User login
An Itchy Neck
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:

- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.

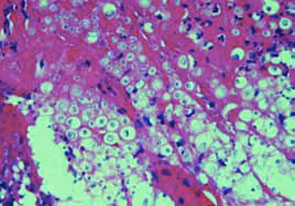
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:
- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:
- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.