User login
NCCN Reaffirms Lung Cancer Screening of Heavy Smokers
The benefits of routine lung cancer screening in high-risk individuals outweigh the potential risks, according to members of a National Comprehensive Cancer Network guidelines panel that recommended low-dose helical CT screening of two high-risk groups.
Mary E. Reid, Ph.D., of the Roswell Park Cancer Institute in Buffalo, N.Y., acknowledged the burdens – in particular, the cost and requisite resource utilization – associated with following all high-risk patients who screen positive. But, she said, "the evidence [in favor of] the recommendations is really strong and supports their implementation."

Lung cancer, she noted, is the only one of the top four deadliest cancers (lung, prostate, breast, and colorectal) that is not currently subject to routine screening.
Dr. Reid and colleagues on the National Comprehensive Cancer Network (NCCN) Guidelines Panel for Lung Cancer Screening presented the update at the NCCN annual conference March 14-18 in Hollywood, Fla. It had been issued in October 2011 and followed a New England Journal of Medicine report that low-dose CT screening of heavy smokers reduced lung cancer mortality by 20%, compared with annual chest x-rays, in the National Lung Screening Trial (NLST).
The revised guidelines recommend annual low-dose helical CT screening for the following two groups of high-risk individuals:
• Those aged 55-74 years with a minimum smoking history of 30 pack-years who either are current smokers or quit within the past 15 years.
• Those aged 50 years or older with a minimum smoking history of 20 pack-years plus one additional lung cancer risk factor, excluding secondhand smoke exposure.
Evidence from the randomized, controlled NLST suggests that early detection via screening reduced lung-cancer specific mortality in the former risk group, which characterizes the NLST patient population. Specifically, 1 in 100 high-risk individuals who were enrolled in the study screened positive on their first low-dose CT exam, and one life was saved for every 320 high-risk individuals screened over 2 years (three screens) (N. Engl. J. Med. 2011;365:395-409). The NCCN recommendation for this group is category 1, the highest level.
The recommendation for annual screening in the second high-risk group is based on less-robust evidence and a nonuniform consensus of the NCCN panel members, Dr. Reid said. As such, it is a less-emphatic category 2B recommendation.
The NCCN screening recommendations have been deemed by some experts to be premature in the absence of cost-efficacy analysis, particularly because of the high false-positive rates observed in both the CT group (96.4%) and the radiography group (94.5%), as well as the potentially harmful effects of radiation exposure associated with low-dose CT screening.
Despite the favorable outcome of their study, the NLST authors stressed the need for rigorous cost-effectiveness analyses before the crafting of public policy recommendations. "The reductions in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote. "The cost component of low-dose CT screening includes not only the screening examination itself but also the diagnostic follow-up and treatment."
In addition to recommending appropriate candidates for routine screening and the proposed frequency of the scans, the new NCCN guidelines outline lung cancer risk factors, address the risks and benefits of screening as well as screening accuracy, and offer an algorithm for the evaluation and follow-up of positive screens.
Specifically, the guidelines recommend the following:
• Basing the frequency of low-dose CT in high-risk patients on the size and status (solid, nonsolid, part-solid, ground-glass, ground-glass opacity) of the nodule on baseline CT.
• Excising all nodules that increase in size or become solid or part-solid during follow-up.
• Considering PET with CT for nodules 8 mm or larger at baseline.
• Performing biopsy or excision of nodules that are suspicious for lung cancer, based on PET with CT findings.
• Reexamining within 1 month solid endobronchial nodules with low-dose CT immediately after vigorous coughing.
• Counseling smokers to quit.
The NCCN is the first professional organization to recommend routine low-dose CT screening for individuals who are considered to be at high-risk for lung cancer, according to Dr. Reid. Last summer, the International Association for the Study of Lung Cancer issued a call for physicians to discuss lung cancer screening with patients who match the high-risk smoking history of those enrolled in the NSLT.
Dr. Reid disclosed no financial conflicts of interest. Disclosures of the NCCN Guidelines Panel for Lung Cancer Screening are online.
Mary E. Reid, Ph.D., Roswell Park Cancer Institute, Lung cancer, NCCN, National Lung Screening Trial, NLST,
The benefits of routine lung cancer screening in high-risk individuals outweigh the potential risks, according to members of a National Comprehensive Cancer Network guidelines panel that recommended low-dose helical CT screening of two high-risk groups.
Mary E. Reid, Ph.D., of the Roswell Park Cancer Institute in Buffalo, N.Y., acknowledged the burdens – in particular, the cost and requisite resource utilization – associated with following all high-risk patients who screen positive. But, she said, "the evidence [in favor of] the recommendations is really strong and supports their implementation."
Lung cancer, she noted, is the only one of the top four deadliest cancers (lung, prostate, breast, and colorectal) that is not currently subject to routine screening.
Dr. Reid and colleagues on the National Comprehensive Cancer Network (NCCN) Guidelines Panel for Lung Cancer Screening presented the update at the NCCN annual conference March 14-18 in Hollywood, Fla. It had been issued in October 2011 and followed a New England Journal of Medicine report that low-dose CT screening of heavy smokers reduced lung cancer mortality by 20%, compared with annual chest x-rays, in the National Lung Screening Trial (NLST).
The revised guidelines recommend annual low-dose helical CT screening for the following two groups of high-risk individuals:
• Those aged 55-74 years with a minimum smoking history of 30 pack-years who either are current smokers or quit within the past 15 years.
• Those aged 50 years or older with a minimum smoking history of 20 pack-years plus one additional lung cancer risk factor, excluding secondhand smoke exposure.
Evidence from the randomized, controlled NLST suggests that early detection via screening reduced lung-cancer specific mortality in the former risk group, which characterizes the NLST patient population. Specifically, 1 in 100 high-risk individuals who were enrolled in the study screened positive on their first low-dose CT exam, and one life was saved for every 320 high-risk individuals screened over 2 years (three screens) (N. Engl. J. Med. 2011;365:395-409). The NCCN recommendation for this group is category 1, the highest level.
The recommendation for annual screening in the second high-risk group is based on less-robust evidence and a nonuniform consensus of the NCCN panel members, Dr. Reid said. As such, it is a less-emphatic category 2B recommendation.
The NCCN screening recommendations have been deemed by some experts to be premature in the absence of cost-efficacy analysis, particularly because of the high false-positive rates observed in both the CT group (96.4%) and the radiography group (94.5%), as well as the potentially harmful effects of radiation exposure associated with low-dose CT screening.
Despite the favorable outcome of their study, the NLST authors stressed the need for rigorous cost-effectiveness analyses before the crafting of public policy recommendations. "The reductions in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote. "The cost component of low-dose CT screening includes not only the screening examination itself but also the diagnostic follow-up and treatment."
In addition to recommending appropriate candidates for routine screening and the proposed frequency of the scans, the new NCCN guidelines outline lung cancer risk factors, address the risks and benefits of screening as well as screening accuracy, and offer an algorithm for the evaluation and follow-up of positive screens.
Specifically, the guidelines recommend the following:
• Basing the frequency of low-dose CT in high-risk patients on the size and status (solid, nonsolid, part-solid, ground-glass, ground-glass opacity) of the nodule on baseline CT.
• Excising all nodules that increase in size or become solid or part-solid during follow-up.
• Considering PET with CT for nodules 8 mm or larger at baseline.
• Performing biopsy or excision of nodules that are suspicious for lung cancer, based on PET with CT findings.
• Reexamining within 1 month solid endobronchial nodules with low-dose CT immediately after vigorous coughing.
• Counseling smokers to quit.
The NCCN is the first professional organization to recommend routine low-dose CT screening for individuals who are considered to be at high-risk for lung cancer, according to Dr. Reid. Last summer, the International Association for the Study of Lung Cancer issued a call for physicians to discuss lung cancer screening with patients who match the high-risk smoking history of those enrolled in the NSLT.
Dr. Reid disclosed no financial conflicts of interest. Disclosures of the NCCN Guidelines Panel for Lung Cancer Screening are online.
The benefits of routine lung cancer screening in high-risk individuals outweigh the potential risks, according to members of a National Comprehensive Cancer Network guidelines panel that recommended low-dose helical CT screening of two high-risk groups.
Mary E. Reid, Ph.D., of the Roswell Park Cancer Institute in Buffalo, N.Y., acknowledged the burdens – in particular, the cost and requisite resource utilization – associated with following all high-risk patients who screen positive. But, she said, "the evidence [in favor of] the recommendations is really strong and supports their implementation."
Lung cancer, she noted, is the only one of the top four deadliest cancers (lung, prostate, breast, and colorectal) that is not currently subject to routine screening.
Dr. Reid and colleagues on the National Comprehensive Cancer Network (NCCN) Guidelines Panel for Lung Cancer Screening presented the update at the NCCN annual conference March 14-18 in Hollywood, Fla. It had been issued in October 2011 and followed a New England Journal of Medicine report that low-dose CT screening of heavy smokers reduced lung cancer mortality by 20%, compared with annual chest x-rays, in the National Lung Screening Trial (NLST).
The revised guidelines recommend annual low-dose helical CT screening for the following two groups of high-risk individuals:
• Those aged 55-74 years with a minimum smoking history of 30 pack-years who either are current smokers or quit within the past 15 years.
• Those aged 50 years or older with a minimum smoking history of 20 pack-years plus one additional lung cancer risk factor, excluding secondhand smoke exposure.
Evidence from the randomized, controlled NLST suggests that early detection via screening reduced lung-cancer specific mortality in the former risk group, which characterizes the NLST patient population. Specifically, 1 in 100 high-risk individuals who were enrolled in the study screened positive on their first low-dose CT exam, and one life was saved for every 320 high-risk individuals screened over 2 years (three screens) (N. Engl. J. Med. 2011;365:395-409). The NCCN recommendation for this group is category 1, the highest level.
The recommendation for annual screening in the second high-risk group is based on less-robust evidence and a nonuniform consensus of the NCCN panel members, Dr. Reid said. As such, it is a less-emphatic category 2B recommendation.
The NCCN screening recommendations have been deemed by some experts to be premature in the absence of cost-efficacy analysis, particularly because of the high false-positive rates observed in both the CT group (96.4%) and the radiography group (94.5%), as well as the potentially harmful effects of radiation exposure associated with low-dose CT screening.
Despite the favorable outcome of their study, the NLST authors stressed the need for rigorous cost-effectiveness analyses before the crafting of public policy recommendations. "The reductions in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote. "The cost component of low-dose CT screening includes not only the screening examination itself but also the diagnostic follow-up and treatment."
In addition to recommending appropriate candidates for routine screening and the proposed frequency of the scans, the new NCCN guidelines outline lung cancer risk factors, address the risks and benefits of screening as well as screening accuracy, and offer an algorithm for the evaluation and follow-up of positive screens.
Specifically, the guidelines recommend the following:
• Basing the frequency of low-dose CT in high-risk patients on the size and status (solid, nonsolid, part-solid, ground-glass, ground-glass opacity) of the nodule on baseline CT.
• Excising all nodules that increase in size or become solid or part-solid during follow-up.
• Considering PET with CT for nodules 8 mm or larger at baseline.
• Performing biopsy or excision of nodules that are suspicious for lung cancer, based on PET with CT findings.
• Reexamining within 1 month solid endobronchial nodules with low-dose CT immediately after vigorous coughing.
• Counseling smokers to quit.
The NCCN is the first professional organization to recommend routine low-dose CT screening for individuals who are considered to be at high-risk for lung cancer, according to Dr. Reid. Last summer, the International Association for the Study of Lung Cancer issued a call for physicians to discuss lung cancer screening with patients who match the high-risk smoking history of those enrolled in the NSLT.
Dr. Reid disclosed no financial conflicts of interest. Disclosures of the NCCN Guidelines Panel for Lung Cancer Screening are online.
Mary E. Reid, Ph.D., Roswell Park Cancer Institute, Lung cancer, NCCN, National Lung Screening Trial, NLST,
Mary E. Reid, Ph.D., Roswell Park Cancer Institute, Lung cancer, NCCN, National Lung Screening Trial, NLST,
FROM THE ANNUAL CONFERENCE OF THE NATIONAL COMPREHENSIVE CANCER NETWORK
NCCN Cancer Guidelines Focus on Adolescent, Young Adult Needs
New guidelines from the National Comprehensive Cancer Network recognize adolescent and young adult cancer patients as a distinct group with needs that are not being met by routine care for adults or for children.
The adolescent and young adult (AYA) oncology guidelines call for referral of these patients to cancer centers specializing in their age group as well as the individual’s specific type of cancer. The guidelines advocate a host of supportive services, including psychosocial assessment and fertility preservation counseling.
AYA patients are diagnosed with cancer when 15-39 years of age. They account for more than 70,000 new cancers every year, and their 5-year survival rate is lower than that of any other age group, according to Dr. Peter F. Coccia, chair of the National Comprehensive Cancer Network (NCCN) panel that made the recommendations.
Dr. Coccia, section chief, hematology/oncology at the University of Nebraska Medical Center in Omaha, presented the new guidelines along with Bradley J. Zebrack, Ph.D., of the University of Michigan Comprehensive Cancer Center in Ann Arbor, during the annual conference of the NCCN in Hollywood, Fla.
The frequency and distribution of cancer types that affect patients in this age demographic differ from the range in the pediatric and adult oncology populations, Dr. Coccia said in an interview. The best outcomes for adolescent and young adult patients are seen in patients with "pediatric-type" cancers, such as acute lymphoblastic leukemia and bone and soft-tissue sarcomas. Patients with adult-onset cancers, such as breast and colon cancer, have the worst outcomes.
He attributed the lack of survival gains to low enrollment in clinical trials (approximately 10% of 15- to 19-year-old patients and 1%-2% of 20- to 39-year-old patients), insufficient health insurance, inconsistent access to routine health care – and thus limited access to early diagnosis and aggressive early therapy – and reduced compliance with prescribed treatments.
Further distinguishing this patient group are the unique, age-related social and developmental considerations, according to Dr. Zebrack. This is the period when individuals establish their identity. "They are separating from their parents, becoming more involved with peers and dating, developing a sexual identity, and making decisions about the education, careers, and families," he said.
With their cancer diagnosis, they are confronting mortality before they would otherwise have to and considering the possible loss of reproductive capacity, he elaborated. They are becoming more versus less dependent on their parents and their plans for the future are being disrupted.
All of these considerations warrant specialized oncology and support services that are designed to focus on the unique biological, clinical, psychosocial, and survivorship issues of the age group, according to the guidelines. "The distinct biology of disease as well as other age-related issues in the AYA population [fertility, long-term side effects, insurance/financial issues, transportation to clinic appointments, child care, psychosocial support, and adherence to therapy] should be considered in the treatment decision-making process," the authors wrote.
In addition to advising that AYA cancer patients be referred to cancer centers "with expertise and experience in treating patients in this age group and the cancers that affect them," the guidelines strongly encourage participation in clinical trials as a way to improve access to state-of-the art treatment and to provide critical insight into the optimal management for this group, according to Dr. Coccia.
The guidelines advise the following for AYA patients:
– Undergo a comprehensive assessment following the cancer diagnosis, including psychosocial assessment, discussion of infertility risks, options for fertility preservation, and genetic and familial risk assessment within 2 months of treatment initiation.
– Be managed by a multidisciplinary team comprising experts in cancer treatment and in specific developmental issues such as fertility, education, career development, employment, family planning, pregnancy, sexually transmitted diseases, and substance use.
– Be treated with aggressive therapy in the absence of contraindications, accompanied by appropriate management of symptoms and side effects to minimize treatment severity and toxicity.
– Be apprised at the time of diagnosis of the risk of infertility due to cancer treatment and be referred to a fertility preservation clinic within 24 hours when appropriate and desired.
– Be apprised of and evaluated for treatment-associated risks in the case of pregnancy and be referred to a gynecologic oncologist and perinatologist with expertise and knowledge of the physiological changes that occur during pregnancy.
– Undergo assessment for developmentally appropriate psychosocial and supportive care across multiple domains, including individual function (developmental, emotional, and behavioral issues); relationships (family, peer, and health care provider); socioeconomic issues; and supportive care interventions.
– Be offered interdisciplinary palliative and end-of-life care as needed to control symptoms, relieve suffering, and improve patient and family quality of life.
To address the increased risk of late effects related to cancer treatment and the risk for long-term effects among AYA cancer survivors, the guidelines recommend cardiovascular, pulmonary, neuroendocrine, renal, gonadal, and neuropsychological screening interventions adapted from the Children’s Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers, which are based on treatment exposure.
Of critical importance, according to Dr. Zebrack, "every member of the [management] team must be trained in how to communicate with teens and young adults to make sure all of their needs are understood and are being met."
Some members of the NCCN AYA Oncology Panel disclosed financial and research relationships with multiple companies.
New guidelines from the National Comprehensive Cancer Network recognize adolescent and young adult cancer patients as a distinct group with needs that are not being met by routine care for adults or for children.
The adolescent and young adult (AYA) oncology guidelines call for referral of these patients to cancer centers specializing in their age group as well as the individual’s specific type of cancer. The guidelines advocate a host of supportive services, including psychosocial assessment and fertility preservation counseling.
AYA patients are diagnosed with cancer when 15-39 years of age. They account for more than 70,000 new cancers every year, and their 5-year survival rate is lower than that of any other age group, according to Dr. Peter F. Coccia, chair of the National Comprehensive Cancer Network (NCCN) panel that made the recommendations.
Dr. Coccia, section chief, hematology/oncology at the University of Nebraska Medical Center in Omaha, presented the new guidelines along with Bradley J. Zebrack, Ph.D., of the University of Michigan Comprehensive Cancer Center in Ann Arbor, during the annual conference of the NCCN in Hollywood, Fla.
The frequency and distribution of cancer types that affect patients in this age demographic differ from the range in the pediatric and adult oncology populations, Dr. Coccia said in an interview. The best outcomes for adolescent and young adult patients are seen in patients with "pediatric-type" cancers, such as acute lymphoblastic leukemia and bone and soft-tissue sarcomas. Patients with adult-onset cancers, such as breast and colon cancer, have the worst outcomes.
He attributed the lack of survival gains to low enrollment in clinical trials (approximately 10% of 15- to 19-year-old patients and 1%-2% of 20- to 39-year-old patients), insufficient health insurance, inconsistent access to routine health care – and thus limited access to early diagnosis and aggressive early therapy – and reduced compliance with prescribed treatments.
Further distinguishing this patient group are the unique, age-related social and developmental considerations, according to Dr. Zebrack. This is the period when individuals establish their identity. "They are separating from their parents, becoming more involved with peers and dating, developing a sexual identity, and making decisions about the education, careers, and families," he said.
With their cancer diagnosis, they are confronting mortality before they would otherwise have to and considering the possible loss of reproductive capacity, he elaborated. They are becoming more versus less dependent on their parents and their plans for the future are being disrupted.
All of these considerations warrant specialized oncology and support services that are designed to focus on the unique biological, clinical, psychosocial, and survivorship issues of the age group, according to the guidelines. "The distinct biology of disease as well as other age-related issues in the AYA population [fertility, long-term side effects, insurance/financial issues, transportation to clinic appointments, child care, psychosocial support, and adherence to therapy] should be considered in the treatment decision-making process," the authors wrote.
In addition to advising that AYA cancer patients be referred to cancer centers "with expertise and experience in treating patients in this age group and the cancers that affect them," the guidelines strongly encourage participation in clinical trials as a way to improve access to state-of-the art treatment and to provide critical insight into the optimal management for this group, according to Dr. Coccia.
The guidelines advise the following for AYA patients:
– Undergo a comprehensive assessment following the cancer diagnosis, including psychosocial assessment, discussion of infertility risks, options for fertility preservation, and genetic and familial risk assessment within 2 months of treatment initiation.
– Be managed by a multidisciplinary team comprising experts in cancer treatment and in specific developmental issues such as fertility, education, career development, employment, family planning, pregnancy, sexually transmitted diseases, and substance use.
– Be treated with aggressive therapy in the absence of contraindications, accompanied by appropriate management of symptoms and side effects to minimize treatment severity and toxicity.
– Be apprised at the time of diagnosis of the risk of infertility due to cancer treatment and be referred to a fertility preservation clinic within 24 hours when appropriate and desired.
– Be apprised of and evaluated for treatment-associated risks in the case of pregnancy and be referred to a gynecologic oncologist and perinatologist with expertise and knowledge of the physiological changes that occur during pregnancy.
– Undergo assessment for developmentally appropriate psychosocial and supportive care across multiple domains, including individual function (developmental, emotional, and behavioral issues); relationships (family, peer, and health care provider); socioeconomic issues; and supportive care interventions.
– Be offered interdisciplinary palliative and end-of-life care as needed to control symptoms, relieve suffering, and improve patient and family quality of life.
To address the increased risk of late effects related to cancer treatment and the risk for long-term effects among AYA cancer survivors, the guidelines recommend cardiovascular, pulmonary, neuroendocrine, renal, gonadal, and neuropsychological screening interventions adapted from the Children’s Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers, which are based on treatment exposure.
Of critical importance, according to Dr. Zebrack, "every member of the [management] team must be trained in how to communicate with teens and young adults to make sure all of their needs are understood and are being met."
Some members of the NCCN AYA Oncology Panel disclosed financial and research relationships with multiple companies.
New guidelines from the National Comprehensive Cancer Network recognize adolescent and young adult cancer patients as a distinct group with needs that are not being met by routine care for adults or for children.
The adolescent and young adult (AYA) oncology guidelines call for referral of these patients to cancer centers specializing in their age group as well as the individual’s specific type of cancer. The guidelines advocate a host of supportive services, including psychosocial assessment and fertility preservation counseling.
AYA patients are diagnosed with cancer when 15-39 years of age. They account for more than 70,000 new cancers every year, and their 5-year survival rate is lower than that of any other age group, according to Dr. Peter F. Coccia, chair of the National Comprehensive Cancer Network (NCCN) panel that made the recommendations.
Dr. Coccia, section chief, hematology/oncology at the University of Nebraska Medical Center in Omaha, presented the new guidelines along with Bradley J. Zebrack, Ph.D., of the University of Michigan Comprehensive Cancer Center in Ann Arbor, during the annual conference of the NCCN in Hollywood, Fla.
The frequency and distribution of cancer types that affect patients in this age demographic differ from the range in the pediatric and adult oncology populations, Dr. Coccia said in an interview. The best outcomes for adolescent and young adult patients are seen in patients with "pediatric-type" cancers, such as acute lymphoblastic leukemia and bone and soft-tissue sarcomas. Patients with adult-onset cancers, such as breast and colon cancer, have the worst outcomes.
He attributed the lack of survival gains to low enrollment in clinical trials (approximately 10% of 15- to 19-year-old patients and 1%-2% of 20- to 39-year-old patients), insufficient health insurance, inconsistent access to routine health care – and thus limited access to early diagnosis and aggressive early therapy – and reduced compliance with prescribed treatments.
Further distinguishing this patient group are the unique, age-related social and developmental considerations, according to Dr. Zebrack. This is the period when individuals establish their identity. "They are separating from their parents, becoming more involved with peers and dating, developing a sexual identity, and making decisions about the education, careers, and families," he said.
With their cancer diagnosis, they are confronting mortality before they would otherwise have to and considering the possible loss of reproductive capacity, he elaborated. They are becoming more versus less dependent on their parents and their plans for the future are being disrupted.
All of these considerations warrant specialized oncology and support services that are designed to focus on the unique biological, clinical, psychosocial, and survivorship issues of the age group, according to the guidelines. "The distinct biology of disease as well as other age-related issues in the AYA population [fertility, long-term side effects, insurance/financial issues, transportation to clinic appointments, child care, psychosocial support, and adherence to therapy] should be considered in the treatment decision-making process," the authors wrote.
In addition to advising that AYA cancer patients be referred to cancer centers "with expertise and experience in treating patients in this age group and the cancers that affect them," the guidelines strongly encourage participation in clinical trials as a way to improve access to state-of-the art treatment and to provide critical insight into the optimal management for this group, according to Dr. Coccia.
The guidelines advise the following for AYA patients:
– Undergo a comprehensive assessment following the cancer diagnosis, including psychosocial assessment, discussion of infertility risks, options for fertility preservation, and genetic and familial risk assessment within 2 months of treatment initiation.
– Be managed by a multidisciplinary team comprising experts in cancer treatment and in specific developmental issues such as fertility, education, career development, employment, family planning, pregnancy, sexually transmitted diseases, and substance use.
– Be treated with aggressive therapy in the absence of contraindications, accompanied by appropriate management of symptoms and side effects to minimize treatment severity and toxicity.
– Be apprised at the time of diagnosis of the risk of infertility due to cancer treatment and be referred to a fertility preservation clinic within 24 hours when appropriate and desired.
– Be apprised of and evaluated for treatment-associated risks in the case of pregnancy and be referred to a gynecologic oncologist and perinatologist with expertise and knowledge of the physiological changes that occur during pregnancy.
– Undergo assessment for developmentally appropriate psychosocial and supportive care across multiple domains, including individual function (developmental, emotional, and behavioral issues); relationships (family, peer, and health care provider); socioeconomic issues; and supportive care interventions.
– Be offered interdisciplinary palliative and end-of-life care as needed to control symptoms, relieve suffering, and improve patient and family quality of life.
To address the increased risk of late effects related to cancer treatment and the risk for long-term effects among AYA cancer survivors, the guidelines recommend cardiovascular, pulmonary, neuroendocrine, renal, gonadal, and neuropsychological screening interventions adapted from the Children’s Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers, which are based on treatment exposure.
Of critical importance, according to Dr. Zebrack, "every member of the [management] team must be trained in how to communicate with teens and young adults to make sure all of their needs are understood and are being met."
Some members of the NCCN AYA Oncology Panel disclosed financial and research relationships with multiple companies.
Breath Markers May Improve Lung Cancer Screening
New noninvasive screening technologies are poised to improve the diagnostic yield of advanced imaging in lung cancer and, by so doing, improve patient outcomes. A blood test for detecting genetic mutations in circulating tumor cells of lung cancer specimens and a colorimetric sensor array that identifies cancerous compounds in exhaled human breath are among the technologies that could lead to earlier diagnosis and treatment, said Dr. Paul A. Bunn, executive director of the International Association for the Study of Lung Cancer (IASLC).
Lung cancer treatment has been hampered in the past by late diagnoses, typically achieved using invasive procedures only after symptoms have presented, said Dr. Bunn, the James Dudley Professor of Lung Cancer Research at the University of Colorado at Denver.
"Major breakthroughs are leading to interventions that make a huge difference and make it an exciting time for lung cancer," he said.
In particular, a test identifying lung cancer biomarkers through exhaled breath may also help clinicians and researchers identify which patients with abnormal CT scans need more aggressive follow-up. Dr. Nir Peled of Tel Hashomer, Israel, presented data from a comparative survey using breath analyses, in which investigators captured the "metabolic biosignatures" – the pattern of volatile organic compounds (VOCs) – of 74 patients with solitary pulmonary nodules to determine the VOC profiles for malignant and benign lung nodules.
"On analysis, two [VOCs] in patients’ exhaled breath showed statistically significant differences in concentration for benign and malignant lung nodules, and the sensor array distinguished between the corresponding collective VOC patterns with nearly 90% accuracy," Dr. Peled said in an interview.
Further, looking specifically at the malignant nodules, "the sensor array distinguished between small and non–small cell lung cancer with an accuracy approaching 94% and between early and advanced disease with nearly 90% accuracy."
Dr. Peled reported no disclosures.
New noninvasive screening technologies are poised to improve the diagnostic yield of advanced imaging in lung cancer and, by so doing, improve patient outcomes. A blood test for detecting genetic mutations in circulating tumor cells of lung cancer specimens and a colorimetric sensor array that identifies cancerous compounds in exhaled human breath are among the technologies that could lead to earlier diagnosis and treatment, said Dr. Paul A. Bunn, executive director of the International Association for the Study of Lung Cancer (IASLC).
Lung cancer treatment has been hampered in the past by late diagnoses, typically achieved using invasive procedures only after symptoms have presented, said Dr. Bunn, the James Dudley Professor of Lung Cancer Research at the University of Colorado at Denver.
"Major breakthroughs are leading to interventions that make a huge difference and make it an exciting time for lung cancer," he said.
In particular, a test identifying lung cancer biomarkers through exhaled breath may also help clinicians and researchers identify which patients with abnormal CT scans need more aggressive follow-up. Dr. Nir Peled of Tel Hashomer, Israel, presented data from a comparative survey using breath analyses, in which investigators captured the "metabolic biosignatures" – the pattern of volatile organic compounds (VOCs) – of 74 patients with solitary pulmonary nodules to determine the VOC profiles for malignant and benign lung nodules.
"On analysis, two [VOCs] in patients’ exhaled breath showed statistically significant differences in concentration for benign and malignant lung nodules, and the sensor array distinguished between the corresponding collective VOC patterns with nearly 90% accuracy," Dr. Peled said in an interview.
Further, looking specifically at the malignant nodules, "the sensor array distinguished between small and non–small cell lung cancer with an accuracy approaching 94% and between early and advanced disease with nearly 90% accuracy."
Dr. Peled reported no disclosures.
New noninvasive screening technologies are poised to improve the diagnostic yield of advanced imaging in lung cancer and, by so doing, improve patient outcomes. A blood test for detecting genetic mutations in circulating tumor cells of lung cancer specimens and a colorimetric sensor array that identifies cancerous compounds in exhaled human breath are among the technologies that could lead to earlier diagnosis and treatment, said Dr. Paul A. Bunn, executive director of the International Association for the Study of Lung Cancer (IASLC).
Lung cancer treatment has been hampered in the past by late diagnoses, typically achieved using invasive procedures only after symptoms have presented, said Dr. Bunn, the James Dudley Professor of Lung Cancer Research at the University of Colorado at Denver.
"Major breakthroughs are leading to interventions that make a huge difference and make it an exciting time for lung cancer," he said.
In particular, a test identifying lung cancer biomarkers through exhaled breath may also help clinicians and researchers identify which patients with abnormal CT scans need more aggressive follow-up. Dr. Nir Peled of Tel Hashomer, Israel, presented data from a comparative survey using breath analyses, in which investigators captured the "metabolic biosignatures" – the pattern of volatile organic compounds (VOCs) – of 74 patients with solitary pulmonary nodules to determine the VOC profiles for malignant and benign lung nodules.
"On analysis, two [VOCs] in patients’ exhaled breath showed statistically significant differences in concentration for benign and malignant lung nodules, and the sensor array distinguished between the corresponding collective VOC patterns with nearly 90% accuracy," Dr. Peled said in an interview.
Further, looking specifically at the malignant nodules, "the sensor array distinguished between small and non–small cell lung cancer with an accuracy approaching 94% and between early and advanced disease with nearly 90% accuracy."
Dr. Peled reported no disclosures.
Breath Markers May Improve Lung Cancer Screening
New noninvasive screening technologies are poised to improve the diagnostic yield of advanced imaging in lung cancer and, by so doing, improve patient outcomes. A blood test for detecting genetic mutations in circulating tumor cells of lung cancer specimens and a colorimetric sensor array that identifies cancerous compounds in exhaled human breath are among the technologies that could lead to earlier diagnosis and treatment, said Dr. Paul A. Bunn, executive director of the International Association for the Study of Lung Cancer (IASLC).
Lung cancer treatment has been hampered in the past by late diagnoses, typically achieved using invasive procedures only after symptoms have presented, said Dr. Bunn, the James Dudley Professor of Lung Cancer Research at the University of Colorado at Denver.
"Major breakthroughs are leading to interventions that make a huge difference and make it an exciting time for lung cancer," he said.
In particular, a test identifying lung cancer biomarkers through exhaled breath may also help clinicians and researchers identify which patients with abnormal CT scans need more aggressive follow-up. Dr. Nir Peled of Tel Hashomer, Israel, presented data from a comparative survey using breath analyses, in which investigators captured the "metabolic biosignatures" – the pattern of volatile organic compounds (VOCs) – of 74 patients with solitary pulmonary nodules to determine the VOC profiles for malignant and benign lung nodules.
"On analysis, two [VOCs] in patients’ exhaled breath showed statistically significant differences in concentration for benign and malignant lung nodules, and the sensor array distinguished between the corresponding collective VOC patterns with nearly 90% accuracy," Dr. Peled said in an interview.
Further, looking specifically at the malignant nodules, "the sensor array distinguished between small and non–small cell lung cancer with an accuracy approaching 94% and between early and advanced disease with nearly 90% accuracy."
Dr. Peled reported no disclosures.
New noninvasive screening technologies are poised to improve the diagnostic yield of advanced imaging in lung cancer and, by so doing, improve patient outcomes. A blood test for detecting genetic mutations in circulating tumor cells of lung cancer specimens and a colorimetric sensor array that identifies cancerous compounds in exhaled human breath are among the technologies that could lead to earlier diagnosis and treatment, said Dr. Paul A. Bunn, executive director of the International Association for the Study of Lung Cancer (IASLC).
Lung cancer treatment has been hampered in the past by late diagnoses, typically achieved using invasive procedures only after symptoms have presented, said Dr. Bunn, the James Dudley Professor of Lung Cancer Research at the University of Colorado at Denver.
"Major breakthroughs are leading to interventions that make a huge difference and make it an exciting time for lung cancer," he said.
In particular, a test identifying lung cancer biomarkers through exhaled breath may also help clinicians and researchers identify which patients with abnormal CT scans need more aggressive follow-up. Dr. Nir Peled of Tel Hashomer, Israel, presented data from a comparative survey using breath analyses, in which investigators captured the "metabolic biosignatures" – the pattern of volatile organic compounds (VOCs) – of 74 patients with solitary pulmonary nodules to determine the VOC profiles for malignant and benign lung nodules.
"On analysis, two [VOCs] in patients’ exhaled breath showed statistically significant differences in concentration for benign and malignant lung nodules, and the sensor array distinguished between the corresponding collective VOC patterns with nearly 90% accuracy," Dr. Peled said in an interview.
Further, looking specifically at the malignant nodules, "the sensor array distinguished between small and non–small cell lung cancer with an accuracy approaching 94% and between early and advanced disease with nearly 90% accuracy."
Dr. Peled reported no disclosures.
New noninvasive screening technologies are poised to improve the diagnostic yield of advanced imaging in lung cancer and, by so doing, improve patient outcomes. A blood test for detecting genetic mutations in circulating tumor cells of lung cancer specimens and a colorimetric sensor array that identifies cancerous compounds in exhaled human breath are among the technologies that could lead to earlier diagnosis and treatment, said Dr. Paul A. Bunn, executive director of the International Association for the Study of Lung Cancer (IASLC).
Lung cancer treatment has been hampered in the past by late diagnoses, typically achieved using invasive procedures only after symptoms have presented, said Dr. Bunn, the James Dudley Professor of Lung Cancer Research at the University of Colorado at Denver.
"Major breakthroughs are leading to interventions that make a huge difference and make it an exciting time for lung cancer," he said.
In particular, a test identifying lung cancer biomarkers through exhaled breath may also help clinicians and researchers identify which patients with abnormal CT scans need more aggressive follow-up. Dr. Nir Peled of Tel Hashomer, Israel, presented data from a comparative survey using breath analyses, in which investigators captured the "metabolic biosignatures" – the pattern of volatile organic compounds (VOCs) – of 74 patients with solitary pulmonary nodules to determine the VOC profiles for malignant and benign lung nodules.
"On analysis, two [VOCs] in patients’ exhaled breath showed statistically significant differences in concentration for benign and malignant lung nodules, and the sensor array distinguished between the corresponding collective VOC patterns with nearly 90% accuracy," Dr. Peled said in an interview.
Further, looking specifically at the malignant nodules, "the sensor array distinguished between small and non–small cell lung cancer with an accuracy approaching 94% and between early and advanced disease with nearly 90% accuracy."
Dr. Peled reported no disclosures.
Feeding Regimen Moot For Critical ALI Patients?
HOUSTON – Restricting the amount of initial enteral intake in mechanically ventilated patients who have acute lung injury neither reduces the duration of mechanical ventilation nor improves mortality relative to full enteral feeding, but the nutritional strategy may be slightly easier on the stomach, according to a study reported at the annual congress of the Society of Critical Care Medicine.
The importance of nutrition support in critically ill patients with acute lung injury (ALI) is well accepted as a means of maintaining gut integrity, modulating both stress and the systemic immune response, and attenuating disease severity, but conflicting data regarding the timing, formulation, and amount of enteral nutrition have contributed to uncertainty about the optimal feeding protocol, according to Dr. Todd W. Rice of Vanderbilt University Medical Center in Nashville, Tenn.
"How much nutrition we need to promote the protective benefits, we don’t know. Providing a little bit of nutrition (called trophic feeding) has been shown to decrease intestinal intolerances, compared with full-calorie feeds, but it may do so at the risk of malnutrition, worse immune function, and loss of muscle strength," he said. Full-calorie feeding, on the other hand, may lead to more intolerances, may cause hyperglycemia and other imbalances, may increase septic complications, and may fuel the inflammatory fire, he added.
In the current study, which was published simultaneously in JAMA, Dr. Rice and colleagues in the EDEN (Early vs. Delayed Enteral Nutrition in ALI) trial sought to examine the relative advantages of restricting the amount of initial enteral intake in mechanically ventilated ALI patients. Specifically, the prospective, randomized, open-label trial compared the effect on clinical outcomes and survival of initial trophic enteral feeding – approximately 25% of the full target feeding – with initial full-calorie feeding for the first 6 days of mechanical ventilation in ALI patients. "We hypothesized that reduced trophic feeding during the first [6 days] would increase ventilator-free days and reduce instances of gastrointestinal intolerances compared with the conventional full enteral nutrition strategy," he said.
The study’s primary end point was ventilator-free days through day 28; secondary end points were daily percentage of goal enteral feeding, frequency of gastrointestinal intolerances, 60-day mortality before hospital discharge with unassisted breathing, ICU- and organ failure–free days, and new infections (JAMA 2012 Feb. 5[doi:10.1001/jama2012.137]).
The multicenter study population comprised 1,000 patients, from January 2008 through mid-April 2011, who were initiated on mechanical ventilation within 48 hours of developing ALI. Within 6 hours of randomization, enteric nutrition was initiated in 508 patients assigned to trophic nutrition and 492 assigned to full feeding, and was continued until death, extubation, or day 6, Dr. Rice explained. Per standard protocol, enteral nutrition in the full-feeding group began at 25 mL/hr and advanced to goal weights (25-30 kcal/day of nonprotein calories and 1.2-1.6 g/kg per day of protein) as quickly as possible; gastric residual volumes were checked every 6 hours while enteral feeding was increased. In the trophic group, enteral feeding was initiated at 10-20 kcal/hr and gastric residual volumes were checked every 12 hours. After 6 days, patients in the trophic group who still required mechanical ventilation were advanced to the full-energy feeding rates, he said.
Baseline characteristics of the two groups were similar, Dr. Rice noted. "The primary etiologies of lung injury in both groups of patients were pneumonia and sepsis, and the average APACHE III [Acute Physiology and Chronic Health Evaluation III] score was approximately 92. These were sick patients," he said. For the first 6 days, the full- and trophic feeding groups received 1,300 kcal/day and 400 kcal/day, respectively.
With respect to the primary end point (28 days), the average number of ventilator-free days in both groups was similar, at 14.9 in the trophic group and 15.0 in the full-feeding group. "There were also no differences in 60-day mortality, organ failure–free days, ICU-free days, or the incidence of infection between groups," he said. Similarly, with respect to body mass index category or lung injury severity, "there were no between-group differences in ventilator free days or survival."
The full-feeding group did have a higher number of gastrointestinal intolerances on any one day, and statistically significant increase on days 2 and 3, but the overall percentages of intolerances were low, Dr. Rice said. There were no differences in albumin and protein levels between the groups over the first 7 days, he said.
Regarding the immediate clinical relevance of the findings, Dr. Rice stressed that the study wasn’t designed as an equivalence trial, "so I can’t tell you both feeding strategies are similar, but you can look at the results." In fact, he said, although the study did not show a benefit other than improved gastrointestinal tolerance, his group has moved toward trophic feeds because of the ease of administration
Dr. Rice had no financial conflicts.
HOUSTON – Restricting the amount of initial enteral intake in mechanically ventilated patients who have acute lung injury neither reduces the duration of mechanical ventilation nor improves mortality relative to full enteral feeding, but the nutritional strategy may be slightly easier on the stomach, according to a study reported at the annual congress of the Society of Critical Care Medicine.
The importance of nutrition support in critically ill patients with acute lung injury (ALI) is well accepted as a means of maintaining gut integrity, modulating both stress and the systemic immune response, and attenuating disease severity, but conflicting data regarding the timing, formulation, and amount of enteral nutrition have contributed to uncertainty about the optimal feeding protocol, according to Dr. Todd W. Rice of Vanderbilt University Medical Center in Nashville, Tenn.
"How much nutrition we need to promote the protective benefits, we don’t know. Providing a little bit of nutrition (called trophic feeding) has been shown to decrease intestinal intolerances, compared with full-calorie feeds, but it may do so at the risk of malnutrition, worse immune function, and loss of muscle strength," he said. Full-calorie feeding, on the other hand, may lead to more intolerances, may cause hyperglycemia and other imbalances, may increase septic complications, and may fuel the inflammatory fire, he added.
In the current study, which was published simultaneously in JAMA, Dr. Rice and colleagues in the EDEN (Early vs. Delayed Enteral Nutrition in ALI) trial sought to examine the relative advantages of restricting the amount of initial enteral intake in mechanically ventilated ALI patients. Specifically, the prospective, randomized, open-label trial compared the effect on clinical outcomes and survival of initial trophic enteral feeding – approximately 25% of the full target feeding – with initial full-calorie feeding for the first 6 days of mechanical ventilation in ALI patients. "We hypothesized that reduced trophic feeding during the first [6 days] would increase ventilator-free days and reduce instances of gastrointestinal intolerances compared with the conventional full enteral nutrition strategy," he said.
The study’s primary end point was ventilator-free days through day 28; secondary end points were daily percentage of goal enteral feeding, frequency of gastrointestinal intolerances, 60-day mortality before hospital discharge with unassisted breathing, ICU- and organ failure–free days, and new infections (JAMA 2012 Feb. 5[doi:10.1001/jama2012.137]).
The multicenter study population comprised 1,000 patients, from January 2008 through mid-April 2011, who were initiated on mechanical ventilation within 48 hours of developing ALI. Within 6 hours of randomization, enteric nutrition was initiated in 508 patients assigned to trophic nutrition and 492 assigned to full feeding, and was continued until death, extubation, or day 6, Dr. Rice explained. Per standard protocol, enteral nutrition in the full-feeding group began at 25 mL/hr and advanced to goal weights (25-30 kcal/day of nonprotein calories and 1.2-1.6 g/kg per day of protein) as quickly as possible; gastric residual volumes were checked every 6 hours while enteral feeding was increased. In the trophic group, enteral feeding was initiated at 10-20 kcal/hr and gastric residual volumes were checked every 12 hours. After 6 days, patients in the trophic group who still required mechanical ventilation were advanced to the full-energy feeding rates, he said.
Baseline characteristics of the two groups were similar, Dr. Rice noted. "The primary etiologies of lung injury in both groups of patients were pneumonia and sepsis, and the average APACHE III [Acute Physiology and Chronic Health Evaluation III] score was approximately 92. These were sick patients," he said. For the first 6 days, the full- and trophic feeding groups received 1,300 kcal/day and 400 kcal/day, respectively.
With respect to the primary end point (28 days), the average number of ventilator-free days in both groups was similar, at 14.9 in the trophic group and 15.0 in the full-feeding group. "There were also no differences in 60-day mortality, organ failure–free days, ICU-free days, or the incidence of infection between groups," he said. Similarly, with respect to body mass index category or lung injury severity, "there were no between-group differences in ventilator free days or survival."
The full-feeding group did have a higher number of gastrointestinal intolerances on any one day, and statistically significant increase on days 2 and 3, but the overall percentages of intolerances were low, Dr. Rice said. There were no differences in albumin and protein levels between the groups over the first 7 days, he said.
Regarding the immediate clinical relevance of the findings, Dr. Rice stressed that the study wasn’t designed as an equivalence trial, "so I can’t tell you both feeding strategies are similar, but you can look at the results." In fact, he said, although the study did not show a benefit other than improved gastrointestinal tolerance, his group has moved toward trophic feeds because of the ease of administration
Dr. Rice had no financial conflicts.
HOUSTON – Restricting the amount of initial enteral intake in mechanically ventilated patients who have acute lung injury neither reduces the duration of mechanical ventilation nor improves mortality relative to full enteral feeding, but the nutritional strategy may be slightly easier on the stomach, according to a study reported at the annual congress of the Society of Critical Care Medicine.
The importance of nutrition support in critically ill patients with acute lung injury (ALI) is well accepted as a means of maintaining gut integrity, modulating both stress and the systemic immune response, and attenuating disease severity, but conflicting data regarding the timing, formulation, and amount of enteral nutrition have contributed to uncertainty about the optimal feeding protocol, according to Dr. Todd W. Rice of Vanderbilt University Medical Center in Nashville, Tenn.
"How much nutrition we need to promote the protective benefits, we don’t know. Providing a little bit of nutrition (called trophic feeding) has been shown to decrease intestinal intolerances, compared with full-calorie feeds, but it may do so at the risk of malnutrition, worse immune function, and loss of muscle strength," he said. Full-calorie feeding, on the other hand, may lead to more intolerances, may cause hyperglycemia and other imbalances, may increase septic complications, and may fuel the inflammatory fire, he added.
In the current study, which was published simultaneously in JAMA, Dr. Rice and colleagues in the EDEN (Early vs. Delayed Enteral Nutrition in ALI) trial sought to examine the relative advantages of restricting the amount of initial enteral intake in mechanically ventilated ALI patients. Specifically, the prospective, randomized, open-label trial compared the effect on clinical outcomes and survival of initial trophic enteral feeding – approximately 25% of the full target feeding – with initial full-calorie feeding for the first 6 days of mechanical ventilation in ALI patients. "We hypothesized that reduced trophic feeding during the first [6 days] would increase ventilator-free days and reduce instances of gastrointestinal intolerances compared with the conventional full enteral nutrition strategy," he said.
The study’s primary end point was ventilator-free days through day 28; secondary end points were daily percentage of goal enteral feeding, frequency of gastrointestinal intolerances, 60-day mortality before hospital discharge with unassisted breathing, ICU- and organ failure–free days, and new infections (JAMA 2012 Feb. 5[doi:10.1001/jama2012.137]).
The multicenter study population comprised 1,000 patients, from January 2008 through mid-April 2011, who were initiated on mechanical ventilation within 48 hours of developing ALI. Within 6 hours of randomization, enteric nutrition was initiated in 508 patients assigned to trophic nutrition and 492 assigned to full feeding, and was continued until death, extubation, or day 6, Dr. Rice explained. Per standard protocol, enteral nutrition in the full-feeding group began at 25 mL/hr and advanced to goal weights (25-30 kcal/day of nonprotein calories and 1.2-1.6 g/kg per day of protein) as quickly as possible; gastric residual volumes were checked every 6 hours while enteral feeding was increased. In the trophic group, enteral feeding was initiated at 10-20 kcal/hr and gastric residual volumes were checked every 12 hours. After 6 days, patients in the trophic group who still required mechanical ventilation were advanced to the full-energy feeding rates, he said.
Baseline characteristics of the two groups were similar, Dr. Rice noted. "The primary etiologies of lung injury in both groups of patients were pneumonia and sepsis, and the average APACHE III [Acute Physiology and Chronic Health Evaluation III] score was approximately 92. These were sick patients," he said. For the first 6 days, the full- and trophic feeding groups received 1,300 kcal/day and 400 kcal/day, respectively.
With respect to the primary end point (28 days), the average number of ventilator-free days in both groups was similar, at 14.9 in the trophic group and 15.0 in the full-feeding group. "There were also no differences in 60-day mortality, organ failure–free days, ICU-free days, or the incidence of infection between groups," he said. Similarly, with respect to body mass index category or lung injury severity, "there were no between-group differences in ventilator free days or survival."
The full-feeding group did have a higher number of gastrointestinal intolerances on any one day, and statistically significant increase on days 2 and 3, but the overall percentages of intolerances were low, Dr. Rice said. There were no differences in albumin and protein levels between the groups over the first 7 days, he said.
Regarding the immediate clinical relevance of the findings, Dr. Rice stressed that the study wasn’t designed as an equivalence trial, "so I can’t tell you both feeding strategies are similar, but you can look at the results." In fact, he said, although the study did not show a benefit other than improved gastrointestinal tolerance, his group has moved toward trophic feeds because of the ease of administration
Dr. Rice had no financial conflicts.
Major Finding: At day 28, the average number of ventilator-free days in ALI patients who had been mechanically ventilated was 14.9 among those who received trophic enteral feeding for the first 6 days, followed by full-calorie feeding, and was 15.0 days among those who received full calorie enteral feeding from the outset.
Data Source: This was a multicenter, randomized, prospective, open-label trial comprising 1,000 mechanically ventilated ALI patients that was designed to assess the effect on clinical outcomes and survival of initial trophic enteral feeding, compared with full-calorie feeding, for the first 6 days of mechanical ventilation.
Disclosures: Dr. Rice and his fellow researchers disclosed having no financial conflicts of interest.
Feeding Regimen Moot For Critical ALI Patients?
HOUSTON – Restricting the amount of initial enteral intake in mechanically ventilated patients who have acute lung injury neither reduces the duration of mechanical ventilation nor improves mortality relative to full enteral feeding, but the nutritional strategy may be slightly easier on the stomach, according to a study reported at the annual congress of the Society of Critical Care Medicine.
The importance of nutrition support in critically ill patients with acute lung injury (ALI) is well accepted as a means of maintaining gut integrity, modulating both stress and the systemic immune response, and attenuating disease severity, but conflicting data regarding the timing, formulation, and amount of enteral nutrition have contributed to uncertainty about the optimal feeding protocol, according to Dr. Todd W. Rice of Vanderbilt University Medical Center in Nashville, Tenn.
"How much nutrition we need to promote the protective benefits, we don’t know. Providing a little bit of nutrition (called trophic feeding) has been shown to decrease intestinal intolerances, compared with full-calorie feeds, but it may do so at the risk of malnutrition, worse immune function, and loss of muscle strength," he said. Full-calorie feeding, on the other hand, may lead to more intolerances, may cause hyperglycemia and other imbalances, may increase septic complications, and may fuel the inflammatory fire, he added.
In the current study, which was published simultaneously in JAMA, Dr. Rice and colleagues in the EDEN (Early vs. Delayed Enteral Nutrition in ALI) trial sought to examine the relative advantages of restricting the amount of initial enteral intake in mechanically ventilated ALI patients. Specifically, the prospective, randomized, open-label trial compared the effect on clinical outcomes and survival of initial trophic enteral feeding – approximately 25% of the full target feeding – with initial full-calorie feeding for the first 6 days of mechanical ventilation in ALI patients. "We hypothesized that reduced trophic feeding during the first [6 days] would increase ventilator-free days and reduce instances of gastrointestinal intolerances compared with the conventional full enteral nutrition strategy," he said.
The study’s primary end point was ventilator-free days through day 28; secondary end points were daily percentage of goal enteral feeding, frequency of gastrointestinal intolerances, 60-day mortality before hospital discharge with unassisted breathing, ICU- and organ failure–free days, and new infections (JAMA 2012 Feb. 5[doi:10.1001/jama2012.137]).
The multicenter study population comprised 1,000 patients, from January 2008 through mid-April 2011, who were initiated on mechanical ventilation within 48 hours of developing ALI. Within 6 hours of randomization, enteric nutrition was initiated in 508 patients assigned to trophic nutrition and 492 assigned to full feeding, and was continued until death, extubation, or day 6, Dr. Rice explained. Per standard protocol, enteral nutrition in the full-feeding group began at 25 mL/hr and advanced to goal weights (25-30 kcal/day of nonprotein calories and 1.2-1.6 g/kg per day of protein) as quickly as possible; gastric residual volumes were checked every 6 hours while enteral feeding was increased. In the trophic group, enteral feeding was initiated at 10-20 kcal/hr and gastric residual volumes were checked every 12 hours. After 6 days, patients in the trophic group who still required mechanical ventilation were advanced to the full-energy feeding rates, he said.
Baseline characteristics of the two groups were similar, Dr. Rice noted. "The primary etiologies of lung injury in both groups of patients were pneumonia and sepsis, and the average APACHE III [Acute Physiology and Chronic Health Evaluation III] score was approximately 92. These were sick patients," he said. For the first 6 days, the full- and trophic feeding groups received 1,300 kcal/day and 400 kcal/day, respectively.
With respect to the primary end point (28 days), the average number of ventilator-free days in both groups was similar, at 14.9 in the trophic group and 15.0 in the full-feeding group. "There were also no differences in 60-day mortality, organ failure–free days, ICU-free days, or the incidence of infection between groups," he said. Similarly, with respect to body mass index category or lung injury severity, "there were no between-group differences in ventilator free days or survival."
The full-feeding group did have a higher number of gastrointestinal intolerances on any one day, and statistically significant increase on days 2 and 3, but the overall percentages of intolerances were low, Dr. Rice said. There were no differences in albumin and protein levels between the groups over the first 7 days, he said.
Regarding the immediate clinical relevance of the findings, Dr. Rice stressed that the study wasn’t designed as an equivalence trial, "so I can’t tell you both feeding strategies are similar, but you can look at the results." In fact, he said, although the study did not show a benefit other than improved gastrointestinal tolerance, his group has moved toward trophic feeds because of the ease of administration
Dr. Rice had no financial conflicts.
HOUSTON – Restricting the amount of initial enteral intake in mechanically ventilated patients who have acute lung injury neither reduces the duration of mechanical ventilation nor improves mortality relative to full enteral feeding, but the nutritional strategy may be slightly easier on the stomach, according to a study reported at the annual congress of the Society of Critical Care Medicine.
The importance of nutrition support in critically ill patients with acute lung injury (ALI) is well accepted as a means of maintaining gut integrity, modulating both stress and the systemic immune response, and attenuating disease severity, but conflicting data regarding the timing, formulation, and amount of enteral nutrition have contributed to uncertainty about the optimal feeding protocol, according to Dr. Todd W. Rice of Vanderbilt University Medical Center in Nashville, Tenn.
"How much nutrition we need to promote the protective benefits, we don’t know. Providing a little bit of nutrition (called trophic feeding) has been shown to decrease intestinal intolerances, compared with full-calorie feeds, but it may do so at the risk of malnutrition, worse immune function, and loss of muscle strength," he said. Full-calorie feeding, on the other hand, may lead to more intolerances, may cause hyperglycemia and other imbalances, may increase septic complications, and may fuel the inflammatory fire, he added.
In the current study, which was published simultaneously in JAMA, Dr. Rice and colleagues in the EDEN (Early vs. Delayed Enteral Nutrition in ALI) trial sought to examine the relative advantages of restricting the amount of initial enteral intake in mechanically ventilated ALI patients. Specifically, the prospective, randomized, open-label trial compared the effect on clinical outcomes and survival of initial trophic enteral feeding – approximately 25% of the full target feeding – with initial full-calorie feeding for the first 6 days of mechanical ventilation in ALI patients. "We hypothesized that reduced trophic feeding during the first [6 days] would increase ventilator-free days and reduce instances of gastrointestinal intolerances compared with the conventional full enteral nutrition strategy," he said.
The study’s primary end point was ventilator-free days through day 28; secondary end points were daily percentage of goal enteral feeding, frequency of gastrointestinal intolerances, 60-day mortality before hospital discharge with unassisted breathing, ICU- and organ failure–free days, and new infections (JAMA 2012 Feb. 5[doi:10.1001/jama2012.137]).
The multicenter study population comprised 1,000 patients, from January 2008 through mid-April 2011, who were initiated on mechanical ventilation within 48 hours of developing ALI. Within 6 hours of randomization, enteric nutrition was initiated in 508 patients assigned to trophic nutrition and 492 assigned to full feeding, and was continued until death, extubation, or day 6, Dr. Rice explained. Per standard protocol, enteral nutrition in the full-feeding group began at 25 mL/hr and advanced to goal weights (25-30 kcal/day of nonprotein calories and 1.2-1.6 g/kg per day of protein) as quickly as possible; gastric residual volumes were checked every 6 hours while enteral feeding was increased. In the trophic group, enteral feeding was initiated at 10-20 kcal/hr and gastric residual volumes were checked every 12 hours. After 6 days, patients in the trophic group who still required mechanical ventilation were advanced to the full-energy feeding rates, he said.
Baseline characteristics of the two groups were similar, Dr. Rice noted. "The primary etiologies of lung injury in both groups of patients were pneumonia and sepsis, and the average APACHE III [Acute Physiology and Chronic Health Evaluation III] score was approximately 92. These were sick patients," he said. For the first 6 days, the full- and trophic feeding groups received 1,300 kcal/day and 400 kcal/day, respectively.
With respect to the primary end point (28 days), the average number of ventilator-free days in both groups was similar, at 14.9 in the trophic group and 15.0 in the full-feeding group. "There were also no differences in 60-day mortality, organ failure–free days, ICU-free days, or the incidence of infection between groups," he said. Similarly, with respect to body mass index category or lung injury severity, "there were no between-group differences in ventilator free days or survival."
The full-feeding group did have a higher number of gastrointestinal intolerances on any one day, and statistically significant increase on days 2 and 3, but the overall percentages of intolerances were low, Dr. Rice said. There were no differences in albumin and protein levels between the groups over the first 7 days, he said.
Regarding the immediate clinical relevance of the findings, Dr. Rice stressed that the study wasn’t designed as an equivalence trial, "so I can’t tell you both feeding strategies are similar, but you can look at the results." In fact, he said, although the study did not show a benefit other than improved gastrointestinal tolerance, his group has moved toward trophic feeds because of the ease of administration
Dr. Rice had no financial conflicts.
HOUSTON – Restricting the amount of initial enteral intake in mechanically ventilated patients who have acute lung injury neither reduces the duration of mechanical ventilation nor improves mortality relative to full enteral feeding, but the nutritional strategy may be slightly easier on the stomach, according to a study reported at the annual congress of the Society of Critical Care Medicine.
The importance of nutrition support in critically ill patients with acute lung injury (ALI) is well accepted as a means of maintaining gut integrity, modulating both stress and the systemic immune response, and attenuating disease severity, but conflicting data regarding the timing, formulation, and amount of enteral nutrition have contributed to uncertainty about the optimal feeding protocol, according to Dr. Todd W. Rice of Vanderbilt University Medical Center in Nashville, Tenn.
"How much nutrition we need to promote the protective benefits, we don’t know. Providing a little bit of nutrition (called trophic feeding) has been shown to decrease intestinal intolerances, compared with full-calorie feeds, but it may do so at the risk of malnutrition, worse immune function, and loss of muscle strength," he said. Full-calorie feeding, on the other hand, may lead to more intolerances, may cause hyperglycemia and other imbalances, may increase septic complications, and may fuel the inflammatory fire, he added.
In the current study, which was published simultaneously in JAMA, Dr. Rice and colleagues in the EDEN (Early vs. Delayed Enteral Nutrition in ALI) trial sought to examine the relative advantages of restricting the amount of initial enteral intake in mechanically ventilated ALI patients. Specifically, the prospective, randomized, open-label trial compared the effect on clinical outcomes and survival of initial trophic enteral feeding – approximately 25% of the full target feeding – with initial full-calorie feeding for the first 6 days of mechanical ventilation in ALI patients. "We hypothesized that reduced trophic feeding during the first [6 days] would increase ventilator-free days and reduce instances of gastrointestinal intolerances compared with the conventional full enteral nutrition strategy," he said.
The study’s primary end point was ventilator-free days through day 28; secondary end points were daily percentage of goal enteral feeding, frequency of gastrointestinal intolerances, 60-day mortality before hospital discharge with unassisted breathing, ICU- and organ failure–free days, and new infections (JAMA 2012 Feb. 5[doi:10.1001/jama2012.137]).
The multicenter study population comprised 1,000 patients, from January 2008 through mid-April 2011, who were initiated on mechanical ventilation within 48 hours of developing ALI. Within 6 hours of randomization, enteric nutrition was initiated in 508 patients assigned to trophic nutrition and 492 assigned to full feeding, and was continued until death, extubation, or day 6, Dr. Rice explained. Per standard protocol, enteral nutrition in the full-feeding group began at 25 mL/hr and advanced to goal weights (25-30 kcal/day of nonprotein calories and 1.2-1.6 g/kg per day of protein) as quickly as possible; gastric residual volumes were checked every 6 hours while enteral feeding was increased. In the trophic group, enteral feeding was initiated at 10-20 kcal/hr and gastric residual volumes were checked every 12 hours. After 6 days, patients in the trophic group who still required mechanical ventilation were advanced to the full-energy feeding rates, he said.
Baseline characteristics of the two groups were similar, Dr. Rice noted. "The primary etiologies of lung injury in both groups of patients were pneumonia and sepsis, and the average APACHE III [Acute Physiology and Chronic Health Evaluation III] score was approximately 92. These were sick patients," he said. For the first 6 days, the full- and trophic feeding groups received 1,300 kcal/day and 400 kcal/day, respectively.
With respect to the primary end point (28 days), the average number of ventilator-free days in both groups was similar, at 14.9 in the trophic group and 15.0 in the full-feeding group. "There were also no differences in 60-day mortality, organ failure–free days, ICU-free days, or the incidence of infection between groups," he said. Similarly, with respect to body mass index category or lung injury severity, "there were no between-group differences in ventilator free days or survival."
The full-feeding group did have a higher number of gastrointestinal intolerances on any one day, and statistically significant increase on days 2 and 3, but the overall percentages of intolerances were low, Dr. Rice said. There were no differences in albumin and protein levels between the groups over the first 7 days, he said.
Regarding the immediate clinical relevance of the findings, Dr. Rice stressed that the study wasn’t designed as an equivalence trial, "so I can’t tell you both feeding strategies are similar, but you can look at the results." In fact, he said, although the study did not show a benefit other than improved gastrointestinal tolerance, his group has moved toward trophic feeds because of the ease of administration
Dr. Rice had no financial conflicts.
Major Finding: At day 28, the average number of ventilator-free days in ALI patients who had been mechanically ventilated was 14.9 among those who received trophic enteral feeding for the first 6 days, followed by full-calorie feeding, and was 15.0 days among those who received full calorie enteral feeding from the outset.
Data Source: This was a multicenter, randomized, prospective, open-label trial comprising 1,000 mechanically ventilated ALI patients that was designed to assess the effect on clinical outcomes and survival of initial trophic enteral feeding, compared with full-calorie feeding, for the first 6 days of mechanical ventilation.
Disclosures: Dr. Rice and his fellow researchers disclosed having no financial conflicts of interest.
NIMH Framework Will Usher in New Era of Research
HOUSTON – A multidimensional framework being developed by the National Institute of Mental Health is poised to bring the understanding of neuropsychiatric disorders up to par conceptually with the insight being achieved in most other medical disciplines, according to Dr. Thomas Insel.
In contrast to current diagnostic constructs that rely on categorical labels based on signs and symptoms alone, the Research Domain Criteria (RDoC) integrate dimensions of observable behavior with neurobiologic measures and genetics, said Dr. Insel, director of the National Institute of Mental Health. The experimental system will "cut across traditional definitions of mental disorders" by assessing basic dimensions of functioning, such as fear circuitry and working memory, across these multiple units of analysis, he said. While the concept itself is not new – most medical disciplines integrate multiple sources of information, such as biomarkers and imaging, into their diagnostic tool kits – its application to psychiatry is revolutionary, he said.

"Think about it. We don’t use the word ‘cure’ in psychiatry," yet the term is part of the lexicon of nearly every other medical specialty, Dr. Insel said in a plenary presentation at the annual meeting of the American College of Psychiatrists. "The reality is, for most mental illnesses, the etiology is unknown, prediction is poor, detection is late, diagnosis is by observation, prevention is not well developed, and treatment is trial and error."
And while most psychiatrists have seen spectacular individual successes and have experienced the satisfaction of helping people in fundamental ways, "on population-based measures, the dial has not moved much, and when it has moved, the movement has been in the wrong direction, as evidenced by the increased prevalence and increases in associated morbidity and mortality," Dr. Insel said. This is incongruous with the extraordinary advances in biomedical research that have transformed our understanding of so many diseases over the past 50 years, he said. "No such advances have been made in the diseases that we treat, such as major depression, schizophrenia, bipolar disorder, eating disorders, or [attention-deficit/hyperactivity disorder] in children."
The public health implications linked to this lack of advancement are staggering, Dr. Insel said. "The World Health Organization's most recent estimate is that mental health disorders are the largest source of disability from all medical causes, a major cause of death, and one of the major drivers of health care costs from within and outside the system," he said, noting that the estimated direct and indirect costs of mental disorders are more than $317 billion annually.
"What we’ve come to realize is that part of the reason we have not made significant progress is because we haven’t thought about these disorders in the right way," Dr. Insel stressed. "Our focus in thinking about serious mental illness has historically come from the standpoint of these being mental or behavioral problems requiring mental or behavioral interventions."
Such a mind-set suggests that focusing on observable signs and symptoms exclusively will lead to a precise diagnosis, although experience suggests otherwise, Dr. Insel said. "The lesson from other areas of medicine is that a diagnosis that relies solely on manifest symptoms is not the best guide to choosing the most effective treatment." This is because symptom-focused diagnostic labels, such as depression or schizophrenia, frequently belie heterogeneous disorders that defy such narrow classification, he said.
Neuroscientific research during the past decade has determined that mental disorders are brain and developmental disorders that result from complex genetic risk plus experiential factors, Dr. Insel explained. As such, the consideration of all of the various factors will enable precise diagnoses and prediction of treatment response. "We are talking about a completely different way of approaching these illnesses that offers real hope for transforming the statistics and moving the dial."
The much-heralded and occasionally controversial move to the DSM-5 is among the pioneering efforts to reflect this new understanding. The goal of the DSM-5 is to move beyond the signs and symptoms classification of mental illness to incorporate biologic measures, according to Dr. David J. Kupfer, the Thomas Detre Professor of Psychiatry at the University of Pittsburgh and chair of the DSM-5 Task Force. "The DSM-5 is intended to be a living document with recommendations that are guided by research evidence as it evolves," he said in a plenary presentation at the meeting. It will incorporate dimensional concepts, including measurement of distress, disability, and severity; the development of the various illnesses across the life span; and new knowledge on genetic and environmental risk factors and prevention, he said.
"The reality is, for most mental illnesses, the etiology is unknown, prediction is poor, detection is late, diagnosis is by observation, prevention is not well developed, and treatment is trial and error."
For example, the DSM-5 will consider schizophrenia as a multidimensional syndrome rather then a discrete entity to capture the continuum of its phenomenology and pathophysiology and to help track the course of illness evolution, including prodromal states, said Dr. Kupfer, also professor of neuroscience and clinical and translational science at the university. The diagnostic criteria will include measures of cognition (attention, processing speed, delusions, and other thought disturbances) and mood (affective and negative symptoms). As a result of such changes, he explained, the DSM-5 will begin to bridge the gap between presumptive and evidence-based pathophysiologic etiologies.
The NIMH’s RDoC initiative is a complementary approach to the DSM-5. It is based on three assumptions: Mental illness results from dysfunctional brain circuitry rather than identifiable brain lesions; the dysfunction is identifiable using various clinical neuroscience tools, including electrophysiology, neuroimaging, and new methods for in vivo quantification of connections; and data from genetic and clinical neuroscience research will lead to diagnostic biosignatures, according to Dr. Insel.
The RDoC framework is a matrix consisting of rows of functional constructs – the biologic mechanisms that drive behavioral abnormalities – which are grouped under five major domains: negative affect (fear/extinction, stress/distress, aggression); positive affect (reward seeking, reward/habit learning); cognition (attention, perception, working memory, declarative memory, language behavior, cognitive control); social processes (imitation, theory of mind, social dominance, facial expression identification, attachment/separation fear, self-representation areas); and arousal/regulatory processes (arousal and regulation, resting state activity), Dr. Insel explained. Six units of analysis – genes, molecules, cells, circuits, behavior, and self-reports – make up the columns of the matrix and are used to evaluate the domains and constructs.
Because the RDoC domains traverse diagnostic categories, "it most likely will not parallel current diagnostic categories," Dr. Insel said. "Unlike existing systems in which a disorder is either present or absent, RDoC is dimensional; it incorporates measures of magnitude, analogous to cholesterol or blood pressure tests." Ultimately, the project will foster the development of reliable and valid tests for acquiring such dimensional information, he said.
"The idea is that abnormalities in any of the domains or constructs are not necessarily exclusive to one disorder but may be features of multiple disorders," Dr. Insel said. Through data classification done in this way, "the goal is to uncover common biological mechanisms associated with the various domains, which may lead to new molecular and neuroimaging targets for drug discovery." Such insights are critical to real progress he said. "Right now, we don’t know enough about the pathophysiology of depression to know that the serotonin transporter is the target that we should have. We know that it is the place that we have been focused, yet we haven’t reduced the suicide rate among people with affective illness."
The development of the RDoC is ongoing, with no definitive timeline. "It is a long-term project designed to help the research community by designing fundamental, biologically based organizational principles underlying various psychopathologies," Dr. Insel said in an interview. Considering mental disorders in this way will enable new research paradigms, particularly target validation, he said. "Target validation is the coin of the realm in virtually every area of medicine, yet it is almost entirely ignored in our field. Until now, our whole field has revolved around giving compounds to patients and assuming that we understood what we were doing, so if something doesn’t work, we either keep trying or up the dose, without ever knowing if we’ve hit the target. It’s not informative, and there’s no way to make sense of the failure."
In contrast, understanding mental disorders as circuit illnesses and using neuroimaging technology, such as functional MRI and PET imaging, "we now have the technological ability to know whether we’re influencing the target of interest," Dr. Insel said. The next step, he said, is to design trials embedded with experimental medicine, specifically short, deep trials with a small number of patients, "to determine whether a given compound actually engages the target or not, and to determine the success or failure of the compound quickly."
In fact, success is predicated on failing "fast and often," Dr. Insel said. "Experimental medicine is set up for a fast-scale approach: running compounds through so you know what is not working as quickly as possible. Once you determine that a compound has engaged the target, if the patient doesn’t get better, you forget that target and move on."
To identify potential targets and develop experimental treatments to engage them, "we need studies of pathophysiology that go all the way from understanding the molecular basis of these disorders to understanding the social basis, which will get us to the point where we have biomarkers or diagnostics," Dr. Insel said. "For the first time, we will be able to develop treatments that are focused on targets that we truly understand, paving the way for prevention, recovery, and cure."
Dr. Insel and Dr. Kupfer said they had no relevant financial disclosures.
HOUSTON – A multidimensional framework being developed by the National Institute of Mental Health is poised to bring the understanding of neuropsychiatric disorders up to par conceptually with the insight being achieved in most other medical disciplines, according to Dr. Thomas Insel.
In contrast to current diagnostic constructs that rely on categorical labels based on signs and symptoms alone, the Research Domain Criteria (RDoC) integrate dimensions of observable behavior with neurobiologic measures and genetics, said Dr. Insel, director of the National Institute of Mental Health. The experimental system will "cut across traditional definitions of mental disorders" by assessing basic dimensions of functioning, such as fear circuitry and working memory, across these multiple units of analysis, he said. While the concept itself is not new – most medical disciplines integrate multiple sources of information, such as biomarkers and imaging, into their diagnostic tool kits – its application to psychiatry is revolutionary, he said.
"Think about it. We don’t use the word ‘cure’ in psychiatry," yet the term is part of the lexicon of nearly every other medical specialty, Dr. Insel said in a plenary presentation at the annual meeting of the American College of Psychiatrists. "The reality is, for most mental illnesses, the etiology is unknown, prediction is poor, detection is late, diagnosis is by observation, prevention is not well developed, and treatment is trial and error."
And while most psychiatrists have seen spectacular individual successes and have experienced the satisfaction of helping people in fundamental ways, "on population-based measures, the dial has not moved much, and when it has moved, the movement has been in the wrong direction, as evidenced by the increased prevalence and increases in associated morbidity and mortality," Dr. Insel said. This is incongruous with the extraordinary advances in biomedical research that have transformed our understanding of so many diseases over the past 50 years, he said. "No such advances have been made in the diseases that we treat, such as major depression, schizophrenia, bipolar disorder, eating disorders, or [attention-deficit/hyperactivity disorder] in children."
The public health implications linked to this lack of advancement are staggering, Dr. Insel said. "The World Health Organization's most recent estimate is that mental health disorders are the largest source of disability from all medical causes, a major cause of death, and one of the major drivers of health care costs from within and outside the system," he said, noting that the estimated direct and indirect costs of mental disorders are more than $317 billion annually.
"What we’ve come to realize is that part of the reason we have not made significant progress is because we haven’t thought about these disorders in the right way," Dr. Insel stressed. "Our focus in thinking about serious mental illness has historically come from the standpoint of these being mental or behavioral problems requiring mental or behavioral interventions."
Such a mind-set suggests that focusing on observable signs and symptoms exclusively will lead to a precise diagnosis, although experience suggests otherwise, Dr. Insel said. "The lesson from other areas of medicine is that a diagnosis that relies solely on manifest symptoms is not the best guide to choosing the most effective treatment." This is because symptom-focused diagnostic labels, such as depression or schizophrenia, frequently belie heterogeneous disorders that defy such narrow classification, he said.
Neuroscientific research during the past decade has determined that mental disorders are brain and developmental disorders that result from complex genetic risk plus experiential factors, Dr. Insel explained. As such, the consideration of all of the various factors will enable precise diagnoses and prediction of treatment response. "We are talking about a completely different way of approaching these illnesses that offers real hope for transforming the statistics and moving the dial."
The much-heralded and occasionally controversial move to the DSM-5 is among the pioneering efforts to reflect this new understanding. The goal of the DSM-5 is to move beyond the signs and symptoms classification of mental illness to incorporate biologic measures, according to Dr. David J. Kupfer, the Thomas Detre Professor of Psychiatry at the University of Pittsburgh and chair of the DSM-5 Task Force. "The DSM-5 is intended to be a living document with recommendations that are guided by research evidence as it evolves," he said in a plenary presentation at the meeting. It will incorporate dimensional concepts, including measurement of distress, disability, and severity; the development of the various illnesses across the life span; and new knowledge on genetic and environmental risk factors and prevention, he said.
"The reality is, for most mental illnesses, the etiology is unknown, prediction is poor, detection is late, diagnosis is by observation, prevention is not well developed, and treatment is trial and error."
For example, the DSM-5 will consider schizophrenia as a multidimensional syndrome rather then a discrete entity to capture the continuum of its phenomenology and pathophysiology and to help track the course of illness evolution, including prodromal states, said Dr. Kupfer, also professor of neuroscience and clinical and translational science at the university. The diagnostic criteria will include measures of cognition (attention, processing speed, delusions, and other thought disturbances) and mood (affective and negative symptoms). As a result of such changes, he explained, the DSM-5 will begin to bridge the gap between presumptive and evidence-based pathophysiologic etiologies.
The NIMH’s RDoC initiative is a complementary approach to the DSM-5. It is based on three assumptions: Mental illness results from dysfunctional brain circuitry rather than identifiable brain lesions; the dysfunction is identifiable using various clinical neuroscience tools, including electrophysiology, neuroimaging, and new methods for in vivo quantification of connections; and data from genetic and clinical neuroscience research will lead to diagnostic biosignatures, according to Dr. Insel.
The RDoC framework is a matrix consisting of rows of functional constructs – the biologic mechanisms that drive behavioral abnormalities – which are grouped under five major domains: negative affect (fear/extinction, stress/distress, aggression); positive affect (reward seeking, reward/habit learning); cognition (attention, perception, working memory, declarative memory, language behavior, cognitive control); social processes (imitation, theory of mind, social dominance, facial expression identification, attachment/separation fear, self-representation areas); and arousal/regulatory processes (arousal and regulation, resting state activity), Dr. Insel explained. Six units of analysis – genes, molecules, cells, circuits, behavior, and self-reports – make up the columns of the matrix and are used to evaluate the domains and constructs.
Because the RDoC domains traverse diagnostic categories, "it most likely will not parallel current diagnostic categories," Dr. Insel said. "Unlike existing systems in which a disorder is either present or absent, RDoC is dimensional; it incorporates measures of magnitude, analogous to cholesterol or blood pressure tests." Ultimately, the project will foster the development of reliable and valid tests for acquiring such dimensional information, he said.
"The idea is that abnormalities in any of the domains or constructs are not necessarily exclusive to one disorder but may be features of multiple disorders," Dr. Insel said. Through data classification done in this way, "the goal is to uncover common biological mechanisms associated with the various domains, which may lead to new molecular and neuroimaging targets for drug discovery." Such insights are critical to real progress he said. "Right now, we don’t know enough about the pathophysiology of depression to know that the serotonin transporter is the target that we should have. We know that it is the place that we have been focused, yet we haven’t reduced the suicide rate among people with affective illness."
The development of the RDoC is ongoing, with no definitive timeline. "It is a long-term project designed to help the research community by designing fundamental, biologically based organizational principles underlying various psychopathologies," Dr. Insel said in an interview. Considering mental disorders in this way will enable new research paradigms, particularly target validation, he said. "Target validation is the coin of the realm in virtually every area of medicine, yet it is almost entirely ignored in our field. Until now, our whole field has revolved around giving compounds to patients and assuming that we understood what we were doing, so if something doesn’t work, we either keep trying or up the dose, without ever knowing if we’ve hit the target. It’s not informative, and there’s no way to make sense of the failure."
In contrast, understanding mental disorders as circuit illnesses and using neuroimaging technology, such as functional MRI and PET imaging, "we now have the technological ability to know whether we’re influencing the target of interest," Dr. Insel said. The next step, he said, is to design trials embedded with experimental medicine, specifically short, deep trials with a small number of patients, "to determine whether a given compound actually engages the target or not, and to determine the success or failure of the compound quickly."
In fact, success is predicated on failing "fast and often," Dr. Insel said. "Experimental medicine is set up for a fast-scale approach: running compounds through so you know what is not working as quickly as possible. Once you determine that a compound has engaged the target, if the patient doesn’t get better, you forget that target and move on."
To identify potential targets and develop experimental treatments to engage them, "we need studies of pathophysiology that go all the way from understanding the molecular basis of these disorders to understanding the social basis, which will get us to the point where we have biomarkers or diagnostics," Dr. Insel said. "For the first time, we will be able to develop treatments that are focused on targets that we truly understand, paving the way for prevention, recovery, and cure."
Dr. Insel and Dr. Kupfer said they had no relevant financial disclosures.
HOUSTON – A multidimensional framework being developed by the National Institute of Mental Health is poised to bring the understanding of neuropsychiatric disorders up to par conceptually with the insight being achieved in most other medical disciplines, according to Dr. Thomas Insel.
In contrast to current diagnostic constructs that rely on categorical labels based on signs and symptoms alone, the Research Domain Criteria (RDoC) integrate dimensions of observable behavior with neurobiologic measures and genetics, said Dr. Insel, director of the National Institute of Mental Health. The experimental system will "cut across traditional definitions of mental disorders" by assessing basic dimensions of functioning, such as fear circuitry and working memory, across these multiple units of analysis, he said. While the concept itself is not new – most medical disciplines integrate multiple sources of information, such as biomarkers and imaging, into their diagnostic tool kits – its application to psychiatry is revolutionary, he said.
"Think about it. We don’t use the word ‘cure’ in psychiatry," yet the term is part of the lexicon of nearly every other medical specialty, Dr. Insel said in a plenary presentation at the annual meeting of the American College of Psychiatrists. "The reality is, for most mental illnesses, the etiology is unknown, prediction is poor, detection is late, diagnosis is by observation, prevention is not well developed, and treatment is trial and error."
And while most psychiatrists have seen spectacular individual successes and have experienced the satisfaction of helping people in fundamental ways, "on population-based measures, the dial has not moved much, and when it has moved, the movement has been in the wrong direction, as evidenced by the increased prevalence and increases in associated morbidity and mortality," Dr. Insel said. This is incongruous with the extraordinary advances in biomedical research that have transformed our understanding of so many diseases over the past 50 years, he said. "No such advances have been made in the diseases that we treat, such as major depression, schizophrenia, bipolar disorder, eating disorders, or [attention-deficit/hyperactivity disorder] in children."
The public health implications linked to this lack of advancement are staggering, Dr. Insel said. "The World Health Organization's most recent estimate is that mental health disorders are the largest source of disability from all medical causes, a major cause of death, and one of the major drivers of health care costs from within and outside the system," he said, noting that the estimated direct and indirect costs of mental disorders are more than $317 billion annually.
"What we’ve come to realize is that part of the reason we have not made significant progress is because we haven’t thought about these disorders in the right way," Dr. Insel stressed. "Our focus in thinking about serious mental illness has historically come from the standpoint of these being mental or behavioral problems requiring mental or behavioral interventions."
Such a mind-set suggests that focusing on observable signs and symptoms exclusively will lead to a precise diagnosis, although experience suggests otherwise, Dr. Insel said. "The lesson from other areas of medicine is that a diagnosis that relies solely on manifest symptoms is not the best guide to choosing the most effective treatment." This is because symptom-focused diagnostic labels, such as depression or schizophrenia, frequently belie heterogeneous disorders that defy such narrow classification, he said.
Neuroscientific research during the past decade has determined that mental disorders are brain and developmental disorders that result from complex genetic risk plus experiential factors, Dr. Insel explained. As such, the consideration of all of the various factors will enable precise diagnoses and prediction of treatment response. "We are talking about a completely different way of approaching these illnesses that offers real hope for transforming the statistics and moving the dial."
The much-heralded and occasionally controversial move to the DSM-5 is among the pioneering efforts to reflect this new understanding. The goal of the DSM-5 is to move beyond the signs and symptoms classification of mental illness to incorporate biologic measures, according to Dr. David J. Kupfer, the Thomas Detre Professor of Psychiatry at the University of Pittsburgh and chair of the DSM-5 Task Force. "The DSM-5 is intended to be a living document with recommendations that are guided by research evidence as it evolves," he said in a plenary presentation at the meeting. It will incorporate dimensional concepts, including measurement of distress, disability, and severity; the development of the various illnesses across the life span; and new knowledge on genetic and environmental risk factors and prevention, he said.
"The reality is, for most mental illnesses, the etiology is unknown, prediction is poor, detection is late, diagnosis is by observation, prevention is not well developed, and treatment is trial and error."
For example, the DSM-5 will consider schizophrenia as a multidimensional syndrome rather then a discrete entity to capture the continuum of its phenomenology and pathophysiology and to help track the course of illness evolution, including prodromal states, said Dr. Kupfer, also professor of neuroscience and clinical and translational science at the university. The diagnostic criteria will include measures of cognition (attention, processing speed, delusions, and other thought disturbances) and mood (affective and negative symptoms). As a result of such changes, he explained, the DSM-5 will begin to bridge the gap between presumptive and evidence-based pathophysiologic etiologies.
The NIMH’s RDoC initiative is a complementary approach to the DSM-5. It is based on three assumptions: Mental illness results from dysfunctional brain circuitry rather than identifiable brain lesions; the dysfunction is identifiable using various clinical neuroscience tools, including electrophysiology, neuroimaging, and new methods for in vivo quantification of connections; and data from genetic and clinical neuroscience research will lead to diagnostic biosignatures, according to Dr. Insel.
The RDoC framework is a matrix consisting of rows of functional constructs – the biologic mechanisms that drive behavioral abnormalities – which are grouped under five major domains: negative affect (fear/extinction, stress/distress, aggression); positive affect (reward seeking, reward/habit learning); cognition (attention, perception, working memory, declarative memory, language behavior, cognitive control); social processes (imitation, theory of mind, social dominance, facial expression identification, attachment/separation fear, self-representation areas); and arousal/regulatory processes (arousal and regulation, resting state activity), Dr. Insel explained. Six units of analysis – genes, molecules, cells, circuits, behavior, and self-reports – make up the columns of the matrix and are used to evaluate the domains and constructs.
Because the RDoC domains traverse diagnostic categories, "it most likely will not parallel current diagnostic categories," Dr. Insel said. "Unlike existing systems in which a disorder is either present or absent, RDoC is dimensional; it incorporates measures of magnitude, analogous to cholesterol or blood pressure tests." Ultimately, the project will foster the development of reliable and valid tests for acquiring such dimensional information, he said.
"The idea is that abnormalities in any of the domains or constructs are not necessarily exclusive to one disorder but may be features of multiple disorders," Dr. Insel said. Through data classification done in this way, "the goal is to uncover common biological mechanisms associated with the various domains, which may lead to new molecular and neuroimaging targets for drug discovery." Such insights are critical to real progress he said. "Right now, we don’t know enough about the pathophysiology of depression to know that the serotonin transporter is the target that we should have. We know that it is the place that we have been focused, yet we haven’t reduced the suicide rate among people with affective illness."
The development of the RDoC is ongoing, with no definitive timeline. "It is a long-term project designed to help the research community by designing fundamental, biologically based organizational principles underlying various psychopathologies," Dr. Insel said in an interview. Considering mental disorders in this way will enable new research paradigms, particularly target validation, he said. "Target validation is the coin of the realm in virtually every area of medicine, yet it is almost entirely ignored in our field. Until now, our whole field has revolved around giving compounds to patients and assuming that we understood what we were doing, so if something doesn’t work, we either keep trying or up the dose, without ever knowing if we’ve hit the target. It’s not informative, and there’s no way to make sense of the failure."
In contrast, understanding mental disorders as circuit illnesses and using neuroimaging technology, such as functional MRI and PET imaging, "we now have the technological ability to know whether we’re influencing the target of interest," Dr. Insel said. The next step, he said, is to design trials embedded with experimental medicine, specifically short, deep trials with a small number of patients, "to determine whether a given compound actually engages the target or not, and to determine the success or failure of the compound quickly."
In fact, success is predicated on failing "fast and often," Dr. Insel said. "Experimental medicine is set up for a fast-scale approach: running compounds through so you know what is not working as quickly as possible. Once you determine that a compound has engaged the target, if the patient doesn’t get better, you forget that target and move on."
To identify potential targets and develop experimental treatments to engage them, "we need studies of pathophysiology that go all the way from understanding the molecular basis of these disorders to understanding the social basis, which will get us to the point where we have biomarkers or diagnostics," Dr. Insel said. "For the first time, we will be able to develop treatments that are focused on targets that we truly understand, paving the way for prevention, recovery, and cure."
Dr. Insel and Dr. Kupfer said they had no relevant financial disclosures.
EXPERT ANALYSIS FROM THE ANNUAL MEETEING OF THE AMERICAN COLLEGE OF PSYCHIATRISTS
Repeat BAL Advised With Prolonged Therapy for Ventilator-Associated Pneumonia
HOUSTON – Repeat bronchoalveolar lavage should be considered for tailoring the duration of antibiotic therapy and for reassessing resistance profiles in patients with ventilator-associated pneumonia from infection with non–lactose fermenting gram-negative bacilli.
New clinical evidence endorses prolonged antibiotic therapy in these patients. Importantly, the findings also indicate that these patients have persistent primary infections, rather than recurrent infections, as has been previously suggested, Dr. Gina R. Shirah reported at Annual Congress of the Society for Critical Care Medicine.
The distinction between persistent and recurrent infection is important, she emphasized, as the former may signal drug resistance in some patients. For this reason, repeat bronchoalveolar lavage (BAL) should be considered during therapy, both to tailor duration of antibiotics and reassess for changes in resistance profiles.
The American Thoracic Society recommends an 8-day antimicrobial treatment protocol for ventilator-associated pneumonia (VAP) but advises a longer course of therapy in patients with non–lactose fermenting gram-negative rods (NLF-GNR), which include Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia (Am. J. Respir. Crit. Care Med. 2005;171:388-416). The recommendation is based on the findings of a pioneering randomized study by the PneumA Trial Group that showed 8-day treatment to be as effective as 15-day treatment except in a subgroup of patients with NLF-GNR, in whom they observed higher recurrence rates (JAMA 2003;290:2588-98).
Dr. Shirah and her fellow researchers at the Maricopa Integrated Health System in Phoenix, including lead investigator Dr. Tammy Kopelman, conducted a study that indicates 8-day antibiotic regimens were associated with persistent primary infections, not recurrent infections, in patients with gram-negative bacilli.
The researchers retrospectively studied patients at a level I trauma center admitted over a 4½-year time period. They examined data for all ventilator-associated pneumonia patients who were diagnosed via bronchoalveolar lavage – and who underwent subsequent BAL during the antimicrobial treatment course. Based upon initial BAL pathogen, the patients were classified into two groups: those with NLF-GNR and those with all other pathogens, including Enterobacteriaceae, methicillin-resistant Staphylococcus aureus, and community-acquired Haemophilus spp, methicillin-sensitive S. aureus, and Streptococcus spp. They were then further divided based on whether the repeat BAL was conducted within fewer than 8 days of appropriate antibiotic therapy or at day 8 or later, Dr. Shirah said. "Persistent primary infection was defined as a less than 2-log 10 decrease of the initial species on subsequent bronchoalveolar lavage," she explained.
Of the 77 surgical intensive care unit patients who met the study criteria, 99% received appropriate empiric therapy, said Dr. Shirah. The average subsequent BAL performance was on day 7 (range, 3-14 days), with 37 patients undergoing the procedure after 8 days of therapy; of those, 13 patients were in the NLF-GNR group. Within that group, persistent primary infection after more than 8 days of appropriate antimicrobial therapy was reported in nine of the patients (69%) – seven with P. aeruginosa and two with A. baumannii.
By comparison, only two patients in the second group (8%) – both with Enterobacteriaceae – had evidence of persistent primary infection, representing a statistically significant difference, she said. "Importantly, in the [NLF-GNB] group, 56% of the pathogens obtained on repeat BAL remained sensitive to the treatment antibiotics, so nearly half of the patients required alternative antibiotic treatment."
The investigators also sought to determine whether persistent infection could have been predicted. They separated patients into three groups based on treatment status: treated (microbiologic cure on subsequent BAL); persistently infected antimicrobial sensitive; and persistently infected antimicrobial resistant. A comparison of clinical parameters across the groups showed that although there was some variation in white blood cell count, temperature, and ventilator needs "none of the differences were statistically significant," and thus not predictive of short-course treatment success or persistent infection, Dr. Shirah said.
The data strongly support the conclusion that a shortened course of antibiotics in patients with VAP caused by NLF-GNR will frequently lead to a persistent primary infection, said Dr. Shirah, noting that, in the case of NLF-GNR, "changes in antibiotic profiles are common and without reliable clinical indicators." For this reason, she stressed, repeat BAL should be considered during therapy, both to tailor duration of antibiotics and to reassess for changes in resistance profiles.
"Eight days is simply not enough," Dr. Shirah said.
On behalf of her coinvestigators and herself, Dr. Shirah reported no conflicts of interest with respect to this study.
HOUSTON – Repeat bronchoalveolar lavage should be considered for tailoring the duration of antibiotic therapy and for reassessing resistance profiles in patients with ventilator-associated pneumonia from infection with non–lactose fermenting gram-negative bacilli.
New clinical evidence endorses prolonged antibiotic therapy in these patients. Importantly, the findings also indicate that these patients have persistent primary infections, rather than recurrent infections, as has been previously suggested, Dr. Gina R. Shirah reported at Annual Congress of the Society for Critical Care Medicine.
The distinction between persistent and recurrent infection is important, she emphasized, as the former may signal drug resistance in some patients. For this reason, repeat bronchoalveolar lavage (BAL) should be considered during therapy, both to tailor duration of antibiotics and reassess for changes in resistance profiles.
The American Thoracic Society recommends an 8-day antimicrobial treatment protocol for ventilator-associated pneumonia (VAP) but advises a longer course of therapy in patients with non–lactose fermenting gram-negative rods (NLF-GNR), which include Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia (Am. J. Respir. Crit. Care Med. 2005;171:388-416). The recommendation is based on the findings of a pioneering randomized study by the PneumA Trial Group that showed 8-day treatment to be as effective as 15-day treatment except in a subgroup of patients with NLF-GNR, in whom they observed higher recurrence rates (JAMA 2003;290:2588-98).
Dr. Shirah and her fellow researchers at the Maricopa Integrated Health System in Phoenix, including lead investigator Dr. Tammy Kopelman, conducted a study that indicates 8-day antibiotic regimens were associated with persistent primary infections, not recurrent infections, in patients with gram-negative bacilli.
The researchers retrospectively studied patients at a level I trauma center admitted over a 4½-year time period. They examined data for all ventilator-associated pneumonia patients who were diagnosed via bronchoalveolar lavage – and who underwent subsequent BAL during the antimicrobial treatment course. Based upon initial BAL pathogen, the patients were classified into two groups: those with NLF-GNR and those with all other pathogens, including Enterobacteriaceae, methicillin-resistant Staphylococcus aureus, and community-acquired Haemophilus spp, methicillin-sensitive S. aureus, and Streptococcus spp. They were then further divided based on whether the repeat BAL was conducted within fewer than 8 days of appropriate antibiotic therapy or at day 8 or later, Dr. Shirah said. "Persistent primary infection was defined as a less than 2-log 10 decrease of the initial species on subsequent bronchoalveolar lavage," she explained.
Of the 77 surgical intensive care unit patients who met the study criteria, 99% received appropriate empiric therapy, said Dr. Shirah. The average subsequent BAL performance was on day 7 (range, 3-14 days), with 37 patients undergoing the procedure after 8 days of therapy; of those, 13 patients were in the NLF-GNR group. Within that group, persistent primary infection after more than 8 days of appropriate antimicrobial therapy was reported in nine of the patients (69%) – seven with P. aeruginosa and two with A. baumannii.
By comparison, only two patients in the second group (8%) – both with Enterobacteriaceae – had evidence of persistent primary infection, representing a statistically significant difference, she said. "Importantly, in the [NLF-GNB] group, 56% of the pathogens obtained on repeat BAL remained sensitive to the treatment antibiotics, so nearly half of the patients required alternative antibiotic treatment."
The investigators also sought to determine whether persistent infection could have been predicted. They separated patients into three groups based on treatment status: treated (microbiologic cure on subsequent BAL); persistently infected antimicrobial sensitive; and persistently infected antimicrobial resistant. A comparison of clinical parameters across the groups showed that although there was some variation in white blood cell count, temperature, and ventilator needs "none of the differences were statistically significant," and thus not predictive of short-course treatment success or persistent infection, Dr. Shirah said.
The data strongly support the conclusion that a shortened course of antibiotics in patients with VAP caused by NLF-GNR will frequently lead to a persistent primary infection, said Dr. Shirah, noting that, in the case of NLF-GNR, "changes in antibiotic profiles are common and without reliable clinical indicators." For this reason, she stressed, repeat BAL should be considered during therapy, both to tailor duration of antibiotics and to reassess for changes in resistance profiles.
"Eight days is simply not enough," Dr. Shirah said.
On behalf of her coinvestigators and herself, Dr. Shirah reported no conflicts of interest with respect to this study.
HOUSTON – Repeat bronchoalveolar lavage should be considered for tailoring the duration of antibiotic therapy and for reassessing resistance profiles in patients with ventilator-associated pneumonia from infection with non–lactose fermenting gram-negative bacilli.
New clinical evidence endorses prolonged antibiotic therapy in these patients. Importantly, the findings also indicate that these patients have persistent primary infections, rather than recurrent infections, as has been previously suggested, Dr. Gina R. Shirah reported at Annual Congress of the Society for Critical Care Medicine.
The distinction between persistent and recurrent infection is important, she emphasized, as the former may signal drug resistance in some patients. For this reason, repeat bronchoalveolar lavage (BAL) should be considered during therapy, both to tailor duration of antibiotics and reassess for changes in resistance profiles.
The American Thoracic Society recommends an 8-day antimicrobial treatment protocol for ventilator-associated pneumonia (VAP) but advises a longer course of therapy in patients with non–lactose fermenting gram-negative rods (NLF-GNR), which include Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia (Am. J. Respir. Crit. Care Med. 2005;171:388-416). The recommendation is based on the findings of a pioneering randomized study by the PneumA Trial Group that showed 8-day treatment to be as effective as 15-day treatment except in a subgroup of patients with NLF-GNR, in whom they observed higher recurrence rates (JAMA 2003;290:2588-98).
Dr. Shirah and her fellow researchers at the Maricopa Integrated Health System in Phoenix, including lead investigator Dr. Tammy Kopelman, conducted a study that indicates 8-day antibiotic regimens were associated with persistent primary infections, not recurrent infections, in patients with gram-negative bacilli.
The researchers retrospectively studied patients at a level I trauma center admitted over a 4½-year time period. They examined data for all ventilator-associated pneumonia patients who were diagnosed via bronchoalveolar lavage – and who underwent subsequent BAL during the antimicrobial treatment course. Based upon initial BAL pathogen, the patients were classified into two groups: those with NLF-GNR and those with all other pathogens, including Enterobacteriaceae, methicillin-resistant Staphylococcus aureus, and community-acquired Haemophilus spp, methicillin-sensitive S. aureus, and Streptococcus spp. They were then further divided based on whether the repeat BAL was conducted within fewer than 8 days of appropriate antibiotic therapy or at day 8 or later, Dr. Shirah said. "Persistent primary infection was defined as a less than 2-log 10 decrease of the initial species on subsequent bronchoalveolar lavage," she explained.
Of the 77 surgical intensive care unit patients who met the study criteria, 99% received appropriate empiric therapy, said Dr. Shirah. The average subsequent BAL performance was on day 7 (range, 3-14 days), with 37 patients undergoing the procedure after 8 days of therapy; of those, 13 patients were in the NLF-GNR group. Within that group, persistent primary infection after more than 8 days of appropriate antimicrobial therapy was reported in nine of the patients (69%) – seven with P. aeruginosa and two with A. baumannii.
By comparison, only two patients in the second group (8%) – both with Enterobacteriaceae – had evidence of persistent primary infection, representing a statistically significant difference, she said. "Importantly, in the [NLF-GNB] group, 56% of the pathogens obtained on repeat BAL remained sensitive to the treatment antibiotics, so nearly half of the patients required alternative antibiotic treatment."
The investigators also sought to determine whether persistent infection could have been predicted. They separated patients into three groups based on treatment status: treated (microbiologic cure on subsequent BAL); persistently infected antimicrobial sensitive; and persistently infected antimicrobial resistant. A comparison of clinical parameters across the groups showed that although there was some variation in white blood cell count, temperature, and ventilator needs "none of the differences were statistically significant," and thus not predictive of short-course treatment success or persistent infection, Dr. Shirah said.
The data strongly support the conclusion that a shortened course of antibiotics in patients with VAP caused by NLF-GNR will frequently lead to a persistent primary infection, said Dr. Shirah, noting that, in the case of NLF-GNR, "changes in antibiotic profiles are common and without reliable clinical indicators." For this reason, she stressed, repeat BAL should be considered during therapy, both to tailor duration of antibiotics and to reassess for changes in resistance profiles.
"Eight days is simply not enough," Dr. Shirah said.
On behalf of her coinvestigators and herself, Dr. Shirah reported no conflicts of interest with respect to this study.
FROM THE ANNUAL CONGRESS OF THE SOCIETY FOR CRITICAL CARE MEDICINE
Major Finding: Repeat bronchoalveolar lavage (BAL) of 37 patients after 8 days of appropriate antimicrobial therapy indicated that 69% patients with non–lactose fermenting gram-negative rods had persistent primary infection, compared with 8% patients with all other pathogens.
Data Source: Results came from a retrospective study of 77 patients with BAL-diagnosed ventilator-associated pneumonia who underwent repeat BAL while on antibiotic therapy at a level 1 trauma center.
Disclosures: The investigators reported having no relevant financial disclosures.
RAP Scores Guide Ultrasonography for VTE in Trauma Patients
HOUSTON – Nearly 30% of trauma patients who were identified upon admission as being high risk for venous thromboembolism using a validated risk assessment tool went on to develop the thrombotic condition during their ICU stay, a study has shown.
Importantly, the deep vein thromboses in most of these patients were asymptomatic and might have gone undetected with potentially life-threatening consequences but for periodic ultrasound screening, Dr. Chad Thorson reported at the annual congress of the Society of Critical Care Medicine.
"Routine venous thromboembolism screening in the trauma population has been widely debated, and there currently is no protocol for it," according to Dr. Thorson of the Ryder Trauma Center at the University of Miami. Although the principal diagnostic screening tool – venous duplex ultrasound (VDU) – is not considered cost effective for screening all trauma patients, the investigators sought to determine whether prescreening trauma patients using the risk assessment profile (RAP) would yield a cohort of high- risk patients in whom increased vigilance and VDU screening are warranted (J. Trauma 1997;42:100-3).
Toward this end, all patients admitted to the Ryder Center’s level 1 trauma intensive care unit from November 2009 through January 2012 were prospectively screened with RAP, which stratifies an individual’s venous thromboembolism (VTE) risk based on underlying conditions, iatrogenic factors, injury-related factors, and age, within 24 hours of admission.
"Patients with [RAP] scores of 10 or higher received bilateral lower-extremity venous duplex ultrasounds at the time of admission and then weekly throughout their ICU stay," Dr. Thorson said, noting that logistic regression was performed on risk factors to identify independent predictors of VTE development. Among the risk factors considered were RAP score, RAP score higher than 20, femoral central venous catheterization for more than 24 hours, operative intervention duration longer than 2 hours, lower-extremity fracture, pelvic fracture, and spinal cord injury with paraplegia.
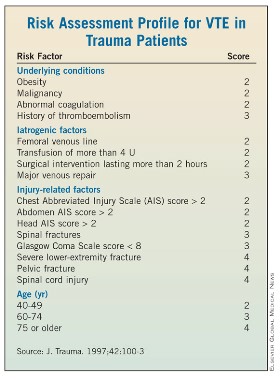
Of 534 trauma ICU admissions during the study period, 106 patients (mean age, 47 years) were identified as high risk based on their RAP score. Blunt trauma was the primary mechanism of injury in 79% of the population, and the mean injury severity score of the predominantly male (74%) high-risk population was 30, said Dr. Thorson.
Routine VDU screening identified 30 VTEs, including 20 that were asymptomatic and 10 that were symptomatic, despite the patients having received thromboprophylaxis (heparin 5,000 U every 8 hours or dalteparin 5,000 U daily), Dr. Thorson reported. Four of the symptomatic events were pulmonary emboli, and of the asymptomatic VTEs, six were identified on admission, seven were identified within the first week of admission, and four were identified within 2 weeks of admission, he said.
A comparison of those who did and did not develop VTEs showed significant differences in the number of risk factors, overall RAP score, and RAP score greater than 20, Dr. Thorson reported. Specifically, those in the non-VTE group averaged five risk factors compared with seven in the VTE group, and the respective median RAP scores were 14 and 19, he said. In addition, 6 patients in the non-VTE and 11 in the VTE group had RAP scores higher than 20. In the stepwise logistic regression analysis, RAP score and a combination of pelvic fracture and prolonged operative intervention were independent predictors of VTE development, he said.
Prescreening trauma patients with RAP is useful for identifying patients at increased risk of VTE who may be candidates for increased surveillance, according to Dr. Thorson. "There is plenty of debate with regard to the utility and cost effectiveness of routine screening, as well as the benefit of identifying asymptomatic deep vein thromboses," Dr. Thorson said in an interview.
"Ideally, we hope to find a decrease in the rate of pulmonary embolism as a result of screening, as this consequence can be devastating."
An important implication of the screening protocol, however, is identifying that DVT/VTE should not be included on the Centers for Medicare and Medicaid Services’ list of preventable complications (defined as errors in medical care that are clearly identifiable and preventable, and thus may no longer be eligible for reimbursement).
"A decision to no longer pay for [VTE] treatment could have devastating effects on many urban trauma centers," Dr. Thorson stressed.
The prescreening study was supported by grants from the Office of Naval Research and the U.S. Army Medical Research and Materiel Command. Dr. Thorson reported that he had no relevant financial disclosures.
Trauma patients are at high risk for VTE, and in the absence of bleeding contraindications, all should be receiving pharmacologic prophylaxis with LDUH/LMWH. Therefore, a risk assessment program for VTE doesn't make much sense: Everyone "rules in" for VTE prophylaxis with medication unless a contraindication exists, according to Dr. Franklin A. Michota.
This observational study used a risk assessment program to identify patients for whom surveillance venous duplex ultrasound might be indicated on top of pharmacologic prophylaxis. Currently, VDU surveillance is not recommended in trauma patients, according to the recently published ninth American College of Chest Physicians' guidelines on antithrombotic therapy and the prevention of thrombosis (Chest 2012;141[suppl.]:e227S-77S). In fact, the ACCP specifically recommends that surveillance not be performed (grade 2C evidence). The rationale is well outlined in the guidelines. It is not clear that using VDU to detect and treat asymptomatic DVT reduces the risk of pulmonary embolism or fatal pulmonary embolism, and some studies have demonstrated that pulmonary embolism can occur even when VDU is negative.
As reported in the ACCP chapter on the prevention of VTE in surgery patients, a large retrospective study from a single center found that over a 6-year period ending in 2000, the frequency of surveillance VDU decreased from 32% to 3.4%, yet there was no increase in the incidence of pulmonary embolism. Also it is well known that surveillance VDU can lead to false-positive findings (asymptomatic distal clot that does not pose a risk for symptoms or embolization), and the risk of treating the false positives with full anticoagulation in the trauma surgery population may increase adverse outcomes.
This new study identified 30 VTEs in 106 high-risk trauma patients with surveillance VDU. However, the investigators reported that 10 of the events were symptomatic, so the VDU was not a screening tool; it was a diagnostic test for signs and symptoms, and therefore, those 10 symptomatic events need to be removed. That leaves you with 20 VTEs in 106 high-risk trauma patients (18.8%). So the real question is, Where were these clots located? If they were distal asymptomatic events, then they may all be false positives. If they were all proximal DVTs, then perhaps this study deserves more credit.
But we should also look at the intensity of VTE prophylaxis provided in this study cohort. The ACCP also recommends mechanical compression on top of pharmacologic prophylaxis in high-risk trauma patients. Was that done here? Perhaps the 20 VTEs were due to inadequate prophylaxis.
Dr. Michota is the director of academic affairs in the department of hospital medicine at the Cleveland Clinic. He reported having no relevant financial disclosures.
Trauma patients are at high risk for VTE, and in the absence of bleeding contraindications, all should be receiving pharmacologic prophylaxis with LDUH/LMWH. Therefore, a risk assessment program for VTE doesn't make much sense: Everyone "rules in" for VTE prophylaxis with medication unless a contraindication exists, according to Dr. Franklin A. Michota.
This observational study used a risk assessment program to identify patients for whom surveillance venous duplex ultrasound might be indicated on top of pharmacologic prophylaxis. Currently, VDU surveillance is not recommended in trauma patients, according to the recently published ninth American College of Chest Physicians' guidelines on antithrombotic therapy and the prevention of thrombosis (Chest 2012;141[suppl.]:e227S-77S). In fact, the ACCP specifically recommends that surveillance not be performed (grade 2C evidence). The rationale is well outlined in the guidelines. It is not clear that using VDU to detect and treat asymptomatic DVT reduces the risk of pulmonary embolism or fatal pulmonary embolism, and some studies have demonstrated that pulmonary embolism can occur even when VDU is negative.
As reported in the ACCP chapter on the prevention of VTE in surgery patients, a large retrospective study from a single center found that over a 6-year period ending in 2000, the frequency of surveillance VDU decreased from 32% to 3.4%, yet there was no increase in the incidence of pulmonary embolism. Also it is well known that surveillance VDU can lead to false-positive findings (asymptomatic distal clot that does not pose a risk for symptoms or embolization), and the risk of treating the false positives with full anticoagulation in the trauma surgery population may increase adverse outcomes.
This new study identified 30 VTEs in 106 high-risk trauma patients with surveillance VDU. However, the investigators reported that 10 of the events were symptomatic, so the VDU was not a screening tool; it was a diagnostic test for signs and symptoms, and therefore, those 10 symptomatic events need to be removed. That leaves you with 20 VTEs in 106 high-risk trauma patients (18.8%). So the real question is, Where were these clots located? If they were distal asymptomatic events, then they may all be false positives. If they were all proximal DVTs, then perhaps this study deserves more credit.
But we should also look at the intensity of VTE prophylaxis provided in this study cohort. The ACCP also recommends mechanical compression on top of pharmacologic prophylaxis in high-risk trauma patients. Was that done here? Perhaps the 20 VTEs were due to inadequate prophylaxis.
Dr. Michota is the director of academic affairs in the department of hospital medicine at the Cleveland Clinic. He reported having no relevant financial disclosures.
Trauma patients are at high risk for VTE, and in the absence of bleeding contraindications, all should be receiving pharmacologic prophylaxis with LDUH/LMWH. Therefore, a risk assessment program for VTE doesn't make much sense: Everyone "rules in" for VTE prophylaxis with medication unless a contraindication exists, according to Dr. Franklin A. Michota.
This observational study used a risk assessment program to identify patients for whom surveillance venous duplex ultrasound might be indicated on top of pharmacologic prophylaxis. Currently, VDU surveillance is not recommended in trauma patients, according to the recently published ninth American College of Chest Physicians' guidelines on antithrombotic therapy and the prevention of thrombosis (Chest 2012;141[suppl.]:e227S-77S). In fact, the ACCP specifically recommends that surveillance not be performed (grade 2C evidence). The rationale is well outlined in the guidelines. It is not clear that using VDU to detect and treat asymptomatic DVT reduces the risk of pulmonary embolism or fatal pulmonary embolism, and some studies have demonstrated that pulmonary embolism can occur even when VDU is negative.
As reported in the ACCP chapter on the prevention of VTE in surgery patients, a large retrospective study from a single center found that over a 6-year period ending in 2000, the frequency of surveillance VDU decreased from 32% to 3.4%, yet there was no increase in the incidence of pulmonary embolism. Also it is well known that surveillance VDU can lead to false-positive findings (asymptomatic distal clot that does not pose a risk for symptoms or embolization), and the risk of treating the false positives with full anticoagulation in the trauma surgery population may increase adverse outcomes.
This new study identified 30 VTEs in 106 high-risk trauma patients with surveillance VDU. However, the investigators reported that 10 of the events were symptomatic, so the VDU was not a screening tool; it was a diagnostic test for signs and symptoms, and therefore, those 10 symptomatic events need to be removed. That leaves you with 20 VTEs in 106 high-risk trauma patients (18.8%). So the real question is, Where were these clots located? If they were distal asymptomatic events, then they may all be false positives. If they were all proximal DVTs, then perhaps this study deserves more credit.
But we should also look at the intensity of VTE prophylaxis provided in this study cohort. The ACCP also recommends mechanical compression on top of pharmacologic prophylaxis in high-risk trauma patients. Was that done here? Perhaps the 20 VTEs were due to inadequate prophylaxis.
Dr. Michota is the director of academic affairs in the department of hospital medicine at the Cleveland Clinic. He reported having no relevant financial disclosures.
HOUSTON – Nearly 30% of trauma patients who were identified upon admission as being high risk for venous thromboembolism using a validated risk assessment tool went on to develop the thrombotic condition during their ICU stay, a study has shown.
Importantly, the deep vein thromboses in most of these patients were asymptomatic and might have gone undetected with potentially life-threatening consequences but for periodic ultrasound screening, Dr. Chad Thorson reported at the annual congress of the Society of Critical Care Medicine.
"Routine venous thromboembolism screening in the trauma population has been widely debated, and there currently is no protocol for it," according to Dr. Thorson of the Ryder Trauma Center at the University of Miami. Although the principal diagnostic screening tool – venous duplex ultrasound (VDU) – is not considered cost effective for screening all trauma patients, the investigators sought to determine whether prescreening trauma patients using the risk assessment profile (RAP) would yield a cohort of high- risk patients in whom increased vigilance and VDU screening are warranted (J. Trauma 1997;42:100-3).
Toward this end, all patients admitted to the Ryder Center’s level 1 trauma intensive care unit from November 2009 through January 2012 were prospectively screened with RAP, which stratifies an individual’s venous thromboembolism (VTE) risk based on underlying conditions, iatrogenic factors, injury-related factors, and age, within 24 hours of admission.
"Patients with [RAP] scores of 10 or higher received bilateral lower-extremity venous duplex ultrasounds at the time of admission and then weekly throughout their ICU stay," Dr. Thorson said, noting that logistic regression was performed on risk factors to identify independent predictors of VTE development. Among the risk factors considered were RAP score, RAP score higher than 20, femoral central venous catheterization for more than 24 hours, operative intervention duration longer than 2 hours, lower-extremity fracture, pelvic fracture, and spinal cord injury with paraplegia.
Of 534 trauma ICU admissions during the study period, 106 patients (mean age, 47 years) were identified as high risk based on their RAP score. Blunt trauma was the primary mechanism of injury in 79% of the population, and the mean injury severity score of the predominantly male (74%) high-risk population was 30, said Dr. Thorson.
Routine VDU screening identified 30 VTEs, including 20 that were asymptomatic and 10 that were symptomatic, despite the patients having received thromboprophylaxis (heparin 5,000 U every 8 hours or dalteparin 5,000 U daily), Dr. Thorson reported. Four of the symptomatic events were pulmonary emboli, and of the asymptomatic VTEs, six were identified on admission, seven were identified within the first week of admission, and four were identified within 2 weeks of admission, he said.
A comparison of those who did and did not develop VTEs showed significant differences in the number of risk factors, overall RAP score, and RAP score greater than 20, Dr. Thorson reported. Specifically, those in the non-VTE group averaged five risk factors compared with seven in the VTE group, and the respective median RAP scores were 14 and 19, he said. In addition, 6 patients in the non-VTE and 11 in the VTE group had RAP scores higher than 20. In the stepwise logistic regression analysis, RAP score and a combination of pelvic fracture and prolonged operative intervention were independent predictors of VTE development, he said.
Prescreening trauma patients with RAP is useful for identifying patients at increased risk of VTE who may be candidates for increased surveillance, according to Dr. Thorson. "There is plenty of debate with regard to the utility and cost effectiveness of routine screening, as well as the benefit of identifying asymptomatic deep vein thromboses," Dr. Thorson said in an interview.
"Ideally, we hope to find a decrease in the rate of pulmonary embolism as a result of screening, as this consequence can be devastating."
An important implication of the screening protocol, however, is identifying that DVT/VTE should not be included on the Centers for Medicare and Medicaid Services’ list of preventable complications (defined as errors in medical care that are clearly identifiable and preventable, and thus may no longer be eligible for reimbursement).
"A decision to no longer pay for [VTE] treatment could have devastating effects on many urban trauma centers," Dr. Thorson stressed.
The prescreening study was supported by grants from the Office of Naval Research and the U.S. Army Medical Research and Materiel Command. Dr. Thorson reported that he had no relevant financial disclosures.
HOUSTON – Nearly 30% of trauma patients who were identified upon admission as being high risk for venous thromboembolism using a validated risk assessment tool went on to develop the thrombotic condition during their ICU stay, a study has shown.
Importantly, the deep vein thromboses in most of these patients were asymptomatic and might have gone undetected with potentially life-threatening consequences but for periodic ultrasound screening, Dr. Chad Thorson reported at the annual congress of the Society of Critical Care Medicine.
"Routine venous thromboembolism screening in the trauma population has been widely debated, and there currently is no protocol for it," according to Dr. Thorson of the Ryder Trauma Center at the University of Miami. Although the principal diagnostic screening tool – venous duplex ultrasound (VDU) – is not considered cost effective for screening all trauma patients, the investigators sought to determine whether prescreening trauma patients using the risk assessment profile (RAP) would yield a cohort of high- risk patients in whom increased vigilance and VDU screening are warranted (J. Trauma 1997;42:100-3).
Toward this end, all patients admitted to the Ryder Center’s level 1 trauma intensive care unit from November 2009 through January 2012 were prospectively screened with RAP, which stratifies an individual’s venous thromboembolism (VTE) risk based on underlying conditions, iatrogenic factors, injury-related factors, and age, within 24 hours of admission.
"Patients with [RAP] scores of 10 or higher received bilateral lower-extremity venous duplex ultrasounds at the time of admission and then weekly throughout their ICU stay," Dr. Thorson said, noting that logistic regression was performed on risk factors to identify independent predictors of VTE development. Among the risk factors considered were RAP score, RAP score higher than 20, femoral central venous catheterization for more than 24 hours, operative intervention duration longer than 2 hours, lower-extremity fracture, pelvic fracture, and spinal cord injury with paraplegia.
Of 534 trauma ICU admissions during the study period, 106 patients (mean age, 47 years) were identified as high risk based on their RAP score. Blunt trauma was the primary mechanism of injury in 79% of the population, and the mean injury severity score of the predominantly male (74%) high-risk population was 30, said Dr. Thorson.
Routine VDU screening identified 30 VTEs, including 20 that were asymptomatic and 10 that were symptomatic, despite the patients having received thromboprophylaxis (heparin 5,000 U every 8 hours or dalteparin 5,000 U daily), Dr. Thorson reported. Four of the symptomatic events were pulmonary emboli, and of the asymptomatic VTEs, six were identified on admission, seven were identified within the first week of admission, and four were identified within 2 weeks of admission, he said.
A comparison of those who did and did not develop VTEs showed significant differences in the number of risk factors, overall RAP score, and RAP score greater than 20, Dr. Thorson reported. Specifically, those in the non-VTE group averaged five risk factors compared with seven in the VTE group, and the respective median RAP scores were 14 and 19, he said. In addition, 6 patients in the non-VTE and 11 in the VTE group had RAP scores higher than 20. In the stepwise logistic regression analysis, RAP score and a combination of pelvic fracture and prolonged operative intervention were independent predictors of VTE development, he said.
Prescreening trauma patients with RAP is useful for identifying patients at increased risk of VTE who may be candidates for increased surveillance, according to Dr. Thorson. "There is plenty of debate with regard to the utility and cost effectiveness of routine screening, as well as the benefit of identifying asymptomatic deep vein thromboses," Dr. Thorson said in an interview.
"Ideally, we hope to find a decrease in the rate of pulmonary embolism as a result of screening, as this consequence can be devastating."
An important implication of the screening protocol, however, is identifying that DVT/VTE should not be included on the Centers for Medicare and Medicaid Services’ list of preventable complications (defined as errors in medical care that are clearly identifiable and preventable, and thus may no longer be eligible for reimbursement).
"A decision to no longer pay for [VTE] treatment could have devastating effects on many urban trauma centers," Dr. Thorson stressed.
The prescreening study was supported by grants from the Office of Naval Research and the U.S. Army Medical Research and Materiel Command. Dr. Thorson reported that he had no relevant financial disclosures.
FROM THE ANNUAL CONGRESS OF THE SOCIETY OF CRITICAL CARE MEDICINE
Major Finding: Of 106 trauma patients identified through a prescreening protocol as being high risk for venous thromboembolism, 30 developed the condition during their ICU stay despite their receiving standard thromboprophylaxis.
Data Source: A prospective study in which 106 patients deemed to be at high risk of venous thromboembolism underwent venous duplex ultrasound at the time of admission and then weekly throughout their ICU stay.
Disclosures: The prescreening study was supported by grants from the Office of Naval Research and the U.S. Army Medical Research and Materiel Command. Dr. Thorson reported that he had no relevant financial disclosures.
ARDS Outcome Linked to Oxygenation at 48 Hours
HOUSTON – Failure to achieve threshold respiratory parameters within the first 48 hours after implementation of high-frequency oscillatory ventilation was linked to higher mortality in patients with severe acute respiratory distress syndrome.
This finding from a retrospective study suggests that the absence of sufficient early improvements in oxygenation in patients with the fulminant lung condition may justify a switch to an alternate ventilation strategy, according to Dr. Samantha Tarras of the University of Michigan Health System in Ann Arbor.
Although high-frequency oscillatory ventilation (HFOV) is indicated as a rescue therapy for patients with severe acute respiratory distress syndrome (ARDS), specific threshold parameters predictive of outcome have not been described, contributing to uncertainty about its optimal application, she said at the annual congress of the Society of Critical Care Medicine.
In a retrospective investigation, Dr. Tarras and her colleagues evaluated the link between threshold oxygenation values and mortality in patients placed on HFOV in the University of Michigan extracorporeal membrane oxygenation (ECMO) referral surgical ICU during 2005-2011. Patients were excluded from analysis if their baseline PaO2/FiO2 (P/F) ratio was 100 or more; if they had ECMO support; or if transition to conventional ventilation, withdrawal of care, or death occurred within the first 48 hours.
Of 112 patients placed on HFOV as part of a standardized ARDS treatment algorithm during the period of study, 58 met entry criteria, according to Dr. Tarras. "Most of the patients were male, young, and critically ill. The median number of days on mechanical ventilation prior to HFOV was 3, and the largest risk factors for ARDS were pneumonia followed by sepsis," she said. The mean P/F ratio at baseline of the patients included in the analysis was 58.4, the mean oxygenation index at baseline was 51.5, and in-hospital mortality was 41.3%, she said.
In univariate analyses, the mortality of patients who failed to reach a threshold P/F ratio of at least 100 within 48 hours was 75%, three times higher than the 24.3% observed in patients who achieved the threshold ratio, Dr. Tarras reported. The sensitivity and specificity of this threshold for predicting survival were 82.4% and 62.5%, respectively, and the positive and negative predictive values were 75.7% and 71.4%, respectively. "Similarly, a significant mortality rate was identified at a threshold oxygenation index of 25 at 48 hours," she said.
Failure to reach the threshold P/F ratio of 100 remained significantly associated with mortality in a multivariate logistic regression model that incorporated patient age, APACHE (Acute Physiology and Chronic Health Evaluation) score, and number of days of mechanical ventilation prior to initiation of HFOV, said Dr. Tarras. "The area under the receiver operator characteristic curve for model performance was 0.774," she noted.
The findings are limited by the lack of information on patients’ cause of death, which could have an effect, Dr. Tarras acknowledged. Even so, "the results tell us that for patients whose oxygenation is not improving after 48 hours of HFOV, clinicians should start thinking about other rescue strategies as well as referral to an ECMO center." Additionally, she said, "this group of patients that is at greater risk of death despite 48 hours [of HFOV] should be targeted in future intervention trials."
Dr. Tarras disclosed having no relevant conflicts of interest.
HOUSTON – Failure to achieve threshold respiratory parameters within the first 48 hours after implementation of high-frequency oscillatory ventilation was linked to higher mortality in patients with severe acute respiratory distress syndrome.
This finding from a retrospective study suggests that the absence of sufficient early improvements in oxygenation in patients with the fulminant lung condition may justify a switch to an alternate ventilation strategy, according to Dr. Samantha Tarras of the University of Michigan Health System in Ann Arbor.
Although high-frequency oscillatory ventilation (HFOV) is indicated as a rescue therapy for patients with severe acute respiratory distress syndrome (ARDS), specific threshold parameters predictive of outcome have not been described, contributing to uncertainty about its optimal application, she said at the annual congress of the Society of Critical Care Medicine.
In a retrospective investigation, Dr. Tarras and her colleagues evaluated the link between threshold oxygenation values and mortality in patients placed on HFOV in the University of Michigan extracorporeal membrane oxygenation (ECMO) referral surgical ICU during 2005-2011. Patients were excluded from analysis if their baseline PaO2/FiO2 (P/F) ratio was 100 or more; if they had ECMO support; or if transition to conventional ventilation, withdrawal of care, or death occurred within the first 48 hours.
Of 112 patients placed on HFOV as part of a standardized ARDS treatment algorithm during the period of study, 58 met entry criteria, according to Dr. Tarras. "Most of the patients were male, young, and critically ill. The median number of days on mechanical ventilation prior to HFOV was 3, and the largest risk factors for ARDS were pneumonia followed by sepsis," she said. The mean P/F ratio at baseline of the patients included in the analysis was 58.4, the mean oxygenation index at baseline was 51.5, and in-hospital mortality was 41.3%, she said.
In univariate analyses, the mortality of patients who failed to reach a threshold P/F ratio of at least 100 within 48 hours was 75%, three times higher than the 24.3% observed in patients who achieved the threshold ratio, Dr. Tarras reported. The sensitivity and specificity of this threshold for predicting survival were 82.4% and 62.5%, respectively, and the positive and negative predictive values were 75.7% and 71.4%, respectively. "Similarly, a significant mortality rate was identified at a threshold oxygenation index of 25 at 48 hours," she said.
Failure to reach the threshold P/F ratio of 100 remained significantly associated with mortality in a multivariate logistic regression model that incorporated patient age, APACHE (Acute Physiology and Chronic Health Evaluation) score, and number of days of mechanical ventilation prior to initiation of HFOV, said Dr. Tarras. "The area under the receiver operator characteristic curve for model performance was 0.774," she noted.
The findings are limited by the lack of information on patients’ cause of death, which could have an effect, Dr. Tarras acknowledged. Even so, "the results tell us that for patients whose oxygenation is not improving after 48 hours of HFOV, clinicians should start thinking about other rescue strategies as well as referral to an ECMO center." Additionally, she said, "this group of patients that is at greater risk of death despite 48 hours [of HFOV] should be targeted in future intervention trials."
Dr. Tarras disclosed having no relevant conflicts of interest.
HOUSTON – Failure to achieve threshold respiratory parameters within the first 48 hours after implementation of high-frequency oscillatory ventilation was linked to higher mortality in patients with severe acute respiratory distress syndrome.
This finding from a retrospective study suggests that the absence of sufficient early improvements in oxygenation in patients with the fulminant lung condition may justify a switch to an alternate ventilation strategy, according to Dr. Samantha Tarras of the University of Michigan Health System in Ann Arbor.
Although high-frequency oscillatory ventilation (HFOV) is indicated as a rescue therapy for patients with severe acute respiratory distress syndrome (ARDS), specific threshold parameters predictive of outcome have not been described, contributing to uncertainty about its optimal application, she said at the annual congress of the Society of Critical Care Medicine.
In a retrospective investigation, Dr. Tarras and her colleagues evaluated the link between threshold oxygenation values and mortality in patients placed on HFOV in the University of Michigan extracorporeal membrane oxygenation (ECMO) referral surgical ICU during 2005-2011. Patients were excluded from analysis if their baseline PaO2/FiO2 (P/F) ratio was 100 or more; if they had ECMO support; or if transition to conventional ventilation, withdrawal of care, or death occurred within the first 48 hours.
Of 112 patients placed on HFOV as part of a standardized ARDS treatment algorithm during the period of study, 58 met entry criteria, according to Dr. Tarras. "Most of the patients were male, young, and critically ill. The median number of days on mechanical ventilation prior to HFOV was 3, and the largest risk factors for ARDS were pneumonia followed by sepsis," she said. The mean P/F ratio at baseline of the patients included in the analysis was 58.4, the mean oxygenation index at baseline was 51.5, and in-hospital mortality was 41.3%, she said.
In univariate analyses, the mortality of patients who failed to reach a threshold P/F ratio of at least 100 within 48 hours was 75%, three times higher than the 24.3% observed in patients who achieved the threshold ratio, Dr. Tarras reported. The sensitivity and specificity of this threshold for predicting survival were 82.4% and 62.5%, respectively, and the positive and negative predictive values were 75.7% and 71.4%, respectively. "Similarly, a significant mortality rate was identified at a threshold oxygenation index of 25 at 48 hours," she said.
Failure to reach the threshold P/F ratio of 100 remained significantly associated with mortality in a multivariate logistic regression model that incorporated patient age, APACHE (Acute Physiology and Chronic Health Evaluation) score, and number of days of mechanical ventilation prior to initiation of HFOV, said Dr. Tarras. "The area under the receiver operator characteristic curve for model performance was 0.774," she noted.
The findings are limited by the lack of information on patients’ cause of death, which could have an effect, Dr. Tarras acknowledged. Even so, "the results tell us that for patients whose oxygenation is not improving after 48 hours of HFOV, clinicians should start thinking about other rescue strategies as well as referral to an ECMO center." Additionally, she said, "this group of patients that is at greater risk of death despite 48 hours [of HFOV] should be targeted in future intervention trials."
Dr. Tarras disclosed having no relevant conflicts of interest.
FROM THE ANNUAL CONGRESS OF THE SOCIETY OF CRITICAL CARE MEDICINE
Major Finding: The mortality of patients with ARDS who failed to reach a threshold P/F ratio of at least 100 within 48 hours of initiation of high-frequency oscillatory ventilation was 75%, compared with a mortality of 24.3% among similar patients who achieved the ratio.
Data Source: A retrospective study comparing mortality in 58 surgical ICU patients with ARDS who received at least 48 hours of high-frequency oscillatory ventilation.
Disclosures: Dr. Tarras disclosed having no relevant conflicts of interest.