User login
Principal Investigations
What can you do with a quarter of a million dollars? In some places, that amount can buy a home that can shelter a family for decades. In other places, it is enough to pay annual malpractice insurance premiums for physicians practicing in high-risk specialties—with a little left over.
But if you wanted to use that money for an enduring healthcare project that would provide the most good for the most people, how would you do it? Hospitalists can look to the Agency for Healthcare Research and Quality (AHRQ) for stellar examples of well-invested dollars with excellent return.
AHRQ Funding
With a staff of approximately 300, the tiny AHRQ is the lead federal agency charged with improving the quality, safety, efficiency, and effectiveness of healthcare for all Americans. It creates a priority research agenda annually, and funds studies in areas where improvement is deemed most needed. These include patient safety, data development, pharmaceutical outcomes, and other areas described on its Web site (www.ahrq.gov/).
In 2005, AHRQ announced its Partnerships in Implementing Patient Safety (PIPS) and committed up to $9 million in total costs to fund new grants of less than $300,000 per year, lasting two years. AHRQ indicated that eligible safe practice intervention projects would be required to include “tool kits,” and a comprehensive implementation tool kit to help others overcome barriers and allay adoption concerns. AHRQ’s goal was and is to disseminate funded projects’ perfected tools widely for adaptation and/or adoption by diverse healthcare settings.
AHRQ asked that principal investigators (PIs) be experienced senior level individuals familiar with implementing change in healthcare settings. Their expectation was that PIs would devote at least 15% of their time to the project for its duration. Thus the competitive challenge to potential PIs was great:
- Select a worthy project from among the endless areas where healthcare needs improvement, and then plan specific, realistic, achievable interventions that could create measurable improvement over two years;
- Implement the program; and
- Develop a plan and tools so basic and user-friendly that they could feasibly be applied in not just the local practice setting, but in other healthcare settings.
Although the size and duration of the awards varied, many of the 17 projects they funded received slightly more than a quarter of a million dollars. Among the funded projects, two boast hospitalists as their PIs and address areas of obvious concern in most healthcare settings. Greg Maynard, MD, MS, at the University of California, San Diego, was funded to implement a venous thromboembolism (VTE) intervention program. And Mark V. Williams, MD, FACP, professor of medicine, Emory University School of Medicine, Atlanta, and editor of the Journal of Hospital Medicine, was funded to implement a discharge bundle of patient safety interventions respectively.
Stalking the Silent Killer
Dr. Maynard’s project, “Optimal Prevention of Hospital Acquired Venous Thromboembolism,” focuses on eliminating preventable hospital-acquired VTE at an academic healthcare facility that has a large population of Hispanic patients.
The project’s timeliness and utility is clear: Although the exact incidence of VTE is unknown, experts estimate that approximately 260,000 are clinically recognized annually in acutely hospitalized patients.1 Pulmonary embolism (PE) resulting from deep vein thrombosis (DVT) is the most common cause of preventable hospital death, the majority of hospitalized patients with risk factors for DVT receive no prophylaxis, and the rate of fatal PE more than doubles between age 50 and 80.2,3 The problem is easily recognizable, but “Getting people to do what they need to do to prevent VTE can be hard,” says Dr. Maynard.
This project was carefully planned. It used a rigorous quality improvement process, involving all appropriate clinicians, nurses, managers, and technical support personnel.
Dr. Maynard and his team anticipated roadblocks and negotiated in advance to reduce their effects. They accepted that when patients are hospitalized, things frequently happen that cause physicians to stop VTE prophylaxis: A hemoglobin or platelet count may fall, the patient may have difficulty taking the drug, or the patient’s status may change abruptly. Or the prophylaxis might be accidentally discontinued—perhaps when a patient is transferred.
The team also looked at other institutions’ solutions. Then, using a basic understanding of the ways in which their process was missing VTE prophylaxis opportunities, they built interventions.
This team considered logistics carefully because it was clear that the only intervention that could decrease risk would have to be repetitive in nature. “The process we ultimately selected is very, very quick, yet valid,” says Dr. Maynard, while acknowledging that presenting any intervention repeatedly has the potential to interfere with care. “Other models require the physician to use math and add points. This one does not, and takes only seconds.”
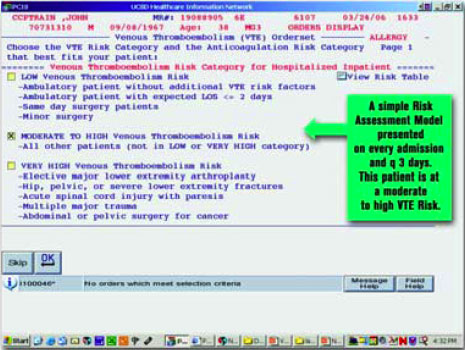
Beginning April 19, 2006, the University of California, San Diego (UCSD) will introduce an intervention that presents a VTE risk assessment screen on every patient who is admitted. This process inquires about the need for prophylaxis every three days for the duration of hospitalization, and physicians cannot skip the screen. If risk factors are present and bleeding risk is not, the screen presents appropriate VTE options.
For example, the system will suggest enoxaparin 40 mg daily, enoxaparin 30 mg twice daily, or appropriately dosed warfarin for a high-risk orthopedic surgery patient who has no bleeding risk. Every three days, the process repeats itself, making explicit decisions or suggestions about appropriate prophylaxis. (Figure 1, below, shows a sample screen for a patient with moderately high risk.
Much evidence about VTE is still being gathered. For example, opinions vary about when to start prophylaxis or how long to continue it. Dr. Maynard and his team also addressed real versus relative contraindications—another area of debate among clinicians. Many clinicians are uncertain about how soon after surgery to restart VTE prophylaxis. After orthopedic spine surgery, for example, some might start it on day five, while others may not restart prophylaxis even after day 10. At UCSD, clinical stakeholders in the process came to consensus, and now all restart by day seven.
The tool kit UCSD is developing recognizes that every institution is unique. Those that choose to implement a similar program must identify their baseline rate of VTE and monitor change over time to determine if progress is being made. Every institution must define adequate VTE prophylaxis and tailor the tools appropriately.
Wait? No Need
One compelling aspect of Dr. Maynard’s project is that some of UCSD’s VTE tools are already available on the SHM Web site in the “VTE Resource Room.” With or without AHRQ funding, UCSD planned to develop and implement a VTE awareness program. UCSD’s grant department provided the support Dr. Maynard and his colleagues needed to apply for the AHRQ funding, and Dr. Maynard says the funding they received helped UCSD “disseminate the program better and to carry it out with more rigor.”
UCSD worked with SHM to develop the tool kit. In return, SHM is providing and promoting the VTE tool kit at no charge to interested parties. Additionally, SHM recently received funding via an unrestricted sponsorship to create a mentored implementation project for the “VTE Resource Room.” Interested institutions will be mentored by UCSD staff who have experience with the tool kit.
Over time, Dr. Maynard will measure the effects of the intervention to ensure it is working. In addition to creating a malleable tool kit, UCSD research hospitalists will examine race, gender, and age to determine the effects of these on the likelihood of getting adequate prophylaxis.
Hospital Patient Safe-D(ischarge)
Dr. Williams and his colleagues at Emory University and the University of Ottawa received funding for “Hospital Patient Safe-D(ischarge): A Discharge Bundle for Patients,” a program that builds on previous AHRQ funding. This intervention implements a “discharge bundle” of patient safety interventions to improve patient transition from the hospital to home or another healthcare setting.
“We hope that every patient will undergo discharge, and of course the majority do, but the discharge process has almost been treated as an afterthought,” explains Dr. Williams. “Doctors spend a lot of time on diagnosis and treatment, but not on discharge. This process of transition from total care with a call button, lots of nursing attention, daily visits from the doctor, and delivered meals to greater independence, has not been well researched.”
What little research exists tends to indicate that discharge processes are very heterogeneous.
So far, Dr. Williams’ team’s examination of the process has produced only one surprise: The team has discovered that the discharge process is even more capricious than they suspected. As patients prepare to leave the hospital, what could and should be an orderly process that educates and prepares patients to assume responsibility for their own care in a new and better way is often interrupted or disjointed.
Preparing patients for discharge once fell to the nursing staff. As nursing faces staffing shortages and expanded roles, the discharge process often belongs to everyone and to no one. That physicians’ discharge visits pay much less than the time required to do it well also complicates the problem. The researchers were not surprised, however, to learn that many patients do not know their diagnosis or treatment plan as discharge is imminent. Their goal is to develop a consistent, comprehensive discharge process that will be a national model.
Here again, the precepts of continuous quality improvement are apparent. Dr. Williams’ team’s effort represents collaboration among physicians, pharmacists, nurses, and patients; involves SHM and several other professional organizations; and calls upon an advisory committee consisting of nationally recognized patient care and safety experts.
The discharge bundle of patient safety interventions—a concept advocated by the Joint Commission on Accreditation of Healthcare Organizations and other quality-promoting groups—adds a post-discharge continuity check to medication reconciliation and patient-centered education at discharge.
The four project phases—implement, evaluate, develop a tool, and disseminate the discharge bundle—overlap and ensure success.
Dr. Williams believes that the group of patients most likely to benefit from this intervention is the elderly. “The elderly bear the greatest burden of chronic disease and typically have several concurrent health problems,” he says.
Educating elders at the time of discharge should decrease the medication error rate and improve adherence to other treatments and recommended lifestyle changes. To gauge the appropriateness of the discharge bundle, John Banja, PhD, an expert in communication and safety, observes the discharge process directly. All communications must be patient-centered, and thus presented in a manner that patients will understand and appreciate. Banja relies on his background in patient safety and disability/rehabilitation to assess the discharge process.
Initial enrollment in this study seems successful. More than 50 patients have consented to participate, but Banja projects a need for 200 to complete the entire process. Recently, the team increased its planned maximum accrual to 300 to increase the statistical power of their findings. The participants like the program because most of them find discharge somewhat discomforting. Patients know they have knowledge gaps and appreciate clinicians’ efforts to fill those gaps seamlessly. A small investment of time can prevent problems after discharge.
Added Value
Clearly, the findings from these AHRQ-funded studies have the potential to reduce morbidity and mortality in a logarithmic manner as other institutions adapt these new tool kits. Dr. Williams indicates that recipients of PIPS funding receive more than just funding and the satisfaction of creating tools that will help all Americans.
“The AHRQ sponsors quarterly conference calls for all participants, regardless of their research topic, and an annual meeting in June to bring all investigators together,” he says.
The opportunity to learn how others address problems, plan interventions, and tackle hurdles proves invaluable. In addition, being privy to interim study results or learning how others handle research dilemmas helps hospitalists expand their skill sets.
Listening to Drs. Maynard and Williams is a not-so-subtle reminder that every hospital needs a well-structured quality improvement plan, and that hospitalists are essential in the plan’s success. Every hospitalist needs an understanding of the precepts these PIs used to earn this well-deserved funding: interdisciplinary and professional organization collaboration, good communication, realistic planning, managing change by measuring, and above all, sharing success. TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
References
- Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med. 1991 May;151(5):933-938.
- Clagett GP, Anderson FA Jr, Heit J, et al. Prevention of venous thromboembolism. Chest. 1995 Oct;108(4 Suppl):312S-334S.
- Geerts WH, Heit JA, Clagett GP, et al. Prevention of venous thromboembolism. Chest. 2001;119(1 Suppl):132S-175S.
What can you do with a quarter of a million dollars? In some places, that amount can buy a home that can shelter a family for decades. In other places, it is enough to pay annual malpractice insurance premiums for physicians practicing in high-risk specialties—with a little left over.
But if you wanted to use that money for an enduring healthcare project that would provide the most good for the most people, how would you do it? Hospitalists can look to the Agency for Healthcare Research and Quality (AHRQ) for stellar examples of well-invested dollars with excellent return.
AHRQ Funding
With a staff of approximately 300, the tiny AHRQ is the lead federal agency charged with improving the quality, safety, efficiency, and effectiveness of healthcare for all Americans. It creates a priority research agenda annually, and funds studies in areas where improvement is deemed most needed. These include patient safety, data development, pharmaceutical outcomes, and other areas described on its Web site (www.ahrq.gov/).
In 2005, AHRQ announced its Partnerships in Implementing Patient Safety (PIPS) and committed up to $9 million in total costs to fund new grants of less than $300,000 per year, lasting two years. AHRQ indicated that eligible safe practice intervention projects would be required to include “tool kits,” and a comprehensive implementation tool kit to help others overcome barriers and allay adoption concerns. AHRQ’s goal was and is to disseminate funded projects’ perfected tools widely for adaptation and/or adoption by diverse healthcare settings.
AHRQ asked that principal investigators (PIs) be experienced senior level individuals familiar with implementing change in healthcare settings. Their expectation was that PIs would devote at least 15% of their time to the project for its duration. Thus the competitive challenge to potential PIs was great:
- Select a worthy project from among the endless areas where healthcare needs improvement, and then plan specific, realistic, achievable interventions that could create measurable improvement over two years;
- Implement the program; and
- Develop a plan and tools so basic and user-friendly that they could feasibly be applied in not just the local practice setting, but in other healthcare settings.
Although the size and duration of the awards varied, many of the 17 projects they funded received slightly more than a quarter of a million dollars. Among the funded projects, two boast hospitalists as their PIs and address areas of obvious concern in most healthcare settings. Greg Maynard, MD, MS, at the University of California, San Diego, was funded to implement a venous thromboembolism (VTE) intervention program. And Mark V. Williams, MD, FACP, professor of medicine, Emory University School of Medicine, Atlanta, and editor of the Journal of Hospital Medicine, was funded to implement a discharge bundle of patient safety interventions respectively.
Stalking the Silent Killer
Dr. Maynard’s project, “Optimal Prevention of Hospital Acquired Venous Thromboembolism,” focuses on eliminating preventable hospital-acquired VTE at an academic healthcare facility that has a large population of Hispanic patients.
The project’s timeliness and utility is clear: Although the exact incidence of VTE is unknown, experts estimate that approximately 260,000 are clinically recognized annually in acutely hospitalized patients.1 Pulmonary embolism (PE) resulting from deep vein thrombosis (DVT) is the most common cause of preventable hospital death, the majority of hospitalized patients with risk factors for DVT receive no prophylaxis, and the rate of fatal PE more than doubles between age 50 and 80.2,3 The problem is easily recognizable, but “Getting people to do what they need to do to prevent VTE can be hard,” says Dr. Maynard.
This project was carefully planned. It used a rigorous quality improvement process, involving all appropriate clinicians, nurses, managers, and technical support personnel.
Dr. Maynard and his team anticipated roadblocks and negotiated in advance to reduce their effects. They accepted that when patients are hospitalized, things frequently happen that cause physicians to stop VTE prophylaxis: A hemoglobin or platelet count may fall, the patient may have difficulty taking the drug, or the patient’s status may change abruptly. Or the prophylaxis might be accidentally discontinued—perhaps when a patient is transferred.
The team also looked at other institutions’ solutions. Then, using a basic understanding of the ways in which their process was missing VTE prophylaxis opportunities, they built interventions.
This team considered logistics carefully because it was clear that the only intervention that could decrease risk would have to be repetitive in nature. “The process we ultimately selected is very, very quick, yet valid,” says Dr. Maynard, while acknowledging that presenting any intervention repeatedly has the potential to interfere with care. “Other models require the physician to use math and add points. This one does not, and takes only seconds.”
Beginning April 19, 2006, the University of California, San Diego (UCSD) will introduce an intervention that presents a VTE risk assessment screen on every patient who is admitted. This process inquires about the need for prophylaxis every three days for the duration of hospitalization, and physicians cannot skip the screen. If risk factors are present and bleeding risk is not, the screen presents appropriate VTE options.
For example, the system will suggest enoxaparin 40 mg daily, enoxaparin 30 mg twice daily, or appropriately dosed warfarin for a high-risk orthopedic surgery patient who has no bleeding risk. Every three days, the process repeats itself, making explicit decisions or suggestions about appropriate prophylaxis. (Figure 1, below, shows a sample screen for a patient with moderately high risk.
Much evidence about VTE is still being gathered. For example, opinions vary about when to start prophylaxis or how long to continue it. Dr. Maynard and his team also addressed real versus relative contraindications—another area of debate among clinicians. Many clinicians are uncertain about how soon after surgery to restart VTE prophylaxis. After orthopedic spine surgery, for example, some might start it on day five, while others may not restart prophylaxis even after day 10. At UCSD, clinical stakeholders in the process came to consensus, and now all restart by day seven.
The tool kit UCSD is developing recognizes that every institution is unique. Those that choose to implement a similar program must identify their baseline rate of VTE and monitor change over time to determine if progress is being made. Every institution must define adequate VTE prophylaxis and tailor the tools appropriately.
Wait? No Need
One compelling aspect of Dr. Maynard’s project is that some of UCSD’s VTE tools are already available on the SHM Web site in the “VTE Resource Room.” With or without AHRQ funding, UCSD planned to develop and implement a VTE awareness program. UCSD’s grant department provided the support Dr. Maynard and his colleagues needed to apply for the AHRQ funding, and Dr. Maynard says the funding they received helped UCSD “disseminate the program better and to carry it out with more rigor.”
UCSD worked with SHM to develop the tool kit. In return, SHM is providing and promoting the VTE tool kit at no charge to interested parties. Additionally, SHM recently received funding via an unrestricted sponsorship to create a mentored implementation project for the “VTE Resource Room.” Interested institutions will be mentored by UCSD staff who have experience with the tool kit.
Over time, Dr. Maynard will measure the effects of the intervention to ensure it is working. In addition to creating a malleable tool kit, UCSD research hospitalists will examine race, gender, and age to determine the effects of these on the likelihood of getting adequate prophylaxis.
Hospital Patient Safe-D(ischarge)
Dr. Williams and his colleagues at Emory University and the University of Ottawa received funding for “Hospital Patient Safe-D(ischarge): A Discharge Bundle for Patients,” a program that builds on previous AHRQ funding. This intervention implements a “discharge bundle” of patient safety interventions to improve patient transition from the hospital to home or another healthcare setting.
“We hope that every patient will undergo discharge, and of course the majority do, but the discharge process has almost been treated as an afterthought,” explains Dr. Williams. “Doctors spend a lot of time on diagnosis and treatment, but not on discharge. This process of transition from total care with a call button, lots of nursing attention, daily visits from the doctor, and delivered meals to greater independence, has not been well researched.”
What little research exists tends to indicate that discharge processes are very heterogeneous.
So far, Dr. Williams’ team’s examination of the process has produced only one surprise: The team has discovered that the discharge process is even more capricious than they suspected. As patients prepare to leave the hospital, what could and should be an orderly process that educates and prepares patients to assume responsibility for their own care in a new and better way is often interrupted or disjointed.
Preparing patients for discharge once fell to the nursing staff. As nursing faces staffing shortages and expanded roles, the discharge process often belongs to everyone and to no one. That physicians’ discharge visits pay much less than the time required to do it well also complicates the problem. The researchers were not surprised, however, to learn that many patients do not know their diagnosis or treatment plan as discharge is imminent. Their goal is to develop a consistent, comprehensive discharge process that will be a national model.
Here again, the precepts of continuous quality improvement are apparent. Dr. Williams’ team’s effort represents collaboration among physicians, pharmacists, nurses, and patients; involves SHM and several other professional organizations; and calls upon an advisory committee consisting of nationally recognized patient care and safety experts.
The discharge bundle of patient safety interventions—a concept advocated by the Joint Commission on Accreditation of Healthcare Organizations and other quality-promoting groups—adds a post-discharge continuity check to medication reconciliation and patient-centered education at discharge.
The four project phases—implement, evaluate, develop a tool, and disseminate the discharge bundle—overlap and ensure success.
Dr. Williams believes that the group of patients most likely to benefit from this intervention is the elderly. “The elderly bear the greatest burden of chronic disease and typically have several concurrent health problems,” he says.
Educating elders at the time of discharge should decrease the medication error rate and improve adherence to other treatments and recommended lifestyle changes. To gauge the appropriateness of the discharge bundle, John Banja, PhD, an expert in communication and safety, observes the discharge process directly. All communications must be patient-centered, and thus presented in a manner that patients will understand and appreciate. Banja relies on his background in patient safety and disability/rehabilitation to assess the discharge process.
Initial enrollment in this study seems successful. More than 50 patients have consented to participate, but Banja projects a need for 200 to complete the entire process. Recently, the team increased its planned maximum accrual to 300 to increase the statistical power of their findings. The participants like the program because most of them find discharge somewhat discomforting. Patients know they have knowledge gaps and appreciate clinicians’ efforts to fill those gaps seamlessly. A small investment of time can prevent problems after discharge.
Added Value
Clearly, the findings from these AHRQ-funded studies have the potential to reduce morbidity and mortality in a logarithmic manner as other institutions adapt these new tool kits. Dr. Williams indicates that recipients of PIPS funding receive more than just funding and the satisfaction of creating tools that will help all Americans.
“The AHRQ sponsors quarterly conference calls for all participants, regardless of their research topic, and an annual meeting in June to bring all investigators together,” he says.
The opportunity to learn how others address problems, plan interventions, and tackle hurdles proves invaluable. In addition, being privy to interim study results or learning how others handle research dilemmas helps hospitalists expand their skill sets.
Listening to Drs. Maynard and Williams is a not-so-subtle reminder that every hospital needs a well-structured quality improvement plan, and that hospitalists are essential in the plan’s success. Every hospitalist needs an understanding of the precepts these PIs used to earn this well-deserved funding: interdisciplinary and professional organization collaboration, good communication, realistic planning, managing change by measuring, and above all, sharing success. TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
References
- Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med. 1991 May;151(5):933-938.
- Clagett GP, Anderson FA Jr, Heit J, et al. Prevention of venous thromboembolism. Chest. 1995 Oct;108(4 Suppl):312S-334S.
- Geerts WH, Heit JA, Clagett GP, et al. Prevention of venous thromboembolism. Chest. 2001;119(1 Suppl):132S-175S.
What can you do with a quarter of a million dollars? In some places, that amount can buy a home that can shelter a family for decades. In other places, it is enough to pay annual malpractice insurance premiums for physicians practicing in high-risk specialties—with a little left over.
But if you wanted to use that money for an enduring healthcare project that would provide the most good for the most people, how would you do it? Hospitalists can look to the Agency for Healthcare Research and Quality (AHRQ) for stellar examples of well-invested dollars with excellent return.
AHRQ Funding
With a staff of approximately 300, the tiny AHRQ is the lead federal agency charged with improving the quality, safety, efficiency, and effectiveness of healthcare for all Americans. It creates a priority research agenda annually, and funds studies in areas where improvement is deemed most needed. These include patient safety, data development, pharmaceutical outcomes, and other areas described on its Web site (www.ahrq.gov/).
In 2005, AHRQ announced its Partnerships in Implementing Patient Safety (PIPS) and committed up to $9 million in total costs to fund new grants of less than $300,000 per year, lasting two years. AHRQ indicated that eligible safe practice intervention projects would be required to include “tool kits,” and a comprehensive implementation tool kit to help others overcome barriers and allay adoption concerns. AHRQ’s goal was and is to disseminate funded projects’ perfected tools widely for adaptation and/or adoption by diverse healthcare settings.
AHRQ asked that principal investigators (PIs) be experienced senior level individuals familiar with implementing change in healthcare settings. Their expectation was that PIs would devote at least 15% of their time to the project for its duration. Thus the competitive challenge to potential PIs was great:
- Select a worthy project from among the endless areas where healthcare needs improvement, and then plan specific, realistic, achievable interventions that could create measurable improvement over two years;
- Implement the program; and
- Develop a plan and tools so basic and user-friendly that they could feasibly be applied in not just the local practice setting, but in other healthcare settings.
Although the size and duration of the awards varied, many of the 17 projects they funded received slightly more than a quarter of a million dollars. Among the funded projects, two boast hospitalists as their PIs and address areas of obvious concern in most healthcare settings. Greg Maynard, MD, MS, at the University of California, San Diego, was funded to implement a venous thromboembolism (VTE) intervention program. And Mark V. Williams, MD, FACP, professor of medicine, Emory University School of Medicine, Atlanta, and editor of the Journal of Hospital Medicine, was funded to implement a discharge bundle of patient safety interventions respectively.
Stalking the Silent Killer
Dr. Maynard’s project, “Optimal Prevention of Hospital Acquired Venous Thromboembolism,” focuses on eliminating preventable hospital-acquired VTE at an academic healthcare facility that has a large population of Hispanic patients.
The project’s timeliness and utility is clear: Although the exact incidence of VTE is unknown, experts estimate that approximately 260,000 are clinically recognized annually in acutely hospitalized patients.1 Pulmonary embolism (PE) resulting from deep vein thrombosis (DVT) is the most common cause of preventable hospital death, the majority of hospitalized patients with risk factors for DVT receive no prophylaxis, and the rate of fatal PE more than doubles between age 50 and 80.2,3 The problem is easily recognizable, but “Getting people to do what they need to do to prevent VTE can be hard,” says Dr. Maynard.
This project was carefully planned. It used a rigorous quality improvement process, involving all appropriate clinicians, nurses, managers, and technical support personnel.
Dr. Maynard and his team anticipated roadblocks and negotiated in advance to reduce their effects. They accepted that when patients are hospitalized, things frequently happen that cause physicians to stop VTE prophylaxis: A hemoglobin or platelet count may fall, the patient may have difficulty taking the drug, or the patient’s status may change abruptly. Or the prophylaxis might be accidentally discontinued—perhaps when a patient is transferred.
The team also looked at other institutions’ solutions. Then, using a basic understanding of the ways in which their process was missing VTE prophylaxis opportunities, they built interventions.
This team considered logistics carefully because it was clear that the only intervention that could decrease risk would have to be repetitive in nature. “The process we ultimately selected is very, very quick, yet valid,” says Dr. Maynard, while acknowledging that presenting any intervention repeatedly has the potential to interfere with care. “Other models require the physician to use math and add points. This one does not, and takes only seconds.”
Beginning April 19, 2006, the University of California, San Diego (UCSD) will introduce an intervention that presents a VTE risk assessment screen on every patient who is admitted. This process inquires about the need for prophylaxis every three days for the duration of hospitalization, and physicians cannot skip the screen. If risk factors are present and bleeding risk is not, the screen presents appropriate VTE options.
For example, the system will suggest enoxaparin 40 mg daily, enoxaparin 30 mg twice daily, or appropriately dosed warfarin for a high-risk orthopedic surgery patient who has no bleeding risk. Every three days, the process repeats itself, making explicit decisions or suggestions about appropriate prophylaxis. (Figure 1, below, shows a sample screen for a patient with moderately high risk.
Much evidence about VTE is still being gathered. For example, opinions vary about when to start prophylaxis or how long to continue it. Dr. Maynard and his team also addressed real versus relative contraindications—another area of debate among clinicians. Many clinicians are uncertain about how soon after surgery to restart VTE prophylaxis. After orthopedic spine surgery, for example, some might start it on day five, while others may not restart prophylaxis even after day 10. At UCSD, clinical stakeholders in the process came to consensus, and now all restart by day seven.
The tool kit UCSD is developing recognizes that every institution is unique. Those that choose to implement a similar program must identify their baseline rate of VTE and monitor change over time to determine if progress is being made. Every institution must define adequate VTE prophylaxis and tailor the tools appropriately.
Wait? No Need
One compelling aspect of Dr. Maynard’s project is that some of UCSD’s VTE tools are already available on the SHM Web site in the “VTE Resource Room.” With or without AHRQ funding, UCSD planned to develop and implement a VTE awareness program. UCSD’s grant department provided the support Dr. Maynard and his colleagues needed to apply for the AHRQ funding, and Dr. Maynard says the funding they received helped UCSD “disseminate the program better and to carry it out with more rigor.”
UCSD worked with SHM to develop the tool kit. In return, SHM is providing and promoting the VTE tool kit at no charge to interested parties. Additionally, SHM recently received funding via an unrestricted sponsorship to create a mentored implementation project for the “VTE Resource Room.” Interested institutions will be mentored by UCSD staff who have experience with the tool kit.
Over time, Dr. Maynard will measure the effects of the intervention to ensure it is working. In addition to creating a malleable tool kit, UCSD research hospitalists will examine race, gender, and age to determine the effects of these on the likelihood of getting adequate prophylaxis.
Hospital Patient Safe-D(ischarge)
Dr. Williams and his colleagues at Emory University and the University of Ottawa received funding for “Hospital Patient Safe-D(ischarge): A Discharge Bundle for Patients,” a program that builds on previous AHRQ funding. This intervention implements a “discharge bundle” of patient safety interventions to improve patient transition from the hospital to home or another healthcare setting.
“We hope that every patient will undergo discharge, and of course the majority do, but the discharge process has almost been treated as an afterthought,” explains Dr. Williams. “Doctors spend a lot of time on diagnosis and treatment, but not on discharge. This process of transition from total care with a call button, lots of nursing attention, daily visits from the doctor, and delivered meals to greater independence, has not been well researched.”
What little research exists tends to indicate that discharge processes are very heterogeneous.
So far, Dr. Williams’ team’s examination of the process has produced only one surprise: The team has discovered that the discharge process is even more capricious than they suspected. As patients prepare to leave the hospital, what could and should be an orderly process that educates and prepares patients to assume responsibility for their own care in a new and better way is often interrupted or disjointed.
Preparing patients for discharge once fell to the nursing staff. As nursing faces staffing shortages and expanded roles, the discharge process often belongs to everyone and to no one. That physicians’ discharge visits pay much less than the time required to do it well also complicates the problem. The researchers were not surprised, however, to learn that many patients do not know their diagnosis or treatment plan as discharge is imminent. Their goal is to develop a consistent, comprehensive discharge process that will be a national model.
Here again, the precepts of continuous quality improvement are apparent. Dr. Williams’ team’s effort represents collaboration among physicians, pharmacists, nurses, and patients; involves SHM and several other professional organizations; and calls upon an advisory committee consisting of nationally recognized patient care and safety experts.
The discharge bundle of patient safety interventions—a concept advocated by the Joint Commission on Accreditation of Healthcare Organizations and other quality-promoting groups—adds a post-discharge continuity check to medication reconciliation and patient-centered education at discharge.
The four project phases—implement, evaluate, develop a tool, and disseminate the discharge bundle—overlap and ensure success.
Dr. Williams believes that the group of patients most likely to benefit from this intervention is the elderly. “The elderly bear the greatest burden of chronic disease and typically have several concurrent health problems,” he says.
Educating elders at the time of discharge should decrease the medication error rate and improve adherence to other treatments and recommended lifestyle changes. To gauge the appropriateness of the discharge bundle, John Banja, PhD, an expert in communication and safety, observes the discharge process directly. All communications must be patient-centered, and thus presented in a manner that patients will understand and appreciate. Banja relies on his background in patient safety and disability/rehabilitation to assess the discharge process.
Initial enrollment in this study seems successful. More than 50 patients have consented to participate, but Banja projects a need for 200 to complete the entire process. Recently, the team increased its planned maximum accrual to 300 to increase the statistical power of their findings. The participants like the program because most of them find discharge somewhat discomforting. Patients know they have knowledge gaps and appreciate clinicians’ efforts to fill those gaps seamlessly. A small investment of time can prevent problems after discharge.
Added Value
Clearly, the findings from these AHRQ-funded studies have the potential to reduce morbidity and mortality in a logarithmic manner as other institutions adapt these new tool kits. Dr. Williams indicates that recipients of PIPS funding receive more than just funding and the satisfaction of creating tools that will help all Americans.
“The AHRQ sponsors quarterly conference calls for all participants, regardless of their research topic, and an annual meeting in June to bring all investigators together,” he says.
The opportunity to learn how others address problems, plan interventions, and tackle hurdles proves invaluable. In addition, being privy to interim study results or learning how others handle research dilemmas helps hospitalists expand their skill sets.
Listening to Drs. Maynard and Williams is a not-so-subtle reminder that every hospital needs a well-structured quality improvement plan, and that hospitalists are essential in the plan’s success. Every hospitalist needs an understanding of the precepts these PIs used to earn this well-deserved funding: interdisciplinary and professional organization collaboration, good communication, realistic planning, managing change by measuring, and above all, sharing success. TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
References
- Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med. 1991 May;151(5):933-938.
- Clagett GP, Anderson FA Jr, Heit J, et al. Prevention of venous thromboembolism. Chest. 1995 Oct;108(4 Suppl):312S-334S.
- Geerts WH, Heit JA, Clagett GP, et al. Prevention of venous thromboembolism. Chest. 2001;119(1 Suppl):132S-175S.
Hospital of Distinction
From time to time, headlines highlight people or organizations recognized as outliers because the outcomes of their work garner national notice. More often than not tragic, accidental outcomes rivet our attention. Occasionally, though, it is the opposite: the achievement of an outcome so unusual and inconceivably distinguished that it warrants emulation. The receipt of the 2005 Malcolm Baldrige National Quality Award by Bronson Methodist Hospital, Kalamazoo, Mich., is an example of the latter. It was no accident—this is an organization that pursues validation of its excellence assertively and enthusiastically. It is unusual because it is only the fifth healthcare organization to be counted among the ranks of Baldrige winners, and it is distinguished because the award comes from our nation’s highest elected leader.
The management team at Bronson is quick to point out that it took every employee’s involvement and enthusiasm to win this honor. Among those employees are 15 hospitalists, representing 11 full-time equivalents.
The Baldrige Award
Established in 1987 by an act of Congress, the Baldrige Award is presented annually by the President of the United States to qualifying organizations of any size in five categories: manufacturing, service, small business, education, and healthcare.
The application fee—ranging from $5,000 for large organizations to $500 for non-profit educational institutions—supports a minimum of 300 hours of review by eight or more business and quality experts, with on-site visits generating more than 1,000 hours of in-depth review. An extensive feedback report highlighting strengths and areas to improve is part of the review.
Contenders must be judged outstanding in seven areas to win. (See “Baldrige Award Criteria,” top left.) The criteria focus on two goals: delivering continuously improving value to customers and improving overall organizational performance. This helps organizations enhance their effectiveness and sustainability. Since 1999, when the Baldrige criteria for healthcare were first introduced, 116 healthcare organizations have applied.
The Beginning
According to, Katie Harrelson, RN, vice president of Patient Care Services and chief nurse executive, Bronson has always strived to be the best. In the late 1990s, they began looking at various quality models, and discovered the Baldrige Criteria.
“We began using the criteria because they provided a focus, or framework, to help us define who we are,” says Harrelson. “Physicians became partners, and patients are our customers. Bronson’s hospitalists are strong partners, and our relationship with them is great. It had to be in order to standardize care practices and continue our efforts to be a national leader in healthcare quality.”
She describes the organization’s three strategic objectives: clinical excellence, customer and service excellence, and corporate effectiveness. These “3 Cs” provide focus for Bronson and that are on the tip of all employees’ tongues.
As Bronson embarked on the journey to excellence, it already employed hospitalists. “Bronson started using hospitalists at a time when many of the community’s primary care physicians were older and retiring, or looking for an alternative admission method,” says Scott Larson, MD, senior vice president Medical Affairs and chief medical officer, “There were economic pressures, too. It’s less efficient for individual practitioners to conduct hospital rounds for a small number of patients than to use hospitalists, and hospitalists are more familiar with hospital protocol.”
By 2003 Bronson was continuing to integrate hospitalists into their program, and hospitalists were employing the precepts of performance improvement like other Bronson employees.
Excellence requires, among other things, good communication and unprecedented cooperation. Thus, employees from different departments and disciplines needed to identify new ways to improve existing care processes and work together as a multidisciplinary team. Hospitalists had a unique role that led to several changes.
“Hospitalists are involved in pretty much anything that happens at Bronson,” says Hussein Akl, MD, medical director for Bronson’s Hospitalist Service.
It was that involvement that led Bronson to change its approach to hip fracture care. Previously, the surgeon managed the hip fracture patient from admission to discharge. Bronson’s hospitalists proposed a new model, however: The hospitalists would manage the patient medically, leaving the surgeons to focus on what they do best: repairing the hip.
The success of the program is measured in clinical outcomes; length of stay has declined significantly since the specialists began collaborating in this way. In 2005 HealthGrades, an organization located in Golden, Colo., that rates care in 5,000 U.S. hospitals, awarded Bronson its highest rating (five stars) for hip replacement surgery and for treatment of acute myocardial infarction.
Hospitalists also took the lead in preparing for Primary Stroke Center Certification, a status Bronson achieved from the Joint Commission on Accreditation of Healthcare Organizations last year, and are leading physician engagement in Bronson’s computerized physician order entry project.
Dr. Larson emphasizes that achieving a level of excellence that meets Baldrige standards requires alignment, meaning that organizational, department or service, and individual performance goals must be congruent. Dr. Akl concurs: “Hospitalists had to align with our orthopedists to improve hip fracture care, and with neurologists on stroke.”
This level of excellence also requires constant vigilance and measurement, which is why Bronson uses scorecards to follow core indicators that reflect compliance with best practices for conditions like heart failure, and community acquired pneumonia. They also track their risk-adjusted Medicare mortality rate, which at 3.5% in 2005 was better than their 2004 rate (4.8%) and considerably better than the national average. Scorecards are distributed electronically and discussed in all meetings. Targets established at the beginning of the year are reviewed, and the hospitalist service’s performance is examined and compared with aggregate data for other admitting physicians. Management acknowledges that drilling data down to the individual level—except in rare cases—is often difficult and does not necessarily reflect an individual’s true performance.
“Patients are co-managed often, making individual provider data somewhat misleading,” explains Dr. Larson.
If recruitment and retention are an indication of employee satisfaction, Bronson’s hospitalists are satisfied. Few hospitalists have left; however, one hospitalist who left returned a year later citing Bronson’s well-structured program, the fact that all hospitalists have equal decision-making authority, and physician-based care (Bronson does not use physician extenders) as re-employment incentives.
“Of course, he said the pay was good, too,” quips Dr. Akl. At Bronson, results are rewarded and recognized generously.
The Patient’s Perspective
Bronson’s approach to hospital care translates into distinct differences—from the moment patients enter until discharge. Also recognized internationally as a Pebble Project Partner, Bronson’s facility design proves that function follows form. (See “The Pebble Project,” p. 39.) The building has a first-class hotel feel to it, with well-planned spaces and indoor gardens. Staff emphasizes privacy and service—not just care. Acknowledging that patients have needs and responsibilities outside the hospital that don’t pause while they are admitted, Bronson offers amenities such as wireless computers so patients can stay connected to their lives, beepers so family members can leave a surgical waiting area without fear of missing the surgeon’s post-operative visit, 24-hour room service, and a concierge to run errands or quarterback problems.
Increasingly evidence links architectural design to outcomes in many healthcare settings, and Bronson has acted on the evidence. The hospital is easy to navigate, and because a major building campaign finished this facility in 2000 every patient room is private with its own hand-washing station. Patients needn’t worry about a roommate’s noisy guest or snoring, but, more importantly, private rooms are associated with lower nosocomial infection rates and speedier recovery.
Operating and labor costs are also lower because patients are not transferred as often. At Bronson, infection rates fell 11% overall compared with the rate in their former facility that had a combination of private and semi-private rooms.
Bronson continues to monitor infection rates and also tracks employee turnover, outcome measures, length of stay, cost per unit of service, waiting times, patient satisfaction levels, nosocomial infection rates, and organizational behaviors.
Sharing Caring
Bronson’s hospitalists actively engage in information sharing. They share their protocols within the Bronson healthcare system and with other hospitals and providers. One recent project has been the successful effort to improve the discharge process—an area of emphasis for many quality-promoting oversight organizations and other facilities. Their next step is to automate their interventions.
Some also participate in a half-day Physician Leadership Academy, a gathering held quarterly to develop physician leadership skills and collaborate on identifying and implementing best practices.
Because Bronson’s overall atmosphere and organizational culture differ from older facilities or less avant-garde organizations, Harrelson, Dr. Larson, and Dr. Akl have difficulty identifying one unit where care might be considerably different than what the patient would receive elsewhere. Dr. Akl says that the hospitalists as a group discussed this question and determined that all Bronson units are held to the same high standards, but that the Adult Medical Unit (AMU) is an interesting model for serving the geriatric population.
In the AMU hospitalists lead the team to reach desirable outcomes. The unit’s propensity to admit elderly patients created unique needs that staff has met in correspondingly unique ways. Nursing’s commitment and capability is evident because all AMU nurses are NICHE (Nurses Improving Care for Health System Elders) certified. NICHE certification promotes systematic nursing change that ensures sensitive and exemplary patient-centered care for older patients. The hospitalists, too, have participated in this cultural change and created a protocol that anticipates elderly patients’ needs, and all hospitalists rotate through AMU to support this part of the continuum of care.
The Outcomes
Bronson measures everything, and uses established best practices, benchmarks, and data to ensure that they meet and exceed national standards. They monitor clinical excellence using Centers for Medicare and Medicaid Services performance rates, Blue Cross Blue Shield targets, and the CareScience (Philadelphia) database. They also follow the JCAHO standards and Leapfrog Groups’ National Quality Forum’s measures.
They monitor patient satisfaction using Gallup Polls and “listen and learn” methods that build on the idea that the customer’s opinion and experience is often more valuable than that of an outside consultant. And, they monitor corporate effectiveness using tools that measure employee learning, vacancy rates, and commitment to the environment and the community.
Bronson’s persistence and desire to be the best has paid off. Patients receive beta-blockers and pre-surgical antibiotics at rates that exceed best practice. They have significantly reduced the incidence of ventilator-acquired pneumonia in all ICUs—the pediatric ICU has had none since 2004. Patient satisfaction increased from an already high 95% in 2002 to an astounding 97% in 2004.
For the past three years, Bronson has been named by Fortune and Working Mother magazines as one of the nation’s 100 best companies to work for. They have also been named by Solucient as one of the 100 Top Hospitals in the United States for 2005. Another acknowledgment is the Environmental Leadership Award from Hospitals for a Healthy Environment for reducing waste and pollution. The list of their achievements and awards is seemingly endless, but so too is their energy to continue to improve and deliver excellent care.
Bronson’s approach is what it takes to earn that ultimate recognition of quality: the Malcolm Baldrige National Quality Award. TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
From time to time, headlines highlight people or organizations recognized as outliers because the outcomes of their work garner national notice. More often than not tragic, accidental outcomes rivet our attention. Occasionally, though, it is the opposite: the achievement of an outcome so unusual and inconceivably distinguished that it warrants emulation. The receipt of the 2005 Malcolm Baldrige National Quality Award by Bronson Methodist Hospital, Kalamazoo, Mich., is an example of the latter. It was no accident—this is an organization that pursues validation of its excellence assertively and enthusiastically. It is unusual because it is only the fifth healthcare organization to be counted among the ranks of Baldrige winners, and it is distinguished because the award comes from our nation’s highest elected leader.
The management team at Bronson is quick to point out that it took every employee’s involvement and enthusiasm to win this honor. Among those employees are 15 hospitalists, representing 11 full-time equivalents.
The Baldrige Award
Established in 1987 by an act of Congress, the Baldrige Award is presented annually by the President of the United States to qualifying organizations of any size in five categories: manufacturing, service, small business, education, and healthcare.
The application fee—ranging from $5,000 for large organizations to $500 for non-profit educational institutions—supports a minimum of 300 hours of review by eight or more business and quality experts, with on-site visits generating more than 1,000 hours of in-depth review. An extensive feedback report highlighting strengths and areas to improve is part of the review.
Contenders must be judged outstanding in seven areas to win. (See “Baldrige Award Criteria,” top left.) The criteria focus on two goals: delivering continuously improving value to customers and improving overall organizational performance. This helps organizations enhance their effectiveness and sustainability. Since 1999, when the Baldrige criteria for healthcare were first introduced, 116 healthcare organizations have applied.
The Beginning
According to, Katie Harrelson, RN, vice president of Patient Care Services and chief nurse executive, Bronson has always strived to be the best. In the late 1990s, they began looking at various quality models, and discovered the Baldrige Criteria.
“We began using the criteria because they provided a focus, or framework, to help us define who we are,” says Harrelson. “Physicians became partners, and patients are our customers. Bronson’s hospitalists are strong partners, and our relationship with them is great. It had to be in order to standardize care practices and continue our efforts to be a national leader in healthcare quality.”
She describes the organization’s three strategic objectives: clinical excellence, customer and service excellence, and corporate effectiveness. These “3 Cs” provide focus for Bronson and that are on the tip of all employees’ tongues.
As Bronson embarked on the journey to excellence, it already employed hospitalists. “Bronson started using hospitalists at a time when many of the community’s primary care physicians were older and retiring, or looking for an alternative admission method,” says Scott Larson, MD, senior vice president Medical Affairs and chief medical officer, “There were economic pressures, too. It’s less efficient for individual practitioners to conduct hospital rounds for a small number of patients than to use hospitalists, and hospitalists are more familiar with hospital protocol.”
By 2003 Bronson was continuing to integrate hospitalists into their program, and hospitalists were employing the precepts of performance improvement like other Bronson employees.
Excellence requires, among other things, good communication and unprecedented cooperation. Thus, employees from different departments and disciplines needed to identify new ways to improve existing care processes and work together as a multidisciplinary team. Hospitalists had a unique role that led to several changes.
“Hospitalists are involved in pretty much anything that happens at Bronson,” says Hussein Akl, MD, medical director for Bronson’s Hospitalist Service.
It was that involvement that led Bronson to change its approach to hip fracture care. Previously, the surgeon managed the hip fracture patient from admission to discharge. Bronson’s hospitalists proposed a new model, however: The hospitalists would manage the patient medically, leaving the surgeons to focus on what they do best: repairing the hip.
The success of the program is measured in clinical outcomes; length of stay has declined significantly since the specialists began collaborating in this way. In 2005 HealthGrades, an organization located in Golden, Colo., that rates care in 5,000 U.S. hospitals, awarded Bronson its highest rating (five stars) for hip replacement surgery and for treatment of acute myocardial infarction.
Hospitalists also took the lead in preparing for Primary Stroke Center Certification, a status Bronson achieved from the Joint Commission on Accreditation of Healthcare Organizations last year, and are leading physician engagement in Bronson’s computerized physician order entry project.
Dr. Larson emphasizes that achieving a level of excellence that meets Baldrige standards requires alignment, meaning that organizational, department or service, and individual performance goals must be congruent. Dr. Akl concurs: “Hospitalists had to align with our orthopedists to improve hip fracture care, and with neurologists on stroke.”
This level of excellence also requires constant vigilance and measurement, which is why Bronson uses scorecards to follow core indicators that reflect compliance with best practices for conditions like heart failure, and community acquired pneumonia. They also track their risk-adjusted Medicare mortality rate, which at 3.5% in 2005 was better than their 2004 rate (4.8%) and considerably better than the national average. Scorecards are distributed electronically and discussed in all meetings. Targets established at the beginning of the year are reviewed, and the hospitalist service’s performance is examined and compared with aggregate data for other admitting physicians. Management acknowledges that drilling data down to the individual level—except in rare cases—is often difficult and does not necessarily reflect an individual’s true performance.
“Patients are co-managed often, making individual provider data somewhat misleading,” explains Dr. Larson.
If recruitment and retention are an indication of employee satisfaction, Bronson’s hospitalists are satisfied. Few hospitalists have left; however, one hospitalist who left returned a year later citing Bronson’s well-structured program, the fact that all hospitalists have equal decision-making authority, and physician-based care (Bronson does not use physician extenders) as re-employment incentives.
“Of course, he said the pay was good, too,” quips Dr. Akl. At Bronson, results are rewarded and recognized generously.
The Patient’s Perspective
Bronson’s approach to hospital care translates into distinct differences—from the moment patients enter until discharge. Also recognized internationally as a Pebble Project Partner, Bronson’s facility design proves that function follows form. (See “The Pebble Project,” p. 39.) The building has a first-class hotel feel to it, with well-planned spaces and indoor gardens. Staff emphasizes privacy and service—not just care. Acknowledging that patients have needs and responsibilities outside the hospital that don’t pause while they are admitted, Bronson offers amenities such as wireless computers so patients can stay connected to their lives, beepers so family members can leave a surgical waiting area without fear of missing the surgeon’s post-operative visit, 24-hour room service, and a concierge to run errands or quarterback problems.
Increasingly evidence links architectural design to outcomes in many healthcare settings, and Bronson has acted on the evidence. The hospital is easy to navigate, and because a major building campaign finished this facility in 2000 every patient room is private with its own hand-washing station. Patients needn’t worry about a roommate’s noisy guest or snoring, but, more importantly, private rooms are associated with lower nosocomial infection rates and speedier recovery.
Operating and labor costs are also lower because patients are not transferred as often. At Bronson, infection rates fell 11% overall compared with the rate in their former facility that had a combination of private and semi-private rooms.
Bronson continues to monitor infection rates and also tracks employee turnover, outcome measures, length of stay, cost per unit of service, waiting times, patient satisfaction levels, nosocomial infection rates, and organizational behaviors.
Sharing Caring
Bronson’s hospitalists actively engage in information sharing. They share their protocols within the Bronson healthcare system and with other hospitals and providers. One recent project has been the successful effort to improve the discharge process—an area of emphasis for many quality-promoting oversight organizations and other facilities. Their next step is to automate their interventions.
Some also participate in a half-day Physician Leadership Academy, a gathering held quarterly to develop physician leadership skills and collaborate on identifying and implementing best practices.
Because Bronson’s overall atmosphere and organizational culture differ from older facilities or less avant-garde organizations, Harrelson, Dr. Larson, and Dr. Akl have difficulty identifying one unit where care might be considerably different than what the patient would receive elsewhere. Dr. Akl says that the hospitalists as a group discussed this question and determined that all Bronson units are held to the same high standards, but that the Adult Medical Unit (AMU) is an interesting model for serving the geriatric population.
In the AMU hospitalists lead the team to reach desirable outcomes. The unit’s propensity to admit elderly patients created unique needs that staff has met in correspondingly unique ways. Nursing’s commitment and capability is evident because all AMU nurses are NICHE (Nurses Improving Care for Health System Elders) certified. NICHE certification promotes systematic nursing change that ensures sensitive and exemplary patient-centered care for older patients. The hospitalists, too, have participated in this cultural change and created a protocol that anticipates elderly patients’ needs, and all hospitalists rotate through AMU to support this part of the continuum of care.
The Outcomes
Bronson measures everything, and uses established best practices, benchmarks, and data to ensure that they meet and exceed national standards. They monitor clinical excellence using Centers for Medicare and Medicaid Services performance rates, Blue Cross Blue Shield targets, and the CareScience (Philadelphia) database. They also follow the JCAHO standards and Leapfrog Groups’ National Quality Forum’s measures.
They monitor patient satisfaction using Gallup Polls and “listen and learn” methods that build on the idea that the customer’s opinion and experience is often more valuable than that of an outside consultant. And, they monitor corporate effectiveness using tools that measure employee learning, vacancy rates, and commitment to the environment and the community.
Bronson’s persistence and desire to be the best has paid off. Patients receive beta-blockers and pre-surgical antibiotics at rates that exceed best practice. They have significantly reduced the incidence of ventilator-acquired pneumonia in all ICUs—the pediatric ICU has had none since 2004. Patient satisfaction increased from an already high 95% in 2002 to an astounding 97% in 2004.
For the past three years, Bronson has been named by Fortune and Working Mother magazines as one of the nation’s 100 best companies to work for. They have also been named by Solucient as one of the 100 Top Hospitals in the United States for 2005. Another acknowledgment is the Environmental Leadership Award from Hospitals for a Healthy Environment for reducing waste and pollution. The list of their achievements and awards is seemingly endless, but so too is their energy to continue to improve and deliver excellent care.
Bronson’s approach is what it takes to earn that ultimate recognition of quality: the Malcolm Baldrige National Quality Award. TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
From time to time, headlines highlight people or organizations recognized as outliers because the outcomes of their work garner national notice. More often than not tragic, accidental outcomes rivet our attention. Occasionally, though, it is the opposite: the achievement of an outcome so unusual and inconceivably distinguished that it warrants emulation. The receipt of the 2005 Malcolm Baldrige National Quality Award by Bronson Methodist Hospital, Kalamazoo, Mich., is an example of the latter. It was no accident—this is an organization that pursues validation of its excellence assertively and enthusiastically. It is unusual because it is only the fifth healthcare organization to be counted among the ranks of Baldrige winners, and it is distinguished because the award comes from our nation’s highest elected leader.
The management team at Bronson is quick to point out that it took every employee’s involvement and enthusiasm to win this honor. Among those employees are 15 hospitalists, representing 11 full-time equivalents.
The Baldrige Award
Established in 1987 by an act of Congress, the Baldrige Award is presented annually by the President of the United States to qualifying organizations of any size in five categories: manufacturing, service, small business, education, and healthcare.
The application fee—ranging from $5,000 for large organizations to $500 for non-profit educational institutions—supports a minimum of 300 hours of review by eight or more business and quality experts, with on-site visits generating more than 1,000 hours of in-depth review. An extensive feedback report highlighting strengths and areas to improve is part of the review.
Contenders must be judged outstanding in seven areas to win. (See “Baldrige Award Criteria,” top left.) The criteria focus on two goals: delivering continuously improving value to customers and improving overall organizational performance. This helps organizations enhance their effectiveness and sustainability. Since 1999, when the Baldrige criteria for healthcare were first introduced, 116 healthcare organizations have applied.
The Beginning
According to, Katie Harrelson, RN, vice president of Patient Care Services and chief nurse executive, Bronson has always strived to be the best. In the late 1990s, they began looking at various quality models, and discovered the Baldrige Criteria.
“We began using the criteria because they provided a focus, or framework, to help us define who we are,” says Harrelson. “Physicians became partners, and patients are our customers. Bronson’s hospitalists are strong partners, and our relationship with them is great. It had to be in order to standardize care practices and continue our efforts to be a national leader in healthcare quality.”
She describes the organization’s three strategic objectives: clinical excellence, customer and service excellence, and corporate effectiveness. These “3 Cs” provide focus for Bronson and that are on the tip of all employees’ tongues.
As Bronson embarked on the journey to excellence, it already employed hospitalists. “Bronson started using hospitalists at a time when many of the community’s primary care physicians were older and retiring, or looking for an alternative admission method,” says Scott Larson, MD, senior vice president Medical Affairs and chief medical officer, “There were economic pressures, too. It’s less efficient for individual practitioners to conduct hospital rounds for a small number of patients than to use hospitalists, and hospitalists are more familiar with hospital protocol.”
By 2003 Bronson was continuing to integrate hospitalists into their program, and hospitalists were employing the precepts of performance improvement like other Bronson employees.
Excellence requires, among other things, good communication and unprecedented cooperation. Thus, employees from different departments and disciplines needed to identify new ways to improve existing care processes and work together as a multidisciplinary team. Hospitalists had a unique role that led to several changes.
“Hospitalists are involved in pretty much anything that happens at Bronson,” says Hussein Akl, MD, medical director for Bronson’s Hospitalist Service.
It was that involvement that led Bronson to change its approach to hip fracture care. Previously, the surgeon managed the hip fracture patient from admission to discharge. Bronson’s hospitalists proposed a new model, however: The hospitalists would manage the patient medically, leaving the surgeons to focus on what they do best: repairing the hip.
The success of the program is measured in clinical outcomes; length of stay has declined significantly since the specialists began collaborating in this way. In 2005 HealthGrades, an organization located in Golden, Colo., that rates care in 5,000 U.S. hospitals, awarded Bronson its highest rating (five stars) for hip replacement surgery and for treatment of acute myocardial infarction.
Hospitalists also took the lead in preparing for Primary Stroke Center Certification, a status Bronson achieved from the Joint Commission on Accreditation of Healthcare Organizations last year, and are leading physician engagement in Bronson’s computerized physician order entry project.
Dr. Larson emphasizes that achieving a level of excellence that meets Baldrige standards requires alignment, meaning that organizational, department or service, and individual performance goals must be congruent. Dr. Akl concurs: “Hospitalists had to align with our orthopedists to improve hip fracture care, and with neurologists on stroke.”
This level of excellence also requires constant vigilance and measurement, which is why Bronson uses scorecards to follow core indicators that reflect compliance with best practices for conditions like heart failure, and community acquired pneumonia. They also track their risk-adjusted Medicare mortality rate, which at 3.5% in 2005 was better than their 2004 rate (4.8%) and considerably better than the national average. Scorecards are distributed electronically and discussed in all meetings. Targets established at the beginning of the year are reviewed, and the hospitalist service’s performance is examined and compared with aggregate data for other admitting physicians. Management acknowledges that drilling data down to the individual level—except in rare cases—is often difficult and does not necessarily reflect an individual’s true performance.
“Patients are co-managed often, making individual provider data somewhat misleading,” explains Dr. Larson.
If recruitment and retention are an indication of employee satisfaction, Bronson’s hospitalists are satisfied. Few hospitalists have left; however, one hospitalist who left returned a year later citing Bronson’s well-structured program, the fact that all hospitalists have equal decision-making authority, and physician-based care (Bronson does not use physician extenders) as re-employment incentives.
“Of course, he said the pay was good, too,” quips Dr. Akl. At Bronson, results are rewarded and recognized generously.
The Patient’s Perspective
Bronson’s approach to hospital care translates into distinct differences—from the moment patients enter until discharge. Also recognized internationally as a Pebble Project Partner, Bronson’s facility design proves that function follows form. (See “The Pebble Project,” p. 39.) The building has a first-class hotel feel to it, with well-planned spaces and indoor gardens. Staff emphasizes privacy and service—not just care. Acknowledging that patients have needs and responsibilities outside the hospital that don’t pause while they are admitted, Bronson offers amenities such as wireless computers so patients can stay connected to their lives, beepers so family members can leave a surgical waiting area without fear of missing the surgeon’s post-operative visit, 24-hour room service, and a concierge to run errands or quarterback problems.
Increasingly evidence links architectural design to outcomes in many healthcare settings, and Bronson has acted on the evidence. The hospital is easy to navigate, and because a major building campaign finished this facility in 2000 every patient room is private with its own hand-washing station. Patients needn’t worry about a roommate’s noisy guest or snoring, but, more importantly, private rooms are associated with lower nosocomial infection rates and speedier recovery.
Operating and labor costs are also lower because patients are not transferred as often. At Bronson, infection rates fell 11% overall compared with the rate in their former facility that had a combination of private and semi-private rooms.
Bronson continues to monitor infection rates and also tracks employee turnover, outcome measures, length of stay, cost per unit of service, waiting times, patient satisfaction levels, nosocomial infection rates, and organizational behaviors.
Sharing Caring
Bronson’s hospitalists actively engage in information sharing. They share their protocols within the Bronson healthcare system and with other hospitals and providers. One recent project has been the successful effort to improve the discharge process—an area of emphasis for many quality-promoting oversight organizations and other facilities. Their next step is to automate their interventions.
Some also participate in a half-day Physician Leadership Academy, a gathering held quarterly to develop physician leadership skills and collaborate on identifying and implementing best practices.
Because Bronson’s overall atmosphere and organizational culture differ from older facilities or less avant-garde organizations, Harrelson, Dr. Larson, and Dr. Akl have difficulty identifying one unit where care might be considerably different than what the patient would receive elsewhere. Dr. Akl says that the hospitalists as a group discussed this question and determined that all Bronson units are held to the same high standards, but that the Adult Medical Unit (AMU) is an interesting model for serving the geriatric population.
In the AMU hospitalists lead the team to reach desirable outcomes. The unit’s propensity to admit elderly patients created unique needs that staff has met in correspondingly unique ways. Nursing’s commitment and capability is evident because all AMU nurses are NICHE (Nurses Improving Care for Health System Elders) certified. NICHE certification promotes systematic nursing change that ensures sensitive and exemplary patient-centered care for older patients. The hospitalists, too, have participated in this cultural change and created a protocol that anticipates elderly patients’ needs, and all hospitalists rotate through AMU to support this part of the continuum of care.
The Outcomes
Bronson measures everything, and uses established best practices, benchmarks, and data to ensure that they meet and exceed national standards. They monitor clinical excellence using Centers for Medicare and Medicaid Services performance rates, Blue Cross Blue Shield targets, and the CareScience (Philadelphia) database. They also follow the JCAHO standards and Leapfrog Groups’ National Quality Forum’s measures.
They monitor patient satisfaction using Gallup Polls and “listen and learn” methods that build on the idea that the customer’s opinion and experience is often more valuable than that of an outside consultant. And, they monitor corporate effectiveness using tools that measure employee learning, vacancy rates, and commitment to the environment and the community.
Bronson’s persistence and desire to be the best has paid off. Patients receive beta-blockers and pre-surgical antibiotics at rates that exceed best practice. They have significantly reduced the incidence of ventilator-acquired pneumonia in all ICUs—the pediatric ICU has had none since 2004. Patient satisfaction increased from an already high 95% in 2002 to an astounding 97% in 2004.
For the past three years, Bronson has been named by Fortune and Working Mother magazines as one of the nation’s 100 best companies to work for. They have also been named by Solucient as one of the 100 Top Hospitals in the United States for 2005. Another acknowledgment is the Environmental Leadership Award from Hospitals for a Healthy Environment for reducing waste and pollution. The list of their achievements and awards is seemingly endless, but so too is their energy to continue to improve and deliver excellent care.
Bronson’s approach is what it takes to earn that ultimate recognition of quality: the Malcolm Baldrige National Quality Award. TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.