in the community say the risks are, he says. Physicians need to be knowledgeable about the risks of the procedure based on the medical literature, their training, and their discussions with colleagues.14
“Oftentimes, in order to give and get full informed consent, we use the knowledge from our subspecialty consultants,” says Dennis Manning, MD, FACP, FACC, a hospitalist and director of quality in the Department of Medicine and an assistant professor at the Mayo Clinic College of Medicine, Rochester, Minn. “We ask them, ‘What do you think the risks are?’ We might have to pick their brains in order to become fully aware of the hazards in a particular patient.”
“Risk is the category where litigation pops up and where you see the most challenges,” says O’Rourke, because the patient filing a claim may say, “ ‘Well, the doctor didn’t tell me about this risk and had I known this occurred, I would have elected to forego this procedure; I would have chosen one of the other alternatives.’ ”
If a patient develops a complication and the hospitalist must initiate a new intervention, then it’s the hospitalist’s duty to get informed consent for that next intervention. “Every time a physician undertakes a particular intervention, the patient has to be informed in why that intervention is being taken and what the risks, benefits, and alternatives are,” says O’Rourke.
If a patient is incapable of giving consent, then consider whether there is a significant risk in waiting until the patient is capable of giving informed consent. If the answer is “no,” then consider whether or not to delay the intervention. “If there’s no potential harm caused by waiting until the patient hits a higher level of consciousness,” says O’Rourke, “then that’s perfectly appropriate.”
In an emergency situation, a surrogate may need to make the decision. If neither one of those alternatives is available, “the law presumes that the patient is going to do what is reasonable and necessary in order to preserve his or her health, unless there’s been some instruction otherwise,” notes O’Rourke.
Teach Back
Studies show that when patients are asked to repeat what they understood from their informed consent discussions, they have greater recall and comprehension of the risks and benefits of surgical procedures.2,15 “Teach back” is an especially valuable technique to use with low literacy patients. The NQF discovered that the providers and departments using teach back were widely recognized by their peers as having the most well-informed patients compared with departments that did not use this method.2 (See “Teach Back in Action,” above right.) A number of studies have found that when a provider asks a patient to restate information or instructions, the benefits include providing a check for lapses of recall and understanding, revealing health beliefs, reinforcing and individualizing health messages, and motivating patients by activating dialogue.15
In May 2003, the NQF published Safe Practices for Better Healthcare, which endorsed a set of consensus standards for 30 healthcare practices, one of which (Safe Practice 10) recommends that all healthcare professionals ask patients to teach back what they have been told by their providers during their informed consent discussions.2
In its 2001 report, Making Health Care Safer: A Critical Analysis of Patient Safety Practices (project director, Robert M. Wachter, MD), the Agency for Healthcare Research and Quality suggested that special attention be paid to implementing 11 particular practices, one of which was “asking that patients recall and restate what they have been told during the informed consent process.”16
Even if you are not asking for a signed form, physicians, nurses, interpreters, and any professional who communicates with patients regarding their healthcare decisions is involved in the informed consent process and should use teach back—especially with those patients who find even basic health information difficult to understand. Although the NQF found that physicians were reluctant to incorporate this technique into their communications, the providers reported anecdotally that teach back takes less than a minute to complete; research backs up the claim that the more the technique is practiced, the speedier it gets.2
The provision of this “interactive communication loop,” as it has been called,15 has also been shown to affect clinical outcomes. In a study by Schillinger and colleagues conducted at an outpatient general internal medicine clinic and at San Francisco General Hospital, physicians assessed recall and comprehension of any new concept in 12 (20%) of 61 outpatient visits by diabetic patients for 15 (12%) of 124 concepts.15 The patients whose physicians assessed their recall by means of teach back were more likely to have hemoglobin A1c levels below the mean compared with patients whose doctors did not. The two variables found to be independently associated with good glycemic control were higher health literacy levels and physicians’ application of the teach-back strategy.
Consent Forms
The informed consent process is intended to protect patients and physicians both.7 Legal doctrine, including hospital accreditation standards, ethical theories, and perspectives on the physician-patient relationship, emphasizes the importance of full patient comprehension regarding treatment. But many hospitals do not use forms that contribute to that objective. In a study by Bottrell and colleagues of 540 forms from 157 hospitals nationwide, 96% indicated the nature of the procedure for the patient; however, only 26% of forms included all four elements of informed consent: procedure, risks, benefits, and alternative treatment options. Thirty-five percent included three of four elements, 23% provided two of four elements, 14% listed only one element, and 2% contained none of the elements.
In general, the investigators concluded, the forms appear to be designed to authorize treatment or protect hospitals and caregivers from liability rather than to help patients clarify information or make decisions. Even hospitals in states that have statutes requiring institutions to include all four elements on their forms were no more likely to do so than those in other states. Fewer than 40% of forms were found to support models of shared decision making, the basis of patient autonomy and the overarching intention for informed consent.
“Generally … informed consent forms are seen as mere documentation vehicles, and perhaps as legal protection, regardless of whether the process of informed consent was successfully accomplished or of minimal quality,” this study’s authors wrote, and because patients are not blind to the intentions of these forms, this may add to their discomfort.7 Most forms, the authors concluded, are insufficient because the language used does not accommodate low health literacy or because there are no graphic features.
On the other hand, “informed consent can sometimes get very awkward and cumbersome,” says William Jacott, MD, special advisor for professional relations at the Joint Commission on Accreditation of Healthcare Organizations, St. Paul, Minn., for the past five years and liaison to SHM for the past two. Some institutions or organizations interpret Joint Commission and other legal standards excessively, he says, “and I’ve seen 10-page consent forms, which just overwhelms the patient, let alone the doctor. So an over-interpretation and overkill need to be avoided.”
Conclusion: Communication and Documentation
The ways in which hospitalists can avoid the pitfalls of faulty informed consent conversations include close communication with surgeons as well as other colleagues.
“We have a great tendency to communicate via the medical record,” says Dr. Jacott, and if a patient’s co-managers (the hospitalist and subspecialist) don’t communicate, “one might assume the other has already done [informed consent], and nobody does it.”
He has also seen instances in teaching hospitals in which both the surgeon and the hospitalist incorrectly assume that the house staff has acquired informed consent.
Nurses can also help hospitalists ensure that patients are comfortable with their treatment choices. “Nurses often have more firsthand information about when patients are confused or scared or dubious or are somehow being coerced or manipulated into consenting to something,” says Dr. Rich.
Hospitalists should also avoid making assumptions about the completeness of their colleagues’ discussions with patients and should look for clear documentation as well as record their own. “Some subspecialists play fast and loose with informed consent,” Dr. Rich says, “and [may] resent a medical staff colleague who takes it seriously and attempts to hold them accountable for really doing it right. And for the hospitalist, that’s where it is critical that their institution stand behind them.”
A hospitalist’s responsibilities with regard to informed consent also include ensuring that the patient’s consent is truly informed. Using the teach back method, allowing time for the patient to ask questions and voice concerns, and including all four elements of informed consent on the patient’s consent form are just some of the ways the hospitalist can play an essential role in the continuum that is informed consent.
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Epstein M. Why effective consent presupposes autonomous authorisation: a counterorthodox argument. J Med Ethics. 2006;32:342-345.
- National Quality Forum. Implementing a national voluntary consensus standard for informed consent: a user’s guide for healthcare professionals. September 2005. Available at: www.qualityforum.org/publications.html. Accessed September 5, 2006.
- Rizzo v Schiller, 445 SE2d 153 (Va. 1994). Available at: www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=10184327&dopt=Abstract. Accessed September 11, 2006.
- Gorab v Zook, 943 P2d 423 (Colo. 1997). Available at: http://caselaw.lp.findlaw.com/scripts/getcase.pl?court=co&vol=2003app%5C3477&invol=1. Accessed September 11, 2006.
- Schuck PH. Rethinking informed consent. Yale Law J. 1994;103:899-959.
- Culbertson v Mernitz, 602 NE2d 98 (Ind. 1992).
- Bottrell MM, Alpert H, Fischbach RL, et al. Hospital informed consent for procedure forms: facilitating quality patient-physician interaction. Arch Surg. 2000 Jan;135(1):26-33.
- Bernat JL, Peterson LM. Patient-centered informed consent in surgical practice. Arch Surg. 2006 Jan;141(7):86-92.
- Marcus EN. The silent epidemic—the health effects of illiteracy. N Engl J Med. 2006;355:339-341.
- Flores G. Language barriers to health care in the United States. N Engl J Med. 2006 Jul;355:229-231.
- Carmona RH. Health literacy: a national priority. J Gen Intern Med. 2006;21:803.
- Pantilat SZ, Alpers A, Wachter RM. A new doctor in the house: ethical issues in hospitalist systems. JAMA. 1999 Jul 14;282:171-174.
- Henry LA. What the hospitalist movement means to family physicians. Fam Pract Manag. 1998 Nov-Dec;5(10):54-62.
- Rajput V, Bekes CE. Ethical issues in hospital medicine. Med Clin North Am. 2002 Jul;86(4):869-886.
- Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003 Jan 13;163(1):83-90.
- University of California at San Francisco (UCSF)-Stanford University Evidence-based Practice Center. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment: Number 43. AHRQ Publication No. 01-E058, July 2001. Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/clinic/ptsafety/. Accessed September 5, 2006.
- Baum N. Comprehension is the key: the challenge hospitals face is that many patients do not understand the fundamental information regarding their treatment plans. Patient Safety Quality Healthcare. May/June 2006:35-38.
Since the late 1960s, a growing body of evidence has suggested the chances that patients truly understand what they are consenting to in informed consent documents are not only unlikely but “remote.”1 A review of 70 studies conducted in a variety of clinical settings demonstrated that, although consent and refusals were legally and institutionally valid, they failed to result in “genuinely autonomous decision making.”
Factors associated with such outcomes included low socioeconomic status, poor education, old age, lengthy hospital stay, stress, language barriers, and misinterpretation of probabilistic data. Accompanying disclosure practices were also found inadequate, though perfectly legal.
Research by the National Quality Forum (NQF) revealed that, despite having signed a consent form, 18% to 45% of patients are unable to recall even the major risks associated with their surgeries. Many cannot answer basic questions about the services or procedures they agreed to receive, while 44% do not know the exact nature of their operation, and most (60% to 69%) do not understand or read the information contained in generic hospital consent forms.2 Treating patients such as these can lead to compromised care and safety and increased medical malpractice risk.
Many bioethicists endorse the position that “striving for fully informed consent is generally unfeasible and perhaps even undesirable.”-- Others argue that the concept of fully informed consent should at least serve as an ideal. For that to be achieved, patients would need to understand fully their conditions and treatment. At a minimum, then, and as law, patients have the right to be given information that will optimize their autonomy.3-6 That information includes:
- The nature of the procedure or treatment being offered, including whether it is diagnostic or therapeutic;
- The risks and potential complications of a procedure or medical treatment;
- The benefits of the procedure; and
- Treatment alternatives, along with their risks and benefits.7
The ideal is far from reality. Frequently cited factors interfering with full comprehension, in addition to those already mentioned, include personal or cultural beliefs and low health literacy rates.1,2 Providers’ inability to communicate clearly in a rushed environment is also a factor, as is a tendency for providers who see the act of acquiring informed consent as a legal formality to delegate to a junior colleague.
But “the patient’s consent happens during the process of dialogue with the surgeon,” wrote Bernat and Peterson in the January 2006 Archives of Surgery:8 “The signature on a surgical consent form is merely the culmination and formalization of this preceding consent discussion and agreement.”
A signed consent form represents evidence of the patient’s consent—not of his or her understanding. That signed form may not be sufficient to protect providers in cases of liability. According to Jury Verdict Research, informed consent issues are among the top 10 most common reasons patients file malpractice claims.2
The low health literacy of almost half of adults in the United States limits their ability to understand the basic health information and services that are needed to make appropriate health decisions. In fact, articles in two of the July 2006 issues of the New England Journal of Medicine, as well as the entire August 2006 issue of the Journal of General Internal Medicine, are devoted to the subject of health literacy.9-11
Given that surgeons and other specialists are often responsible for securing informed consent, what are the areas of informed consent to which hospitalists should be attuned?
Key Considerations for the Hospitalist
Ordinarily, the person whose name is at the top of the patient’s chart has full responsibility for informed consent, although sometimes a subspecialty consultant, such as a cardiologist asking for a particular study, might help. A hospitalist might be named as the responsible provider in an area in which he or she is active.
Ben Rich, JD, PhD, a professor of bioethics at the University of California-Davis School (UCD) of Medicine in Sacramento, Calif., has considered the critical problems or distinctions that the hospitalist, as opposed to other physicians, may have in the area of informed consent. One area that strikes him as potentially risky is that of advance directives. Dr. Rich, who teaches a course on medicine and law at UCD, says that for decades experts have urged primary care physicians (PCPs) to discuss advance directives with patients as part of routine care. Even so, he acknowledges, if a patient is in critical condition and is hospitalized, “it is entirely possible that their personal physician won’t even know about it. So here is the person who is supposed to have apprised herself of the patient’s values and priorities in circumstances like that, and they’re out of the picture. And the person who is trying to interpret advance directives, if there is one, is the hospitalist.”
It might be difficult for the hospitalist to interpret any ambiguities. If the hospitalist believes it is impossible to know what the patient understood at the time they drafted the directive about the circumstances they are now facing, he or she may be more likely to dismiss it as invalid and simply make a decision as to what is medically appropriate, says Dr. Rich.
The discontinuity of care imposed by the hospitalist systems raises several ethical concerns, wrote Steven Pantilat, MD, in JAMA.12 The primary care physician and patient have previously negotiated, through the process of medical decision-making, the patient’s goals and values regarding medical interventions. “Because hospitalist systems leave no formal inpatient role for the PCP,” wrote Dr. Pantilat, “ … patients can no longer rely on agreements reached in the office following them to the hospital. Nonetheless, the hospitalist shares the PCP’s obligations to respect the ethical principles that agreements about preferences for care or individual values often represent.”
Another important but somewhat controversial issue involves whether a consent discussion held preoperatively also encompasses the management of post-procedure complications.8 Although it is impossible to mention all possible serious complications beforehand, it is prudent to reference the patient’s goals and general treatment preferences and to ensure that a family member (if not the designated surrogate) is present during this conversation. Just the same, each new intervention or procedure requires a new conversation and, in some cases, a new signed form. “Because at the end of the day,” says Patrick O’Rourke, JD, an attorney in Denver who regularly represents physicians in medical malpractice cases, “physicians are the people who have the obligation to obtain informed consent; the hospital as an institution does not, because hospitals don’t practice medicine; physicians do.”
Particularly with patients who face serious illness and those confronting what may be a chronic condition going forward, says Dr. Rich, “there’s a school of thought [that maintains] that part of the informed consent process is obsessively focused on procedures and pays woefully inadequate attention to the reasonable goals of care. This is nowhere more obvious than in the ICU setting.”
Continuums of Care and Consent
Indeed, any expert on medical law will tell you that informed consent is a process—not an event.8 Though a hospitalist may not have secured the signature on a consent form, a hospitalist’s practice is as much a part of a patient’s ongoing process of “consent” as is that of the surgeon who performed the patient’s operation.
The American Academy of Family Physicians has adopted the following guideline: “During the period of hospitalization, decisions regarding care, consultation, admission, transfer, and discharge should be the sole responsibility of the inpatient care physician in consultation with the patient and, as appropriate, the patient’s family physician and/or family members.”13 The times when patients actually sign informed consent documents are junctures in the continuum of consent that covers a lifetime healthcare experience. Hospitalists, then, are involved in informed consent from patient assignment to patient discharge.
“And the manner in which the process is conducted is at least as important as substantive information given,” says Dr. Rich. “A skilled and experienced physician can give any patient two descriptions of the procedure that they’re recommending,” he says. “[After o]ne, couched in a certain way, but not inaccurate, the patient would say, ‘Well, of course, I want that.’ And if the physician gives it in the other way, still accurate, the patient would say, Well, who would want that? And it all has to do with the terms you use, your tone of voice, your body language, the setting in which you provide it. … All that can profoundly shape the informed consent process. And it is not something that physicians are routinely taught.”
Because the process of informed consent is ongoing, discussions may continue for several sessions over a length of time before a patient decides to undergo a treatment. This gives patients more time to think of questions or concerns they may have. Addressing those concerns is a crucial part of the process.
“The reason that’s important is that you always want to offer and document that you have an opportunity to address what the patient’s questions were so the consent is truly informed,” says O’Rourke. One-way delivery of information is not equivalent to the dialogue implied by the term “informed consent.” “It is vitally important to ask, ‘What other information can I give you?’” he explains, especially because informed consent cases often deal with complications that develop after surgery.
Community Standard
The risks of procedures mentioned in informed consent discussions comprise a special category, says O’Rourke, “because there are some things that are not easily foreseen.” Some complications are not within the range generally anticipated after a procedure. “And the way the law works is that you don’t have to imagine the million-to-one shot [complication]; you would review the risks in terms of what a physician should disclose … in terms of significance.”
Physicians are judged by how well they informed patients of the risks as assessed by a community standard of what reasonable practitioners in the community say the risks are, he says. Physicians need to be knowledgeable about the risks of the procedure based on the medical literature, their training, and their discussions with colleagues.14
“Oftentimes, in order to give and get full informed consent, we use the knowledge from our subspecialty consultants,” says Dennis Manning, MD, FACP, FACC, a hospitalist and director of quality in the Department of Medicine and an assistant professor at the Mayo Clinic College of Medicine, Rochester, Minn. “We ask them, ‘What do you think the risks are?’ We might have to pick their brains in order to become fully aware of the hazards in a particular patient.”
“Risk is the category where litigation pops up and where you see the most challenges,” says O’Rourke, because the patient filing a claim may say, “ ‘Well, the doctor didn’t tell me about this risk and had I known this occurred, I would have elected to forego this procedure; I would have chosen one of the other alternatives.’ ”
If a patient develops a complication and the hospitalist must initiate a new intervention, then it’s the hospitalist’s duty to get informed consent for that next intervention. “Every time a physician undertakes a particular intervention, the patient has to be informed in why that intervention is being taken and what the risks, benefits, and alternatives are,” says O’Rourke.
If a patient is incapable of giving consent, then consider whether there is a significant risk in waiting until the patient is capable of giving informed consent. If the answer is “no,” then consider whether or not to delay the intervention. “If there’s no potential harm caused by waiting until the patient hits a higher level of consciousness,” says O’Rourke, “then that’s perfectly appropriate.”
In an emergency situation, a surrogate may need to make the decision. If neither one of those alternatives is available, “the law presumes that the patient is going to do what is reasonable and necessary in order to preserve his or her health, unless there’s been some instruction otherwise,” notes O’Rourke.
Teach Back
Studies show that when patients are asked to repeat what they understood from their informed consent discussions, they have greater recall and comprehension of the risks and benefits of surgical procedures.2,15 “Teach back” is an especially valuable technique to use with low literacy patients. The NQF discovered that the providers and departments using teach back were widely recognized by their peers as having the most well-informed patients compared with departments that did not use this method.2 (See “Teach Back in Action,” above right.) A number of studies have found that when a provider asks a patient to restate information or instructions, the benefits include providing a check for lapses of recall and understanding, revealing health beliefs, reinforcing and individualizing health messages, and motivating patients by activating dialogue.15
In May 2003, the NQF published Safe Practices for Better Healthcare, which endorsed a set of consensus standards for 30 healthcare practices, one of which (Safe Practice 10) recommends that all healthcare professionals ask patients to teach back what they have been told by their providers during their informed consent discussions.2
In its 2001 report, Making Health Care Safer: A Critical Analysis of Patient Safety Practices (project director, Robert M. Wachter, MD), the Agency for Healthcare Research and Quality suggested that special attention be paid to implementing 11 particular practices, one of which was “asking that patients recall and restate what they have been told during the informed consent process.”16
Even if you are not asking for a signed form, physicians, nurses, interpreters, and any professional who communicates with patients regarding their healthcare decisions is involved in the informed consent process and should use teach back—especially with those patients who find even basic health information difficult to understand. Although the NQF found that physicians were reluctant to incorporate this technique into their communications, the providers reported anecdotally that teach back takes less than a minute to complete; research backs up the claim that the more the technique is practiced, the speedier it gets.2
The provision of this “interactive communication loop,” as it has been called,15 has also been shown to affect clinical outcomes. In a study by Schillinger and colleagues conducted at an outpatient general internal medicine clinic and at San Francisco General Hospital, physicians assessed recall and comprehension of any new concept in 12 (20%) of 61 outpatient visits by diabetic patients for 15 (12%) of 124 concepts.15 The patients whose physicians assessed their recall by means of teach back were more likely to have hemoglobin A1c levels below the mean compared with patients whose doctors did not. The two variables found to be independently associated with good glycemic control were higher health literacy levels and physicians’ application of the teach-back strategy.
Consent Forms
The informed consent process is intended to protect patients and physicians both.7 Legal doctrine, including hospital accreditation standards, ethical theories, and perspectives on the physician-patient relationship, emphasizes the importance of full patient comprehension regarding treatment. But many hospitals do not use forms that contribute to that objective. In a study by Bottrell and colleagues of 540 forms from 157 hospitals nationwide, 96% indicated the nature of the procedure for the patient; however, only 26% of forms included all four elements of informed consent: procedure, risks, benefits, and alternative treatment options. Thirty-five percent included three of four elements, 23% provided two of four elements, 14% listed only one element, and 2% contained none of the elements.
In general, the investigators concluded, the forms appear to be designed to authorize treatment or protect hospitals and caregivers from liability rather than to help patients clarify information or make decisions. Even hospitals in states that have statutes requiring institutions to include all four elements on their forms were no more likely to do so than those in other states. Fewer than 40% of forms were found to support models of shared decision making, the basis of patient autonomy and the overarching intention for informed consent.
“Generally … informed consent forms are seen as mere documentation vehicles, and perhaps as legal protection, regardless of whether the process of informed consent was successfully accomplished or of minimal quality,” this study’s authors wrote, and because patients are not blind to the intentions of these forms, this may add to their discomfort.7 Most forms, the authors concluded, are insufficient because the language used does not accommodate low health literacy or because there are no graphic features.
On the other hand, “informed consent can sometimes get very awkward and cumbersome,” says William Jacott, MD, special advisor for professional relations at the Joint Commission on Accreditation of Healthcare Organizations, St. Paul, Minn., for the past five years and liaison to SHM for the past two. Some institutions or organizations interpret Joint Commission and other legal standards excessively, he says, “and I’ve seen 10-page consent forms, which just overwhelms the patient, let alone the doctor. So an over-interpretation and overkill need to be avoided.”
Conclusion: Communication and Documentation
The ways in which hospitalists can avoid the pitfalls of faulty informed consent conversations include close communication with surgeons as well as other colleagues.
“We have a great tendency to communicate via the medical record,” says Dr. Jacott, and if a patient’s co-managers (the hospitalist and subspecialist) don’t communicate, “one might assume the other has already done [informed consent], and nobody does it.”
He has also seen instances in teaching hospitals in which both the surgeon and the hospitalist incorrectly assume that the house staff has acquired informed consent.
Nurses can also help hospitalists ensure that patients are comfortable with their treatment choices. “Nurses often have more firsthand information about when patients are confused or scared or dubious or are somehow being coerced or manipulated into consenting to something,” says Dr. Rich.
Hospitalists should also avoid making assumptions about the completeness of their colleagues’ discussions with patients and should look for clear documentation as well as record their own. “Some subspecialists play fast and loose with informed consent,” Dr. Rich says, “and [may] resent a medical staff colleague who takes it seriously and attempts to hold them accountable for really doing it right. And for the hospitalist, that’s where it is critical that their institution stand behind them.”
A hospitalist’s responsibilities with regard to informed consent also include ensuring that the patient’s consent is truly informed. Using the teach back method, allowing time for the patient to ask questions and voice concerns, and including all four elements of informed consent on the patient’s consent form are just some of the ways the hospitalist can play an essential role in the continuum that is informed consent.
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Epstein M. Why effective consent presupposes autonomous authorisation: a counterorthodox argument. J Med Ethics. 2006;32:342-345.
- National Quality Forum. Implementing a national voluntary consensus standard for informed consent: a user’s guide for healthcare professionals. September 2005. Available at: www.qualityforum.org/publications.html. Accessed September 5, 2006.
- Rizzo v Schiller, 445 SE2d 153 (Va. 1994). Available at: www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=10184327&dopt=Abstract. Accessed September 11, 2006.
- Gorab v Zook, 943 P2d 423 (Colo. 1997). Available at: http://caselaw.lp.findlaw.com/scripts/getcase.pl?court=co&vol=2003app%5C3477&invol=1. Accessed September 11, 2006.
- Schuck PH. Rethinking informed consent. Yale Law J. 1994;103:899-959.
- Culbertson v Mernitz, 602 NE2d 98 (Ind. 1992).
- Bottrell MM, Alpert H, Fischbach RL, et al. Hospital informed consent for procedure forms: facilitating quality patient-physician interaction. Arch Surg. 2000 Jan;135(1):26-33.
- Bernat JL, Peterson LM. Patient-centered informed consent in surgical practice. Arch Surg. 2006 Jan;141(7):86-92.
- Marcus EN. The silent epidemic—the health effects of illiteracy. N Engl J Med. 2006;355:339-341.
- Flores G. Language barriers to health care in the United States. N Engl J Med. 2006 Jul;355:229-231.
- Carmona RH. Health literacy: a national priority. J Gen Intern Med. 2006;21:803.
- Pantilat SZ, Alpers A, Wachter RM. A new doctor in the house: ethical issues in hospitalist systems. JAMA. 1999 Jul 14;282:171-174.
- Henry LA. What the hospitalist movement means to family physicians. Fam Pract Manag. 1998 Nov-Dec;5(10):54-62.
- Rajput V, Bekes CE. Ethical issues in hospital medicine. Med Clin North Am. 2002 Jul;86(4):869-886.
- Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003 Jan 13;163(1):83-90.
- University of California at San Francisco (UCSF)-Stanford University Evidence-based Practice Center. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment: Number 43. AHRQ Publication No. 01-E058, July 2001. Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/clinic/ptsafety/. Accessed September 5, 2006.
- Baum N. Comprehension is the key: the challenge hospitals face is that many patients do not understand the fundamental information regarding their treatment plans. Patient Safety Quality Healthcare. May/June 2006:35-38.
Things You Can Do To Save Lives
In April 2005, the American Hospital Association’s magazine, Hospital and Health Networks (H&HN), published the article “25 Things You Can Do to Save Lives Now.”1 In it, experts from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), the Institute for Healthcare Improvement (IHI), the National Quality Forum (NQF), and the Centers for Medicare and Medicaid Services (CMS), commented on an action plan to advance hospitals’ patient safety activities.
Now The Hospitalist has researched hospitalists’ views on these same 25 items. Those views are presented below.
A number of these items “are already highly ensconced in the JCAHO and CMS criteria,” says Dennis Manning, MD, FACP, FACC, director of quality in the Department of Medicine and an assistant professor at the Mayo Clinic College of Medicine, Rochester, Minn. “In terms of power of the things on the list for potentially saving lives, what we sometimes look at are the things that have the potential for the most prevention.”
Brian Alverson, MD, pediatric hospitalist at Hasbro Children’s Hospital in Providence, R.I., adds his thoughts on the 25 items: “We have to hold in our minds a healthy nervousness about patients being hospitalized, in that there is an inherent danger to that phenomenon. No matter how hard we strive for perfection in patient care, to err is human.”
Shortening hospital length of stay to within a safe range, he believes, is one of the best ways to reduce those daily dangers.
Some of the 25 items pose more challenges for hospitalists than others, and the contrary is true as well. Some were judged to be of lesser concern due to guidelines or imperatives imposed on hospitals by regulatory organizations. Other items fall outside hospitalists’ accountabilities, such as incorrect labeling on X-rays or CT scans, overly long working hours, medical mishaps (such as wrong-site, wrong-person, and wrong-implant surgeries), and ventilator-associated pneumonia. A few items were those that hospitalists found challenging, but for which they had few suggestions for solutions. In some, there were obstacles standing in the way of their making headway toward conquering the menace. These included:
1. Improper Patient Identification
“Until we set up a system that improves that, such as an automated system,” says one hospitalist, “I’ll be honest with you, I think we can remind ourselves ’till we’re blue in the face and we’re still going to make mistakes.”
2. Flu Shots
“Flu shots are probably more important in the pediatrics group than in any [other] except the geriatric group,” says Dr. Alverson, who strongly believes that pediatricians should be able to administer flu shots in the inpatient setting, “because we can catch these kids with chronic lung disease—many of [whom] are admitted multiple times.”
3. Fall Prevention
This item is one of the National Patient Safety goals, and one that every institution is trying to address. In pediatrics, says Dr. Alverson, the greater problem “is getting people to raise the rails of cribs. Kids often fall out of cribs because people forget to raise the rail afterwards, or don’t raise it high enough for a particularly athletic or acrobatic toddler.”
The other items on the list of 25 are below, including a section for medication-related items and the sidebar on a venous thromboembolism (VTE) prevention program.
4. Wash Hands
Provider hand-washing has been well studied, says one hospitalist, and “the data are so depressing that no one wants to deal with it.” Another says, “We just nag the hell out of people.”
One of the hospitalists interviewed for this story read the H&HN article and responds, “We do all these things.” But a lack of self-perception regarding this issue—as well as others—is also well-documented: Physicians who are queried will say they always wash their hands when, in fact, they do so less than 50% of the time.2-5
Despite the value of hand sanitizers—whether they are available at unit entrances, along the floors, at individual rooms, or carried in tiny dispensers that can be attached to a stethoscope—some pathogens, such as the now-epidemic Clostridium difficile, are not vulnerable to the antisepsis in those mechanisms.
“C. dif is a set of spores that are less effectively cleaned by the topical hand sanitizers,” says Dr. Alverson, who is also an assistant professor of pediatrics at Brown University in Providence, R.I. “In those cases, soap and water is what you need.”
Peter Angood, MD, FRCS(C), FACS, FCCM, vice president and chief patient safety officer of JCAHO, Oakbrook, Ill., says provider hand-washing is a huge patient safety issue and, in general, a multi-factorial problem that is more complicated than it would seem on the surface.
“We can rationalize and cut [providers] all kinds of slack, but at the bottom line is human behavior and their willingness to comply or not comply,” he says. “It’s like everything else: Why do some people speed when they know the speed limit is 55?”
Addressing the solution must be multi-factorial as well, but all hospitalists can serve as role models for their colleagues and students, including remaining open to reminders from patients and families.
5. Remain on Kidney Alert
Contrast media in radiologic procedures can cause allergic reactions that lead to kidney failure. This is a particularly vexing problem for elderly patients at the end stages of renal dysfunction and patients who have vascular disease, says Dr. Manning. Although the effects are not generally fatal, the medium can be organ-damaging. “This is a hazard that’s known, and it has some mitigating strategies,” he says, “but often it can’t be entirely eliminated.”
Measures that reduce the chance of injury, say Dr. Manning, include ensuring that the contrast medium is required; confirming that the procedure is correct for the patient, with the right diagnosis, with a regulated creatinine, and well coordinated with the radiology department; “and then getting true informed consent.” But at a minimum, he emphasizes, is the importance of hydration. “There is some evidence that hydration with particular types of intravenous fluids can help reduce the incidence of the kidney revolting.” And, he says, “there are a number of things that we have to do to make sure this is standardized.”
6. Use Rapid Response Teams
Use of “[r]apid response teams [RRTs] is one of the most powerful items on the list,” says Dr. Manning, who serves on SHM’s committee on Hospital Quality and Patient Safety as well as the committee helping to design the Ideal Discharge for the Elderly Patient checklist. “Whereas every hospital has a plan for response,” he says, RRTs are “really a backup plan.”
In 2003, Dr. Manning served as faculty for an IHI program in which a collaborative aimed at reducing overall hospital mortality. The formation and application of RRTs at six hospitals in the United States and two in the United Kingdom was the most promising of the several interventions, with impact on a variety of patients whose conditions were deteriorating in non-ICU care areas.
The advantage of RRTs with children, says Daniel Rauch, MD, FAAP, director of the Pediatric Hospitalist Program at NYU Medical Center, New York City, is that it is often difficult for providers to know what may be wrong with a child who is exhibiting symptoms. “Is the kid grunting because they’re constipated, because that’s the developmental stage they’re in, they’re in pain, or are they really cramping on you?” he asks.
7. Check for Pressure Ulcers
Checking for pressure ulcers is the task of nurses and physicians, say hospitalists, and they agree that it has to be done at admission. “The patient’s entire skin needs to be checked,” says Dr. Manning, “and often it takes both the nurse and doctor to roll the patient and get a good look at their bottom or their back … especially if the patient might have come from a nursing home and has a chronic serious illness.”
Also important, he says, is to fully assess the type of decubitus skin situation or any skin problem and then to monitor the patient to prevent advancement. “Multidisciplinary rounds can help,” he says, “and collaborative communication is key.”

8. Give the Patient and Family a Voice
“We fully embrace the involvement of the patient in the process of their care,” says Dr. Angood, who is also the co-director of the Joint Commission International Center for Patient Safety, for which patient and family involvement is a priority.
Giving patients and family members a voice is a fine idea, say our hospitalists, especially with children: No one knows a patient like their parents. As the H&HN article points out, anecdotal evidence is largely responsible for the belief that patient and family involvement helps reduce the likelihood for errors, and patient and family participation on safety committees can be a boon to advancing safety as well as satisfaction. But, says Dr. Alverson, “one has to keep in mind that parents have a perspective and not the only perspective on patient safety. I think a broad group of people has to sit down to address these issues.”
In the post-surgical setting, says Dr. Rauch, hospitalists make an invaluable contribution. “If surgeons don’t even come by to listen to the parents or see the child, it’s helpful to have that co-management of someone who’s used to listening to parents, who credits the parents for knowing their kids, and who will do the appropriate thing.” Dr. Angood, who is a past president of the Society of Critical Care Medicine, believes “that that patient-physician relationship is still going to be the driver for the majority of healthcare for some time yet.”
9. Reduce Catheter-Related Bloodstream Infections
“If it’s not required, we want every foreign body out,” says Dr. Manning. “We have to ask ourselves every day whether they are still required.”
The geriatric service at the Mayo Clinic (Rochester, Minn.) developed a daily mnemonic of A-B-C-D-E where B stands for binders. This, he says, “is a way for us to remind ourselves that any therapeutic foreign objects that are tethering the patient—and many of them are catheters—are of concern. We need to push the question [Is this still required?] to ourselves and then act on it.”
Dr. Alverson says, “There are certain infections [for which] we’re starting to move away from PICC [peripherally inserted central catheters] line management, and one way to mitigate that is to be on top of when you can actually discontinue the catheter.” For example, “in pediatrics, there are emerging data that with osteomyelitis you can have a shortened course of IV antibiotics and then switch to oral antibiotics. … That can reduce by half your PICC line duration. Being savvy about this is important.”
10. Reduce Heart Attack Death Rates
“There are about eight interventions for heart attacks that have increased survival,” says Dr. Manning. “So every hospital is working with these. We are using the all-or-none criteria, meaning that there are assurances [in place] that every patient will get all of them.”
Re-engineering systems has been particularly meaningful in preventing and treating heart attacks, says Dr. Manning, who represented SHM at a meeting of the Alliance for Cardiac Care Excellence (ACE), a CMS-based coalition that includes leaders from more than 30 healthcare organizations, and is working to ensure that all hospitalized cardiac patients regularly receive care consistent with nationally accepted standards.
11. Institute Multidisciplinary Rounds
Time constraints mean rounding with 10 people will necessarily be slower, says Dr. Alverson. In academic institutions where the hospitalist has the dual responsibility of teaching, this is especially time-consuming. Although there is an increasing emphasis that providers should participate at bedside rounds, and this is “clearly better from the patient’s perspective and, I would argue, better from the educational perspective,” says Dr. Alverson, it is “fairly bad from the getting-things-done-in-a-timely-fashion perspective. So it’s tough, and to a certain degree, in a practical world you have to pick and choose.”
When a nurse representative is there to respond to the question, “ ‘Why didn’t the kid get his formula? [and says] because he didn’t like the taste,’ that’s something that we might not pick up on,” says Dr. Alverson.
At NYU Medical Center, where Dr. Rauch works, formal rounds take place at least once a week (sometimes more), depending on volume, and they informally take place twice a day, every day.
“It works pretty well,” he says. “The nurses are a critically important part of teams; everybody recognizes that, and they are included in decisions.” Physicians put out the welcome mat for nurses even in casual circumstances. “Sometimes I am discussing things with the house staff [and] a nurse will pull up a chair and become part of the conversation. It’s a part of our culture.”
Although it is unusual to get a pharmacist to round with his team, says Dr. Alverson, a nearby pharmacy school sends students to join rounds, providing what might otherwise be a missing element of education.
12. Avoid Miscommunication
A number of the hospitalists interviewed were asked what they considered to be the top two or three communication points for hospitalists. Verbal orders, clarifying with read-backs, clear handwriting, and order sets were named frequently. In academic settings, says one hospitalist, instructors should be careful to make sure that residents, interns, and medical students understand what you’re saying and why you’re saying it. Good communication with the family was also cited as crucial.
“The most challenging issue is communicating at all,” says Dr. Rauch, who is also an associate professor of pediatrics at the NYU School of Medicine. Although he was the only one to phrase it this way, it is probably not a unique view. “In a large, old, academic medical institution, there are a lot of hierarchical issues that [impede] rapidly responding to [patients’] needs.” Unfortunately, it may mean communicating up one authorization pathway and down another. “And you can see the layers of time and the game of telephone as the concerns go around,” he says. “We’ve tried to break that down so the people who are on site can speak to someone who can make a decision.”
Along with that, he says, it is important from the outset to make it very clear who makes the decision. “For example, when the patient is a child getting neurosurgery because they have a seizure disorder and they also are developmentally delayed and they have medical issues, you now have at least three services involved with managing the child,” says Dr. Rauch. When three people are making decisions, he points out, no decision gets made. “You really have to decide when that child comes in who is going to call the shots for what issue. It’s usually the hospitalist who brings it up, and when it works, it works well.”

13. Empower Nurses and Other Clinicians
Nursing staff should have the power to halt unsafe practices. To Tahl Humes, MD, hospitalist at Exempla St. Joseph’s Hospital in Denver, halting unsafe practices depends, once again, on good lines of communication, and recognizing that patient care is a joint responsibility. For example, she says, “instead of just going to see the patient, writing the note, writing the order, and putting the chart away,” the hospitalists “talk with nurses daily and tell them what they’re planning to do,” so there is more opportunity to catch what might be unsafe practices.
14. Reduce Wound Infections
Although reducing wound infections is something in which their surgical colleagues take the lead, says Dr. Manning, “in our perioperative consultation care, we often work with surgery and anesthesiology in the pre-op evaluations of the patients. So in the surgical care improvement projects, we are often partners.”
Hospitalists are also frequently members on quality committees that help to brainstorm solutions to serious problems. One such project is the Surgical Care Improvement Program (SCIP), spearheaded by David Hunt, MD, with the Office of Clinical Standards and Quality, CMS. SCIP is an effort to transform the prevention of postoperative complications. Its goal is to reduce surgical complications by 25% in the United States by the year 2010 in four target areas: surgical site infections, and cardiac, respiratory, and venous thromboembolic complications. (See Figures 1 and 2, p. 33.)
This includes those patients who are already on beta-blockers. “From the hospitalist’s standpoint,” says Dr. Manning, “we have a real role in … [ensuring] that their beta blockade is maintained.”
Dr. Humes says that at her institution, a wound care nurse can have that responsibility. If a provider is concerned about any patient in this regard, he or she can order that the patient be seen by a wound care nurse and, depending on what’s needed, by a physical therapist.
Now we move on to address those issues that are medication-related:
15. Know Risky Meds
Pediatric hospitalists are involved with postoperative patients at Dr. Rauch’s institution. All patients’ orders are double-checked, he says, and computer order entry also helps providers calculate pediatric dosage norms or dosages calculated by weight.
The hospitalist has the opportunity to be involved in the pharmacy’s selection of drugs for the formulary, says Erin Stucky, MD, pediatric hospitalist at University of California, San Diego, and to help decide the drug choices within a certain class and limit the numbers of things that are used most frequently that are visually different in appearance. “And although that’s the pharmacist’s purview,” she says, “the hospitalist has a vested interest in being on the Pharmacy and Therapeutics Committee to review and restate to pharmacists what they’re using based on clinical need and to find a way for that drug to be safely stored in pharmacy if, indeed, there are a couple of drugs from one class that are truly useful.”
A drug’s generic name, brand name, dose strength, frequency of administration, place of use, indications, and contraindications are all important factors to determine the potential risks of drugs. But “you can’t say a list of risky medications at one institution is the same as it should be elsewhere,” says Dr. Stucky. Risky medications will depend on the setting in which the physician works. Hospitalists need to think logically about the drugs that are the most used or are new, including any new drug that has a different method by which it is administered or a different interaction capability with standard drugs.
“If there’s a new antibiotic that’s known to be processed through the liver and you have multiple patients with heart failure medications who have a medication basis that could be at conflict with that new drug, that’s a potentially risky medication,” she points out. “It may be easier in some ways for the pharmacist to be the rate-limiting factor for how they’re dispensed and for which patients they recheck [against] that incompatibility list.” But in large part, the avoidance of those risky-medication errors must be a commitment of the pharmacist and a bedside nurse.

16. Beware of Sound-Alike and Look-Alike Drugs
Dr. Stucky believes a majority of physicians don’t know the color or size of the pills they’re prescribing. “I would challenge all hospitalists to take every opportunity at the bedside,” she says, “to watch the process happening and know what those drugs and pills need to look like.”
Another opportunity is to educate family members “to remind them that [the patient is] going to be getting these medicines, these are the names of the medicines, and please ask the nurse about these medicines when you get them,” she says. If the hospitalist gives a new drug to the patient, the family can be another safeguard.
Dr. Stucky points out that you can tell the patient and family, “I’m going to tell the nurse that you’re going to be asking about this because … you are the best guide to help us make sure that these medicines are administered safely.” She also emphasizes that assigning this responsibility to the patient is important “because when people leave the hospital, we suddenly expect them to know how to take 18 pills.”
If, on a given unit, you have to handle cases with multiple diagnoses, says Dr. Stucky, it may be difficult to physically isolate the look-alike drugs. “At our institution we found that we actually had to pull the machines out,” she says, referring to the PIXUS units. “You can’t have them on the same wall even in different locations. You have to choose one or the other [similar looking pills].”
The sound-alike drugs are most ripe for errors with verbal orders. “Hospitalists can set a precedent in their institutions that any verbal orders should have the reason for that order given,” she explains. If you order clonazepam, after you finish giving the order verbally to the nurse, you should state, “This is for seizures.”
“When the nurse is writing it down, she may or may not be the one to know that that drug name is indeed in that drug class, but the pharmacist will know,” explains Dr. Stucky.

17. Reconcile Medications
“It is important for people to do verbal sign-out, certainly among attendings,” says Dr. Alverson, “to explain [in better depth] what’s going on with the patient and to maintain those avenues of communication in case something goes wrong. Hospitals get in trouble when physicians aren’t able to communicate or speak with each other readily.”
The biggest challenge for the pediatric hospitalists at NYU Hospital, says Dr. Rauch, is assessing the most up-to-date list of medications. “For instance,” he says, “we had a child yesterday as part of post-op care. I hadn’t met them pre-op. The father said, ‘I think my daughter’s on an experimental protocol with this additional medication.’ It wasn’t something we were used to so we called Mom: Can you bring in the protocol? She said, ‘Oh, she hasn’t been on that drug in a long time.’”
In fact, whether the patient is a child or adult, the majority of cases assigned to hospitalists are unplanned admissions and this is something with which all hospitalists struggle. But regarding transferring patients from unit to unit, says Dr. Stucky, “this is a whole different ballgame. That’s where we have a huge opportunity to make an impact.”
She suggests that matching medications to patients can be ameliorated by computer-based systems in which at each new place the hospitalist can fill in a printout regarding whether they’re continuing a drug order, changing it, or discontinuing it, and this system also works effectively on discharge. “In a perfect world,” says Dr. Stucky, … “the hospitalist would be the implementer of this kind of medication reconciliation in their institution.”
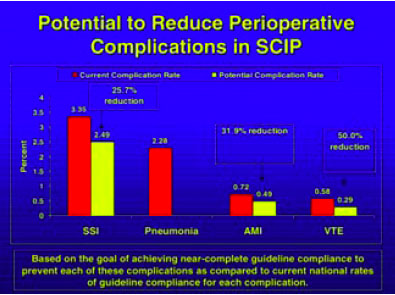
18. Avoid Unacceptable Drug Abbreviations
Some medications have abbreviations that can be misinterpreted. The classic ones, say several hospitalists, are magnesium and morphine. Others pertain to miswritten units of administration.
Read-backs on verbal medication orders was one of the elements most cited by our hospitalists as priority communication practices. Eliminating confusing abbreviations is one of JCAHO’s National Patient Safety Goals and “hospitals are aggressively rolling out ways to remind physicians not to use them,” says Dr. Alverson.
At Dr. Manning’s institution they use the Safest in America criteria, a collaboration of 10 Twin Cities and the hospital systems in Rochester, Minn., as well as the Institute for Clinical Systems Improvement. At Mayo, they call it “Write It Right.” An accentuated campaign to reduce ambiguities in medication communications, he says, has resulted in “profound improvement” in standardizing medication prescribing and following the read-back rules.
Dr. Stucky suggests that hospitalists take on mini-projects where they review the past six months of order-writing errors in their institutions, noticing any trends and, particularly, any unit-specific trends (such as the misunderstanding of the abbreviation cc). If you notice the errors are unit-specific, you can also analyze whether they are treatment-specific. In that way, “order sets can be pre-typed and all the providers have to do is fill in the numbers,” she says, adding that hospitalists can perform these analyses outside their own patient area.
19. Improper Drug Labeling, Packaging, and Storage
Drug names, labels, and packaging contribute significantly to medication errors. The risk for errors is determined by both the product and the environment in which it is used. Most hospitalists say they are continually developing new protocols and checking information multiple times. Sometimes, small changes go a long way. “Our patient safety officer has a favorite phrase: ‘How can I facilitate you to do something different next Tuesday?’ Within your own hospital, that means look at your system and pick something you know you can change,” says Dr. Stucky. “You can’t buy IT tomorrow; you can’t do physician order entries [because] your computer system doesn’t allow it—but what can you do?”

Conclusion
Dr. Angood encourages hospitalists to continue learning how to interact with other disciplines that are also evolving into hospital-based practices and to learn how to manage the specific details-of-change topics such as this list of 25—not just to gloss over them, but to understand them, and to encourage patient involvement and nurture the physician-patient relationship to help change the culture within health care.
“We can pick these kinds of topics and can dissect them all down, but each time, in the end, it is a matter of people and their behaviors as a culture inside a system,” he says. “The system can be changed a little bit, but still it is ultimately about the culture of people.” TH
Andrea Sattinger writes regularly for The Hospitalist.
References
- Runy LA. 25 things you can do to save lives now. Hosp Health Netw. 2005 Apr;79(4):27-28.
- Meengs MR, Giles BK, Chisholm CD, et al. Hand washing frequency in an emergency department. Ann Emerg Med. 1994 Jun;23(6):1307-1312.
- McGuckina M, Watermana R, Storrb J, et al. Evaluation of a patient-empowering hand hygiene programme in the UK. J Hosp Infect. 2001 Jul;48(3):222-227.
- Whitby M, McLaws ML, Ross MW. Why healthcare workers don't wash their hands: a behavioral explanation. Infect Control Hosp Epidemiol. 2006 May;27(5):484-492.
- Lipsett PA, Swoboda SM. Handwashing compliance depends on professional status. Surg Infect. 2001 Fall;2(3):241-245.
In April 2005, the American Hospital Association’s magazine, Hospital and Health Networks (H&HN), published the article “25 Things You Can Do to Save Lives Now.”1 In it, experts from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), the Institute for Healthcare Improvement (IHI), the National Quality Forum (NQF), and the Centers for Medicare and Medicaid Services (CMS), commented on an action plan to advance hospitals’ patient safety activities.
Now The Hospitalist has researched hospitalists’ views on these same 25 items. Those views are presented below.
A number of these items “are already highly ensconced in the JCAHO and CMS criteria,” says Dennis Manning, MD, FACP, FACC, director of quality in the Department of Medicine and an assistant professor at the Mayo Clinic College of Medicine, Rochester, Minn. “In terms of power of the things on the list for potentially saving lives, what we sometimes look at are the things that have the potential for the most prevention.”
Brian Alverson, MD, pediatric hospitalist at Hasbro Children’s Hospital in Providence, R.I., adds his thoughts on the 25 items: “We have to hold in our minds a healthy nervousness about patients being hospitalized, in that there is an inherent danger to that phenomenon. No matter how hard we strive for perfection in patient care, to err is human.”
Shortening hospital length of stay to within a safe range, he believes, is one of the best ways to reduce those daily dangers.
Some of the 25 items pose more challenges for hospitalists than others, and the contrary is true as well. Some were judged to be of lesser concern due to guidelines or imperatives imposed on hospitals by regulatory organizations. Other items fall outside hospitalists’ accountabilities, such as incorrect labeling on X-rays or CT scans, overly long working hours, medical mishaps (such as wrong-site, wrong-person, and wrong-implant surgeries), and ventilator-associated pneumonia. A few items were those that hospitalists found challenging, but for which they had few suggestions for solutions. In some, there were obstacles standing in the way of their making headway toward conquering the menace. These included:
1. Improper Patient Identification
“Until we set up a system that improves that, such as an automated system,” says one hospitalist, “I’ll be honest with you, I think we can remind ourselves ’till we’re blue in the face and we’re still going to make mistakes.”
2. Flu Shots
“Flu shots are probably more important in the pediatrics group than in any [other] except the geriatric group,” says Dr. Alverson, who strongly believes that pediatricians should be able to administer flu shots in the inpatient setting, “because we can catch these kids with chronic lung disease—many of [whom] are admitted multiple times.”
3. Fall Prevention
This item is one of the National Patient Safety goals, and one that every institution is trying to address. In pediatrics, says Dr. Alverson, the greater problem “is getting people to raise the rails of cribs. Kids often fall out of cribs because people forget to raise the rail afterwards, or don’t raise it high enough for a particularly athletic or acrobatic toddler.”
The other items on the list of 25 are below, including a section for medication-related items and the sidebar on a venous thromboembolism (VTE) prevention program.
4. Wash Hands
Provider hand-washing has been well studied, says one hospitalist, and “the data are so depressing that no one wants to deal with it.” Another says, “We just nag the hell out of people.”
One of the hospitalists interviewed for this story read the H&HN article and responds, “We do all these things.” But a lack of self-perception regarding this issue—as well as others—is also well-documented: Physicians who are queried will say they always wash their hands when, in fact, they do so less than 50% of the time.2-5
Despite the value of hand sanitizers—whether they are available at unit entrances, along the floors, at individual rooms, or carried in tiny dispensers that can be attached to a stethoscope—some pathogens, such as the now-epidemic Clostridium difficile, are not vulnerable to the antisepsis in those mechanisms.
“C. dif is a set of spores that are less effectively cleaned by the topical hand sanitizers,” says Dr. Alverson, who is also an assistant professor of pediatrics at Brown University in Providence, R.I. “In those cases, soap and water is what you need.”
Peter Angood, MD, FRCS(C), FACS, FCCM, vice president and chief patient safety officer of JCAHO, Oakbrook, Ill., says provider hand-washing is a huge patient safety issue and, in general, a multi-factorial problem that is more complicated than it would seem on the surface.
“We can rationalize and cut [providers] all kinds of slack, but at the bottom line is human behavior and their willingness to comply or not comply,” he says. “It’s like everything else: Why do some people speed when they know the speed limit is 55?”
Addressing the solution must be multi-factorial as well, but all hospitalists can serve as role models for their colleagues and students, including remaining open to reminders from patients and families.
5. Remain on Kidney Alert
Contrast media in radiologic procedures can cause allergic reactions that lead to kidney failure. This is a particularly vexing problem for elderly patients at the end stages of renal dysfunction and patients who have vascular disease, says Dr. Manning. Although the effects are not generally fatal, the medium can be organ-damaging. “This is a hazard that’s known, and it has some mitigating strategies,” he says, “but often it can’t be entirely eliminated.”
Measures that reduce the chance of injury, say Dr. Manning, include ensuring that the contrast medium is required; confirming that the procedure is correct for the patient, with the right diagnosis, with a regulated creatinine, and well coordinated with the radiology department; “and then getting true informed consent.” But at a minimum, he emphasizes, is the importance of hydration. “There is some evidence that hydration with particular types of intravenous fluids can help reduce the incidence of the kidney revolting.” And, he says, “there are a number of things that we have to do to make sure this is standardized.”
6. Use Rapid Response Teams
Use of “[r]apid response teams [RRTs] is one of the most powerful items on the list,” says Dr. Manning, who serves on SHM’s committee on Hospital Quality and Patient Safety as well as the committee helping to design the Ideal Discharge for the Elderly Patient checklist. “Whereas every hospital has a plan for response,” he says, RRTs are “really a backup plan.”
In 2003, Dr. Manning served as faculty for an IHI program in which a collaborative aimed at reducing overall hospital mortality. The formation and application of RRTs at six hospitals in the United States and two in the United Kingdom was the most promising of the several interventions, with impact on a variety of patients whose conditions were deteriorating in non-ICU care areas.
The advantage of RRTs with children, says Daniel Rauch, MD, FAAP, director of the Pediatric Hospitalist Program at NYU Medical Center, New York City, is that it is often difficult for providers to know what may be wrong with a child who is exhibiting symptoms. “Is the kid grunting because they’re constipated, because that’s the developmental stage they’re in, they’re in pain, or are they really cramping on you?” he asks.
7. Check for Pressure Ulcers
Checking for pressure ulcers is the task of nurses and physicians, say hospitalists, and they agree that it has to be done at admission. “The patient’s entire skin needs to be checked,” says Dr. Manning, “and often it takes both the nurse and doctor to roll the patient and get a good look at their bottom or their back … especially if the patient might have come from a nursing home and has a chronic serious illness.”
Also important, he says, is to fully assess the type of decubitus skin situation or any skin problem and then to monitor the patient to prevent advancement. “Multidisciplinary rounds can help,” he says, “and collaborative communication is key.”
8. Give the Patient and Family a Voice
“We fully embrace the involvement of the patient in the process of their care,” says Dr. Angood, who is also the co-director of the Joint Commission International Center for Patient Safety, for which patient and family involvement is a priority.
Giving patients and family members a voice is a fine idea, say our hospitalists, especially with children: No one knows a patient like their parents. As the H&HN article points out, anecdotal evidence is largely responsible for the belief that patient and family involvement helps reduce the likelihood for errors, and patient and family participation on safety committees can be a boon to advancing safety as well as satisfaction. But, says Dr. Alverson, “one has to keep in mind that parents have a perspective and not the only perspective on patient safety. I think a broad group of people has to sit down to address these issues.”
In the post-surgical setting, says Dr. Rauch, hospitalists make an invaluable contribution. “If surgeons don’t even come by to listen to the parents or see the child, it’s helpful to have that co-management of someone who’s used to listening to parents, who credits the parents for knowing their kids, and who will do the appropriate thing.” Dr. Angood, who is a past president of the Society of Critical Care Medicine, believes “that that patient-physician relationship is still going to be the driver for the majority of healthcare for some time yet.”
9. Reduce Catheter-Related Bloodstream Infections
“If it’s not required, we want every foreign body out,” says Dr. Manning. “We have to ask ourselves every day whether they are still required.”
The geriatric service at the Mayo Clinic (Rochester, Minn.) developed a daily mnemonic of A-B-C-D-E where B stands for binders. This, he says, “is a way for us to remind ourselves that any therapeutic foreign objects that are tethering the patient—and many of them are catheters—are of concern. We need to push the question [Is this still required?] to ourselves and then act on it.”
Dr. Alverson says, “There are certain infections [for which] we’re starting to move away from PICC [peripherally inserted central catheters] line management, and one way to mitigate that is to be on top of when you can actually discontinue the catheter.” For example, “in pediatrics, there are emerging data that with osteomyelitis you can have a shortened course of IV antibiotics and then switch to oral antibiotics. … That can reduce by half your PICC line duration. Being savvy about this is important.”
10. Reduce Heart Attack Death Rates
“There are about eight interventions for heart attacks that have increased survival,” says Dr. Manning. “So every hospital is working with these. We are using the all-or-none criteria, meaning that there are assurances [in place] that every patient will get all of them.”
Re-engineering systems has been particularly meaningful in preventing and treating heart attacks, says Dr. Manning, who represented SHM at a meeting of the Alliance for Cardiac Care Excellence (ACE), a CMS-based coalition that includes leaders from more than 30 healthcare organizations, and is working to ensure that all hospitalized cardiac patients regularly receive care consistent with nationally accepted standards.
11. Institute Multidisciplinary Rounds
Time constraints mean rounding with 10 people will necessarily be slower, says Dr. Alverson. In academic institutions where the hospitalist has the dual responsibility of teaching, this is especially time-consuming. Although there is an increasing emphasis that providers should participate at bedside rounds, and this is “clearly better from the patient’s perspective and, I would argue, better from the educational perspective,” says Dr. Alverson, it is “fairly bad from the getting-things-done-in-a-timely-fashion perspective. So it’s tough, and to a certain degree, in a practical world you have to pick and choose.”
When a nurse representative is there to respond to the question, “ ‘Why didn’t the kid get his formula? [and says] because he didn’t like the taste,’ that’s something that we might not pick up on,” says Dr. Alverson.
At NYU Medical Center, where Dr. Rauch works, formal rounds take place at least once a week (sometimes more), depending on volume, and they informally take place twice a day, every day.
“It works pretty well,” he says. “The nurses are a critically important part of teams; everybody recognizes that, and they are included in decisions.” Physicians put out the welcome mat for nurses even in casual circumstances. “Sometimes I am discussing things with the house staff [and] a nurse will pull up a chair and become part of the conversation. It’s a part of our culture.”
Although it is unusual to get a pharmacist to round with his team, says Dr. Alverson, a nearby pharmacy school sends students to join rounds, providing what might otherwise be a missing element of education.
12. Avoid Miscommunication
A number of the hospitalists interviewed were asked what they considered to be the top two or three communication points for hospitalists. Verbal orders, clarifying with read-backs, clear handwriting, and order sets were named frequently. In academic settings, says one hospitalist, instructors should be careful to make sure that residents, interns, and medical students understand what you’re saying and why you’re saying it. Good communication with the family was also cited as crucial.
“The most challenging issue is communicating at all,” says Dr. Rauch, who is also an associate professor of pediatrics at the NYU School of Medicine. Although he was the only one to phrase it this way, it is probably not a unique view. “In a large, old, academic medical institution, there are a lot of hierarchical issues that [impede] rapidly responding to [patients’] needs.” Unfortunately, it may mean communicating up one authorization pathway and down another. “And you can see the layers of time and the game of telephone as the concerns go around,” he says. “We’ve tried to break that down so the people who are on site can speak to someone who can make a decision.”
Along with that, he says, it is important from the outset to make it very clear who makes the decision. “For example, when the patient is a child getting neurosurgery because they have a seizure disorder and they also are developmentally delayed and they have medical issues, you now have at least three services involved with managing the child,” says Dr. Rauch. When three people are making decisions, he points out, no decision gets made. “You really have to decide when that child comes in who is going to call the shots for what issue. It’s usually the hospitalist who brings it up, and when it works, it works well.”
13. Empower Nurses and Other Clinicians
Nursing staff should have the power to halt unsafe practices. To Tahl Humes, MD, hospitalist at Exempla St. Joseph’s Hospital in Denver, halting unsafe practices depends, once again, on good lines of communication, and recognizing that patient care is a joint responsibility. For example, she says, “instead of just going to see the patient, writing the note, writing the order, and putting the chart away,” the hospitalists “talk with nurses daily and tell them what they’re planning to do,” so there is more opportunity to catch what might be unsafe practices.
14. Reduce Wound Infections
Although reducing wound infections is something in which their surgical colleagues take the lead, says Dr. Manning, “in our perioperative consultation care, we often work with surgery and anesthesiology in the pre-op evaluations of the patients. So in the surgical care improvement projects, we are often partners.”
Hospitalists are also frequently members on quality committees that help to brainstorm solutions to serious problems. One such project is the Surgical Care Improvement Program (SCIP), spearheaded by David Hunt, MD, with the Office of Clinical Standards and Quality, CMS. SCIP is an effort to transform the prevention of postoperative complications. Its goal is to reduce surgical complications by 25% in the United States by the year 2010 in four target areas: surgical site infections, and cardiac, respiratory, and venous thromboembolic complications. (See Figures 1 and 2, p. 33.)
This includes those patients who are already on beta-blockers. “From the hospitalist’s standpoint,” says Dr. Manning, “we have a real role in … [ensuring] that their beta blockade is maintained.”
Dr. Humes says that at her institution, a wound care nurse can have that responsibility. If a provider is concerned about any patient in this regard, he or she can order that the patient be seen by a wound care nurse and, depending on what’s needed, by a physical therapist.
Now we move on to address those issues that are medication-related:
15. Know Risky Meds
Pediatric hospitalists are involved with postoperative patients at Dr. Rauch’s institution. All patients’ orders are double-checked, he says, and computer order entry also helps providers calculate pediatric dosage norms or dosages calculated by weight.
The hospitalist has the opportunity to be involved in the pharmacy’s selection of drugs for the formulary, says Erin Stucky, MD, pediatric hospitalist at University of California, San Diego, and to help decide the drug choices within a certain class and limit the numbers of things that are used most frequently that are visually different in appearance. “And although that’s the pharmacist’s purview,” she says, “the hospitalist has a vested interest in being on the Pharmacy and Therapeutics Committee to review and restate to pharmacists what they’re using based on clinical need and to find a way for that drug to be safely stored in pharmacy if, indeed, there are a couple of drugs from one class that are truly useful.”
A drug’s generic name, brand name, dose strength, frequency of administration, place of use, indications, and contraindications are all important factors to determine the potential risks of drugs. But “you can’t say a list of risky medications at one institution is the same as it should be elsewhere,” says Dr. Stucky. Risky medications will depend on the setting in which the physician works. Hospitalists need to think logically about the drugs that are the most used or are new, including any new drug that has a different method by which it is administered or a different interaction capability with standard drugs.
“If there’s a new antibiotic that’s known to be processed through the liver and you have multiple patients with heart failure medications who have a medication basis that could be at conflict with that new drug, that’s a potentially risky medication,” she points out. “It may be easier in some ways for the pharmacist to be the rate-limiting factor for how they’re dispensed and for which patients they recheck [against] that incompatibility list.” But in large part, the avoidance of those risky-medication errors must be a commitment of the pharmacist and a bedside nurse.
16. Beware of Sound-Alike and Look-Alike Drugs
Dr. Stucky believes a majority of physicians don’t know the color or size of the pills they’re prescribing. “I would challenge all hospitalists to take every opportunity at the bedside,” she says, “to watch the process happening and know what those drugs and pills need to look like.”
Another opportunity is to educate family members “to remind them that [the patient is] going to be getting these medicines, these are the names of the medicines, and please ask the nurse about these medicines when you get them,” she says. If the hospitalist gives a new drug to the patient, the family can be another safeguard.
Dr. Stucky points out that you can tell the patient and family, “I’m going to tell the nurse that you’re going to be asking about this because … you are the best guide to help us make sure that these medicines are administered safely.” She also emphasizes that assigning this responsibility to the patient is important “because when people leave the hospital, we suddenly expect them to know how to take 18 pills.”
If, on a given unit, you have to handle cases with multiple diagnoses, says Dr. Stucky, it may be difficult to physically isolate the look-alike drugs. “At our institution we found that we actually had to pull the machines out,” she says, referring to the PIXUS units. “You can’t have them on the same wall even in different locations. You have to choose one or the other [similar looking pills].”
The sound-alike drugs are most ripe for errors with verbal orders. “Hospitalists can set a precedent in their institutions that any verbal orders should have the reason for that order given,” she explains. If you order clonazepam, after you finish giving the order verbally to the nurse, you should state, “This is for seizures.”
“When the nurse is writing it down, she may or may not be the one to know that that drug name is indeed in that drug class, but the pharmacist will know,” explains Dr. Stucky.
17. Reconcile Medications
“It is important for people to do verbal sign-out, certainly among attendings,” says Dr. Alverson, “to explain [in better depth] what’s going on with the patient and to maintain those avenues of communication in case something goes wrong. Hospitals get in trouble when physicians aren’t able to communicate or speak with each other readily.”
The biggest challenge for the pediatric hospitalists at NYU Hospital, says Dr. Rauch, is assessing the most up-to-date list of medications. “For instance,” he says, “we had a child yesterday as part of post-op care. I hadn’t met them pre-op. The father said, ‘I think my daughter’s on an experimental protocol with this additional medication.’ It wasn’t something we were used to so we called Mom: Can you bring in the protocol? She said, ‘Oh, she hasn’t been on that drug in a long time.’”
In fact, whether the patient is a child or adult, the majority of cases assigned to hospitalists are unplanned admissions and this is something with which all hospitalists struggle. But regarding transferring patients from unit to unit, says Dr. Stucky, “this is a whole different ballgame. That’s where we have a huge opportunity to make an impact.”
She suggests that matching medications to patients can be ameliorated by computer-based systems in which at each new place the hospitalist can fill in a printout regarding whether they’re continuing a drug order, changing it, or discontinuing it, and this system also works effectively on discharge. “In a perfect world,” says Dr. Stucky, … “the hospitalist would be the implementer of this kind of medication reconciliation in their institution.”
18. Avoid Unacceptable Drug Abbreviations
Some medications have abbreviations that can be misinterpreted. The classic ones, say several hospitalists, are magnesium and morphine. Others pertain to miswritten units of administration.
Read-backs on verbal medication orders was one of the elements most cited by our hospitalists as priority communication practices. Eliminating confusing abbreviations is one of JCAHO’s National Patient Safety Goals and “hospitals are aggressively rolling out ways to remind physicians not to use them,” says Dr. Alverson.
At Dr. Manning’s institution they use the Safest in America criteria, a collaboration of 10 Twin Cities and the hospital systems in Rochester, Minn., as well as the Institute for Clinical Systems Improvement. At Mayo, they call it “Write It Right.” An accentuated campaign to reduce ambiguities in medication communications, he says, has resulted in “profound improvement” in standardizing medication prescribing and following the read-back rules.
Dr. Stucky suggests that hospitalists take on mini-projects where they review the past six months of order-writing errors in their institutions, noticing any trends and, particularly, any unit-specific trends (such as the misunderstanding of the abbreviation cc). If you notice the errors are unit-specific, you can also analyze whether they are treatment-specific. In that way, “order sets can be pre-typed and all the providers have to do is fill in the numbers,” she says, adding that hospitalists can perform these analyses outside their own patient area.
19. Improper Drug Labeling, Packaging, and Storage
Drug names, labels, and packaging contribute significantly to medication errors. The risk for errors is determined by both the product and the environment in which it is used. Most hospitalists say they are continually developing new protocols and checking information multiple times. Sometimes, small changes go a long way. “Our patient safety officer has a favorite phrase: ‘How can I facilitate you to do something different next Tuesday?’ Within your own hospital, that means look at your system and pick something you know you can change,” says Dr. Stucky. “You can’t buy IT tomorrow; you can’t do physician order entries [because] your computer system doesn’t allow it—but what can you do?”
Conclusion
Dr. Angood encourages hospitalists to continue learning how to interact with other disciplines that are also evolving into hospital-based practices and to learn how to manage the specific details-of-change topics such as this list of 25—not just to gloss over them, but to understand them, and to encourage patient involvement and nurture the physician-patient relationship to help change the culture within health care.
“We can pick these kinds of topics and can dissect them all down, but each time, in the end, it is a matter of people and their behaviors as a culture inside a system,” he says. “The system can be changed a little bit, but still it is ultimately about the culture of people.” TH
Andrea Sattinger writes regularly for The Hospitalist.
References
- Runy LA. 25 things you can do to save lives now. Hosp Health Netw. 2005 Apr;79(4):27-28.
- Meengs MR, Giles BK, Chisholm CD, et al. Hand washing frequency in an emergency department. Ann Emerg Med. 1994 Jun;23(6):1307-1312.
- McGuckina M, Watermana R, Storrb J, et al. Evaluation of a patient-empowering hand hygiene programme in the UK. J Hosp Infect. 2001 Jul;48(3):222-227.
- Whitby M, McLaws ML, Ross MW. Why healthcare workers don't wash their hands: a behavioral explanation. Infect Control Hosp Epidemiol. 2006 May;27(5):484-492.
- Lipsett PA, Swoboda SM. Handwashing compliance depends on professional status. Surg Infect. 2001 Fall;2(3):241-245.
In April 2005, the American Hospital Association’s magazine, Hospital and Health Networks (H&HN), published the article “25 Things You Can Do to Save Lives Now.”1 In it, experts from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), the Institute for Healthcare Improvement (IHI), the National Quality Forum (NQF), and the Centers for Medicare and Medicaid Services (CMS), commented on an action plan to advance hospitals’ patient safety activities.
Now The Hospitalist has researched hospitalists’ views on these same 25 items. Those views are presented below.
A number of these items “are already highly ensconced in the JCAHO and CMS criteria,” says Dennis Manning, MD, FACP, FACC, director of quality in the Department of Medicine and an assistant professor at the Mayo Clinic College of Medicine, Rochester, Minn. “In terms of power of the things on the list for potentially saving lives, what we sometimes look at are the things that have the potential for the most prevention.”
Brian Alverson, MD, pediatric hospitalist at Hasbro Children’s Hospital in Providence, R.I., adds his thoughts on the 25 items: “We have to hold in our minds a healthy nervousness about patients being hospitalized, in that there is an inherent danger to that phenomenon. No matter how hard we strive for perfection in patient care, to err is human.”
Shortening hospital length of stay to within a safe range, he believes, is one of the best ways to reduce those daily dangers.
Some of the 25 items pose more challenges for hospitalists than others, and the contrary is true as well. Some were judged to be of lesser concern due to guidelines or imperatives imposed on hospitals by regulatory organizations. Other items fall outside hospitalists’ accountabilities, such as incorrect labeling on X-rays or CT scans, overly long working hours, medical mishaps (such as wrong-site, wrong-person, and wrong-implant surgeries), and ventilator-associated pneumonia. A few items were those that hospitalists found challenging, but for which they had few suggestions for solutions. In some, there were obstacles standing in the way of their making headway toward conquering the menace. These included:
1. Improper Patient Identification
“Until we set up a system that improves that, such as an automated system,” says one hospitalist, “I’ll be honest with you, I think we can remind ourselves ’till we’re blue in the face and we’re still going to make mistakes.”
2. Flu Shots
“Flu shots are probably more important in the pediatrics group than in any [other] except the geriatric group,” says Dr. Alverson, who strongly believes that pediatricians should be able to administer flu shots in the inpatient setting, “because we can catch these kids with chronic lung disease—many of [whom] are admitted multiple times.”
3. Fall Prevention
This item is one of the National Patient Safety goals, and one that every institution is trying to address. In pediatrics, says Dr. Alverson, the greater problem “is getting people to raise the rails of cribs. Kids often fall out of cribs because people forget to raise the rail afterwards, or don’t raise it high enough for a particularly athletic or acrobatic toddler.”
The other items on the list of 25 are below, including a section for medication-related items and the sidebar on a venous thromboembolism (VTE) prevention program.
4. Wash Hands
Provider hand-washing has been well studied, says one hospitalist, and “the data are so depressing that no one wants to deal with it.” Another says, “We just nag the hell out of people.”
One of the hospitalists interviewed for this story read the H&HN article and responds, “We do all these things.” But a lack of self-perception regarding this issue—as well as others—is also well-documented: Physicians who are queried will say they always wash their hands when, in fact, they do so less than 50% of the time.2-5
Despite the value of hand sanitizers—whether they are available at unit entrances, along the floors, at individual rooms, or carried in tiny dispensers that can be attached to a stethoscope—some pathogens, such as the now-epidemic Clostridium difficile, are not vulnerable to the antisepsis in those mechanisms.
“C. dif is a set of spores that are less effectively cleaned by the topical hand sanitizers,” says Dr. Alverson, who is also an assistant professor of pediatrics at Brown University in Providence, R.I. “In those cases, soap and water is what you need.”
Peter Angood, MD, FRCS(C), FACS, FCCM, vice president and chief patient safety officer of JCAHO, Oakbrook, Ill., says provider hand-washing is a huge patient safety issue and, in general, a multi-factorial problem that is more complicated than it would seem on the surface.
“We can rationalize and cut [providers] all kinds of slack, but at the bottom line is human behavior and their willingness to comply or not comply,” he says. “It’s like everything else: Why do some people speed when they know the speed limit is 55?”
Addressing the solution must be multi-factorial as well, but all hospitalists can serve as role models for their colleagues and students, including remaining open to reminders from patients and families.
5. Remain on Kidney Alert
Contrast media in radiologic procedures can cause allergic reactions that lead to kidney failure. This is a particularly vexing problem for elderly patients at the end stages of renal dysfunction and patients who have vascular disease, says Dr. Manning. Although the effects are not generally fatal, the medium can be organ-damaging. “This is a hazard that’s known, and it has some mitigating strategies,” he says, “but often it can’t be entirely eliminated.”
Measures that reduce the chance of injury, say Dr. Manning, include ensuring that the contrast medium is required; confirming that the procedure is correct for the patient, with the right diagnosis, with a regulated creatinine, and well coordinated with the radiology department; “and then getting true informed consent.” But at a minimum, he emphasizes, is the importance of hydration. “There is some evidence that hydration with particular types of intravenous fluids can help reduce the incidence of the kidney revolting.” And, he says, “there are a number of things that we have to do to make sure this is standardized.”
6. Use Rapid Response Teams
Use of “[r]apid response teams [RRTs] is one of the most powerful items on the list,” says Dr. Manning, who serves on SHM’s committee on Hospital Quality and Patient Safety as well as the committee helping to design the Ideal Discharge for the Elderly Patient checklist. “Whereas every hospital has a plan for response,” he says, RRTs are “really a backup plan.”
In 2003, Dr. Manning served as faculty for an IHI program in which a collaborative aimed at reducing overall hospital mortality. The formation and application of RRTs at six hospitals in the United States and two in the United Kingdom was the most promising of the several interventions, with impact on a variety of patients whose conditions were deteriorating in non-ICU care areas.
The advantage of RRTs with children, says Daniel Rauch, MD, FAAP, director of the Pediatric Hospitalist Program at NYU Medical Center, New York City, is that it is often difficult for providers to know what may be wrong with a child who is exhibiting symptoms. “Is the kid grunting because they’re constipated, because that’s the developmental stage they’re in, they’re in pain, or are they really cramping on you?” he asks.
7. Check for Pressure Ulcers
Checking for pressure ulcers is the task of nurses and physicians, say hospitalists, and they agree that it has to be done at admission. “The patient’s entire skin needs to be checked,” says Dr. Manning, “and often it takes both the nurse and doctor to roll the patient and get a good look at their bottom or their back … especially if the patient might have come from a nursing home and has a chronic serious illness.”
Also important, he says, is to fully assess the type of decubitus skin situation or any skin problem and then to monitor the patient to prevent advancement. “Multidisciplinary rounds can help,” he says, “and collaborative communication is key.”
8. Give the Patient and Family a Voice
“We fully embrace the involvement of the patient in the process of their care,” says Dr. Angood, who is also the co-director of the Joint Commission International Center for Patient Safety, for which patient and family involvement is a priority.
Giving patients and family members a voice is a fine idea, say our hospitalists, especially with children: No one knows a patient like their parents. As the H&HN article points out, anecdotal evidence is largely responsible for the belief that patient and family involvement helps reduce the likelihood for errors, and patient and family participation on safety committees can be a boon to advancing safety as well as satisfaction. But, says Dr. Alverson, “one has to keep in mind that parents have a perspective and not the only perspective on patient safety. I think a broad group of people has to sit down to address these issues.”
In the post-surgical setting, says Dr. Rauch, hospitalists make an invaluable contribution. “If surgeons don’t even come by to listen to the parents or see the child, it’s helpful to have that co-management of someone who’s used to listening to parents, who credits the parents for knowing their kids, and who will do the appropriate thing.” Dr. Angood, who is a past president of the Society of Critical Care Medicine, believes “that that patient-physician relationship is still going to be the driver for the majority of healthcare for some time yet.”
9. Reduce Catheter-Related Bloodstream Infections
“If it’s not required, we want every foreign body out,” says Dr. Manning. “We have to ask ourselves every day whether they are still required.”
The geriatric service at the Mayo Clinic (Rochester, Minn.) developed a daily mnemonic of A-B-C-D-E where B stands for binders. This, he says, “is a way for us to remind ourselves that any therapeutic foreign objects that are tethering the patient—and many of them are catheters—are of concern. We need to push the question [Is this still required?] to ourselves and then act on it.”
Dr. Alverson says, “There are certain infections [for which] we’re starting to move away from PICC [peripherally inserted central catheters] line management, and one way to mitigate that is to be on top of when you can actually discontinue the catheter.” For example, “in pediatrics, there are emerging data that with osteomyelitis you can have a shortened course of IV antibiotics and then switch to oral antibiotics. … That can reduce by half your PICC line duration. Being savvy about this is important.”
10. Reduce Heart Attack Death Rates
“There are about eight interventions for heart attacks that have increased survival,” says Dr. Manning. “So every hospital is working with these. We are using the all-or-none criteria, meaning that there are assurances [in place] that every patient will get all of them.”
Re-engineering systems has been particularly meaningful in preventing and treating heart attacks, says Dr. Manning, who represented SHM at a meeting of the Alliance for Cardiac Care Excellence (ACE), a CMS-based coalition that includes leaders from more than 30 healthcare organizations, and is working to ensure that all hospitalized cardiac patients regularly receive care consistent with nationally accepted standards.
11. Institute Multidisciplinary Rounds
Time constraints mean rounding with 10 people will necessarily be slower, says Dr. Alverson. In academic institutions where the hospitalist has the dual responsibility of teaching, this is especially time-consuming. Although there is an increasing emphasis that providers should participate at bedside rounds, and this is “clearly better from the patient’s perspective and, I would argue, better from the educational perspective,” says Dr. Alverson, it is “fairly bad from the getting-things-done-in-a-timely-fashion perspective. So it’s tough, and to a certain degree, in a practical world you have to pick and choose.”
When a nurse representative is there to respond to the question, “ ‘Why didn’t the kid get his formula? [and says] because he didn’t like the taste,’ that’s something that we might not pick up on,” says Dr. Alverson.
At NYU Medical Center, where Dr. Rauch works, formal rounds take place at least once a week (sometimes more), depending on volume, and they informally take place twice a day, every day.
“It works pretty well,” he says. “The nurses are a critically important part of teams; everybody recognizes that, and they are included in decisions.” Physicians put out the welcome mat for nurses even in casual circumstances. “Sometimes I am discussing things with the house staff [and] a nurse will pull up a chair and become part of the conversation. It’s a part of our culture.”
Although it is unusual to get a pharmacist to round with his team, says Dr. Alverson, a nearby pharmacy school sends students to join rounds, providing what might otherwise be a missing element of education.
12. Avoid Miscommunication
A number of the hospitalists interviewed were asked what they considered to be the top two or three communication points for hospitalists. Verbal orders, clarifying with read-backs, clear handwriting, and order sets were named frequently. In academic settings, says one hospitalist, instructors should be careful to make sure that residents, interns, and medical students understand what you’re saying and why you’re saying it. Good communication with the family was also cited as crucial.
“The most challenging issue is communicating at all,” says Dr. Rauch, who is also an associate professor of pediatrics at the NYU School of Medicine. Although he was the only one to phrase it this way, it is probably not a unique view. “In a large, old, academic medical institution, there are a lot of hierarchical issues that [impede] rapidly responding to [patients’] needs.” Unfortunately, it may mean communicating up one authorization pathway and down another. “And you can see the layers of time and the game of telephone as the concerns go around,” he says. “We’ve tried to break that down so the people who are on site can speak to someone who can make a decision.”
Along with that, he says, it is important from the outset to make it very clear who makes the decision. “For example, when the patient is a child getting neurosurgery because they have a seizure disorder and they also are developmentally delayed and they have medical issues, you now have at least three services involved with managing the child,” says Dr. Rauch. When three people are making decisions, he points out, no decision gets made. “You really have to decide when that child comes in who is going to call the shots for what issue. It’s usually the hospitalist who brings it up, and when it works, it works well.”
13. Empower Nurses and Other Clinicians
Nursing staff should have the power to halt unsafe practices. To Tahl Humes, MD, hospitalist at Exempla St. Joseph’s Hospital in Denver, halting unsafe practices depends, once again, on good lines of communication, and recognizing that patient care is a joint responsibility. For example, she says, “instead of just going to see the patient, writing the note, writing the order, and putting the chart away,” the hospitalists “talk with nurses daily and tell them what they’re planning to do,” so there is more opportunity to catch what might be unsafe practices.
14. Reduce Wound Infections
Although reducing wound infections is something in which their surgical colleagues take the lead, says Dr. Manning, “in our perioperative consultation care, we often work with surgery and anesthesiology in the pre-op evaluations of the patients. So in the surgical care improvement projects, we are often partners.”
Hospitalists are also frequently members on quality committees that help to brainstorm solutions to serious problems. One such project is the Surgical Care Improvement Program (SCIP), spearheaded by David Hunt, MD, with the Office of Clinical Standards and Quality, CMS. SCIP is an effort to transform the prevention of postoperative complications. Its goal is to reduce surgical complications by 25% in the United States by the year 2010 in four target areas: surgical site infections, and cardiac, respiratory, and venous thromboembolic complications. (See Figures 1 and 2, p. 33.)
This includes those patients who are already on beta-blockers. “From the hospitalist’s standpoint,” says Dr. Manning, “we have a real role in … [ensuring] that their beta blockade is maintained.”
Dr. Humes says that at her institution, a wound care nurse can have that responsibility. If a provider is concerned about any patient in this regard, he or she can order that the patient be seen by a wound care nurse and, depending on what’s needed, by a physical therapist.
Now we move on to address those issues that are medication-related:
15. Know Risky Meds
Pediatric hospitalists are involved with postoperative patients at Dr. Rauch’s institution. All patients’ orders are double-checked, he says, and computer order entry also helps providers calculate pediatric dosage norms or dosages calculated by weight.
The hospitalist has the opportunity to be involved in the pharmacy’s selection of drugs for the formulary, says Erin Stucky, MD, pediatric hospitalist at University of California, San Diego, and to help decide the drug choices within a certain class and limit the numbers of things that are used most frequently that are visually different in appearance. “And although that’s the pharmacist’s purview,” she says, “the hospitalist has a vested interest in being on the Pharmacy and Therapeutics Committee to review and restate to pharmacists what they’re using based on clinical need and to find a way for that drug to be safely stored in pharmacy if, indeed, there are a couple of drugs from one class that are truly useful.”
A drug’s generic name, brand name, dose strength, frequency of administration, place of use, indications, and contraindications are all important factors to determine the potential risks of drugs. But “you can’t say a list of risky medications at one institution is the same as it should be elsewhere,” says Dr. Stucky. Risky medications will depend on the setting in which the physician works. Hospitalists need to think logically about the drugs that are the most used or are new, including any new drug that has a different method by which it is administered or a different interaction capability with standard drugs.
“If there’s a new antibiotic that’s known to be processed through the liver and you have multiple patients with heart failure medications who have a medication basis that could be at conflict with that new drug, that’s a potentially risky medication,” she points out. “It may be easier in some ways for the pharmacist to be the rate-limiting factor for how they’re dispensed and for which patients they recheck [against] that incompatibility list.” But in large part, the avoidance of those risky-medication errors must be a commitment of the pharmacist and a bedside nurse.
16. Beware of Sound-Alike and Look-Alike Drugs
Dr. Stucky believes a majority of physicians don’t know the color or size of the pills they’re prescribing. “I would challenge all hospitalists to take every opportunity at the bedside,” she says, “to watch the process happening and know what those drugs and pills need to look like.”
Another opportunity is to educate family members “to remind them that [the patient is] going to be getting these medicines, these are the names of the medicines, and please ask the nurse about these medicines when you get them,” she says. If the hospitalist gives a new drug to the patient, the family can be another safeguard.
Dr. Stucky points out that you can tell the patient and family, “I’m going to tell the nurse that you’re going to be asking about this because … you are the best guide to help us make sure that these medicines are administered safely.” She also emphasizes that assigning this responsibility to the patient is important “because when people leave the hospital, we suddenly expect them to know how to take 18 pills.”
If, on a given unit, you have to handle cases with multiple diagnoses, says Dr. Stucky, it may be difficult to physically isolate the look-alike drugs. “At our institution we found that we actually had to pull the machines out,” she says, referring to the PIXUS units. “You can’t have them on the same wall even in different locations. You have to choose one or the other [similar looking pills].”
The sound-alike drugs are most ripe for errors with verbal orders. “Hospitalists can set a precedent in their institutions that any verbal orders should have the reason for that order given,” she explains. If you order clonazepam, after you finish giving the order verbally to the nurse, you should state, “This is for seizures.”
“When the nurse is writing it down, she may or may not be the one to know that that drug name is indeed in that drug class, but the pharmacist will know,” explains Dr. Stucky.
17. Reconcile Medications
“It is important for people to do verbal sign-out, certainly among attendings,” says Dr. Alverson, “to explain [in better depth] what’s going on with the patient and to maintain those avenues of communication in case something goes wrong. Hospitals get in trouble when physicians aren’t able to communicate or speak with each other readily.”
The biggest challenge for the pediatric hospitalists at NYU Hospital, says Dr. Rauch, is assessing the most up-to-date list of medications. “For instance,” he says, “we had a child yesterday as part of post-op care. I hadn’t met them pre-op. The father said, ‘I think my daughter’s on an experimental protocol with this additional medication.’ It wasn’t something we were used to so we called Mom: Can you bring in the protocol? She said, ‘Oh, she hasn’t been on that drug in a long time.’”
In fact, whether the patient is a child or adult, the majority of cases assigned to hospitalists are unplanned admissions and this is something with which all hospitalists struggle. But regarding transferring patients from unit to unit, says Dr. Stucky, “this is a whole different ballgame. That’s where we have a huge opportunity to make an impact.”
She suggests that matching medications to patients can be ameliorated by computer-based systems in which at each new place the hospitalist can fill in a printout regarding whether they’re continuing a drug order, changing it, or discontinuing it, and this system also works effectively on discharge. “In a perfect world,” says Dr. Stucky, … “the hospitalist would be the implementer of this kind of medication reconciliation in their institution.”
18. Avoid Unacceptable Drug Abbreviations
Some medications have abbreviations that can be misinterpreted. The classic ones, say several hospitalists, are magnesium and morphine. Others pertain to miswritten units of administration.
Read-backs on verbal medication orders was one of the elements most cited by our hospitalists as priority communication practices. Eliminating confusing abbreviations is one of JCAHO’s National Patient Safety Goals and “hospitals are aggressively rolling out ways to remind physicians not to use them,” says Dr. Alverson.
At Dr. Manning’s institution they use the Safest in America criteria, a collaboration of 10 Twin Cities and the hospital systems in Rochester, Minn., as well as the Institute for Clinical Systems Improvement. At Mayo, they call it “Write It Right.” An accentuated campaign to reduce ambiguities in medication communications, he says, has resulted in “profound improvement” in standardizing medication prescribing and following the read-back rules.
Dr. Stucky suggests that hospitalists take on mini-projects where they review the past six months of order-writing errors in their institutions, noticing any trends and, particularly, any unit-specific trends (such as the misunderstanding of the abbreviation cc). If you notice the errors are unit-specific, you can also analyze whether they are treatment-specific. In that way, “order sets can be pre-typed and all the providers have to do is fill in the numbers,” she says, adding that hospitalists can perform these analyses outside their own patient area.
19. Improper Drug Labeling, Packaging, and Storage
Drug names, labels, and packaging contribute significantly to medication errors. The risk for errors is determined by both the product and the environment in which it is used. Most hospitalists say they are continually developing new protocols and checking information multiple times. Sometimes, small changes go a long way. “Our patient safety officer has a favorite phrase: ‘How can I facilitate you to do something different next Tuesday?’ Within your own hospital, that means look at your system and pick something you know you can change,” says Dr. Stucky. “You can’t buy IT tomorrow; you can’t do physician order entries [because] your computer system doesn’t allow it—but what can you do?”
Conclusion
Dr. Angood encourages hospitalists to continue learning how to interact with other disciplines that are also evolving into hospital-based practices and to learn how to manage the specific details-of-change topics such as this list of 25—not just to gloss over them, but to understand them, and to encourage patient involvement and nurture the physician-patient relationship to help change the culture within health care.
“We can pick these kinds of topics and can dissect them all down, but each time, in the end, it is a matter of people and their behaviors as a culture inside a system,” he says. “The system can be changed a little bit, but still it is ultimately about the culture of people.” TH
Andrea Sattinger writes regularly for The Hospitalist.
References
- Runy LA. 25 things you can do to save lives now. Hosp Health Netw. 2005 Apr;79(4):27-28.
- Meengs MR, Giles BK, Chisholm CD, et al. Hand washing frequency in an emergency department. Ann Emerg Med. 1994 Jun;23(6):1307-1312.
- McGuckina M, Watermana R, Storrb J, et al. Evaluation of a patient-empowering hand hygiene programme in the UK. J Hosp Infect. 2001 Jul;48(3):222-227.
- Whitby M, McLaws ML, Ross MW. Why healthcare workers don't wash their hands: a behavioral explanation. Infect Control Hosp Epidemiol. 2006 May;27(5):484-492.
- Lipsett PA, Swoboda SM. Handwashing compliance depends on professional status. Surg Infect. 2001 Fall;2(3):241-245.
What Now?

Patient discharge. It’s an everyday occurrence and, therefore, easily taken for granted. The hospitalist, who must help the patient transition back to the primary care physician, knows that this is a mistake. This transition takes an intense amount of communication among hospitalists, primary care and other physicians, nurses, case managers, social and therapy services, the patient, and the family.
Although smooth, effective patient handoffs are critical in maintaining patient safety and ensuring positive health outcomes, they are too often executed haphazardly, and the amount and precision of information as well as the means by which it is transmitted varies considerably. The journey is rife with communication landmines—communication can lapse or be absent, and when information falls through the cracks, continuity of care may be disrupted.
Top Considerations
Considering post-discharge communication in general, “probably the most important thing is to make sure that the hospitalist conveys as much of an impression of how the patient is doing [as possible],” says Richard Frankel, PhD, professor of medicine and geriatrics at Indiana University School of Medicine, Indianapolis, “not only in terms of their medical care or their disease process, but [also] what the patient’s hospital stay has been like, what the perception of their hospital experience has been like. And to be open to additional questions from the primary care physician about issues that might arise post discharge and ambiguities that might exist in the discharge summary.”
After determining a standardized protocol for post-discharge handoffs, “then I think that the most important thing is just practicing using these various protocols,” says Dr. Frankel, who also serves as senior research scientist at the Regenstrief Institute (Indianapolis) and is a research sociologist in the Health Services Research Unit at the Roudebush Veterans Affairs Medical Center, Indianapolis. “When the astronauts train, they train for every possible contingency so that when [a problem] arises it seems like the most common thing in the world, when in fact, what they practice are very low-frequency events, very low-probability problems arising.”
The nuts and bolts of ideal practices include essentials such as dictating notes and, preferably, transcribing and transmitting them by the close of the business day on which the patient is discharged.1 If short notes are sent to the primary care physician at the time of discharge, a longer summary should arrive within a few days. Because primary care physicians disagree as to what should be included in that summary, communication among physicians becomes a key issue in the transition.
“There’s a paucity of data on the subject of how well physicians communicate with each other,” says Darrell Solet, MD, cardiology fellow at the University of Texas, Southwestern Medical Center in Dallas. “A number of organizations have jumped on the bandwagon of improving this process, especially [the] Joint Commission [on] Accreditation of Healthcare Organizations,” he says.
Biggest Challenges
One of the major things the University of Texas Southwestern has emphasized in its residency program’s communication skills curriculum is not only how physicians communicate with their patients but also how well they communicate with each other. “This includes hearing a presentation on the most effective and efficient ways to perform their handoffs and also addressing the specific barriers to communication that they might face, says Dr. Solet.
These barriers to effective handoffs were identified in a study that Dr. Solet and his colleagues, including Dr. Frankel, conducted in 2005 in four hospitals in Indiana.2 At that time, Dr. Solet was the chief resident of ambulatory medicine, Department of Medicine, Indiana University School of Medicine, Indianapolis, and of medical service, Roudebush Veterans Affairs Medical Center, Indianapolis. In general, the study revealed that barriers to communication existed in four areas: physical settings, social settings, language, and communication styles.
Dr. Solet says that inconsistent information poses the biggest threat in the post-discharge communications he has seen. Another high-risk area involves documentation in which the physician writes only a line or two, such as, “This is a 50-ish-year-old man with COPD. Those one-liners are very dangerous,” he says.
In addition to the risks inherent in documentation, the biggest danger areas include pending test results, recommended follow-up studies, misunderstood medication instructions, never-purchased medications, and missed follow-up visits with the primary care physician.
Nelson and Whitcomb1 suggest that a post-discharge summary containing all essential information could overwhelm the primary care physician. They recommend standard forms with separate headings for diagnoses, medications, and hospital course, along with categories such as tests pending and evaluations needed. “Ideally, each hospitalist in a group should use the same format for these reports, so that a reader can quickly become accustomed to extracting information from them,” they write.
Tailor the Summary
Edward J. Merrens, MD, section chief of hospital medicine at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., was one of the authors of a study investigating ways to enhance the timeliness, accuracy, and breadth of clinical information gathered at discharge.3 The improvement project was conducted in a 330-bed tertiary care teaching hospital that averages 12,800 discharges a year.
“In general,” says Dr. Merrens, “we’re sending people out sicker and sicker, and often [the subsequent providers] don’t need a summary of all the interventions and studies and meds and antibiotics [done during the hospitalization], but what to do with the patient next. … Hospitalizations have become less therapeutic confinements where everything gets done, but [rather] where complex interventions occur and patients go out on therapy and are still often sick.”
The discharge summary should be designed in such a way that the primary care physician can simply “pick it up and go” from there, says Dr. Merrens. “We’ve tried to think, who really reads this thing? It could be [the] primary care physician, it may be a patient, it could be a doctor taking care of a patient in a rehabilitation facility, or it may be a visiting nurse service. We try to tailor the summary to those audiences, not just summarize what we’ve done.” His team has included a section on the summary where one can write, for example, “The patient might need more diuresis for their heart failure. They’re probably going to need a follow-up with this,” and Dr. Merrens says this structure has worked well.
“As we move from the Marcus Welby model of ‘you’re always on, you’re always covering, you’re the only doc’ to shift-based care,” he says, “the core of the [provider] group itself needs to communicate well, and it needs to agree on principles.” And this, he says, is a key component of job satisfaction for hospitalists.

—Edward J. Merrens, MD
Back to Long-Term Care
The goals of transitional care include ensuring continuity, providing for safe discharge, and preventing rehospitalization.4 Hospitalists have to recognize which patients are at risk for poor outcomes and devise ways to help prevent these problems. At particularly high risk are patients with the following characteristics:
- Age 80 and older;
- A history of depression;
- Multiple chronic diseases;
- Moderate-to-severe functional impairment;
- Noncompliance with therapy;
- Inadequate social supports;
- Multiple hospitalizations in the previous six months;
- Hospitalization in the last 30 days; and
- Fair or poor self-rating of health.4
Patients who return to long-term care, therefore, need careful transfer of information.
Nursing homes tell Dr. Merrens’ team that there is not enough practical information on the discharge summary about the patient’s current functional abilities. In response, the hospitalists included a section in their discharge documentation that summarizes the patient’s status, answering questions regarding the patient’s mental capacity, her ability to feed herself, her last bowel movement, her contact at the hospital in the event of a post-discharge emergency, and her designated power of attorney (if such a form was signed at the hospital).
At and After Discharge: Communicate with Patients and Families
Communication at the time of discharge involves, again, telling patients what’s next: Clarifying the use and potential side effects of medications, explaining when the patient can resume normal activities, providing the plan for and benefits of any occupational or physical therapy, and emphasizing the importance of follow-up. But it is also a time when patients should be told that they will need to “serve as expert witnesses to their care.”5
Tom Delbanco, MD, chief of the Division of General Medicine and Primary Care at Beth Israel Deaconess Medical Center, Boston, who has written extensively about communications and hospital medicine, reminds hospitalists that when it comes to getting feedback for quality improvement, it is far more helpful to gather patients’ self-reports than their ratings. Practitioners of hospital medicine, he adds, have an imperative not only to inquire into patient experiences, but also to catalog them and share findings with colleagues.
The Picker Institute (Boston), a nonprofit organization dedicated to the advancement of patient-centered healthcare, found that only one in 64 hospitals participating in its first national survey of hospitalized patients could be judged as particularly adept at preparing patients for discharge.5 What the staff were doing differently at that one hospital was very simple: They asked the patients and families to write down any questions they had before they went home; discharge occurred only after all those questions were answered.
Although post-discharge communication involves talking to and instructing patients, it also involves listening and watching for how well patients receive these communications. In the discharge conversation, patients may be groggy from too much or too little sleep, heavily medicated or coming off of major narcotics or general anesthesia, experiencing pain, suffering from anxiety or delirium, or just mentally disoriented from the stress of the hospital experience.5-8
Calkins and colleagues surveyed 99 patients to determine any difference in perceptions between patients and their attending physicians regarding the patients’ understanding of the treatment plan after hospitalization.6 Physicians reported spending more time discussing post-discharge care than did patients, and the doctors believed that 89% of patients understood the potential side effects of their medications when only 57% of the patients reported that they had.
Discharge summaries given directly to patients can help with comprehension and compliance.1 Telephone follow-up is also a valuable tool and, along with a chance to provide answers and encouragement, gives the patient a feeling of being cared for.1 Several studies have shown benefit in phone follow-up, providing a chance for hospitalists to review new test results, clarify misunderstandings, and encourage compliance, as well as to learn any unexpected outcomes, treatment failures, or side effects.9
Written instructions are imperative. One person should be assigned this duty and, on a standardized form, should provide details, not just when and how to call the primary care physician. The bare bones of a summary are not enough—especially if there was not a competent family member present at the final discharge conversation. Further, in many cases, questions arise after the patient is home, when a family member, a nurse, or the patient herself may have questions, particularly about medications.
Test Results and Follow-Up Studies
Among the factors contributing to failures at discharge is disrupted continuity of responsibility for pending test results and radiologic studies. This discontinuity may be especially operational in teaching hospitals, where physicians-in-training may frequently change services or shifts, and yet they remain responsible for all or some of the discharge communication.10 To prevent this disruption and avoid confusion, the institution or team should clarify the person responsible for follow-up on tests or studies. And they must communicate this information to the primary care physician.
Roy and colleagues looked at the prevalence, characteristics, and physician awareness of potentially actionable test results returning after hospital discharge at two major tertiary care centers.10 Of the 2,644 patients discharged from the hospitalist services, 1,095 (41%) had a total of 2,033 test results pending on the day of discharge, and 877 of these results (43%) were abnormal. Of the final 671 results included, 191 (9.4%) from 177 patients were potentially clinically actionable. Surveyed physicians were unaware of almost two-thirds of these potentially actionable results; more than a third of these results would change the patient’s diagnostic or treatment plan, and 12.6% of cases required urgent action. Other data show the unreliability of providing test results at follow-up visits; discharge summaries were available at only 12% to 33% of visits studied in one series.10
When inpatient physicians were asked how they would like electronic results-management systems that could highlight important results, filter out normal results, and help hospitalists track results returning after discharge, they were eager to adopt such systems. A future article in The Hospitalist will cover the emergence of electronic systems to better manage discharge communications.
Follow-up Contact with Patients
Van Walraven and colleagues looked at whether early post-discharge outcomes changed when patients were seen after discharge by physicians who had treated them in the hospital.11 When 938,833 adults from Ontario, Canada, were followed over five years after discharge from a medical or surgical hospitalization, 7.7% died or were readmitted. The adjusted relative risk of death or readmission decreased by 5% and 3% with each additional visit to a hospital physician—as opposed to a community physician or specialist, respectively. The effect of hospital physician visits was seen to have a dose-response effect, with the adjusted risk of 30-day death or nonelective readmission reduced to 7.3%, 7.0%, and 6.7% if patients had one, two, or three visits, respectively.
Hospital physician follow-up, say the authors of the Van Walraven, is a potentially modifiable factor that could decrease the risk of poor outcomes post discharge. Although not all providers embrace the concept, it does address the essential need of continuity of care through the potentially complicated transition from hospital to community. At the very least, the authors write, any physicians who sees the patient should have access to as much information as possible regarding the hospitalization and should be able to contact patients by phone post discharge.11-13
In a survey distributed by Steve Pantilat, MD, and colleagues, primary care physicians reported overwhelmingly that they preferred communicating with hospitalists by telephone at discharge (78%).14 While this may be unrealistic for all handoffs, says Dr. Merrens, hospitalists should make the effort for more complicated or serious cases.
Adverse Drug Events and Other Medication Issues
Although most adverse drug events (ADEs) are caused by the pharmacologic activity of the drug itself and can be predicted and mitigated, some one-third to one-half of ADEs are caused by human error or flawed systems.15
Coleman and colleagues looked at 375 patients, 65 and older, to analyze the medication problems they encountered.8 A significant percentage (14.1%) of older patients experienced one or more medication discrepancies after discharge; 50.8% were categorized as patient-associated; and 49.2% were seen as system-related. A total of 14.3% of the patients who experienced these discrepancies were rehospitalized at 30 days, compared with 6.1% of the patients who did not have any problems.
Of the contributing factors cited by patients, one-third were due to unintentional nonadherence, followed by financial barriers, intentional nonadherence, and neglect in filling a prescription.8 At the system level, incomplete, inaccurate, or illegible discharge instructions (as a result of either poor handwriting or use of Latin abbreviations) were the most commonly identified contributing factors, followed by conflicting information from different informational sources and duplicate prescribing.
Partnering with Case Management
Variability in physicians’ rounding patterns and schedules and in nurses’ and case managers’ shifts and assignments can make it difficult to bring involved parties together. Yet hospitalists look to case managers to follow up on acute services, interact with the patient’s plan of care, communicate with families, arrange follow-up with the primary care physician, and track the patient’s condition for progress.
Cogent Healthcare (Irvine, Calif.), a leading hospitalist company, has devised a means to optimize communication between case managers and hospitalists. The effects of this partnership have been shown to shorten hospital stay and reduce costs with no adverse effect on patient outcomes or patient satisfaction.16, 17 Along with responsibilities during the hospitalization, Cogent’s clinical care coordinators (CCC) make sure the primary care physician gets correct and appropriate information as soon as possible. The CCC phones the patient at home to ensure that the discharge plan is in place, that the patient is compliant with the post–acute treatment plan, and that she or he has a plan to meet with the primary care physician.
Case managers face a good deal of daily frustration, working on the same problems for patient after patient and trying to be available to help hospitalists make clinical practice decisions at the point of care. One way to improve overall post-discharge communication would be to lobby hospitals to provide the resources to support the case managers’ workload and their accessibility to their hospitalist colleagues.16, 18
Conclusion
Effective post-discharge communication includes standardizing an institution’s protocol for handoffs, increasing training and practice in post-discharge communication, and keeping the lines of communication open among hospitalists, primary care physicians, patients, and families. Collecting reported feedback from patients and families shortly after patients have returned home can be used toward quality improvement. Although the effectiveness of post-discharge communication may vary from hospital to hospital and even from hospitalist to hospitalist as well as across each hospitalist-primary care physician pairing, “I think that the interest that’s been stimulated in this whole area is exciting,” says Dr. Frankel. “This is an area where everybody wins. Rather than one person or one hospital winning and another one losing, there’s a new collaborative spirit that is very heartening to see.” TH
Andrea Sattinger writes regularly for The Hospitalist.
References
- Nelson JR, Whitcomb WF. Organizing a hospitalist program: an overview of fundamental concepts. Med Clin North Am. 2002 Jul 8;86(4):887-909.
- Solet DJ, Norvell JM, Rutan GH, et al. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005 Dec;80(12):1094-1099.
- Lurie JD, Merrens EJ, Lee J, et al. An approach to hospital quality improvement. Med Clin North Am. 2002 Jul;86(4):825-845.
- Callahan EH, Thomas DC, Goldhirsch SL, et al. Geriatric hospital medicine. Med Clin North Am. 2002 Jul;86(4):707-729.
- Delbanco T. Hospital medicine: understanding and drawing on the patient's perspective. Am J Med. 2001;111(Suppl 9B):2S-4S. 6. Calkins DR, Davis RB, Reiley P, et al. Patient-physician communication at hospital discharge and patients' understanding of the postdischarge treatment plan. Arch Intern Med. 1997 May 12;157(9):1026-1030.
- Makaryus AN, Friedman EA. Patients' understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005 Aug;80(8):991-994.
- Coleman EA, Smith JD, Raha D, et al. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005 Sep;165(16):1842-1847.
- Nelson JR. The importance of postdischarge telephone follow-up for hospitalists: a view from the trenches. Am J Med. 2001 Dec 21;111(9B):43S-44S.
- Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005 Jul 19;143(2):121-128.
- van Walraven C, Mamdani M, Fang J, et al. Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004 Jun;19(6):624-631.
- Wachter RM, Pantilat SZ. The "continuity visit" and the hospitalist model of care. Am J Med. 2001;111(Suppl 9B):40S-42S.
- Goldman L, Pantilat SZ, Whitcomb WF. Passing the clinical baton: 6 principles to guide the hospitalist. Am J Med. 2001;111(Suppl 9B):36S-39S.
- Pantilat SZ, Lindenauer PK, Katz PP, et al. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111(Suppl 9B):15S-20S.
- Forster AJ. Can you prevent adverse drug events after hospital discharge? CMAJ. 2006 Mar 28;174(7):921-922.
- Ramey MM, Daniels S. Hospitalists and case managers: the perfect partnership. Lippincotts Case Manag. 2004 Nov-Dec;9(6):280-286.
- Ettner SL, Kotlerman J, Afifi A, et al. An alternative approach to reducing the costs of patient care? A controlled trial of the multi-disciplinary doctor-nurse practitioner (MDNP) model. Med Decis Making. 2006 Jan-Feb;26(1):9-17.
- Palmer HC, Armistead NS, Elnicki DM, et al. The effect of a hospitalist service with nurse discharge planner on patient care in an academic teaching hospital. Am J Med. 2001 Dec 1;111(8):627-632.
Patient discharge. It’s an everyday occurrence and, therefore, easily taken for granted. The hospitalist, who must help the patient transition back to the primary care physician, knows that this is a mistake. This transition takes an intense amount of communication among hospitalists, primary care and other physicians, nurses, case managers, social and therapy services, the patient, and the family.
Although smooth, effective patient handoffs are critical in maintaining patient safety and ensuring positive health outcomes, they are too often executed haphazardly, and the amount and precision of information as well as the means by which it is transmitted varies considerably. The journey is rife with communication landmines—communication can lapse or be absent, and when information falls through the cracks, continuity of care may be disrupted.
Top Considerations
Considering post-discharge communication in general, “probably the most important thing is to make sure that the hospitalist conveys as much of an impression of how the patient is doing [as possible],” says Richard Frankel, PhD, professor of medicine and geriatrics at Indiana University School of Medicine, Indianapolis, “not only in terms of their medical care or their disease process, but [also] what the patient’s hospital stay has been like, what the perception of their hospital experience has been like. And to be open to additional questions from the primary care physician about issues that might arise post discharge and ambiguities that might exist in the discharge summary.”
After determining a standardized protocol for post-discharge handoffs, “then I think that the most important thing is just practicing using these various protocols,” says Dr. Frankel, who also serves as senior research scientist at the Regenstrief Institute (Indianapolis) and is a research sociologist in the Health Services Research Unit at the Roudebush Veterans Affairs Medical Center, Indianapolis. “When the astronauts train, they train for every possible contingency so that when [a problem] arises it seems like the most common thing in the world, when in fact, what they practice are very low-frequency events, very low-probability problems arising.”
The nuts and bolts of ideal practices include essentials such as dictating notes and, preferably, transcribing and transmitting them by the close of the business day on which the patient is discharged.1 If short notes are sent to the primary care physician at the time of discharge, a longer summary should arrive within a few days. Because primary care physicians disagree as to what should be included in that summary, communication among physicians becomes a key issue in the transition.
“There’s a paucity of data on the subject of how well physicians communicate with each other,” says Darrell Solet, MD, cardiology fellow at the University of Texas, Southwestern Medical Center in Dallas. “A number of organizations have jumped on the bandwagon of improving this process, especially [the] Joint Commission [on] Accreditation of Healthcare Organizations,” he says.
Biggest Challenges
One of the major things the University of Texas Southwestern has emphasized in its residency program’s communication skills curriculum is not only how physicians communicate with their patients but also how well they communicate with each other. “This includes hearing a presentation on the most effective and efficient ways to perform their handoffs and also addressing the specific barriers to communication that they might face, says Dr. Solet.
These barriers to effective handoffs were identified in a study that Dr. Solet and his colleagues, including Dr. Frankel, conducted in 2005 in four hospitals in Indiana.2 At that time, Dr. Solet was the chief resident of ambulatory medicine, Department of Medicine, Indiana University School of Medicine, Indianapolis, and of medical service, Roudebush Veterans Affairs Medical Center, Indianapolis. In general, the study revealed that barriers to communication existed in four areas: physical settings, social settings, language, and communication styles.
Dr. Solet says that inconsistent information poses the biggest threat in the post-discharge communications he has seen. Another high-risk area involves documentation in which the physician writes only a line or two, such as, “This is a 50-ish-year-old man with COPD. Those one-liners are very dangerous,” he says.
In addition to the risks inherent in documentation, the biggest danger areas include pending test results, recommended follow-up studies, misunderstood medication instructions, never-purchased medications, and missed follow-up visits with the primary care physician.
Nelson and Whitcomb1 suggest that a post-discharge summary containing all essential information could overwhelm the primary care physician. They recommend standard forms with separate headings for diagnoses, medications, and hospital course, along with categories such as tests pending and evaluations needed. “Ideally, each hospitalist in a group should use the same format for these reports, so that a reader can quickly become accustomed to extracting information from them,” they write.
Tailor the Summary
Edward J. Merrens, MD, section chief of hospital medicine at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., was one of the authors of a study investigating ways to enhance the timeliness, accuracy, and breadth of clinical information gathered at discharge.3 The improvement project was conducted in a 330-bed tertiary care teaching hospital that averages 12,800 discharges a year.
“In general,” says Dr. Merrens, “we’re sending people out sicker and sicker, and often [the subsequent providers] don’t need a summary of all the interventions and studies and meds and antibiotics [done during the hospitalization], but what to do with the patient next. … Hospitalizations have become less therapeutic confinements where everything gets done, but [rather] where complex interventions occur and patients go out on therapy and are still often sick.”
The discharge summary should be designed in such a way that the primary care physician can simply “pick it up and go” from there, says Dr. Merrens. “We’ve tried to think, who really reads this thing? It could be [the] primary care physician, it may be a patient, it could be a doctor taking care of a patient in a rehabilitation facility, or it may be a visiting nurse service. We try to tailor the summary to those audiences, not just summarize what we’ve done.” His team has included a section on the summary where one can write, for example, “The patient might need more diuresis for their heart failure. They’re probably going to need a follow-up with this,” and Dr. Merrens says this structure has worked well.
“As we move from the Marcus Welby model of ‘you’re always on, you’re always covering, you’re the only doc’ to shift-based care,” he says, “the core of the [provider] group itself needs to communicate well, and it needs to agree on principles.” And this, he says, is a key component of job satisfaction for hospitalists.
—Edward J. Merrens, MD
Back to Long-Term Care
The goals of transitional care include ensuring continuity, providing for safe discharge, and preventing rehospitalization.4 Hospitalists have to recognize which patients are at risk for poor outcomes and devise ways to help prevent these problems. At particularly high risk are patients with the following characteristics:
- Age 80 and older;
- A history of depression;
- Multiple chronic diseases;
- Moderate-to-severe functional impairment;
- Noncompliance with therapy;
- Inadequate social supports;
- Multiple hospitalizations in the previous six months;
- Hospitalization in the last 30 days; and
- Fair or poor self-rating of health.4
Patients who return to long-term care, therefore, need careful transfer of information.
Nursing homes tell Dr. Merrens’ team that there is not enough practical information on the discharge summary about the patient’s current functional abilities. In response, the hospitalists included a section in their discharge documentation that summarizes the patient’s status, answering questions regarding the patient’s mental capacity, her ability to feed herself, her last bowel movement, her contact at the hospital in the event of a post-discharge emergency, and her designated power of attorney (if such a form was signed at the hospital).
At and After Discharge: Communicate with Patients and Families
Communication at the time of discharge involves, again, telling patients what’s next: Clarifying the use and potential side effects of medications, explaining when the patient can resume normal activities, providing the plan for and benefits of any occupational or physical therapy, and emphasizing the importance of follow-up. But it is also a time when patients should be told that they will need to “serve as expert witnesses to their care.”5
Tom Delbanco, MD, chief of the Division of General Medicine and Primary Care at Beth Israel Deaconess Medical Center, Boston, who has written extensively about communications and hospital medicine, reminds hospitalists that when it comes to getting feedback for quality improvement, it is far more helpful to gather patients’ self-reports than their ratings. Practitioners of hospital medicine, he adds, have an imperative not only to inquire into patient experiences, but also to catalog them and share findings with colleagues.
The Picker Institute (Boston), a nonprofit organization dedicated to the advancement of patient-centered healthcare, found that only one in 64 hospitals participating in its first national survey of hospitalized patients could be judged as particularly adept at preparing patients for discharge.5 What the staff were doing differently at that one hospital was very simple: They asked the patients and families to write down any questions they had before they went home; discharge occurred only after all those questions were answered.
Although post-discharge communication involves talking to and instructing patients, it also involves listening and watching for how well patients receive these communications. In the discharge conversation, patients may be groggy from too much or too little sleep, heavily medicated or coming off of major narcotics or general anesthesia, experiencing pain, suffering from anxiety or delirium, or just mentally disoriented from the stress of the hospital experience.5-8
Calkins and colleagues surveyed 99 patients to determine any difference in perceptions between patients and their attending physicians regarding the patients’ understanding of the treatment plan after hospitalization.6 Physicians reported spending more time discussing post-discharge care than did patients, and the doctors believed that 89% of patients understood the potential side effects of their medications when only 57% of the patients reported that they had.
Discharge summaries given directly to patients can help with comprehension and compliance.1 Telephone follow-up is also a valuable tool and, along with a chance to provide answers and encouragement, gives the patient a feeling of being cared for.1 Several studies have shown benefit in phone follow-up, providing a chance for hospitalists to review new test results, clarify misunderstandings, and encourage compliance, as well as to learn any unexpected outcomes, treatment failures, or side effects.9
Written instructions are imperative. One person should be assigned this duty and, on a standardized form, should provide details, not just when and how to call the primary care physician. The bare bones of a summary are not enough—especially if there was not a competent family member present at the final discharge conversation. Further, in many cases, questions arise after the patient is home, when a family member, a nurse, or the patient herself may have questions, particularly about medications.
Test Results and Follow-Up Studies
Among the factors contributing to failures at discharge is disrupted continuity of responsibility for pending test results and radiologic studies. This discontinuity may be especially operational in teaching hospitals, where physicians-in-training may frequently change services or shifts, and yet they remain responsible for all or some of the discharge communication.10 To prevent this disruption and avoid confusion, the institution or team should clarify the person responsible for follow-up on tests or studies. And they must communicate this information to the primary care physician.
Roy and colleagues looked at the prevalence, characteristics, and physician awareness of potentially actionable test results returning after hospital discharge at two major tertiary care centers.10 Of the 2,644 patients discharged from the hospitalist services, 1,095 (41%) had a total of 2,033 test results pending on the day of discharge, and 877 of these results (43%) were abnormal. Of the final 671 results included, 191 (9.4%) from 177 patients were potentially clinically actionable. Surveyed physicians were unaware of almost two-thirds of these potentially actionable results; more than a third of these results would change the patient’s diagnostic or treatment plan, and 12.6% of cases required urgent action. Other data show the unreliability of providing test results at follow-up visits; discharge summaries were available at only 12% to 33% of visits studied in one series.10
When inpatient physicians were asked how they would like electronic results-management systems that could highlight important results, filter out normal results, and help hospitalists track results returning after discharge, they were eager to adopt such systems. A future article in The Hospitalist will cover the emergence of electronic systems to better manage discharge communications.
Follow-up Contact with Patients
Van Walraven and colleagues looked at whether early post-discharge outcomes changed when patients were seen after discharge by physicians who had treated them in the hospital.11 When 938,833 adults from Ontario, Canada, were followed over five years after discharge from a medical or surgical hospitalization, 7.7% died or were readmitted. The adjusted relative risk of death or readmission decreased by 5% and 3% with each additional visit to a hospital physician—as opposed to a community physician or specialist, respectively. The effect of hospital physician visits was seen to have a dose-response effect, with the adjusted risk of 30-day death or nonelective readmission reduced to 7.3%, 7.0%, and 6.7% if patients had one, two, or three visits, respectively.
Hospital physician follow-up, say the authors of the Van Walraven, is a potentially modifiable factor that could decrease the risk of poor outcomes post discharge. Although not all providers embrace the concept, it does address the essential need of continuity of care through the potentially complicated transition from hospital to community. At the very least, the authors write, any physicians who sees the patient should have access to as much information as possible regarding the hospitalization and should be able to contact patients by phone post discharge.11-13
In a survey distributed by Steve Pantilat, MD, and colleagues, primary care physicians reported overwhelmingly that they preferred communicating with hospitalists by telephone at discharge (78%).14 While this may be unrealistic for all handoffs, says Dr. Merrens, hospitalists should make the effort for more complicated or serious cases.
Adverse Drug Events and Other Medication Issues
Although most adverse drug events (ADEs) are caused by the pharmacologic activity of the drug itself and can be predicted and mitigated, some one-third to one-half of ADEs are caused by human error or flawed systems.15
Coleman and colleagues looked at 375 patients, 65 and older, to analyze the medication problems they encountered.8 A significant percentage (14.1%) of older patients experienced one or more medication discrepancies after discharge; 50.8% were categorized as patient-associated; and 49.2% were seen as system-related. A total of 14.3% of the patients who experienced these discrepancies were rehospitalized at 30 days, compared with 6.1% of the patients who did not have any problems.
Of the contributing factors cited by patients, one-third were due to unintentional nonadherence, followed by financial barriers, intentional nonadherence, and neglect in filling a prescription.8 At the system level, incomplete, inaccurate, or illegible discharge instructions (as a result of either poor handwriting or use of Latin abbreviations) were the most commonly identified contributing factors, followed by conflicting information from different informational sources and duplicate prescribing.
Partnering with Case Management
Variability in physicians’ rounding patterns and schedules and in nurses’ and case managers’ shifts and assignments can make it difficult to bring involved parties together. Yet hospitalists look to case managers to follow up on acute services, interact with the patient’s plan of care, communicate with families, arrange follow-up with the primary care physician, and track the patient’s condition for progress.
Cogent Healthcare (Irvine, Calif.), a leading hospitalist company, has devised a means to optimize communication between case managers and hospitalists. The effects of this partnership have been shown to shorten hospital stay and reduce costs with no adverse effect on patient outcomes or patient satisfaction.16, 17 Along with responsibilities during the hospitalization, Cogent’s clinical care coordinators (CCC) make sure the primary care physician gets correct and appropriate information as soon as possible. The CCC phones the patient at home to ensure that the discharge plan is in place, that the patient is compliant with the post–acute treatment plan, and that she or he has a plan to meet with the primary care physician.
Case managers face a good deal of daily frustration, working on the same problems for patient after patient and trying to be available to help hospitalists make clinical practice decisions at the point of care. One way to improve overall post-discharge communication would be to lobby hospitals to provide the resources to support the case managers’ workload and their accessibility to their hospitalist colleagues.16, 18
Conclusion
Effective post-discharge communication includes standardizing an institution’s protocol for handoffs, increasing training and practice in post-discharge communication, and keeping the lines of communication open among hospitalists, primary care physicians, patients, and families. Collecting reported feedback from patients and families shortly after patients have returned home can be used toward quality improvement. Although the effectiveness of post-discharge communication may vary from hospital to hospital and even from hospitalist to hospitalist as well as across each hospitalist-primary care physician pairing, “I think that the interest that’s been stimulated in this whole area is exciting,” says Dr. Frankel. “This is an area where everybody wins. Rather than one person or one hospital winning and another one losing, there’s a new collaborative spirit that is very heartening to see.” TH
Andrea Sattinger writes regularly for The Hospitalist.
References
- Nelson JR, Whitcomb WF. Organizing a hospitalist program: an overview of fundamental concepts. Med Clin North Am. 2002 Jul 8;86(4):887-909.
- Solet DJ, Norvell JM, Rutan GH, et al. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005 Dec;80(12):1094-1099.
- Lurie JD, Merrens EJ, Lee J, et al. An approach to hospital quality improvement. Med Clin North Am. 2002 Jul;86(4):825-845.
- Callahan EH, Thomas DC, Goldhirsch SL, et al. Geriatric hospital medicine. Med Clin North Am. 2002 Jul;86(4):707-729.
- Delbanco T. Hospital medicine: understanding and drawing on the patient's perspective. Am J Med. 2001;111(Suppl 9B):2S-4S. 6. Calkins DR, Davis RB, Reiley P, et al. Patient-physician communication at hospital discharge and patients' understanding of the postdischarge treatment plan. Arch Intern Med. 1997 May 12;157(9):1026-1030.
- Makaryus AN, Friedman EA. Patients' understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005 Aug;80(8):991-994.
- Coleman EA, Smith JD, Raha D, et al. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005 Sep;165(16):1842-1847.
- Nelson JR. The importance of postdischarge telephone follow-up for hospitalists: a view from the trenches. Am J Med. 2001 Dec 21;111(9B):43S-44S.
- Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005 Jul 19;143(2):121-128.
- van Walraven C, Mamdani M, Fang J, et al. Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004 Jun;19(6):624-631.
- Wachter RM, Pantilat SZ. The "continuity visit" and the hospitalist model of care. Am J Med. 2001;111(Suppl 9B):40S-42S.
- Goldman L, Pantilat SZ, Whitcomb WF. Passing the clinical baton: 6 principles to guide the hospitalist. Am J Med. 2001;111(Suppl 9B):36S-39S.
- Pantilat SZ, Lindenauer PK, Katz PP, et al. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111(Suppl 9B):15S-20S.
- Forster AJ. Can you prevent adverse drug events after hospital discharge? CMAJ. 2006 Mar 28;174(7):921-922.
- Ramey MM, Daniels S. Hospitalists and case managers: the perfect partnership. Lippincotts Case Manag. 2004 Nov-Dec;9(6):280-286.
- Ettner SL, Kotlerman J, Afifi A, et al. An alternative approach to reducing the costs of patient care? A controlled trial of the multi-disciplinary doctor-nurse practitioner (MDNP) model. Med Decis Making. 2006 Jan-Feb;26(1):9-17.
- Palmer HC, Armistead NS, Elnicki DM, et al. The effect of a hospitalist service with nurse discharge planner on patient care in an academic teaching hospital. Am J Med. 2001 Dec 1;111(8):627-632.
Patient discharge. It’s an everyday occurrence and, therefore, easily taken for granted. The hospitalist, who must help the patient transition back to the primary care physician, knows that this is a mistake. This transition takes an intense amount of communication among hospitalists, primary care and other physicians, nurses, case managers, social and therapy services, the patient, and the family.
Although smooth, effective patient handoffs are critical in maintaining patient safety and ensuring positive health outcomes, they are too often executed haphazardly, and the amount and precision of information as well as the means by which it is transmitted varies considerably. The journey is rife with communication landmines—communication can lapse or be absent, and when information falls through the cracks, continuity of care may be disrupted.
Top Considerations
Considering post-discharge communication in general, “probably the most important thing is to make sure that the hospitalist conveys as much of an impression of how the patient is doing [as possible],” says Richard Frankel, PhD, professor of medicine and geriatrics at Indiana University School of Medicine, Indianapolis, “not only in terms of their medical care or their disease process, but [also] what the patient’s hospital stay has been like, what the perception of their hospital experience has been like. And to be open to additional questions from the primary care physician about issues that might arise post discharge and ambiguities that might exist in the discharge summary.”
After determining a standardized protocol for post-discharge handoffs, “then I think that the most important thing is just practicing using these various protocols,” says Dr. Frankel, who also serves as senior research scientist at the Regenstrief Institute (Indianapolis) and is a research sociologist in the Health Services Research Unit at the Roudebush Veterans Affairs Medical Center, Indianapolis. “When the astronauts train, they train for every possible contingency so that when [a problem] arises it seems like the most common thing in the world, when in fact, what they practice are very low-frequency events, very low-probability problems arising.”
The nuts and bolts of ideal practices include essentials such as dictating notes and, preferably, transcribing and transmitting them by the close of the business day on which the patient is discharged.1 If short notes are sent to the primary care physician at the time of discharge, a longer summary should arrive within a few days. Because primary care physicians disagree as to what should be included in that summary, communication among physicians becomes a key issue in the transition.
“There’s a paucity of data on the subject of how well physicians communicate with each other,” says Darrell Solet, MD, cardiology fellow at the University of Texas, Southwestern Medical Center in Dallas. “A number of organizations have jumped on the bandwagon of improving this process, especially [the] Joint Commission [on] Accreditation of Healthcare Organizations,” he says.
Biggest Challenges
One of the major things the University of Texas Southwestern has emphasized in its residency program’s communication skills curriculum is not only how physicians communicate with their patients but also how well they communicate with each other. “This includes hearing a presentation on the most effective and efficient ways to perform their handoffs and also addressing the specific barriers to communication that they might face, says Dr. Solet.
These barriers to effective handoffs were identified in a study that Dr. Solet and his colleagues, including Dr. Frankel, conducted in 2005 in four hospitals in Indiana.2 At that time, Dr. Solet was the chief resident of ambulatory medicine, Department of Medicine, Indiana University School of Medicine, Indianapolis, and of medical service, Roudebush Veterans Affairs Medical Center, Indianapolis. In general, the study revealed that barriers to communication existed in four areas: physical settings, social settings, language, and communication styles.
Dr. Solet says that inconsistent information poses the biggest threat in the post-discharge communications he has seen. Another high-risk area involves documentation in which the physician writes only a line or two, such as, “This is a 50-ish-year-old man with COPD. Those one-liners are very dangerous,” he says.
In addition to the risks inherent in documentation, the biggest danger areas include pending test results, recommended follow-up studies, misunderstood medication instructions, never-purchased medications, and missed follow-up visits with the primary care physician.
Nelson and Whitcomb1 suggest that a post-discharge summary containing all essential information could overwhelm the primary care physician. They recommend standard forms with separate headings for diagnoses, medications, and hospital course, along with categories such as tests pending and evaluations needed. “Ideally, each hospitalist in a group should use the same format for these reports, so that a reader can quickly become accustomed to extracting information from them,” they write.
Tailor the Summary
Edward J. Merrens, MD, section chief of hospital medicine at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., was one of the authors of a study investigating ways to enhance the timeliness, accuracy, and breadth of clinical information gathered at discharge.3 The improvement project was conducted in a 330-bed tertiary care teaching hospital that averages 12,800 discharges a year.
“In general,” says Dr. Merrens, “we’re sending people out sicker and sicker, and often [the subsequent providers] don’t need a summary of all the interventions and studies and meds and antibiotics [done during the hospitalization], but what to do with the patient next. … Hospitalizations have become less therapeutic confinements where everything gets done, but [rather] where complex interventions occur and patients go out on therapy and are still often sick.”
The discharge summary should be designed in such a way that the primary care physician can simply “pick it up and go” from there, says Dr. Merrens. “We’ve tried to think, who really reads this thing? It could be [the] primary care physician, it may be a patient, it could be a doctor taking care of a patient in a rehabilitation facility, or it may be a visiting nurse service. We try to tailor the summary to those audiences, not just summarize what we’ve done.” His team has included a section on the summary where one can write, for example, “The patient might need more diuresis for their heart failure. They’re probably going to need a follow-up with this,” and Dr. Merrens says this structure has worked well.
“As we move from the Marcus Welby model of ‘you’re always on, you’re always covering, you’re the only doc’ to shift-based care,” he says, “the core of the [provider] group itself needs to communicate well, and it needs to agree on principles.” And this, he says, is a key component of job satisfaction for hospitalists.
—Edward J. Merrens, MD
Back to Long-Term Care
The goals of transitional care include ensuring continuity, providing for safe discharge, and preventing rehospitalization.4 Hospitalists have to recognize which patients are at risk for poor outcomes and devise ways to help prevent these problems. At particularly high risk are patients with the following characteristics:
- Age 80 and older;
- A history of depression;
- Multiple chronic diseases;
- Moderate-to-severe functional impairment;
- Noncompliance with therapy;
- Inadequate social supports;
- Multiple hospitalizations in the previous six months;
- Hospitalization in the last 30 days; and
- Fair or poor self-rating of health.4
Patients who return to long-term care, therefore, need careful transfer of information.
Nursing homes tell Dr. Merrens’ team that there is not enough practical information on the discharge summary about the patient’s current functional abilities. In response, the hospitalists included a section in their discharge documentation that summarizes the patient’s status, answering questions regarding the patient’s mental capacity, her ability to feed herself, her last bowel movement, her contact at the hospital in the event of a post-discharge emergency, and her designated power of attorney (if such a form was signed at the hospital).
At and After Discharge: Communicate with Patients and Families
Communication at the time of discharge involves, again, telling patients what’s next: Clarifying the use and potential side effects of medications, explaining when the patient can resume normal activities, providing the plan for and benefits of any occupational or physical therapy, and emphasizing the importance of follow-up. But it is also a time when patients should be told that they will need to “serve as expert witnesses to their care.”5
Tom Delbanco, MD, chief of the Division of General Medicine and Primary Care at Beth Israel Deaconess Medical Center, Boston, who has written extensively about communications and hospital medicine, reminds hospitalists that when it comes to getting feedback for quality improvement, it is far more helpful to gather patients’ self-reports than their ratings. Practitioners of hospital medicine, he adds, have an imperative not only to inquire into patient experiences, but also to catalog them and share findings with colleagues.
The Picker Institute (Boston), a nonprofit organization dedicated to the advancement of patient-centered healthcare, found that only one in 64 hospitals participating in its first national survey of hospitalized patients could be judged as particularly adept at preparing patients for discharge.5 What the staff were doing differently at that one hospital was very simple: They asked the patients and families to write down any questions they had before they went home; discharge occurred only after all those questions were answered.
Although post-discharge communication involves talking to and instructing patients, it also involves listening and watching for how well patients receive these communications. In the discharge conversation, patients may be groggy from too much or too little sleep, heavily medicated or coming off of major narcotics or general anesthesia, experiencing pain, suffering from anxiety or delirium, or just mentally disoriented from the stress of the hospital experience.5-8
Calkins and colleagues surveyed 99 patients to determine any difference in perceptions between patients and their attending physicians regarding the patients’ understanding of the treatment plan after hospitalization.6 Physicians reported spending more time discussing post-discharge care than did patients, and the doctors believed that 89% of patients understood the potential side effects of their medications when only 57% of the patients reported that they had.
Discharge summaries given directly to patients can help with comprehension and compliance.1 Telephone follow-up is also a valuable tool and, along with a chance to provide answers and encouragement, gives the patient a feeling of being cared for.1 Several studies have shown benefit in phone follow-up, providing a chance for hospitalists to review new test results, clarify misunderstandings, and encourage compliance, as well as to learn any unexpected outcomes, treatment failures, or side effects.9
Written instructions are imperative. One person should be assigned this duty and, on a standardized form, should provide details, not just when and how to call the primary care physician. The bare bones of a summary are not enough—especially if there was not a competent family member present at the final discharge conversation. Further, in many cases, questions arise after the patient is home, when a family member, a nurse, or the patient herself may have questions, particularly about medications.
Test Results and Follow-Up Studies
Among the factors contributing to failures at discharge is disrupted continuity of responsibility for pending test results and radiologic studies. This discontinuity may be especially operational in teaching hospitals, where physicians-in-training may frequently change services or shifts, and yet they remain responsible for all or some of the discharge communication.10 To prevent this disruption and avoid confusion, the institution or team should clarify the person responsible for follow-up on tests or studies. And they must communicate this information to the primary care physician.
Roy and colleagues looked at the prevalence, characteristics, and physician awareness of potentially actionable test results returning after hospital discharge at two major tertiary care centers.10 Of the 2,644 patients discharged from the hospitalist services, 1,095 (41%) had a total of 2,033 test results pending on the day of discharge, and 877 of these results (43%) were abnormal. Of the final 671 results included, 191 (9.4%) from 177 patients were potentially clinically actionable. Surveyed physicians were unaware of almost two-thirds of these potentially actionable results; more than a third of these results would change the patient’s diagnostic or treatment plan, and 12.6% of cases required urgent action. Other data show the unreliability of providing test results at follow-up visits; discharge summaries were available at only 12% to 33% of visits studied in one series.10
When inpatient physicians were asked how they would like electronic results-management systems that could highlight important results, filter out normal results, and help hospitalists track results returning after discharge, they were eager to adopt such systems. A future article in The Hospitalist will cover the emergence of electronic systems to better manage discharge communications.
Follow-up Contact with Patients
Van Walraven and colleagues looked at whether early post-discharge outcomes changed when patients were seen after discharge by physicians who had treated them in the hospital.11 When 938,833 adults from Ontario, Canada, were followed over five years after discharge from a medical or surgical hospitalization, 7.7% died or were readmitted. The adjusted relative risk of death or readmission decreased by 5% and 3% with each additional visit to a hospital physician—as opposed to a community physician or specialist, respectively. The effect of hospital physician visits was seen to have a dose-response effect, with the adjusted risk of 30-day death or nonelective readmission reduced to 7.3%, 7.0%, and 6.7% if patients had one, two, or three visits, respectively.
Hospital physician follow-up, say the authors of the Van Walraven, is a potentially modifiable factor that could decrease the risk of poor outcomes post discharge. Although not all providers embrace the concept, it does address the essential need of continuity of care through the potentially complicated transition from hospital to community. At the very least, the authors write, any physicians who sees the patient should have access to as much information as possible regarding the hospitalization and should be able to contact patients by phone post discharge.11-13
In a survey distributed by Steve Pantilat, MD, and colleagues, primary care physicians reported overwhelmingly that they preferred communicating with hospitalists by telephone at discharge (78%).14 While this may be unrealistic for all handoffs, says Dr. Merrens, hospitalists should make the effort for more complicated or serious cases.
Adverse Drug Events and Other Medication Issues
Although most adverse drug events (ADEs) are caused by the pharmacologic activity of the drug itself and can be predicted and mitigated, some one-third to one-half of ADEs are caused by human error or flawed systems.15
Coleman and colleagues looked at 375 patients, 65 and older, to analyze the medication problems they encountered.8 A significant percentage (14.1%) of older patients experienced one or more medication discrepancies after discharge; 50.8% were categorized as patient-associated; and 49.2% were seen as system-related. A total of 14.3% of the patients who experienced these discrepancies were rehospitalized at 30 days, compared with 6.1% of the patients who did not have any problems.
Of the contributing factors cited by patients, one-third were due to unintentional nonadherence, followed by financial barriers, intentional nonadherence, and neglect in filling a prescription.8 At the system level, incomplete, inaccurate, or illegible discharge instructions (as a result of either poor handwriting or use of Latin abbreviations) were the most commonly identified contributing factors, followed by conflicting information from different informational sources and duplicate prescribing.
Partnering with Case Management
Variability in physicians’ rounding patterns and schedules and in nurses’ and case managers’ shifts and assignments can make it difficult to bring involved parties together. Yet hospitalists look to case managers to follow up on acute services, interact with the patient’s plan of care, communicate with families, arrange follow-up with the primary care physician, and track the patient’s condition for progress.
Cogent Healthcare (Irvine, Calif.), a leading hospitalist company, has devised a means to optimize communication between case managers and hospitalists. The effects of this partnership have been shown to shorten hospital stay and reduce costs with no adverse effect on patient outcomes or patient satisfaction.16, 17 Along with responsibilities during the hospitalization, Cogent’s clinical care coordinators (CCC) make sure the primary care physician gets correct and appropriate information as soon as possible. The CCC phones the patient at home to ensure that the discharge plan is in place, that the patient is compliant with the post–acute treatment plan, and that she or he has a plan to meet with the primary care physician.
Case managers face a good deal of daily frustration, working on the same problems for patient after patient and trying to be available to help hospitalists make clinical practice decisions at the point of care. One way to improve overall post-discharge communication would be to lobby hospitals to provide the resources to support the case managers’ workload and their accessibility to their hospitalist colleagues.16, 18
Conclusion
Effective post-discharge communication includes standardizing an institution’s protocol for handoffs, increasing training and practice in post-discharge communication, and keeping the lines of communication open among hospitalists, primary care physicians, patients, and families. Collecting reported feedback from patients and families shortly after patients have returned home can be used toward quality improvement. Although the effectiveness of post-discharge communication may vary from hospital to hospital and even from hospitalist to hospitalist as well as across each hospitalist-primary care physician pairing, “I think that the interest that’s been stimulated in this whole area is exciting,” says Dr. Frankel. “This is an area where everybody wins. Rather than one person or one hospital winning and another one losing, there’s a new collaborative spirit that is very heartening to see.” TH
Andrea Sattinger writes regularly for The Hospitalist.
References
- Nelson JR, Whitcomb WF. Organizing a hospitalist program: an overview of fundamental concepts. Med Clin North Am. 2002 Jul 8;86(4):887-909.
- Solet DJ, Norvell JM, Rutan GH, et al. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005 Dec;80(12):1094-1099.
- Lurie JD, Merrens EJ, Lee J, et al. An approach to hospital quality improvement. Med Clin North Am. 2002 Jul;86(4):825-845.
- Callahan EH, Thomas DC, Goldhirsch SL, et al. Geriatric hospital medicine. Med Clin North Am. 2002 Jul;86(4):707-729.
- Delbanco T. Hospital medicine: understanding and drawing on the patient's perspective. Am J Med. 2001;111(Suppl 9B):2S-4S. 6. Calkins DR, Davis RB, Reiley P, et al. Patient-physician communication at hospital discharge and patients' understanding of the postdischarge treatment plan. Arch Intern Med. 1997 May 12;157(9):1026-1030.
- Makaryus AN, Friedman EA. Patients' understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005 Aug;80(8):991-994.
- Coleman EA, Smith JD, Raha D, et al. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005 Sep;165(16):1842-1847.
- Nelson JR. The importance of postdischarge telephone follow-up for hospitalists: a view from the trenches. Am J Med. 2001 Dec 21;111(9B):43S-44S.
- Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005 Jul 19;143(2):121-128.
- van Walraven C, Mamdani M, Fang J, et al. Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004 Jun;19(6):624-631.
- Wachter RM, Pantilat SZ. The "continuity visit" and the hospitalist model of care. Am J Med. 2001;111(Suppl 9B):40S-42S.
- Goldman L, Pantilat SZ, Whitcomb WF. Passing the clinical baton: 6 principles to guide the hospitalist. Am J Med. 2001;111(Suppl 9B):36S-39S.
- Pantilat SZ, Lindenauer PK, Katz PP, et al. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111(Suppl 9B):15S-20S.
- Forster AJ. Can you prevent adverse drug events after hospital discharge? CMAJ. 2006 Mar 28;174(7):921-922.
- Ramey MM, Daniels S. Hospitalists and case managers: the perfect partnership. Lippincotts Case Manag. 2004 Nov-Dec;9(6):280-286.
- Ettner SL, Kotlerman J, Afifi A, et al. An alternative approach to reducing the costs of patient care? A controlled trial of the multi-disciplinary doctor-nurse practitioner (MDNP) model. Med Decis Making. 2006 Jan-Feb;26(1):9-17.
- Palmer HC, Armistead NS, Elnicki DM, et al. The effect of a hospitalist service with nurse discharge planner on patient care in an academic teaching hospital. Am J Med. 2001 Dec 1;111(8):627-632.
Risky Business II: A Whole New Category of Risk
Five years ago, it was clearly recognized that malpractice law associated with hospitalist systems was an emerging phenomenon.1 But today this is rapidly changing, says Linda Greenwald, RN, MS, the editor of Risk Management Publications at the ProMutual Insurance Group, Boston, who keeps an eye on emerging trends related to medical malpractice litigation.
“There’s a whole new category of risk coming up,” she says, “because it’s a whole new specialty that kind of exploded on the scene, and some time needs to be spent defining the role of hospitalists.”
The 2006 winter issue of the company’s newsletter, Perspectives on Clinical Risk Management, was devoted to the subject of hospitalists.2 Patient safety concerns and communication, particularly as they relate to post-discharge communication, were the two overriding issues Greenwald identified connecting malpractice risk and hospitalists. (An upcoming issue of The Hospitalist will address the topic of post-discharge communication.) From her research, Greenwald gathered that hospitalists were considered “like the residents of yore,” expected to “cover the entire house,” to be everything and do everything for everyone.
The newsletter issue advises hospitalists to explain to patients and families who you are and what your role is, and to ask them pointedly whether they have concerns about that. Many patients feel abandoned by their primary care physicians; they don’t understand the new system, and they need to be reassured about the continuity of care. In a larger sense, ProMutual also suggests that institutions provide some type of public forum in their community for the public and providers both, to openly discuss ways to make the hospitalist system work for them all.
—Meg Gaines, JD, LLM
That Dollar Sign
Accumulating evidence shows that some of the contributory causes of rising healthcare-related litigiousness include patients’ higher expectations, poor provider-patient communication, and society’s adversarial legal stance.3
What is really to blame for the rising malpractice costs? “The medical system in our country is grounded in money,” says Meg Gaines, JD, LLM, clinical professor of law at the University of Wisconsin Law School, Madison. “It’s grounded in profit or, at the least, fiscal survival, depending on the institution. … In the bottom line equation, one of the variables is a dollar sign.”
Therefore, she says, anyone working in the hospital needs to recognize that, to a great extent, their working life revolves around that equation.
“The press has made this connection between [the number and amounts of payouts for] lawsuits and rising malpractice costs,” says Professor Gaines. “[It’s not] that there isn’t a connection. But what we do know, and what there is ample research to show, is that malpractice rates are much more linked to the rise and fall of the stock market.”4-10
To an insurance provider, she explains, the premiums are basically a loss leader; that is, a product sold below cost. “They don’t make money on premiums,” says Professor Gaines. “They make money investing premiums. You can see the correlation between rates and stock market performance over time.”
Professor Gaines says that the media has led the public to believe that the high cost of healthcare is due to skyrocketing medical malpractice awards. “Many of the states that put caps on their awards for malpractice torts are doing fine, but so are many states without caps,” she says. “It behooves the press to pit wicked lawyers against angelic doctors, or vice versa,” but it’s a lot more complicated than that. “And that rhetoric takes away from the real point, which is this: Nobody disagrees that too many patients are injured through negligence. But the number of patients injured through documented negligence who actually sue is somewhere between 2%-8%,” which is a very small percentage. Maybe too small.
Bad things happen to good people, and not everybody sues; it’s the people who feel that they’re cared for that tend not to sue. The documentation for this is increasing daily.
“Patients who have good, communicative relationships with their doctors don’t sue,” says Professor Gaines. “We generally don’t sue people we love or who love us.” And that’s a good thing, she speculates. “But it is important for doctors to think about this: So your patients don’t sue you, but you do make mistakes, right? And sometimes you cause injury. So how does that work for you that you have malpractice insurance that covers you for injury that you cause, but your patients won’t sue you because they love you?” she asks. “How do we all sleep at night thinking it’s a good thing that between 92%-98% of people who are injured by our negligence don’t get compensated?”
The Value of Litigation
With respect to the issue of patient safety, says George J. Annas, JD, MPH, Edward R. Utley professor of health law and the chairman of the Department of Health Law, Bioethics, and Human Rights at Boston University School of Public Health, rather than doctors and lawyers viewing each other as “predator and prey,” it would be far more beneficial for them to see each other as “natural allies.”11 He suggests that we recall the intended purpose of litigation and its value for society.
Professor Gaines concurs: “We live in this world where on the medical side people are so litigation-phobic that we really aren’t able to see the value of litigation anymore.” Healthcare itself can be viewed as a patient that might be healthier if required to pay the price of unhealthy practices: namely, failing to engage in communication and safety practices that would reduce error and injury. Shaking up that system might lead to better healthcare.11
In fact, the claim that the malpractice system is fraught with frivolous litigation has been called “overblown” and not substantiated in the literature.12 The malpractice system is effective in separating claims without merit from those with merit and compensating the latter. In an analysis of outcomes and claims costs from 1,452 closed malpractice claims from five liability insurers, “three-quarters of the litigation outcomes were concordant with the merits of the claim.”12
“Some of the most excellent doctors I know have said to me on the QT, ‘I’m sure glad you lawyers are around because if you weren’t I don’t know how we’d ever get rid of the scary doctors.’ ” says Professor Gaines. “And if the rate of malpractice claims for merited negligence “is only 2%-8%,” she says, “we’re probably not doing a great job of it.”
What makes doctors scary to patients? Or, rather, what makes a good doctor? When patients and physicians were both asked this question (pertaining to outpatient physicians), more patients than doctors considered the exchange of health-related information to be an essential aspect of their healthcare. Physicians placed it far lower on their list.13 These kinds of differences in perception may influence the quality of interactions between physicians and patients, the study concluded.
Professor Gaines, who has consulted with hundreds of physicians and nurses in her role as director of the Center for Patient Partnerships at the University of Wisconsin, encourages them to spend time in meaningful communication with their patients. “Their argument usually is: I don’t have time.” she says. “My answer is: You don’t have time not to.”
Communication and Patient Safety Concerns
The needs for superb patient safety and optimal healthcare communication are intertwined. In research on quality of care, patient safety is now specifically named as a factor and is distinguished from effectiveness.4 Malpractice litigation is often pursued when patients experience an adverse outcome coupled with a lack of empathy from and a withholding of essential information by physicians.14 Senators Hillary Clinton (D-NY) and Barack Obama (D-IL) cite documentation for this when they advocate for patient safety to be the centerpiece of medical liability reform.
As careful as hospitalists might be to protect their patients from safety hazards and errors, however, they alone cannot protect themselves and their institutions from wrongdoing or the risk of litigation.
“In hospital care, the challenge is to reform corporate governance to make hospital boards take their responsibility for patient safety at least as seriously as they take the hospital’s financial condition,”11 writes Professor Annas, who’s affiliated with both Boston University’s School of Law and School of Medicine. “Hospitals that do not take specific actions to improve safety should be viewed as negligent and be subject to malpractice lawsuits when a violation of the right to safety results in injury.”
It is also the hospital’s obligation, he says, to maintain a safe environment for healthcare providers. And hospitalists and other providers who “live” in hospitals have an ethical obligation to advance the connection of patient safety and communication in hospital-medicine-led quality improvement as well as whole-hospital initiatives.3,11,15,16 That means that staffing, technologies, and facilities must all be up to par so providers can work with the assurance that available resources will support their efforts to provide the best care for their patients.11
Those objectives were taken on by the University of Michigan (Ann Arbor) in a program launched in 2002 to reduce litigation costs, accelerate provision of compensation to patients, and increase the numbers of patients who are compensated for their injuries. The link between the medical liability environment and patient safety was well illustrated in their results. The program involved three strategic components:
- Acknowledge cases in which a patient was hurt because of medical error and compensate these patients quickly and fairly;
- Aggressively defend cases that the hospital considers to be without merit; and
- Study all adverse events to determine how procedures could be improved.
Whereas the organization had approximately 260 claims and lawsuits pending at any given time prior to August 2001, by August 2005 the number had dropped to 114. The average time from the filing of a claim to its resolution was reduced by 11 months, and annual litigation costs dropped from about $3 million to $1 million.14
This program clearly connected the dots between responsibility, compensation for merited negligence, systems quality improvement, and communication across the board. Senators Rodham Clinton and Obama infused their bill with the sensibility that these humane criteria are particularly important.14 When healthcare providers, administrators, and regulators around the world are being advised that a “post-event communication-cum-mediation framework” is the key national strategy for resolving malpractice disputes,3 the need for empathy, apology, and responsibility are implied. (See “I’m Sorry,” June 2006, p.25.)
“When I talk about patient safety, I imagine hospitalists are particularly attuned to this,” says Professor Gaines, “I am talking about what a physician could do in 15 seconds if every single patient is actively engaged in their [own] care.” It’s a no-brainer and “the easiest thing in the world if patients are invited and made to feel welcome as full members of the team.”
Inattention to little things can cause the risky miscommunications that lead to serious problems, both medically and legally. And yet, says Professor Gaines, the remedy is sometimes as easy as “having an informed patient partner as the final check.”
The Bottom Line for Hospitalists
When asked what she wants to say to hospitalists from her personal experience as a hospital inpatient as well as that of her extensive professional background as a criminal defense lawyer, law professor, and patient advocate, Professor Gaines began with her own expression of empathy. “First, in many ways you’re being asked to do an impossible job,” she says. “And patients like me, critics, and commentators will say, ‘Hey! You’re not doing it as well as you could.’ ”
Hospitalists, she says, might be prone to say, “ ‘Leave me alone. I’m doing the best I can.” You’re doing what may be an untenable job, you’ve got specialists leaning on you from one angle, patients and families … wailing on you from another level, and you’re … stuck in between: a utility player, the one everyone loves to boo off the field when you’re having a bad day.”
On the other hand, she says, “Every day I am carving another little bit of my epitaph, and what it says at the end is of my making. And if you can’t carve in these circumstances, then change them or do something about it. But when the bell tolls for thee, the fact that you worked in a busy hospital and had a bunch of overqualified guys breathing down your neck and under-informed patients blaming you for things that aren’t really your fault—that’s going to be footnote material. Carve out your ground, stand it, and do the job you can be proud of. And nobody and nothing gets you off the hook for that.”
Conclusion
The rising costs of medical malpractice litigation are far more a function of the fluctuations of the economy, among other factors, than of the number and size of malpractice claims payouts. Data show that the vast majority of expenditures that go toward litigation are not due to frivolous claims or unmerited compensation. In fact, litigation may hold value in serving to remind hospitals and providers that the best means of warding off lawsuits is to invest resources in patient safety, including prioritizing communication with patients, families, and colleagues. TH
Andrea Sattinger wrote “Risky Business I” in the Feb. 2006 issue (p. 1).
References
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9S.
- Greenwald L, ed. Hospitalists. Perspectives on Clinical Risk Management. Winter 2006.
- Harold TK. Minimizing medical litigation, part 2. J Med Pract Manage. 2006 Mar-Apr;21(5):257-261.
- Brennan TA, Gawande A, Thomas E, et al. Accidental deaths, saved lives, and improved quality. N Engl J Med. 2005 Sep 29;353(13):1405-1409.
- Brennan TA, Mello MM. Patient safety and medical malpractice: a case study. Ann Intern Med. 2003 Aug 19;139(4):267-273.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation N Engl J Med. 1996 Dec 26;335(26):1963-1967.
- Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991 Feb 7;324(6):370-376.
- Harvard Medical Practice Study. Patients, doctors, and lawyers: medical injury, malpractice litigation, and patient compensation in New York. Report of the Harvard Medical Practice Study to the state of New York. Cambridge, Mass: President and Fellows of Harvard College; 1990: www.nysl.nysed.gov/scandoclinks/OCM21331963.htm. Last accessed July 11, 2006.
- Localio AR, Lawthers AG, Brennan TA et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Mills DH, ed. California Medical Association and California Hospital Association Report on the Medical Insurance Feasibility Study. San Francisco, Calif: Sutter Publications; 1977.
- Annas GJ. The patient's right to safety—improving the quality of care through litigation against hospitals. N Engl J Med. 2006 May 11;354(19):2063-2066.
- Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006 May 11;354(19):2024-2033.
- Laine C, Davidoff F, Lewis CE, et al. Important elements of outpatient care: a comparison of patients' and physicians' opinions. Ann Intern Med. 1996 Oct 15;125(8):640-645.
- Clinton HR, Obama B. Making patient safety the centerpiece of medical liability reform. N Engl J Med. 2006;354:2205-2208.
- Studdert DM, Mello MM, Brennan TA. Medical malpractice. N Engl J Med. 2004;350:283-292.
- Delbanco TL. Quality of care through the patient's eyes. BMJ. 1996;313:832-833.
Five years ago, it was clearly recognized that malpractice law associated with hospitalist systems was an emerging phenomenon.1 But today this is rapidly changing, says Linda Greenwald, RN, MS, the editor of Risk Management Publications at the ProMutual Insurance Group, Boston, who keeps an eye on emerging trends related to medical malpractice litigation.
“There’s a whole new category of risk coming up,” she says, “because it’s a whole new specialty that kind of exploded on the scene, and some time needs to be spent defining the role of hospitalists.”
The 2006 winter issue of the company’s newsletter, Perspectives on Clinical Risk Management, was devoted to the subject of hospitalists.2 Patient safety concerns and communication, particularly as they relate to post-discharge communication, were the two overriding issues Greenwald identified connecting malpractice risk and hospitalists. (An upcoming issue of The Hospitalist will address the topic of post-discharge communication.) From her research, Greenwald gathered that hospitalists were considered “like the residents of yore,” expected to “cover the entire house,” to be everything and do everything for everyone.
The newsletter issue advises hospitalists to explain to patients and families who you are and what your role is, and to ask them pointedly whether they have concerns about that. Many patients feel abandoned by their primary care physicians; they don’t understand the new system, and they need to be reassured about the continuity of care. In a larger sense, ProMutual also suggests that institutions provide some type of public forum in their community for the public and providers both, to openly discuss ways to make the hospitalist system work for them all.
—Meg Gaines, JD, LLM
That Dollar Sign
Accumulating evidence shows that some of the contributory causes of rising healthcare-related litigiousness include patients’ higher expectations, poor provider-patient communication, and society’s adversarial legal stance.3
What is really to blame for the rising malpractice costs? “The medical system in our country is grounded in money,” says Meg Gaines, JD, LLM, clinical professor of law at the University of Wisconsin Law School, Madison. “It’s grounded in profit or, at the least, fiscal survival, depending on the institution. … In the bottom line equation, one of the variables is a dollar sign.”
Therefore, she says, anyone working in the hospital needs to recognize that, to a great extent, their working life revolves around that equation.
“The press has made this connection between [the number and amounts of payouts for] lawsuits and rising malpractice costs,” says Professor Gaines. “[It’s not] that there isn’t a connection. But what we do know, and what there is ample research to show, is that malpractice rates are much more linked to the rise and fall of the stock market.”4-10
To an insurance provider, she explains, the premiums are basically a loss leader; that is, a product sold below cost. “They don’t make money on premiums,” says Professor Gaines. “They make money investing premiums. You can see the correlation between rates and stock market performance over time.”
Professor Gaines says that the media has led the public to believe that the high cost of healthcare is due to skyrocketing medical malpractice awards. “Many of the states that put caps on their awards for malpractice torts are doing fine, but so are many states without caps,” she says. “It behooves the press to pit wicked lawyers against angelic doctors, or vice versa,” but it’s a lot more complicated than that. “And that rhetoric takes away from the real point, which is this: Nobody disagrees that too many patients are injured through negligence. But the number of patients injured through documented negligence who actually sue is somewhere between 2%-8%,” which is a very small percentage. Maybe too small.
Bad things happen to good people, and not everybody sues; it’s the people who feel that they’re cared for that tend not to sue. The documentation for this is increasing daily.
“Patients who have good, communicative relationships with their doctors don’t sue,” says Professor Gaines. “We generally don’t sue people we love or who love us.” And that’s a good thing, she speculates. “But it is important for doctors to think about this: So your patients don’t sue you, but you do make mistakes, right? And sometimes you cause injury. So how does that work for you that you have malpractice insurance that covers you for injury that you cause, but your patients won’t sue you because they love you?” she asks. “How do we all sleep at night thinking it’s a good thing that between 92%-98% of people who are injured by our negligence don’t get compensated?”
The Value of Litigation
With respect to the issue of patient safety, says George J. Annas, JD, MPH, Edward R. Utley professor of health law and the chairman of the Department of Health Law, Bioethics, and Human Rights at Boston University School of Public Health, rather than doctors and lawyers viewing each other as “predator and prey,” it would be far more beneficial for them to see each other as “natural allies.”11 He suggests that we recall the intended purpose of litigation and its value for society.
Professor Gaines concurs: “We live in this world where on the medical side people are so litigation-phobic that we really aren’t able to see the value of litigation anymore.” Healthcare itself can be viewed as a patient that might be healthier if required to pay the price of unhealthy practices: namely, failing to engage in communication and safety practices that would reduce error and injury. Shaking up that system might lead to better healthcare.11
In fact, the claim that the malpractice system is fraught with frivolous litigation has been called “overblown” and not substantiated in the literature.12 The malpractice system is effective in separating claims without merit from those with merit and compensating the latter. In an analysis of outcomes and claims costs from 1,452 closed malpractice claims from five liability insurers, “three-quarters of the litigation outcomes were concordant with the merits of the claim.”12
“Some of the most excellent doctors I know have said to me on the QT, ‘I’m sure glad you lawyers are around because if you weren’t I don’t know how we’d ever get rid of the scary doctors.’ ” says Professor Gaines. “And if the rate of malpractice claims for merited negligence “is only 2%-8%,” she says, “we’re probably not doing a great job of it.”
What makes doctors scary to patients? Or, rather, what makes a good doctor? When patients and physicians were both asked this question (pertaining to outpatient physicians), more patients than doctors considered the exchange of health-related information to be an essential aspect of their healthcare. Physicians placed it far lower on their list.13 These kinds of differences in perception may influence the quality of interactions between physicians and patients, the study concluded.
Professor Gaines, who has consulted with hundreds of physicians and nurses in her role as director of the Center for Patient Partnerships at the University of Wisconsin, encourages them to spend time in meaningful communication with their patients. “Their argument usually is: I don’t have time.” she says. “My answer is: You don’t have time not to.”
Communication and Patient Safety Concerns
The needs for superb patient safety and optimal healthcare communication are intertwined. In research on quality of care, patient safety is now specifically named as a factor and is distinguished from effectiveness.4 Malpractice litigation is often pursued when patients experience an adverse outcome coupled with a lack of empathy from and a withholding of essential information by physicians.14 Senators Hillary Clinton (D-NY) and Barack Obama (D-IL) cite documentation for this when they advocate for patient safety to be the centerpiece of medical liability reform.
As careful as hospitalists might be to protect their patients from safety hazards and errors, however, they alone cannot protect themselves and their institutions from wrongdoing or the risk of litigation.
“In hospital care, the challenge is to reform corporate governance to make hospital boards take their responsibility for patient safety at least as seriously as they take the hospital’s financial condition,”11 writes Professor Annas, who’s affiliated with both Boston University’s School of Law and School of Medicine. “Hospitals that do not take specific actions to improve safety should be viewed as negligent and be subject to malpractice lawsuits when a violation of the right to safety results in injury.”
It is also the hospital’s obligation, he says, to maintain a safe environment for healthcare providers. And hospitalists and other providers who “live” in hospitals have an ethical obligation to advance the connection of patient safety and communication in hospital-medicine-led quality improvement as well as whole-hospital initiatives.3,11,15,16 That means that staffing, technologies, and facilities must all be up to par so providers can work with the assurance that available resources will support their efforts to provide the best care for their patients.11
Those objectives were taken on by the University of Michigan (Ann Arbor) in a program launched in 2002 to reduce litigation costs, accelerate provision of compensation to patients, and increase the numbers of patients who are compensated for their injuries. The link between the medical liability environment and patient safety was well illustrated in their results. The program involved three strategic components:
- Acknowledge cases in which a patient was hurt because of medical error and compensate these patients quickly and fairly;
- Aggressively defend cases that the hospital considers to be without merit; and
- Study all adverse events to determine how procedures could be improved.
Whereas the organization had approximately 260 claims and lawsuits pending at any given time prior to August 2001, by August 2005 the number had dropped to 114. The average time from the filing of a claim to its resolution was reduced by 11 months, and annual litigation costs dropped from about $3 million to $1 million.14
This program clearly connected the dots between responsibility, compensation for merited negligence, systems quality improvement, and communication across the board. Senators Rodham Clinton and Obama infused their bill with the sensibility that these humane criteria are particularly important.14 When healthcare providers, administrators, and regulators around the world are being advised that a “post-event communication-cum-mediation framework” is the key national strategy for resolving malpractice disputes,3 the need for empathy, apology, and responsibility are implied. (See “I’m Sorry,” June 2006, p.25.)
“When I talk about patient safety, I imagine hospitalists are particularly attuned to this,” says Professor Gaines, “I am talking about what a physician could do in 15 seconds if every single patient is actively engaged in their [own] care.” It’s a no-brainer and “the easiest thing in the world if patients are invited and made to feel welcome as full members of the team.”
Inattention to little things can cause the risky miscommunications that lead to serious problems, both medically and legally. And yet, says Professor Gaines, the remedy is sometimes as easy as “having an informed patient partner as the final check.”
The Bottom Line for Hospitalists
When asked what she wants to say to hospitalists from her personal experience as a hospital inpatient as well as that of her extensive professional background as a criminal defense lawyer, law professor, and patient advocate, Professor Gaines began with her own expression of empathy. “First, in many ways you’re being asked to do an impossible job,” she says. “And patients like me, critics, and commentators will say, ‘Hey! You’re not doing it as well as you could.’ ”
Hospitalists, she says, might be prone to say, “ ‘Leave me alone. I’m doing the best I can.” You’re doing what may be an untenable job, you’ve got specialists leaning on you from one angle, patients and families … wailing on you from another level, and you’re … stuck in between: a utility player, the one everyone loves to boo off the field when you’re having a bad day.”
On the other hand, she says, “Every day I am carving another little bit of my epitaph, and what it says at the end is of my making. And if you can’t carve in these circumstances, then change them or do something about it. But when the bell tolls for thee, the fact that you worked in a busy hospital and had a bunch of overqualified guys breathing down your neck and under-informed patients blaming you for things that aren’t really your fault—that’s going to be footnote material. Carve out your ground, stand it, and do the job you can be proud of. And nobody and nothing gets you off the hook for that.”
Conclusion
The rising costs of medical malpractice litigation are far more a function of the fluctuations of the economy, among other factors, than of the number and size of malpractice claims payouts. Data show that the vast majority of expenditures that go toward litigation are not due to frivolous claims or unmerited compensation. In fact, litigation may hold value in serving to remind hospitals and providers that the best means of warding off lawsuits is to invest resources in patient safety, including prioritizing communication with patients, families, and colleagues. TH
Andrea Sattinger wrote “Risky Business I” in the Feb. 2006 issue (p. 1).
References
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9S.
- Greenwald L, ed. Hospitalists. Perspectives on Clinical Risk Management. Winter 2006.
- Harold TK. Minimizing medical litigation, part 2. J Med Pract Manage. 2006 Mar-Apr;21(5):257-261.
- Brennan TA, Gawande A, Thomas E, et al. Accidental deaths, saved lives, and improved quality. N Engl J Med. 2005 Sep 29;353(13):1405-1409.
- Brennan TA, Mello MM. Patient safety and medical malpractice: a case study. Ann Intern Med. 2003 Aug 19;139(4):267-273.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation N Engl J Med. 1996 Dec 26;335(26):1963-1967.
- Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991 Feb 7;324(6):370-376.
- Harvard Medical Practice Study. Patients, doctors, and lawyers: medical injury, malpractice litigation, and patient compensation in New York. Report of the Harvard Medical Practice Study to the state of New York. Cambridge, Mass: President and Fellows of Harvard College; 1990: www.nysl.nysed.gov/scandoclinks/OCM21331963.htm. Last accessed July 11, 2006.
- Localio AR, Lawthers AG, Brennan TA et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Mills DH, ed. California Medical Association and California Hospital Association Report on the Medical Insurance Feasibility Study. San Francisco, Calif: Sutter Publications; 1977.
- Annas GJ. The patient's right to safety—improving the quality of care through litigation against hospitals. N Engl J Med. 2006 May 11;354(19):2063-2066.
- Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006 May 11;354(19):2024-2033.
- Laine C, Davidoff F, Lewis CE, et al. Important elements of outpatient care: a comparison of patients' and physicians' opinions. Ann Intern Med. 1996 Oct 15;125(8):640-645.
- Clinton HR, Obama B. Making patient safety the centerpiece of medical liability reform. N Engl J Med. 2006;354:2205-2208.
- Studdert DM, Mello MM, Brennan TA. Medical malpractice. N Engl J Med. 2004;350:283-292.
- Delbanco TL. Quality of care through the patient's eyes. BMJ. 1996;313:832-833.
Five years ago, it was clearly recognized that malpractice law associated with hospitalist systems was an emerging phenomenon.1 But today this is rapidly changing, says Linda Greenwald, RN, MS, the editor of Risk Management Publications at the ProMutual Insurance Group, Boston, who keeps an eye on emerging trends related to medical malpractice litigation.
“There’s a whole new category of risk coming up,” she says, “because it’s a whole new specialty that kind of exploded on the scene, and some time needs to be spent defining the role of hospitalists.”
The 2006 winter issue of the company’s newsletter, Perspectives on Clinical Risk Management, was devoted to the subject of hospitalists.2 Patient safety concerns and communication, particularly as they relate to post-discharge communication, were the two overriding issues Greenwald identified connecting malpractice risk and hospitalists. (An upcoming issue of The Hospitalist will address the topic of post-discharge communication.) From her research, Greenwald gathered that hospitalists were considered “like the residents of yore,” expected to “cover the entire house,” to be everything and do everything for everyone.
The newsletter issue advises hospitalists to explain to patients and families who you are and what your role is, and to ask them pointedly whether they have concerns about that. Many patients feel abandoned by their primary care physicians; they don’t understand the new system, and they need to be reassured about the continuity of care. In a larger sense, ProMutual also suggests that institutions provide some type of public forum in their community for the public and providers both, to openly discuss ways to make the hospitalist system work for them all.
—Meg Gaines, JD, LLM
That Dollar Sign
Accumulating evidence shows that some of the contributory causes of rising healthcare-related litigiousness include patients’ higher expectations, poor provider-patient communication, and society’s adversarial legal stance.3
What is really to blame for the rising malpractice costs? “The medical system in our country is grounded in money,” says Meg Gaines, JD, LLM, clinical professor of law at the University of Wisconsin Law School, Madison. “It’s grounded in profit or, at the least, fiscal survival, depending on the institution. … In the bottom line equation, one of the variables is a dollar sign.”
Therefore, she says, anyone working in the hospital needs to recognize that, to a great extent, their working life revolves around that equation.
“The press has made this connection between [the number and amounts of payouts for] lawsuits and rising malpractice costs,” says Professor Gaines. “[It’s not] that there isn’t a connection. But what we do know, and what there is ample research to show, is that malpractice rates are much more linked to the rise and fall of the stock market.”4-10
To an insurance provider, she explains, the premiums are basically a loss leader; that is, a product sold below cost. “They don’t make money on premiums,” says Professor Gaines. “They make money investing premiums. You can see the correlation between rates and stock market performance over time.”
Professor Gaines says that the media has led the public to believe that the high cost of healthcare is due to skyrocketing medical malpractice awards. “Many of the states that put caps on their awards for malpractice torts are doing fine, but so are many states without caps,” she says. “It behooves the press to pit wicked lawyers against angelic doctors, or vice versa,” but it’s a lot more complicated than that. “And that rhetoric takes away from the real point, which is this: Nobody disagrees that too many patients are injured through negligence. But the number of patients injured through documented negligence who actually sue is somewhere between 2%-8%,” which is a very small percentage. Maybe too small.
Bad things happen to good people, and not everybody sues; it’s the people who feel that they’re cared for that tend not to sue. The documentation for this is increasing daily.
“Patients who have good, communicative relationships with their doctors don’t sue,” says Professor Gaines. “We generally don’t sue people we love or who love us.” And that’s a good thing, she speculates. “But it is important for doctors to think about this: So your patients don’t sue you, but you do make mistakes, right? And sometimes you cause injury. So how does that work for you that you have malpractice insurance that covers you for injury that you cause, but your patients won’t sue you because they love you?” she asks. “How do we all sleep at night thinking it’s a good thing that between 92%-98% of people who are injured by our negligence don’t get compensated?”
The Value of Litigation
With respect to the issue of patient safety, says George J. Annas, JD, MPH, Edward R. Utley professor of health law and the chairman of the Department of Health Law, Bioethics, and Human Rights at Boston University School of Public Health, rather than doctors and lawyers viewing each other as “predator and prey,” it would be far more beneficial for them to see each other as “natural allies.”11 He suggests that we recall the intended purpose of litigation and its value for society.
Professor Gaines concurs: “We live in this world where on the medical side people are so litigation-phobic that we really aren’t able to see the value of litigation anymore.” Healthcare itself can be viewed as a patient that might be healthier if required to pay the price of unhealthy practices: namely, failing to engage in communication and safety practices that would reduce error and injury. Shaking up that system might lead to better healthcare.11
In fact, the claim that the malpractice system is fraught with frivolous litigation has been called “overblown” and not substantiated in the literature.12 The malpractice system is effective in separating claims without merit from those with merit and compensating the latter. In an analysis of outcomes and claims costs from 1,452 closed malpractice claims from five liability insurers, “three-quarters of the litigation outcomes were concordant with the merits of the claim.”12
“Some of the most excellent doctors I know have said to me on the QT, ‘I’m sure glad you lawyers are around because if you weren’t I don’t know how we’d ever get rid of the scary doctors.’ ” says Professor Gaines. “And if the rate of malpractice claims for merited negligence “is only 2%-8%,” she says, “we’re probably not doing a great job of it.”
What makes doctors scary to patients? Or, rather, what makes a good doctor? When patients and physicians were both asked this question (pertaining to outpatient physicians), more patients than doctors considered the exchange of health-related information to be an essential aspect of their healthcare. Physicians placed it far lower on their list.13 These kinds of differences in perception may influence the quality of interactions between physicians and patients, the study concluded.
Professor Gaines, who has consulted with hundreds of physicians and nurses in her role as director of the Center for Patient Partnerships at the University of Wisconsin, encourages them to spend time in meaningful communication with their patients. “Their argument usually is: I don’t have time.” she says. “My answer is: You don’t have time not to.”
Communication and Patient Safety Concerns
The needs for superb patient safety and optimal healthcare communication are intertwined. In research on quality of care, patient safety is now specifically named as a factor and is distinguished from effectiveness.4 Malpractice litigation is often pursued when patients experience an adverse outcome coupled with a lack of empathy from and a withholding of essential information by physicians.14 Senators Hillary Clinton (D-NY) and Barack Obama (D-IL) cite documentation for this when they advocate for patient safety to be the centerpiece of medical liability reform.
As careful as hospitalists might be to protect their patients from safety hazards and errors, however, they alone cannot protect themselves and their institutions from wrongdoing or the risk of litigation.
“In hospital care, the challenge is to reform corporate governance to make hospital boards take their responsibility for patient safety at least as seriously as they take the hospital’s financial condition,”11 writes Professor Annas, who’s affiliated with both Boston University’s School of Law and School of Medicine. “Hospitals that do not take specific actions to improve safety should be viewed as negligent and be subject to malpractice lawsuits when a violation of the right to safety results in injury.”
It is also the hospital’s obligation, he says, to maintain a safe environment for healthcare providers. And hospitalists and other providers who “live” in hospitals have an ethical obligation to advance the connection of patient safety and communication in hospital-medicine-led quality improvement as well as whole-hospital initiatives.3,11,15,16 That means that staffing, technologies, and facilities must all be up to par so providers can work with the assurance that available resources will support their efforts to provide the best care for their patients.11
Those objectives were taken on by the University of Michigan (Ann Arbor) in a program launched in 2002 to reduce litigation costs, accelerate provision of compensation to patients, and increase the numbers of patients who are compensated for their injuries. The link between the medical liability environment and patient safety was well illustrated in their results. The program involved three strategic components:
- Acknowledge cases in which a patient was hurt because of medical error and compensate these patients quickly and fairly;
- Aggressively defend cases that the hospital considers to be without merit; and
- Study all adverse events to determine how procedures could be improved.
Whereas the organization had approximately 260 claims and lawsuits pending at any given time prior to August 2001, by August 2005 the number had dropped to 114. The average time from the filing of a claim to its resolution was reduced by 11 months, and annual litigation costs dropped from about $3 million to $1 million.14
This program clearly connected the dots between responsibility, compensation for merited negligence, systems quality improvement, and communication across the board. Senators Rodham Clinton and Obama infused their bill with the sensibility that these humane criteria are particularly important.14 When healthcare providers, administrators, and regulators around the world are being advised that a “post-event communication-cum-mediation framework” is the key national strategy for resolving malpractice disputes,3 the need for empathy, apology, and responsibility are implied. (See “I’m Sorry,” June 2006, p.25.)
“When I talk about patient safety, I imagine hospitalists are particularly attuned to this,” says Professor Gaines, “I am talking about what a physician could do in 15 seconds if every single patient is actively engaged in their [own] care.” It’s a no-brainer and “the easiest thing in the world if patients are invited and made to feel welcome as full members of the team.”
Inattention to little things can cause the risky miscommunications that lead to serious problems, both medically and legally. And yet, says Professor Gaines, the remedy is sometimes as easy as “having an informed patient partner as the final check.”
The Bottom Line for Hospitalists
When asked what she wants to say to hospitalists from her personal experience as a hospital inpatient as well as that of her extensive professional background as a criminal defense lawyer, law professor, and patient advocate, Professor Gaines began with her own expression of empathy. “First, in many ways you’re being asked to do an impossible job,” she says. “And patients like me, critics, and commentators will say, ‘Hey! You’re not doing it as well as you could.’ ”
Hospitalists, she says, might be prone to say, “ ‘Leave me alone. I’m doing the best I can.” You’re doing what may be an untenable job, you’ve got specialists leaning on you from one angle, patients and families … wailing on you from another level, and you’re … stuck in between: a utility player, the one everyone loves to boo off the field when you’re having a bad day.”
On the other hand, she says, “Every day I am carving another little bit of my epitaph, and what it says at the end is of my making. And if you can’t carve in these circumstances, then change them or do something about it. But when the bell tolls for thee, the fact that you worked in a busy hospital and had a bunch of overqualified guys breathing down your neck and under-informed patients blaming you for things that aren’t really your fault—that’s going to be footnote material. Carve out your ground, stand it, and do the job you can be proud of. And nobody and nothing gets you off the hook for that.”
Conclusion
The rising costs of medical malpractice litigation are far more a function of the fluctuations of the economy, among other factors, than of the number and size of malpractice claims payouts. Data show that the vast majority of expenditures that go toward litigation are not due to frivolous claims or unmerited compensation. In fact, litigation may hold value in serving to remind hospitals and providers that the best means of warding off lawsuits is to invest resources in patient safety, including prioritizing communication with patients, families, and colleagues. TH
Andrea Sattinger wrote “Risky Business I” in the Feb. 2006 issue (p. 1).
References
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9S.
- Greenwald L, ed. Hospitalists. Perspectives on Clinical Risk Management. Winter 2006.
- Harold TK. Minimizing medical litigation, part 2. J Med Pract Manage. 2006 Mar-Apr;21(5):257-261.
- Brennan TA, Gawande A, Thomas E, et al. Accidental deaths, saved lives, and improved quality. N Engl J Med. 2005 Sep 29;353(13):1405-1409.
- Brennan TA, Mello MM. Patient safety and medical malpractice: a case study. Ann Intern Med. 2003 Aug 19;139(4):267-273.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation N Engl J Med. 1996 Dec 26;335(26):1963-1967.
- Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991 Feb 7;324(6):370-376.
- Harvard Medical Practice Study. Patients, doctors, and lawyers: medical injury, malpractice litigation, and patient compensation in New York. Report of the Harvard Medical Practice Study to the state of New York. Cambridge, Mass: President and Fellows of Harvard College; 1990: www.nysl.nysed.gov/scandoclinks/OCM21331963.htm. Last accessed July 11, 2006.
- Localio AR, Lawthers AG, Brennan TA et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Mills DH, ed. California Medical Association and California Hospital Association Report on the Medical Insurance Feasibility Study. San Francisco, Calif: Sutter Publications; 1977.
- Annas GJ. The patient's right to safety—improving the quality of care through litigation against hospitals. N Engl J Med. 2006 May 11;354(19):2063-2066.
- Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006 May 11;354(19):2024-2033.
- Laine C, Davidoff F, Lewis CE, et al. Important elements of outpatient care: a comparison of patients' and physicians' opinions. Ann Intern Med. 1996 Oct 15;125(8):640-645.
- Clinton HR, Obama B. Making patient safety the centerpiece of medical liability reform. N Engl J Med. 2006;354:2205-2208.
- Studdert DM, Mello MM, Brennan TA. Medical malpractice. N Engl J Med. 2004;350:283-292.
- Delbanco TL. Quality of care through the patient's eyes. BMJ. 1996;313:832-833.
Uncertain Prognosis
They’ve already been in the hospital three or four times, and now they’re back,” says Howard Epstein, MD, an internal medicine-trained hospitalist and the medical director of the palliative care program at Regions Hospital, St. Paul, Minn., describing patients who have acute exacerbations of their life-threatening chronic illnesses. “It’s a challenge we face all the time.”
Hospitalists spend a good deal of their time caring for dying patients, and data show that, by many accounts, they do it well.1 But just how near these patients are to death is often uncertain, especially for patients with diagnoses such as advanced heart and lung failure. Despite their slow decline, during any episode in which they are hospitalized, they may indeed die.
“As hospitalists, we encounter these situations regularly, maybe even daily,” wrote Steve Pantilat, MD, SHM past president, in his column in The Hospitalist (July/August 2005, p. 4): “We are the physicians who care for the seriously ill and the dying. The question is not whether we will take care of these patients; rather, when we do, will we be ready and able?”
End of life and palliative care are areas that hospitalists consider important but feel their training is generally inadequate.2 The conversations with patients and families can be challenging and take time, yet the time is worth the investment and they are a critical part of quality care. “We can learn how to conduct these discussions better,” wrote Dr. Pantilat, “and can practice phrases that will help them go more smoothly.”1,3-14 (See “Practice Phrases,” p. 34.)
Is there a difference in the way hospitalists treat those acute exacerbations if they come from or are attempting to return to their homes in the community or in long-term care? Not really, says Dr. Epstein. The exceptions may be in determining what kind of assistance a patient is getting or not getting outside the hospital (e.g., they’ll return home to a “supercaregiver spouse” versus returning to an assisted or skilled nursing facility). A patient in long-term care usually has multiple comorbidities, or their functional state has declined to the point where they need more assistance, palliative care only, or referral to hospice.
When a patient who has chronic obstructive pulmonary disease (COPD) comes in with an acute exacerbation, he says, it’s a good example of when you need to ask those clarifying questions. “If they’re deteriorating and you can paint that broad picture and help them to see that and that they’re going toward some inexorable decline,” says Dr. Epstein, “then they might make different decisions with that information.”
What’s Good in a Good Death?
Phrases such as “good death” and “dying with dignity” bear some interpretation, says Eva Chittenden, MD, a hospitalist with the University of California at San Francisco and a faculty member of its Palliative Care Leadership Center. Most palliative care experts might further define this to mean dying with appropriate respect for who that person is or who that person has been up until this point. A good death, she says, might better be referred to as a death that is “as good as possible.
“People say they want to die at home, but on the other hand, they also want to live forever,” says Dr. Chittenden. The reality is that most people die in acute-care hospitals while receiving invasive therapies.5-6,15 “We want a peaceful death, we want a pain-free death, we want a death where we’re surrounded by our families,” she says, “but at the same time we want to delay that forever. And those two things come into extreme conflict.7,9
“If you have cancer, maybe you don’t want to talk with your oncologist about death and dying because you want them to save your life. So you don’t even want to go there. And then you’re admitted to the hospital you’re told, ‘You’re extremely sick; you have pneumonia, but if we intubate you, we might be able to turn this situation around versus, if we don’t intubate you, you will surely die.’ And people don’t want to make that decision, because they’re not ready to die, even if ideally they’d want to have that good death,” says Dr. Chittenden, noting that not all providers have come to terms with how to use the available medical technology, when to stop using it, and how to talk about prognosis.
Talking about Prognosis
“In no case of serious illness … is predicting the future straightforward or meaningless,” writes Nicholas Christakis, in Death Foretold: Prophecy and Prognosis in Medical Care.16 “Part of the problem is that even formulating, much less communicating, a prediction about death is unpleasant, so physicians are inclined to refrain from it. But when they are able to formulate a prediction and fail to do so, the quality of care that patients receive may suffer.”
According to Dr. Epstein, you have to practice the conversations. “It’s a skill set, just like doing a bedside procedure … something that you have to do over and over and get comfortable doing,” he explains. “And it shocks people out of their seats when they actually hear the ‘D word.’ ” But part of meeting your responsibility to patients and their families requires speaking the truth.
Dr. Epstein says there are numerous resources available to help hospitalists overcome their discomfort and fears about being incorrect about how long the patient has to live. “I think it is OK to also say, ‘Look, I’m not God and I don't have a crystal ball, but I have seen lots of people in your situation and having watched them go through this point in their life, this is my expert opinion … ,’ ” he advises.
This involves telling the patient, “These are your chances of making a full recovery to the point where you might appreciate the quality of life you would have.” You don’t have to give numbers; you can use words such as good, bad, or poor.
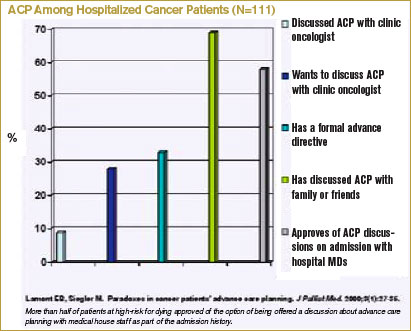
For those with advanced systemic failure, you might discuss prognoses in words that patients can better understand by making a comparison to someone has a cancer diagnosis. For instance, “I’ll say, ‘Your chances for living for a year are about as good as someone living with metastatic lung cancer,’ ” says Dr. Epstein. “I think that’s something that patients grasp a lot easier.”
In addition to the fear of being incorrect in prognosticating, physicians often don’t want their patients to lose hope. “Whereas in truth people are already thinking about these things, and there are studies that show people want their doctors to bring it up,” says Dr. Chittenden.7
A number of these studies were conducted by Dr. Christakis and Elizabeth Lamont, MD, a medical oncologist now practicing at Massachusetts General Hospital Cancer Center and assistant professor of medicine and health care policy at Harvard Medical School.15,17-19 Their findings have shown that doctors’ inaccuracies in their prognoses for terminally ill patients are systematically optimistic and that this may adversely affect the quality of care given to patients near the end of life.17
In their study of 326 patients in five hospices in Chicago, Drs. Christakis and Lamont showed that even if patients with cancer requested survival estimates, doctors would provide a frank estimate only 37% of the time and would provide no estimate, a conscious overestimate, or a conscious underestimate most of the time (63%).18 This, they concluded, may contribute to the observed disparities between physicians’ and patients’ estimates of survival.
Dr. Lamont’s interest in prognosis at end of life and the subject of advanced care planning arose from her experiences as a resident when she was cross-covering the oncology services. “I would be called to see [for example] a 35-year-old woman with widely metastatic breast cancer including brain metastases who was clearly at the end of life,” she says. “She became acutely short of breath, and my concern was that she was having a pulmonary embolism. … I was trying to decide whether to send her to the ICU. I was trying to inform her about the risks of anticoagulation … and I asked, ‘Have you talked about whether or not you’d want to go to the intensive care unit, whether or not you’d want your heart restarted, whether or not you’d want to be put on a ventilator if you couldn’t be breathe on your own; have you talked about these kinds of things with your oncologist?’ [Her answer was,] ‘Oh, no!’ ” Dr. Lamont figured that if she would have these conversations anyway, it would make more sense to have them as part of the admission history and physical. The study she subsequently designed and conducted involved 111 newly admitted patients with cancer whom she interviewed about (among other things) whether they had advanced care preferences (ACP) and whether they had discussed advanced directives with their medical oncologists. Only 9% of patients said that they had advanced directives, although 69% of patients had discussed their ACP with someone else (such as family).19 (See “ACP among Hospitalized Cancer Patients,” below.) However, 58% of patients approved of the option of being offered a discussion about advanced care planning with medical house staff as part of the admission history.
In other words, for the population of patients at high risk for dying during their current hospitalization, more than half would be open to discussing ACP with those whom they do not know well—such as hospitalists.
Advance Care Planning
A study just published in Archives of Internal Medicine suggests that elderly people who suffer from terminal illnesses become increasingly more willing to accept a life-preserving treatment, resulting in further physical disability or more pain if they were already diminished in those domains.20 Terri Fried, MD, an associate professor of internal medicine at Yale, and her colleagues studied 226 older men and women with advanced cancer, congestive heart failure (CHF), or COPD. In the course of in-home interviews conducted over two years, the investigators explored whether the participants would accept life-prolonging treatment if it resulted in one of four diminished health states: mild physical disability, severe physical disability, mental disability, or moderately severe daily pain.
Results showed that the likelihood of a treatment resulting in mild or severe functional disability rating as acceptable increased with each month of participation in the study. More than half of the patients had prepared living wills, and these individuals were more likely to prefer death to disability, but preferences could also change. These findings suggest that even though providers, patients, and families may have already had conversations about advance care planning, a patient’s change in health status might herald the need for a new conversation.
Dr. Lamont says there are two major areas in which hospitalists can politically advocate for changes that could facilitate better advance care planning. The first is to adopt the model proposed in her study, whereby patients are queried regarding advanced directives as part of the admission history.19 Patients for whom this could be added as a new data field would include, for example, those with advanced cancer, metastatic solid tumors, relapsed leukemia, relapsed lymphoma, or with acute exacerbations of illnesses such as CHF or COPD. The second area where hospitalists could advocate for change is national healthcare policy. Like a number of others, Dr. Lamont believes CMS should begin reimbursing for high-quality end-of-life care discussions, the measures of which would be determined at both local and national levels.
Communication Training
“The more hospital medicine training gets incorporated into internal medicine residency,” says Dr. Epstein, “the greater the opportunity to train new hospitalists to have these difficult conversations: how to have a family meeting, to identify the issues, to see if there are any ethical issues involved, any legal issues, and how to negotiate a reasonable plan of care based on the patient’s goals.”2,8,21
In addition to helping with control of physical symptoms, such as pain and nausea control, physicians facilitate decision-making. “We try to address a lot of the existential and reconciliation and legacy issues,” says Dr. Chittenden. Because of the number of situations in which the patient is a woman or man in their 40s or 50s who have young children, she says, “we help the parents come to terms with this and get our child-life specialist involved to help the parents think about how to talk with the kids.”
Because of the growth of the palliative care movement, the training is beginning to improve. “The LCME [Liaison Committee on Medical Education], the licensure group for medical schools, mandates that there be some end-of-life care exposure,” says Dr. Chittenden. “And the ACGME [Accreditation Council for Graduate Medical Education], which licenses the residency programs, strongly suggests that there be opportunities to learn about this. … Slowly but surely we are realizing this needs to happen, but we are far from doing it well.”
What would be ideal? A two-week rotation for residents in a palliative care service? “That would be wonderful,” says Dr. Epstein. “As more palliative care services pop up across the country, the chance of that happening would increase. … And even if you’re not in palliative care and you’re a hospitalist and you do these kinds of things well, the residents should be watching you have those kinds of conversations.”
Explaining that he is paraphrasing Mark Leenay, MD, the former program director at Fairview-University, Minnesota, and the physician who spearheaded the development of a clinical team that comprehensively addresses the multiple aspects of suffering from life-threatening illness, Dr. Epstein says: “I can train anybody to do symptom management in hospice, but how to walk into a room and understand … and negotiate the family dynamics and the patient’s plan of care … to communicate on different levels with different people with … their own agendas, and all the pieces of information … [and different interpretations] … to take it all in and digest it for that meeting and spit it out in a way [in which] everyone can relate and come to some sort of consensus, hopefully, at the end of the meeting? That’s the art. And that takes practice.”
Conclusion
Patients with life-threatening chronic illnesses are often admitted to the hospital multiple times in the course of the period that could be considered the end of life. Important nonmedical issues for hospitalists to address at each new admission include communication regarding prognosis and advance care planning, and addressing existential issues greatly contributes to the quality of care. TH
Resources
- The Hastings Center is involved in bioethics and other issues surrounding end-of-life care (www.thehastingscenter.org/default.asp). The Special Report listed in “References” is downloadable from their Web site.23
- Education in Palliative and End-of-Life Care (EPEC) curriculum (www.epec.net).
- The American Board of Hospice and Palliative Medicine (www.abhpm.org).
- The American Association of Hospice and Palliative Medicine (www.aahpm.org).
- Harvard’s Center for Palliative Care offers courses that emphasize teaching (www.hms.harvard.edu/cdi/pallcare/).
- The Center to Advance Palliative Care (CAPC), Mount Sinai School of Medicine, New York, serves as a resource for hospital-based palliative care program development. CAPC supports six regional Palliative Care Leadership Centers (www.capc.org).
The following Web sites include models for advance directives.
- Five Wishes: www.agingwithdignity.org
- Individual decisions: www.newgrangepress.com
- Respecting choices at end of life: www.gundersenlutheran.com/eolprograms
- Physician orders for life-sustaining treatment: www.polst.org
References
- Auerbach AD, Pantilat SZ. End-of-Life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004 May 15;116(10):669-675.
- Plauth WH, Pantilat SZ, Wachter RM, et al. Hospitalists' perceptions of their residency training needs: result of a national survey. Am J Med. 2001;111(3):247-254.
- Lo B, Quill TE, Tulsky J. Discussing palliative care with patients. ACP--ASIM End-of-Life Care Consensus Panel. American College of Physicians--American Society of Internal Medicine. Ann Intern Med. 1999 May 4;130(9):744-749.
- Quill TE. Initiating end-of-life discussions with seriously ill patients: addressing the "elephant in the room." JAMA. 2000 Nov 15;284(19):2502-2507.
- Kaufman SR. And a Time to Die: How American Hospitals Shape the End of Life. New York: Scribner; 2005.
- Kaufman SR. A commentary: hospital experience and meaning at the end of life. Gerontologist. 2002 Oct;42 Spec No. 3:34-39.
- Pantilat SZ. End-of-life care for the hospitalized patient. Med Clin North Am. 2002 Jul;86(4):749-770.
- Tulsky JA. Beyond advance directives: importance of communication skills at the end of life. JAMA. 2005 Jul 20;294(3):359-365.
- Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. CMAJ. 2006 Feb 28;174(5):627-633.
- Barbato M. Caring for the dying: the doctor as healer. MJAust. 2003 May 19;178(10):508-509.
- Fallowfield LJ, Jenkins VA, Beveridge HA. Truth may hurt but deceit hurts more: communication in palliative care. Palliat Med. 2002 Jul;16(4):297-303.
- Fins JJ, Miller FG, Acres CA, et al. End-of-life decision-making in the hospital: current practice and future prospects. J Pain Symptom Manage. 1999 Jan;17(1):6-15.
- Kalish RA. Death, grief and caring relationships. Belmont, California: Brooks/Cole; 1985.
- Lynn J, Schuster JL, Kabcenell A. Improving Care for the End of Life: A Sourcebook for Health Care Managers and Clinicians. New York: Oxford University Press; 2000.
- Lamont EB. A demographic and prognostic approach to defining the end of life. J Palliat Med. 2005;8 Suppl 1:S12-21.
- Christakis NA. Death Foretold: Prophecy and Prognosis in Medical Care. Chicago: University of Chicago Press; 2001.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors' prognoses in terminally ill patients: prospective cohort study. BMJ. 2000 Feb;320(7233):469-472.
- Lamont EB, Christakis NA. Prognostic disclosure to patients with cancer near the end of life. Ann Intern Med. 2001 Jun 19; 134 (12):1096-1105.
- Lamont EB, Siegler M. Paradoxes in cancer patients' advance care planning. J Palliat Med. 2000 Spring;3(1):27-35.
- Fried TR, Byers AL, Gallo WT, et al. Prospective study of health status preferences and changes in preferences over time in older adults. Arch Intern Med. 2006 Apr 24;166(8):890-895.
- McPhee SJ, Rabow MW, Pantilat SZ, et al. Finding our way--perspectives on care at the close of life. JAMA. 2000 Nov 15;284(19):2512-2513.
- Solie D. How to Say It to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Jennings B, Kaebnick GE, Murray TH. Improving End of Life Care: Why Has It Been So Difficult? Hastings Center Special Report. 2005;35.
They’ve already been in the hospital three or four times, and now they’re back,” says Howard Epstein, MD, an internal medicine-trained hospitalist and the medical director of the palliative care program at Regions Hospital, St. Paul, Minn., describing patients who have acute exacerbations of their life-threatening chronic illnesses. “It’s a challenge we face all the time.”
Hospitalists spend a good deal of their time caring for dying patients, and data show that, by many accounts, they do it well.1 But just how near these patients are to death is often uncertain, especially for patients with diagnoses such as advanced heart and lung failure. Despite their slow decline, during any episode in which they are hospitalized, they may indeed die.
“As hospitalists, we encounter these situations regularly, maybe even daily,” wrote Steve Pantilat, MD, SHM past president, in his column in The Hospitalist (July/August 2005, p. 4): “We are the physicians who care for the seriously ill and the dying. The question is not whether we will take care of these patients; rather, when we do, will we be ready and able?”
End of life and palliative care are areas that hospitalists consider important but feel their training is generally inadequate.2 The conversations with patients and families can be challenging and take time, yet the time is worth the investment and they are a critical part of quality care. “We can learn how to conduct these discussions better,” wrote Dr. Pantilat, “and can practice phrases that will help them go more smoothly.”1,3-14 (See “Practice Phrases,” p. 34.)
Is there a difference in the way hospitalists treat those acute exacerbations if they come from or are attempting to return to their homes in the community or in long-term care? Not really, says Dr. Epstein. The exceptions may be in determining what kind of assistance a patient is getting or not getting outside the hospital (e.g., they’ll return home to a “supercaregiver spouse” versus returning to an assisted or skilled nursing facility). A patient in long-term care usually has multiple comorbidities, or their functional state has declined to the point where they need more assistance, palliative care only, or referral to hospice.
When a patient who has chronic obstructive pulmonary disease (COPD) comes in with an acute exacerbation, he says, it’s a good example of when you need to ask those clarifying questions. “If they’re deteriorating and you can paint that broad picture and help them to see that and that they’re going toward some inexorable decline,” says Dr. Epstein, “then they might make different decisions with that information.”
What’s Good in a Good Death?
Phrases such as “good death” and “dying with dignity” bear some interpretation, says Eva Chittenden, MD, a hospitalist with the University of California at San Francisco and a faculty member of its Palliative Care Leadership Center. Most palliative care experts might further define this to mean dying with appropriate respect for who that person is or who that person has been up until this point. A good death, she says, might better be referred to as a death that is “as good as possible.
“People say they want to die at home, but on the other hand, they also want to live forever,” says Dr. Chittenden. The reality is that most people die in acute-care hospitals while receiving invasive therapies.5-6,15 “We want a peaceful death, we want a pain-free death, we want a death where we’re surrounded by our families,” she says, “but at the same time we want to delay that forever. And those two things come into extreme conflict.7,9
“If you have cancer, maybe you don’t want to talk with your oncologist about death and dying because you want them to save your life. So you don’t even want to go there. And then you’re admitted to the hospital you’re told, ‘You’re extremely sick; you have pneumonia, but if we intubate you, we might be able to turn this situation around versus, if we don’t intubate you, you will surely die.’ And people don’t want to make that decision, because they’re not ready to die, even if ideally they’d want to have that good death,” says Dr. Chittenden, noting that not all providers have come to terms with how to use the available medical technology, when to stop using it, and how to talk about prognosis.
Talking about Prognosis
“In no case of serious illness … is predicting the future straightforward or meaningless,” writes Nicholas Christakis, in Death Foretold: Prophecy and Prognosis in Medical Care.16 “Part of the problem is that even formulating, much less communicating, a prediction about death is unpleasant, so physicians are inclined to refrain from it. But when they are able to formulate a prediction and fail to do so, the quality of care that patients receive may suffer.”
According to Dr. Epstein, you have to practice the conversations. “It’s a skill set, just like doing a bedside procedure … something that you have to do over and over and get comfortable doing,” he explains. “And it shocks people out of their seats when they actually hear the ‘D word.’ ” But part of meeting your responsibility to patients and their families requires speaking the truth.
Dr. Epstein says there are numerous resources available to help hospitalists overcome their discomfort and fears about being incorrect about how long the patient has to live. “I think it is OK to also say, ‘Look, I’m not God and I don't have a crystal ball, but I have seen lots of people in your situation and having watched them go through this point in their life, this is my expert opinion … ,’ ” he advises.
This involves telling the patient, “These are your chances of making a full recovery to the point where you might appreciate the quality of life you would have.” You don’t have to give numbers; you can use words such as good, bad, or poor.
For those with advanced systemic failure, you might discuss prognoses in words that patients can better understand by making a comparison to someone has a cancer diagnosis. For instance, “I’ll say, ‘Your chances for living for a year are about as good as someone living with metastatic lung cancer,’ ” says Dr. Epstein. “I think that’s something that patients grasp a lot easier.”
In addition to the fear of being incorrect in prognosticating, physicians often don’t want their patients to lose hope. “Whereas in truth people are already thinking about these things, and there are studies that show people want their doctors to bring it up,” says Dr. Chittenden.7
A number of these studies were conducted by Dr. Christakis and Elizabeth Lamont, MD, a medical oncologist now practicing at Massachusetts General Hospital Cancer Center and assistant professor of medicine and health care policy at Harvard Medical School.15,17-19 Their findings have shown that doctors’ inaccuracies in their prognoses for terminally ill patients are systematically optimistic and that this may adversely affect the quality of care given to patients near the end of life.17
In their study of 326 patients in five hospices in Chicago, Drs. Christakis and Lamont showed that even if patients with cancer requested survival estimates, doctors would provide a frank estimate only 37% of the time and would provide no estimate, a conscious overestimate, or a conscious underestimate most of the time (63%).18 This, they concluded, may contribute to the observed disparities between physicians’ and patients’ estimates of survival.
Dr. Lamont’s interest in prognosis at end of life and the subject of advanced care planning arose from her experiences as a resident when she was cross-covering the oncology services. “I would be called to see [for example] a 35-year-old woman with widely metastatic breast cancer including brain metastases who was clearly at the end of life,” she says. “She became acutely short of breath, and my concern was that she was having a pulmonary embolism. … I was trying to decide whether to send her to the ICU. I was trying to inform her about the risks of anticoagulation … and I asked, ‘Have you talked about whether or not you’d want to go to the intensive care unit, whether or not you’d want your heart restarted, whether or not you’d want to be put on a ventilator if you couldn’t be breathe on your own; have you talked about these kinds of things with your oncologist?’ [Her answer was,] ‘Oh, no!’ ” Dr. Lamont figured that if she would have these conversations anyway, it would make more sense to have them as part of the admission history and physical. The study she subsequently designed and conducted involved 111 newly admitted patients with cancer whom she interviewed about (among other things) whether they had advanced care preferences (ACP) and whether they had discussed advanced directives with their medical oncologists. Only 9% of patients said that they had advanced directives, although 69% of patients had discussed their ACP with someone else (such as family).19 (See “ACP among Hospitalized Cancer Patients,” below.) However, 58% of patients approved of the option of being offered a discussion about advanced care planning with medical house staff as part of the admission history.
In other words, for the population of patients at high risk for dying during their current hospitalization, more than half would be open to discussing ACP with those whom they do not know well—such as hospitalists.
Advance Care Planning
A study just published in Archives of Internal Medicine suggests that elderly people who suffer from terminal illnesses become increasingly more willing to accept a life-preserving treatment, resulting in further physical disability or more pain if they were already diminished in those domains.20 Terri Fried, MD, an associate professor of internal medicine at Yale, and her colleagues studied 226 older men and women with advanced cancer, congestive heart failure (CHF), or COPD. In the course of in-home interviews conducted over two years, the investigators explored whether the participants would accept life-prolonging treatment if it resulted in one of four diminished health states: mild physical disability, severe physical disability, mental disability, or moderately severe daily pain.
Results showed that the likelihood of a treatment resulting in mild or severe functional disability rating as acceptable increased with each month of participation in the study. More than half of the patients had prepared living wills, and these individuals were more likely to prefer death to disability, but preferences could also change. These findings suggest that even though providers, patients, and families may have already had conversations about advance care planning, a patient’s change in health status might herald the need for a new conversation.
Dr. Lamont says there are two major areas in which hospitalists can politically advocate for changes that could facilitate better advance care planning. The first is to adopt the model proposed in her study, whereby patients are queried regarding advanced directives as part of the admission history.19 Patients for whom this could be added as a new data field would include, for example, those with advanced cancer, metastatic solid tumors, relapsed leukemia, relapsed lymphoma, or with acute exacerbations of illnesses such as CHF or COPD. The second area where hospitalists could advocate for change is national healthcare policy. Like a number of others, Dr. Lamont believes CMS should begin reimbursing for high-quality end-of-life care discussions, the measures of which would be determined at both local and national levels.
Communication Training
“The more hospital medicine training gets incorporated into internal medicine residency,” says Dr. Epstein, “the greater the opportunity to train new hospitalists to have these difficult conversations: how to have a family meeting, to identify the issues, to see if there are any ethical issues involved, any legal issues, and how to negotiate a reasonable plan of care based on the patient’s goals.”2,8,21
In addition to helping with control of physical symptoms, such as pain and nausea control, physicians facilitate decision-making. “We try to address a lot of the existential and reconciliation and legacy issues,” says Dr. Chittenden. Because of the number of situations in which the patient is a woman or man in their 40s or 50s who have young children, she says, “we help the parents come to terms with this and get our child-life specialist involved to help the parents think about how to talk with the kids.”
Because of the growth of the palliative care movement, the training is beginning to improve. “The LCME [Liaison Committee on Medical Education], the licensure group for medical schools, mandates that there be some end-of-life care exposure,” says Dr. Chittenden. “And the ACGME [Accreditation Council for Graduate Medical Education], which licenses the residency programs, strongly suggests that there be opportunities to learn about this. … Slowly but surely we are realizing this needs to happen, but we are far from doing it well.”
What would be ideal? A two-week rotation for residents in a palliative care service? “That would be wonderful,” says Dr. Epstein. “As more palliative care services pop up across the country, the chance of that happening would increase. … And even if you’re not in palliative care and you’re a hospitalist and you do these kinds of things well, the residents should be watching you have those kinds of conversations.”
Explaining that he is paraphrasing Mark Leenay, MD, the former program director at Fairview-University, Minnesota, and the physician who spearheaded the development of a clinical team that comprehensively addresses the multiple aspects of suffering from life-threatening illness, Dr. Epstein says: “I can train anybody to do symptom management in hospice, but how to walk into a room and understand … and negotiate the family dynamics and the patient’s plan of care … to communicate on different levels with different people with … their own agendas, and all the pieces of information … [and different interpretations] … to take it all in and digest it for that meeting and spit it out in a way [in which] everyone can relate and come to some sort of consensus, hopefully, at the end of the meeting? That’s the art. And that takes practice.”
Conclusion
Patients with life-threatening chronic illnesses are often admitted to the hospital multiple times in the course of the period that could be considered the end of life. Important nonmedical issues for hospitalists to address at each new admission include communication regarding prognosis and advance care planning, and addressing existential issues greatly contributes to the quality of care. TH
Resources
- The Hastings Center is involved in bioethics and other issues surrounding end-of-life care (www.thehastingscenter.org/default.asp). The Special Report listed in “References” is downloadable from their Web site.23
- Education in Palliative and End-of-Life Care (EPEC) curriculum (www.epec.net).
- The American Board of Hospice and Palliative Medicine (www.abhpm.org).
- The American Association of Hospice and Palliative Medicine (www.aahpm.org).
- Harvard’s Center for Palliative Care offers courses that emphasize teaching (www.hms.harvard.edu/cdi/pallcare/).
- The Center to Advance Palliative Care (CAPC), Mount Sinai School of Medicine, New York, serves as a resource for hospital-based palliative care program development. CAPC supports six regional Palliative Care Leadership Centers (www.capc.org).
The following Web sites include models for advance directives.
- Five Wishes: www.agingwithdignity.org
- Individual decisions: www.newgrangepress.com
- Respecting choices at end of life: www.gundersenlutheran.com/eolprograms
- Physician orders for life-sustaining treatment: www.polst.org
References
- Auerbach AD, Pantilat SZ. End-of-Life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004 May 15;116(10):669-675.
- Plauth WH, Pantilat SZ, Wachter RM, et al. Hospitalists' perceptions of their residency training needs: result of a national survey. Am J Med. 2001;111(3):247-254.
- Lo B, Quill TE, Tulsky J. Discussing palliative care with patients. ACP--ASIM End-of-Life Care Consensus Panel. American College of Physicians--American Society of Internal Medicine. Ann Intern Med. 1999 May 4;130(9):744-749.
- Quill TE. Initiating end-of-life discussions with seriously ill patients: addressing the "elephant in the room." JAMA. 2000 Nov 15;284(19):2502-2507.
- Kaufman SR. And a Time to Die: How American Hospitals Shape the End of Life. New York: Scribner; 2005.
- Kaufman SR. A commentary: hospital experience and meaning at the end of life. Gerontologist. 2002 Oct;42 Spec No. 3:34-39.
- Pantilat SZ. End-of-life care for the hospitalized patient. Med Clin North Am. 2002 Jul;86(4):749-770.
- Tulsky JA. Beyond advance directives: importance of communication skills at the end of life. JAMA. 2005 Jul 20;294(3):359-365.
- Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. CMAJ. 2006 Feb 28;174(5):627-633.
- Barbato M. Caring for the dying: the doctor as healer. MJAust. 2003 May 19;178(10):508-509.
- Fallowfield LJ, Jenkins VA, Beveridge HA. Truth may hurt but deceit hurts more: communication in palliative care. Palliat Med. 2002 Jul;16(4):297-303.
- Fins JJ, Miller FG, Acres CA, et al. End-of-life decision-making in the hospital: current practice and future prospects. J Pain Symptom Manage. 1999 Jan;17(1):6-15.
- Kalish RA. Death, grief and caring relationships. Belmont, California: Brooks/Cole; 1985.
- Lynn J, Schuster JL, Kabcenell A. Improving Care for the End of Life: A Sourcebook for Health Care Managers and Clinicians. New York: Oxford University Press; 2000.
- Lamont EB. A demographic and prognostic approach to defining the end of life. J Palliat Med. 2005;8 Suppl 1:S12-21.
- Christakis NA. Death Foretold: Prophecy and Prognosis in Medical Care. Chicago: University of Chicago Press; 2001.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors' prognoses in terminally ill patients: prospective cohort study. BMJ. 2000 Feb;320(7233):469-472.
- Lamont EB, Christakis NA. Prognostic disclosure to patients with cancer near the end of life. Ann Intern Med. 2001 Jun 19; 134 (12):1096-1105.
- Lamont EB, Siegler M. Paradoxes in cancer patients' advance care planning. J Palliat Med. 2000 Spring;3(1):27-35.
- Fried TR, Byers AL, Gallo WT, et al. Prospective study of health status preferences and changes in preferences over time in older adults. Arch Intern Med. 2006 Apr 24;166(8):890-895.
- McPhee SJ, Rabow MW, Pantilat SZ, et al. Finding our way--perspectives on care at the close of life. JAMA. 2000 Nov 15;284(19):2512-2513.
- Solie D. How to Say It to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Jennings B, Kaebnick GE, Murray TH. Improving End of Life Care: Why Has It Been So Difficult? Hastings Center Special Report. 2005;35.
They’ve already been in the hospital three or four times, and now they’re back,” says Howard Epstein, MD, an internal medicine-trained hospitalist and the medical director of the palliative care program at Regions Hospital, St. Paul, Minn., describing patients who have acute exacerbations of their life-threatening chronic illnesses. “It’s a challenge we face all the time.”
Hospitalists spend a good deal of their time caring for dying patients, and data show that, by many accounts, they do it well.1 But just how near these patients are to death is often uncertain, especially for patients with diagnoses such as advanced heart and lung failure. Despite their slow decline, during any episode in which they are hospitalized, they may indeed die.
“As hospitalists, we encounter these situations regularly, maybe even daily,” wrote Steve Pantilat, MD, SHM past president, in his column in The Hospitalist (July/August 2005, p. 4): “We are the physicians who care for the seriously ill and the dying. The question is not whether we will take care of these patients; rather, when we do, will we be ready and able?”
End of life and palliative care are areas that hospitalists consider important but feel their training is generally inadequate.2 The conversations with patients and families can be challenging and take time, yet the time is worth the investment and they are a critical part of quality care. “We can learn how to conduct these discussions better,” wrote Dr. Pantilat, “and can practice phrases that will help them go more smoothly.”1,3-14 (See “Practice Phrases,” p. 34.)
Is there a difference in the way hospitalists treat those acute exacerbations if they come from or are attempting to return to their homes in the community or in long-term care? Not really, says Dr. Epstein. The exceptions may be in determining what kind of assistance a patient is getting or not getting outside the hospital (e.g., they’ll return home to a “supercaregiver spouse” versus returning to an assisted or skilled nursing facility). A patient in long-term care usually has multiple comorbidities, or their functional state has declined to the point where they need more assistance, palliative care only, or referral to hospice.
When a patient who has chronic obstructive pulmonary disease (COPD) comes in with an acute exacerbation, he says, it’s a good example of when you need to ask those clarifying questions. “If they’re deteriorating and you can paint that broad picture and help them to see that and that they’re going toward some inexorable decline,” says Dr. Epstein, “then they might make different decisions with that information.”
What’s Good in a Good Death?
Phrases such as “good death” and “dying with dignity” bear some interpretation, says Eva Chittenden, MD, a hospitalist with the University of California at San Francisco and a faculty member of its Palliative Care Leadership Center. Most palliative care experts might further define this to mean dying with appropriate respect for who that person is or who that person has been up until this point. A good death, she says, might better be referred to as a death that is “as good as possible.
“People say they want to die at home, but on the other hand, they also want to live forever,” says Dr. Chittenden. The reality is that most people die in acute-care hospitals while receiving invasive therapies.5-6,15 “We want a peaceful death, we want a pain-free death, we want a death where we’re surrounded by our families,” she says, “but at the same time we want to delay that forever. And those two things come into extreme conflict.7,9
“If you have cancer, maybe you don’t want to talk with your oncologist about death and dying because you want them to save your life. So you don’t even want to go there. And then you’re admitted to the hospital you’re told, ‘You’re extremely sick; you have pneumonia, but if we intubate you, we might be able to turn this situation around versus, if we don’t intubate you, you will surely die.’ And people don’t want to make that decision, because they’re not ready to die, even if ideally they’d want to have that good death,” says Dr. Chittenden, noting that not all providers have come to terms with how to use the available medical technology, when to stop using it, and how to talk about prognosis.
Talking about Prognosis
“In no case of serious illness … is predicting the future straightforward or meaningless,” writes Nicholas Christakis, in Death Foretold: Prophecy and Prognosis in Medical Care.16 “Part of the problem is that even formulating, much less communicating, a prediction about death is unpleasant, so physicians are inclined to refrain from it. But when they are able to formulate a prediction and fail to do so, the quality of care that patients receive may suffer.”
According to Dr. Epstein, you have to practice the conversations. “It’s a skill set, just like doing a bedside procedure … something that you have to do over and over and get comfortable doing,” he explains. “And it shocks people out of their seats when they actually hear the ‘D word.’ ” But part of meeting your responsibility to patients and their families requires speaking the truth.
Dr. Epstein says there are numerous resources available to help hospitalists overcome their discomfort and fears about being incorrect about how long the patient has to live. “I think it is OK to also say, ‘Look, I’m not God and I don't have a crystal ball, but I have seen lots of people in your situation and having watched them go through this point in their life, this is my expert opinion … ,’ ” he advises.
This involves telling the patient, “These are your chances of making a full recovery to the point where you might appreciate the quality of life you would have.” You don’t have to give numbers; you can use words such as good, bad, or poor.
For those with advanced systemic failure, you might discuss prognoses in words that patients can better understand by making a comparison to someone has a cancer diagnosis. For instance, “I’ll say, ‘Your chances for living for a year are about as good as someone living with metastatic lung cancer,’ ” says Dr. Epstein. “I think that’s something that patients grasp a lot easier.”
In addition to the fear of being incorrect in prognosticating, physicians often don’t want their patients to lose hope. “Whereas in truth people are already thinking about these things, and there are studies that show people want their doctors to bring it up,” says Dr. Chittenden.7
A number of these studies were conducted by Dr. Christakis and Elizabeth Lamont, MD, a medical oncologist now practicing at Massachusetts General Hospital Cancer Center and assistant professor of medicine and health care policy at Harvard Medical School.15,17-19 Their findings have shown that doctors’ inaccuracies in their prognoses for terminally ill patients are systematically optimistic and that this may adversely affect the quality of care given to patients near the end of life.17
In their study of 326 patients in five hospices in Chicago, Drs. Christakis and Lamont showed that even if patients with cancer requested survival estimates, doctors would provide a frank estimate only 37% of the time and would provide no estimate, a conscious overestimate, or a conscious underestimate most of the time (63%).18 This, they concluded, may contribute to the observed disparities between physicians’ and patients’ estimates of survival.
Dr. Lamont’s interest in prognosis at end of life and the subject of advanced care planning arose from her experiences as a resident when she was cross-covering the oncology services. “I would be called to see [for example] a 35-year-old woman with widely metastatic breast cancer including brain metastases who was clearly at the end of life,” she says. “She became acutely short of breath, and my concern was that she was having a pulmonary embolism. … I was trying to decide whether to send her to the ICU. I was trying to inform her about the risks of anticoagulation … and I asked, ‘Have you talked about whether or not you’d want to go to the intensive care unit, whether or not you’d want your heart restarted, whether or not you’d want to be put on a ventilator if you couldn’t be breathe on your own; have you talked about these kinds of things with your oncologist?’ [Her answer was,] ‘Oh, no!’ ” Dr. Lamont figured that if she would have these conversations anyway, it would make more sense to have them as part of the admission history and physical. The study she subsequently designed and conducted involved 111 newly admitted patients with cancer whom she interviewed about (among other things) whether they had advanced care preferences (ACP) and whether they had discussed advanced directives with their medical oncologists. Only 9% of patients said that they had advanced directives, although 69% of patients had discussed their ACP with someone else (such as family).19 (See “ACP among Hospitalized Cancer Patients,” below.) However, 58% of patients approved of the option of being offered a discussion about advanced care planning with medical house staff as part of the admission history.
In other words, for the population of patients at high risk for dying during their current hospitalization, more than half would be open to discussing ACP with those whom they do not know well—such as hospitalists.
Advance Care Planning
A study just published in Archives of Internal Medicine suggests that elderly people who suffer from terminal illnesses become increasingly more willing to accept a life-preserving treatment, resulting in further physical disability or more pain if they were already diminished in those domains.20 Terri Fried, MD, an associate professor of internal medicine at Yale, and her colleagues studied 226 older men and women with advanced cancer, congestive heart failure (CHF), or COPD. In the course of in-home interviews conducted over two years, the investigators explored whether the participants would accept life-prolonging treatment if it resulted in one of four diminished health states: mild physical disability, severe physical disability, mental disability, or moderately severe daily pain.
Results showed that the likelihood of a treatment resulting in mild or severe functional disability rating as acceptable increased with each month of participation in the study. More than half of the patients had prepared living wills, and these individuals were more likely to prefer death to disability, but preferences could also change. These findings suggest that even though providers, patients, and families may have already had conversations about advance care planning, a patient’s change in health status might herald the need for a new conversation.
Dr. Lamont says there are two major areas in which hospitalists can politically advocate for changes that could facilitate better advance care planning. The first is to adopt the model proposed in her study, whereby patients are queried regarding advanced directives as part of the admission history.19 Patients for whom this could be added as a new data field would include, for example, those with advanced cancer, metastatic solid tumors, relapsed leukemia, relapsed lymphoma, or with acute exacerbations of illnesses such as CHF or COPD. The second area where hospitalists could advocate for change is national healthcare policy. Like a number of others, Dr. Lamont believes CMS should begin reimbursing for high-quality end-of-life care discussions, the measures of which would be determined at both local and national levels.
Communication Training
“The more hospital medicine training gets incorporated into internal medicine residency,” says Dr. Epstein, “the greater the opportunity to train new hospitalists to have these difficult conversations: how to have a family meeting, to identify the issues, to see if there are any ethical issues involved, any legal issues, and how to negotiate a reasonable plan of care based on the patient’s goals.”2,8,21
In addition to helping with control of physical symptoms, such as pain and nausea control, physicians facilitate decision-making. “We try to address a lot of the existential and reconciliation and legacy issues,” says Dr. Chittenden. Because of the number of situations in which the patient is a woman or man in their 40s or 50s who have young children, she says, “we help the parents come to terms with this and get our child-life specialist involved to help the parents think about how to talk with the kids.”
Because of the growth of the palliative care movement, the training is beginning to improve. “The LCME [Liaison Committee on Medical Education], the licensure group for medical schools, mandates that there be some end-of-life care exposure,” says Dr. Chittenden. “And the ACGME [Accreditation Council for Graduate Medical Education], which licenses the residency programs, strongly suggests that there be opportunities to learn about this. … Slowly but surely we are realizing this needs to happen, but we are far from doing it well.”
What would be ideal? A two-week rotation for residents in a palliative care service? “That would be wonderful,” says Dr. Epstein. “As more palliative care services pop up across the country, the chance of that happening would increase. … And even if you’re not in palliative care and you’re a hospitalist and you do these kinds of things well, the residents should be watching you have those kinds of conversations.”
Explaining that he is paraphrasing Mark Leenay, MD, the former program director at Fairview-University, Minnesota, and the physician who spearheaded the development of a clinical team that comprehensively addresses the multiple aspects of suffering from life-threatening illness, Dr. Epstein says: “I can train anybody to do symptom management in hospice, but how to walk into a room and understand … and negotiate the family dynamics and the patient’s plan of care … to communicate on different levels with different people with … their own agendas, and all the pieces of information … [and different interpretations] … to take it all in and digest it for that meeting and spit it out in a way [in which] everyone can relate and come to some sort of consensus, hopefully, at the end of the meeting? That’s the art. And that takes practice.”
Conclusion
Patients with life-threatening chronic illnesses are often admitted to the hospital multiple times in the course of the period that could be considered the end of life. Important nonmedical issues for hospitalists to address at each new admission include communication regarding prognosis and advance care planning, and addressing existential issues greatly contributes to the quality of care. TH
Resources
- The Hastings Center is involved in bioethics and other issues surrounding end-of-life care (www.thehastingscenter.org/default.asp). The Special Report listed in “References” is downloadable from their Web site.23
- Education in Palliative and End-of-Life Care (EPEC) curriculum (www.epec.net).
- The American Board of Hospice and Palliative Medicine (www.abhpm.org).
- The American Association of Hospice and Palliative Medicine (www.aahpm.org).
- Harvard’s Center for Palliative Care offers courses that emphasize teaching (www.hms.harvard.edu/cdi/pallcare/).
- The Center to Advance Palliative Care (CAPC), Mount Sinai School of Medicine, New York, serves as a resource for hospital-based palliative care program development. CAPC supports six regional Palliative Care Leadership Centers (www.capc.org).
The following Web sites include models for advance directives.
- Five Wishes: www.agingwithdignity.org
- Individual decisions: www.newgrangepress.com
- Respecting choices at end of life: www.gundersenlutheran.com/eolprograms
- Physician orders for life-sustaining treatment: www.polst.org
References
- Auerbach AD, Pantilat SZ. End-of-Life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004 May 15;116(10):669-675.
- Plauth WH, Pantilat SZ, Wachter RM, et al. Hospitalists' perceptions of their residency training needs: result of a national survey. Am J Med. 2001;111(3):247-254.
- Lo B, Quill TE, Tulsky J. Discussing palliative care with patients. ACP--ASIM End-of-Life Care Consensus Panel. American College of Physicians--American Society of Internal Medicine. Ann Intern Med. 1999 May 4;130(9):744-749.
- Quill TE. Initiating end-of-life discussions with seriously ill patients: addressing the "elephant in the room." JAMA. 2000 Nov 15;284(19):2502-2507.
- Kaufman SR. And a Time to Die: How American Hospitals Shape the End of Life. New York: Scribner; 2005.
- Kaufman SR. A commentary: hospital experience and meaning at the end of life. Gerontologist. 2002 Oct;42 Spec No. 3:34-39.
- Pantilat SZ. End-of-life care for the hospitalized patient. Med Clin North Am. 2002 Jul;86(4):749-770.
- Tulsky JA. Beyond advance directives: importance of communication skills at the end of life. JAMA. 2005 Jul 20;294(3):359-365.
- Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. CMAJ. 2006 Feb 28;174(5):627-633.
- Barbato M. Caring for the dying: the doctor as healer. MJAust. 2003 May 19;178(10):508-509.
- Fallowfield LJ, Jenkins VA, Beveridge HA. Truth may hurt but deceit hurts more: communication in palliative care. Palliat Med. 2002 Jul;16(4):297-303.
- Fins JJ, Miller FG, Acres CA, et al. End-of-life decision-making in the hospital: current practice and future prospects. J Pain Symptom Manage. 1999 Jan;17(1):6-15.
- Kalish RA. Death, grief and caring relationships. Belmont, California: Brooks/Cole; 1985.
- Lynn J, Schuster JL, Kabcenell A. Improving Care for the End of Life: A Sourcebook for Health Care Managers and Clinicians. New York: Oxford University Press; 2000.
- Lamont EB. A demographic and prognostic approach to defining the end of life. J Palliat Med. 2005;8 Suppl 1:S12-21.
- Christakis NA. Death Foretold: Prophecy and Prognosis in Medical Care. Chicago: University of Chicago Press; 2001.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors' prognoses in terminally ill patients: prospective cohort study. BMJ. 2000 Feb;320(7233):469-472.
- Lamont EB, Christakis NA. Prognostic disclosure to patients with cancer near the end of life. Ann Intern Med. 2001 Jun 19; 134 (12):1096-1105.
- Lamont EB, Siegler M. Paradoxes in cancer patients' advance care planning. J Palliat Med. 2000 Spring;3(1):27-35.
- Fried TR, Byers AL, Gallo WT, et al. Prospective study of health status preferences and changes in preferences over time in older adults. Arch Intern Med. 2006 Apr 24;166(8):890-895.
- McPhee SJ, Rabow MW, Pantilat SZ, et al. Finding our way--perspectives on care at the close of life. JAMA. 2000 Nov 15;284(19):2512-2513.
- Solie D. How to Say It to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Jennings B, Kaebnick GE, Murray TH. Improving End of Life Care: Why Has It Been So Difficult? Hastings Center Special Report. 2005;35.
Listen Between the Lines
When an elderly person is admitted to the hospital, Adrienne Green, MD, sees an opportunity for something beyond addressing the medical issues at hand.
“One of the key issues that is important for practical, everyday care is trying to figure out how the elderly are not functioning well at home,” says Dr. Green, an associate clinical professor of medicine at the University of California at San Francisco and a member of UCSF’s hospitalist group. “I think we do a great job of managing their diseases, but what we don’t do very well is helping them out with other things [such as coping with] their losses and the fact that they may be just barely hanging on at home in terms of their ability to care for themselves; and this hospitalization may really have set them back.”
Eva Chittenden, MD, an assistant clinical professor of medicine, also at UCSF, agrees. “Many hospitalists are so focused on the hospital that they’re not thinking about the ‘before the hospital’ and the ‘after the hospital,’” she says.
But after identifying the challenges that elderly patients face, communication itself may be challenging. Elderly individuals struggle with issues of control and allowing people to tell them what they need to change in their lives may not be an easy task. What are the best ways to communicate with hospitalized elderly patients to facilitate the best “whole-person” care?

—David Solie, MS, PA
Under the Radar Screen
The hospitalists interviewed for this article agreed that getting a broader picture of an elderly patient’s health and well-being involves discovering how they are really doing at home. Dr. Green asks simple questions, particularly about activities of daily living, such as whether they’re doing their own shopping and cooking. She also involves the family, “because very frequently the patient will say, ‘I’m doing fine,’ and the family member is in the background shaking their head.”
She also looks for clues about whether the patient needs more help at home, whether they are compliant with their medications, and if not, why (e.g., can they open their medicine bottles)?
“I frequently have the elderly patients evaluated for home care just to get someone into their house … ,” says Dr. Green. “I think that probably 80% of our patients who are over 80 who come into the hospital have things in their homes that are not safe, such as throw rugs.” Even if patients are basically doing OK, “if I can get some home care for them, I know we’ll uncover a ton [of things that can be improved],” she says. “These patients may have … kind of snuck under the radar screen of their families and their primary [care physician], and I think the hospitalization kind of opens that up in some ways.”
Facing Resistance
Even if issues are uncovered by means of interviews and home-health visits, however, many elderly patients present a particular communication challenge. This, says David Solie, MS, PA, author of How to Say It to Seniors: Closing the Communication Gap with Our Elders, is because of the difference in circumstances and current experiences between the elderly and their hospitalist providers.1 It is common knowledge that younger people go through stages of development, but the elderly do, too, says Solie, who is medical director and CEO of Second Opinion Insurance Services in Woodland Hills, Calif., a brokerage that specializes in the insurance needs of impaired-risk, elderly individuals.
The last human developmental stage compels elderly adults to work hard at maintaining control over their lives in the face of almost daily losses. A big part of the losses they experience involve their health and functioning, and the ways different patients cope with loss and the perceived stresses of healthcare have been analyzed and categorized.2-5
But in addition to loss of control, the elderly also face the daunting task of discovering what their legacy will be—what will live on after they die. “The way our elders communicate contains clues to the urgency they feel in trying to resolve these items on their agendas,” writes Solie. “In almost every conversation with older adults, control and legacy issues rise to the surface.”
A Matter of Loss
By the time a person is old (over 70) or old-old (over 85) their losses may have manifested in many areas: They’ve lost:
- Parents;
- Other relatives—perhaps including children;
- Friends;
- Places of residence (both homes and the familiarity of cities or towns);
- Possessions;
- Other relationships (sometimes other healthcare providers);
- Careers;
- Consultative authority (“ours is not a culture that values the wisdom of our elders,” writes Solie);
- Identity;
- Financial independence;
- Habits and pleasures;
- Physical space (the room at their son or daughter’s or in assisted living or the nursing home can’t compare to the homes, gardens, and expanses of view they may have had as younger people), and, of course; and
- Physical and mental capacities.
Sometimes the losses elders sustain occur in rapid-fire sequence, with little or no recovery time in between.1,6
It is no wonder that older adults, in one way or another, exhibit what we consider resistance to their changing lives. In terms of a hospitalization, this may mean saying “no” to medications, individual providers, tests, surgery, home-health visits, or something as small as being talked to or touched in what they perceive as a disturbing, overly familiar, or mechanized manner.
“Many patients are resistant to having people come into their homes and help them, and at the same time they are resistant to going to a skilled nursing care facility,” says Dr. Green, “and it has to do with their [feelings of the] loss of independence and control over their lives.”
“It’s very easy if you’re in medicine to normalize your context of the hospital,” says Solie. “In other words, the hospital seems familiar to you and you’re very comfortable moving around there, and mainly because you’re in control. You’re the doctor … and you move in the hospital in order to make things happen and you never feel all that threatened. But when you bring an older person who already has a heightened sensitivity toward losing control into the hospital—this complex, technological world of medicine—and they have the cumulative disadvantage of being sick,” says Solie, “it’s really important to remember that there will probably be no other state that they’ll be in, except maybe nursing home care, where they will feel so out of control.”
A good first step in communicating with older patients is to quickly develop a rapport with them and show them you recognize what they’re up against.7 “They really want to know whether or not I get it,” says Solie.
The way you communicate that you get it, he says, is fairly straightforward: When I’m first interacting with the patient, I say, “if you are like my [other] elderly patients … I’m sure you’re feeling a lot of anxiety over [not having much] control and, first of all, I want to assure you that I’m going to make sure you understand the choices and help you make all the decisions. And … I’m definitely going to … put everything in a language that you understand. But if I’m not successful, I’m going to employ someone from your family. We’re going to work together. Even though you’re hospitalized and even though you’re fighting this illness (or whatever the condition might be), you still [have] the right to make choices, and my goal is to partner with you. My expertise is medicine, but you have an expertise in your life.”
In other words, you are signaling that you recognize that control is the issue. Acknowledge the loss, ask about the value of the event or decision to the patient, ask what you can do to help them deal with their feelings or make up their minds. It also allows you to remind an older patient’s children that control is a big and normal concern for their mother or father.

—Eva Chittenden, MD
Hospitalists at a Different Time and Place
The elderly desperately need people who can serve them as natural healers, who are not constantly in a hurry, and who care what they are thinking and feeling. How can hospitalists relate to those who are in the midst of life review and who are hanging on to an escaping control? How can they serve their patients in a way that meets all needs?
Fighting—with denial or ignorance—the resistance that patients might put up will more than likely provoke them. A fight for control can undermine and sabotage the best intentions of the provider and the greatest wishes for the patient to experience comfort or regain health and well-being. Rather than justifying wresting control from elderly patients because it’s for their own good, advises Solie, what we must do instead is to “step back, hand them the control baton, and allow them to run with it.”1
A person’s admission to the hospital “might be such a huge crisis for them, whereas for us it’s our routine work,” says Dr. Chittenden, who practices as a hospitalist and also works on her institution’s inpatient palliative care service. “And many people who are hospitalists—who are even in their late 20s, 30s, 40s—have been totally healthy their whole life, so it is hard to relate to what it’s like to be older and to be losing function, losing friends who are also dying, losing their house … . I think that it can be very helpful for the hospitalist to take a little more time and explore some of those issues [of loss and legacy]. I try to meet the person where they’re at and try to understand what their goals, needs, ... and fears are [as well as] their functional status.”
Allowing older patients to engage with you about their lives and their pasts is a privilege for any healthcare provider. Engaging with them in a way that will help facilitate their loosening the reins on control may expedite and allow greater quality into their healthcare. It may provide an opening whereby you can order that home-health visit with less struggle.
Create Openings
“There are a lot of different ‘on-ramps’ to asking the life-review questions, which are extremely comforting,” says Solie. “For example, you might say, ‘Mary, I notice that you were born in Iowa. You know, my family on my father’s side came from Iowa. Where were you raised?’ And ‘Do you have a big family on your farm, because my aunt had cows.’”
Once you get a response that engages the patient, then you “are in the slipstream. Physicians have such a high experience curve, they see so many patients,” he says. “They don’t have to go very far into their inventory of experiences [to find one] that essentially matches up with that patient.”
Any kind of comment that will key you in to their background experience can help establish some kind of foundation for relationship. Another example: “You know, Mary, I was working with this woman who was about your age and she was raised in the Midwest and was dealing with some of these issues of congestive heart failure, and one of her big concerns was something that I didn’t appreciate until I understood what an impact it was having on her life.”
This kind of communication, says Solie, can help to relieve some of the patient’s control anxieties, “because she feels that if I ‘get it,’ she’s open to what I have to say, such as, ‘The first thing, we have to deal with is there is too much fluid going on in your body and it’s putting a big strain on your heart, so the first couple days all we did for that [other] woman was try to pull some fluid off and keep everything in balance.’”
You’ve communicated that you have a plan, that you can be trusted, and that you will help her to exercise as much control as possible. Creating and accessing those openings is also “the ideal way to weave the family into this whole life-review process, which is where the patient lives, psychologically and emotionally, when outside the hospital environment,” he says. “We become so myopic when we’re caught in the hospital environment that the world becomes a narrow tunnel and we forget the greater matrix outside that we’re all connected to.”
The Boon of Biology
Whereas the physiology and anatomy of humans deteriorate with time, some of the changes in mental processes in old age may actually enhance the ability to reflect and make informed judgments. Solie’s view is that what younger people may view as slow behavior, confusing speech patterns, and physical frailty don’t hinder the tasks that are before the elderly. On the contrary, they assist the fulfillment of their developmental agendas to feel in control when they’re losing control and to let go enough to reveal the legacy that will survive after they go.
Research on the aging brain indicates that changes in brain chemistry facilitate the life-review process.1,6 In general, reflection is the normal mode of existence for elderly adults and their primary focus. Thus, viewing them as diminished because they communicate differently than younger people do is doing them a disservice.
Those slowed mental processes, Dr. Chittenden concurs, “are conducive to reflection. Someone younger will pathologize it. … I agree that we don’t value the slowing down process, but I also think that when this population is in the hospital we are tending to look at loss of functional status or the quick mental traits that we value as opposed to [that which is] adaptive [and] that enables them to look at things differently and reflect.”
The key to connecting the dots of where they are and where they need to be (both medically and psychosocially), as well as how they occur to their providers and their families as opposed to how they occur to themselves, is to listen to and speak with them by making use of what you know about this stage of their life as it affects their communication. You can do this, says Solie, by invoking the “access code,” which is “to clearly understand that at the top of their agenda—no matter what else is happening—is the need for control and the need to develop and go after a legacy, and that means life review. If you know that, you will never lose your reference point with them.”
Communication Habits of the Elderly
Solie identifies some verbal behaviors that are common in older people. In many cases these behaviors may reveal something between the lines.
- Lack of urgency. Older people need more time to decide things. Accept that slower pace as normal. Don’t take it personally. Adjust your schedule to allow time to deliver news or ask for choices and then allow time for them to discuss with their families or contemplate on their own; return to them at a later time. Become expert at spontaneous facilitation. Use your access code to get their attention and gain their trust.
- Nonlinear conversations. Although older patients may appear to wander off topic, they may do so in the urge to ground themselves in what their priorities are, what their feelings are, what their choices will be. Signal you’re willing to listen and that you’re tuned in to the content, even if you don’t know where it is leading. (Obviously, someone who is demented or delirious presents a different scenario altogether, and depression is common and frequently overlooked.) Listen for patterns and themes. Nonlinear conversations can lead to spontaneous revelations and great insights for your patients and for yourself and can help patients revisit life dramas that test and clarify values. This, too, is a part of healthcare.
- Repetition and attention to details. In situations when dementia is ruled out, a patient’s repetition may indicate a means to emphasize an important point or value. Keep in mind, too, that as we age, we all repeat stories to some degree. Details in stories may be the means by which older adults connect to their pasts and may also serve as clues to what is important to these people. Don’t assume details demand any action on your part. You are only being asked to listen as the older person sorts things out.
- Uncoupling. Solie describes uncoupling as any time an older person appears to disconnect from you in the course of a conversation. For a professional, this can feel as if you are dismissed or ignored just when you think you’ve hit the mark with a comment or question. Go back and assess the information you’ve gathered by doing some verification. Rethink the objective: Any action that works against their maintaining control and discovering a legacy will produce uncoupling.
“I try to be aware of when I’m losing people,” says Dr. Chittenden of this phenomenon. “I would say, ‘I seem to be losing you and I’m wondering what you’re thinking right now.’ I would try to find out where they’re at and if it was something I said that didn’t gel with them, didn’t make sense to them, or wasn’t their priority.” This is something, she emphasizes, that a hospitalist needs to watch for with patients of all ages. “Whether you’re older or younger,” she says, the communication can be complicated because “you’re … in the hospital culture and the priorities of doctors are so often different from the priorities of patients.”
Conclusion
Older and especially old-old individuals in some ways live in an era other than the one traversed by the young and middle-aged.6 Their purposes, agendas, and mission are different and the slowing down of their functioning can facilitate their attempts to put their lives into perspective and manage what control they can still exercise or are still allowed. Viewing older patients with the utmost respect and acknowledging the challenges they face at these last phases of their lives can better help you to partner with them and their families in their care. TH
Andrea Sattinger also writes about the importance of apology in this issue.
References
- Solie D. How to Say it to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Chochinov HM, Cann BJ. Interventions to enhance the spiritual aspects of dying. J Palliat Med. 2005;8:Suppl 1:S103-115.
- Dennis KE. Patients' control and the information imperative: clarification and confirmation. Nurs Res. 1990;39(3):162-166.
- Kiesler DJ, Auerbach SM. Integrating measurement of control and affiliation in studies of physician-patient interaction: the interpersonal circumplex. Soc Sci Med. 2003;57(9):1707-1722.
- Breemhaar B, Visser AP, Kleijnen JG. Perceptions and behaviour among elderly hospital patients: description and explanation of age differences in satisfaction, knowledge, emotions and behaviour. Soc Sci Med. 1990;31(12):1377-1385.
- Pipher M. Another Country: Navigating the Emotional Terrain of Our Elders. New York: Riverhead Books; 1999.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
When an elderly person is admitted to the hospital, Adrienne Green, MD, sees an opportunity for something beyond addressing the medical issues at hand.
“One of the key issues that is important for practical, everyday care is trying to figure out how the elderly are not functioning well at home,” says Dr. Green, an associate clinical professor of medicine at the University of California at San Francisco and a member of UCSF’s hospitalist group. “I think we do a great job of managing their diseases, but what we don’t do very well is helping them out with other things [such as coping with] their losses and the fact that they may be just barely hanging on at home in terms of their ability to care for themselves; and this hospitalization may really have set them back.”
Eva Chittenden, MD, an assistant clinical professor of medicine, also at UCSF, agrees. “Many hospitalists are so focused on the hospital that they’re not thinking about the ‘before the hospital’ and the ‘after the hospital,’” she says.
But after identifying the challenges that elderly patients face, communication itself may be challenging. Elderly individuals struggle with issues of control and allowing people to tell them what they need to change in their lives may not be an easy task. What are the best ways to communicate with hospitalized elderly patients to facilitate the best “whole-person” care?
—David Solie, MS, PA
Under the Radar Screen
The hospitalists interviewed for this article agreed that getting a broader picture of an elderly patient’s health and well-being involves discovering how they are really doing at home. Dr. Green asks simple questions, particularly about activities of daily living, such as whether they’re doing their own shopping and cooking. She also involves the family, “because very frequently the patient will say, ‘I’m doing fine,’ and the family member is in the background shaking their head.”
She also looks for clues about whether the patient needs more help at home, whether they are compliant with their medications, and if not, why (e.g., can they open their medicine bottles)?
“I frequently have the elderly patients evaluated for home care just to get someone into their house … ,” says Dr. Green. “I think that probably 80% of our patients who are over 80 who come into the hospital have things in their homes that are not safe, such as throw rugs.” Even if patients are basically doing OK, “if I can get some home care for them, I know we’ll uncover a ton [of things that can be improved],” she says. “These patients may have … kind of snuck under the radar screen of their families and their primary [care physician], and I think the hospitalization kind of opens that up in some ways.”
Facing Resistance
Even if issues are uncovered by means of interviews and home-health visits, however, many elderly patients present a particular communication challenge. This, says David Solie, MS, PA, author of How to Say It to Seniors: Closing the Communication Gap with Our Elders, is because of the difference in circumstances and current experiences between the elderly and their hospitalist providers.1 It is common knowledge that younger people go through stages of development, but the elderly do, too, says Solie, who is medical director and CEO of Second Opinion Insurance Services in Woodland Hills, Calif., a brokerage that specializes in the insurance needs of impaired-risk, elderly individuals.
The last human developmental stage compels elderly adults to work hard at maintaining control over their lives in the face of almost daily losses. A big part of the losses they experience involve their health and functioning, and the ways different patients cope with loss and the perceived stresses of healthcare have been analyzed and categorized.2-5
But in addition to loss of control, the elderly also face the daunting task of discovering what their legacy will be—what will live on after they die. “The way our elders communicate contains clues to the urgency they feel in trying to resolve these items on their agendas,” writes Solie. “In almost every conversation with older adults, control and legacy issues rise to the surface.”
A Matter of Loss
By the time a person is old (over 70) or old-old (over 85) their losses may have manifested in many areas: They’ve lost:
- Parents;
- Other relatives—perhaps including children;
- Friends;
- Places of residence (both homes and the familiarity of cities or towns);
- Possessions;
- Other relationships (sometimes other healthcare providers);
- Careers;
- Consultative authority (“ours is not a culture that values the wisdom of our elders,” writes Solie);
- Identity;
- Financial independence;
- Habits and pleasures;
- Physical space (the room at their son or daughter’s or in assisted living or the nursing home can’t compare to the homes, gardens, and expanses of view they may have had as younger people), and, of course; and
- Physical and mental capacities.
Sometimes the losses elders sustain occur in rapid-fire sequence, with little or no recovery time in between.1,6
It is no wonder that older adults, in one way or another, exhibit what we consider resistance to their changing lives. In terms of a hospitalization, this may mean saying “no” to medications, individual providers, tests, surgery, home-health visits, or something as small as being talked to or touched in what they perceive as a disturbing, overly familiar, or mechanized manner.
“Many patients are resistant to having people come into their homes and help them, and at the same time they are resistant to going to a skilled nursing care facility,” says Dr. Green, “and it has to do with their [feelings of the] loss of independence and control over their lives.”
“It’s very easy if you’re in medicine to normalize your context of the hospital,” says Solie. “In other words, the hospital seems familiar to you and you’re very comfortable moving around there, and mainly because you’re in control. You’re the doctor … and you move in the hospital in order to make things happen and you never feel all that threatened. But when you bring an older person who already has a heightened sensitivity toward losing control into the hospital—this complex, technological world of medicine—and they have the cumulative disadvantage of being sick,” says Solie, “it’s really important to remember that there will probably be no other state that they’ll be in, except maybe nursing home care, where they will feel so out of control.”
A good first step in communicating with older patients is to quickly develop a rapport with them and show them you recognize what they’re up against.7 “They really want to know whether or not I get it,” says Solie.
The way you communicate that you get it, he says, is fairly straightforward: When I’m first interacting with the patient, I say, “if you are like my [other] elderly patients … I’m sure you’re feeling a lot of anxiety over [not having much] control and, first of all, I want to assure you that I’m going to make sure you understand the choices and help you make all the decisions. And … I’m definitely going to … put everything in a language that you understand. But if I’m not successful, I’m going to employ someone from your family. We’re going to work together. Even though you’re hospitalized and even though you’re fighting this illness (or whatever the condition might be), you still [have] the right to make choices, and my goal is to partner with you. My expertise is medicine, but you have an expertise in your life.”
In other words, you are signaling that you recognize that control is the issue. Acknowledge the loss, ask about the value of the event or decision to the patient, ask what you can do to help them deal with their feelings or make up their minds. It also allows you to remind an older patient’s children that control is a big and normal concern for their mother or father.
—Eva Chittenden, MD
Hospitalists at a Different Time and Place
The elderly desperately need people who can serve them as natural healers, who are not constantly in a hurry, and who care what they are thinking and feeling. How can hospitalists relate to those who are in the midst of life review and who are hanging on to an escaping control? How can they serve their patients in a way that meets all needs?
Fighting—with denial or ignorance—the resistance that patients might put up will more than likely provoke them. A fight for control can undermine and sabotage the best intentions of the provider and the greatest wishes for the patient to experience comfort or regain health and well-being. Rather than justifying wresting control from elderly patients because it’s for their own good, advises Solie, what we must do instead is to “step back, hand them the control baton, and allow them to run with it.”1
A person’s admission to the hospital “might be such a huge crisis for them, whereas for us it’s our routine work,” says Dr. Chittenden, who practices as a hospitalist and also works on her institution’s inpatient palliative care service. “And many people who are hospitalists—who are even in their late 20s, 30s, 40s—have been totally healthy their whole life, so it is hard to relate to what it’s like to be older and to be losing function, losing friends who are also dying, losing their house … . I think that it can be very helpful for the hospitalist to take a little more time and explore some of those issues [of loss and legacy]. I try to meet the person where they’re at and try to understand what their goals, needs, ... and fears are [as well as] their functional status.”
Allowing older patients to engage with you about their lives and their pasts is a privilege for any healthcare provider. Engaging with them in a way that will help facilitate their loosening the reins on control may expedite and allow greater quality into their healthcare. It may provide an opening whereby you can order that home-health visit with less struggle.
Create Openings
“There are a lot of different ‘on-ramps’ to asking the life-review questions, which are extremely comforting,” says Solie. “For example, you might say, ‘Mary, I notice that you were born in Iowa. You know, my family on my father’s side came from Iowa. Where were you raised?’ And ‘Do you have a big family on your farm, because my aunt had cows.’”
Once you get a response that engages the patient, then you “are in the slipstream. Physicians have such a high experience curve, they see so many patients,” he says. “They don’t have to go very far into their inventory of experiences [to find one] that essentially matches up with that patient.”
Any kind of comment that will key you in to their background experience can help establish some kind of foundation for relationship. Another example: “You know, Mary, I was working with this woman who was about your age and she was raised in the Midwest and was dealing with some of these issues of congestive heart failure, and one of her big concerns was something that I didn’t appreciate until I understood what an impact it was having on her life.”
This kind of communication, says Solie, can help to relieve some of the patient’s control anxieties, “because she feels that if I ‘get it,’ she’s open to what I have to say, such as, ‘The first thing, we have to deal with is there is too much fluid going on in your body and it’s putting a big strain on your heart, so the first couple days all we did for that [other] woman was try to pull some fluid off and keep everything in balance.’”
You’ve communicated that you have a plan, that you can be trusted, and that you will help her to exercise as much control as possible. Creating and accessing those openings is also “the ideal way to weave the family into this whole life-review process, which is where the patient lives, psychologically and emotionally, when outside the hospital environment,” he says. “We become so myopic when we’re caught in the hospital environment that the world becomes a narrow tunnel and we forget the greater matrix outside that we’re all connected to.”
The Boon of Biology
Whereas the physiology and anatomy of humans deteriorate with time, some of the changes in mental processes in old age may actually enhance the ability to reflect and make informed judgments. Solie’s view is that what younger people may view as slow behavior, confusing speech patterns, and physical frailty don’t hinder the tasks that are before the elderly. On the contrary, they assist the fulfillment of their developmental agendas to feel in control when they’re losing control and to let go enough to reveal the legacy that will survive after they go.
Research on the aging brain indicates that changes in brain chemistry facilitate the life-review process.1,6 In general, reflection is the normal mode of existence for elderly adults and their primary focus. Thus, viewing them as diminished because they communicate differently than younger people do is doing them a disservice.
Those slowed mental processes, Dr. Chittenden concurs, “are conducive to reflection. Someone younger will pathologize it. … I agree that we don’t value the slowing down process, but I also think that when this population is in the hospital we are tending to look at loss of functional status or the quick mental traits that we value as opposed to [that which is] adaptive [and] that enables them to look at things differently and reflect.”
The key to connecting the dots of where they are and where they need to be (both medically and psychosocially), as well as how they occur to their providers and their families as opposed to how they occur to themselves, is to listen to and speak with them by making use of what you know about this stage of their life as it affects their communication. You can do this, says Solie, by invoking the “access code,” which is “to clearly understand that at the top of their agenda—no matter what else is happening—is the need for control and the need to develop and go after a legacy, and that means life review. If you know that, you will never lose your reference point with them.”
Communication Habits of the Elderly
Solie identifies some verbal behaviors that are common in older people. In many cases these behaviors may reveal something between the lines.
- Lack of urgency. Older people need more time to decide things. Accept that slower pace as normal. Don’t take it personally. Adjust your schedule to allow time to deliver news or ask for choices and then allow time for them to discuss with their families or contemplate on their own; return to them at a later time. Become expert at spontaneous facilitation. Use your access code to get their attention and gain their trust.
- Nonlinear conversations. Although older patients may appear to wander off topic, they may do so in the urge to ground themselves in what their priorities are, what their feelings are, what their choices will be. Signal you’re willing to listen and that you’re tuned in to the content, even if you don’t know where it is leading. (Obviously, someone who is demented or delirious presents a different scenario altogether, and depression is common and frequently overlooked.) Listen for patterns and themes. Nonlinear conversations can lead to spontaneous revelations and great insights for your patients and for yourself and can help patients revisit life dramas that test and clarify values. This, too, is a part of healthcare.
- Repetition and attention to details. In situations when dementia is ruled out, a patient’s repetition may indicate a means to emphasize an important point or value. Keep in mind, too, that as we age, we all repeat stories to some degree. Details in stories may be the means by which older adults connect to their pasts and may also serve as clues to what is important to these people. Don’t assume details demand any action on your part. You are only being asked to listen as the older person sorts things out.
- Uncoupling. Solie describes uncoupling as any time an older person appears to disconnect from you in the course of a conversation. For a professional, this can feel as if you are dismissed or ignored just when you think you’ve hit the mark with a comment or question. Go back and assess the information you’ve gathered by doing some verification. Rethink the objective: Any action that works against their maintaining control and discovering a legacy will produce uncoupling.
“I try to be aware of when I’m losing people,” says Dr. Chittenden of this phenomenon. “I would say, ‘I seem to be losing you and I’m wondering what you’re thinking right now.’ I would try to find out where they’re at and if it was something I said that didn’t gel with them, didn’t make sense to them, or wasn’t their priority.” This is something, she emphasizes, that a hospitalist needs to watch for with patients of all ages. “Whether you’re older or younger,” she says, the communication can be complicated because “you’re … in the hospital culture and the priorities of doctors are so often different from the priorities of patients.”
Conclusion
Older and especially old-old individuals in some ways live in an era other than the one traversed by the young and middle-aged.6 Their purposes, agendas, and mission are different and the slowing down of their functioning can facilitate their attempts to put their lives into perspective and manage what control they can still exercise or are still allowed. Viewing older patients with the utmost respect and acknowledging the challenges they face at these last phases of their lives can better help you to partner with them and their families in their care. TH
Andrea Sattinger also writes about the importance of apology in this issue.
References
- Solie D. How to Say it to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Chochinov HM, Cann BJ. Interventions to enhance the spiritual aspects of dying. J Palliat Med. 2005;8:Suppl 1:S103-115.
- Dennis KE. Patients' control and the information imperative: clarification and confirmation. Nurs Res. 1990;39(3):162-166.
- Kiesler DJ, Auerbach SM. Integrating measurement of control and affiliation in studies of physician-patient interaction: the interpersonal circumplex. Soc Sci Med. 2003;57(9):1707-1722.
- Breemhaar B, Visser AP, Kleijnen JG. Perceptions and behaviour among elderly hospital patients: description and explanation of age differences in satisfaction, knowledge, emotions and behaviour. Soc Sci Med. 1990;31(12):1377-1385.
- Pipher M. Another Country: Navigating the Emotional Terrain of Our Elders. New York: Riverhead Books; 1999.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
When an elderly person is admitted to the hospital, Adrienne Green, MD, sees an opportunity for something beyond addressing the medical issues at hand.
“One of the key issues that is important for practical, everyday care is trying to figure out how the elderly are not functioning well at home,” says Dr. Green, an associate clinical professor of medicine at the University of California at San Francisco and a member of UCSF’s hospitalist group. “I think we do a great job of managing their diseases, but what we don’t do very well is helping them out with other things [such as coping with] their losses and the fact that they may be just barely hanging on at home in terms of their ability to care for themselves; and this hospitalization may really have set them back.”
Eva Chittenden, MD, an assistant clinical professor of medicine, also at UCSF, agrees. “Many hospitalists are so focused on the hospital that they’re not thinking about the ‘before the hospital’ and the ‘after the hospital,’” she says.
But after identifying the challenges that elderly patients face, communication itself may be challenging. Elderly individuals struggle with issues of control and allowing people to tell them what they need to change in their lives may not be an easy task. What are the best ways to communicate with hospitalized elderly patients to facilitate the best “whole-person” care?
—David Solie, MS, PA
Under the Radar Screen
The hospitalists interviewed for this article agreed that getting a broader picture of an elderly patient’s health and well-being involves discovering how they are really doing at home. Dr. Green asks simple questions, particularly about activities of daily living, such as whether they’re doing their own shopping and cooking. She also involves the family, “because very frequently the patient will say, ‘I’m doing fine,’ and the family member is in the background shaking their head.”
She also looks for clues about whether the patient needs more help at home, whether they are compliant with their medications, and if not, why (e.g., can they open their medicine bottles)?
“I frequently have the elderly patients evaluated for home care just to get someone into their house … ,” says Dr. Green. “I think that probably 80% of our patients who are over 80 who come into the hospital have things in their homes that are not safe, such as throw rugs.” Even if patients are basically doing OK, “if I can get some home care for them, I know we’ll uncover a ton [of things that can be improved],” she says. “These patients may have … kind of snuck under the radar screen of their families and their primary [care physician], and I think the hospitalization kind of opens that up in some ways.”
Facing Resistance
Even if issues are uncovered by means of interviews and home-health visits, however, many elderly patients present a particular communication challenge. This, says David Solie, MS, PA, author of How to Say It to Seniors: Closing the Communication Gap with Our Elders, is because of the difference in circumstances and current experiences between the elderly and their hospitalist providers.1 It is common knowledge that younger people go through stages of development, but the elderly do, too, says Solie, who is medical director and CEO of Second Opinion Insurance Services in Woodland Hills, Calif., a brokerage that specializes in the insurance needs of impaired-risk, elderly individuals.
The last human developmental stage compels elderly adults to work hard at maintaining control over their lives in the face of almost daily losses. A big part of the losses they experience involve their health and functioning, and the ways different patients cope with loss and the perceived stresses of healthcare have been analyzed and categorized.2-5
But in addition to loss of control, the elderly also face the daunting task of discovering what their legacy will be—what will live on after they die. “The way our elders communicate contains clues to the urgency they feel in trying to resolve these items on their agendas,” writes Solie. “In almost every conversation with older adults, control and legacy issues rise to the surface.”
A Matter of Loss
By the time a person is old (over 70) or old-old (over 85) their losses may have manifested in many areas: They’ve lost:
- Parents;
- Other relatives—perhaps including children;
- Friends;
- Places of residence (both homes and the familiarity of cities or towns);
- Possessions;
- Other relationships (sometimes other healthcare providers);
- Careers;
- Consultative authority (“ours is not a culture that values the wisdom of our elders,” writes Solie);
- Identity;
- Financial independence;
- Habits and pleasures;
- Physical space (the room at their son or daughter’s or in assisted living or the nursing home can’t compare to the homes, gardens, and expanses of view they may have had as younger people), and, of course; and
- Physical and mental capacities.
Sometimes the losses elders sustain occur in rapid-fire sequence, with little or no recovery time in between.1,6
It is no wonder that older adults, in one way or another, exhibit what we consider resistance to their changing lives. In terms of a hospitalization, this may mean saying “no” to medications, individual providers, tests, surgery, home-health visits, or something as small as being talked to or touched in what they perceive as a disturbing, overly familiar, or mechanized manner.
“Many patients are resistant to having people come into their homes and help them, and at the same time they are resistant to going to a skilled nursing care facility,” says Dr. Green, “and it has to do with their [feelings of the] loss of independence and control over their lives.”
“It’s very easy if you’re in medicine to normalize your context of the hospital,” says Solie. “In other words, the hospital seems familiar to you and you’re very comfortable moving around there, and mainly because you’re in control. You’re the doctor … and you move in the hospital in order to make things happen and you never feel all that threatened. But when you bring an older person who already has a heightened sensitivity toward losing control into the hospital—this complex, technological world of medicine—and they have the cumulative disadvantage of being sick,” says Solie, “it’s really important to remember that there will probably be no other state that they’ll be in, except maybe nursing home care, where they will feel so out of control.”
A good first step in communicating with older patients is to quickly develop a rapport with them and show them you recognize what they’re up against.7 “They really want to know whether or not I get it,” says Solie.
The way you communicate that you get it, he says, is fairly straightforward: When I’m first interacting with the patient, I say, “if you are like my [other] elderly patients … I’m sure you’re feeling a lot of anxiety over [not having much] control and, first of all, I want to assure you that I’m going to make sure you understand the choices and help you make all the decisions. And … I’m definitely going to … put everything in a language that you understand. But if I’m not successful, I’m going to employ someone from your family. We’re going to work together. Even though you’re hospitalized and even though you’re fighting this illness (or whatever the condition might be), you still [have] the right to make choices, and my goal is to partner with you. My expertise is medicine, but you have an expertise in your life.”
In other words, you are signaling that you recognize that control is the issue. Acknowledge the loss, ask about the value of the event or decision to the patient, ask what you can do to help them deal with their feelings or make up their minds. It also allows you to remind an older patient’s children that control is a big and normal concern for their mother or father.
—Eva Chittenden, MD
Hospitalists at a Different Time and Place
The elderly desperately need people who can serve them as natural healers, who are not constantly in a hurry, and who care what they are thinking and feeling. How can hospitalists relate to those who are in the midst of life review and who are hanging on to an escaping control? How can they serve their patients in a way that meets all needs?
Fighting—with denial or ignorance—the resistance that patients might put up will more than likely provoke them. A fight for control can undermine and sabotage the best intentions of the provider and the greatest wishes for the patient to experience comfort or regain health and well-being. Rather than justifying wresting control from elderly patients because it’s for their own good, advises Solie, what we must do instead is to “step back, hand them the control baton, and allow them to run with it.”1
A person’s admission to the hospital “might be such a huge crisis for them, whereas for us it’s our routine work,” says Dr. Chittenden, who practices as a hospitalist and also works on her institution’s inpatient palliative care service. “And many people who are hospitalists—who are even in their late 20s, 30s, 40s—have been totally healthy their whole life, so it is hard to relate to what it’s like to be older and to be losing function, losing friends who are also dying, losing their house … . I think that it can be very helpful for the hospitalist to take a little more time and explore some of those issues [of loss and legacy]. I try to meet the person where they’re at and try to understand what their goals, needs, ... and fears are [as well as] their functional status.”
Allowing older patients to engage with you about their lives and their pasts is a privilege for any healthcare provider. Engaging with them in a way that will help facilitate their loosening the reins on control may expedite and allow greater quality into their healthcare. It may provide an opening whereby you can order that home-health visit with less struggle.
Create Openings
“There are a lot of different ‘on-ramps’ to asking the life-review questions, which are extremely comforting,” says Solie. “For example, you might say, ‘Mary, I notice that you were born in Iowa. You know, my family on my father’s side came from Iowa. Where were you raised?’ And ‘Do you have a big family on your farm, because my aunt had cows.’”
Once you get a response that engages the patient, then you “are in the slipstream. Physicians have such a high experience curve, they see so many patients,” he says. “They don’t have to go very far into their inventory of experiences [to find one] that essentially matches up with that patient.”
Any kind of comment that will key you in to their background experience can help establish some kind of foundation for relationship. Another example: “You know, Mary, I was working with this woman who was about your age and she was raised in the Midwest and was dealing with some of these issues of congestive heart failure, and one of her big concerns was something that I didn’t appreciate until I understood what an impact it was having on her life.”
This kind of communication, says Solie, can help to relieve some of the patient’s control anxieties, “because she feels that if I ‘get it,’ she’s open to what I have to say, such as, ‘The first thing, we have to deal with is there is too much fluid going on in your body and it’s putting a big strain on your heart, so the first couple days all we did for that [other] woman was try to pull some fluid off and keep everything in balance.’”
You’ve communicated that you have a plan, that you can be trusted, and that you will help her to exercise as much control as possible. Creating and accessing those openings is also “the ideal way to weave the family into this whole life-review process, which is where the patient lives, psychologically and emotionally, when outside the hospital environment,” he says. “We become so myopic when we’re caught in the hospital environment that the world becomes a narrow tunnel and we forget the greater matrix outside that we’re all connected to.”
The Boon of Biology
Whereas the physiology and anatomy of humans deteriorate with time, some of the changes in mental processes in old age may actually enhance the ability to reflect and make informed judgments. Solie’s view is that what younger people may view as slow behavior, confusing speech patterns, and physical frailty don’t hinder the tasks that are before the elderly. On the contrary, they assist the fulfillment of their developmental agendas to feel in control when they’re losing control and to let go enough to reveal the legacy that will survive after they go.
Research on the aging brain indicates that changes in brain chemistry facilitate the life-review process.1,6 In general, reflection is the normal mode of existence for elderly adults and their primary focus. Thus, viewing them as diminished because they communicate differently than younger people do is doing them a disservice.
Those slowed mental processes, Dr. Chittenden concurs, “are conducive to reflection. Someone younger will pathologize it. … I agree that we don’t value the slowing down process, but I also think that when this population is in the hospital we are tending to look at loss of functional status or the quick mental traits that we value as opposed to [that which is] adaptive [and] that enables them to look at things differently and reflect.”
The key to connecting the dots of where they are and where they need to be (both medically and psychosocially), as well as how they occur to their providers and their families as opposed to how they occur to themselves, is to listen to and speak with them by making use of what you know about this stage of their life as it affects their communication. You can do this, says Solie, by invoking the “access code,” which is “to clearly understand that at the top of their agenda—no matter what else is happening—is the need for control and the need to develop and go after a legacy, and that means life review. If you know that, you will never lose your reference point with them.”
Communication Habits of the Elderly
Solie identifies some verbal behaviors that are common in older people. In many cases these behaviors may reveal something between the lines.
- Lack of urgency. Older people need more time to decide things. Accept that slower pace as normal. Don’t take it personally. Adjust your schedule to allow time to deliver news or ask for choices and then allow time for them to discuss with their families or contemplate on their own; return to them at a later time. Become expert at spontaneous facilitation. Use your access code to get their attention and gain their trust.
- Nonlinear conversations. Although older patients may appear to wander off topic, they may do so in the urge to ground themselves in what their priorities are, what their feelings are, what their choices will be. Signal you’re willing to listen and that you’re tuned in to the content, even if you don’t know where it is leading. (Obviously, someone who is demented or delirious presents a different scenario altogether, and depression is common and frequently overlooked.) Listen for patterns and themes. Nonlinear conversations can lead to spontaneous revelations and great insights for your patients and for yourself and can help patients revisit life dramas that test and clarify values. This, too, is a part of healthcare.
- Repetition and attention to details. In situations when dementia is ruled out, a patient’s repetition may indicate a means to emphasize an important point or value. Keep in mind, too, that as we age, we all repeat stories to some degree. Details in stories may be the means by which older adults connect to their pasts and may also serve as clues to what is important to these people. Don’t assume details demand any action on your part. You are only being asked to listen as the older person sorts things out.
- Uncoupling. Solie describes uncoupling as any time an older person appears to disconnect from you in the course of a conversation. For a professional, this can feel as if you are dismissed or ignored just when you think you’ve hit the mark with a comment or question. Go back and assess the information you’ve gathered by doing some verification. Rethink the objective: Any action that works against their maintaining control and discovering a legacy will produce uncoupling.
“I try to be aware of when I’m losing people,” says Dr. Chittenden of this phenomenon. “I would say, ‘I seem to be losing you and I’m wondering what you’re thinking right now.’ I would try to find out where they’re at and if it was something I said that didn’t gel with them, didn’t make sense to them, or wasn’t their priority.” This is something, she emphasizes, that a hospitalist needs to watch for with patients of all ages. “Whether you’re older or younger,” she says, the communication can be complicated because “you’re … in the hospital culture and the priorities of doctors are so often different from the priorities of patients.”
Conclusion
Older and especially old-old individuals in some ways live in an era other than the one traversed by the young and middle-aged.6 Their purposes, agendas, and mission are different and the slowing down of their functioning can facilitate their attempts to put their lives into perspective and manage what control they can still exercise or are still allowed. Viewing older patients with the utmost respect and acknowledging the challenges they face at these last phases of their lives can better help you to partner with them and their families in their care. TH
Andrea Sattinger also writes about the importance of apology in this issue.
References
- Solie D. How to Say it to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Chochinov HM, Cann BJ. Interventions to enhance the spiritual aspects of dying. J Palliat Med. 2005;8:Suppl 1:S103-115.
- Dennis KE. Patients' control and the information imperative: clarification and confirmation. Nurs Res. 1990;39(3):162-166.
- Kiesler DJ, Auerbach SM. Integrating measurement of control and affiliation in studies of physician-patient interaction: the interpersonal circumplex. Soc Sci Med. 2003;57(9):1707-1722.
- Breemhaar B, Visser AP, Kleijnen JG. Perceptions and behaviour among elderly hospital patients: description and explanation of age differences in satisfaction, knowledge, emotions and behaviour. Soc Sci Med. 1990;31(12):1377-1385.
- Pipher M. Another Country: Navigating the Emotional Terrain of Our Elders. New York: Riverhead Books; 1999.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
I'm Sorry
Apologizing to a patient is the right thing to do,” says Michael S. Woods, MD, a general surgeon at St. Vincent’s Regional Medical Center in Santa Fe, N.M. “It is the respectful thing in any relationship in terms of trust whenever there is a violation, whether it is real or perceived.” Dr. Woods, the author of Healing Words: The Power of Apology in Medicine, teaches and consults with corporations around the country about apology as well as physician leadership.1-2 In fact, his study of apology stemmed from examining the subject of physician leadership, and he and other experts consider the vital components of leadership to be effective communication, integrity, honesty, and respectful treatment of other individuals.3,4
Dr. Woods also works with Doug Wojcieszak, a public relations consultant whose victims’ rights group proposed “Sorry Works!” This program recommends apologies and settlements when medical mistakes occur. (See “A History of Sorry Works!” p. 26.) Dr. Woods says Wojcieszak comes from an interesting angle that he supports. “Something I increasingly try to hammer home when I speak is that one of the most important components of the apology law has nothing to do with the backhand of the reduction of litigation as much as the fact that it gives the physician the green light to say ‘I’m sorry,’” says Dr. Woods.
The Benefit of Healing
Providers may be less than open when things go terribly wrong because of feelings of fear, shame, and guilt regarding the consequences to the patient as well as to themselves.1,3 Apology heals by restoring the patient’s dignity and self-respect, providing assurance of shared values, and assuring patients that they are not at fault, they are now safe, and that the caregiver shares their suffering.4,7
Two Senses of Apology
There are circumstances other than when errors occur in which a physician’s apology may carry the power to improve patient care. Peter Barnett, MD, MPH, a clinical associate professor of medicine at the University of New Mexico in Albuquerque, says that in general there are two senses of apology.
“The first sense of apology regards the situation,” he says. For example, you might say, ‘I’m sorry you have cancer,’ or ‘I’m sorry that our system doesn’t allow your family doctor to be taking care of you in the hospital.’ It’s an expression of sympathy, but I think apology works better.”
The other sense of apology regards responsibility, says Dr. Barnett, citing the example, “I’m sorry I gave you the wrong drug.”
Situational needs for apology include when patients have been waiting a long time, such as when a hospitalist meets them in the emergency department. “In those cases you would say, ‘I’m sorry that you had to wait so long,’” says Dr. Barnett. “It’s not my fault, but I really am sorry.”
Bridging the Gap
Dr. Barnett, who practices hospital medicine part-time along with his major focus in addiction medicine, was formerly the director of the UNM hospitalist team. He explains that one of the primary reasons hospitalists may need to apologize to patients is that the hospitalist and patient have no prior relationship that could serve as a foundation for interpreting each other’s behavior.8
He believes apologizing for the delays and inconveniences that happen in the hospital “can help bridge the relationship gap in hospital medicine. Because what people believe about their primary care physicians is that they know and care about them,” he says. “To minimize their anxiety about you, show them that you do care about them by getting to know them well, and apology is the one of the best ways of doing that.”
When asked to elaborate what he means by “getting to know them well,” Dr. Barnett says, “I might tell someone, ‘I’d like to get to know you better; what can you tell me about yourself that would help bring me up to speed?’” It’s open-ended, he says, and you let the patient choose the topic. “Most people will say something. … It’s empathic inquiry with really good reflective listening; that is probably the simplest way of summarizing what it takes.”
Dr. Barnett suggests this kind of inquiry can mitigate the gaps in relationships that may lead to misunderstandings, edgy situations, and errors that may later call for apology. He recommends asking or saying some of the following to patients:
- What do you know about your illness?
- What do you believe about your illness?
- What are your feelings, values, beliefs, and preferences about/for your treatment?
- What can you tell me about your experiences in the hospital?
For patients who have been ill many times and have had a lot of medical experience, you could ask:
- Could you tell me about your doctors?
- What do you like about doctors?
- What don’t you like about your doctors?
These questions can help you discern who they are as a patient, and it gives patients the opportunity to be candid with you.
“It’s not about finding information that’s embarrassing or critical to your predecessor physicians, but it allows you to not make the same mistakes inadvertently,” says Dr. Barnett, who considers it concrete information. “I want them to have good medical care. I don’t want to make them unhappy. I want to avoid pitfalls. I think the two of us—the patient and I—should avoid pitfalls together.”
Asking the patient in a straightforward way what they want and don’t want gives the patient an opportunity to give the physician advice on how to stay out of trouble with them.
Apology When Disclosing Errors
The matter of assuming responsibility for errors is more complicated as it pertains to the use of apology, but it is an “idea whose time has come.”9 Although it is hard to quantify, plenty of evidence shows that apologizing for errors reduces the number of lawsuits and may reduce the settlement value of malpractice claims.3,5-7,10-26 Although there is not always agreement about the specifics of full disclosure, above all patients have the right to know what happens during their medical care and, therefore, restricting the information that is given to a patient can have legal ramifications.
Beyond this, writes Lucian Leape, MD, adjunct professor of health policy at the Harvard School of Public Health and an internationally recognized leader in the patient safety movement, wrote in the March-April issue of Physician Executive that apology is a “therapeutic necessity” that allows the patient to recognize a physician’s humanity and fallibility as well as his or her remorse at having caused harm.9 In the long run, apologizing to patients defuses more situations than it aggravates, and it pays off emotionally, financially, and in practice morale.5,6,9
Data from studies of medical practices that issue apologies in circumstances where accountability is clearly established show that litigation claims are reduced. In one 1992 study, 24% of people who sued physicians said they did so because the doctor was dishonest and withheld information. Nineteen percent said that they either sued to deter subsequent malpractice or for revenge.11,12 In each case of legal action, the investigators hypothesized that the doctor could have avoided the lawsuit by taking responsibility and apologizing up front and making amends at that time. It has been estimated that more than half of claims relegated to litigation could be avoided with use of prudent disclosure and apology.3,21
“My mantra, if you will,” says Dr. Woods, “is that [when] you apologize because it’s the right thing to do, all the benefits naturally ensue.”
Anticipating Apology
The issue of complications, adverse events, and errors carries its own protocol in terms of whether and how apology is offered. “Hopefully some of these have been anticipated,” says Dr. Barnett. “For instance, when you spoke with the patient about their pneumonia, you’ve said something about the possibility that pneumonias could become complicated, and [they] might have some kind of complications; or if they’ve had a heart attack, [you mentioned that] they might have some complications. So you’re actually already warning people about what could happen and you’ve said you’re going to try to prevent it, but it could [still happen].”
Apology can be appropriately offered when those events do occur and you genuinely express disappointment that you and the patient share.
“There are some quite complicated systematic problems [related to apology and hospital medicine],” says Dr. Barnett. “Some are communication aspects and some are legal ones. What I have heard from the attorneys is that you want to keep the apology relatively simple, … and it shouldn’t include any statements about other people who may have been involved, such as pharmacy or nurses.”
The other important issue related to hospitalists and apology, says Dr. Barnett, is that because of the lack of relationship, the severity of illness of the patients you are treating, and the strangeness of systems, people come to the hospital expecting errors. They expect them and may be afraid of them. In particular, when a medication error is made, they expect those errors to be disclosed to them.7,27 Dr. Barnett believes patients are waiting and watching, and hoping that nothing happens to them. Complicating the issue, he says, is that “many hospitalists are fairly guarded in this respect. The emotional deck is sort of stacked against everybody, so if the hospitalist is sensitive about the situation, that tends actually to make the situation worse. If you can apologize sincerely and simply, the patient may be reassured that you’re not trying to conceal anything, you’re honest, you’re on top of it, and you’ll do your best to deal with it,” he says, adding, “they know that that stuff happens; they hope that it is not hidden, ignored, or mismanaged.”
Start Early and Let It Flow
Dr. Woods’ advice is to offer apology earlier rather than later and to widen the spectrum of those to whom you wish to show your empathy, sympathy, respect, and compassion.
“What I promote to organizations is that they drive this into the consciousness of the organization by getting people to apologize for the least infraction—not waiting for the grave errors.” He interprets this as apologizing “when you’re running 30 minutes late, apologize when you’ve interrupted the patient or the family when they’re speaking. These are the things we would do for our spouse or our significant other or our family members; why is it any different at work?”
He also believes it is inherent for doctors as leaders to “apologize to your staff members, apologize to the nurses.” Because the image you express serves as a role model in this regard and will permeate your practice culture. Drive respectful treatment as a basic common social courtesy into the organizational consciousness, says Dr. Woods, and then in any circumstance where an apology is offered, it is perceived as authentic.
Conclusion
Hospitalists may find a need to apologize to patients and families for situations and circumstances in the hospital environment as well as the gap in relationship that exists when hospitalists and patients first encounter each other. Apologizing early rather than later as well as simply and authentically goes a long way to help achieve the ethical and business objectives held by most hospital physicians. TH
Andrea Sattinger wrote about error reporting in the May issue.
References
- Woods MS, Star JI. Healing Words: The Power of Apology in Medicine. Santa Fe, N.M.: Doctors in Touch; 2004.
- Woods MS. Applying Personal Leadership Principles to Health Care: The DEPO Principle. Orlando, Fl.: American College of Physician Executives; 2001.
- Leape LL. National Patient Safety Foundation. Understanding the power of apology: how saying “I’m sorry" helps heal patients and caregivers. Focus on Patient Safety. 2005;8:1-3.
- Lazare A. On Apology. Oxford, U.K.: Oxford University Press; 2004.
- Boothman RC. Apologies and a strong defense at the University of Michigan Health System. Physician Exec. 2006 Mar-Apr; 32(2):7-10.
- Weber DO. Who’s sorry now? Special report: patient trust and safety. Physician Exec. 2006 Mar-Apr:32(2)6-14.
- When Things Go Wrong: Responding to Adverse Events. A Consensus Statement of the Harvard Hospitals. Burlington, Massachusetts: Massachusetts Coalition for the Prevention of Medical Errors; 2006.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
- Leape LL. Full disclosure and apology—an idea whose time has come. Physician Exec. Mar-Apr 2006 32:16-18.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. Jun 27 1994;154(12):1365-1370.
- Cohen JR. Apology and organizations: Exploring an example from medical practice. Fordham Urban Law J. 2000;27(5):1447-1482.
- Cohen JR. Advising clients to apologize. South Calif Law Rev. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care. JAMA. 1994 Nov 23-30;272(20):1588-1591.
- Gesensway D. Hospitalists and the malpractice insurance crisis. The Hospitalist. 2002Jul/Aug;11-13.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997 Feb19;227(7):553-559.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002 Apr;48(4):281-290.
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003 Jun 5;348(23):2281-2284.
- Shapiro RS, Simpson DE, Lawrence SL, et al. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989 Oct;149(10):2190-2196.
- Zimmerman R. Doctors' new tool to fight lawsuits: saying 'I'm sorry.' Malpractice insurers find owning up to errors soothes patient anger. 'The risks are extraordinary.' J Okla State Med Assoc. 2004 Jun;97(6):245-247.
- Ambady N, LaPlante D, Nguyen T, et al. Surgeons' tone of voice: a clue to malpractice history. Surgery. 2002 Jul;132(1):5-9.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999 Dec 21;131(12):970-972.
- Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation. N Engl J Med. 1996 Dec;335(26):1963-1967.
- Hickson GB, Federspiel CF, Pichert JW, et al. Patient complaints and malpractice risk. JAMA. 2002 Jun 12;287(22):2951-1957.
- Stelfox HT, Gandhi TK, Orav EJ, et al. The relation of patient satisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005 Oct;118(10):1126-1133.
- Pham HH, Devers KJ, Kuo S, et al. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005 Feb;20(2):101-107.
- Harris Interactive(R). Telephone survey conducted for the American Academy on Physician and Patient, March 3-6, 2006.
Apologizing to a patient is the right thing to do,” says Michael S. Woods, MD, a general surgeon at St. Vincent’s Regional Medical Center in Santa Fe, N.M. “It is the respectful thing in any relationship in terms of trust whenever there is a violation, whether it is real or perceived.” Dr. Woods, the author of Healing Words: The Power of Apology in Medicine, teaches and consults with corporations around the country about apology as well as physician leadership.1-2 In fact, his study of apology stemmed from examining the subject of physician leadership, and he and other experts consider the vital components of leadership to be effective communication, integrity, honesty, and respectful treatment of other individuals.3,4
Dr. Woods also works with Doug Wojcieszak, a public relations consultant whose victims’ rights group proposed “Sorry Works!” This program recommends apologies and settlements when medical mistakes occur. (See “A History of Sorry Works!” p. 26.) Dr. Woods says Wojcieszak comes from an interesting angle that he supports. “Something I increasingly try to hammer home when I speak is that one of the most important components of the apology law has nothing to do with the backhand of the reduction of litigation as much as the fact that it gives the physician the green light to say ‘I’m sorry,’” says Dr. Woods.
The Benefit of Healing
Providers may be less than open when things go terribly wrong because of feelings of fear, shame, and guilt regarding the consequences to the patient as well as to themselves.1,3 Apology heals by restoring the patient’s dignity and self-respect, providing assurance of shared values, and assuring patients that they are not at fault, they are now safe, and that the caregiver shares their suffering.4,7
Two Senses of Apology
There are circumstances other than when errors occur in which a physician’s apology may carry the power to improve patient care. Peter Barnett, MD, MPH, a clinical associate professor of medicine at the University of New Mexico in Albuquerque, says that in general there are two senses of apology.
“The first sense of apology regards the situation,” he says. For example, you might say, ‘I’m sorry you have cancer,’ or ‘I’m sorry that our system doesn’t allow your family doctor to be taking care of you in the hospital.’ It’s an expression of sympathy, but I think apology works better.”
The other sense of apology regards responsibility, says Dr. Barnett, citing the example, “I’m sorry I gave you the wrong drug.”
Situational needs for apology include when patients have been waiting a long time, such as when a hospitalist meets them in the emergency department. “In those cases you would say, ‘I’m sorry that you had to wait so long,’” says Dr. Barnett. “It’s not my fault, but I really am sorry.”
Bridging the Gap
Dr. Barnett, who practices hospital medicine part-time along with his major focus in addiction medicine, was formerly the director of the UNM hospitalist team. He explains that one of the primary reasons hospitalists may need to apologize to patients is that the hospitalist and patient have no prior relationship that could serve as a foundation for interpreting each other’s behavior.8
He believes apologizing for the delays and inconveniences that happen in the hospital “can help bridge the relationship gap in hospital medicine. Because what people believe about their primary care physicians is that they know and care about them,” he says. “To minimize their anxiety about you, show them that you do care about them by getting to know them well, and apology is the one of the best ways of doing that.”
When asked to elaborate what he means by “getting to know them well,” Dr. Barnett says, “I might tell someone, ‘I’d like to get to know you better; what can you tell me about yourself that would help bring me up to speed?’” It’s open-ended, he says, and you let the patient choose the topic. “Most people will say something. … It’s empathic inquiry with really good reflective listening; that is probably the simplest way of summarizing what it takes.”
Dr. Barnett suggests this kind of inquiry can mitigate the gaps in relationships that may lead to misunderstandings, edgy situations, and errors that may later call for apology. He recommends asking or saying some of the following to patients:
- What do you know about your illness?
- What do you believe about your illness?
- What are your feelings, values, beliefs, and preferences about/for your treatment?
- What can you tell me about your experiences in the hospital?
For patients who have been ill many times and have had a lot of medical experience, you could ask:
- Could you tell me about your doctors?
- What do you like about doctors?
- What don’t you like about your doctors?
These questions can help you discern who they are as a patient, and it gives patients the opportunity to be candid with you.
“It’s not about finding information that’s embarrassing or critical to your predecessor physicians, but it allows you to not make the same mistakes inadvertently,” says Dr. Barnett, who considers it concrete information. “I want them to have good medical care. I don’t want to make them unhappy. I want to avoid pitfalls. I think the two of us—the patient and I—should avoid pitfalls together.”
Asking the patient in a straightforward way what they want and don’t want gives the patient an opportunity to give the physician advice on how to stay out of trouble with them.
Apology When Disclosing Errors
The matter of assuming responsibility for errors is more complicated as it pertains to the use of apology, but it is an “idea whose time has come.”9 Although it is hard to quantify, plenty of evidence shows that apologizing for errors reduces the number of lawsuits and may reduce the settlement value of malpractice claims.3,5-7,10-26 Although there is not always agreement about the specifics of full disclosure, above all patients have the right to know what happens during their medical care and, therefore, restricting the information that is given to a patient can have legal ramifications.
Beyond this, writes Lucian Leape, MD, adjunct professor of health policy at the Harvard School of Public Health and an internationally recognized leader in the patient safety movement, wrote in the March-April issue of Physician Executive that apology is a “therapeutic necessity” that allows the patient to recognize a physician’s humanity and fallibility as well as his or her remorse at having caused harm.9 In the long run, apologizing to patients defuses more situations than it aggravates, and it pays off emotionally, financially, and in practice morale.5,6,9
Data from studies of medical practices that issue apologies in circumstances where accountability is clearly established show that litigation claims are reduced. In one 1992 study, 24% of people who sued physicians said they did so because the doctor was dishonest and withheld information. Nineteen percent said that they either sued to deter subsequent malpractice or for revenge.11,12 In each case of legal action, the investigators hypothesized that the doctor could have avoided the lawsuit by taking responsibility and apologizing up front and making amends at that time. It has been estimated that more than half of claims relegated to litigation could be avoided with use of prudent disclosure and apology.3,21
“My mantra, if you will,” says Dr. Woods, “is that [when] you apologize because it’s the right thing to do, all the benefits naturally ensue.”
Anticipating Apology
The issue of complications, adverse events, and errors carries its own protocol in terms of whether and how apology is offered. “Hopefully some of these have been anticipated,” says Dr. Barnett. “For instance, when you spoke with the patient about their pneumonia, you’ve said something about the possibility that pneumonias could become complicated, and [they] might have some kind of complications; or if they’ve had a heart attack, [you mentioned that] they might have some complications. So you’re actually already warning people about what could happen and you’ve said you’re going to try to prevent it, but it could [still happen].”
Apology can be appropriately offered when those events do occur and you genuinely express disappointment that you and the patient share.
“There are some quite complicated systematic problems [related to apology and hospital medicine],” says Dr. Barnett. “Some are communication aspects and some are legal ones. What I have heard from the attorneys is that you want to keep the apology relatively simple, … and it shouldn’t include any statements about other people who may have been involved, such as pharmacy or nurses.”
The other important issue related to hospitalists and apology, says Dr. Barnett, is that because of the lack of relationship, the severity of illness of the patients you are treating, and the strangeness of systems, people come to the hospital expecting errors. They expect them and may be afraid of them. In particular, when a medication error is made, they expect those errors to be disclosed to them.7,27 Dr. Barnett believes patients are waiting and watching, and hoping that nothing happens to them. Complicating the issue, he says, is that “many hospitalists are fairly guarded in this respect. The emotional deck is sort of stacked against everybody, so if the hospitalist is sensitive about the situation, that tends actually to make the situation worse. If you can apologize sincerely and simply, the patient may be reassured that you’re not trying to conceal anything, you’re honest, you’re on top of it, and you’ll do your best to deal with it,” he says, adding, “they know that that stuff happens; they hope that it is not hidden, ignored, or mismanaged.”
Start Early and Let It Flow
Dr. Woods’ advice is to offer apology earlier rather than later and to widen the spectrum of those to whom you wish to show your empathy, sympathy, respect, and compassion.
“What I promote to organizations is that they drive this into the consciousness of the organization by getting people to apologize for the least infraction—not waiting for the grave errors.” He interprets this as apologizing “when you’re running 30 minutes late, apologize when you’ve interrupted the patient or the family when they’re speaking. These are the things we would do for our spouse or our significant other or our family members; why is it any different at work?”
He also believes it is inherent for doctors as leaders to “apologize to your staff members, apologize to the nurses.” Because the image you express serves as a role model in this regard and will permeate your practice culture. Drive respectful treatment as a basic common social courtesy into the organizational consciousness, says Dr. Woods, and then in any circumstance where an apology is offered, it is perceived as authentic.
Conclusion
Hospitalists may find a need to apologize to patients and families for situations and circumstances in the hospital environment as well as the gap in relationship that exists when hospitalists and patients first encounter each other. Apologizing early rather than later as well as simply and authentically goes a long way to help achieve the ethical and business objectives held by most hospital physicians. TH
Andrea Sattinger wrote about error reporting in the May issue.
References
- Woods MS, Star JI. Healing Words: The Power of Apology in Medicine. Santa Fe, N.M.: Doctors in Touch; 2004.
- Woods MS. Applying Personal Leadership Principles to Health Care: The DEPO Principle. Orlando, Fl.: American College of Physician Executives; 2001.
- Leape LL. National Patient Safety Foundation. Understanding the power of apology: how saying “I’m sorry" helps heal patients and caregivers. Focus on Patient Safety. 2005;8:1-3.
- Lazare A. On Apology. Oxford, U.K.: Oxford University Press; 2004.
- Boothman RC. Apologies and a strong defense at the University of Michigan Health System. Physician Exec. 2006 Mar-Apr; 32(2):7-10.
- Weber DO. Who’s sorry now? Special report: patient trust and safety. Physician Exec. 2006 Mar-Apr:32(2)6-14.
- When Things Go Wrong: Responding to Adverse Events. A Consensus Statement of the Harvard Hospitals. Burlington, Massachusetts: Massachusetts Coalition for the Prevention of Medical Errors; 2006.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
- Leape LL. Full disclosure and apology—an idea whose time has come. Physician Exec. Mar-Apr 2006 32:16-18.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. Jun 27 1994;154(12):1365-1370.
- Cohen JR. Apology and organizations: Exploring an example from medical practice. Fordham Urban Law J. 2000;27(5):1447-1482.
- Cohen JR. Advising clients to apologize. South Calif Law Rev. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care. JAMA. 1994 Nov 23-30;272(20):1588-1591.
- Gesensway D. Hospitalists and the malpractice insurance crisis. The Hospitalist. 2002Jul/Aug;11-13.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997 Feb19;227(7):553-559.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002 Apr;48(4):281-290.
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003 Jun 5;348(23):2281-2284.
- Shapiro RS, Simpson DE, Lawrence SL, et al. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989 Oct;149(10):2190-2196.
- Zimmerman R. Doctors' new tool to fight lawsuits: saying 'I'm sorry.' Malpractice insurers find owning up to errors soothes patient anger. 'The risks are extraordinary.' J Okla State Med Assoc. 2004 Jun;97(6):245-247.
- Ambady N, LaPlante D, Nguyen T, et al. Surgeons' tone of voice: a clue to malpractice history. Surgery. 2002 Jul;132(1):5-9.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999 Dec 21;131(12):970-972.
- Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation. N Engl J Med. 1996 Dec;335(26):1963-1967.
- Hickson GB, Federspiel CF, Pichert JW, et al. Patient complaints and malpractice risk. JAMA. 2002 Jun 12;287(22):2951-1957.
- Stelfox HT, Gandhi TK, Orav EJ, et al. The relation of patient satisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005 Oct;118(10):1126-1133.
- Pham HH, Devers KJ, Kuo S, et al. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005 Feb;20(2):101-107.
- Harris Interactive(R). Telephone survey conducted for the American Academy on Physician and Patient, March 3-6, 2006.
Apologizing to a patient is the right thing to do,” says Michael S. Woods, MD, a general surgeon at St. Vincent’s Regional Medical Center in Santa Fe, N.M. “It is the respectful thing in any relationship in terms of trust whenever there is a violation, whether it is real or perceived.” Dr. Woods, the author of Healing Words: The Power of Apology in Medicine, teaches and consults with corporations around the country about apology as well as physician leadership.1-2 In fact, his study of apology stemmed from examining the subject of physician leadership, and he and other experts consider the vital components of leadership to be effective communication, integrity, honesty, and respectful treatment of other individuals.3,4
Dr. Woods also works with Doug Wojcieszak, a public relations consultant whose victims’ rights group proposed “Sorry Works!” This program recommends apologies and settlements when medical mistakes occur. (See “A History of Sorry Works!” p. 26.) Dr. Woods says Wojcieszak comes from an interesting angle that he supports. “Something I increasingly try to hammer home when I speak is that one of the most important components of the apology law has nothing to do with the backhand of the reduction of litigation as much as the fact that it gives the physician the green light to say ‘I’m sorry,’” says Dr. Woods.
The Benefit of Healing
Providers may be less than open when things go terribly wrong because of feelings of fear, shame, and guilt regarding the consequences to the patient as well as to themselves.1,3 Apology heals by restoring the patient’s dignity and self-respect, providing assurance of shared values, and assuring patients that they are not at fault, they are now safe, and that the caregiver shares their suffering.4,7
Two Senses of Apology
There are circumstances other than when errors occur in which a physician’s apology may carry the power to improve patient care. Peter Barnett, MD, MPH, a clinical associate professor of medicine at the University of New Mexico in Albuquerque, says that in general there are two senses of apology.
“The first sense of apology regards the situation,” he says. For example, you might say, ‘I’m sorry you have cancer,’ or ‘I’m sorry that our system doesn’t allow your family doctor to be taking care of you in the hospital.’ It’s an expression of sympathy, but I think apology works better.”
The other sense of apology regards responsibility, says Dr. Barnett, citing the example, “I’m sorry I gave you the wrong drug.”
Situational needs for apology include when patients have been waiting a long time, such as when a hospitalist meets them in the emergency department. “In those cases you would say, ‘I’m sorry that you had to wait so long,’” says Dr. Barnett. “It’s not my fault, but I really am sorry.”
Bridging the Gap
Dr. Barnett, who practices hospital medicine part-time along with his major focus in addiction medicine, was formerly the director of the UNM hospitalist team. He explains that one of the primary reasons hospitalists may need to apologize to patients is that the hospitalist and patient have no prior relationship that could serve as a foundation for interpreting each other’s behavior.8
He believes apologizing for the delays and inconveniences that happen in the hospital “can help bridge the relationship gap in hospital medicine. Because what people believe about their primary care physicians is that they know and care about them,” he says. “To minimize their anxiety about you, show them that you do care about them by getting to know them well, and apology is the one of the best ways of doing that.”
When asked to elaborate what he means by “getting to know them well,” Dr. Barnett says, “I might tell someone, ‘I’d like to get to know you better; what can you tell me about yourself that would help bring me up to speed?’” It’s open-ended, he says, and you let the patient choose the topic. “Most people will say something. … It’s empathic inquiry with really good reflective listening; that is probably the simplest way of summarizing what it takes.”
Dr. Barnett suggests this kind of inquiry can mitigate the gaps in relationships that may lead to misunderstandings, edgy situations, and errors that may later call for apology. He recommends asking or saying some of the following to patients:
- What do you know about your illness?
- What do you believe about your illness?
- What are your feelings, values, beliefs, and preferences about/for your treatment?
- What can you tell me about your experiences in the hospital?
For patients who have been ill many times and have had a lot of medical experience, you could ask:
- Could you tell me about your doctors?
- What do you like about doctors?
- What don’t you like about your doctors?
These questions can help you discern who they are as a patient, and it gives patients the opportunity to be candid with you.
“It’s not about finding information that’s embarrassing or critical to your predecessor physicians, but it allows you to not make the same mistakes inadvertently,” says Dr. Barnett, who considers it concrete information. “I want them to have good medical care. I don’t want to make them unhappy. I want to avoid pitfalls. I think the two of us—the patient and I—should avoid pitfalls together.”
Asking the patient in a straightforward way what they want and don’t want gives the patient an opportunity to give the physician advice on how to stay out of trouble with them.
Apology When Disclosing Errors
The matter of assuming responsibility for errors is more complicated as it pertains to the use of apology, but it is an “idea whose time has come.”9 Although it is hard to quantify, plenty of evidence shows that apologizing for errors reduces the number of lawsuits and may reduce the settlement value of malpractice claims.3,5-7,10-26 Although there is not always agreement about the specifics of full disclosure, above all patients have the right to know what happens during their medical care and, therefore, restricting the information that is given to a patient can have legal ramifications.
Beyond this, writes Lucian Leape, MD, adjunct professor of health policy at the Harvard School of Public Health and an internationally recognized leader in the patient safety movement, wrote in the March-April issue of Physician Executive that apology is a “therapeutic necessity” that allows the patient to recognize a physician’s humanity and fallibility as well as his or her remorse at having caused harm.9 In the long run, apologizing to patients defuses more situations than it aggravates, and it pays off emotionally, financially, and in practice morale.5,6,9
Data from studies of medical practices that issue apologies in circumstances where accountability is clearly established show that litigation claims are reduced. In one 1992 study, 24% of people who sued physicians said they did so because the doctor was dishonest and withheld information. Nineteen percent said that they either sued to deter subsequent malpractice or for revenge.11,12 In each case of legal action, the investigators hypothesized that the doctor could have avoided the lawsuit by taking responsibility and apologizing up front and making amends at that time. It has been estimated that more than half of claims relegated to litigation could be avoided with use of prudent disclosure and apology.3,21
“My mantra, if you will,” says Dr. Woods, “is that [when] you apologize because it’s the right thing to do, all the benefits naturally ensue.”
Anticipating Apology
The issue of complications, adverse events, and errors carries its own protocol in terms of whether and how apology is offered. “Hopefully some of these have been anticipated,” says Dr. Barnett. “For instance, when you spoke with the patient about their pneumonia, you’ve said something about the possibility that pneumonias could become complicated, and [they] might have some kind of complications; or if they’ve had a heart attack, [you mentioned that] they might have some complications. So you’re actually already warning people about what could happen and you’ve said you’re going to try to prevent it, but it could [still happen].”
Apology can be appropriately offered when those events do occur and you genuinely express disappointment that you and the patient share.
“There are some quite complicated systematic problems [related to apology and hospital medicine],” says Dr. Barnett. “Some are communication aspects and some are legal ones. What I have heard from the attorneys is that you want to keep the apology relatively simple, … and it shouldn’t include any statements about other people who may have been involved, such as pharmacy or nurses.”
The other important issue related to hospitalists and apology, says Dr. Barnett, is that because of the lack of relationship, the severity of illness of the patients you are treating, and the strangeness of systems, people come to the hospital expecting errors. They expect them and may be afraid of them. In particular, when a medication error is made, they expect those errors to be disclosed to them.7,27 Dr. Barnett believes patients are waiting and watching, and hoping that nothing happens to them. Complicating the issue, he says, is that “many hospitalists are fairly guarded in this respect. The emotional deck is sort of stacked against everybody, so if the hospitalist is sensitive about the situation, that tends actually to make the situation worse. If you can apologize sincerely and simply, the patient may be reassured that you’re not trying to conceal anything, you’re honest, you’re on top of it, and you’ll do your best to deal with it,” he says, adding, “they know that that stuff happens; they hope that it is not hidden, ignored, or mismanaged.”
Start Early and Let It Flow
Dr. Woods’ advice is to offer apology earlier rather than later and to widen the spectrum of those to whom you wish to show your empathy, sympathy, respect, and compassion.
“What I promote to organizations is that they drive this into the consciousness of the organization by getting people to apologize for the least infraction—not waiting for the grave errors.” He interprets this as apologizing “when you’re running 30 minutes late, apologize when you’ve interrupted the patient or the family when they’re speaking. These are the things we would do for our spouse or our significant other or our family members; why is it any different at work?”
He also believes it is inherent for doctors as leaders to “apologize to your staff members, apologize to the nurses.” Because the image you express serves as a role model in this regard and will permeate your practice culture. Drive respectful treatment as a basic common social courtesy into the organizational consciousness, says Dr. Woods, and then in any circumstance where an apology is offered, it is perceived as authentic.
Conclusion
Hospitalists may find a need to apologize to patients and families for situations and circumstances in the hospital environment as well as the gap in relationship that exists when hospitalists and patients first encounter each other. Apologizing early rather than later as well as simply and authentically goes a long way to help achieve the ethical and business objectives held by most hospital physicians. TH
Andrea Sattinger wrote about error reporting in the May issue.
References
- Woods MS, Star JI. Healing Words: The Power of Apology in Medicine. Santa Fe, N.M.: Doctors in Touch; 2004.
- Woods MS. Applying Personal Leadership Principles to Health Care: The DEPO Principle. Orlando, Fl.: American College of Physician Executives; 2001.
- Leape LL. National Patient Safety Foundation. Understanding the power of apology: how saying “I’m sorry" helps heal patients and caregivers. Focus on Patient Safety. 2005;8:1-3.
- Lazare A. On Apology. Oxford, U.K.: Oxford University Press; 2004.
- Boothman RC. Apologies and a strong defense at the University of Michigan Health System. Physician Exec. 2006 Mar-Apr; 32(2):7-10.
- Weber DO. Who’s sorry now? Special report: patient trust and safety. Physician Exec. 2006 Mar-Apr:32(2)6-14.
- When Things Go Wrong: Responding to Adverse Events. A Consensus Statement of the Harvard Hospitals. Burlington, Massachusetts: Massachusetts Coalition for the Prevention of Medical Errors; 2006.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
- Leape LL. Full disclosure and apology—an idea whose time has come. Physician Exec. Mar-Apr 2006 32:16-18.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. Jun 27 1994;154(12):1365-1370.
- Cohen JR. Apology and organizations: Exploring an example from medical practice. Fordham Urban Law J. 2000;27(5):1447-1482.
- Cohen JR. Advising clients to apologize. South Calif Law Rev. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care. JAMA. 1994 Nov 23-30;272(20):1588-1591.
- Gesensway D. Hospitalists and the malpractice insurance crisis. The Hospitalist. 2002Jul/Aug;11-13.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997 Feb19;227(7):553-559.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002 Apr;48(4):281-290.
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003 Jun 5;348(23):2281-2284.
- Shapiro RS, Simpson DE, Lawrence SL, et al. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989 Oct;149(10):2190-2196.
- Zimmerman R. Doctors' new tool to fight lawsuits: saying 'I'm sorry.' Malpractice insurers find owning up to errors soothes patient anger. 'The risks are extraordinary.' J Okla State Med Assoc. 2004 Jun;97(6):245-247.
- Ambady N, LaPlante D, Nguyen T, et al. Surgeons' tone of voice: a clue to malpractice history. Surgery. 2002 Jul;132(1):5-9.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999 Dec 21;131(12):970-972.
- Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation. N Engl J Med. 1996 Dec;335(26):1963-1967.
- Hickson GB, Federspiel CF, Pichert JW, et al. Patient complaints and malpractice risk. JAMA. 2002 Jun 12;287(22):2951-1957.
- Stelfox HT, Gandhi TK, Orav EJ, et al. The relation of patient satisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005 Oct;118(10):1126-1133.
- Pham HH, Devers KJ, Kuo S, et al. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005 Feb;20(2):101-107.
- Harris Interactive(R). Telephone survey conducted for the American Academy on Physician and Patient, March 3-6, 2006.
Near Misses
The medical literature pertaining to patient safety is voluminous, especially since the publication of the 1999 Institute of Medicine (IOM) report estimating that between 44,000 and 98,000 Americans die from medical errors each year.1 When focusing on hospitalists and the matter of near misses, however, where the outcome of the error has been intercepted before harm can occur, the volume of published information is far more limited.2
“There are few good data about the role that hospitalists play in preventing adverse events,” says Saul Weingart, MD, PhD, vice president for patient safety at the Dana-Farber Cancer Institute, Boston, “so most accounts are anecdotal. My own sense is that hospital medicine plays a critical role in preventing and mitigating errors in the acute care setting.”
One study, conducted by two hospitalists in a 200-bed academic hospital and published in 2003 in the Journal of General Internal Medicine, distinguished near misses from adverse events.3 The investigators set out to determine the frequency, types, and consequences of errors that can be detected by hospitalists during routine clinical care, and to compare the types of errors first discovered by hospitalists to those discovered by other providers.
Sarwat Chaudhry, MD, a former hospitalist who is now a health services researcher and assistant professor of medicine at the Yale School of Medicine in New Haven, Conn., was the lead investigator in that study. “Oftentimes the errors that are ‘sexier’ and more exciting for people to talk about are the adverse events,” she says. “But I think what are perhaps more common and more informative are the near misses.”
Definitions
For purposes of Chaudhry, et al.’s study, “adverse events” were defined as adverse outcomes that resulted from errors.3 Errors that did not result in patient harm, but could have, were categorized as near misses. The umbrella definition of error fit that which was used in the IOM report; that is, “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim.”1 Cases in which a bad outcome occurred (such as death or disability) without a preventable cause were not considered errors and, therefore, were not included in the data.
A more practical understanding of a near miss is apparent in the following illustration: “If pharmacy came to me and said, ‘Oh, Dr. Chaudhry, one of the physicians on your team wrote for drug X but the patient is also on drug Y and that’s a known contraindication so we don’t think this should be administered, do you agree?’ I’d say, ‘Yes, I agree.’ So the drug was never given, but it was a near miss for the way it was written if it hadn’t been picked up on.”
—Saul Weingart, MD, PhD
In fact there are two kinds of near misses. “One is where the error is intercepted by [a] pharmacy or somebody else before harm is done,” says Dr. Weingart. “The other kind is where the error reaches the patient—for instance, where he or she receives the antibiotic to which they are allergic—but no reaction takes place.”
An important element in the study was that both types of errors were identified during the course of routine, clinical care by Dr. Chaudhry and her colleague, Kolawole Olofinboba, MD. Errors first detected by other healthcare workers were also recorded. Of the 528 patients included in the study, 10.4% experienced at least one error: 6.2% a near miss and 4.2% an adverse event. Interestingly, most of the errors first detected by house staff, nurses, and laboratory technicians were adverse events, whereas most of the errors first detected by the attending hospitalists, pharmacists, and consultants were near misses. Drug errors were the most common type of error overall.
Although differences did not achieve statistical significance, Dr. Chaudhry says the data were illuminating and the hospital administration was anxious to clarify the processes of care that could be modified to make the workflow more efficient and the different pieces of each patient’s critical data more integrated.
“For instance,” she says, “at our hospital there was a lot of separation of data. … The vitals were right outside the patient’s room. The list of medications was kept in a central pharmacy location, and the medical chart with everyone’s notes was in a third location.”
After the study’s completion, the integration of data was facilitated by the adoption of an electronic medical record (EMR) and there is ongoing research at that institution concerning whether that has affected error rates.

—Sarwat Chaudhry, MD
Lessons Learned
“This was one of the first and, still I think, only studies of attending physicians reporting their own errors,” says Dr. Chaudhry, “as well as reporting the scope, type, and frequency of the errors.”
There were several lessons learned. The first is that near misses are very common—at least as common as adverse events and perhaps more frequent. The second is that the nature of near misses is similar enough to that of adverse events that they can still be informative in preventing harm to patients. The third lesson arises from the investigators’ review of the kinds of errors that were reported by the different providers. “Different types of providers are going to pick up on different kinds of errors,” says Dr. Chaudhry. “Pharmacy, of course, is going to be detecting drug errors. But nurses are going to be detecting a different kind of error than residents, and residents are detecting a different kind of error than attending physicians.”
Dr. Weingart, who was trained as an internist, says his sense is that “we often pick up errors that occur just upstream in the process of care. For instance, pharmacy finds doctor prescribing errors and nursing finds pharmacy dispensing errors.”
Drs. Chaudhry and Olofinboba discovered 17/47 (36%) of the errors on their own, and pharmacists, resident physicians, consulting physicians, nurses, and ancillary staff discovered the remaining 30/47 (64%). The hospitalists were more likely to detect therapeutic errors; house staff physicians were more likely to detect drug errors. House staff also detected procedural errors at a higher rate than did the hospitalists. Consequently, Dr. Chaudhry emphasizes, another highlight of these data shows that “engaging as many different kinds of healthcare providers in error reporting is very important to understand what’s going on.”
Documenting Errors
The two hospitalists in Dr. Chaudhry’s study underwent no formal training in error detection, and all errors identified were documented. This in itself is a remarkable aspect of this study for hospitalists to note.
“In most hospitals, the risk management department feels like breaking out a bottle of champagne to celebrate every time a physician submits an incident report,” says Dr. Weingart, “because in most hospitals physicians don’t view incident reporting as part of their responsibility. On the other hand, physicians constantly talk about the errors, near misses, and adverse events they encounter day-to-day. Unfortunately, formal incident reporting isn’t an activity that most physicians see as a part of their duty to deliver excellent care at the bedside.” By virtue of this, he says, “critical information is often lost to the system. Error experience is transmitted person-to-person but isn’t captured and analyzed.”
The good news here, however, is that by simply launching a study of this nature and capturing the data it is reasonable to expect that any hospitalist group could take it on and any hospital’s quality of care would be improved.
“There is a spectrum of practice review that is conducted by a variety of people,” says Dr. Chaudhry. “On one end of the spectrum, you have the uninvolved reviewer coming in and doing formal chart reviews … and our process was at other end of spectrum, where we were going about our daily business, the routine clinical care of patients.”
By maintaining the potential for errors at the forefront of their thinking, she says, it became the background against which they performed the constant daily review of patient data. “When I would go to the bedside in the morning,” she says, “to see the patient, talk to the patient, review the chart, look at notes, look at vitals, look at meds—that was my process for picking up on errors.”
—Saul Weingart, MD, PhD
Barriers and Opportunities
There are two major barriers to performing this kind of research in other institutions where hospitalists practice, but they are easily resolved. The first is the importance of standardizing definitions.
“We came to consensus before the study began of what things should count and what things shouldn’t count,” says Dr. Chaudhry. “Because there is a degree of subjectivity and especially when a patient experiences harm, it’s a bit easier to attribute that to an error—though not always. For instance, with a patient with asthma who ends up with fluid overload and gets intubated. Well, was that an error? … Or was that just the patient’s own asthma getting worse? How much did the fluid contribute to that?”
There is still a degree of judgment, even there, she says, “but as much as possible we wanted to come to consensus at least about our definitions, our terminology, and our categorization.”
The second barrier to performing this research is the real or perceived risk of litigation. There was a lot of concern at the beginning of her study, says Dr. Chaudhry (and again at the time of publication), regarding the aftermath of disclosing errors.
“As much as the Institute of Medicine and other accreditation and safety organizations talk about how error reporting is so important and that physicians have to be willing to come forward with their errors, there are really no formal, legal, protective mechanisms in place,” she says, adding that this was true three years ago, and she does not believe much has changed.
Consequently, when constructing the study, she reached out to the authors of other error studies and asked them how they had handled the risk of potential litigation. Most of them told her they did not think there was much risk of being sued, but disclosing errors in the literature is certainly not something an institution or individuals would be clamoring to do. If a multi-center study of this nature might be undertaken, she says, these barriers could be traversed and it would be worth it. “Because if we let that opportunity slip through our fingers, it will be taken on by nonphysicians,” she cautions, “by the external reviewers, by the accreditation organizations, by professional quality control people.”
Dr. Chaudhry’s overall recommendation to hospitalists involves the position they hold at this time. “Hospitalists are ideally poised to take a lead in promoting patient safety by becoming more involved and developing the systems for error reporting,” she says.
Dr. Weingart tells hospitalist audiences that the most important areas for detecting errors in their practice include safe prescription writing and error-proofing high-risk activities (such as hand-offs and sign-outs, and follow-up of test results). He also recommends that hospitalists play the role of responsible citizens in their institutions and be open to ways your patients can contribute by helping you detect errors in their care.4 These issues will be addressed in more detail in future articles in The Hospitalist.
Although Dr. Chaudhry is no longer practicing as a hospitalist, she believes that hospital teams working closely together in patient care have a strong advantage to identify any errors.
“As physicians, with hospital medicine expanding,” she says, “this is the opportune time to take on a leadership role, and this needs to be part of the hospitalist mission. Not everyone has to come out and report their adverse events, especially since the legal risks are still unclear. But a safe way and equally informative way to work on preventing harm is to focus on those near misses.”
Conclusion
Hospitalists who search for near misses, volunteer this information, and enroll their colleagues in doing the same contribute to reforming systems and processes that will ultimately reduce the potential for all errors. Those who pay close attention to standardized rules for prescription-writing, error-proofing high-risk activities, and their roles for institutional citizenship and encouraging patient contribution in regard to possible errors, are doing the best possible job to prevent harm to patients and the institution as a whole. TH
Andrea Sattinger will write about apology in medicine in the June issue.
References
- Kohn LT, Corrigan JM, Donaldson MS, Institute of Medicine Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
- Bleich S. Medical Errors: Five Years After the IOM Report. New York: Commonwealth Fund; July 2005: Available at: www.mihealthandsafety.org/pdfs/pub-4-commonwealth.pdf. Last accessed March 22, 2006.
- Chaudhry SI, Olofinboba KA, Krumholz HM. Detection of errors by attending physicians on a general medicine service. J Gen Intern Med. 2003 Aug;18(8):595-600.
- Weingart SN, Pagovich O, Sands DZ, et al. What can hospitalized patients tell us about adverse events? Learning from patient-reported incidents. J Gen Intern Med. 2005 Sep;20(9):830-836.
The medical literature pertaining to patient safety is voluminous, especially since the publication of the 1999 Institute of Medicine (IOM) report estimating that between 44,000 and 98,000 Americans die from medical errors each year.1 When focusing on hospitalists and the matter of near misses, however, where the outcome of the error has been intercepted before harm can occur, the volume of published information is far more limited.2
“There are few good data about the role that hospitalists play in preventing adverse events,” says Saul Weingart, MD, PhD, vice president for patient safety at the Dana-Farber Cancer Institute, Boston, “so most accounts are anecdotal. My own sense is that hospital medicine plays a critical role in preventing and mitigating errors in the acute care setting.”
One study, conducted by two hospitalists in a 200-bed academic hospital and published in 2003 in the Journal of General Internal Medicine, distinguished near misses from adverse events.3 The investigators set out to determine the frequency, types, and consequences of errors that can be detected by hospitalists during routine clinical care, and to compare the types of errors first discovered by hospitalists to those discovered by other providers.
Sarwat Chaudhry, MD, a former hospitalist who is now a health services researcher and assistant professor of medicine at the Yale School of Medicine in New Haven, Conn., was the lead investigator in that study. “Oftentimes the errors that are ‘sexier’ and more exciting for people to talk about are the adverse events,” she says. “But I think what are perhaps more common and more informative are the near misses.”
Definitions
For purposes of Chaudhry, et al.’s study, “adverse events” were defined as adverse outcomes that resulted from errors.3 Errors that did not result in patient harm, but could have, were categorized as near misses. The umbrella definition of error fit that which was used in the IOM report; that is, “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim.”1 Cases in which a bad outcome occurred (such as death or disability) without a preventable cause were not considered errors and, therefore, were not included in the data.
A more practical understanding of a near miss is apparent in the following illustration: “If pharmacy came to me and said, ‘Oh, Dr. Chaudhry, one of the physicians on your team wrote for drug X but the patient is also on drug Y and that’s a known contraindication so we don’t think this should be administered, do you agree?’ I’d say, ‘Yes, I agree.’ So the drug was never given, but it was a near miss for the way it was written if it hadn’t been picked up on.”
—Saul Weingart, MD, PhD
In fact there are two kinds of near misses. “One is where the error is intercepted by [a] pharmacy or somebody else before harm is done,” says Dr. Weingart. “The other kind is where the error reaches the patient—for instance, where he or she receives the antibiotic to which they are allergic—but no reaction takes place.”
An important element in the study was that both types of errors were identified during the course of routine, clinical care by Dr. Chaudhry and her colleague, Kolawole Olofinboba, MD. Errors first detected by other healthcare workers were also recorded. Of the 528 patients included in the study, 10.4% experienced at least one error: 6.2% a near miss and 4.2% an adverse event. Interestingly, most of the errors first detected by house staff, nurses, and laboratory technicians were adverse events, whereas most of the errors first detected by the attending hospitalists, pharmacists, and consultants were near misses. Drug errors were the most common type of error overall.
Although differences did not achieve statistical significance, Dr. Chaudhry says the data were illuminating and the hospital administration was anxious to clarify the processes of care that could be modified to make the workflow more efficient and the different pieces of each patient’s critical data more integrated.
“For instance,” she says, “at our hospital there was a lot of separation of data. … The vitals were right outside the patient’s room. The list of medications was kept in a central pharmacy location, and the medical chart with everyone’s notes was in a third location.”
After the study’s completion, the integration of data was facilitated by the adoption of an electronic medical record (EMR) and there is ongoing research at that institution concerning whether that has affected error rates.
—Sarwat Chaudhry, MD
Lessons Learned
“This was one of the first and, still I think, only studies of attending physicians reporting their own errors,” says Dr. Chaudhry, “as well as reporting the scope, type, and frequency of the errors.”
There were several lessons learned. The first is that near misses are very common—at least as common as adverse events and perhaps more frequent. The second is that the nature of near misses is similar enough to that of adverse events that they can still be informative in preventing harm to patients. The third lesson arises from the investigators’ review of the kinds of errors that were reported by the different providers. “Different types of providers are going to pick up on different kinds of errors,” says Dr. Chaudhry. “Pharmacy, of course, is going to be detecting drug errors. But nurses are going to be detecting a different kind of error than residents, and residents are detecting a different kind of error than attending physicians.”
Dr. Weingart, who was trained as an internist, says his sense is that “we often pick up errors that occur just upstream in the process of care. For instance, pharmacy finds doctor prescribing errors and nursing finds pharmacy dispensing errors.”
Drs. Chaudhry and Olofinboba discovered 17/47 (36%) of the errors on their own, and pharmacists, resident physicians, consulting physicians, nurses, and ancillary staff discovered the remaining 30/47 (64%). The hospitalists were more likely to detect therapeutic errors; house staff physicians were more likely to detect drug errors. House staff also detected procedural errors at a higher rate than did the hospitalists. Consequently, Dr. Chaudhry emphasizes, another highlight of these data shows that “engaging as many different kinds of healthcare providers in error reporting is very important to understand what’s going on.”
Documenting Errors
The two hospitalists in Dr. Chaudhry’s study underwent no formal training in error detection, and all errors identified were documented. This in itself is a remarkable aspect of this study for hospitalists to note.
“In most hospitals, the risk management department feels like breaking out a bottle of champagne to celebrate every time a physician submits an incident report,” says Dr. Weingart, “because in most hospitals physicians don’t view incident reporting as part of their responsibility. On the other hand, physicians constantly talk about the errors, near misses, and adverse events they encounter day-to-day. Unfortunately, formal incident reporting isn’t an activity that most physicians see as a part of their duty to deliver excellent care at the bedside.” By virtue of this, he says, “critical information is often lost to the system. Error experience is transmitted person-to-person but isn’t captured and analyzed.”
The good news here, however, is that by simply launching a study of this nature and capturing the data it is reasonable to expect that any hospitalist group could take it on and any hospital’s quality of care would be improved.
“There is a spectrum of practice review that is conducted by a variety of people,” says Dr. Chaudhry. “On one end of the spectrum, you have the uninvolved reviewer coming in and doing formal chart reviews … and our process was at other end of spectrum, where we were going about our daily business, the routine clinical care of patients.”
By maintaining the potential for errors at the forefront of their thinking, she says, it became the background against which they performed the constant daily review of patient data. “When I would go to the bedside in the morning,” she says, “to see the patient, talk to the patient, review the chart, look at notes, look at vitals, look at meds—that was my process for picking up on errors.”
—Saul Weingart, MD, PhD
Barriers and Opportunities
There are two major barriers to performing this kind of research in other institutions where hospitalists practice, but they are easily resolved. The first is the importance of standardizing definitions.
“We came to consensus before the study began of what things should count and what things shouldn’t count,” says Dr. Chaudhry. “Because there is a degree of subjectivity and especially when a patient experiences harm, it’s a bit easier to attribute that to an error—though not always. For instance, with a patient with asthma who ends up with fluid overload and gets intubated. Well, was that an error? … Or was that just the patient’s own asthma getting worse? How much did the fluid contribute to that?”
There is still a degree of judgment, even there, she says, “but as much as possible we wanted to come to consensus at least about our definitions, our terminology, and our categorization.”
The second barrier to performing this research is the real or perceived risk of litigation. There was a lot of concern at the beginning of her study, says Dr. Chaudhry (and again at the time of publication), regarding the aftermath of disclosing errors.
“As much as the Institute of Medicine and other accreditation and safety organizations talk about how error reporting is so important and that physicians have to be willing to come forward with their errors, there are really no formal, legal, protective mechanisms in place,” she says, adding that this was true three years ago, and she does not believe much has changed.
Consequently, when constructing the study, she reached out to the authors of other error studies and asked them how they had handled the risk of potential litigation. Most of them told her they did not think there was much risk of being sued, but disclosing errors in the literature is certainly not something an institution or individuals would be clamoring to do. If a multi-center study of this nature might be undertaken, she says, these barriers could be traversed and it would be worth it. “Because if we let that opportunity slip through our fingers, it will be taken on by nonphysicians,” she cautions, “by the external reviewers, by the accreditation organizations, by professional quality control people.”
Dr. Chaudhry’s overall recommendation to hospitalists involves the position they hold at this time. “Hospitalists are ideally poised to take a lead in promoting patient safety by becoming more involved and developing the systems for error reporting,” she says.
Dr. Weingart tells hospitalist audiences that the most important areas for detecting errors in their practice include safe prescription writing and error-proofing high-risk activities (such as hand-offs and sign-outs, and follow-up of test results). He also recommends that hospitalists play the role of responsible citizens in their institutions and be open to ways your patients can contribute by helping you detect errors in their care.4 These issues will be addressed in more detail in future articles in The Hospitalist.
Although Dr. Chaudhry is no longer practicing as a hospitalist, she believes that hospital teams working closely together in patient care have a strong advantage to identify any errors.
“As physicians, with hospital medicine expanding,” she says, “this is the opportune time to take on a leadership role, and this needs to be part of the hospitalist mission. Not everyone has to come out and report their adverse events, especially since the legal risks are still unclear. But a safe way and equally informative way to work on preventing harm is to focus on those near misses.”
Conclusion
Hospitalists who search for near misses, volunteer this information, and enroll their colleagues in doing the same contribute to reforming systems and processes that will ultimately reduce the potential for all errors. Those who pay close attention to standardized rules for prescription-writing, error-proofing high-risk activities, and their roles for institutional citizenship and encouraging patient contribution in regard to possible errors, are doing the best possible job to prevent harm to patients and the institution as a whole. TH
Andrea Sattinger will write about apology in medicine in the June issue.
References
- Kohn LT, Corrigan JM, Donaldson MS, Institute of Medicine Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
- Bleich S. Medical Errors: Five Years After the IOM Report. New York: Commonwealth Fund; July 2005: Available at: www.mihealthandsafety.org/pdfs/pub-4-commonwealth.pdf. Last accessed March 22, 2006.
- Chaudhry SI, Olofinboba KA, Krumholz HM. Detection of errors by attending physicians on a general medicine service. J Gen Intern Med. 2003 Aug;18(8):595-600.
- Weingart SN, Pagovich O, Sands DZ, et al. What can hospitalized patients tell us about adverse events? Learning from patient-reported incidents. J Gen Intern Med. 2005 Sep;20(9):830-836.
The medical literature pertaining to patient safety is voluminous, especially since the publication of the 1999 Institute of Medicine (IOM) report estimating that between 44,000 and 98,000 Americans die from medical errors each year.1 When focusing on hospitalists and the matter of near misses, however, where the outcome of the error has been intercepted before harm can occur, the volume of published information is far more limited.2
“There are few good data about the role that hospitalists play in preventing adverse events,” says Saul Weingart, MD, PhD, vice president for patient safety at the Dana-Farber Cancer Institute, Boston, “so most accounts are anecdotal. My own sense is that hospital medicine plays a critical role in preventing and mitigating errors in the acute care setting.”
One study, conducted by two hospitalists in a 200-bed academic hospital and published in 2003 in the Journal of General Internal Medicine, distinguished near misses from adverse events.3 The investigators set out to determine the frequency, types, and consequences of errors that can be detected by hospitalists during routine clinical care, and to compare the types of errors first discovered by hospitalists to those discovered by other providers.
Sarwat Chaudhry, MD, a former hospitalist who is now a health services researcher and assistant professor of medicine at the Yale School of Medicine in New Haven, Conn., was the lead investigator in that study. “Oftentimes the errors that are ‘sexier’ and more exciting for people to talk about are the adverse events,” she says. “But I think what are perhaps more common and more informative are the near misses.”
Definitions
For purposes of Chaudhry, et al.’s study, “adverse events” were defined as adverse outcomes that resulted from errors.3 Errors that did not result in patient harm, but could have, were categorized as near misses. The umbrella definition of error fit that which was used in the IOM report; that is, “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim.”1 Cases in which a bad outcome occurred (such as death or disability) without a preventable cause were not considered errors and, therefore, were not included in the data.
A more practical understanding of a near miss is apparent in the following illustration: “If pharmacy came to me and said, ‘Oh, Dr. Chaudhry, one of the physicians on your team wrote for drug X but the patient is also on drug Y and that’s a known contraindication so we don’t think this should be administered, do you agree?’ I’d say, ‘Yes, I agree.’ So the drug was never given, but it was a near miss for the way it was written if it hadn’t been picked up on.”
—Saul Weingart, MD, PhD
In fact there are two kinds of near misses. “One is where the error is intercepted by [a] pharmacy or somebody else before harm is done,” says Dr. Weingart. “The other kind is where the error reaches the patient—for instance, where he or she receives the antibiotic to which they are allergic—but no reaction takes place.”
An important element in the study was that both types of errors were identified during the course of routine, clinical care by Dr. Chaudhry and her colleague, Kolawole Olofinboba, MD. Errors first detected by other healthcare workers were also recorded. Of the 528 patients included in the study, 10.4% experienced at least one error: 6.2% a near miss and 4.2% an adverse event. Interestingly, most of the errors first detected by house staff, nurses, and laboratory technicians were adverse events, whereas most of the errors first detected by the attending hospitalists, pharmacists, and consultants were near misses. Drug errors were the most common type of error overall.
Although differences did not achieve statistical significance, Dr. Chaudhry says the data were illuminating and the hospital administration was anxious to clarify the processes of care that could be modified to make the workflow more efficient and the different pieces of each patient’s critical data more integrated.
“For instance,” she says, “at our hospital there was a lot of separation of data. … The vitals were right outside the patient’s room. The list of medications was kept in a central pharmacy location, and the medical chart with everyone’s notes was in a third location.”
After the study’s completion, the integration of data was facilitated by the adoption of an electronic medical record (EMR) and there is ongoing research at that institution concerning whether that has affected error rates.
—Sarwat Chaudhry, MD
Lessons Learned
“This was one of the first and, still I think, only studies of attending physicians reporting their own errors,” says Dr. Chaudhry, “as well as reporting the scope, type, and frequency of the errors.”
There were several lessons learned. The first is that near misses are very common—at least as common as adverse events and perhaps more frequent. The second is that the nature of near misses is similar enough to that of adverse events that they can still be informative in preventing harm to patients. The third lesson arises from the investigators’ review of the kinds of errors that were reported by the different providers. “Different types of providers are going to pick up on different kinds of errors,” says Dr. Chaudhry. “Pharmacy, of course, is going to be detecting drug errors. But nurses are going to be detecting a different kind of error than residents, and residents are detecting a different kind of error than attending physicians.”
Dr. Weingart, who was trained as an internist, says his sense is that “we often pick up errors that occur just upstream in the process of care. For instance, pharmacy finds doctor prescribing errors and nursing finds pharmacy dispensing errors.”
Drs. Chaudhry and Olofinboba discovered 17/47 (36%) of the errors on their own, and pharmacists, resident physicians, consulting physicians, nurses, and ancillary staff discovered the remaining 30/47 (64%). The hospitalists were more likely to detect therapeutic errors; house staff physicians were more likely to detect drug errors. House staff also detected procedural errors at a higher rate than did the hospitalists. Consequently, Dr. Chaudhry emphasizes, another highlight of these data shows that “engaging as many different kinds of healthcare providers in error reporting is very important to understand what’s going on.”
Documenting Errors
The two hospitalists in Dr. Chaudhry’s study underwent no formal training in error detection, and all errors identified were documented. This in itself is a remarkable aspect of this study for hospitalists to note.
“In most hospitals, the risk management department feels like breaking out a bottle of champagne to celebrate every time a physician submits an incident report,” says Dr. Weingart, “because in most hospitals physicians don’t view incident reporting as part of their responsibility. On the other hand, physicians constantly talk about the errors, near misses, and adverse events they encounter day-to-day. Unfortunately, formal incident reporting isn’t an activity that most physicians see as a part of their duty to deliver excellent care at the bedside.” By virtue of this, he says, “critical information is often lost to the system. Error experience is transmitted person-to-person but isn’t captured and analyzed.”
The good news here, however, is that by simply launching a study of this nature and capturing the data it is reasonable to expect that any hospitalist group could take it on and any hospital’s quality of care would be improved.
“There is a spectrum of practice review that is conducted by a variety of people,” says Dr. Chaudhry. “On one end of the spectrum, you have the uninvolved reviewer coming in and doing formal chart reviews … and our process was at other end of spectrum, where we were going about our daily business, the routine clinical care of patients.”
By maintaining the potential for errors at the forefront of their thinking, she says, it became the background against which they performed the constant daily review of patient data. “When I would go to the bedside in the morning,” she says, “to see the patient, talk to the patient, review the chart, look at notes, look at vitals, look at meds—that was my process for picking up on errors.”
—Saul Weingart, MD, PhD
Barriers and Opportunities
There are two major barriers to performing this kind of research in other institutions where hospitalists practice, but they are easily resolved. The first is the importance of standardizing definitions.
“We came to consensus before the study began of what things should count and what things shouldn’t count,” says Dr. Chaudhry. “Because there is a degree of subjectivity and especially when a patient experiences harm, it’s a bit easier to attribute that to an error—though not always. For instance, with a patient with asthma who ends up with fluid overload and gets intubated. Well, was that an error? … Or was that just the patient’s own asthma getting worse? How much did the fluid contribute to that?”
There is still a degree of judgment, even there, she says, “but as much as possible we wanted to come to consensus at least about our definitions, our terminology, and our categorization.”
The second barrier to performing this research is the real or perceived risk of litigation. There was a lot of concern at the beginning of her study, says Dr. Chaudhry (and again at the time of publication), regarding the aftermath of disclosing errors.
“As much as the Institute of Medicine and other accreditation and safety organizations talk about how error reporting is so important and that physicians have to be willing to come forward with their errors, there are really no formal, legal, protective mechanisms in place,” she says, adding that this was true three years ago, and she does not believe much has changed.
Consequently, when constructing the study, she reached out to the authors of other error studies and asked them how they had handled the risk of potential litigation. Most of them told her they did not think there was much risk of being sued, but disclosing errors in the literature is certainly not something an institution or individuals would be clamoring to do. If a multi-center study of this nature might be undertaken, she says, these barriers could be traversed and it would be worth it. “Because if we let that opportunity slip through our fingers, it will be taken on by nonphysicians,” she cautions, “by the external reviewers, by the accreditation organizations, by professional quality control people.”
Dr. Chaudhry’s overall recommendation to hospitalists involves the position they hold at this time. “Hospitalists are ideally poised to take a lead in promoting patient safety by becoming more involved and developing the systems for error reporting,” she says.
Dr. Weingart tells hospitalist audiences that the most important areas for detecting errors in their practice include safe prescription writing and error-proofing high-risk activities (such as hand-offs and sign-outs, and follow-up of test results). He also recommends that hospitalists play the role of responsible citizens in their institutions and be open to ways your patients can contribute by helping you detect errors in their care.4 These issues will be addressed in more detail in future articles in The Hospitalist.
Although Dr. Chaudhry is no longer practicing as a hospitalist, she believes that hospital teams working closely together in patient care have a strong advantage to identify any errors.
“As physicians, with hospital medicine expanding,” she says, “this is the opportune time to take on a leadership role, and this needs to be part of the hospitalist mission. Not everyone has to come out and report their adverse events, especially since the legal risks are still unclear. But a safe way and equally informative way to work on preventing harm is to focus on those near misses.”
Conclusion
Hospitalists who search for near misses, volunteer this information, and enroll their colleagues in doing the same contribute to reforming systems and processes that will ultimately reduce the potential for all errors. Those who pay close attention to standardized rules for prescription-writing, error-proofing high-risk activities, and their roles for institutional citizenship and encouraging patient contribution in regard to possible errors, are doing the best possible job to prevent harm to patients and the institution as a whole. TH
Andrea Sattinger will write about apology in medicine in the June issue.
References
- Kohn LT, Corrigan JM, Donaldson MS, Institute of Medicine Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
- Bleich S. Medical Errors: Five Years After the IOM Report. New York: Commonwealth Fund; July 2005: Available at: www.mihealthandsafety.org/pdfs/pub-4-commonwealth.pdf. Last accessed March 22, 2006.
- Chaudhry SI, Olofinboba KA, Krumholz HM. Detection of errors by attending physicians on a general medicine service. J Gen Intern Med. 2003 Aug;18(8):595-600.
- Weingart SN, Pagovich O, Sands DZ, et al. What can hospitalized patients tell us about adverse events? Learning from patient-reported incidents. J Gen Intern Med. 2005 Sep;20(9):830-836.
Malpractice Primer
Enter text here
Enter text here
Enter text here