User login
Balancing Act
When you start work as a hospitalist, you’ll tend to immerse yourself in your new job. But you should also strive to maintain a work-life balance from the start, to guard against eventual burnout.
“It’s really work-family-self balance, because of the importance of self-care,” says Maureen Murray of Maureen Murray Associates in Pittsburgh, who provides professional training in stress management and work-life balance. “Self-care is more than just running or dieting—it’s the foundation of a balanced life.”
Areas of Self-Care
“If you don’t put yourself first, you won’t be very effective at caring for others,” says Murray. Her training program categorizes self-care into four areas:
Physical: What keeps me healthy? “Most people already know the answer to this,” says Murray. “Some form of regular activity, eating reasonably well, and getting some rest.” Mental: What energizes my mind? The answer is “something different,” according to Murray.
- Read a book or see a movie;
- Try a new cuisine; or
- Go out with friends who aren’t in the medical profession.
Emotional: What gives me contentment and joy? “This can be spending quality time with loved ones and friends because friends are often the first to fall through the cracks when we get busy,” says Murray. “The answer might also be a hobby that puts you ‘in the zone.’”
Spiritual: What feeds my spirit? This will be different for different people: attend church; take a walk in nature; meditate or pray; or read something inspirational.
The Eight-Step Program
Here are eight things you can do—starting now—to ensure a healthy balance in your career:
- Select the best job for you. Keep your work-life-self balance in mind during the job search, particularly when it comes to comparing schedules, time off, benefits.
- Consider location. If you have a family, or plan to have children soon, “choose a workplace that’s near your extended family,” advises Murray.
- Find someone who’s doing it right. “After you start, look around and find role models who seem to be balancing their lives pretty well,” says Murray. “Look for the physician who’s not stressed, who’s juggling a family and work. Then ask them how they do it so well. Having a role model like this is really important.”
- Talk about work. “There’s a temptation to isolate yourself and work really long hours,” warns Murray. “Grab a cup of coffee with a colleague or go for a walk with a friend.”
- Be aware of stress. “You need to feel you’re in control of something—so control your reaction to stress,” says Murray. “Read about stress, but let go of the idea that coping with it is out of your hands.”
- Plan ahead. Have a contingency plan for things that need to be done. “Ask yourself, ‘What’s my backup plan for childcare … and what’s my backup to the backup?’ ” says Murray. When you plan ahead, you can avoid stressful situations.
- Laugh. “Laughter releases endorphins, which make you feel good,” Murray points out. “Seek the company of those you laugh with. And when you have options for what to watch on TV or on DVD, always choose the comedy.”
- State your needs. “People need to communicate their needs about life balance,” Murray stresses. “This can be very difficult to do, whether it’s to your partner or your boss. State what you need in a positive way. ”
Be vigilant in maintaining a healthy work-life-self balance, with an emphasis on self, and your hospitalist career should be a happy one. TH
When you start work as a hospitalist, you’ll tend to immerse yourself in your new job. But you should also strive to maintain a work-life balance from the start, to guard against eventual burnout.
“It’s really work-family-self balance, because of the importance of self-care,” says Maureen Murray of Maureen Murray Associates in Pittsburgh, who provides professional training in stress management and work-life balance. “Self-care is more than just running or dieting—it’s the foundation of a balanced life.”
Areas of Self-Care
“If you don’t put yourself first, you won’t be very effective at caring for others,” says Murray. Her training program categorizes self-care into four areas:
Physical: What keeps me healthy? “Most people already know the answer to this,” says Murray. “Some form of regular activity, eating reasonably well, and getting some rest.” Mental: What energizes my mind? The answer is “something different,” according to Murray.
- Read a book or see a movie;
- Try a new cuisine; or
- Go out with friends who aren’t in the medical profession.
Emotional: What gives me contentment and joy? “This can be spending quality time with loved ones and friends because friends are often the first to fall through the cracks when we get busy,” says Murray. “The answer might also be a hobby that puts you ‘in the zone.’”
Spiritual: What feeds my spirit? This will be different for different people: attend church; take a walk in nature; meditate or pray; or read something inspirational.
The Eight-Step Program
Here are eight things you can do—starting now—to ensure a healthy balance in your career:
- Select the best job for you. Keep your work-life-self balance in mind during the job search, particularly when it comes to comparing schedules, time off, benefits.
- Consider location. If you have a family, or plan to have children soon, “choose a workplace that’s near your extended family,” advises Murray.
- Find someone who’s doing it right. “After you start, look around and find role models who seem to be balancing their lives pretty well,” says Murray. “Look for the physician who’s not stressed, who’s juggling a family and work. Then ask them how they do it so well. Having a role model like this is really important.”
- Talk about work. “There’s a temptation to isolate yourself and work really long hours,” warns Murray. “Grab a cup of coffee with a colleague or go for a walk with a friend.”
- Be aware of stress. “You need to feel you’re in control of something—so control your reaction to stress,” says Murray. “Read about stress, but let go of the idea that coping with it is out of your hands.”
- Plan ahead. Have a contingency plan for things that need to be done. “Ask yourself, ‘What’s my backup plan for childcare … and what’s my backup to the backup?’ ” says Murray. When you plan ahead, you can avoid stressful situations.
- Laugh. “Laughter releases endorphins, which make you feel good,” Murray points out. “Seek the company of those you laugh with. And when you have options for what to watch on TV or on DVD, always choose the comedy.”
- State your needs. “People need to communicate their needs about life balance,” Murray stresses. “This can be very difficult to do, whether it’s to your partner or your boss. State what you need in a positive way. ”
Be vigilant in maintaining a healthy work-life-self balance, with an emphasis on self, and your hospitalist career should be a happy one. TH
When you start work as a hospitalist, you’ll tend to immerse yourself in your new job. But you should also strive to maintain a work-life balance from the start, to guard against eventual burnout.
“It’s really work-family-self balance, because of the importance of self-care,” says Maureen Murray of Maureen Murray Associates in Pittsburgh, who provides professional training in stress management and work-life balance. “Self-care is more than just running or dieting—it’s the foundation of a balanced life.”
Areas of Self-Care
“If you don’t put yourself first, you won’t be very effective at caring for others,” says Murray. Her training program categorizes self-care into four areas:
Physical: What keeps me healthy? “Most people already know the answer to this,” says Murray. “Some form of regular activity, eating reasonably well, and getting some rest.” Mental: What energizes my mind? The answer is “something different,” according to Murray.
- Read a book or see a movie;
- Try a new cuisine; or
- Go out with friends who aren’t in the medical profession.
Emotional: What gives me contentment and joy? “This can be spending quality time with loved ones and friends because friends are often the first to fall through the cracks when we get busy,” says Murray. “The answer might also be a hobby that puts you ‘in the zone.’”
Spiritual: What feeds my spirit? This will be different for different people: attend church; take a walk in nature; meditate or pray; or read something inspirational.
The Eight-Step Program
Here are eight things you can do—starting now—to ensure a healthy balance in your career:
- Select the best job for you. Keep your work-life-self balance in mind during the job search, particularly when it comes to comparing schedules, time off, benefits.
- Consider location. If you have a family, or plan to have children soon, “choose a workplace that’s near your extended family,” advises Murray.
- Find someone who’s doing it right. “After you start, look around and find role models who seem to be balancing their lives pretty well,” says Murray. “Look for the physician who’s not stressed, who’s juggling a family and work. Then ask them how they do it so well. Having a role model like this is really important.”
- Talk about work. “There’s a temptation to isolate yourself and work really long hours,” warns Murray. “Grab a cup of coffee with a colleague or go for a walk with a friend.”
- Be aware of stress. “You need to feel you’re in control of something—so control your reaction to stress,” says Murray. “Read about stress, but let go of the idea that coping with it is out of your hands.”
- Plan ahead. Have a contingency plan for things that need to be done. “Ask yourself, ‘What’s my backup plan for childcare … and what’s my backup to the backup?’ ” says Murray. When you plan ahead, you can avoid stressful situations.
- Laugh. “Laughter releases endorphins, which make you feel good,” Murray points out. “Seek the company of those you laugh with. And when you have options for what to watch on TV or on DVD, always choose the comedy.”
- State your needs. “People need to communicate their needs about life balance,” Murray stresses. “This can be very difficult to do, whether it’s to your partner or your boss. State what you need in a positive way. ”
Be vigilant in maintaining a healthy work-life-self balance, with an emphasis on self, and your hospitalist career should be a happy one. TH
Hospital Medicine, Recognized
Recent developments at the American Board of Internal Medicine (ABIM) could affect your re-certification process as a working hospitalist. In 2004 SHM petitioned the ABIM to consider a program that would recognize the specific skills and knowledge of hospitalists. Last fall, ABIM voted to begin development of a Focused Recognition of Hospital Medicine through its Maintenance of Certification (MOC) system.
This focused recognition would give hospitalists a formal credential that recognizes hospital medicine as a distinct field within internal medicine. This is the first time in its history that ABIM has offered focused recognition for any subset of internal medicine, and—if approved—the first time that the umbrella organization, the American Board of Medical Specialties (ABMS), will offer a focused recognition for a subset of any specialty.
The Details
Robert Wachter, MD, professor of medicine at the University of California, San Francisco, is chair of ABIM’s Committee on Hospital Medicine Focused Recognition (HMFR). This committee is finalizing the details of how the focused recognition will work. Issues on their agenda include:
- Demonstration of a focused practice: The committee is considering setting a minimum volume of hospitalized patients for this that can reasonably apply to academic physicians, physician-administrators, and researchers—as well as clinical hospitalists.
- Requirements for demonstrating performance in practice: For MOC requirements, ABIM is increasingly examining the use of real practice data. In other words, measuring what physicians do rather than what they know.
- Tests for MOC: The exam for MOC with Focused Recognition of Hospital Medicine could be taken from the current MOC, with the same core content on internal medicine as well as new content relevant to hospital medicine, or it could be an entirely different test, focusing on hospital medicine.
The timeframe for an MOC with a Focused Recognition of Hospital Medicine is likely to be shorter than a standard MOC. “The minimum number of years that would elapse is still being discussed, but it would be no fewer than two and no more than four or five,” says Dr. Wachter. “Now, you don’t have to do an MOC until year 10. I’m hoping that people would start working toward their MOC as soon as they end their residency, but—people being people—they may not actually start work on this until year nine.”
What the Future Holds
In June the Committee on HMFR will present its recommendations for the process to the ABIM board, including how HMFR would relate to the rest of ABIM certification and MOC in internal medicine. Once approved, the plan will be presented to ABMS. “It will have to go through a process at ABMS, which takes a year or 18 months,” warns Holly Humphrey, MD, professor of medicine and dean for Medical Education at Pritzker School of Medicine, University of Chicago.
The goal is not to limit the practice of hospital medicine to those who have been through the focused recognition certification, but rather to lend credibility to the field. “What may change is that people hiring hospitalists may value this,” speculates Dr. Wachter. “The market will dictate” how necessary the re-certification becomes. TH
Recent developments at the American Board of Internal Medicine (ABIM) could affect your re-certification process as a working hospitalist. In 2004 SHM petitioned the ABIM to consider a program that would recognize the specific skills and knowledge of hospitalists. Last fall, ABIM voted to begin development of a Focused Recognition of Hospital Medicine through its Maintenance of Certification (MOC) system.
This focused recognition would give hospitalists a formal credential that recognizes hospital medicine as a distinct field within internal medicine. This is the first time in its history that ABIM has offered focused recognition for any subset of internal medicine, and—if approved—the first time that the umbrella organization, the American Board of Medical Specialties (ABMS), will offer a focused recognition for a subset of any specialty.
The Details
Robert Wachter, MD, professor of medicine at the University of California, San Francisco, is chair of ABIM’s Committee on Hospital Medicine Focused Recognition (HMFR). This committee is finalizing the details of how the focused recognition will work. Issues on their agenda include:
- Demonstration of a focused practice: The committee is considering setting a minimum volume of hospitalized patients for this that can reasonably apply to academic physicians, physician-administrators, and researchers—as well as clinical hospitalists.
- Requirements for demonstrating performance in practice: For MOC requirements, ABIM is increasingly examining the use of real practice data. In other words, measuring what physicians do rather than what they know.
- Tests for MOC: The exam for MOC with Focused Recognition of Hospital Medicine could be taken from the current MOC, with the same core content on internal medicine as well as new content relevant to hospital medicine, or it could be an entirely different test, focusing on hospital medicine.
The timeframe for an MOC with a Focused Recognition of Hospital Medicine is likely to be shorter than a standard MOC. “The minimum number of years that would elapse is still being discussed, but it would be no fewer than two and no more than four or five,” says Dr. Wachter. “Now, you don’t have to do an MOC until year 10. I’m hoping that people would start working toward their MOC as soon as they end their residency, but—people being people—they may not actually start work on this until year nine.”
What the Future Holds
In June the Committee on HMFR will present its recommendations for the process to the ABIM board, including how HMFR would relate to the rest of ABIM certification and MOC in internal medicine. Once approved, the plan will be presented to ABMS. “It will have to go through a process at ABMS, which takes a year or 18 months,” warns Holly Humphrey, MD, professor of medicine and dean for Medical Education at Pritzker School of Medicine, University of Chicago.
The goal is not to limit the practice of hospital medicine to those who have been through the focused recognition certification, but rather to lend credibility to the field. “What may change is that people hiring hospitalists may value this,” speculates Dr. Wachter. “The market will dictate” how necessary the re-certification becomes. TH
Recent developments at the American Board of Internal Medicine (ABIM) could affect your re-certification process as a working hospitalist. In 2004 SHM petitioned the ABIM to consider a program that would recognize the specific skills and knowledge of hospitalists. Last fall, ABIM voted to begin development of a Focused Recognition of Hospital Medicine through its Maintenance of Certification (MOC) system.
This focused recognition would give hospitalists a formal credential that recognizes hospital medicine as a distinct field within internal medicine. This is the first time in its history that ABIM has offered focused recognition for any subset of internal medicine, and—if approved—the first time that the umbrella organization, the American Board of Medical Specialties (ABMS), will offer a focused recognition for a subset of any specialty.
The Details
Robert Wachter, MD, professor of medicine at the University of California, San Francisco, is chair of ABIM’s Committee on Hospital Medicine Focused Recognition (HMFR). This committee is finalizing the details of how the focused recognition will work. Issues on their agenda include:
- Demonstration of a focused practice: The committee is considering setting a minimum volume of hospitalized patients for this that can reasonably apply to academic physicians, physician-administrators, and researchers—as well as clinical hospitalists.
- Requirements for demonstrating performance in practice: For MOC requirements, ABIM is increasingly examining the use of real practice data. In other words, measuring what physicians do rather than what they know.
- Tests for MOC: The exam for MOC with Focused Recognition of Hospital Medicine could be taken from the current MOC, with the same core content on internal medicine as well as new content relevant to hospital medicine, or it could be an entirely different test, focusing on hospital medicine.
The timeframe for an MOC with a Focused Recognition of Hospital Medicine is likely to be shorter than a standard MOC. “The minimum number of years that would elapse is still being discussed, but it would be no fewer than two and no more than four or five,” says Dr. Wachter. “Now, you don’t have to do an MOC until year 10. I’m hoping that people would start working toward their MOC as soon as they end their residency, but—people being people—they may not actually start work on this until year nine.”
What the Future Holds
In June the Committee on HMFR will present its recommendations for the process to the ABIM board, including how HMFR would relate to the rest of ABIM certification and MOC in internal medicine. Once approved, the plan will be presented to ABMS. “It will have to go through a process at ABMS, which takes a year or 18 months,” warns Holly Humphrey, MD, professor of medicine and dean for Medical Education at Pritzker School of Medicine, University of Chicago.
The goal is not to limit the practice of hospital medicine to those who have been through the focused recognition certification, but rather to lend credibility to the field. “What may change is that people hiring hospitalists may value this,” speculates Dr. Wachter. “The market will dictate” how necessary the re-certification becomes. TH
Want Help with Your Job Search?
Heather A. Harris, MD, director of Eden Inpatient Services at Eden Medical Center in Castro Valley, Calif., has been a hospitalist for nearly four years and helped start her hospital medicine practice, which currently employs eight full-time day hospitalists and “a cadre of night folks.”
“I’ve been on both ends of looking for a job and hiring hospitalists,” she says. Below, she and other hospitalists share advice on how to choose your first position in hospital medicine.
Begin Early
The best job search begins before you graduate. “When you’re looking for a job, start as early as possible,” advises Sameer Badlani, MD, hospitalist and instructor at the University of Chicago. “Most people don’t realize how long it takes.”
To prepare for employment, take steps toward getting your medical license and put your paperwork in order. “If you know which state or states you want to be in, go ahead and start the state licensing as soon as possible,” says Dr. Badlani. “Each state has its own set of forms, and you can at least have the packet ready to send in.”
You can also prepare your certification materials so that they are ready to turn over to your future employer: “The FCVS [Federation Credentials Verification Service] is a repository for all your training certificates,” explains Dr. Badlani. “It costs $250 to get a copy of all your certificates, and an additional $30 every time you send it out to a [potential employer]. Some states will only accept certificates from FCVS, and I think that someday all states will require this.”
As a first step for the actual job search, Dr. Harris recommends trying to network through your university and your residency program. “Your program may keep a list of where residents have gone to work; you can at least talk to recent graduates that you know,” she says. “Call them up and see how they like what they’re doing.”
You can broaden your search by joining the industry association and exploring job postings. “I’d recommend that anyone become a member of SHM,” says Dr. Harris. “There are a variety of job postings available through their Web site. You can also simply “Google” ‘hospitalist jobs,’ and find all kinds of national services, headhunters, and companies.” To view job postings t through SHM’s online Career Center, visit www.hospitalmedicine.org and click “Career Center.”
Hospitalist Sanjiv Panwala, MD, a hospitalist at Providence Medical Center, Portland, Ore., has created www.mdgrad.com, a Web site that includes portals to hospital medicine job postings.
Narrow Your Search
When you take these first steps, you’ll discover just how many positions you have to choose from. How can you narrow your job search?
“Clearly, [you have] to distinguish the things that are important to you,” says Dr. Harris. “There’s quite a distinction between an academic and community-based position; you need to think this through before you begin your job search.”
Regardless of this first decision, there are universal factors to consider. “As in any job search, you start by thinking about the area of the country you want to be in, urban versus rural, and other factors,” explains Dr. Harris. “Then you think about the things that separate [hospital medicine] programs from one another.” You’ll find you have a lot of choices.
“There seem to be [hospital medicine] jobs everywhere,” says Dr. Panwala. “The money is in Texas or the Midwest, if that’s what’s important to you.”
Once you’ve decided on your general career path and where you’d like to live and work, consider what type of work you want to do. “One thing you should think about is whether you want to see patients in critical care arenas, or just those patients on the floors,” says Dr. Harris. “These are very different populations, and require different skill sets. You should also consider whether or not you want to work with residents. Residents work in some community settings, too.”
An Academic Job Search
If you decide you want to work in an academic setting, you don’t have to go far to start your search. “I’d think you could start by talking to the head of your department and ask if they can look around and put in a word for you,” says Dr. Harris.
Mark V. Williams, MD, FACP, director of Emory Healthcare’s Hospital Medicine Unit in Atlanta and editor of The Journal of Hospital Medicine, will become chief of the new Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago later this year. He recommends scoping out how a potential employer’s hospital medicine group is perceived and treated within the institution.
“People coming out of residency should look at the amount of support provided by the department of medicine for the hospital medicine group,” he says. “Are the hospitalists active members of the department, with key faculty in leadership positions such as residency or associate residency program director, or are they being hired just to deliver clinical care? Ask if there is funded support for hospital medicine research faculty. If not, the job may be just like working in a community setting, only community settings historically pay better.”
Signs that an institution has a strong commitment to the field include the presence of a division of hospital medicine, and possibly even a hospital medicine fellowship.
Questions to Ask
Even if you’ve got your eye on a specific hospital medicine group, go though the interview process at several institutions so that you can see what the market offers. Important factors to consider include:
Who would I work for? Who owns the hospital medicine practice? “There are differences in who’s sponsoring the group,” says Dr. Harris. “It may be independent, employed by the hospital, or a national group that contracts with the hospital. The answer will give you insights into the job. You may not get the entire picture, but you’ll get a clue.” Consider whether the practice can offer opportunities for advancement—possibly even partnership—and the type of clinical or administrative work you prefer.
What type of schedule would I work? How is the schedule arranged? Consider the number of hours you’d spend on call, and the number of nights and weekends you’d be expected to cover.
“Residents don’t have a sustainable schedule, so anything that’s not ridiculous sounds good,” warns Dr. Harris. “But a seven-on, seven-off shift is very tiring and can lead to burnout over time. So consider whether a given schedule is realistic for the long-term.” Find out how many vacation days are included—or if there are none.
What is the workload? During the interviewing process, ask about the average number of encounters per day. Definitely ask those “nitty-gritty” questions about patient load, admissions, and so on, advises Dr. Harris.
Pay special attention to the number of encounters. “Seeing 18 to 20 patients a day is a lot; those are the turn-and-burn organizations that aren’t necessarily sustainable,” says Dr. Panwala. “The money offered for this may be appealing to younger hospitalists. But remember, if you’re getting paid more, nothing is free.”
Dr. Harris adds, “Ask if that includes admissions and—if there’s critical care work—ask how many of those encounters are in critical care, because those patients will take more time.”
Michael-Anthony Williams, MD, regional CMO of Sound Inpatient Physicians in Denver, advises job seekers to look at “what they have to do” for the salary offered. “Look at … the number of days worked, the length of those days, and the number of encounters per day. You have to ask questions about these things, because the information isn’t necessarily going to be laid out in front of you.”
What about compensation and benefits? Your first consideration of salary, benefits, and other compensation should be to ensure the figures are in line with what the market offers. You can find general information on what hospitalists make from SHM’s “Bi-Annual Survey on the State of the Hospital Medicine Movement,” available at www.hospitalmedicine.org. The Medical Group Management Association (MGMA) and the Association of American Medical Colleges (AAMC) provide salary scales, and salaries for positions at public institutions like university hospitals are public information.
Do your homework, and then simply ask each interviewer what the salary range is for hospitalists. “It doesn’t put me off to have these discussions [on compensation and benefits] early on,” says Dr. Harris.
You may be tempted to choose a job based on salary—but be careful: “Don’t always look at the amount of money as the deciding factor,” says Dr. Badlani. “If a job offers $5,000 or $10,000 more, what are they expecting for that extra salary? And consider how much of that additional money will go to taxes.”
As you gather information on these areas, you’ll need to keep it straight. Dr. Harris advises you to create a simple system that allows you to compare hospital medicine practices you’re considering. “Come up with a chart and list out everything,” she says. “It’s going to vary considerably” from practice to practice, and you’ll need a method to compare one job possibility with another.
How the Process Works
Here is how the interviewing process is likely to flow: “Generally, people send me their resumes, then I’ll have a phone interview with the best candidates,” says Dr. Harris. “If that works out, the next step is that they’ll come in for a tour of the hospital and meet some of the other folks in the group.”
Candidates are invited to call or e-mail physicians in the group with questions; the group will decide which candidate to hire.
That face-to-face meeting with members of the group is essential. “Spend time with other hospitalists,” advises Dr. Badlani. “See what their daily work looks like, including what kind of patients you’ll be seeing.”
You should ask those hospitalists some of the same questions you’ve asked your main interviewer, including questions about schedule, workload, and compensation. “Talk to as many people in the practice as possible,” says Dr. Michael-Anthony Williams. “They’ll give you an honest answer.”
If you like what you see and the group likes you, you’ll get a job offer followed by a contract to sign. “When we extend an offer, they have time to determine what they want,” says Dr. Harris, explaining that she realizes a candidate may be faced with several job options. “When they say yes, we’ll extend a contract and begin the credentialing process.”
The process is not over at this point; you may be months away from your first day on the job. “You need to become credentialed for each hospital you’ll work at, and for the group,” explains Dr. Harris. “At our hospital, that can take three to four months—other places take around two months. Just so you know that you shouldn’t be looking for a job in June and thinking you’ll work in July.”
You’ll have a part to play in the credentialing process. There will be paperwork to fill out, and you’ll need to provide your diploma and medical license and letters of support. “The credentialing committee at our hospital won’t proceed until [all of this] is 100% complete,” says Dr. Harris.
Find a Good Fit
The most important factor to consider in taking a job is simply, are you a good fit for the group? Finding a good match for the group’s values and mission is crucial to the success of the organization and the new hire.
When you meet with hospitalists in the group, “Ask what the mission or values are of the group,” says Dr. Michael-Anthony Williams. “Do they know what their mission is—and is it coherent? Coherence will lend stability over time.”
Dr. Panwala stresses finding a “like-minded” group. “You’ll work with them day in and day out. If you don’t mesh well, you’re going to be miserable,” he says. “You turn your patient over to another hospitalist at 8 p.m., and when you come in the next morning, you take over someone else’s patients. It’s very much a marriage.”
What Interviewers Look For
Because its essential to find a good personality fit for a group, allow decision-makers to get a sense of who you are during the interview phase.
“It’s important to be honest about your values and about who you are,” says Dr. Harris. She believes that most hospital medicine directors look for candidates who are “actively interested in being a hospitalist—preferably for a long time,” for physicians who are team players, and for traits that include flexibility and responsibility.
“I look for someone who’s outgoing,” adds Dr. Mark Williams. “ I want a nice person—someone who’s willing to bend over backward to help others. I appreciate people who’ve won humanitarian awards in residency.”
There are also more basic traits you should display. “General etiquette is important,” stresses Dr. Harris. “Be prompt in your responses when using phone and e-mail. If you’re interested in the position, be engaged in the process. After you come in to the hospital, send a brief letter or a quick e-mail thanking the person and expressing your interest—or your lack of interest. This doesn’t have to be very formal.”
When interviewing candidates for academic hospitalist positions, Dr. Mark Williams says, “I look for residents who have won awards, who have laudatory letters of recommendation from their program director. I love letters that say this resident was in the top of their class, or the best we’ve seen in five years. I look for those who have done research, and those who published case report abstracts, which shows they’re industrious.”
Dr. Mark Williams also asks questions of candidates early in the process and listens carefully to their responses. “I especially look for good communication skills, which are so critical for hospitalists,” he says. “If someone has poor communication skills, they’ll have a tough time on the job.”
To determine their skills, “I’ll ask about their goals, and ask what they see as their weakness,” he says. “It’s very positive to see someone articulate their weaknesses.”
Before You Sign
When you’re presented with a contract, it’s time to take a close look at what’s being offered. “Before you sign anything, you need to come to an agreement with the other party in the contract that this is exactly what we agreed to. Otherwise, it’s no deal,” says Fred A. McCurdy, MD, PhD, MBA, FAAP, FACPE, professor and regional chairman of pediatrics, Texas Tech University Health Sciences Center at Amarillo. “Everything needs to be really specific in the offer letter or the contract—their duties, expectations—all clarified up front.”
Examine the benefits, including retirement and insurance. Ideally, you want disability insurance—and malpractice insurance with tail coverage is essential. (Tail coverage, also called extended reporting coverage, covers you after you leave a group in case a patient files a lawsuit years after the fact.)
Make sure you understand what the contract says, and make sure your employer doesn’t hold too much power. “Check to see if you can be assigned to areas of work that would be a deal-breaker—if you can be sent to another city or state to work, for example,” says Dr. McCurdy.
As a new physician, you do have some leverage to negotiate for better compensation or schedule. Dr. McCurdy says of recent residents, “The two biggest benefits they bring to the table are their youth and the fact that they’re current and up to date on what’s going on in [internal medicine]. They have energy, and they’ll bring energy to the program; and they’ve spent three years in intense study and have the most up-to-date knowledge of anyone you can hire.”
Point out these advantages to the right interviewer, and you may be able to negotiate.
Dr. Badlani encourages new hires to negotiate their moving expenses, bonuses, and malpractice insurance.
But keep in mind that not all hospital medicine programs can or will negotiate. “It’s quite variable,” admits Dr. McCurdy.
Dr. Harris’ program is a prime example. “In my experience, we don’t have a tremendous amount of negotiating,” she says. “Basically, we say, ‘Here’s the deal.’ ”
Dr. McCurdy advises having someone else read the contract for you. “When you’re enthusiastic about a new job, you don’t see everything,” he explains. “And you need to have a lawyer read it to make sure it’s a correctly constructed legal document.”
Dr. Harris simply advises that you “read through the contract with a fine-tooth comb. Does it have a non-compete clause that prohibits you from practicing in the region after you leave? You can find a job [locally] without this clause.”
Dr. McCurdy has allowed new hires to strike these clauses from their contracts, but it’s a trade-off. “Non-compete clauses are hard to enforce,” he acknowledges. “Our boilerplate contract has one, because we want to send the message that we don’t want to spend two years training you and then have you leave and go to work for the competition. So if [a candidate] wants to strike that clause from the contract, I’ll say that’s fine, but on the basis of that I’ll make it a binding three-year contract.”
What if, after researching, interviewing, reviewing the contract, and taking every step possible to ensure you get the best job, you find you’ve made a mistake? “Remember, your contract is only for one year,” Dr. Badlani points out. “You can always change next year if you don’t like your [first choice].” TH
Heather A. Harris, MD, director of Eden Inpatient Services at Eden Medical Center in Castro Valley, Calif., has been a hospitalist for nearly four years and helped start her hospital medicine practice, which currently employs eight full-time day hospitalists and “a cadre of night folks.”
“I’ve been on both ends of looking for a job and hiring hospitalists,” she says. Below, she and other hospitalists share advice on how to choose your first position in hospital medicine.
Begin Early
The best job search begins before you graduate. “When you’re looking for a job, start as early as possible,” advises Sameer Badlani, MD, hospitalist and instructor at the University of Chicago. “Most people don’t realize how long it takes.”
To prepare for employment, take steps toward getting your medical license and put your paperwork in order. “If you know which state or states you want to be in, go ahead and start the state licensing as soon as possible,” says Dr. Badlani. “Each state has its own set of forms, and you can at least have the packet ready to send in.”
You can also prepare your certification materials so that they are ready to turn over to your future employer: “The FCVS [Federation Credentials Verification Service] is a repository for all your training certificates,” explains Dr. Badlani. “It costs $250 to get a copy of all your certificates, and an additional $30 every time you send it out to a [potential employer]. Some states will only accept certificates from FCVS, and I think that someday all states will require this.”
As a first step for the actual job search, Dr. Harris recommends trying to network through your university and your residency program. “Your program may keep a list of where residents have gone to work; you can at least talk to recent graduates that you know,” she says. “Call them up and see how they like what they’re doing.”
You can broaden your search by joining the industry association and exploring job postings. “I’d recommend that anyone become a member of SHM,” says Dr. Harris. “There are a variety of job postings available through their Web site. You can also simply “Google” ‘hospitalist jobs,’ and find all kinds of national services, headhunters, and companies.” To view job postings t through SHM’s online Career Center, visit www.hospitalmedicine.org and click “Career Center.”
Hospitalist Sanjiv Panwala, MD, a hospitalist at Providence Medical Center, Portland, Ore., has created www.mdgrad.com, a Web site that includes portals to hospital medicine job postings.
Narrow Your Search
When you take these first steps, you’ll discover just how many positions you have to choose from. How can you narrow your job search?
“Clearly, [you have] to distinguish the things that are important to you,” says Dr. Harris. “There’s quite a distinction between an academic and community-based position; you need to think this through before you begin your job search.”
Regardless of this first decision, there are universal factors to consider. “As in any job search, you start by thinking about the area of the country you want to be in, urban versus rural, and other factors,” explains Dr. Harris. “Then you think about the things that separate [hospital medicine] programs from one another.” You’ll find you have a lot of choices.
“There seem to be [hospital medicine] jobs everywhere,” says Dr. Panwala. “The money is in Texas or the Midwest, if that’s what’s important to you.”
Once you’ve decided on your general career path and where you’d like to live and work, consider what type of work you want to do. “One thing you should think about is whether you want to see patients in critical care arenas, or just those patients on the floors,” says Dr. Harris. “These are very different populations, and require different skill sets. You should also consider whether or not you want to work with residents. Residents work in some community settings, too.”
An Academic Job Search
If you decide you want to work in an academic setting, you don’t have to go far to start your search. “I’d think you could start by talking to the head of your department and ask if they can look around and put in a word for you,” says Dr. Harris.
Mark V. Williams, MD, FACP, director of Emory Healthcare’s Hospital Medicine Unit in Atlanta and editor of The Journal of Hospital Medicine, will become chief of the new Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago later this year. He recommends scoping out how a potential employer’s hospital medicine group is perceived and treated within the institution.
“People coming out of residency should look at the amount of support provided by the department of medicine for the hospital medicine group,” he says. “Are the hospitalists active members of the department, with key faculty in leadership positions such as residency or associate residency program director, or are they being hired just to deliver clinical care? Ask if there is funded support for hospital medicine research faculty. If not, the job may be just like working in a community setting, only community settings historically pay better.”
Signs that an institution has a strong commitment to the field include the presence of a division of hospital medicine, and possibly even a hospital medicine fellowship.
Questions to Ask
Even if you’ve got your eye on a specific hospital medicine group, go though the interview process at several institutions so that you can see what the market offers. Important factors to consider include:
Who would I work for? Who owns the hospital medicine practice? “There are differences in who’s sponsoring the group,” says Dr. Harris. “It may be independent, employed by the hospital, or a national group that contracts with the hospital. The answer will give you insights into the job. You may not get the entire picture, but you’ll get a clue.” Consider whether the practice can offer opportunities for advancement—possibly even partnership—and the type of clinical or administrative work you prefer.
What type of schedule would I work? How is the schedule arranged? Consider the number of hours you’d spend on call, and the number of nights and weekends you’d be expected to cover.
“Residents don’t have a sustainable schedule, so anything that’s not ridiculous sounds good,” warns Dr. Harris. “But a seven-on, seven-off shift is very tiring and can lead to burnout over time. So consider whether a given schedule is realistic for the long-term.” Find out how many vacation days are included—or if there are none.
What is the workload? During the interviewing process, ask about the average number of encounters per day. Definitely ask those “nitty-gritty” questions about patient load, admissions, and so on, advises Dr. Harris.
Pay special attention to the number of encounters. “Seeing 18 to 20 patients a day is a lot; those are the turn-and-burn organizations that aren’t necessarily sustainable,” says Dr. Panwala. “The money offered for this may be appealing to younger hospitalists. But remember, if you’re getting paid more, nothing is free.”
Dr. Harris adds, “Ask if that includes admissions and—if there’s critical care work—ask how many of those encounters are in critical care, because those patients will take more time.”
Michael-Anthony Williams, MD, regional CMO of Sound Inpatient Physicians in Denver, advises job seekers to look at “what they have to do” for the salary offered. “Look at … the number of days worked, the length of those days, and the number of encounters per day. You have to ask questions about these things, because the information isn’t necessarily going to be laid out in front of you.”
What about compensation and benefits? Your first consideration of salary, benefits, and other compensation should be to ensure the figures are in line with what the market offers. You can find general information on what hospitalists make from SHM’s “Bi-Annual Survey on the State of the Hospital Medicine Movement,” available at www.hospitalmedicine.org. The Medical Group Management Association (MGMA) and the Association of American Medical Colleges (AAMC) provide salary scales, and salaries for positions at public institutions like university hospitals are public information.
Do your homework, and then simply ask each interviewer what the salary range is for hospitalists. “It doesn’t put me off to have these discussions [on compensation and benefits] early on,” says Dr. Harris.
You may be tempted to choose a job based on salary—but be careful: “Don’t always look at the amount of money as the deciding factor,” says Dr. Badlani. “If a job offers $5,000 or $10,000 more, what are they expecting for that extra salary? And consider how much of that additional money will go to taxes.”
As you gather information on these areas, you’ll need to keep it straight. Dr. Harris advises you to create a simple system that allows you to compare hospital medicine practices you’re considering. “Come up with a chart and list out everything,” she says. “It’s going to vary considerably” from practice to practice, and you’ll need a method to compare one job possibility with another.
How the Process Works
Here is how the interviewing process is likely to flow: “Generally, people send me their resumes, then I’ll have a phone interview with the best candidates,” says Dr. Harris. “If that works out, the next step is that they’ll come in for a tour of the hospital and meet some of the other folks in the group.”
Candidates are invited to call or e-mail physicians in the group with questions; the group will decide which candidate to hire.
That face-to-face meeting with members of the group is essential. “Spend time with other hospitalists,” advises Dr. Badlani. “See what their daily work looks like, including what kind of patients you’ll be seeing.”
You should ask those hospitalists some of the same questions you’ve asked your main interviewer, including questions about schedule, workload, and compensation. “Talk to as many people in the practice as possible,” says Dr. Michael-Anthony Williams. “They’ll give you an honest answer.”
If you like what you see and the group likes you, you’ll get a job offer followed by a contract to sign. “When we extend an offer, they have time to determine what they want,” says Dr. Harris, explaining that she realizes a candidate may be faced with several job options. “When they say yes, we’ll extend a contract and begin the credentialing process.”
The process is not over at this point; you may be months away from your first day on the job. “You need to become credentialed for each hospital you’ll work at, and for the group,” explains Dr. Harris. “At our hospital, that can take three to four months—other places take around two months. Just so you know that you shouldn’t be looking for a job in June and thinking you’ll work in July.”
You’ll have a part to play in the credentialing process. There will be paperwork to fill out, and you’ll need to provide your diploma and medical license and letters of support. “The credentialing committee at our hospital won’t proceed until [all of this] is 100% complete,” says Dr. Harris.
Find a Good Fit
The most important factor to consider in taking a job is simply, are you a good fit for the group? Finding a good match for the group’s values and mission is crucial to the success of the organization and the new hire.
When you meet with hospitalists in the group, “Ask what the mission or values are of the group,” says Dr. Michael-Anthony Williams. “Do they know what their mission is—and is it coherent? Coherence will lend stability over time.”
Dr. Panwala stresses finding a “like-minded” group. “You’ll work with them day in and day out. If you don’t mesh well, you’re going to be miserable,” he says. “You turn your patient over to another hospitalist at 8 p.m., and when you come in the next morning, you take over someone else’s patients. It’s very much a marriage.”
What Interviewers Look For
Because its essential to find a good personality fit for a group, allow decision-makers to get a sense of who you are during the interview phase.
“It’s important to be honest about your values and about who you are,” says Dr. Harris. She believes that most hospital medicine directors look for candidates who are “actively interested in being a hospitalist—preferably for a long time,” for physicians who are team players, and for traits that include flexibility and responsibility.
“I look for someone who’s outgoing,” adds Dr. Mark Williams. “ I want a nice person—someone who’s willing to bend over backward to help others. I appreciate people who’ve won humanitarian awards in residency.”
There are also more basic traits you should display. “General etiquette is important,” stresses Dr. Harris. “Be prompt in your responses when using phone and e-mail. If you’re interested in the position, be engaged in the process. After you come in to the hospital, send a brief letter or a quick e-mail thanking the person and expressing your interest—or your lack of interest. This doesn’t have to be very formal.”
When interviewing candidates for academic hospitalist positions, Dr. Mark Williams says, “I look for residents who have won awards, who have laudatory letters of recommendation from their program director. I love letters that say this resident was in the top of their class, or the best we’ve seen in five years. I look for those who have done research, and those who published case report abstracts, which shows they’re industrious.”
Dr. Mark Williams also asks questions of candidates early in the process and listens carefully to their responses. “I especially look for good communication skills, which are so critical for hospitalists,” he says. “If someone has poor communication skills, they’ll have a tough time on the job.”
To determine their skills, “I’ll ask about their goals, and ask what they see as their weakness,” he says. “It’s very positive to see someone articulate their weaknesses.”
Before You Sign
When you’re presented with a contract, it’s time to take a close look at what’s being offered. “Before you sign anything, you need to come to an agreement with the other party in the contract that this is exactly what we agreed to. Otherwise, it’s no deal,” says Fred A. McCurdy, MD, PhD, MBA, FAAP, FACPE, professor and regional chairman of pediatrics, Texas Tech University Health Sciences Center at Amarillo. “Everything needs to be really specific in the offer letter or the contract—their duties, expectations—all clarified up front.”
Examine the benefits, including retirement and insurance. Ideally, you want disability insurance—and malpractice insurance with tail coverage is essential. (Tail coverage, also called extended reporting coverage, covers you after you leave a group in case a patient files a lawsuit years after the fact.)
Make sure you understand what the contract says, and make sure your employer doesn’t hold too much power. “Check to see if you can be assigned to areas of work that would be a deal-breaker—if you can be sent to another city or state to work, for example,” says Dr. McCurdy.
As a new physician, you do have some leverage to negotiate for better compensation or schedule. Dr. McCurdy says of recent residents, “The two biggest benefits they bring to the table are their youth and the fact that they’re current and up to date on what’s going on in [internal medicine]. They have energy, and they’ll bring energy to the program; and they’ve spent three years in intense study and have the most up-to-date knowledge of anyone you can hire.”
Point out these advantages to the right interviewer, and you may be able to negotiate.
Dr. Badlani encourages new hires to negotiate their moving expenses, bonuses, and malpractice insurance.
But keep in mind that not all hospital medicine programs can or will negotiate. “It’s quite variable,” admits Dr. McCurdy.
Dr. Harris’ program is a prime example. “In my experience, we don’t have a tremendous amount of negotiating,” she says. “Basically, we say, ‘Here’s the deal.’ ”
Dr. McCurdy advises having someone else read the contract for you. “When you’re enthusiastic about a new job, you don’t see everything,” he explains. “And you need to have a lawyer read it to make sure it’s a correctly constructed legal document.”
Dr. Harris simply advises that you “read through the contract with a fine-tooth comb. Does it have a non-compete clause that prohibits you from practicing in the region after you leave? You can find a job [locally] without this clause.”
Dr. McCurdy has allowed new hires to strike these clauses from their contracts, but it’s a trade-off. “Non-compete clauses are hard to enforce,” he acknowledges. “Our boilerplate contract has one, because we want to send the message that we don’t want to spend two years training you and then have you leave and go to work for the competition. So if [a candidate] wants to strike that clause from the contract, I’ll say that’s fine, but on the basis of that I’ll make it a binding three-year contract.”
What if, after researching, interviewing, reviewing the contract, and taking every step possible to ensure you get the best job, you find you’ve made a mistake? “Remember, your contract is only for one year,” Dr. Badlani points out. “You can always change next year if you don’t like your [first choice].” TH
Heather A. Harris, MD, director of Eden Inpatient Services at Eden Medical Center in Castro Valley, Calif., has been a hospitalist for nearly four years and helped start her hospital medicine practice, which currently employs eight full-time day hospitalists and “a cadre of night folks.”
“I’ve been on both ends of looking for a job and hiring hospitalists,” she says. Below, she and other hospitalists share advice on how to choose your first position in hospital medicine.
Begin Early
The best job search begins before you graduate. “When you’re looking for a job, start as early as possible,” advises Sameer Badlani, MD, hospitalist and instructor at the University of Chicago. “Most people don’t realize how long it takes.”
To prepare for employment, take steps toward getting your medical license and put your paperwork in order. “If you know which state or states you want to be in, go ahead and start the state licensing as soon as possible,” says Dr. Badlani. “Each state has its own set of forms, and you can at least have the packet ready to send in.”
You can also prepare your certification materials so that they are ready to turn over to your future employer: “The FCVS [Federation Credentials Verification Service] is a repository for all your training certificates,” explains Dr. Badlani. “It costs $250 to get a copy of all your certificates, and an additional $30 every time you send it out to a [potential employer]. Some states will only accept certificates from FCVS, and I think that someday all states will require this.”
As a first step for the actual job search, Dr. Harris recommends trying to network through your university and your residency program. “Your program may keep a list of where residents have gone to work; you can at least talk to recent graduates that you know,” she says. “Call them up and see how they like what they’re doing.”
You can broaden your search by joining the industry association and exploring job postings. “I’d recommend that anyone become a member of SHM,” says Dr. Harris. “There are a variety of job postings available through their Web site. You can also simply “Google” ‘hospitalist jobs,’ and find all kinds of national services, headhunters, and companies.” To view job postings t through SHM’s online Career Center, visit www.hospitalmedicine.org and click “Career Center.”
Hospitalist Sanjiv Panwala, MD, a hospitalist at Providence Medical Center, Portland, Ore., has created www.mdgrad.com, a Web site that includes portals to hospital medicine job postings.
Narrow Your Search
When you take these first steps, you’ll discover just how many positions you have to choose from. How can you narrow your job search?
“Clearly, [you have] to distinguish the things that are important to you,” says Dr. Harris. “There’s quite a distinction between an academic and community-based position; you need to think this through before you begin your job search.”
Regardless of this first decision, there are universal factors to consider. “As in any job search, you start by thinking about the area of the country you want to be in, urban versus rural, and other factors,” explains Dr. Harris. “Then you think about the things that separate [hospital medicine] programs from one another.” You’ll find you have a lot of choices.
“There seem to be [hospital medicine] jobs everywhere,” says Dr. Panwala. “The money is in Texas or the Midwest, if that’s what’s important to you.”
Once you’ve decided on your general career path and where you’d like to live and work, consider what type of work you want to do. “One thing you should think about is whether you want to see patients in critical care arenas, or just those patients on the floors,” says Dr. Harris. “These are very different populations, and require different skill sets. You should also consider whether or not you want to work with residents. Residents work in some community settings, too.”
An Academic Job Search
If you decide you want to work in an academic setting, you don’t have to go far to start your search. “I’d think you could start by talking to the head of your department and ask if they can look around and put in a word for you,” says Dr. Harris.
Mark V. Williams, MD, FACP, director of Emory Healthcare’s Hospital Medicine Unit in Atlanta and editor of The Journal of Hospital Medicine, will become chief of the new Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago later this year. He recommends scoping out how a potential employer’s hospital medicine group is perceived and treated within the institution.
“People coming out of residency should look at the amount of support provided by the department of medicine for the hospital medicine group,” he says. “Are the hospitalists active members of the department, with key faculty in leadership positions such as residency or associate residency program director, or are they being hired just to deliver clinical care? Ask if there is funded support for hospital medicine research faculty. If not, the job may be just like working in a community setting, only community settings historically pay better.”
Signs that an institution has a strong commitment to the field include the presence of a division of hospital medicine, and possibly even a hospital medicine fellowship.
Questions to Ask
Even if you’ve got your eye on a specific hospital medicine group, go though the interview process at several institutions so that you can see what the market offers. Important factors to consider include:
Who would I work for? Who owns the hospital medicine practice? “There are differences in who’s sponsoring the group,” says Dr. Harris. “It may be independent, employed by the hospital, or a national group that contracts with the hospital. The answer will give you insights into the job. You may not get the entire picture, but you’ll get a clue.” Consider whether the practice can offer opportunities for advancement—possibly even partnership—and the type of clinical or administrative work you prefer.
What type of schedule would I work? How is the schedule arranged? Consider the number of hours you’d spend on call, and the number of nights and weekends you’d be expected to cover.
“Residents don’t have a sustainable schedule, so anything that’s not ridiculous sounds good,” warns Dr. Harris. “But a seven-on, seven-off shift is very tiring and can lead to burnout over time. So consider whether a given schedule is realistic for the long-term.” Find out how many vacation days are included—or if there are none.
What is the workload? During the interviewing process, ask about the average number of encounters per day. Definitely ask those “nitty-gritty” questions about patient load, admissions, and so on, advises Dr. Harris.
Pay special attention to the number of encounters. “Seeing 18 to 20 patients a day is a lot; those are the turn-and-burn organizations that aren’t necessarily sustainable,” says Dr. Panwala. “The money offered for this may be appealing to younger hospitalists. But remember, if you’re getting paid more, nothing is free.”
Dr. Harris adds, “Ask if that includes admissions and—if there’s critical care work—ask how many of those encounters are in critical care, because those patients will take more time.”
Michael-Anthony Williams, MD, regional CMO of Sound Inpatient Physicians in Denver, advises job seekers to look at “what they have to do” for the salary offered. “Look at … the number of days worked, the length of those days, and the number of encounters per day. You have to ask questions about these things, because the information isn’t necessarily going to be laid out in front of you.”
What about compensation and benefits? Your first consideration of salary, benefits, and other compensation should be to ensure the figures are in line with what the market offers. You can find general information on what hospitalists make from SHM’s “Bi-Annual Survey on the State of the Hospital Medicine Movement,” available at www.hospitalmedicine.org. The Medical Group Management Association (MGMA) and the Association of American Medical Colleges (AAMC) provide salary scales, and salaries for positions at public institutions like university hospitals are public information.
Do your homework, and then simply ask each interviewer what the salary range is for hospitalists. “It doesn’t put me off to have these discussions [on compensation and benefits] early on,” says Dr. Harris.
You may be tempted to choose a job based on salary—but be careful: “Don’t always look at the amount of money as the deciding factor,” says Dr. Badlani. “If a job offers $5,000 or $10,000 more, what are they expecting for that extra salary? And consider how much of that additional money will go to taxes.”
As you gather information on these areas, you’ll need to keep it straight. Dr. Harris advises you to create a simple system that allows you to compare hospital medicine practices you’re considering. “Come up with a chart and list out everything,” she says. “It’s going to vary considerably” from practice to practice, and you’ll need a method to compare one job possibility with another.
How the Process Works
Here is how the interviewing process is likely to flow: “Generally, people send me their resumes, then I’ll have a phone interview with the best candidates,” says Dr. Harris. “If that works out, the next step is that they’ll come in for a tour of the hospital and meet some of the other folks in the group.”
Candidates are invited to call or e-mail physicians in the group with questions; the group will decide which candidate to hire.
That face-to-face meeting with members of the group is essential. “Spend time with other hospitalists,” advises Dr. Badlani. “See what their daily work looks like, including what kind of patients you’ll be seeing.”
You should ask those hospitalists some of the same questions you’ve asked your main interviewer, including questions about schedule, workload, and compensation. “Talk to as many people in the practice as possible,” says Dr. Michael-Anthony Williams. “They’ll give you an honest answer.”
If you like what you see and the group likes you, you’ll get a job offer followed by a contract to sign. “When we extend an offer, they have time to determine what they want,” says Dr. Harris, explaining that she realizes a candidate may be faced with several job options. “When they say yes, we’ll extend a contract and begin the credentialing process.”
The process is not over at this point; you may be months away from your first day on the job. “You need to become credentialed for each hospital you’ll work at, and for the group,” explains Dr. Harris. “At our hospital, that can take three to four months—other places take around two months. Just so you know that you shouldn’t be looking for a job in June and thinking you’ll work in July.”
You’ll have a part to play in the credentialing process. There will be paperwork to fill out, and you’ll need to provide your diploma and medical license and letters of support. “The credentialing committee at our hospital won’t proceed until [all of this] is 100% complete,” says Dr. Harris.
Find a Good Fit
The most important factor to consider in taking a job is simply, are you a good fit for the group? Finding a good match for the group’s values and mission is crucial to the success of the organization and the new hire.
When you meet with hospitalists in the group, “Ask what the mission or values are of the group,” says Dr. Michael-Anthony Williams. “Do they know what their mission is—and is it coherent? Coherence will lend stability over time.”
Dr. Panwala stresses finding a “like-minded” group. “You’ll work with them day in and day out. If you don’t mesh well, you’re going to be miserable,” he says. “You turn your patient over to another hospitalist at 8 p.m., and when you come in the next morning, you take over someone else’s patients. It’s very much a marriage.”
What Interviewers Look For
Because its essential to find a good personality fit for a group, allow decision-makers to get a sense of who you are during the interview phase.
“It’s important to be honest about your values and about who you are,” says Dr. Harris. She believes that most hospital medicine directors look for candidates who are “actively interested in being a hospitalist—preferably for a long time,” for physicians who are team players, and for traits that include flexibility and responsibility.
“I look for someone who’s outgoing,” adds Dr. Mark Williams. “ I want a nice person—someone who’s willing to bend over backward to help others. I appreciate people who’ve won humanitarian awards in residency.”
There are also more basic traits you should display. “General etiquette is important,” stresses Dr. Harris. “Be prompt in your responses when using phone and e-mail. If you’re interested in the position, be engaged in the process. After you come in to the hospital, send a brief letter or a quick e-mail thanking the person and expressing your interest—or your lack of interest. This doesn’t have to be very formal.”
When interviewing candidates for academic hospitalist positions, Dr. Mark Williams says, “I look for residents who have won awards, who have laudatory letters of recommendation from their program director. I love letters that say this resident was in the top of their class, or the best we’ve seen in five years. I look for those who have done research, and those who published case report abstracts, which shows they’re industrious.”
Dr. Mark Williams also asks questions of candidates early in the process and listens carefully to their responses. “I especially look for good communication skills, which are so critical for hospitalists,” he says. “If someone has poor communication skills, they’ll have a tough time on the job.”
To determine their skills, “I’ll ask about their goals, and ask what they see as their weakness,” he says. “It’s very positive to see someone articulate their weaknesses.”
Before You Sign
When you’re presented with a contract, it’s time to take a close look at what’s being offered. “Before you sign anything, you need to come to an agreement with the other party in the contract that this is exactly what we agreed to. Otherwise, it’s no deal,” says Fred A. McCurdy, MD, PhD, MBA, FAAP, FACPE, professor and regional chairman of pediatrics, Texas Tech University Health Sciences Center at Amarillo. “Everything needs to be really specific in the offer letter or the contract—their duties, expectations—all clarified up front.”
Examine the benefits, including retirement and insurance. Ideally, you want disability insurance—and malpractice insurance with tail coverage is essential. (Tail coverage, also called extended reporting coverage, covers you after you leave a group in case a patient files a lawsuit years after the fact.)
Make sure you understand what the contract says, and make sure your employer doesn’t hold too much power. “Check to see if you can be assigned to areas of work that would be a deal-breaker—if you can be sent to another city or state to work, for example,” says Dr. McCurdy.
As a new physician, you do have some leverage to negotiate for better compensation or schedule. Dr. McCurdy says of recent residents, “The two biggest benefits they bring to the table are their youth and the fact that they’re current and up to date on what’s going on in [internal medicine]. They have energy, and they’ll bring energy to the program; and they’ve spent three years in intense study and have the most up-to-date knowledge of anyone you can hire.”
Point out these advantages to the right interviewer, and you may be able to negotiate.
Dr. Badlani encourages new hires to negotiate their moving expenses, bonuses, and malpractice insurance.
But keep in mind that not all hospital medicine programs can or will negotiate. “It’s quite variable,” admits Dr. McCurdy.
Dr. Harris’ program is a prime example. “In my experience, we don’t have a tremendous amount of negotiating,” she says. “Basically, we say, ‘Here’s the deal.’ ”
Dr. McCurdy advises having someone else read the contract for you. “When you’re enthusiastic about a new job, you don’t see everything,” he explains. “And you need to have a lawyer read it to make sure it’s a correctly constructed legal document.”
Dr. Harris simply advises that you “read through the contract with a fine-tooth comb. Does it have a non-compete clause that prohibits you from practicing in the region after you leave? You can find a job [locally] without this clause.”
Dr. McCurdy has allowed new hires to strike these clauses from their contracts, but it’s a trade-off. “Non-compete clauses are hard to enforce,” he acknowledges. “Our boilerplate contract has one, because we want to send the message that we don’t want to spend two years training you and then have you leave and go to work for the competition. So if [a candidate] wants to strike that clause from the contract, I’ll say that’s fine, but on the basis of that I’ll make it a binding three-year contract.”
What if, after researching, interviewing, reviewing the contract, and taking every step possible to ensure you get the best job, you find you’ve made a mistake? “Remember, your contract is only for one year,” Dr. Badlani points out. “You can always change next year if you don’t like your [first choice].” TH
Customize Your Education
A standard internal medicine residency program will only take you only so far in teaching you to be a hospitalist. The rest is up to you. “There have been some changes in resident training,” says Vineet Arora, MD, MA, assistant professor of medicine and associate program director, Internal Medicine Residency Program at the University of Chicago. “Future hospitalists should consider how current resident training may or may not help prepare them for a hospital medicine career.”
Given this advice, residents who plan to enter hospital medicine must be especially proactive in shaping their education, experience, and skills. The steps outlined here can serve as a general guide.
—Vineet Arora, MD, MA
Six Ways to Shape Your Residency Toward Hospital Medicine
1) Find a mentor: Your first step is to find a professor or working hospitalist who can help you plan and carry out your education. “Training to become a hospitalist is more than just being a super-resident,” explains Dr. Arora. “It carries special competencies.”
A hospitalist mentor can help you understand what your program does and does not offer, and how to accumulate the best knowledge and skills for a career in hospital medicine.
2) Practice applicable procedures: It’s important to note that your program’s procedures requirements may not be adequate for some hospitalist positions. This can hold true even for residency programs that follow the American Board of Internal Medicine (ABIM) procedural requirements.
“There’s been a change in procedural requirements in the last year,” says Dr. Arora. “Although the Board says you must be able to know, understand, and explain certain procedures it does not require that you perform these procedures competently. So, residents no longer need to demonstrate these procedures. If your program has adopted these requirements, you’ll be at a disadvantage in your job search.”
Check with your residency program director on your program’s requirements and how they match procedure requirements of your future employer. “I don’t think it should be a requirement for hospitalists, but it’s good to have,” says Bradley T. Rosen, MD, MBA, Division of General Internal Medicine at Cedars-Sinai Medical Center, Los Angeles, of the required procedures. “It depends on where you’re going to practice hospital medicine. In smaller, less urban hospitals and in less densely populated areas, the more versatile the hospitalist will have to be. The less support you have in terms of subspecialties, the more important it is to do procedures. Many hospitalists [in these environments] manage patients in the ICU—those patients need a lot of procedures.”
Every hospital will have its own credentialing criteria, but most match the ABIM requirements. “You’d have to know when you’re applying what you have and what you need,” says Dr. Rosen. “If you’re adept at doing procedures, that gives the advantage to you in a job search.”
Regardless of what type of hospital medicine position you want, document every procedure you do in residency. “Consider keeping a log book of your procedures to make sure they meet requirements for hospital credentialing committees,” advises Dr. Arora. “If you want to be a successful, competitive hospitalist [candidate], you have to keep a log book to prove your procedure experience.”
The good news is that if you need more experience with procedures for a certain position, you can get it on the job. “If you meet the hospital’s criteria you can be hired with basic privileges, then be given temporary privileges to perform certain procedures with proctoring, before those privileges become permanent,” says Dr. Rosen. “The ABIM requirements will get you in the door at most hospitals for those procedures.”
3) Add education in key areas: An internal medicine residency may not offer adequate training in some vital aspects of hospital medicine. “Supplement your education with key areas that may not be covered, such as perioperative medicine and hospital-acquired hazards,” advises Dr. Arora.
She recommends you sign up for an elective rotation in perioperative medicine and consultation. “A lot of hospitalists might be responsible for perioperative care or consultation, or surgical co-management,” she says. “This isn’t currently a core competency of many residency programs, so elective rotation is important to consider.”
Another area on which you should concentrate is the prevention against hospital-acquired conditions. These include deep vein thrombosis (DVT), nosocomial infections, delirium, pressure ulcers, and falls.
4) Study communication methods: Look beyond the clinical knowledge and skills you need, and learn how hospital medicine works. This includes methods of communication for discharge and general communication with patients’ primary care providers (PCPs).
“The system in which residents train may not be good about communication with primary care physicians,” says Dr. Arora. “It’s important to think about timely discharge summaries and how they can affect your practice. You may not find this on the academic side, so it’s worth rotating in a community-based hospital to see what a workday is like. Maybe your hospital [communicates with PCPs] by e-mail, and another uses faxes. You need to understand how communication takes place.”
Jeanne M. Farnan, MD, hospitalist scholar at The University of Chicago Hospitals, Section, General Internal Medicine, believes today’s residents are experienced in transitions of care due to the recently reduced duty hours. “Communications for these transitions will become more of a priority, [and] much more pertinent for medical school deans and directors,” she speculates. “These communications need to be a more structured curriculum so that residents learn to communicate more effectively with other physicians, working as part of a multi-disciplinary team.”
Meanwhile, residents can find role models for good communications. “See what the attending physicians are doing,” advises Dr. Farnan. “These skills can be learned on the job, because clearly residents have been learning this way. Look to see how physicians do it well, the strategies they use. Talk to all the stakeholders; ask PCPs what details they like to see when receiving communications about their hospitalized patients.”
5) Perform a QI project: Hospitalists play a vital role in their hospitals’ quality improvement (QI) efforts. Regardless of which career path you’re pursuing within hospital medicine, you should focus on QI in your residency.
“You’ll need basic skills in quality improvement and patient safety,” says Dr. Arora. “It’s best if you can become part of a QI committee or be mentored on a QI project.”
Read about QI tools and resources on SHM’s Web site (www.hospitalmedicine.org) under “Quality & Safety.”
6) Self-study: Supplement your residency education by reading on your own. “Targeted reading will be helpful, especially if you’re not doing a fellowship,” says Dr. Arora. Read The Hospitalist and the Journal of Hospital Medicine, pick up a textbook on hospital medicine, and study SHM’s The Core Competencies in Hospital Medicine: A Framework for Curriculum Development (available online at www.hospitalmedicine.org under “Education.”)
“The Core Competencies are designed as a blueprint or framework to help faculty design their curricula for inpatient training,” explains co-editor Alpesh Amin, MD, MBA, FACP, professor and executive director of the hospitalist program at the University of California, Irvine, School of Medicine. “The competencies talk about the clinical issues, procedures, and systems-based practice” performed in hospital medicine. “It’s not meant to be comprehensive, but it’s pretty inclusive of what we thought hospitalists should know,” he says.
Each chapter in The Core Competencies includes knowledge, skills, and attitudes for the subject covered. “Chapters could be used as [residents] try to develop skills around these specific areas,” says Dr. Amin.
Your residency experience is vital to becoming a good physician, but it may not be enough to make you truly competitive in the field of hospital medicine. “Residency is a good foundation, but you need to be aware of how to make the best of it,” advises Dr. Arora. Follow these steps, and you’ll be better prepared to join your first choice of hospital medicine practice. TH
A standard internal medicine residency program will only take you only so far in teaching you to be a hospitalist. The rest is up to you. “There have been some changes in resident training,” says Vineet Arora, MD, MA, assistant professor of medicine and associate program director, Internal Medicine Residency Program at the University of Chicago. “Future hospitalists should consider how current resident training may or may not help prepare them for a hospital medicine career.”
Given this advice, residents who plan to enter hospital medicine must be especially proactive in shaping their education, experience, and skills. The steps outlined here can serve as a general guide.
—Vineet Arora, MD, MA
Six Ways to Shape Your Residency Toward Hospital Medicine
1) Find a mentor: Your first step is to find a professor or working hospitalist who can help you plan and carry out your education. “Training to become a hospitalist is more than just being a super-resident,” explains Dr. Arora. “It carries special competencies.”
A hospitalist mentor can help you understand what your program does and does not offer, and how to accumulate the best knowledge and skills for a career in hospital medicine.
2) Practice applicable procedures: It’s important to note that your program’s procedures requirements may not be adequate for some hospitalist positions. This can hold true even for residency programs that follow the American Board of Internal Medicine (ABIM) procedural requirements.
“There’s been a change in procedural requirements in the last year,” says Dr. Arora. “Although the Board says you must be able to know, understand, and explain certain procedures it does not require that you perform these procedures competently. So, residents no longer need to demonstrate these procedures. If your program has adopted these requirements, you’ll be at a disadvantage in your job search.”
Check with your residency program director on your program’s requirements and how they match procedure requirements of your future employer. “I don’t think it should be a requirement for hospitalists, but it’s good to have,” says Bradley T. Rosen, MD, MBA, Division of General Internal Medicine at Cedars-Sinai Medical Center, Los Angeles, of the required procedures. “It depends on where you’re going to practice hospital medicine. In smaller, less urban hospitals and in less densely populated areas, the more versatile the hospitalist will have to be. The less support you have in terms of subspecialties, the more important it is to do procedures. Many hospitalists [in these environments] manage patients in the ICU—those patients need a lot of procedures.”
Every hospital will have its own credentialing criteria, but most match the ABIM requirements. “You’d have to know when you’re applying what you have and what you need,” says Dr. Rosen. “If you’re adept at doing procedures, that gives the advantage to you in a job search.”
Regardless of what type of hospital medicine position you want, document every procedure you do in residency. “Consider keeping a log book of your procedures to make sure they meet requirements for hospital credentialing committees,” advises Dr. Arora. “If you want to be a successful, competitive hospitalist [candidate], you have to keep a log book to prove your procedure experience.”
The good news is that if you need more experience with procedures for a certain position, you can get it on the job. “If you meet the hospital’s criteria you can be hired with basic privileges, then be given temporary privileges to perform certain procedures with proctoring, before those privileges become permanent,” says Dr. Rosen. “The ABIM requirements will get you in the door at most hospitals for those procedures.”
3) Add education in key areas: An internal medicine residency may not offer adequate training in some vital aspects of hospital medicine. “Supplement your education with key areas that may not be covered, such as perioperative medicine and hospital-acquired hazards,” advises Dr. Arora.
She recommends you sign up for an elective rotation in perioperative medicine and consultation. “A lot of hospitalists might be responsible for perioperative care or consultation, or surgical co-management,” she says. “This isn’t currently a core competency of many residency programs, so elective rotation is important to consider.”
Another area on which you should concentrate is the prevention against hospital-acquired conditions. These include deep vein thrombosis (DVT), nosocomial infections, delirium, pressure ulcers, and falls.
4) Study communication methods: Look beyond the clinical knowledge and skills you need, and learn how hospital medicine works. This includes methods of communication for discharge and general communication with patients’ primary care providers (PCPs).
“The system in which residents train may not be good about communication with primary care physicians,” says Dr. Arora. “It’s important to think about timely discharge summaries and how they can affect your practice. You may not find this on the academic side, so it’s worth rotating in a community-based hospital to see what a workday is like. Maybe your hospital [communicates with PCPs] by e-mail, and another uses faxes. You need to understand how communication takes place.”
Jeanne M. Farnan, MD, hospitalist scholar at The University of Chicago Hospitals, Section, General Internal Medicine, believes today’s residents are experienced in transitions of care due to the recently reduced duty hours. “Communications for these transitions will become more of a priority, [and] much more pertinent for medical school deans and directors,” she speculates. “These communications need to be a more structured curriculum so that residents learn to communicate more effectively with other physicians, working as part of a multi-disciplinary team.”
Meanwhile, residents can find role models for good communications. “See what the attending physicians are doing,” advises Dr. Farnan. “These skills can be learned on the job, because clearly residents have been learning this way. Look to see how physicians do it well, the strategies they use. Talk to all the stakeholders; ask PCPs what details they like to see when receiving communications about their hospitalized patients.”
5) Perform a QI project: Hospitalists play a vital role in their hospitals’ quality improvement (QI) efforts. Regardless of which career path you’re pursuing within hospital medicine, you should focus on QI in your residency.
“You’ll need basic skills in quality improvement and patient safety,” says Dr. Arora. “It’s best if you can become part of a QI committee or be mentored on a QI project.”
Read about QI tools and resources on SHM’s Web site (www.hospitalmedicine.org) under “Quality & Safety.”
6) Self-study: Supplement your residency education by reading on your own. “Targeted reading will be helpful, especially if you’re not doing a fellowship,” says Dr. Arora. Read The Hospitalist and the Journal of Hospital Medicine, pick up a textbook on hospital medicine, and study SHM’s The Core Competencies in Hospital Medicine: A Framework for Curriculum Development (available online at www.hospitalmedicine.org under “Education.”)
“The Core Competencies are designed as a blueprint or framework to help faculty design their curricula for inpatient training,” explains co-editor Alpesh Amin, MD, MBA, FACP, professor and executive director of the hospitalist program at the University of California, Irvine, School of Medicine. “The competencies talk about the clinical issues, procedures, and systems-based practice” performed in hospital medicine. “It’s not meant to be comprehensive, but it’s pretty inclusive of what we thought hospitalists should know,” he says.
Each chapter in The Core Competencies includes knowledge, skills, and attitudes for the subject covered. “Chapters could be used as [residents] try to develop skills around these specific areas,” says Dr. Amin.
Your residency experience is vital to becoming a good physician, but it may not be enough to make you truly competitive in the field of hospital medicine. “Residency is a good foundation, but you need to be aware of how to make the best of it,” advises Dr. Arora. Follow these steps, and you’ll be better prepared to join your first choice of hospital medicine practice. TH
A standard internal medicine residency program will only take you only so far in teaching you to be a hospitalist. The rest is up to you. “There have been some changes in resident training,” says Vineet Arora, MD, MA, assistant professor of medicine and associate program director, Internal Medicine Residency Program at the University of Chicago. “Future hospitalists should consider how current resident training may or may not help prepare them for a hospital medicine career.”
Given this advice, residents who plan to enter hospital medicine must be especially proactive in shaping their education, experience, and skills. The steps outlined here can serve as a general guide.
—Vineet Arora, MD, MA
Six Ways to Shape Your Residency Toward Hospital Medicine
1) Find a mentor: Your first step is to find a professor or working hospitalist who can help you plan and carry out your education. “Training to become a hospitalist is more than just being a super-resident,” explains Dr. Arora. “It carries special competencies.”
A hospitalist mentor can help you understand what your program does and does not offer, and how to accumulate the best knowledge and skills for a career in hospital medicine.
2) Practice applicable procedures: It’s important to note that your program’s procedures requirements may not be adequate for some hospitalist positions. This can hold true even for residency programs that follow the American Board of Internal Medicine (ABIM) procedural requirements.
“There’s been a change in procedural requirements in the last year,” says Dr. Arora. “Although the Board says you must be able to know, understand, and explain certain procedures it does not require that you perform these procedures competently. So, residents no longer need to demonstrate these procedures. If your program has adopted these requirements, you’ll be at a disadvantage in your job search.”
Check with your residency program director on your program’s requirements and how they match procedure requirements of your future employer. “I don’t think it should be a requirement for hospitalists, but it’s good to have,” says Bradley T. Rosen, MD, MBA, Division of General Internal Medicine at Cedars-Sinai Medical Center, Los Angeles, of the required procedures. “It depends on where you’re going to practice hospital medicine. In smaller, less urban hospitals and in less densely populated areas, the more versatile the hospitalist will have to be. The less support you have in terms of subspecialties, the more important it is to do procedures. Many hospitalists [in these environments] manage patients in the ICU—those patients need a lot of procedures.”
Every hospital will have its own credentialing criteria, but most match the ABIM requirements. “You’d have to know when you’re applying what you have and what you need,” says Dr. Rosen. “If you’re adept at doing procedures, that gives the advantage to you in a job search.”
Regardless of what type of hospital medicine position you want, document every procedure you do in residency. “Consider keeping a log book of your procedures to make sure they meet requirements for hospital credentialing committees,” advises Dr. Arora. “If you want to be a successful, competitive hospitalist [candidate], you have to keep a log book to prove your procedure experience.”
The good news is that if you need more experience with procedures for a certain position, you can get it on the job. “If you meet the hospital’s criteria you can be hired with basic privileges, then be given temporary privileges to perform certain procedures with proctoring, before those privileges become permanent,” says Dr. Rosen. “The ABIM requirements will get you in the door at most hospitals for those procedures.”
3) Add education in key areas: An internal medicine residency may not offer adequate training in some vital aspects of hospital medicine. “Supplement your education with key areas that may not be covered, such as perioperative medicine and hospital-acquired hazards,” advises Dr. Arora.
She recommends you sign up for an elective rotation in perioperative medicine and consultation. “A lot of hospitalists might be responsible for perioperative care or consultation, or surgical co-management,” she says. “This isn’t currently a core competency of many residency programs, so elective rotation is important to consider.”
Another area on which you should concentrate is the prevention against hospital-acquired conditions. These include deep vein thrombosis (DVT), nosocomial infections, delirium, pressure ulcers, and falls.
4) Study communication methods: Look beyond the clinical knowledge and skills you need, and learn how hospital medicine works. This includes methods of communication for discharge and general communication with patients’ primary care providers (PCPs).
“The system in which residents train may not be good about communication with primary care physicians,” says Dr. Arora. “It’s important to think about timely discharge summaries and how they can affect your practice. You may not find this on the academic side, so it’s worth rotating in a community-based hospital to see what a workday is like. Maybe your hospital [communicates with PCPs] by e-mail, and another uses faxes. You need to understand how communication takes place.”
Jeanne M. Farnan, MD, hospitalist scholar at The University of Chicago Hospitals, Section, General Internal Medicine, believes today’s residents are experienced in transitions of care due to the recently reduced duty hours. “Communications for these transitions will become more of a priority, [and] much more pertinent for medical school deans and directors,” she speculates. “These communications need to be a more structured curriculum so that residents learn to communicate more effectively with other physicians, working as part of a multi-disciplinary team.”
Meanwhile, residents can find role models for good communications. “See what the attending physicians are doing,” advises Dr. Farnan. “These skills can be learned on the job, because clearly residents have been learning this way. Look to see how physicians do it well, the strategies they use. Talk to all the stakeholders; ask PCPs what details they like to see when receiving communications about their hospitalized patients.”
5) Perform a QI project: Hospitalists play a vital role in their hospitals’ quality improvement (QI) efforts. Regardless of which career path you’re pursuing within hospital medicine, you should focus on QI in your residency.
“You’ll need basic skills in quality improvement and patient safety,” says Dr. Arora. “It’s best if you can become part of a QI committee or be mentored on a QI project.”
Read about QI tools and resources on SHM’s Web site (www.hospitalmedicine.org) under “Quality & Safety.”
6) Self-study: Supplement your residency education by reading on your own. “Targeted reading will be helpful, especially if you’re not doing a fellowship,” says Dr. Arora. Read The Hospitalist and the Journal of Hospital Medicine, pick up a textbook on hospital medicine, and study SHM’s The Core Competencies in Hospital Medicine: A Framework for Curriculum Development (available online at www.hospitalmedicine.org under “Education.”)
“The Core Competencies are designed as a blueprint or framework to help faculty design their curricula for inpatient training,” explains co-editor Alpesh Amin, MD, MBA, FACP, professor and executive director of the hospitalist program at the University of California, Irvine, School of Medicine. “The competencies talk about the clinical issues, procedures, and systems-based practice” performed in hospital medicine. “It’s not meant to be comprehensive, but it’s pretty inclusive of what we thought hospitalists should know,” he says.
Each chapter in The Core Competencies includes knowledge, skills, and attitudes for the subject covered. “Chapters could be used as [residents] try to develop skills around these specific areas,” says Dr. Amin.
Your residency experience is vital to becoming a good physician, but it may not be enough to make you truly competitive in the field of hospital medicine. “Residency is a good foundation, but you need to be aware of how to make the best of it,” advises Dr. Arora. Follow these steps, and you’ll be better prepared to join your first choice of hospital medicine practice. TH
Reasons to Research

If you’re a community-based hospitalist who hasn’t conducted research since your residency or medical school, you may want to consider undertaking a research project to broaden your career and your skill set.
Why Add Research to Your Workload?
If you’re a non-researcher, why would you want to add this new component to an already busy workload?
“I think there are a number of reasons why a hospitalist might want to get involved in doing research,” says Peter Lindenauer, MD, MSc, FACP, medical director, Clinical and Quality Informatics, Baystate Health in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine in Boston. You may decide to undertake research because you’re curious about a specific area and want to make some new discoveries—and expand the general body of knowledge in that area. Or you may undertake a research project, says Dr. Lindenauer, because of “a desire to help your patients more specifically—to provide better care based on your own research findings.”
But some non-academic hospitalists may decide to lead a research project for more personal reasons. “I’m someone whose career has benefited from doing research,” admits Dr. Lindenauer, pointing out that a published research study brings recognition to the study author. “It can help you establish a professional niche. By doing research, you can become a highly visible member of our professional society.”
And a more basic reason, says Dr. Lindenauer, is that “research is something that can provide diversification to your work life, and it can bring professional satisfaction. It spices up one’s career.”
QI: The Perfect Fit
A full-time hospitalist who is a novice or an inexperienced researcher obviously isn’t in a position to lead a multi-center, randomized trial or conduct extensive lab work. There is another type of research, however, that seems the perfect fit for a community-based hospitalist.
“Rather than setting the bar at an unattainable level, hospitalists should consider getting involved in quality improvement research, since hospitalists are often ideally suited to participate [in] and lead the interventions themselves,” says Dr. Lindenauer. “It’s not the only kind of research, but it’s a natural, given the roles that hospitalists play. However, hospitalists can be involved in clinical trials, in analyses of secondary data, and even in doing intervention studies at their own institutions.”
And a quality improvement project, if conducted correctly, is likely to be accepted for publication and/or presentation. “While QI research is somewhat different than traditional, clinical research, there’s an increasing interest in seeing [QI] research published in established medical journals,” explains Dr. Lindenauer. “Some hospitalists have been very successful at doing this and [in] publishing the results and … giving presentations.”
Steps to Get Started
So how should you go about setting up your first QI research project?
Your first step—and possibly the most important—is selecting a research topic. “It’s important to come up with good research questions,” says Dr. Lindenauer. “One framework for choosing a topic is the acronym FINER, which stands for: [is it] feasible, interesting, novel, ethical, and relevant?”
Once you have a likely focus for quality improvement, outline how you mean to go about the project. “You have to choose a study plan and make sure the plan matches the question,” says Dr. Lindenauer.
When you have a basic idea for your project, says Dr. Lindenauer, “You have to find time in an already busy life, and you have to find support.” For one thing, very few questions can be answered by a single physician. For another, you’ll need your hospital’s buy-in.
“For QI research, it’s natural to go to your hospital’s quality improvement department,” says Dr. Lindenauer. “Ask the director of the department to sit down, and then find out what’s on the hospital’s agenda. You’ll need to find some common ground, some overlap between your interests and the hospital’s. Support is so important, and given all the external pressures for improving quality, it’s unlikely that your quality improvement department will support a project that doesn’t align with their plans or focus. So align your interests with those of the hospital and go from there.”
Ideally, you’ll also find some mentorship before or during your first project. “At a community hospital, where no faculty is available, you must identify potential mentors from outside your hospital,” says Dr. Lindenauer. “Find faculty at a university that your hospital is affiliated with or someone who was a mentor to you during your residency or medical school. And sometimes a quality improvement department can supply a mentor.”
Lastly, “find some degree of training,” advises Dr. Lindenauer. “SHM has regularly offered workshops as a first step to starting research. Other societies offer short, intensive training—or a fellowship. If you get … charged up doing research, find a fellowship.”
Build in Review by an IRB
There’s one more crucial step involved in setting up and conducting a QI research project, assuming you want to get your results published: “You should notify [your institutional review board] and have them look at your project,” says Dr. Lindenauer. “The best time to do this is during the conceptualization, once you have your research protocol.”
You should take care of this on your own because your QI department isn’t likely to think it’s necessary. “There’s often a disconnect between the perceived need for the involvement of the IRB between researchers and QI folks,” explains Dr. Lindenauer. “Usually, QI departments don’t tend to seek IRB review for their projects. But if you’re contemplating publishing your research—which is typically the ultimate goal to a research project—this always requires IRB review. This is true even though the case is often that QI projects are exempt.”
One place to begin your education on QI research is on SHM’s Web site, under “Quality & Safety,” where you can browse quality improvement tools and several quality improvement resource rooms. TH
Jane Jerrard has written for The Hospitalist since 2005.
If you’re a community-based hospitalist who hasn’t conducted research since your residency or medical school, you may want to consider undertaking a research project to broaden your career and your skill set.
Why Add Research to Your Workload?
If you’re a non-researcher, why would you want to add this new component to an already busy workload?
“I think there are a number of reasons why a hospitalist might want to get involved in doing research,” says Peter Lindenauer, MD, MSc, FACP, medical director, Clinical and Quality Informatics, Baystate Health in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine in Boston. You may decide to undertake research because you’re curious about a specific area and want to make some new discoveries—and expand the general body of knowledge in that area. Or you may undertake a research project, says Dr. Lindenauer, because of “a desire to help your patients more specifically—to provide better care based on your own research findings.”
But some non-academic hospitalists may decide to lead a research project for more personal reasons. “I’m someone whose career has benefited from doing research,” admits Dr. Lindenauer, pointing out that a published research study brings recognition to the study author. “It can help you establish a professional niche. By doing research, you can become a highly visible member of our professional society.”
And a more basic reason, says Dr. Lindenauer, is that “research is something that can provide diversification to your work life, and it can bring professional satisfaction. It spices up one’s career.”
QI: The Perfect Fit
A full-time hospitalist who is a novice or an inexperienced researcher obviously isn’t in a position to lead a multi-center, randomized trial or conduct extensive lab work. There is another type of research, however, that seems the perfect fit for a community-based hospitalist.
“Rather than setting the bar at an unattainable level, hospitalists should consider getting involved in quality improvement research, since hospitalists are often ideally suited to participate [in] and lead the interventions themselves,” says Dr. Lindenauer. “It’s not the only kind of research, but it’s a natural, given the roles that hospitalists play. However, hospitalists can be involved in clinical trials, in analyses of secondary data, and even in doing intervention studies at their own institutions.”
And a quality improvement project, if conducted correctly, is likely to be accepted for publication and/or presentation. “While QI research is somewhat different than traditional, clinical research, there’s an increasing interest in seeing [QI] research published in established medical journals,” explains Dr. Lindenauer. “Some hospitalists have been very successful at doing this and [in] publishing the results and … giving presentations.”
Steps to Get Started
So how should you go about setting up your first QI research project?
Your first step—and possibly the most important—is selecting a research topic. “It’s important to come up with good research questions,” says Dr. Lindenauer. “One framework for choosing a topic is the acronym FINER, which stands for: [is it] feasible, interesting, novel, ethical, and relevant?”
Once you have a likely focus for quality improvement, outline how you mean to go about the project. “You have to choose a study plan and make sure the plan matches the question,” says Dr. Lindenauer.
When you have a basic idea for your project, says Dr. Lindenauer, “You have to find time in an already busy life, and you have to find support.” For one thing, very few questions can be answered by a single physician. For another, you’ll need your hospital’s buy-in.
“For QI research, it’s natural to go to your hospital’s quality improvement department,” says Dr. Lindenauer. “Ask the director of the department to sit down, and then find out what’s on the hospital’s agenda. You’ll need to find some common ground, some overlap between your interests and the hospital’s. Support is so important, and given all the external pressures for improving quality, it’s unlikely that your quality improvement department will support a project that doesn’t align with their plans or focus. So align your interests with those of the hospital and go from there.”
Ideally, you’ll also find some mentorship before or during your first project. “At a community hospital, where no faculty is available, you must identify potential mentors from outside your hospital,” says Dr. Lindenauer. “Find faculty at a university that your hospital is affiliated with or someone who was a mentor to you during your residency or medical school. And sometimes a quality improvement department can supply a mentor.”
Lastly, “find some degree of training,” advises Dr. Lindenauer. “SHM has regularly offered workshops as a first step to starting research. Other societies offer short, intensive training—or a fellowship. If you get … charged up doing research, find a fellowship.”
Build in Review by an IRB
There’s one more crucial step involved in setting up and conducting a QI research project, assuming you want to get your results published: “You should notify [your institutional review board] and have them look at your project,” says Dr. Lindenauer. “The best time to do this is during the conceptualization, once you have your research protocol.”
You should take care of this on your own because your QI department isn’t likely to think it’s necessary. “There’s often a disconnect between the perceived need for the involvement of the IRB between researchers and QI folks,” explains Dr. Lindenauer. “Usually, QI departments don’t tend to seek IRB review for their projects. But if you’re contemplating publishing your research—which is typically the ultimate goal to a research project—this always requires IRB review. This is true even though the case is often that QI projects are exempt.”
One place to begin your education on QI research is on SHM’s Web site, under “Quality & Safety,” where you can browse quality improvement tools and several quality improvement resource rooms. TH
Jane Jerrard has written for The Hospitalist since 2005.
If you’re a community-based hospitalist who hasn’t conducted research since your residency or medical school, you may want to consider undertaking a research project to broaden your career and your skill set.
Why Add Research to Your Workload?
If you’re a non-researcher, why would you want to add this new component to an already busy workload?
“I think there are a number of reasons why a hospitalist might want to get involved in doing research,” says Peter Lindenauer, MD, MSc, FACP, medical director, Clinical and Quality Informatics, Baystate Health in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine in Boston. You may decide to undertake research because you’re curious about a specific area and want to make some new discoveries—and expand the general body of knowledge in that area. Or you may undertake a research project, says Dr. Lindenauer, because of “a desire to help your patients more specifically—to provide better care based on your own research findings.”
But some non-academic hospitalists may decide to lead a research project for more personal reasons. “I’m someone whose career has benefited from doing research,” admits Dr. Lindenauer, pointing out that a published research study brings recognition to the study author. “It can help you establish a professional niche. By doing research, you can become a highly visible member of our professional society.”
And a more basic reason, says Dr. Lindenauer, is that “research is something that can provide diversification to your work life, and it can bring professional satisfaction. It spices up one’s career.”
QI: The Perfect Fit
A full-time hospitalist who is a novice or an inexperienced researcher obviously isn’t in a position to lead a multi-center, randomized trial or conduct extensive lab work. There is another type of research, however, that seems the perfect fit for a community-based hospitalist.
“Rather than setting the bar at an unattainable level, hospitalists should consider getting involved in quality improvement research, since hospitalists are often ideally suited to participate [in] and lead the interventions themselves,” says Dr. Lindenauer. “It’s not the only kind of research, but it’s a natural, given the roles that hospitalists play. However, hospitalists can be involved in clinical trials, in analyses of secondary data, and even in doing intervention studies at their own institutions.”
And a quality improvement project, if conducted correctly, is likely to be accepted for publication and/or presentation. “While QI research is somewhat different than traditional, clinical research, there’s an increasing interest in seeing [QI] research published in established medical journals,” explains Dr. Lindenauer. “Some hospitalists have been very successful at doing this and [in] publishing the results and … giving presentations.”
Steps to Get Started
So how should you go about setting up your first QI research project?
Your first step—and possibly the most important—is selecting a research topic. “It’s important to come up with good research questions,” says Dr. Lindenauer. “One framework for choosing a topic is the acronym FINER, which stands for: [is it] feasible, interesting, novel, ethical, and relevant?”
Once you have a likely focus for quality improvement, outline how you mean to go about the project. “You have to choose a study plan and make sure the plan matches the question,” says Dr. Lindenauer.
When you have a basic idea for your project, says Dr. Lindenauer, “You have to find time in an already busy life, and you have to find support.” For one thing, very few questions can be answered by a single physician. For another, you’ll need your hospital’s buy-in.
“For QI research, it’s natural to go to your hospital’s quality improvement department,” says Dr. Lindenauer. “Ask the director of the department to sit down, and then find out what’s on the hospital’s agenda. You’ll need to find some common ground, some overlap between your interests and the hospital’s. Support is so important, and given all the external pressures for improving quality, it’s unlikely that your quality improvement department will support a project that doesn’t align with their plans or focus. So align your interests with those of the hospital and go from there.”
Ideally, you’ll also find some mentorship before or during your first project. “At a community hospital, where no faculty is available, you must identify potential mentors from outside your hospital,” says Dr. Lindenauer. “Find faculty at a university that your hospital is affiliated with or someone who was a mentor to you during your residency or medical school. And sometimes a quality improvement department can supply a mentor.”
Lastly, “find some degree of training,” advises Dr. Lindenauer. “SHM has regularly offered workshops as a first step to starting research. Other societies offer short, intensive training—or a fellowship. If you get … charged up doing research, find a fellowship.”
Build in Review by an IRB
There’s one more crucial step involved in setting up and conducting a QI research project, assuming you want to get your results published: “You should notify [your institutional review board] and have them look at your project,” says Dr. Lindenauer. “The best time to do this is during the conceptualization, once you have your research protocol.”
You should take care of this on your own because your QI department isn’t likely to think it’s necessary. “There’s often a disconnect between the perceived need for the involvement of the IRB between researchers and QI folks,” explains Dr. Lindenauer. “Usually, QI departments don’t tend to seek IRB review for their projects. But if you’re contemplating publishing your research—which is typically the ultimate goal to a research project—this always requires IRB review. This is true even though the case is often that QI projects are exempt.”
One place to begin your education on QI research is on SHM’s Web site, under “Quality & Safety,” where you can browse quality improvement tools and several quality improvement resource rooms. TH
Jane Jerrard has written for The Hospitalist since 2005.
Federal Flu Fighters

Experts say that a pandemic flu outbreak will hit the United States—a pandemic large enough to stretch our healthcare resources to the breaking point and overwhelm hospitals.
“They say it’s not if, but when,” says James C. Pile, MD, FACP, Division of Hospital Medicine, Case Western Reserve University, MetroHealth Medical Center, Cleveland, Ohio, an infectious diseases specialist with a longstanding interest in bioterrorism/pandemic preparedness, and former editor of The Hospitalist.
Your Government at Work
The federal government is taking a lead role in preparing for this outbreak or outbreaks. President George W. Bush issued a National Strategy for Pandemic Influenza in November 2005, which focuses on measures to slow or stop the spread of a pandemic flu and on “sustaining infrastructure and mitigating impact to the economy and the functioning of society.”
That strategy charges the Department of Health and Human Services (HHS) with leading federal pandemic preparedness. The HHS is working with state and local agencies on planning and has made $600 million available for state and local preparedness efforts, including the exercising of pandemic plans across communities and at all levels of government.
Total congressional funding for pandemic flu preparedness, says Dr. Pile, is “somewhere in the neighborhood of $5 billion dollars.”
A Working Plan
In May 2006, President Bush released the Implementation Plan for the National Strategy, which stipulates more than 300 actions for federal departments and agencies and sets clear expectations for state and local governments. It also provides guidance for all federal departments and agencies on the development of their own plans.
The latest update on the Implementation Plan (released in December 2006) lists dozens of action items, including:
- The Department of Homeland Security will provide emergency response element training (e.g., incident management, triage, security, and communications) and provide assistance, when requested, to state, local, and public health entities within six months.
- HHS will work with state and local governments to develop protocols for the distribution of critical medical materials such as ventilators in times of medical emergency, also within six months.
- HHS will prepare guidance for local Medical Reserve Corps coordinators describing the role of the Corps during a pandemic. The Medical Reserve Corps comprises teams of local volunteer medical and public health professionals who can contribute their skills and expertise during times of need.
For the latest details on the Implementation Plan and the status of these and other action items, visit www.pandemicflu.gov.
Federal, State, and Local–A Crucial Mix
In addition to providing overall planning and support, says Dr. Pile, “the federal government will also be responsible for helping to supply assets to states and regions that may be overwhelmed” during a pandemic flu outbreak.
Specifically, the government oversees the Strategic National Stockpile (SNS) program, which manages large quantities of medicine and medical supplies. These materials are stockpiled, ready to use in the event of a public health emergency. When federal and local authorities agree that the SNS is needed, supplies will be delivered to any state within 12 hours. Each state has plans to distribute so-called push packs of medicine and medical supplies to affected communities as quickly as possible.
“I’m not sure the federal government will be able to reliably deliver these push packs in a timely manner in the event of a severe, multi-state pandemic,” says Dr. Pile. “During Hurricane Katrina, which certainly posed challenges different from a pandemic flu outbreak but also included a number of similarities, we saw the struggle of the national government to react quickly.” He believes that the stockpiles may not be adequate in a worst-case scenario, such as a pandemic flu on the scale of the 1918 flu epidemic.
“It’s clear there just aren’t enough mechanical ventilators in the country to provide adequate surge capacity in the event of a severe pandemic, with best estimates of 80,000 to 105,000 ventilators nationally, most of which are in use at any given time,” he says.
Another issue is how much help the federal government can actually provide in the event of a pandemic flu. “Some government agencies and individuals have stressed that if there is a really catastrophic national influenza pandemic, the cavalry is not necessarily going to be coming,” says Dr. Pile. “Individual hospitals and regions will very possibly need to rely on their intrinsic resources, at least initially.”
So when a pandemic flu outbreak begins, where can hospitals find support? “HHS will take the lead role at the federal level,” says Dr. Pile. “State departments of health will oversee the response for each state. And at the city and municipal level, it will vary.”
The Role of Hospitalists
At this point, while all levels of government are still shaping plans for handling pandemic flu, what should hospitalists do?
“Hopefully, they’re involved in planning within their own institutions and regionally,” says Dr. Pile. “If not, that’s a great role for them. However, a lot of the people involved in [pandemic flu response] planning are not familiar with hospitalists.”
Woodruff J. English II, MD, hospitalist and co-director of Hospitalist Program, Providence St. Vincent Medical Center, Portland, Ore., is in charge of emergency preparedness, including pandemic flu, for his institution. He worked with his state department of health and the CDC. After conducting a tabletop exercise, Providence St. Vincent Medical Center has a plan in place that includes a number of tents that can set up as triage space for admitting and screening patients, plans to secure the hospital against riots and looters, staffing issues, and much more. “We’re figuring out what questions to ask; I wouldn’t say we’re prepared,” says Dr. English. “We’re taking a careful look at how we do business.”
When a pandemic flu outbreak does occur, hospitalists throughout affected areas will definitely be involved.
“They’d play a front and center role,” speculates Dr. Pile. “Critical care would be rolled out of the critical care unit into other areas of the hospital. Clearly, there wouldn’t be enough critical care physicians, so hospitalists would have to step in.”
At this stage of the government’s Implementation Plan, your hospital medicine program may be called upon to help create your hospital’s preparedness plan for pandemic flu. If you haven’t been asked, check with your director or administrator to see if such a plan exists, perhaps as part of a general emergency preparedness plan.
With the support of the federal and state government, your hospital should be able to take some steps toward preparing for a major outbreak of pandemic flu. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Experts say that a pandemic flu outbreak will hit the United States—a pandemic large enough to stretch our healthcare resources to the breaking point and overwhelm hospitals.
“They say it’s not if, but when,” says James C. Pile, MD, FACP, Division of Hospital Medicine, Case Western Reserve University, MetroHealth Medical Center, Cleveland, Ohio, an infectious diseases specialist with a longstanding interest in bioterrorism/pandemic preparedness, and former editor of The Hospitalist.
Your Government at Work
The federal government is taking a lead role in preparing for this outbreak or outbreaks. President George W. Bush issued a National Strategy for Pandemic Influenza in November 2005, which focuses on measures to slow or stop the spread of a pandemic flu and on “sustaining infrastructure and mitigating impact to the economy and the functioning of society.”
That strategy charges the Department of Health and Human Services (HHS) with leading federal pandemic preparedness. The HHS is working with state and local agencies on planning and has made $600 million available for state and local preparedness efforts, including the exercising of pandemic plans across communities and at all levels of government.
Total congressional funding for pandemic flu preparedness, says Dr. Pile, is “somewhere in the neighborhood of $5 billion dollars.”
A Working Plan
In May 2006, President Bush released the Implementation Plan for the National Strategy, which stipulates more than 300 actions for federal departments and agencies and sets clear expectations for state and local governments. It also provides guidance for all federal departments and agencies on the development of their own plans.
The latest update on the Implementation Plan (released in December 2006) lists dozens of action items, including:
- The Department of Homeland Security will provide emergency response element training (e.g., incident management, triage, security, and communications) and provide assistance, when requested, to state, local, and public health entities within six months.
- HHS will work with state and local governments to develop protocols for the distribution of critical medical materials such as ventilators in times of medical emergency, also within six months.
- HHS will prepare guidance for local Medical Reserve Corps coordinators describing the role of the Corps during a pandemic. The Medical Reserve Corps comprises teams of local volunteer medical and public health professionals who can contribute their skills and expertise during times of need.
For the latest details on the Implementation Plan and the status of these and other action items, visit www.pandemicflu.gov.
Federal, State, and Local–A Crucial Mix
In addition to providing overall planning and support, says Dr. Pile, “the federal government will also be responsible for helping to supply assets to states and regions that may be overwhelmed” during a pandemic flu outbreak.
Specifically, the government oversees the Strategic National Stockpile (SNS) program, which manages large quantities of medicine and medical supplies. These materials are stockpiled, ready to use in the event of a public health emergency. When federal and local authorities agree that the SNS is needed, supplies will be delivered to any state within 12 hours. Each state has plans to distribute so-called push packs of medicine and medical supplies to affected communities as quickly as possible.
“I’m not sure the federal government will be able to reliably deliver these push packs in a timely manner in the event of a severe, multi-state pandemic,” says Dr. Pile. “During Hurricane Katrina, which certainly posed challenges different from a pandemic flu outbreak but also included a number of similarities, we saw the struggle of the national government to react quickly.” He believes that the stockpiles may not be adequate in a worst-case scenario, such as a pandemic flu on the scale of the 1918 flu epidemic.
“It’s clear there just aren’t enough mechanical ventilators in the country to provide adequate surge capacity in the event of a severe pandemic, with best estimates of 80,000 to 105,000 ventilators nationally, most of which are in use at any given time,” he says.
Another issue is how much help the federal government can actually provide in the event of a pandemic flu. “Some government agencies and individuals have stressed that if there is a really catastrophic national influenza pandemic, the cavalry is not necessarily going to be coming,” says Dr. Pile. “Individual hospitals and regions will very possibly need to rely on their intrinsic resources, at least initially.”
So when a pandemic flu outbreak begins, where can hospitals find support? “HHS will take the lead role at the federal level,” says Dr. Pile. “State departments of health will oversee the response for each state. And at the city and municipal level, it will vary.”
The Role of Hospitalists
At this point, while all levels of government are still shaping plans for handling pandemic flu, what should hospitalists do?
“Hopefully, they’re involved in planning within their own institutions and regionally,” says Dr. Pile. “If not, that’s a great role for them. However, a lot of the people involved in [pandemic flu response] planning are not familiar with hospitalists.”
Woodruff J. English II, MD, hospitalist and co-director of Hospitalist Program, Providence St. Vincent Medical Center, Portland, Ore., is in charge of emergency preparedness, including pandemic flu, for his institution. He worked with his state department of health and the CDC. After conducting a tabletop exercise, Providence St. Vincent Medical Center has a plan in place that includes a number of tents that can set up as triage space for admitting and screening patients, plans to secure the hospital against riots and looters, staffing issues, and much more. “We’re figuring out what questions to ask; I wouldn’t say we’re prepared,” says Dr. English. “We’re taking a careful look at how we do business.”
When a pandemic flu outbreak does occur, hospitalists throughout affected areas will definitely be involved.
“They’d play a front and center role,” speculates Dr. Pile. “Critical care would be rolled out of the critical care unit into other areas of the hospital. Clearly, there wouldn’t be enough critical care physicians, so hospitalists would have to step in.”
At this stage of the government’s Implementation Plan, your hospital medicine program may be called upon to help create your hospital’s preparedness plan for pandemic flu. If you haven’t been asked, check with your director or administrator to see if such a plan exists, perhaps as part of a general emergency preparedness plan.
With the support of the federal and state government, your hospital should be able to take some steps toward preparing for a major outbreak of pandemic flu. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Experts say that a pandemic flu outbreak will hit the United States—a pandemic large enough to stretch our healthcare resources to the breaking point and overwhelm hospitals.
“They say it’s not if, but when,” says James C. Pile, MD, FACP, Division of Hospital Medicine, Case Western Reserve University, MetroHealth Medical Center, Cleveland, Ohio, an infectious diseases specialist with a longstanding interest in bioterrorism/pandemic preparedness, and former editor of The Hospitalist.
Your Government at Work
The federal government is taking a lead role in preparing for this outbreak or outbreaks. President George W. Bush issued a National Strategy for Pandemic Influenza in November 2005, which focuses on measures to slow or stop the spread of a pandemic flu and on “sustaining infrastructure and mitigating impact to the economy and the functioning of society.”
That strategy charges the Department of Health and Human Services (HHS) with leading federal pandemic preparedness. The HHS is working with state and local agencies on planning and has made $600 million available for state and local preparedness efforts, including the exercising of pandemic plans across communities and at all levels of government.
Total congressional funding for pandemic flu preparedness, says Dr. Pile, is “somewhere in the neighborhood of $5 billion dollars.”
A Working Plan
In May 2006, President Bush released the Implementation Plan for the National Strategy, which stipulates more than 300 actions for federal departments and agencies and sets clear expectations for state and local governments. It also provides guidance for all federal departments and agencies on the development of their own plans.
The latest update on the Implementation Plan (released in December 2006) lists dozens of action items, including:
- The Department of Homeland Security will provide emergency response element training (e.g., incident management, triage, security, and communications) and provide assistance, when requested, to state, local, and public health entities within six months.
- HHS will work with state and local governments to develop protocols for the distribution of critical medical materials such as ventilators in times of medical emergency, also within six months.
- HHS will prepare guidance for local Medical Reserve Corps coordinators describing the role of the Corps during a pandemic. The Medical Reserve Corps comprises teams of local volunteer medical and public health professionals who can contribute their skills and expertise during times of need.
For the latest details on the Implementation Plan and the status of these and other action items, visit www.pandemicflu.gov.
Federal, State, and Local–A Crucial Mix
In addition to providing overall planning and support, says Dr. Pile, “the federal government will also be responsible for helping to supply assets to states and regions that may be overwhelmed” during a pandemic flu outbreak.
Specifically, the government oversees the Strategic National Stockpile (SNS) program, which manages large quantities of medicine and medical supplies. These materials are stockpiled, ready to use in the event of a public health emergency. When federal and local authorities agree that the SNS is needed, supplies will be delivered to any state within 12 hours. Each state has plans to distribute so-called push packs of medicine and medical supplies to affected communities as quickly as possible.
“I’m not sure the federal government will be able to reliably deliver these push packs in a timely manner in the event of a severe, multi-state pandemic,” says Dr. Pile. “During Hurricane Katrina, which certainly posed challenges different from a pandemic flu outbreak but also included a number of similarities, we saw the struggle of the national government to react quickly.” He believes that the stockpiles may not be adequate in a worst-case scenario, such as a pandemic flu on the scale of the 1918 flu epidemic.
“It’s clear there just aren’t enough mechanical ventilators in the country to provide adequate surge capacity in the event of a severe pandemic, with best estimates of 80,000 to 105,000 ventilators nationally, most of which are in use at any given time,” he says.
Another issue is how much help the federal government can actually provide in the event of a pandemic flu. “Some government agencies and individuals have stressed that if there is a really catastrophic national influenza pandemic, the cavalry is not necessarily going to be coming,” says Dr. Pile. “Individual hospitals and regions will very possibly need to rely on their intrinsic resources, at least initially.”
So when a pandemic flu outbreak begins, where can hospitals find support? “HHS will take the lead role at the federal level,” says Dr. Pile. “State departments of health will oversee the response for each state. And at the city and municipal level, it will vary.”
The Role of Hospitalists
At this point, while all levels of government are still shaping plans for handling pandemic flu, what should hospitalists do?
“Hopefully, they’re involved in planning within their own institutions and regionally,” says Dr. Pile. “If not, that’s a great role for them. However, a lot of the people involved in [pandemic flu response] planning are not familiar with hospitalists.”
Woodruff J. English II, MD, hospitalist and co-director of Hospitalist Program, Providence St. Vincent Medical Center, Portland, Ore., is in charge of emergency preparedness, including pandemic flu, for his institution. He worked with his state department of health and the CDC. After conducting a tabletop exercise, Providence St. Vincent Medical Center has a plan in place that includes a number of tents that can set up as triage space for admitting and screening patients, plans to secure the hospital against riots and looters, staffing issues, and much more. “We’re figuring out what questions to ask; I wouldn’t say we’re prepared,” says Dr. English. “We’re taking a careful look at how we do business.”
When a pandemic flu outbreak does occur, hospitalists throughout affected areas will definitely be involved.
“They’d play a front and center role,” speculates Dr. Pile. “Critical care would be rolled out of the critical care unit into other areas of the hospital. Clearly, there wouldn’t be enough critical care physicians, so hospitalists would have to step in.”
At this stage of the government’s Implementation Plan, your hospital medicine program may be called upon to help create your hospital’s preparedness plan for pandemic flu. If you haven’t been asked, check with your director or administrator to see if such a plan exists, perhaps as part of a general emergency preparedness plan.
With the support of the federal and state government, your hospital should be able to take some steps toward preparing for a major outbreak of pandemic flu. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Constructive Criticism, Part 2

This is the second in a two-part series on providing constructive criticism to your hospitalist peers. Part 1 appeared in the March issue on p. 12.
Have concerns about a colleague’s work performance? Then you have two main options: You can bring it up in a formal peer review (if it’s a clinical issue) or you can approach the individual yourself.
“Medicine is an art and a science. Many problems relate to the art side—communications and relationships, primarily,” says Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Conn. “You may need to talk to a colleague about how they approach family members or how they communicate with patients. In this instance, you’d offer more of a coaching comment.”
While you may hesitate to point out another hospitalist’s problem areas, keep in mind that it is constructive criticism.
“Physicians love to run things past colleagues,” says Kenneth G. Simone, DO, founder and president of Hospitalist and Practice Solutions, Veazie, Maine, and a consultant to hospital medicine groups. “Informal feedback can provide an unbiased and objective perspective, as opposed to [a formal peer review].”
When to Offer Constructive Criticism
In some practices, or for some individuals, sharing constructive criticism with peers is part of the job. “Informal peer discussions should take place every day,” advises Dr. Rohr. “While handoffs pose a risk for losing vital information, they are also an opportunity to consider alternatives for diagnosis and treatment that may benefit patients greatly.”
If this seems like a natural thing to do within your hospital medicine group, follow Dr. Rohr’s advice: “These discussions should be frank but nonjudgmental. If someone has a problem discussing cases in this manner, then the group leader needs to get involved. If a life-threatening error is exposed, then the formal peer review system needs to be activated.”
Providing Peer Feedback
When there is no personal conflict, you may still consider offering constructive criticism if you feel it’s warranted. “I think [peer feedback] is extremely important—if it’s done correctly,” says Dr. Simone. “It provides a safe haven for discussion and can contribute to professional growth.”
According to Dr. Simone, appropriate topics to discuss regarding a colleague’s performance include logistical problems within the practice, such as a doctor who is chronically late for morning rounds; continuity issues, such as a physician who fails to provide detailed information when handing off patients; communication breakdowns, such as forgetting to check out the labs pending on a newly admitted unit-patient with chest pain; behavioral issues, such as a physician who’s verbally abusive to the nurses or disruptive at morning rounds; problems with work ethic, responsiveness, or availability, such as the doctor who never responds to his/her beeper (necessitating a call from nursing to an accommodating provider who’s always willing and available to help); and general team play.
If you believe you need to address one of these topics regarding a colleague’s performance, plan the logistics of the discussion. “This is a conversation best held one on one—in private,” stresses Dr. Simone. “Don’t discuss these issues in front of colleagues, nurses, patients, families … and don’t do it at the end of a long, difficult day.
“Ideally, do it after hours and out of the workplace, though that can be difficult. Remove the person from the hospital floor or the office, and the emotions and adrenaline associated with work,” continues Dr. Simone. “If the environment is stressful, it will raise their defenses, making them more likely to be resistant and argumentative.”
Talking Points
When you offer constructive criticism, approach the topic carefully. “Take a non-confrontational approach,” says Dr. Simone. “Don’t raise your voice, and don’t take the discussion to a personal level. Use objective data as much as possible. Avoid saying ‘I feel that you’re …’ and instead use ‘Coming in 15 minutes late throws everyone’s schedule off.’ ”
Keep the conversation as casual and as light as possible. “This is not a peer review meeting,” Dr. Simone stresses. “Use a soft approach, and you might have greater success. Stay away from power words such as ‘you shouldn’t’ or ‘don’t.’ ”
Some phrases you might use include:
- “I find it helpful if I … ”
- “This has worked for me.”
- “Have you considered … ?”
Even if you use careful wording, don’t be surprised if the other hospitalist doesn’t react well—at least initially. “Unless you’re seasoned at doing this, the individual may get defensive,” warns Dr. Simone. “If you’re consistent throughout the conversation, show support, and are astute enough to break down their defenses, you should be effective.”
Also, keep your cool: “Don’t respond to defensiveness in like [manner],” says Dr. Simone. Throughout the conversation, show your support. “Convey that your intent is to help the individual—not harm them. Ask if you can be of help, and offer to be a resource” to help them improve.
Also remember that your colleague is part of the conversation. “Allow responses,” adds Dr. Simone. “Give them a chance to express themselves.”
End the conversation with an offer to follow up or suggest a next step. “Offer your personal help or suggest a resource such as the employee assistance program,” advises Dr. Simone. “You can check in with them from time to time, but if you have an unwilling party this may be construed as meddlesome. You must consider the personality involved and if you think they’d be amenable to continued conversations.”
Even without a formal follow-up, be sure to voice your approval if you see their negative behavior change. “If you take the time to provide criticism, you should also offer positive feedback if warranted,” says Dr. Simone. “Tell them they’re doing a great job.”
One final piece of advice regarding informal peer feedback: “Avoid writing anything down,” says Dr. Simone. “This may make it discoverable in a court of law, and it’s not your place to put the discussion in writing. If the issue is that serious, take it to the powers that be.” TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the second in a two-part series on providing constructive criticism to your hospitalist peers. Part 1 appeared in the March issue on p. 12.
Have concerns about a colleague’s work performance? Then you have two main options: You can bring it up in a formal peer review (if it’s a clinical issue) or you can approach the individual yourself.
“Medicine is an art and a science. Many problems relate to the art side—communications and relationships, primarily,” says Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Conn. “You may need to talk to a colleague about how they approach family members or how they communicate with patients. In this instance, you’d offer more of a coaching comment.”
While you may hesitate to point out another hospitalist’s problem areas, keep in mind that it is constructive criticism.
“Physicians love to run things past colleagues,” says Kenneth G. Simone, DO, founder and president of Hospitalist and Practice Solutions, Veazie, Maine, and a consultant to hospital medicine groups. “Informal feedback can provide an unbiased and objective perspective, as opposed to [a formal peer review].”
When to Offer Constructive Criticism
In some practices, or for some individuals, sharing constructive criticism with peers is part of the job. “Informal peer discussions should take place every day,” advises Dr. Rohr. “While handoffs pose a risk for losing vital information, they are also an opportunity to consider alternatives for diagnosis and treatment that may benefit patients greatly.”
If this seems like a natural thing to do within your hospital medicine group, follow Dr. Rohr’s advice: “These discussions should be frank but nonjudgmental. If someone has a problem discussing cases in this manner, then the group leader needs to get involved. If a life-threatening error is exposed, then the formal peer review system needs to be activated.”
Providing Peer Feedback
When there is no personal conflict, you may still consider offering constructive criticism if you feel it’s warranted. “I think [peer feedback] is extremely important—if it’s done correctly,” says Dr. Simone. “It provides a safe haven for discussion and can contribute to professional growth.”
According to Dr. Simone, appropriate topics to discuss regarding a colleague’s performance include logistical problems within the practice, such as a doctor who is chronically late for morning rounds; continuity issues, such as a physician who fails to provide detailed information when handing off patients; communication breakdowns, such as forgetting to check out the labs pending on a newly admitted unit-patient with chest pain; behavioral issues, such as a physician who’s verbally abusive to the nurses or disruptive at morning rounds; problems with work ethic, responsiveness, or availability, such as the doctor who never responds to his/her beeper (necessitating a call from nursing to an accommodating provider who’s always willing and available to help); and general team play.
If you believe you need to address one of these topics regarding a colleague’s performance, plan the logistics of the discussion. “This is a conversation best held one on one—in private,” stresses Dr. Simone. “Don’t discuss these issues in front of colleagues, nurses, patients, families … and don’t do it at the end of a long, difficult day.
“Ideally, do it after hours and out of the workplace, though that can be difficult. Remove the person from the hospital floor or the office, and the emotions and adrenaline associated with work,” continues Dr. Simone. “If the environment is stressful, it will raise their defenses, making them more likely to be resistant and argumentative.”
Talking Points
When you offer constructive criticism, approach the topic carefully. “Take a non-confrontational approach,” says Dr. Simone. “Don’t raise your voice, and don’t take the discussion to a personal level. Use objective data as much as possible. Avoid saying ‘I feel that you’re …’ and instead use ‘Coming in 15 minutes late throws everyone’s schedule off.’ ”
Keep the conversation as casual and as light as possible. “This is not a peer review meeting,” Dr. Simone stresses. “Use a soft approach, and you might have greater success. Stay away from power words such as ‘you shouldn’t’ or ‘don’t.’ ”
Some phrases you might use include:
- “I find it helpful if I … ”
- “This has worked for me.”
- “Have you considered … ?”
Even if you use careful wording, don’t be surprised if the other hospitalist doesn’t react well—at least initially. “Unless you’re seasoned at doing this, the individual may get defensive,” warns Dr. Simone. “If you’re consistent throughout the conversation, show support, and are astute enough to break down their defenses, you should be effective.”
Also, keep your cool: “Don’t respond to defensiveness in like [manner],” says Dr. Simone. Throughout the conversation, show your support. “Convey that your intent is to help the individual—not harm them. Ask if you can be of help, and offer to be a resource” to help them improve.
Also remember that your colleague is part of the conversation. “Allow responses,” adds Dr. Simone. “Give them a chance to express themselves.”
End the conversation with an offer to follow up or suggest a next step. “Offer your personal help or suggest a resource such as the employee assistance program,” advises Dr. Simone. “You can check in with them from time to time, but if you have an unwilling party this may be construed as meddlesome. You must consider the personality involved and if you think they’d be amenable to continued conversations.”
Even without a formal follow-up, be sure to voice your approval if you see their negative behavior change. “If you take the time to provide criticism, you should also offer positive feedback if warranted,” says Dr. Simone. “Tell them they’re doing a great job.”
One final piece of advice regarding informal peer feedback: “Avoid writing anything down,” says Dr. Simone. “This may make it discoverable in a court of law, and it’s not your place to put the discussion in writing. If the issue is that serious, take it to the powers that be.” TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the second in a two-part series on providing constructive criticism to your hospitalist peers. Part 1 appeared in the March issue on p. 12.
Have concerns about a colleague’s work performance? Then you have two main options: You can bring it up in a formal peer review (if it’s a clinical issue) or you can approach the individual yourself.
“Medicine is an art and a science. Many problems relate to the art side—communications and relationships, primarily,” says Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Conn. “You may need to talk to a colleague about how they approach family members or how they communicate with patients. In this instance, you’d offer more of a coaching comment.”
While you may hesitate to point out another hospitalist’s problem areas, keep in mind that it is constructive criticism.
“Physicians love to run things past colleagues,” says Kenneth G. Simone, DO, founder and president of Hospitalist and Practice Solutions, Veazie, Maine, and a consultant to hospital medicine groups. “Informal feedback can provide an unbiased and objective perspective, as opposed to [a formal peer review].”
When to Offer Constructive Criticism
In some practices, or for some individuals, sharing constructive criticism with peers is part of the job. “Informal peer discussions should take place every day,” advises Dr. Rohr. “While handoffs pose a risk for losing vital information, they are also an opportunity to consider alternatives for diagnosis and treatment that may benefit patients greatly.”
If this seems like a natural thing to do within your hospital medicine group, follow Dr. Rohr’s advice: “These discussions should be frank but nonjudgmental. If someone has a problem discussing cases in this manner, then the group leader needs to get involved. If a life-threatening error is exposed, then the formal peer review system needs to be activated.”
Providing Peer Feedback
When there is no personal conflict, you may still consider offering constructive criticism if you feel it’s warranted. “I think [peer feedback] is extremely important—if it’s done correctly,” says Dr. Simone. “It provides a safe haven for discussion and can contribute to professional growth.”
According to Dr. Simone, appropriate topics to discuss regarding a colleague’s performance include logistical problems within the practice, such as a doctor who is chronically late for morning rounds; continuity issues, such as a physician who fails to provide detailed information when handing off patients; communication breakdowns, such as forgetting to check out the labs pending on a newly admitted unit-patient with chest pain; behavioral issues, such as a physician who’s verbally abusive to the nurses or disruptive at morning rounds; problems with work ethic, responsiveness, or availability, such as the doctor who never responds to his/her beeper (necessitating a call from nursing to an accommodating provider who’s always willing and available to help); and general team play.
If you believe you need to address one of these topics regarding a colleague’s performance, plan the logistics of the discussion. “This is a conversation best held one on one—in private,” stresses Dr. Simone. “Don’t discuss these issues in front of colleagues, nurses, patients, families … and don’t do it at the end of a long, difficult day.
“Ideally, do it after hours and out of the workplace, though that can be difficult. Remove the person from the hospital floor or the office, and the emotions and adrenaline associated with work,” continues Dr. Simone. “If the environment is stressful, it will raise their defenses, making them more likely to be resistant and argumentative.”
Talking Points
When you offer constructive criticism, approach the topic carefully. “Take a non-confrontational approach,” says Dr. Simone. “Don’t raise your voice, and don’t take the discussion to a personal level. Use objective data as much as possible. Avoid saying ‘I feel that you’re …’ and instead use ‘Coming in 15 minutes late throws everyone’s schedule off.’ ”
Keep the conversation as casual and as light as possible. “This is not a peer review meeting,” Dr. Simone stresses. “Use a soft approach, and you might have greater success. Stay away from power words such as ‘you shouldn’t’ or ‘don’t.’ ”
Some phrases you might use include:
- “I find it helpful if I … ”
- “This has worked for me.”
- “Have you considered … ?”
Even if you use careful wording, don’t be surprised if the other hospitalist doesn’t react well—at least initially. “Unless you’re seasoned at doing this, the individual may get defensive,” warns Dr. Simone. “If you’re consistent throughout the conversation, show support, and are astute enough to break down their defenses, you should be effective.”
Also, keep your cool: “Don’t respond to defensiveness in like [manner],” says Dr. Simone. Throughout the conversation, show your support. “Convey that your intent is to help the individual—not harm them. Ask if you can be of help, and offer to be a resource” to help them improve.
Also remember that your colleague is part of the conversation. “Allow responses,” adds Dr. Simone. “Give them a chance to express themselves.”
End the conversation with an offer to follow up or suggest a next step. “Offer your personal help or suggest a resource such as the employee assistance program,” advises Dr. Simone. “You can check in with them from time to time, but if you have an unwilling party this may be construed as meddlesome. You must consider the personality involved and if you think they’d be amenable to continued conversations.”
Even without a formal follow-up, be sure to voice your approval if you see their negative behavior change. “If you take the time to provide criticism, you should also offer positive feedback if warranted,” says Dr. Simone. “Tell them they’re doing a great job.”
One final piece of advice regarding informal peer feedback: “Avoid writing anything down,” says Dr. Simone. “This may make it discoverable in a court of law, and it’s not your place to put the discussion in writing. If the issue is that serious, take it to the powers that be.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Medicare Prepares to “Pay for Performance”

This year, interested physicians will participate in Medicare’s first ever pay-for-performance program. Legislation passed in late 2006 calls for a voluntary Medicare quality reporting program that financially rewards physicians reporting on specific quality measures. Those physicians may receive a bonus of 1.5% of their total Medicare payments during the reporting period. This adds a pay-for-performance component to the current Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid Services (CMS) established in January 2006.
“Medicare is really serious about improving quality of care for beneficiaries, and they’re committed to pay for performance as the way to go about it,” says Patrick Torcson, MD, MMM, FACP, medical director, Hospital Medicine, St. Tammany Parish Hospital, Covington, La.
Performance Measures in the Works
The pay-for-performance quality reporting program will use the 66 unique clinical measures CMS announced in December 2006, with additional modifications to be made through April 2007 using a consensus process.
“From looking at the proposed list of 66 performance measures, we’ve identified seven that are going to be available to hospitalists to report,” says Dr. Torcson. “The seven involve stroke and [myocardial infarction] care.”
Most of the internal medicine-related measures of the 16 included in the original PVRP were designed for an outpatient, office-based practice, and that seems true of the expanded list as well.
The current 66 measures are slightly more relevant to the hospital setting and can potentially be reported by hospitalists, as Dr. Torcson specified. Specifically, quality measures have been added for giving beta-blockers upon admission (quality measure #29) and for stroke and stroke rehabilitation (quality measures #31-#36).
Other measures are expected to be added before the July implementation date, and some may be reportable by hospitalists. These include creation of an advance care plan (#47) and measures for emergency medicine services (#54-#59).
“Medicare plans to have specific performance measures for each of the 39 specialties that they recognize,” explains Dr. Torcson. “Hospital medicine is not yet a CMS-recognized specialty; we’re typically lumped under general internal medicine.”
You can view all the measures at www.cms.hhs.gov/PVRP/01_overview.asp.
How the Program Will Work
The initial reporting period set by the legislation is July 1 through December 31, 2007, and there will be an enrollment period before that for physicians who wish to participate. When a physician enrolls in the program, she will identify which measures apply to her. At that point, CMS will determine if a measure applies.
If less than three quality measures apply for a physician, then 80% reporting on those applicable measures is required to be eligible for the bonus. If four or more measures apply, the physician must report on at least three in order to be eligible.
Bonuses for voluntary reporting would be in a lump sum and won’t be paid until the first quarter of 2008. The method of payment may be subject to certain limits—and it may not offset the physicians’ administrative costs for reporting. Hospital medicine programs will have to consider whether the costs of reporting are worth the bonus.
SHM Involvement
SHM’s Public Policy Committee (PPC) and its Performance and Standards Task Force (PSTF) have been actively involved in getting measures included on the PRVP list that are applicable to hospitalists.
“SHM is a member of the AMA’s Physician Consortium for Performance Improvement (PCPI) and has representatives on work groups that have developed performance measures and will be revising and maintaining measures over time,” says Dr. Torcson. “We hope to eventually include measures that are specific to hospitalized patients.”
In addition to the PCPI, SHM is represented and has influence in the National Quality Forum and the Ambulatory Care Quality Alliance.
“SHM leadership—CEO Larry Wellikson, Eric Siegal, Public Policy chair, and Lakshmi Halasyamani, chair of the Hospital Quality and Patient Safety (HQPS) Committee—have been proactive in positioning SHM to be very involved in the national quality improvement agenda,” says Dr. Torcson. “It’s really a work in progress, but SHM is part of the work groups that are driving this process.”
The Effect on Hospitalists
As they can with the original PVRP, hospitalists can find a few applicable performance measures to report on, so they are eligible to participate—and SHM encourages them to do so.
“The amount of money will be small and the number of [applicable] measures will be limited and not truly representative of a hospitalist’s practice,” says Dr. Torcson, “but performance reporting should be something that every physician, including hospitalists, has as a skill set as their practice moves into the future.”
Moving Ahead
Details on the new program still need to be clarified by CMS in the first half of 2007. Regardless of the details still to be determined for this first major foray into Medicare pay for performance, one thing is clear: CMS is dedicated to the idea of tying financial reward to quality care. And they aren’t the only ones.
“Medicare is not as far along as private insurers,” says Dr. Torcson. “Commercial insurers are much more aggressive about pursuing physician-level performance and efficiency—I think we’ll see more impactful pay-for-performance plans from them first. However, the CMS model will affect 70 million patients, and commercial insurers have tended to use the CMS model for physician reimbursement.”
Dr. Torcson believes this program is simply a first step on that road. “We’re in the infancy of pay-for-performance models for physician reimbursement,” he says. “I think the ultimate model for physician-level value-based purchasing is going to look a lot different than the proposed CMS payment for reporting and payment for performance.”
In the immediate future, the PPC and PSTF will continue to participate in formulating the final quality measures for the CMS voluntary reporting program. Watch the SHM Web site for updates on the status of the program. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
This year, interested physicians will participate in Medicare’s first ever pay-for-performance program. Legislation passed in late 2006 calls for a voluntary Medicare quality reporting program that financially rewards physicians reporting on specific quality measures. Those physicians may receive a bonus of 1.5% of their total Medicare payments during the reporting period. This adds a pay-for-performance component to the current Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid Services (CMS) established in January 2006.
“Medicare is really serious about improving quality of care for beneficiaries, and they’re committed to pay for performance as the way to go about it,” says Patrick Torcson, MD, MMM, FACP, medical director, Hospital Medicine, St. Tammany Parish Hospital, Covington, La.
Performance Measures in the Works
The pay-for-performance quality reporting program will use the 66 unique clinical measures CMS announced in December 2006, with additional modifications to be made through April 2007 using a consensus process.
“From looking at the proposed list of 66 performance measures, we’ve identified seven that are going to be available to hospitalists to report,” says Dr. Torcson. “The seven involve stroke and [myocardial infarction] care.”
Most of the internal medicine-related measures of the 16 included in the original PVRP were designed for an outpatient, office-based practice, and that seems true of the expanded list as well.
The current 66 measures are slightly more relevant to the hospital setting and can potentially be reported by hospitalists, as Dr. Torcson specified. Specifically, quality measures have been added for giving beta-blockers upon admission (quality measure #29) and for stroke and stroke rehabilitation (quality measures #31-#36).
Other measures are expected to be added before the July implementation date, and some may be reportable by hospitalists. These include creation of an advance care plan (#47) and measures for emergency medicine services (#54-#59).
“Medicare plans to have specific performance measures for each of the 39 specialties that they recognize,” explains Dr. Torcson. “Hospital medicine is not yet a CMS-recognized specialty; we’re typically lumped under general internal medicine.”
You can view all the measures at www.cms.hhs.gov/PVRP/01_overview.asp.
How the Program Will Work
The initial reporting period set by the legislation is July 1 through December 31, 2007, and there will be an enrollment period before that for physicians who wish to participate. When a physician enrolls in the program, she will identify which measures apply to her. At that point, CMS will determine if a measure applies.
If less than three quality measures apply for a physician, then 80% reporting on those applicable measures is required to be eligible for the bonus. If four or more measures apply, the physician must report on at least three in order to be eligible.
Bonuses for voluntary reporting would be in a lump sum and won’t be paid until the first quarter of 2008. The method of payment may be subject to certain limits—and it may not offset the physicians’ administrative costs for reporting. Hospital medicine programs will have to consider whether the costs of reporting are worth the bonus.
SHM Involvement
SHM’s Public Policy Committee (PPC) and its Performance and Standards Task Force (PSTF) have been actively involved in getting measures included on the PRVP list that are applicable to hospitalists.
“SHM is a member of the AMA’s Physician Consortium for Performance Improvement (PCPI) and has representatives on work groups that have developed performance measures and will be revising and maintaining measures over time,” says Dr. Torcson. “We hope to eventually include measures that are specific to hospitalized patients.”
In addition to the PCPI, SHM is represented and has influence in the National Quality Forum and the Ambulatory Care Quality Alliance.
“SHM leadership—CEO Larry Wellikson, Eric Siegal, Public Policy chair, and Lakshmi Halasyamani, chair of the Hospital Quality and Patient Safety (HQPS) Committee—have been proactive in positioning SHM to be very involved in the national quality improvement agenda,” says Dr. Torcson. “It’s really a work in progress, but SHM is part of the work groups that are driving this process.”
The Effect on Hospitalists
As they can with the original PVRP, hospitalists can find a few applicable performance measures to report on, so they are eligible to participate—and SHM encourages them to do so.
“The amount of money will be small and the number of [applicable] measures will be limited and not truly representative of a hospitalist’s practice,” says Dr. Torcson, “but performance reporting should be something that every physician, including hospitalists, has as a skill set as their practice moves into the future.”
Moving Ahead
Details on the new program still need to be clarified by CMS in the first half of 2007. Regardless of the details still to be determined for this first major foray into Medicare pay for performance, one thing is clear: CMS is dedicated to the idea of tying financial reward to quality care. And they aren’t the only ones.
“Medicare is not as far along as private insurers,” says Dr. Torcson. “Commercial insurers are much more aggressive about pursuing physician-level performance and efficiency—I think we’ll see more impactful pay-for-performance plans from them first. However, the CMS model will affect 70 million patients, and commercial insurers have tended to use the CMS model for physician reimbursement.”
Dr. Torcson believes this program is simply a first step on that road. “We’re in the infancy of pay-for-performance models for physician reimbursement,” he says. “I think the ultimate model for physician-level value-based purchasing is going to look a lot different than the proposed CMS payment for reporting and payment for performance.”
In the immediate future, the PPC and PSTF will continue to participate in formulating the final quality measures for the CMS voluntary reporting program. Watch the SHM Web site for updates on the status of the program. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
This year, interested physicians will participate in Medicare’s first ever pay-for-performance program. Legislation passed in late 2006 calls for a voluntary Medicare quality reporting program that financially rewards physicians reporting on specific quality measures. Those physicians may receive a bonus of 1.5% of their total Medicare payments during the reporting period. This adds a pay-for-performance component to the current Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid Services (CMS) established in January 2006.
“Medicare is really serious about improving quality of care for beneficiaries, and they’re committed to pay for performance as the way to go about it,” says Patrick Torcson, MD, MMM, FACP, medical director, Hospital Medicine, St. Tammany Parish Hospital, Covington, La.
Performance Measures in the Works
The pay-for-performance quality reporting program will use the 66 unique clinical measures CMS announced in December 2006, with additional modifications to be made through April 2007 using a consensus process.
“From looking at the proposed list of 66 performance measures, we’ve identified seven that are going to be available to hospitalists to report,” says Dr. Torcson. “The seven involve stroke and [myocardial infarction] care.”
Most of the internal medicine-related measures of the 16 included in the original PVRP were designed for an outpatient, office-based practice, and that seems true of the expanded list as well.
The current 66 measures are slightly more relevant to the hospital setting and can potentially be reported by hospitalists, as Dr. Torcson specified. Specifically, quality measures have been added for giving beta-blockers upon admission (quality measure #29) and for stroke and stroke rehabilitation (quality measures #31-#36).
Other measures are expected to be added before the July implementation date, and some may be reportable by hospitalists. These include creation of an advance care plan (#47) and measures for emergency medicine services (#54-#59).
“Medicare plans to have specific performance measures for each of the 39 specialties that they recognize,” explains Dr. Torcson. “Hospital medicine is not yet a CMS-recognized specialty; we’re typically lumped under general internal medicine.”
You can view all the measures at www.cms.hhs.gov/PVRP/01_overview.asp.
How the Program Will Work
The initial reporting period set by the legislation is July 1 through December 31, 2007, and there will be an enrollment period before that for physicians who wish to participate. When a physician enrolls in the program, she will identify which measures apply to her. At that point, CMS will determine if a measure applies.
If less than three quality measures apply for a physician, then 80% reporting on those applicable measures is required to be eligible for the bonus. If four or more measures apply, the physician must report on at least three in order to be eligible.
Bonuses for voluntary reporting would be in a lump sum and won’t be paid until the first quarter of 2008. The method of payment may be subject to certain limits—and it may not offset the physicians’ administrative costs for reporting. Hospital medicine programs will have to consider whether the costs of reporting are worth the bonus.
SHM Involvement
SHM’s Public Policy Committee (PPC) and its Performance and Standards Task Force (PSTF) have been actively involved in getting measures included on the PRVP list that are applicable to hospitalists.
“SHM is a member of the AMA’s Physician Consortium for Performance Improvement (PCPI) and has representatives on work groups that have developed performance measures and will be revising and maintaining measures over time,” says Dr. Torcson. “We hope to eventually include measures that are specific to hospitalized patients.”
In addition to the PCPI, SHM is represented and has influence in the National Quality Forum and the Ambulatory Care Quality Alliance.
“SHM leadership—CEO Larry Wellikson, Eric Siegal, Public Policy chair, and Lakshmi Halasyamani, chair of the Hospital Quality and Patient Safety (HQPS) Committee—have been proactive in positioning SHM to be very involved in the national quality improvement agenda,” says Dr. Torcson. “It’s really a work in progress, but SHM is part of the work groups that are driving this process.”
The Effect on Hospitalists
As they can with the original PVRP, hospitalists can find a few applicable performance measures to report on, so they are eligible to participate—and SHM encourages them to do so.
“The amount of money will be small and the number of [applicable] measures will be limited and not truly representative of a hospitalist’s practice,” says Dr. Torcson, “but performance reporting should be something that every physician, including hospitalists, has as a skill set as their practice moves into the future.”
Moving Ahead
Details on the new program still need to be clarified by CMS in the first half of 2007. Regardless of the details still to be determined for this first major foray into Medicare pay for performance, one thing is clear: CMS is dedicated to the idea of tying financial reward to quality care. And they aren’t the only ones.
“Medicare is not as far along as private insurers,” says Dr. Torcson. “Commercial insurers are much more aggressive about pursuing physician-level performance and efficiency—I think we’ll see more impactful pay-for-performance plans from them first. However, the CMS model will affect 70 million patients, and commercial insurers have tended to use the CMS model for physician reimbursement.”
Dr. Torcson believes this program is simply a first step on that road. “We’re in the infancy of pay-for-performance models for physician reimbursement,” he says. “I think the ultimate model for physician-level value-based purchasing is going to look a lot different than the proposed CMS payment for reporting and payment for performance.”
In the immediate future, the PPC and PSTF will continue to participate in formulating the final quality measures for the CMS voluntary reporting program. Watch the SHM Web site for updates on the status of the program. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
IT for HM
Disclaimer: This article is not intended to promote a specific company or product. Rather its purpose is to give hospitalists an overview of technological solutions available to them today.
Electronic medical records (EMR). Healthcare information technology legislation. With all the focus on ramping up technology in hospitals, are there any IT solutions specific to hospitalists? It turns out that, yes, there are several technology systems on the market today designed especially for hospital medicine groups and the physicians who work for them.
IT and the Bottom Line
David Delaney, MD, vice president and chief medical officer of technology vendor MedAptus, Inc., Boston, says his company’s most popular solution suite is “charge capture—without a doubt. If you look at it from the perspective of driving meaningful revenue, you can increase collections from $20,000-$30,000 per hospitalist. There’s very little that’s more compelling than saying you’ll get paid more for doing the same amount of work. You can use the increased revenue to pay for other applications or to help fund EMR.”
Other major players in hospital medicine applications agree: Charge capture is the biggest draw for hospital medicine groups interested in purchasing their applications. Delaney says that in hospital medicine, “Market penetration [for electronic charge capture] is small but accelerating rapidly. I’d say only about 20% of the market is using true charge capture applications.”
One of the groups within that 20% is Inpatient Management Medical Group (IMMG), Novato, Calif. Arieh Rosenbaum, MD, director of hospitalists for IMMG’s Davies Campus, convinced the group to purchase a solution suite from one of the major vendors covered in this article, arguing that the technology would improve revenues and help the group collect their own data.
“Our first purchase was the billing program,” says Dr. Rosenbaum. “This was a huge change for us; we went from physicians basically carrying pieces of paper around in our pockets to a fully electronic billing system. It definitely helped our revenue; we’ve vastly improved our ability to capture charges.”
Jeffrey D. Kin, MD, of the Fredericksburg (Va.) Hospitalist Group, agrees. His practice purchased a different charge capture product than IMMG but experienced the same results: “There are fewer errors, and our collections are going up,” he says. “There are a lot of upsides to having a computerized system. Last year we copied 80,000 pieces of paper. Not all of that was billing slips, but a lot was.”
Both groups are relatively new customers, and both plan to begin mining the data in their new systems. “We don’t want to rely on the data provided by the hospital,” says Dr. Rosenbaum. “With the information in the system, we can look at diagnoses, length of stay, all sorts of things. This can provide a way for us to prove our value to the hospital.”
Eventually, Dr. Rosenbaum would like to merge core measures into the charge capture process so hospitalists can ensure they are following best practices as they work. “It’s a way to improve ourselves,” he says.
Help for the Working Hospitalist
But there is much more out there besides financial tools. The four leading technology product suites examined for this article offer time-saving and efficiency-boosting utilities geared toward the working hospitalist, including the ability to call up lab results for patients, e-prescribing, integrated communication with colleagues and primary care physicians (PCPs), and much more.
“Our rounding program is helping patient care,” says Dr. Rosenbaum. “It’s the only way we round on my campus now. It’s pretty useful; the simplicity is what sold me on it, and it works concurrently with the billing [software].”
The Fredericksburg Hospitalist Group relies on communications software to alert primary care physicians when their patients are admitted and discharged. “Most [community] physicians have access to the hospital’s computer system,” explains Dr. Kin. “By our alerting them that their patient has been admitted, they can access labs, our dictations—pretty much everything. The idea is that with automatic notification, we give them a heads-up; this is a real help to us.”
Here is an overview of IT solutions that include hospitalist-specific features to spark your imagination on how technology might change your day-to-day job—and probably will.
David J. Brailer, MD, Ph, national coordinator for health information technology at the Department of Health and Human Services, will be a keynote speaker at this year’s Annual Meeting in Dallas at the Gaylord Texan Resort. Dr. Brailer is a recognized leader in the strategy and financing of quality and efficiency in healthcare. He focuses on health information technology and health systems management.
For more information on his address at the Annual Meeting, visit www.hospitalmedicine.org and click the “Events” tab on the left-hand menu.
Hospital Management System (HMS) (BMA Enterprises, Inc.)
A Web-based charge capture and primacy care physician communication system designed specifically for hospitalists, “HMS is a single product with various configuration options,” explains Dennis C. Wiltshire, president.
The charge capture software includes warning messages that alert the user to duplicate charges or missed charges. “An obvious problem with hospitalists is the way their shifts work; one rolls off the shift and another takes over the patient load,” says Wiltshire. “Each physician who sees a patient will see the patient roster with warnings, etc. For example, if, on Tuesday, Dr. Johnson admits the patient and enters the charges, and Dr. Wilson sees the same patient on Thursday and enters his charges, the missed day of service shows up. You then have to check and see what happened on Wednesday.”
As with their competitors’ charge capture programs, billing logic is used to minimize lost charges, and billing files can be created electronically.
Part of HMS’ charge capture package is a feature that allows the customer to create a “favorite list” of ICD9s and CPT codes. “The group administrator informs us of their most frequently used codes,” explains Wiltshire. Those codes are added to the favorites list. “The favorites are group-wide.”
HMS also offers a solution for built-in communication with PCPs upon their patients’ admission and discharge, along with a unique follow-up system for discharged patients.
“As soon as an admission or discharge code is entered, you’ll see a screen for additional comments,” explains Wiltshire. “The PCP information is already in the system—it’s entered upon admission—and the program generates a fax at our site. The fax is sent with customized, pertinent information.”
Why fax? “There’s an issue with e-mail: It’s not secure,” says Wiltshire. “And most PCPs are familiar and comfortable with getting faxes.”
As for follow-up after discharge, says Wiltshire, “It’s a tickler system. Upon discharge, the physician can elect whether to create a follow-up system. It might be a reminder to check the patient’s X-rays or lab results or that an appointment was made with their PCP. You can select these options to create a to-do list, and the patient won’t leave the patient roster until the list is completed.”
Whatever follow-up steps are taken can then be permanently documented and, if appropriate, faxed to the PCP to show completion.
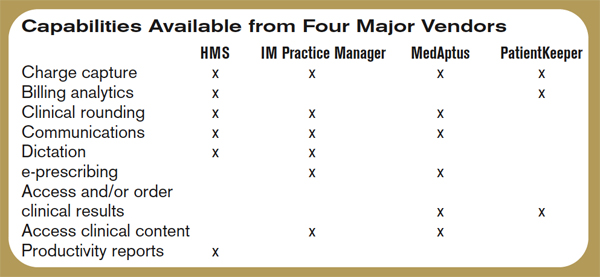
IM Practice Manager 1.0 (Ingenious Med, Inc.)
This overall system includes clinical rounding, charge capture, communication, and business intelligence suites. Ingenious Med can aggregate data across multiple facilities, integrating with hospital EMR, information, and billing systems, enabling real-time management reports, allowing physicians to enter and access data via the Internet or mobile devices, and promoting rapid dissemination of critical information across hospital and national physician networks.
“Customers typically start off with our basic product, which is comprehensive. As the practice matures, that’s where we get customers asking for other modules,” says Steven Liu, MD, founder, CEO, chief architect, and a practicing hospitalist at Emory Eastside Medical Center, Snellville, Ga. “Our suite of products is within Practice Manager. It’s designed primarily for physician practices, which is a little different than those designed for a hospital.”
As the name implies IM Practice Manager includes tools for the practice. “As the hospitalist movement has become a bigger player, hospitalists need to prove their value,” says Dr. Liu. “We provide tools for data-mining performance. These are modeled a lot on SHM and what they state as best requirements, as well as what the individual [hospital medicine practice] requires.”
Dr. Liu stresses that they only include the features that hospitalists really need to do their jobs: “This software is designed by physicians; we don’t do technology for technology’s sake.”
IM Practice Manager offers tools for both the administrators and the hospitalists in a given group. “On the business end, business intelligence is a very important part of any practice,” says Dr. Liu. “We’ve put a lot of resources into creating a comprehensive system. Other utilities are more geared to individual physicians.”
Those utilities include communications: “You can send e-mails as long as they’re within the practice,” says Dr. Liu. “This is secure and controllable. But the system is built to help hospital medicine groups to communicate with everyone they encounter—staff, the back office, patients, and other providers.”
MedAptus Point-of-Care Solution Suite (MedAptus, Inc.)
As with its competitors, MedAptus points to the improved coding compliance, decreased administrative burden, and greatly enhanced reimbursement that result from their electronic charge capture suite.
“We send out compliance or maintenance releases annually, and a real-time call goes out over the Web when new rules are issued,” explains Dr. Delaney. The result is an automatic update for users. “It all happens behind the scenes.”
Other software features target physicians’ daily activities. “The crucial thing is to get it right from the hospitalist’s perspective,” says Dr. Delaney. “Hospital medicine differs a lot [from other physician specialties]. It tends to practices sharing groups of patients, so we have rounding lists of patients built in. Your colleague can pull up a team of patients to see changes and updates to care.”
On dictation, a feature that not all systems offer, Dr. Delaney explains, “If they’re dictating today, this is a tremendous help. It’s seamlessly integrated into the system. However, if they’re currently writing notes, this is a convenient feature, but it’s also a new expense and can add to turnaround time.”
Another feature of MedAptus—one that is unique to its product—is the Clinical Content application, which connects the user to current medical knowledge in books and publications—pre-selected by the customer group—at any point in patient interaction. “We’re very excited about this,” says Dr. Delaney. “It allows just-in-time information on specific clinical questions. It takes you to the exact information you need at any point in the process.”
The overall solution from MedAptus also includes the ability to receive lab and radiology results, as well as clinical notes, electronically at any time, anywhere. “We help leverage and extend existing IT assets in a mobile form factor,” summarizes Dr. Delaney. “We’re on version seven; we’ve had the opportunity to figure out how to fit in with a physician’s work flow.”
PatientKeeper (PatientKeeper, Inc.)
The most established software for hospitalists, PatientKeeper is a single integrated system designed to support a physician throughout the entire day. At any time, from any location, physicians can access their patients’ electronic records, write prescriptions, enter charges, dictate notes, document encounters, place orders, or send secure messages to other caregivers.
Stephen S. Hau, founder and vice president, marketing and business development, agrees that charge capture is the most requested utility. “This is a huge financial advantage for an institution, plus it increases physician satisfaction,” he says. “In three taps, you can capture a charge, and there are 900 rules [in the software] that help ensure the charge is correct and a clean bill is entered.”
But getting back to the daily tasks of hospitalists, “Our whole take is trying to fill the void where institutions have purchased information systems but there’s nothing to support the physician,” says Hau.
For example, Hau says, “One of the tasks that eats up a lot of time is finding information—the ‘chart chase,’ along with communicating with other providers. We help make it easier to send information to each other. You can send a patient-specific instant message, saying, ‘waiting on lab results for patient Molly Doe.’ Now more providers are in play per patient, so communication is more important.”
This improves patient care and even quality of life for working hospitalists. “One physician said he used to get calls at home about discharges,” recalls Hau. “Now he can access the information and discharge a patient over the phone if it’s appropriate. That shortens length of stay.”
PatientKeeper also allows individual users to customize the utility. “The exciting, challenging thing about [designing software for] physicians is that one size does not fit all,” says Hau. “One thing we provide is the ability to easily manage your own patient list; you can organize it by your schedule or by location or rounding path. We call features like that ‘physician delighters.’ These are what has made us so successful.”
Perhaps because of the physician delighters, or perhaps because they’ve been around the longest, PatientKeeper is currently the most widely used technology solution in hospital medicine. “We’re in 350 hospitals across the country, so I guess we’re the market leader,” says Hau. “We just announced two new patents, so we believe we’re also the technology leaders.”
Conclusion
Programs like the ones outlined here are definitely the future of healthcare, but the first step might be the most painful. “The investment is sizeable,” warns Dr. Rosenbaum. “The main problem is that it’s expensive. You need an upfront investment with no real guarantee of the returns.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Disclaimer: This article is not intended to promote a specific company or product. Rather its purpose is to give hospitalists an overview of technological solutions available to them today.
Electronic medical records (EMR). Healthcare information technology legislation. With all the focus on ramping up technology in hospitals, are there any IT solutions specific to hospitalists? It turns out that, yes, there are several technology systems on the market today designed especially for hospital medicine groups and the physicians who work for them.
IT and the Bottom Line
David Delaney, MD, vice president and chief medical officer of technology vendor MedAptus, Inc., Boston, says his company’s most popular solution suite is “charge capture—without a doubt. If you look at it from the perspective of driving meaningful revenue, you can increase collections from $20,000-$30,000 per hospitalist. There’s very little that’s more compelling than saying you’ll get paid more for doing the same amount of work. You can use the increased revenue to pay for other applications or to help fund EMR.”
Other major players in hospital medicine applications agree: Charge capture is the biggest draw for hospital medicine groups interested in purchasing their applications. Delaney says that in hospital medicine, “Market penetration [for electronic charge capture] is small but accelerating rapidly. I’d say only about 20% of the market is using true charge capture applications.”
One of the groups within that 20% is Inpatient Management Medical Group (IMMG), Novato, Calif. Arieh Rosenbaum, MD, director of hospitalists for IMMG’s Davies Campus, convinced the group to purchase a solution suite from one of the major vendors covered in this article, arguing that the technology would improve revenues and help the group collect their own data.
“Our first purchase was the billing program,” says Dr. Rosenbaum. “This was a huge change for us; we went from physicians basically carrying pieces of paper around in our pockets to a fully electronic billing system. It definitely helped our revenue; we’ve vastly improved our ability to capture charges.”
Jeffrey D. Kin, MD, of the Fredericksburg (Va.) Hospitalist Group, agrees. His practice purchased a different charge capture product than IMMG but experienced the same results: “There are fewer errors, and our collections are going up,” he says. “There are a lot of upsides to having a computerized system. Last year we copied 80,000 pieces of paper. Not all of that was billing slips, but a lot was.”
Both groups are relatively new customers, and both plan to begin mining the data in their new systems. “We don’t want to rely on the data provided by the hospital,” says Dr. Rosenbaum. “With the information in the system, we can look at diagnoses, length of stay, all sorts of things. This can provide a way for us to prove our value to the hospital.”
Eventually, Dr. Rosenbaum would like to merge core measures into the charge capture process so hospitalists can ensure they are following best practices as they work. “It’s a way to improve ourselves,” he says.
Help for the Working Hospitalist
But there is much more out there besides financial tools. The four leading technology product suites examined for this article offer time-saving and efficiency-boosting utilities geared toward the working hospitalist, including the ability to call up lab results for patients, e-prescribing, integrated communication with colleagues and primary care physicians (PCPs), and much more.
“Our rounding program is helping patient care,” says Dr. Rosenbaum. “It’s the only way we round on my campus now. It’s pretty useful; the simplicity is what sold me on it, and it works concurrently with the billing [software].”
The Fredericksburg Hospitalist Group relies on communications software to alert primary care physicians when their patients are admitted and discharged. “Most [community] physicians have access to the hospital’s computer system,” explains Dr. Kin. “By our alerting them that their patient has been admitted, they can access labs, our dictations—pretty much everything. The idea is that with automatic notification, we give them a heads-up; this is a real help to us.”
Here is an overview of IT solutions that include hospitalist-specific features to spark your imagination on how technology might change your day-to-day job—and probably will.
David J. Brailer, MD, Ph, national coordinator for health information technology at the Department of Health and Human Services, will be a keynote speaker at this year’s Annual Meeting in Dallas at the Gaylord Texan Resort. Dr. Brailer is a recognized leader in the strategy and financing of quality and efficiency in healthcare. He focuses on health information technology and health systems management.
For more information on his address at the Annual Meeting, visit www.hospitalmedicine.org and click the “Events” tab on the left-hand menu.
Hospital Management System (HMS) (BMA Enterprises, Inc.)
A Web-based charge capture and primacy care physician communication system designed specifically for hospitalists, “HMS is a single product with various configuration options,” explains Dennis C. Wiltshire, president.
The charge capture software includes warning messages that alert the user to duplicate charges or missed charges. “An obvious problem with hospitalists is the way their shifts work; one rolls off the shift and another takes over the patient load,” says Wiltshire. “Each physician who sees a patient will see the patient roster with warnings, etc. For example, if, on Tuesday, Dr. Johnson admits the patient and enters the charges, and Dr. Wilson sees the same patient on Thursday and enters his charges, the missed day of service shows up. You then have to check and see what happened on Wednesday.”
As with their competitors’ charge capture programs, billing logic is used to minimize lost charges, and billing files can be created electronically.
Part of HMS’ charge capture package is a feature that allows the customer to create a “favorite list” of ICD9s and CPT codes. “The group administrator informs us of their most frequently used codes,” explains Wiltshire. Those codes are added to the favorites list. “The favorites are group-wide.”
HMS also offers a solution for built-in communication with PCPs upon their patients’ admission and discharge, along with a unique follow-up system for discharged patients.
“As soon as an admission or discharge code is entered, you’ll see a screen for additional comments,” explains Wiltshire. “The PCP information is already in the system—it’s entered upon admission—and the program generates a fax at our site. The fax is sent with customized, pertinent information.”
Why fax? “There’s an issue with e-mail: It’s not secure,” says Wiltshire. “And most PCPs are familiar and comfortable with getting faxes.”
As for follow-up after discharge, says Wiltshire, “It’s a tickler system. Upon discharge, the physician can elect whether to create a follow-up system. It might be a reminder to check the patient’s X-rays or lab results or that an appointment was made with their PCP. You can select these options to create a to-do list, and the patient won’t leave the patient roster until the list is completed.”
Whatever follow-up steps are taken can then be permanently documented and, if appropriate, faxed to the PCP to show completion.
IM Practice Manager 1.0 (Ingenious Med, Inc.)
This overall system includes clinical rounding, charge capture, communication, and business intelligence suites. Ingenious Med can aggregate data across multiple facilities, integrating with hospital EMR, information, and billing systems, enabling real-time management reports, allowing physicians to enter and access data via the Internet or mobile devices, and promoting rapid dissemination of critical information across hospital and national physician networks.
“Customers typically start off with our basic product, which is comprehensive. As the practice matures, that’s where we get customers asking for other modules,” says Steven Liu, MD, founder, CEO, chief architect, and a practicing hospitalist at Emory Eastside Medical Center, Snellville, Ga. “Our suite of products is within Practice Manager. It’s designed primarily for physician practices, which is a little different than those designed for a hospital.”
As the name implies IM Practice Manager includes tools for the practice. “As the hospitalist movement has become a bigger player, hospitalists need to prove their value,” says Dr. Liu. “We provide tools for data-mining performance. These are modeled a lot on SHM and what they state as best requirements, as well as what the individual [hospital medicine practice] requires.”
Dr. Liu stresses that they only include the features that hospitalists really need to do their jobs: “This software is designed by physicians; we don’t do technology for technology’s sake.”
IM Practice Manager offers tools for both the administrators and the hospitalists in a given group. “On the business end, business intelligence is a very important part of any practice,” says Dr. Liu. “We’ve put a lot of resources into creating a comprehensive system. Other utilities are more geared to individual physicians.”
Those utilities include communications: “You can send e-mails as long as they’re within the practice,” says Dr. Liu. “This is secure and controllable. But the system is built to help hospital medicine groups to communicate with everyone they encounter—staff, the back office, patients, and other providers.”
MedAptus Point-of-Care Solution Suite (MedAptus, Inc.)
As with its competitors, MedAptus points to the improved coding compliance, decreased administrative burden, and greatly enhanced reimbursement that result from their electronic charge capture suite.
“We send out compliance or maintenance releases annually, and a real-time call goes out over the Web when new rules are issued,” explains Dr. Delaney. The result is an automatic update for users. “It all happens behind the scenes.”
Other software features target physicians’ daily activities. “The crucial thing is to get it right from the hospitalist’s perspective,” says Dr. Delaney. “Hospital medicine differs a lot [from other physician specialties]. It tends to practices sharing groups of patients, so we have rounding lists of patients built in. Your colleague can pull up a team of patients to see changes and updates to care.”
On dictation, a feature that not all systems offer, Dr. Delaney explains, “If they’re dictating today, this is a tremendous help. It’s seamlessly integrated into the system. However, if they’re currently writing notes, this is a convenient feature, but it’s also a new expense and can add to turnaround time.”
Another feature of MedAptus—one that is unique to its product—is the Clinical Content application, which connects the user to current medical knowledge in books and publications—pre-selected by the customer group—at any point in patient interaction. “We’re very excited about this,” says Dr. Delaney. “It allows just-in-time information on specific clinical questions. It takes you to the exact information you need at any point in the process.”
The overall solution from MedAptus also includes the ability to receive lab and radiology results, as well as clinical notes, electronically at any time, anywhere. “We help leverage and extend existing IT assets in a mobile form factor,” summarizes Dr. Delaney. “We’re on version seven; we’ve had the opportunity to figure out how to fit in with a physician’s work flow.”
PatientKeeper (PatientKeeper, Inc.)
The most established software for hospitalists, PatientKeeper is a single integrated system designed to support a physician throughout the entire day. At any time, from any location, physicians can access their patients’ electronic records, write prescriptions, enter charges, dictate notes, document encounters, place orders, or send secure messages to other caregivers.
Stephen S. Hau, founder and vice president, marketing and business development, agrees that charge capture is the most requested utility. “This is a huge financial advantage for an institution, plus it increases physician satisfaction,” he says. “In three taps, you can capture a charge, and there are 900 rules [in the software] that help ensure the charge is correct and a clean bill is entered.”
But getting back to the daily tasks of hospitalists, “Our whole take is trying to fill the void where institutions have purchased information systems but there’s nothing to support the physician,” says Hau.
For example, Hau says, “One of the tasks that eats up a lot of time is finding information—the ‘chart chase,’ along with communicating with other providers. We help make it easier to send information to each other. You can send a patient-specific instant message, saying, ‘waiting on lab results for patient Molly Doe.’ Now more providers are in play per patient, so communication is more important.”
This improves patient care and even quality of life for working hospitalists. “One physician said he used to get calls at home about discharges,” recalls Hau. “Now he can access the information and discharge a patient over the phone if it’s appropriate. That shortens length of stay.”
PatientKeeper also allows individual users to customize the utility. “The exciting, challenging thing about [designing software for] physicians is that one size does not fit all,” says Hau. “One thing we provide is the ability to easily manage your own patient list; you can organize it by your schedule or by location or rounding path. We call features like that ‘physician delighters.’ These are what has made us so successful.”
Perhaps because of the physician delighters, or perhaps because they’ve been around the longest, PatientKeeper is currently the most widely used technology solution in hospital medicine. “We’re in 350 hospitals across the country, so I guess we’re the market leader,” says Hau. “We just announced two new patents, so we believe we’re also the technology leaders.”
Conclusion
Programs like the ones outlined here are definitely the future of healthcare, but the first step might be the most painful. “The investment is sizeable,” warns Dr. Rosenbaum. “The main problem is that it’s expensive. You need an upfront investment with no real guarantee of the returns.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Disclaimer: This article is not intended to promote a specific company or product. Rather its purpose is to give hospitalists an overview of technological solutions available to them today.
Electronic medical records (EMR). Healthcare information technology legislation. With all the focus on ramping up technology in hospitals, are there any IT solutions specific to hospitalists? It turns out that, yes, there are several technology systems on the market today designed especially for hospital medicine groups and the physicians who work for them.
IT and the Bottom Line
David Delaney, MD, vice president and chief medical officer of technology vendor MedAptus, Inc., Boston, says his company’s most popular solution suite is “charge capture—without a doubt. If you look at it from the perspective of driving meaningful revenue, you can increase collections from $20,000-$30,000 per hospitalist. There’s very little that’s more compelling than saying you’ll get paid more for doing the same amount of work. You can use the increased revenue to pay for other applications or to help fund EMR.”
Other major players in hospital medicine applications agree: Charge capture is the biggest draw for hospital medicine groups interested in purchasing their applications. Delaney says that in hospital medicine, “Market penetration [for electronic charge capture] is small but accelerating rapidly. I’d say only about 20% of the market is using true charge capture applications.”
One of the groups within that 20% is Inpatient Management Medical Group (IMMG), Novato, Calif. Arieh Rosenbaum, MD, director of hospitalists for IMMG’s Davies Campus, convinced the group to purchase a solution suite from one of the major vendors covered in this article, arguing that the technology would improve revenues and help the group collect their own data.
“Our first purchase was the billing program,” says Dr. Rosenbaum. “This was a huge change for us; we went from physicians basically carrying pieces of paper around in our pockets to a fully electronic billing system. It definitely helped our revenue; we’ve vastly improved our ability to capture charges.”
Jeffrey D. Kin, MD, of the Fredericksburg (Va.) Hospitalist Group, agrees. His practice purchased a different charge capture product than IMMG but experienced the same results: “There are fewer errors, and our collections are going up,” he says. “There are a lot of upsides to having a computerized system. Last year we copied 80,000 pieces of paper. Not all of that was billing slips, but a lot was.”
Both groups are relatively new customers, and both plan to begin mining the data in their new systems. “We don’t want to rely on the data provided by the hospital,” says Dr. Rosenbaum. “With the information in the system, we can look at diagnoses, length of stay, all sorts of things. This can provide a way for us to prove our value to the hospital.”
Eventually, Dr. Rosenbaum would like to merge core measures into the charge capture process so hospitalists can ensure they are following best practices as they work. “It’s a way to improve ourselves,” he says.
Help for the Working Hospitalist
But there is much more out there besides financial tools. The four leading technology product suites examined for this article offer time-saving and efficiency-boosting utilities geared toward the working hospitalist, including the ability to call up lab results for patients, e-prescribing, integrated communication with colleagues and primary care physicians (PCPs), and much more.
“Our rounding program is helping patient care,” says Dr. Rosenbaum. “It’s the only way we round on my campus now. It’s pretty useful; the simplicity is what sold me on it, and it works concurrently with the billing [software].”
The Fredericksburg Hospitalist Group relies on communications software to alert primary care physicians when their patients are admitted and discharged. “Most [community] physicians have access to the hospital’s computer system,” explains Dr. Kin. “By our alerting them that their patient has been admitted, they can access labs, our dictations—pretty much everything. The idea is that with automatic notification, we give them a heads-up; this is a real help to us.”
Here is an overview of IT solutions that include hospitalist-specific features to spark your imagination on how technology might change your day-to-day job—and probably will.
David J. Brailer, MD, Ph, national coordinator for health information technology at the Department of Health and Human Services, will be a keynote speaker at this year’s Annual Meeting in Dallas at the Gaylord Texan Resort. Dr. Brailer is a recognized leader in the strategy and financing of quality and efficiency in healthcare. He focuses on health information technology and health systems management.
For more information on his address at the Annual Meeting, visit www.hospitalmedicine.org and click the “Events” tab on the left-hand menu.
Hospital Management System (HMS) (BMA Enterprises, Inc.)
A Web-based charge capture and primacy care physician communication system designed specifically for hospitalists, “HMS is a single product with various configuration options,” explains Dennis C. Wiltshire, president.
The charge capture software includes warning messages that alert the user to duplicate charges or missed charges. “An obvious problem with hospitalists is the way their shifts work; one rolls off the shift and another takes over the patient load,” says Wiltshire. “Each physician who sees a patient will see the patient roster with warnings, etc. For example, if, on Tuesday, Dr. Johnson admits the patient and enters the charges, and Dr. Wilson sees the same patient on Thursday and enters his charges, the missed day of service shows up. You then have to check and see what happened on Wednesday.”
As with their competitors’ charge capture programs, billing logic is used to minimize lost charges, and billing files can be created electronically.
Part of HMS’ charge capture package is a feature that allows the customer to create a “favorite list” of ICD9s and CPT codes. “The group administrator informs us of their most frequently used codes,” explains Wiltshire. Those codes are added to the favorites list. “The favorites are group-wide.”
HMS also offers a solution for built-in communication with PCPs upon their patients’ admission and discharge, along with a unique follow-up system for discharged patients.
“As soon as an admission or discharge code is entered, you’ll see a screen for additional comments,” explains Wiltshire. “The PCP information is already in the system—it’s entered upon admission—and the program generates a fax at our site. The fax is sent with customized, pertinent information.”
Why fax? “There’s an issue with e-mail: It’s not secure,” says Wiltshire. “And most PCPs are familiar and comfortable with getting faxes.”
As for follow-up after discharge, says Wiltshire, “It’s a tickler system. Upon discharge, the physician can elect whether to create a follow-up system. It might be a reminder to check the patient’s X-rays or lab results or that an appointment was made with their PCP. You can select these options to create a to-do list, and the patient won’t leave the patient roster until the list is completed.”
Whatever follow-up steps are taken can then be permanently documented and, if appropriate, faxed to the PCP to show completion.
IM Practice Manager 1.0 (Ingenious Med, Inc.)
This overall system includes clinical rounding, charge capture, communication, and business intelligence suites. Ingenious Med can aggregate data across multiple facilities, integrating with hospital EMR, information, and billing systems, enabling real-time management reports, allowing physicians to enter and access data via the Internet or mobile devices, and promoting rapid dissemination of critical information across hospital and national physician networks.
“Customers typically start off with our basic product, which is comprehensive. As the practice matures, that’s where we get customers asking for other modules,” says Steven Liu, MD, founder, CEO, chief architect, and a practicing hospitalist at Emory Eastside Medical Center, Snellville, Ga. “Our suite of products is within Practice Manager. It’s designed primarily for physician practices, which is a little different than those designed for a hospital.”
As the name implies IM Practice Manager includes tools for the practice. “As the hospitalist movement has become a bigger player, hospitalists need to prove their value,” says Dr. Liu. “We provide tools for data-mining performance. These are modeled a lot on SHM and what they state as best requirements, as well as what the individual [hospital medicine practice] requires.”
Dr. Liu stresses that they only include the features that hospitalists really need to do their jobs: “This software is designed by physicians; we don’t do technology for technology’s sake.”
IM Practice Manager offers tools for both the administrators and the hospitalists in a given group. “On the business end, business intelligence is a very important part of any practice,” says Dr. Liu. “We’ve put a lot of resources into creating a comprehensive system. Other utilities are more geared to individual physicians.”
Those utilities include communications: “You can send e-mails as long as they’re within the practice,” says Dr. Liu. “This is secure and controllable. But the system is built to help hospital medicine groups to communicate with everyone they encounter—staff, the back office, patients, and other providers.”
MedAptus Point-of-Care Solution Suite (MedAptus, Inc.)
As with its competitors, MedAptus points to the improved coding compliance, decreased administrative burden, and greatly enhanced reimbursement that result from their electronic charge capture suite.
“We send out compliance or maintenance releases annually, and a real-time call goes out over the Web when new rules are issued,” explains Dr. Delaney. The result is an automatic update for users. “It all happens behind the scenes.”
Other software features target physicians’ daily activities. “The crucial thing is to get it right from the hospitalist’s perspective,” says Dr. Delaney. “Hospital medicine differs a lot [from other physician specialties]. It tends to practices sharing groups of patients, so we have rounding lists of patients built in. Your colleague can pull up a team of patients to see changes and updates to care.”
On dictation, a feature that not all systems offer, Dr. Delaney explains, “If they’re dictating today, this is a tremendous help. It’s seamlessly integrated into the system. However, if they’re currently writing notes, this is a convenient feature, but it’s also a new expense and can add to turnaround time.”
Another feature of MedAptus—one that is unique to its product—is the Clinical Content application, which connects the user to current medical knowledge in books and publications—pre-selected by the customer group—at any point in patient interaction. “We’re very excited about this,” says Dr. Delaney. “It allows just-in-time information on specific clinical questions. It takes you to the exact information you need at any point in the process.”
The overall solution from MedAptus also includes the ability to receive lab and radiology results, as well as clinical notes, electronically at any time, anywhere. “We help leverage and extend existing IT assets in a mobile form factor,” summarizes Dr. Delaney. “We’re on version seven; we’ve had the opportunity to figure out how to fit in with a physician’s work flow.”
PatientKeeper (PatientKeeper, Inc.)
The most established software for hospitalists, PatientKeeper is a single integrated system designed to support a physician throughout the entire day. At any time, from any location, physicians can access their patients’ electronic records, write prescriptions, enter charges, dictate notes, document encounters, place orders, or send secure messages to other caregivers.
Stephen S. Hau, founder and vice president, marketing and business development, agrees that charge capture is the most requested utility. “This is a huge financial advantage for an institution, plus it increases physician satisfaction,” he says. “In three taps, you can capture a charge, and there are 900 rules [in the software] that help ensure the charge is correct and a clean bill is entered.”
But getting back to the daily tasks of hospitalists, “Our whole take is trying to fill the void where institutions have purchased information systems but there’s nothing to support the physician,” says Hau.
For example, Hau says, “One of the tasks that eats up a lot of time is finding information—the ‘chart chase,’ along with communicating with other providers. We help make it easier to send information to each other. You can send a patient-specific instant message, saying, ‘waiting on lab results for patient Molly Doe.’ Now more providers are in play per patient, so communication is more important.”
This improves patient care and even quality of life for working hospitalists. “One physician said he used to get calls at home about discharges,” recalls Hau. “Now he can access the information and discharge a patient over the phone if it’s appropriate. That shortens length of stay.”
PatientKeeper also allows individual users to customize the utility. “The exciting, challenging thing about [designing software for] physicians is that one size does not fit all,” says Hau. “One thing we provide is the ability to easily manage your own patient list; you can organize it by your schedule or by location or rounding path. We call features like that ‘physician delighters.’ These are what has made us so successful.”
Perhaps because of the physician delighters, or perhaps because they’ve been around the longest, PatientKeeper is currently the most widely used technology solution in hospital medicine. “We’re in 350 hospitals across the country, so I guess we’re the market leader,” says Hau. “We just announced two new patents, so we believe we’re also the technology leaders.”
Conclusion
Programs like the ones outlined here are definitely the future of healthcare, but the first step might be the most painful. “The investment is sizeable,” warns Dr. Rosenbaum. “The main problem is that it’s expensive. You need an upfront investment with no real guarantee of the returns.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Big Kahunas
Disclaimer: SHM Members William Atchley, MD, FACP, Ron Greeno, MD, Stacy Goldsholl, MD, and Mark V. Williams, MD, FACP, are quoted in this article. Their opinions do not reflect or represent the opinions of SHM.
Hospital medicine may be a young field, but several major providers have already been established. Each of these rapidly growing organizations employs dozens—or even hundreds—of hospitalists and is establishing or revamping hospital medicine programs across the United States.
As these organizations grow, they are shaping hospital medicine. “I think that what the large companies really bring to the table is a vision of what hospital medicine is supposed to be about: evidence-based medicine and other things important to the hospital,” says William Atchley, MD, FACP, a practicing hospitalist in Hampton, Va.
This month, we examine just a few of the many large hospital medicine groups in order to set the stage for this growing trend and the issues presented by these groups. That said, here is an overview of some of the largest national players in hospital medicine, their perspective on the industry, their philosophies, and dialogue about their astonishing growth.
The Players
Which organizations have become the nation’s largest employers of hospitalists?
Cogent Healthcare
Based in Irvine, Calif., Cogent employs approximately 130 full-time hospitalists, with an additional 70 who “work with us in other arrangements; some are partnered with us,” says Ron Greeno, MD, FCCP, Cogent chief medical officer.
Cogent was founded by four physician groups in Los Angeles County. “We started in late 1997 and spent the first several years developing the model,” recalls Dr. Greeno. “In the 2000s, we started building programs for hospitals. We’ve seen growth of around 40% a year for the last several years. Frankly, we started too early; the market wasn’t really ready.”
What sets Cogent apart, says Dr. Greeno, is its focus. “We’re not a physician practice management company,” he stresses. “Our competitors’ goal is to build large, successful practices. We built a practice that’s hospital-centric. This helps the hospital satisfy its goals.”
EmCare
Perhaps the first of the national players to actively undertake hospital medicine, EmCare developed its first hospitalist program in 1993 at Baylor University Medical Center (BUMC) in Texas. “[Baylor is] still with us,” says Michael Wagner, MD, CEO, Hospitalists Division, EmCare.
EmCare has more than 30 years of experience with emergency department (ED) staffing, which is how it got its foot in the hospitalist door.
“In the late ’90s, other hospital EDs talked to us” about bringing in a hospitalist program, says Dr. Wagner. “So in each ED region, we worked to sell [the] hospital medicine program. It didn’t really take off until the 2000s, when non-clients started approaching us.”
Today, EmCare employs 350 hospitalists, 240 of whom work full-time. They provide hospital medicine to 47 clients in 60 programs in 37 states.
Emory Healthcare
Emory Healthcare’s Hospital Medicine Unit in Atlanta is the largest academic hospital medicine program in the United States.
“We occupy five hospitals,” says Mark V. Williams, MD, FACP, director of Emory’s Hospital Medicine Unit and editor of the Journal of Hospital Medicine. “Thirty of our hospitalists teach at the two university hospitals, and an additional eight teach at [one of three] community hospital[s]. Others will teach in-service training as well.”
The two university hospitals—Emory University Hospital and Crawford Long Hospital—are “solely staffed by Emory physicians,” explains Dr. Williams. “A third of what we do in these settings is teaching, and the rest is direct care.”
The university’s hospitalist program started in 1999 with eight hospitalists; today, it employs 60. The difference with an academic hospitalist program, explains Dr. Williams, is that “we’re essentially dealing with staffing teaching teams, teaching, and having research components.”
IPC–The Hospitalist Company
Perhaps the best-known hospitalist employer, IPC (North Hollywood, Calif.) currently has approximately 500 full-time employed hospitalists and 150-200 part-timers working in more than 200 facilities across 23 U.S. markets.
“We have every type of practice, including academic and small hospitals,” says Adam D. Singer, MD, chairman, CEO, and chief medical officer of IPC. The company was re-incorporated in 1995. “We started accelerating in ’97, and we’ve been growing 30 to 50% per year—steady growth. We’re acquiring like-minded groups. We’ve had 10 acquisitions in the last 24 months. All our acquisitions have to be high-minded, quality groups.”
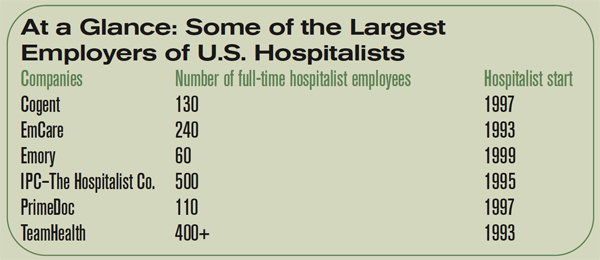
PrimeDoc
Based in Asheville, N.C., PrimeDoc is 100% physician-owned and managed. Counting permanent employees as well as independent contractors, the company staffs approximately 110 hospitalists.
“We do things a little differently,” says Robert J. Reynolds, MD, president and CEO, who also co-founded PrimeDoc in 1997. “We started as a freestanding practice serving one hospital, and we use a private practice model today. We’ve grown by establishing private practices in five states along the Atlantic seaboard.”
Dr. Reynolds admits that the PrimeDoc model is not “terribly unique. We contract with hospitals to provide care to unassigned patients, and we solicit referrals from [primary care physicians] in the community.”
TeamHealth Hospital Medicine
Another company that started out providing ED services—as well as administrative and staffing services—TeamHealth (Wilmington, N.C.) now employees more than 400 hospitalists, most of whom are full-time employees.
“Until this past year, I think we’ve been a little bit of a sleeper in hospital medicine,” says Stacy Goldsholl, MD, president. “That’s all changing now, as we’re aggressively pursuing the number-one place in the market. But we’ve grown as a silent presence through our relational reputations—basically, through word of mouth in the emergency departments. We have more than 400 contracts [in emergency medicine].”
The company continues to add hospital medicine programs through several methods. “We set up new programs from scratch, we restructure existing programs, we acquire large hospital medicine groups,” says Dr. Goldsholl, “and we apply things that work in one model to other models.”
Growth Trends
One feature these organizations have in common: explosive growth. The corporations are acquiring, starting, or partnering with a steady stream of hospital medicine programs.
“We’ve more than doubled in the last year,” says Dr. Goldsholl. “Our pipeline for hospital medicine groups is just exploding. We’re trying to manage the growth we have as well as what’s coming. We hope to double again in the next two years.”
Within that increase in programs comes another growth trend: hospital clients are asking their hospital medicine groups to take on more responsibility. “Our role in the hospital setting is definitely expanding,” says Dr. Goldsholl. “And the hospitalist’s role is only going to increase. We’ll see more hospital-based intensivists, surgicalists, and laborists [OB/GYN physicians]—there’s tremendous growth coming.”
Dr. Reynolds agrees. “In 1997, we basically provided medical care for acute care patients,” he explains. “Now we’re providing care for surgical care patients. We do pre-op eval[uation]s and perioperative management. We’ve also seen more demand for rapid response management, and we’re being asked to do pre-op eval[uation]s for outpatient surgeries.”
More hospitals are proactively seeking out these market leaders to explore adding a new hospital medicine program. “We’re getting calls from smaller and smaller hospitals,” says Dr. Reynolds. “Even the smallest hospitals want to implement a hospital medicine program, and it’s difficult to provide 24-hour coverage and have it make sense financially. But the trend is promising: Every hospital wants this type of service.”
Will these big players gobble up independent programs? That depends on how those programs are doing. “I haven’t heard of any programs being replaced if they’re doing all the right things and their costs are in line,” according to Dr. Atchley. “What you’re seeing is national companies either starting programs or salvaging programs that have failed.”
Industry Trends
Managing a large number of hospital medicine programs provides these companies with a clearer view of what’s happening in the specialty as it grows and changes. One trend that they’re seeing is a sort of second phase, where hospitals that brought in hospitalists several years ago now seek to improve their programs.
“In the past year, we’ve seen [hospitals express] more need, more interest in a hospital medicine management company coming in and restructuring a struggling program or a failed program,” says Dr. Goldsholl.
EmCare observes the same trend. “Hospitals are a lot savvier than they were five or 10 years ago about the setup of a hospital medicine program,” says Dr. Wagner. “Some [hospital administrators] may be on their second or third program, and they know what they want. They ask about recruitment success, retention rates, your data gathering and reporting tools, and what you do specifically to support your physicians in terms of leadership, quality, and satisfaction.”
These expectations are not simply discussed; they become part of the contractual agreement. “Hospitals also want service deliverables written in the contract,” adds Dr. Wagner, “including physician performance in terms of patient satisfaction, primary care physician satisfaction, JCAHO core measures, and medical staff participation.”
Why Big May Be Better
A large group with an established infrastructure that includes standards for quality checks, patient satisfaction, and so on is appealing to hospitals. “Because of economies of scale, we can offer state-of-the-art technologies, billing and collection, and infrastructure,” says Dr. Singer. “We also have the ability to recruit physicians. Small groups cannot compete with that.”
Another attractive feature is the history that these groups have in a relatively new field. “We have a track record of setting up successful programs,” points out Dr. Reynolds. ”We’ve already learned from our mistakes.”
Working for a national corporation has its benefits, including opportunities for education and advancement and an infrastructure support that can take some of the workload off a hospitalist’s shoulders. Dr. Greeno points out that Cogent handles administrative work for the physicians, freeing up their time for patients.
“One guy said, ‘I like working here because it’s the best opportunity to practice pure medicine,’ ” he says. “Our physicians are not case managers; they’re not schedulers.”
And working as part of a large group provides a built-in network of colleagues. “There’s connectivity for the individual hospitalist, as well as the medical director, to learn from other hospitalists all over the country,” says Dr. Goldsholl.
Dr. Wagner names compliance as one of EmCare’s top benefits. “We code physician notes professionally, and the result is we have greater than 95% compliance with Medicare. That’s something a national company can bring to the table.”
Some say that a large organization may be more attractive to job candidates. “Our size demonstrates stability to candidates,” says Dr. Williams. “Recruiting is a 100%-a-year job, and this helps.”
He points out that a larger program can appeal to the hospitalists within it: “Another advantage to our size is that we can draw from a pool of physicians to help out if necessary.”
Of course, physicians who work for larger companies may enjoy a larger compensation package, which can benefit the entire specialty. “In my experience, when [large companies] have come into my area, their salary structure is higher,” says Dr. Atchley. “The result is that other groups in the region have to change their salaries to be more competitive.”
The Upside to Independents
One factor that helps hospitals decide between bringing in a national company and using an independent local group is the cost.
“[Local programs] may not be as expensive as the large groups,” says Dr. Atchley. “When my hospital sent out an RFP [request for proposal], we saw that some of our costs were much less than what a national company” has to charge.
One major concern individual hospitalists and smaller groups may have regarding employment in a national corporation is loss of autonomy. Would they be expected to follow rigid rules and regulations set forth by a distant corporation office? The leaders in those offices say no, absolutely not.
“We actually manage down to a small practice,” says Dr. Singer. “Concerns are that there will be a loss of autonomy; that’s not true.”
Regardless of which type of hospital medicine program one prefers, having options is good for both the hospital and the physician. “Competition is good,” maintains Dr. Atchley. “When these companies come in, they’ll definitely provide superior infrastructure and can track outcomes. Homegrown hospital medicine programs should use the same approach.”
A Glimpse of the Future
Will all hospitalists eventually work for a behemoth corporation? Not a chance, say the CEOs and CMOs of the current hospital medicine company leaders. “There are lessons to be learned from the emergency department,” says Dr. Wagner. “Large companies don’t have the majority of ED contracts. There’s only so much [large companies] can manage before it starts to get picked off by smaller, younger practices that are more nimble and quick to respond.
“All the big players won’t be dominant from a market-share point of view,” he adds. “But what they will do is set expectations for good hospital medicine practices.”
However, the employment model for hospitalists will continue to change. “We’re going to see existing [large] companies increase their regional presence,” predicts Dr. Reynolds. “The hospital-owned model will fade away. Physicians make lousy hospital employees—they just don’t fit into the hospital’s view of an employee.”
Dr. Atchley agrees with this point: “We’ll probably see fewer and fewer programs where the physician is employed by the hospital. That’s pretty much what the SHM surveys are showing.”
And when will the booming market for hospitalists start to slow? “I see [the market] growing well beyond my crystal ball,” says Dr. Singer. “I see a soon-to-be emerging trend of hospitals wanting hospitalists rather than internists. More groups are going to step up and add that—make an internist into a subspecialist. It’s a new way of thinking.”
Even without a crystal ball, leaders in hospital medicine forecast that the field will continue to grow and that hospitalists will become better trained, credentialed, and accepted as a specialty—regardless of what type of organization they work for. TH
Jane Jerrard writes “Career Development” and “Public Policy” for The Hospitalist.
Disclaimer: SHM Members William Atchley, MD, FACP, Ron Greeno, MD, Stacy Goldsholl, MD, and Mark V. Williams, MD, FACP, are quoted in this article. Their opinions do not reflect or represent the opinions of SHM.
Hospital medicine may be a young field, but several major providers have already been established. Each of these rapidly growing organizations employs dozens—or even hundreds—of hospitalists and is establishing or revamping hospital medicine programs across the United States.
As these organizations grow, they are shaping hospital medicine. “I think that what the large companies really bring to the table is a vision of what hospital medicine is supposed to be about: evidence-based medicine and other things important to the hospital,” says William Atchley, MD, FACP, a practicing hospitalist in Hampton, Va.
This month, we examine just a few of the many large hospital medicine groups in order to set the stage for this growing trend and the issues presented by these groups. That said, here is an overview of some of the largest national players in hospital medicine, their perspective on the industry, their philosophies, and dialogue about their astonishing growth.
The Players
Which organizations have become the nation’s largest employers of hospitalists?
Cogent Healthcare
Based in Irvine, Calif., Cogent employs approximately 130 full-time hospitalists, with an additional 70 who “work with us in other arrangements; some are partnered with us,” says Ron Greeno, MD, FCCP, Cogent chief medical officer.
Cogent was founded by four physician groups in Los Angeles County. “We started in late 1997 and spent the first several years developing the model,” recalls Dr. Greeno. “In the 2000s, we started building programs for hospitals. We’ve seen growth of around 40% a year for the last several years. Frankly, we started too early; the market wasn’t really ready.”
What sets Cogent apart, says Dr. Greeno, is its focus. “We’re not a physician practice management company,” he stresses. “Our competitors’ goal is to build large, successful practices. We built a practice that’s hospital-centric. This helps the hospital satisfy its goals.”
EmCare
Perhaps the first of the national players to actively undertake hospital medicine, EmCare developed its first hospitalist program in 1993 at Baylor University Medical Center (BUMC) in Texas. “[Baylor is] still with us,” says Michael Wagner, MD, CEO, Hospitalists Division, EmCare.
EmCare has more than 30 years of experience with emergency department (ED) staffing, which is how it got its foot in the hospitalist door.
“In the late ’90s, other hospital EDs talked to us” about bringing in a hospitalist program, says Dr. Wagner. “So in each ED region, we worked to sell [the] hospital medicine program. It didn’t really take off until the 2000s, when non-clients started approaching us.”
Today, EmCare employs 350 hospitalists, 240 of whom work full-time. They provide hospital medicine to 47 clients in 60 programs in 37 states.
Emory Healthcare
Emory Healthcare’s Hospital Medicine Unit in Atlanta is the largest academic hospital medicine program in the United States.
“We occupy five hospitals,” says Mark V. Williams, MD, FACP, director of Emory’s Hospital Medicine Unit and editor of the Journal of Hospital Medicine. “Thirty of our hospitalists teach at the two university hospitals, and an additional eight teach at [one of three] community hospital[s]. Others will teach in-service training as well.”
The two university hospitals—Emory University Hospital and Crawford Long Hospital—are “solely staffed by Emory physicians,” explains Dr. Williams. “A third of what we do in these settings is teaching, and the rest is direct care.”
The university’s hospitalist program started in 1999 with eight hospitalists; today, it employs 60. The difference with an academic hospitalist program, explains Dr. Williams, is that “we’re essentially dealing with staffing teaching teams, teaching, and having research components.”
IPC–The Hospitalist Company
Perhaps the best-known hospitalist employer, IPC (North Hollywood, Calif.) currently has approximately 500 full-time employed hospitalists and 150-200 part-timers working in more than 200 facilities across 23 U.S. markets.
“We have every type of practice, including academic and small hospitals,” says Adam D. Singer, MD, chairman, CEO, and chief medical officer of IPC. The company was re-incorporated in 1995. “We started accelerating in ’97, and we’ve been growing 30 to 50% per year—steady growth. We’re acquiring like-minded groups. We’ve had 10 acquisitions in the last 24 months. All our acquisitions have to be high-minded, quality groups.”
PrimeDoc
Based in Asheville, N.C., PrimeDoc is 100% physician-owned and managed. Counting permanent employees as well as independent contractors, the company staffs approximately 110 hospitalists.
“We do things a little differently,” says Robert J. Reynolds, MD, president and CEO, who also co-founded PrimeDoc in 1997. “We started as a freestanding practice serving one hospital, and we use a private practice model today. We’ve grown by establishing private practices in five states along the Atlantic seaboard.”
Dr. Reynolds admits that the PrimeDoc model is not “terribly unique. We contract with hospitals to provide care to unassigned patients, and we solicit referrals from [primary care physicians] in the community.”
TeamHealth Hospital Medicine
Another company that started out providing ED services—as well as administrative and staffing services—TeamHealth (Wilmington, N.C.) now employees more than 400 hospitalists, most of whom are full-time employees.
“Until this past year, I think we’ve been a little bit of a sleeper in hospital medicine,” says Stacy Goldsholl, MD, president. “That’s all changing now, as we’re aggressively pursuing the number-one place in the market. But we’ve grown as a silent presence through our relational reputations—basically, through word of mouth in the emergency departments. We have more than 400 contracts [in emergency medicine].”
The company continues to add hospital medicine programs through several methods. “We set up new programs from scratch, we restructure existing programs, we acquire large hospital medicine groups,” says Dr. Goldsholl, “and we apply things that work in one model to other models.”
Growth Trends
One feature these organizations have in common: explosive growth. The corporations are acquiring, starting, or partnering with a steady stream of hospital medicine programs.
“We’ve more than doubled in the last year,” says Dr. Goldsholl. “Our pipeline for hospital medicine groups is just exploding. We’re trying to manage the growth we have as well as what’s coming. We hope to double again in the next two years.”
Within that increase in programs comes another growth trend: hospital clients are asking their hospital medicine groups to take on more responsibility. “Our role in the hospital setting is definitely expanding,” says Dr. Goldsholl. “And the hospitalist’s role is only going to increase. We’ll see more hospital-based intensivists, surgicalists, and laborists [OB/GYN physicians]—there’s tremendous growth coming.”
Dr. Reynolds agrees. “In 1997, we basically provided medical care for acute care patients,” he explains. “Now we’re providing care for surgical care patients. We do pre-op eval[uation]s and perioperative management. We’ve also seen more demand for rapid response management, and we’re being asked to do pre-op eval[uation]s for outpatient surgeries.”
More hospitals are proactively seeking out these market leaders to explore adding a new hospital medicine program. “We’re getting calls from smaller and smaller hospitals,” says Dr. Reynolds. “Even the smallest hospitals want to implement a hospital medicine program, and it’s difficult to provide 24-hour coverage and have it make sense financially. But the trend is promising: Every hospital wants this type of service.”
Will these big players gobble up independent programs? That depends on how those programs are doing. “I haven’t heard of any programs being replaced if they’re doing all the right things and their costs are in line,” according to Dr. Atchley. “What you’re seeing is national companies either starting programs or salvaging programs that have failed.”
Industry Trends
Managing a large number of hospital medicine programs provides these companies with a clearer view of what’s happening in the specialty as it grows and changes. One trend that they’re seeing is a sort of second phase, where hospitals that brought in hospitalists several years ago now seek to improve their programs.
“In the past year, we’ve seen [hospitals express] more need, more interest in a hospital medicine management company coming in and restructuring a struggling program or a failed program,” says Dr. Goldsholl.
EmCare observes the same trend. “Hospitals are a lot savvier than they were five or 10 years ago about the setup of a hospital medicine program,” says Dr. Wagner. “Some [hospital administrators] may be on their second or third program, and they know what they want. They ask about recruitment success, retention rates, your data gathering and reporting tools, and what you do specifically to support your physicians in terms of leadership, quality, and satisfaction.”
These expectations are not simply discussed; they become part of the contractual agreement. “Hospitals also want service deliverables written in the contract,” adds Dr. Wagner, “including physician performance in terms of patient satisfaction, primary care physician satisfaction, JCAHO core measures, and medical staff participation.”
Why Big May Be Better
A large group with an established infrastructure that includes standards for quality checks, patient satisfaction, and so on is appealing to hospitals. “Because of economies of scale, we can offer state-of-the-art technologies, billing and collection, and infrastructure,” says Dr. Singer. “We also have the ability to recruit physicians. Small groups cannot compete with that.”
Another attractive feature is the history that these groups have in a relatively new field. “We have a track record of setting up successful programs,” points out Dr. Reynolds. ”We’ve already learned from our mistakes.”
Working for a national corporation has its benefits, including opportunities for education and advancement and an infrastructure support that can take some of the workload off a hospitalist’s shoulders. Dr. Greeno points out that Cogent handles administrative work for the physicians, freeing up their time for patients.
“One guy said, ‘I like working here because it’s the best opportunity to practice pure medicine,’ ” he says. “Our physicians are not case managers; they’re not schedulers.”
And working as part of a large group provides a built-in network of colleagues. “There’s connectivity for the individual hospitalist, as well as the medical director, to learn from other hospitalists all over the country,” says Dr. Goldsholl.
Dr. Wagner names compliance as one of EmCare’s top benefits. “We code physician notes professionally, and the result is we have greater than 95% compliance with Medicare. That’s something a national company can bring to the table.”
Some say that a large organization may be more attractive to job candidates. “Our size demonstrates stability to candidates,” says Dr. Williams. “Recruiting is a 100%-a-year job, and this helps.”
He points out that a larger program can appeal to the hospitalists within it: “Another advantage to our size is that we can draw from a pool of physicians to help out if necessary.”
Of course, physicians who work for larger companies may enjoy a larger compensation package, which can benefit the entire specialty. “In my experience, when [large companies] have come into my area, their salary structure is higher,” says Dr. Atchley. “The result is that other groups in the region have to change their salaries to be more competitive.”
The Upside to Independents
One factor that helps hospitals decide between bringing in a national company and using an independent local group is the cost.
“[Local programs] may not be as expensive as the large groups,” says Dr. Atchley. “When my hospital sent out an RFP [request for proposal], we saw that some of our costs were much less than what a national company” has to charge.
One major concern individual hospitalists and smaller groups may have regarding employment in a national corporation is loss of autonomy. Would they be expected to follow rigid rules and regulations set forth by a distant corporation office? The leaders in those offices say no, absolutely not.
“We actually manage down to a small practice,” says Dr. Singer. “Concerns are that there will be a loss of autonomy; that’s not true.”
Regardless of which type of hospital medicine program one prefers, having options is good for both the hospital and the physician. “Competition is good,” maintains Dr. Atchley. “When these companies come in, they’ll definitely provide superior infrastructure and can track outcomes. Homegrown hospital medicine programs should use the same approach.”
A Glimpse of the Future
Will all hospitalists eventually work for a behemoth corporation? Not a chance, say the CEOs and CMOs of the current hospital medicine company leaders. “There are lessons to be learned from the emergency department,” says Dr. Wagner. “Large companies don’t have the majority of ED contracts. There’s only so much [large companies] can manage before it starts to get picked off by smaller, younger practices that are more nimble and quick to respond.
“All the big players won’t be dominant from a market-share point of view,” he adds. “But what they will do is set expectations for good hospital medicine practices.”
However, the employment model for hospitalists will continue to change. “We’re going to see existing [large] companies increase their regional presence,” predicts Dr. Reynolds. “The hospital-owned model will fade away. Physicians make lousy hospital employees—they just don’t fit into the hospital’s view of an employee.”
Dr. Atchley agrees with this point: “We’ll probably see fewer and fewer programs where the physician is employed by the hospital. That’s pretty much what the SHM surveys are showing.”
And when will the booming market for hospitalists start to slow? “I see [the market] growing well beyond my crystal ball,” says Dr. Singer. “I see a soon-to-be emerging trend of hospitals wanting hospitalists rather than internists. More groups are going to step up and add that—make an internist into a subspecialist. It’s a new way of thinking.”
Even without a crystal ball, leaders in hospital medicine forecast that the field will continue to grow and that hospitalists will become better trained, credentialed, and accepted as a specialty—regardless of what type of organization they work for. TH
Jane Jerrard writes “Career Development” and “Public Policy” for The Hospitalist.
Disclaimer: SHM Members William Atchley, MD, FACP, Ron Greeno, MD, Stacy Goldsholl, MD, and Mark V. Williams, MD, FACP, are quoted in this article. Their opinions do not reflect or represent the opinions of SHM.
Hospital medicine may be a young field, but several major providers have already been established. Each of these rapidly growing organizations employs dozens—or even hundreds—of hospitalists and is establishing or revamping hospital medicine programs across the United States.
As these organizations grow, they are shaping hospital medicine. “I think that what the large companies really bring to the table is a vision of what hospital medicine is supposed to be about: evidence-based medicine and other things important to the hospital,” says William Atchley, MD, FACP, a practicing hospitalist in Hampton, Va.
This month, we examine just a few of the many large hospital medicine groups in order to set the stage for this growing trend and the issues presented by these groups. That said, here is an overview of some of the largest national players in hospital medicine, their perspective on the industry, their philosophies, and dialogue about their astonishing growth.
The Players
Which organizations have become the nation’s largest employers of hospitalists?
Cogent Healthcare
Based in Irvine, Calif., Cogent employs approximately 130 full-time hospitalists, with an additional 70 who “work with us in other arrangements; some are partnered with us,” says Ron Greeno, MD, FCCP, Cogent chief medical officer.
Cogent was founded by four physician groups in Los Angeles County. “We started in late 1997 and spent the first several years developing the model,” recalls Dr. Greeno. “In the 2000s, we started building programs for hospitals. We’ve seen growth of around 40% a year for the last several years. Frankly, we started too early; the market wasn’t really ready.”
What sets Cogent apart, says Dr. Greeno, is its focus. “We’re not a physician practice management company,” he stresses. “Our competitors’ goal is to build large, successful practices. We built a practice that’s hospital-centric. This helps the hospital satisfy its goals.”
EmCare
Perhaps the first of the national players to actively undertake hospital medicine, EmCare developed its first hospitalist program in 1993 at Baylor University Medical Center (BUMC) in Texas. “[Baylor is] still with us,” says Michael Wagner, MD, CEO, Hospitalists Division, EmCare.
EmCare has more than 30 years of experience with emergency department (ED) staffing, which is how it got its foot in the hospitalist door.
“In the late ’90s, other hospital EDs talked to us” about bringing in a hospitalist program, says Dr. Wagner. “So in each ED region, we worked to sell [the] hospital medicine program. It didn’t really take off until the 2000s, when non-clients started approaching us.”
Today, EmCare employs 350 hospitalists, 240 of whom work full-time. They provide hospital medicine to 47 clients in 60 programs in 37 states.
Emory Healthcare
Emory Healthcare’s Hospital Medicine Unit in Atlanta is the largest academic hospital medicine program in the United States.
“We occupy five hospitals,” says Mark V. Williams, MD, FACP, director of Emory’s Hospital Medicine Unit and editor of the Journal of Hospital Medicine. “Thirty of our hospitalists teach at the two university hospitals, and an additional eight teach at [one of three] community hospital[s]. Others will teach in-service training as well.”
The two university hospitals—Emory University Hospital and Crawford Long Hospital—are “solely staffed by Emory physicians,” explains Dr. Williams. “A third of what we do in these settings is teaching, and the rest is direct care.”
The university’s hospitalist program started in 1999 with eight hospitalists; today, it employs 60. The difference with an academic hospitalist program, explains Dr. Williams, is that “we’re essentially dealing with staffing teaching teams, teaching, and having research components.”
IPC–The Hospitalist Company
Perhaps the best-known hospitalist employer, IPC (North Hollywood, Calif.) currently has approximately 500 full-time employed hospitalists and 150-200 part-timers working in more than 200 facilities across 23 U.S. markets.
“We have every type of practice, including academic and small hospitals,” says Adam D. Singer, MD, chairman, CEO, and chief medical officer of IPC. The company was re-incorporated in 1995. “We started accelerating in ’97, and we’ve been growing 30 to 50% per year—steady growth. We’re acquiring like-minded groups. We’ve had 10 acquisitions in the last 24 months. All our acquisitions have to be high-minded, quality groups.”
PrimeDoc
Based in Asheville, N.C., PrimeDoc is 100% physician-owned and managed. Counting permanent employees as well as independent contractors, the company staffs approximately 110 hospitalists.
“We do things a little differently,” says Robert J. Reynolds, MD, president and CEO, who also co-founded PrimeDoc in 1997. “We started as a freestanding practice serving one hospital, and we use a private practice model today. We’ve grown by establishing private practices in five states along the Atlantic seaboard.”
Dr. Reynolds admits that the PrimeDoc model is not “terribly unique. We contract with hospitals to provide care to unassigned patients, and we solicit referrals from [primary care physicians] in the community.”
TeamHealth Hospital Medicine
Another company that started out providing ED services—as well as administrative and staffing services—TeamHealth (Wilmington, N.C.) now employees more than 400 hospitalists, most of whom are full-time employees.
“Until this past year, I think we’ve been a little bit of a sleeper in hospital medicine,” says Stacy Goldsholl, MD, president. “That’s all changing now, as we’re aggressively pursuing the number-one place in the market. But we’ve grown as a silent presence through our relational reputations—basically, through word of mouth in the emergency departments. We have more than 400 contracts [in emergency medicine].”
The company continues to add hospital medicine programs through several methods. “We set up new programs from scratch, we restructure existing programs, we acquire large hospital medicine groups,” says Dr. Goldsholl, “and we apply things that work in one model to other models.”
Growth Trends
One feature these organizations have in common: explosive growth. The corporations are acquiring, starting, or partnering with a steady stream of hospital medicine programs.
“We’ve more than doubled in the last year,” says Dr. Goldsholl. “Our pipeline for hospital medicine groups is just exploding. We’re trying to manage the growth we have as well as what’s coming. We hope to double again in the next two years.”
Within that increase in programs comes another growth trend: hospital clients are asking their hospital medicine groups to take on more responsibility. “Our role in the hospital setting is definitely expanding,” says Dr. Goldsholl. “And the hospitalist’s role is only going to increase. We’ll see more hospital-based intensivists, surgicalists, and laborists [OB/GYN physicians]—there’s tremendous growth coming.”
Dr. Reynolds agrees. “In 1997, we basically provided medical care for acute care patients,” he explains. “Now we’re providing care for surgical care patients. We do pre-op eval[uation]s and perioperative management. We’ve also seen more demand for rapid response management, and we’re being asked to do pre-op eval[uation]s for outpatient surgeries.”
More hospitals are proactively seeking out these market leaders to explore adding a new hospital medicine program. “We’re getting calls from smaller and smaller hospitals,” says Dr. Reynolds. “Even the smallest hospitals want to implement a hospital medicine program, and it’s difficult to provide 24-hour coverage and have it make sense financially. But the trend is promising: Every hospital wants this type of service.”
Will these big players gobble up independent programs? That depends on how those programs are doing. “I haven’t heard of any programs being replaced if they’re doing all the right things and their costs are in line,” according to Dr. Atchley. “What you’re seeing is national companies either starting programs or salvaging programs that have failed.”
Industry Trends
Managing a large number of hospital medicine programs provides these companies with a clearer view of what’s happening in the specialty as it grows and changes. One trend that they’re seeing is a sort of second phase, where hospitals that brought in hospitalists several years ago now seek to improve their programs.
“In the past year, we’ve seen [hospitals express] more need, more interest in a hospital medicine management company coming in and restructuring a struggling program or a failed program,” says Dr. Goldsholl.
EmCare observes the same trend. “Hospitals are a lot savvier than they were five or 10 years ago about the setup of a hospital medicine program,” says Dr. Wagner. “Some [hospital administrators] may be on their second or third program, and they know what they want. They ask about recruitment success, retention rates, your data gathering and reporting tools, and what you do specifically to support your physicians in terms of leadership, quality, and satisfaction.”
These expectations are not simply discussed; they become part of the contractual agreement. “Hospitals also want service deliverables written in the contract,” adds Dr. Wagner, “including physician performance in terms of patient satisfaction, primary care physician satisfaction, JCAHO core measures, and medical staff participation.”
Why Big May Be Better
A large group with an established infrastructure that includes standards for quality checks, patient satisfaction, and so on is appealing to hospitals. “Because of economies of scale, we can offer state-of-the-art technologies, billing and collection, and infrastructure,” says Dr. Singer. “We also have the ability to recruit physicians. Small groups cannot compete with that.”
Another attractive feature is the history that these groups have in a relatively new field. “We have a track record of setting up successful programs,” points out Dr. Reynolds. ”We’ve already learned from our mistakes.”
Working for a national corporation has its benefits, including opportunities for education and advancement and an infrastructure support that can take some of the workload off a hospitalist’s shoulders. Dr. Greeno points out that Cogent handles administrative work for the physicians, freeing up their time for patients.
“One guy said, ‘I like working here because it’s the best opportunity to practice pure medicine,’ ” he says. “Our physicians are not case managers; they’re not schedulers.”
And working as part of a large group provides a built-in network of colleagues. “There’s connectivity for the individual hospitalist, as well as the medical director, to learn from other hospitalists all over the country,” says Dr. Goldsholl.
Dr. Wagner names compliance as one of EmCare’s top benefits. “We code physician notes professionally, and the result is we have greater than 95% compliance with Medicare. That’s something a national company can bring to the table.”
Some say that a large organization may be more attractive to job candidates. “Our size demonstrates stability to candidates,” says Dr. Williams. “Recruiting is a 100%-a-year job, and this helps.”
He points out that a larger program can appeal to the hospitalists within it: “Another advantage to our size is that we can draw from a pool of physicians to help out if necessary.”
Of course, physicians who work for larger companies may enjoy a larger compensation package, which can benefit the entire specialty. “In my experience, when [large companies] have come into my area, their salary structure is higher,” says Dr. Atchley. “The result is that other groups in the region have to change their salaries to be more competitive.”
The Upside to Independents
One factor that helps hospitals decide between bringing in a national company and using an independent local group is the cost.
“[Local programs] may not be as expensive as the large groups,” says Dr. Atchley. “When my hospital sent out an RFP [request for proposal], we saw that some of our costs were much less than what a national company” has to charge.
One major concern individual hospitalists and smaller groups may have regarding employment in a national corporation is loss of autonomy. Would they be expected to follow rigid rules and regulations set forth by a distant corporation office? The leaders in those offices say no, absolutely not.
“We actually manage down to a small practice,” says Dr. Singer. “Concerns are that there will be a loss of autonomy; that’s not true.”
Regardless of which type of hospital medicine program one prefers, having options is good for both the hospital and the physician. “Competition is good,” maintains Dr. Atchley. “When these companies come in, they’ll definitely provide superior infrastructure and can track outcomes. Homegrown hospital medicine programs should use the same approach.”
A Glimpse of the Future
Will all hospitalists eventually work for a behemoth corporation? Not a chance, say the CEOs and CMOs of the current hospital medicine company leaders. “There are lessons to be learned from the emergency department,” says Dr. Wagner. “Large companies don’t have the majority of ED contracts. There’s only so much [large companies] can manage before it starts to get picked off by smaller, younger practices that are more nimble and quick to respond.
“All the big players won’t be dominant from a market-share point of view,” he adds. “But what they will do is set expectations for good hospital medicine practices.”
However, the employment model for hospitalists will continue to change. “We’re going to see existing [large] companies increase their regional presence,” predicts Dr. Reynolds. “The hospital-owned model will fade away. Physicians make lousy hospital employees—they just don’t fit into the hospital’s view of an employee.”
Dr. Atchley agrees with this point: “We’ll probably see fewer and fewer programs where the physician is employed by the hospital. That’s pretty much what the SHM surveys are showing.”
And when will the booming market for hospitalists start to slow? “I see [the market] growing well beyond my crystal ball,” says Dr. Singer. “I see a soon-to-be emerging trend of hospitals wanting hospitalists rather than internists. More groups are going to step up and add that—make an internist into a subspecialist. It’s a new way of thinking.”
Even without a crystal ball, leaders in hospital medicine forecast that the field will continue to grow and that hospitalists will become better trained, credentialed, and accepted as a specialty—regardless of what type of organization they work for. TH
Jane Jerrard writes “Career Development” and “Public Policy” for The Hospitalist.