User login
Dieting and Gout: Intensive Weight Loss Not Especially Helpful for Symptoms
TOPLINE:
An intensive weight loss program is safe for individuals with gout and obesity but does not ease gout symptoms compared with a “control diet” with basic nutritional counseling.
METHODOLOGY:
- Weight loss is recommended as a gout management strategy, despite little clinical evidence.
- Researchers recruited 61 patients with gout and obesity to participate in a 16-week, randomized, nonblinded, parallel-group trial in Denmark.
- A total of 29 participants were assigned to an intensive, low-calorie diet with provided meal replacements.
- Another 32 participants were assigned to the “control diet” with basic nutritional counseling.
TAKEAWAY:
- Patients in the intensive group lost more weight (−15.4 kg/34 lbs) than those the control group (−7.7 kg/17 lbs).
- There were no differences in pain, fatigue, or gout flares between the two groups.
- Weight loss was associated with reduction in serum urate (SU).
- Patients in the intervention group had a numerically larger mean SU change (−0.6 mg/dL) than the control group (−0.3 mg/dL), but this difference was not statistically significant.
IN PRACTICE:
Weight loss can lower SU levels, but this did not translate to improved gout symptoms.
SOURCE:
Robin Christensen, PhD, and Kristian Zobbe, MD, PhD, of the Parker Institute at Bispebjerg and Frederiksberg Hospital in Copenhagen, Denmark, were co-first authors of the study, published on January 2, 2024, in Arthritis & Rheumatology.
LIMITATIONS:
The study had a relatively small sample size and short-term intervention period, which may have made it difficult to detect differences between the intervention and control groups. Patients in the control group lost a significant amount of weight, which also affected comparisons between the two groups.
DISCLOSURES:
Several of the authors disclosed financial relationships with pharmaceutical companies. The Parker Institute, which funded the study, is supported by grants from the Oak Foundation and the Danish Rheumatism Association.
A version of this article appeared on Medscape.com.
TOPLINE:
An intensive weight loss program is safe for individuals with gout and obesity but does not ease gout symptoms compared with a “control diet” with basic nutritional counseling.
METHODOLOGY:
- Weight loss is recommended as a gout management strategy, despite little clinical evidence.
- Researchers recruited 61 patients with gout and obesity to participate in a 16-week, randomized, nonblinded, parallel-group trial in Denmark.
- A total of 29 participants were assigned to an intensive, low-calorie diet with provided meal replacements.
- Another 32 participants were assigned to the “control diet” with basic nutritional counseling.
TAKEAWAY:
- Patients in the intensive group lost more weight (−15.4 kg/34 lbs) than those the control group (−7.7 kg/17 lbs).
- There were no differences in pain, fatigue, or gout flares between the two groups.
- Weight loss was associated with reduction in serum urate (SU).
- Patients in the intervention group had a numerically larger mean SU change (−0.6 mg/dL) than the control group (−0.3 mg/dL), but this difference was not statistically significant.
IN PRACTICE:
Weight loss can lower SU levels, but this did not translate to improved gout symptoms.
SOURCE:
Robin Christensen, PhD, and Kristian Zobbe, MD, PhD, of the Parker Institute at Bispebjerg and Frederiksberg Hospital in Copenhagen, Denmark, were co-first authors of the study, published on January 2, 2024, in Arthritis & Rheumatology.
LIMITATIONS:
The study had a relatively small sample size and short-term intervention period, which may have made it difficult to detect differences between the intervention and control groups. Patients in the control group lost a significant amount of weight, which also affected comparisons between the two groups.
DISCLOSURES:
Several of the authors disclosed financial relationships with pharmaceutical companies. The Parker Institute, which funded the study, is supported by grants from the Oak Foundation and the Danish Rheumatism Association.
A version of this article appeared on Medscape.com.
TOPLINE:
An intensive weight loss program is safe for individuals with gout and obesity but does not ease gout symptoms compared with a “control diet” with basic nutritional counseling.
METHODOLOGY:
- Weight loss is recommended as a gout management strategy, despite little clinical evidence.
- Researchers recruited 61 patients with gout and obesity to participate in a 16-week, randomized, nonblinded, parallel-group trial in Denmark.
- A total of 29 participants were assigned to an intensive, low-calorie diet with provided meal replacements.
- Another 32 participants were assigned to the “control diet” with basic nutritional counseling.
TAKEAWAY:
- Patients in the intensive group lost more weight (−15.4 kg/34 lbs) than those the control group (−7.7 kg/17 lbs).
- There were no differences in pain, fatigue, or gout flares between the two groups.
- Weight loss was associated with reduction in serum urate (SU).
- Patients in the intervention group had a numerically larger mean SU change (−0.6 mg/dL) than the control group (−0.3 mg/dL), but this difference was not statistically significant.
IN PRACTICE:
Weight loss can lower SU levels, but this did not translate to improved gout symptoms.
SOURCE:
Robin Christensen, PhD, and Kristian Zobbe, MD, PhD, of the Parker Institute at Bispebjerg and Frederiksberg Hospital in Copenhagen, Denmark, were co-first authors of the study, published on January 2, 2024, in Arthritis & Rheumatology.
LIMITATIONS:
The study had a relatively small sample size and short-term intervention period, which may have made it difficult to detect differences between the intervention and control groups. Patients in the control group lost a significant amount of weight, which also affected comparisons between the two groups.
DISCLOSURES:
Several of the authors disclosed financial relationships with pharmaceutical companies. The Parker Institute, which funded the study, is supported by grants from the Oak Foundation and the Danish Rheumatism Association.
A version of this article appeared on Medscape.com.
Novel Solutions Needed to Attract Residents to Pediatric Rheumatology
Pediatric rheumatologists are calling a “Code (p)RED” — a pediatric rheumatology educational deficit.
There are too few pediatric rheumatologists to meet patient demand in the United States, and projections suggest that gap will continue to widen. Disappointing match trends also reflect issues with recruitment: Since 2019, only 50%-75% of pediatric rheumatology fellowship positions have been filled each year. For 2024, the subspecialty filled 32 of 52 positions.
Lack of exposure during medical school and residency, financial concerns, and a lengthy, research-focused fellowship are seen as major contributors to the workforce shortage, and novel solutions are needed to close the gap, experts argued in a recent presentation at the annual meeting of the American College of Rheumatology.
“It’s so important now to get ahead of this because what I’m afraid of is in 10-20 years, we’re not going to have a field,” Colleen Correll, MD, MPH, an associate professor in the division of pediatric rheumatology at the University of Minnesota Medical School in Minneapolis, told this news organization.
Growing Demand, Falling Supply
Because the subspecialty was officially recognized by the American Board of Pediatrics in 1991, “it’s always been a small group of providers,” Dr. Correll said. “It’s honestly always been a recognized issue in our field.”
But a 2022 report by the ACR on the pediatric workforce has brought more attention to the issue. Dr. Correll led the study and is the chair of ACR›s Pediatric Rheumatology Committee. According to the report, an estimated 287 pediatric rheumatologists were working as full-time clinicians in 2015, while the estimated demand was 382 providers. By 2030, this projected supply of pediatric rheumatologists fell to 261, while demand rose to 461 full-time providers.
The distribution of pediatric rheumatologists is also an issue. It’s generally thought that there should be at least one pediatric rheumatologist per 100,000 children, Dr. Correll explained. According to ACR estimates, the northeast region had approximately 0.83 pediatric rheumatologists per 100,000 in 2015, while the south central and southwest regions had 0.17 and 0.20 providers per 100,000 children, respectively. Projected estimates for 2030 dipped to 0.04 or lower for the south central, southwest, and southeast regions.
A separate study from the American Board of Pediatrics, also led by Dr. Correll, that is still under review offered more optimistic projections, suggesting that there would be a 75% increase in pediatric rheumatologists from 0.27 per 100,000 children in 2020 to 0.47 per 100,000 children in 2040.
“This does look better than the ACR study, though 0.47 is still a really small number and an inadequate number to treat our children in need,” she said during her presentation at the annual meeting of the American College of Rheumatology.
Lack of Exposure During Medical Education
Few medical schools have pediatric rheumatology built into their curriculum, whether that is a whole course or a single lecture, said Jay Mehta, MD, who directs the pediatric rheumatology fellowship at the Children’s Hospital of Philadelphia. Dr. Mehta, for example, did not know that pediatric rheumatology was a field before entering residency, he said. But residencies can also lack exposure: An estimated one third of residencies do not have a single pediatric rheumatologist on staff, he said.

“Those are places where people aren’t necessarily getting exposure to pediatric rheumatology,” he told this news organization, “and we know that if you’re not exposed to a field, it’s very, very unlikely that you will go into that field.”
The ACR’s Pediatric Rheumatology Residency Program is one way that the organization is working to address this issue. The program sends pediatric residents with an interest in rheumatology to the ACR annual meeting. The Rheumatology Research Foundation also runs a visiting professorship program, where a pediatric rheumatologist conducts a rheumatology education forum at an institution with no pediatric rheumatology program.
“I’ve done it a couple of times,” Dr. Mehta said during his presentation at the annual meeting. “It’s one of the most rewarding things I’ve done.”
Financial Concerns
Additionally, although pediatric rheumatology requires more training, these subspecialists will likely make less than their general pediatric colleagues over their career. According to one study in Pediatrics, a pediatric resident pursuing rheumatology is projected to make $1.2 million dollars less over the course of their career compared with someone who started their career in general pediatrics immediately after residency. (Negative financial returns were also found for all pediatric subspecialities except for cardiology, critical care, and neonatology.)
This lower earning potential is likely a deterrent, especially for those with educational debt. In one analysis published in October, medical students with at least $200,000 in education debt were 43% more likely to go into higher-paying pediatric subspecialities than those with no debt. Nearly three out of four medical graduates have education debt, according to the American Association of Medical Colleges, with a median debt of $200,000.
While the Pediatric Specialty Loan Repayment Program was specifically designed to aid pediatric subspecialists with their educational debt, qualifying for the program is difficult for pediatric rheumatologists, explained Kristen N. Hayward, MD, of Seattle Children’s in Washington. The program provides up to $100,000 in loan forgiveness in exchange for 3 years of practicing in an underserved area; however, the program stipulates that providers must provide full-time (40 hours per week) clinical care. At academic institutions, where most pediatric rheumatologists practice, there is usually a research component to their position, and even if a provider works the equivalent of 40 hours per week in a clinic in addition to their research, they don’t qualify for the program, Dr. Hayward said.
“It’s very difficult to find someone who’s actually only doing clinical work,” she said.
The ACR has worked to combat some of these economic constraints by demonstrating the direct and downstream value of rheumatologic care, Dr. Hayward said. In a recent white paper, it was estimated that including office visits, consultations, lab testing, and radiology services, one full-time equivalent rheumatologist generates $3.5 million in revenue every year and saves health systems more than $2700 per patient per year.
In addition to placing greater value on rheumatologic care, the healthcare system also needs to recognize the current nonbillable hours that pediatric rheumatologists spend taking care of patients, Dr. Hayward noted.
Especially with electronic medical records (EMRs) and online communication with patients, “there is increasingly a lot of patient care that happens outside of clinic and that takes a lot of time,” Dr. Hayward said. For example, she spends between 1 and 2 hours every day in the EMR refilling medications and responding to patient concerns, and “that all is done in my spare time,” she said. “That’s not billed to the patient in anyway.”
Length of Fellowship
The pediatric rheumatology fellowship is a 3-year program — like other pediatric subspecialities — with a research requirement. By comparison, adult rheumatology fellowships are 2 years, and fellows can pursue additional research training if they have a strong interest.
“It sounds like just 1 more year, but I think it’s coming at a really pivotal point in people’s lives, and that 1 year can make a huge difference,” Dr. Hayward explained.
The 2 years of research might also be a deterrent for individuals who know they are only interested in clinical work, she added. About half of pediatric subspecialists only pursue clinical work after graduation, according to a recent report by the National Academies of Sciences, Engineering, and Medicine (NASEM) focused on the future pediatric physician workforce.
Additionally, only 17% of pediatric rheumatologists spend more than half of their time in research, said Fred Rivara, MD, MPH, chair of the NASEM report, in a statement included in Dr. Hayward’s ACR presentation. The report, which recommended strategies to bolster the pediatric workforce, argued that the American Board of Pediatrics should develop alternative training pathways, including 2-year, clinically heavy fellowships.
The ACR workforce team is also exploring alternative training models like competency-based education, Dr. Hayward said. The Education in Pediatrics Across the Continuum project is already using this approach from medical school to pediatric residency. While this type of outcome-based program has not been tried at the fellowship level, «this has been done, it could be done, and I think we could learn from our colleagues about how they have done this successfully,» she noted.
Ultimately, Dr. Hayward emphasized that there needs to be a “sea change” to close the workforce gap — with multiple interventions addressing these individual challenges.
“Unless we all pitch in and find one way that we can all move this issue forward, we are going to be drowning in a sea of Epic inbox messages,” she said, “and never get to see the patients we want to see.”
Dr. Hayward previously owned stock/stock options for AbbVie/Abbott, Cigna/Express Scripts, Merck, and Teva and has received an educational grant from Pfizer. Dr. Correll and Dr. Mehta had no relevant disclosures.
A version of this article appeared on Medscape.com.
Pediatric rheumatologists are calling a “Code (p)RED” — a pediatric rheumatology educational deficit.
There are too few pediatric rheumatologists to meet patient demand in the United States, and projections suggest that gap will continue to widen. Disappointing match trends also reflect issues with recruitment: Since 2019, only 50%-75% of pediatric rheumatology fellowship positions have been filled each year. For 2024, the subspecialty filled 32 of 52 positions.
Lack of exposure during medical school and residency, financial concerns, and a lengthy, research-focused fellowship are seen as major contributors to the workforce shortage, and novel solutions are needed to close the gap, experts argued in a recent presentation at the annual meeting of the American College of Rheumatology.
“It’s so important now to get ahead of this because what I’m afraid of is in 10-20 years, we’re not going to have a field,” Colleen Correll, MD, MPH, an associate professor in the division of pediatric rheumatology at the University of Minnesota Medical School in Minneapolis, told this news organization.
Growing Demand, Falling Supply
Because the subspecialty was officially recognized by the American Board of Pediatrics in 1991, “it’s always been a small group of providers,” Dr. Correll said. “It’s honestly always been a recognized issue in our field.”
But a 2022 report by the ACR on the pediatric workforce has brought more attention to the issue. Dr. Correll led the study and is the chair of ACR›s Pediatric Rheumatology Committee. According to the report, an estimated 287 pediatric rheumatologists were working as full-time clinicians in 2015, while the estimated demand was 382 providers. By 2030, this projected supply of pediatric rheumatologists fell to 261, while demand rose to 461 full-time providers.
The distribution of pediatric rheumatologists is also an issue. It’s generally thought that there should be at least one pediatric rheumatologist per 100,000 children, Dr. Correll explained. According to ACR estimates, the northeast region had approximately 0.83 pediatric rheumatologists per 100,000 in 2015, while the south central and southwest regions had 0.17 and 0.20 providers per 100,000 children, respectively. Projected estimates for 2030 dipped to 0.04 or lower for the south central, southwest, and southeast regions.
A separate study from the American Board of Pediatrics, also led by Dr. Correll, that is still under review offered more optimistic projections, suggesting that there would be a 75% increase in pediatric rheumatologists from 0.27 per 100,000 children in 2020 to 0.47 per 100,000 children in 2040.
“This does look better than the ACR study, though 0.47 is still a really small number and an inadequate number to treat our children in need,” she said during her presentation at the annual meeting of the American College of Rheumatology.
Lack of Exposure During Medical Education
Few medical schools have pediatric rheumatology built into their curriculum, whether that is a whole course or a single lecture, said Jay Mehta, MD, who directs the pediatric rheumatology fellowship at the Children’s Hospital of Philadelphia. Dr. Mehta, for example, did not know that pediatric rheumatology was a field before entering residency, he said. But residencies can also lack exposure: An estimated one third of residencies do not have a single pediatric rheumatologist on staff, he said.
“Those are places where people aren’t necessarily getting exposure to pediatric rheumatology,” he told this news organization, “and we know that if you’re not exposed to a field, it’s very, very unlikely that you will go into that field.”
The ACR’s Pediatric Rheumatology Residency Program is one way that the organization is working to address this issue. The program sends pediatric residents with an interest in rheumatology to the ACR annual meeting. The Rheumatology Research Foundation also runs a visiting professorship program, where a pediatric rheumatologist conducts a rheumatology education forum at an institution with no pediatric rheumatology program.
“I’ve done it a couple of times,” Dr. Mehta said during his presentation at the annual meeting. “It’s one of the most rewarding things I’ve done.”
Financial Concerns
Additionally, although pediatric rheumatology requires more training, these subspecialists will likely make less than their general pediatric colleagues over their career. According to one study in Pediatrics, a pediatric resident pursuing rheumatology is projected to make $1.2 million dollars less over the course of their career compared with someone who started their career in general pediatrics immediately after residency. (Negative financial returns were also found for all pediatric subspecialities except for cardiology, critical care, and neonatology.)
This lower earning potential is likely a deterrent, especially for those with educational debt. In one analysis published in October, medical students with at least $200,000 in education debt were 43% more likely to go into higher-paying pediatric subspecialities than those with no debt. Nearly three out of four medical graduates have education debt, according to the American Association of Medical Colleges, with a median debt of $200,000.
While the Pediatric Specialty Loan Repayment Program was specifically designed to aid pediatric subspecialists with their educational debt, qualifying for the program is difficult for pediatric rheumatologists, explained Kristen N. Hayward, MD, of Seattle Children’s in Washington. The program provides up to $100,000 in loan forgiveness in exchange for 3 years of practicing in an underserved area; however, the program stipulates that providers must provide full-time (40 hours per week) clinical care. At academic institutions, where most pediatric rheumatologists practice, there is usually a research component to their position, and even if a provider works the equivalent of 40 hours per week in a clinic in addition to their research, they don’t qualify for the program, Dr. Hayward said.
“It’s very difficult to find someone who’s actually only doing clinical work,” she said.
The ACR has worked to combat some of these economic constraints by demonstrating the direct and downstream value of rheumatologic care, Dr. Hayward said. In a recent white paper, it was estimated that including office visits, consultations, lab testing, and radiology services, one full-time equivalent rheumatologist generates $3.5 million in revenue every year and saves health systems more than $2700 per patient per year.
In addition to placing greater value on rheumatologic care, the healthcare system also needs to recognize the current nonbillable hours that pediatric rheumatologists spend taking care of patients, Dr. Hayward noted.
Especially with electronic medical records (EMRs) and online communication with patients, “there is increasingly a lot of patient care that happens outside of clinic and that takes a lot of time,” Dr. Hayward said. For example, she spends between 1 and 2 hours every day in the EMR refilling medications and responding to patient concerns, and “that all is done in my spare time,” she said. “That’s not billed to the patient in anyway.”
Length of Fellowship
The pediatric rheumatology fellowship is a 3-year program — like other pediatric subspecialities — with a research requirement. By comparison, adult rheumatology fellowships are 2 years, and fellows can pursue additional research training if they have a strong interest.
“It sounds like just 1 more year, but I think it’s coming at a really pivotal point in people’s lives, and that 1 year can make a huge difference,” Dr. Hayward explained.
The 2 years of research might also be a deterrent for individuals who know they are only interested in clinical work, she added. About half of pediatric subspecialists only pursue clinical work after graduation, according to a recent report by the National Academies of Sciences, Engineering, and Medicine (NASEM) focused on the future pediatric physician workforce.
Additionally, only 17% of pediatric rheumatologists spend more than half of their time in research, said Fred Rivara, MD, MPH, chair of the NASEM report, in a statement included in Dr. Hayward’s ACR presentation. The report, which recommended strategies to bolster the pediatric workforce, argued that the American Board of Pediatrics should develop alternative training pathways, including 2-year, clinically heavy fellowships.
The ACR workforce team is also exploring alternative training models like competency-based education, Dr. Hayward said. The Education in Pediatrics Across the Continuum project is already using this approach from medical school to pediatric residency. While this type of outcome-based program has not been tried at the fellowship level, «this has been done, it could be done, and I think we could learn from our colleagues about how they have done this successfully,» she noted.
Ultimately, Dr. Hayward emphasized that there needs to be a “sea change” to close the workforce gap — with multiple interventions addressing these individual challenges.
“Unless we all pitch in and find one way that we can all move this issue forward, we are going to be drowning in a sea of Epic inbox messages,” she said, “and never get to see the patients we want to see.”
Dr. Hayward previously owned stock/stock options for AbbVie/Abbott, Cigna/Express Scripts, Merck, and Teva and has received an educational grant from Pfizer. Dr. Correll and Dr. Mehta had no relevant disclosures.
A version of this article appeared on Medscape.com.
Pediatric rheumatologists are calling a “Code (p)RED” — a pediatric rheumatology educational deficit.
There are too few pediatric rheumatologists to meet patient demand in the United States, and projections suggest that gap will continue to widen. Disappointing match trends also reflect issues with recruitment: Since 2019, only 50%-75% of pediatric rheumatology fellowship positions have been filled each year. For 2024, the subspecialty filled 32 of 52 positions.
Lack of exposure during medical school and residency, financial concerns, and a lengthy, research-focused fellowship are seen as major contributors to the workforce shortage, and novel solutions are needed to close the gap, experts argued in a recent presentation at the annual meeting of the American College of Rheumatology.
“It’s so important now to get ahead of this because what I’m afraid of is in 10-20 years, we’re not going to have a field,” Colleen Correll, MD, MPH, an associate professor in the division of pediatric rheumatology at the University of Minnesota Medical School in Minneapolis, told this news organization.
Growing Demand, Falling Supply
Because the subspecialty was officially recognized by the American Board of Pediatrics in 1991, “it’s always been a small group of providers,” Dr. Correll said. “It’s honestly always been a recognized issue in our field.”
But a 2022 report by the ACR on the pediatric workforce has brought more attention to the issue. Dr. Correll led the study and is the chair of ACR›s Pediatric Rheumatology Committee. According to the report, an estimated 287 pediatric rheumatologists were working as full-time clinicians in 2015, while the estimated demand was 382 providers. By 2030, this projected supply of pediatric rheumatologists fell to 261, while demand rose to 461 full-time providers.
The distribution of pediatric rheumatologists is also an issue. It’s generally thought that there should be at least one pediatric rheumatologist per 100,000 children, Dr. Correll explained. According to ACR estimates, the northeast region had approximately 0.83 pediatric rheumatologists per 100,000 in 2015, while the south central and southwest regions had 0.17 and 0.20 providers per 100,000 children, respectively. Projected estimates for 2030 dipped to 0.04 or lower for the south central, southwest, and southeast regions.
A separate study from the American Board of Pediatrics, also led by Dr. Correll, that is still under review offered more optimistic projections, suggesting that there would be a 75% increase in pediatric rheumatologists from 0.27 per 100,000 children in 2020 to 0.47 per 100,000 children in 2040.
“This does look better than the ACR study, though 0.47 is still a really small number and an inadequate number to treat our children in need,” she said during her presentation at the annual meeting of the American College of Rheumatology.
Lack of Exposure During Medical Education
Few medical schools have pediatric rheumatology built into their curriculum, whether that is a whole course or a single lecture, said Jay Mehta, MD, who directs the pediatric rheumatology fellowship at the Children’s Hospital of Philadelphia. Dr. Mehta, for example, did not know that pediatric rheumatology was a field before entering residency, he said. But residencies can also lack exposure: An estimated one third of residencies do not have a single pediatric rheumatologist on staff, he said.
“Those are places where people aren’t necessarily getting exposure to pediatric rheumatology,” he told this news organization, “and we know that if you’re not exposed to a field, it’s very, very unlikely that you will go into that field.”
The ACR’s Pediatric Rheumatology Residency Program is one way that the organization is working to address this issue. The program sends pediatric residents with an interest in rheumatology to the ACR annual meeting. The Rheumatology Research Foundation also runs a visiting professorship program, where a pediatric rheumatologist conducts a rheumatology education forum at an institution with no pediatric rheumatology program.
“I’ve done it a couple of times,” Dr. Mehta said during his presentation at the annual meeting. “It’s one of the most rewarding things I’ve done.”
Financial Concerns
Additionally, although pediatric rheumatology requires more training, these subspecialists will likely make less than their general pediatric colleagues over their career. According to one study in Pediatrics, a pediatric resident pursuing rheumatology is projected to make $1.2 million dollars less over the course of their career compared with someone who started their career in general pediatrics immediately after residency. (Negative financial returns were also found for all pediatric subspecialities except for cardiology, critical care, and neonatology.)
This lower earning potential is likely a deterrent, especially for those with educational debt. In one analysis published in October, medical students with at least $200,000 in education debt were 43% more likely to go into higher-paying pediatric subspecialities than those with no debt. Nearly three out of four medical graduates have education debt, according to the American Association of Medical Colleges, with a median debt of $200,000.
While the Pediatric Specialty Loan Repayment Program was specifically designed to aid pediatric subspecialists with their educational debt, qualifying for the program is difficult for pediatric rheumatologists, explained Kristen N. Hayward, MD, of Seattle Children’s in Washington. The program provides up to $100,000 in loan forgiveness in exchange for 3 years of practicing in an underserved area; however, the program stipulates that providers must provide full-time (40 hours per week) clinical care. At academic institutions, where most pediatric rheumatologists practice, there is usually a research component to their position, and even if a provider works the equivalent of 40 hours per week in a clinic in addition to their research, they don’t qualify for the program, Dr. Hayward said.
“It’s very difficult to find someone who’s actually only doing clinical work,” she said.
The ACR has worked to combat some of these economic constraints by demonstrating the direct and downstream value of rheumatologic care, Dr. Hayward said. In a recent white paper, it was estimated that including office visits, consultations, lab testing, and radiology services, one full-time equivalent rheumatologist generates $3.5 million in revenue every year and saves health systems more than $2700 per patient per year.
In addition to placing greater value on rheumatologic care, the healthcare system also needs to recognize the current nonbillable hours that pediatric rheumatologists spend taking care of patients, Dr. Hayward noted.
Especially with electronic medical records (EMRs) and online communication with patients, “there is increasingly a lot of patient care that happens outside of clinic and that takes a lot of time,” Dr. Hayward said. For example, she spends between 1 and 2 hours every day in the EMR refilling medications and responding to patient concerns, and “that all is done in my spare time,” she said. “That’s not billed to the patient in anyway.”
Length of Fellowship
The pediatric rheumatology fellowship is a 3-year program — like other pediatric subspecialities — with a research requirement. By comparison, adult rheumatology fellowships are 2 years, and fellows can pursue additional research training if they have a strong interest.
“It sounds like just 1 more year, but I think it’s coming at a really pivotal point in people’s lives, and that 1 year can make a huge difference,” Dr. Hayward explained.
The 2 years of research might also be a deterrent for individuals who know they are only interested in clinical work, she added. About half of pediatric subspecialists only pursue clinical work after graduation, according to a recent report by the National Academies of Sciences, Engineering, and Medicine (NASEM) focused on the future pediatric physician workforce.
Additionally, only 17% of pediatric rheumatologists spend more than half of their time in research, said Fred Rivara, MD, MPH, chair of the NASEM report, in a statement included in Dr. Hayward’s ACR presentation. The report, which recommended strategies to bolster the pediatric workforce, argued that the American Board of Pediatrics should develop alternative training pathways, including 2-year, clinically heavy fellowships.
The ACR workforce team is also exploring alternative training models like competency-based education, Dr. Hayward said. The Education in Pediatrics Across the Continuum project is already using this approach from medical school to pediatric residency. While this type of outcome-based program has not been tried at the fellowship level, «this has been done, it could be done, and I think we could learn from our colleagues about how they have done this successfully,» she noted.
Ultimately, Dr. Hayward emphasized that there needs to be a “sea change” to close the workforce gap — with multiple interventions addressing these individual challenges.
“Unless we all pitch in and find one way that we can all move this issue forward, we are going to be drowning in a sea of Epic inbox messages,” she said, “and never get to see the patients we want to see.”
Dr. Hayward previously owned stock/stock options for AbbVie/Abbott, Cigna/Express Scripts, Merck, and Teva and has received an educational grant from Pfizer. Dr. Correll and Dr. Mehta had no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM ACR 2023
Teen and young adult rheumatology patients report gaps in sexual health counseling
SAN DIEGO — Only half of teens and young adults on teratogenic medication report being asked about sexual activity by their rheumatologist, and 38% did not know that their medication would be harmful to a fetus, according to a new survey.
While pediatric rheumatology providers may think that health screenings and contraceptive counseling are happening elsewhere, “this study suggests that a lot of patients are being missed, including those on teratogens,” noted Brittany M. Huynh, MD, MPH, a pediatric rheumatology fellow at the Indiana University School of Medicine in Indianapolis. She led the study and presented the findings at the American College of Rheumatology annual meeting.
For the study, Dr. Huynh and colleagues recruited patients aged 14-23 years who were assigned female at birth and were followed at pediatric rheumatology clinics affiliated with Indiana University. Participants completed a one-time survey between October 2020 and July 2022 and were asked about their sexual reproductive health experience and knowledge. Notably, all but four surveys were completed prior to the US Supreme Court Dobbs decision overturning Roe v. Wade.
Of responses from 108 participants, the most common diagnoses were juvenile idiopathic arthritis (52%) and systemic lupus erythematosus (16%). About one third (36%) of patients were on teratogenic medication, with the most common being methotrexate. About three fourths (76%) were White, and the average age of respondents was 16.7.
Most participants (82%) said they had been asked about sexual activity by a health care provider, but only 38% said their pediatric rheumatologist discussed this topic with them. Of the 39 patients on teratogenic medication, 54% said they had been asked about sexual activity by their pediatric rheumatologist, and only 51% said they had received teratogenicity counseling.
A larger percentage (85%) of this group reported receiving sexual activity screenings by any provider, but there was little difference in counseling about teratogenic medication.
This suggests that this type of risk counseling “is almost exclusively done by (pediatric rheumatologists), if at all,” Dr. Huynh noted during her presentation.
In total, 56% of all patients said a provider had talked to them about how to prevent pregnancy, and 20% said they had been counseled about how to get and use emergency contraception. Only 6% of patients said their pediatric rheumatologist had discussed emergency contraception during appointments.
Although sexual activity screenings were associated with current teratogen use, pregnancy prevention counseling and emergency contraceptive counseling were not associated with teratogen use or reported sexual activity.
The survey also revealed that there were gaps in knowledge about the health effects of rheumatic medication. Of the patients on teratogens, 38% did not know that their medication could harm a fetus if they became pregnant. Only 9% of patients not on teratogens correctly answered that their medication would not harm a fetus.
Previous studies have also shown that rheumatology patients do not know that their medications can be teratogenic, noted Cuoghi Edens, MD, a rheumatologist at the University of Chicago, who sees both adult and pediatric patients. She was not involved with the study. The larger challenge is how to best educate patients, she said.
While hopefully a patient’s primary care provider is discussing these issues with them, these patients often see their rheumatologist more frequently and more consistently than other providers, Dr. Edens said.
“We are sometimes the continuity of care for the patient versus their primary care, even though it should be a group effort of trying to some of these questions,” she said.
Conducting reproductive health screenings in pediatric rheumatology clinics can be difficult though, Dr. Edens noted, not only because of time constraints but also because parents often attend appointments with their child and likely have been for years. These screenings are most accurate when done one-on-one, so pivoting and removing the parents from the room can be awkward for providers, Dr. Edens said.
She advised that starting these conversations early on can be one way to ease into talking about reproductive health. In her own practice, Dr. Huynh sets aside time during appointments to speak with adolescent patients privately.
“We always discuss teratogenic medication. I always talk to them about the fact that I’m going to be doing pregnancy testing with their other screening labs because of the risks associated,” she said. “I also specifically set time aside for patients on teratogens to talk about emergency contraception and offer a prescription, if they’re interested.”
Dr. Huynh emphasized that providing easy access to emergency contraception is key. The ACR reproductive health guidelines — although geared toward adults — recommend discussing emergency contraception with patients, and Dr. Huynh advocates writing prescriptions for interested patients.
“They can fill it and have it easily accessible, so that there are no additional barriers, particularly for people who have these higher risks,” she said.
While emergency contraceptives are also available over the counter, it can be awkward for young people to ask for them, she said, and they can be expensive if not covered under insurance. Providing a prescription is one way to avoid those issues, Dr. Huynh said.
“Certainly, you have to have some parent buy-in, because if there is going to be a script, it’s probably going to be under insurance,” she said. “But in my experience, parents are happy to have it around as long as you’re talking it through with them as well as the young person.”
Dr. Huynh and Dr. Edens had no disclosures.
A version of this article appeared on Medscape.com.
SAN DIEGO — Only half of teens and young adults on teratogenic medication report being asked about sexual activity by their rheumatologist, and 38% did not know that their medication would be harmful to a fetus, according to a new survey.
While pediatric rheumatology providers may think that health screenings and contraceptive counseling are happening elsewhere, “this study suggests that a lot of patients are being missed, including those on teratogens,” noted Brittany M. Huynh, MD, MPH, a pediatric rheumatology fellow at the Indiana University School of Medicine in Indianapolis. She led the study and presented the findings at the American College of Rheumatology annual meeting.
For the study, Dr. Huynh and colleagues recruited patients aged 14-23 years who were assigned female at birth and were followed at pediatric rheumatology clinics affiliated with Indiana University. Participants completed a one-time survey between October 2020 and July 2022 and were asked about their sexual reproductive health experience and knowledge. Notably, all but four surveys were completed prior to the US Supreme Court Dobbs decision overturning Roe v. Wade.
Of responses from 108 participants, the most common diagnoses were juvenile idiopathic arthritis (52%) and systemic lupus erythematosus (16%). About one third (36%) of patients were on teratogenic medication, with the most common being methotrexate. About three fourths (76%) were White, and the average age of respondents was 16.7.
Most participants (82%) said they had been asked about sexual activity by a health care provider, but only 38% said their pediatric rheumatologist discussed this topic with them. Of the 39 patients on teratogenic medication, 54% said they had been asked about sexual activity by their pediatric rheumatologist, and only 51% said they had received teratogenicity counseling.
A larger percentage (85%) of this group reported receiving sexual activity screenings by any provider, but there was little difference in counseling about teratogenic medication.
This suggests that this type of risk counseling “is almost exclusively done by (pediatric rheumatologists), if at all,” Dr. Huynh noted during her presentation.
In total, 56% of all patients said a provider had talked to them about how to prevent pregnancy, and 20% said they had been counseled about how to get and use emergency contraception. Only 6% of patients said their pediatric rheumatologist had discussed emergency contraception during appointments.
Although sexual activity screenings were associated with current teratogen use, pregnancy prevention counseling and emergency contraceptive counseling were not associated with teratogen use or reported sexual activity.
The survey also revealed that there were gaps in knowledge about the health effects of rheumatic medication. Of the patients on teratogens, 38% did not know that their medication could harm a fetus if they became pregnant. Only 9% of patients not on teratogens correctly answered that their medication would not harm a fetus.
Previous studies have also shown that rheumatology patients do not know that their medications can be teratogenic, noted Cuoghi Edens, MD, a rheumatologist at the University of Chicago, who sees both adult and pediatric patients. She was not involved with the study. The larger challenge is how to best educate patients, she said.
While hopefully a patient’s primary care provider is discussing these issues with them, these patients often see their rheumatologist more frequently and more consistently than other providers, Dr. Edens said.
“We are sometimes the continuity of care for the patient versus their primary care, even though it should be a group effort of trying to some of these questions,” she said.
Conducting reproductive health screenings in pediatric rheumatology clinics can be difficult though, Dr. Edens noted, not only because of time constraints but also because parents often attend appointments with their child and likely have been for years. These screenings are most accurate when done one-on-one, so pivoting and removing the parents from the room can be awkward for providers, Dr. Edens said.
She advised that starting these conversations early on can be one way to ease into talking about reproductive health. In her own practice, Dr. Huynh sets aside time during appointments to speak with adolescent patients privately.
“We always discuss teratogenic medication. I always talk to them about the fact that I’m going to be doing pregnancy testing with their other screening labs because of the risks associated,” she said. “I also specifically set time aside for patients on teratogens to talk about emergency contraception and offer a prescription, if they’re interested.”
Dr. Huynh emphasized that providing easy access to emergency contraception is key. The ACR reproductive health guidelines — although geared toward adults — recommend discussing emergency contraception with patients, and Dr. Huynh advocates writing prescriptions for interested patients.
“They can fill it and have it easily accessible, so that there are no additional barriers, particularly for people who have these higher risks,” she said.
While emergency contraceptives are also available over the counter, it can be awkward for young people to ask for them, she said, and they can be expensive if not covered under insurance. Providing a prescription is one way to avoid those issues, Dr. Huynh said.
“Certainly, you have to have some parent buy-in, because if there is going to be a script, it’s probably going to be under insurance,” she said. “But in my experience, parents are happy to have it around as long as you’re talking it through with them as well as the young person.”
Dr. Huynh and Dr. Edens had no disclosures.
A version of this article appeared on Medscape.com.
SAN DIEGO — Only half of teens and young adults on teratogenic medication report being asked about sexual activity by their rheumatologist, and 38% did not know that their medication would be harmful to a fetus, according to a new survey.
While pediatric rheumatology providers may think that health screenings and contraceptive counseling are happening elsewhere, “this study suggests that a lot of patients are being missed, including those on teratogens,” noted Brittany M. Huynh, MD, MPH, a pediatric rheumatology fellow at the Indiana University School of Medicine in Indianapolis. She led the study and presented the findings at the American College of Rheumatology annual meeting.
For the study, Dr. Huynh and colleagues recruited patients aged 14-23 years who were assigned female at birth and were followed at pediatric rheumatology clinics affiliated with Indiana University. Participants completed a one-time survey between October 2020 and July 2022 and were asked about their sexual reproductive health experience and knowledge. Notably, all but four surveys were completed prior to the US Supreme Court Dobbs decision overturning Roe v. Wade.
Of responses from 108 participants, the most common diagnoses were juvenile idiopathic arthritis (52%) and systemic lupus erythematosus (16%). About one third (36%) of patients were on teratogenic medication, with the most common being methotrexate. About three fourths (76%) were White, and the average age of respondents was 16.7.
Most participants (82%) said they had been asked about sexual activity by a health care provider, but only 38% said their pediatric rheumatologist discussed this topic with them. Of the 39 patients on teratogenic medication, 54% said they had been asked about sexual activity by their pediatric rheumatologist, and only 51% said they had received teratogenicity counseling.
A larger percentage (85%) of this group reported receiving sexual activity screenings by any provider, but there was little difference in counseling about teratogenic medication.
This suggests that this type of risk counseling “is almost exclusively done by (pediatric rheumatologists), if at all,” Dr. Huynh noted during her presentation.
In total, 56% of all patients said a provider had talked to them about how to prevent pregnancy, and 20% said they had been counseled about how to get and use emergency contraception. Only 6% of patients said their pediatric rheumatologist had discussed emergency contraception during appointments.
Although sexual activity screenings were associated with current teratogen use, pregnancy prevention counseling and emergency contraceptive counseling were not associated with teratogen use or reported sexual activity.
The survey also revealed that there were gaps in knowledge about the health effects of rheumatic medication. Of the patients on teratogens, 38% did not know that their medication could harm a fetus if they became pregnant. Only 9% of patients not on teratogens correctly answered that their medication would not harm a fetus.
Previous studies have also shown that rheumatology patients do not know that their medications can be teratogenic, noted Cuoghi Edens, MD, a rheumatologist at the University of Chicago, who sees both adult and pediatric patients. She was not involved with the study. The larger challenge is how to best educate patients, she said.
While hopefully a patient’s primary care provider is discussing these issues with them, these patients often see their rheumatologist more frequently and more consistently than other providers, Dr. Edens said.
“We are sometimes the continuity of care for the patient versus their primary care, even though it should be a group effort of trying to some of these questions,” she said.
Conducting reproductive health screenings in pediatric rheumatology clinics can be difficult though, Dr. Edens noted, not only because of time constraints but also because parents often attend appointments with their child and likely have been for years. These screenings are most accurate when done one-on-one, so pivoting and removing the parents from the room can be awkward for providers, Dr. Edens said.
She advised that starting these conversations early on can be one way to ease into talking about reproductive health. In her own practice, Dr. Huynh sets aside time during appointments to speak with adolescent patients privately.
“We always discuss teratogenic medication. I always talk to them about the fact that I’m going to be doing pregnancy testing with their other screening labs because of the risks associated,” she said. “I also specifically set time aside for patients on teratogens to talk about emergency contraception and offer a prescription, if they’re interested.”
Dr. Huynh emphasized that providing easy access to emergency contraception is key. The ACR reproductive health guidelines — although geared toward adults — recommend discussing emergency contraception with patients, and Dr. Huynh advocates writing prescriptions for interested patients.
“They can fill it and have it easily accessible, so that there are no additional barriers, particularly for people who have these higher risks,” she said.
While emergency contraceptives are also available over the counter, it can be awkward for young people to ask for them, she said, and they can be expensive if not covered under insurance. Providing a prescription is one way to avoid those issues, Dr. Huynh said.
“Certainly, you have to have some parent buy-in, because if there is going to be a script, it’s probably going to be under insurance,” she said. “But in my experience, parents are happy to have it around as long as you’re talking it through with them as well as the young person.”
Dr. Huynh and Dr. Edens had no disclosures.
A version of this article appeared on Medscape.com.
FROM ACR 2023
COVID vaccination protects B cell–deficient patients through T-cell responses
TOPLINE:
In individuals with low B-cell counts, T cells have enhanced responses to COVID-19 vaccination and may help prevent severe disease after infection.
METHODOLOGY:
- How the immune systems of B cell–deficient patients respond to SARS-CoV-2 infection and vaccination is not fully understood.
- Researchers evaluated anti–SARS-CoV-2 T-cell responses in 33 patients treated with rituximab (RTX), 12 patients with common variable immune deficiency, and 44 controls.
- The study analyzed effector and memory CD4+ and CD8+ T-cell responses to SARS-CoV-2 after infection and vaccination.
TAKEAWAY:
- All B cell–deficient individuals (those treated with RTX or those with a diagnosis of common variable immune deficiency) had increased effector and memory T-cell responses after SARS-CoV-2 vaccination, compared with controls.
- Patients treated with RTX who were vaccinated against COVID-19 had 4.8-fold reduced odds of moderate or severe disease. (These data were not available for patients with common variable immune deficiency.)
- RTX treatment was associated with a decrease in preexisting T-cell immunity in unvaccinated patients, regardless of prior infection with SARS-CoV-2.
- This association was not found in vaccinated patients treated with RTX.
IN PRACTICE:
“[These findings] provide support for vaccination in this vulnerable population and demonstrate the potential benefit of vaccine-induced CD8+ T-cell responses on reducing disease severity from SARS-CoV-2 infection in the absence of spike protein–specific antibodies,” the authors wrote.
SOURCE:
The study was published online on November 29 in Science Translational Medicine. The first author is Reza Zonozi, MD, who conducted the research while at Massachusetts General Hospital, Boston, and is now in private practice in northern Virginia.
LIMITATIONS:
Researchers did not obtain specimens from patients with common variable immune deficiency after SARS-CoV-2 infection. Only a small subset of immunophenotyped participants had subsequent SARS-CoV-2 infection.
DISCLOSURES:
The research was supported by grants from the National Institutes of Health, the Centers for Disease Control and Prevention, the Howard Hughes Medical Institute, the Ragon Institute of Massachusetts General Hospital, Massachusetts Institute of Technology, and Harvard Medical School, the Mark and Lisa Schwartz Foundation and E. Schwartz; the Lambertus Family Foundation; and S. Edgerly and P. Edgerly. Four authors reported relationships with pharmaceutical companies including AbbVie, Bristol-Myers Squibb, Boehringer Ingelheim, Gilead Sciences, Merck, and Pfizer.
A version of this article first appeared on Medscape.com.
TOPLINE:
In individuals with low B-cell counts, T cells have enhanced responses to COVID-19 vaccination and may help prevent severe disease after infection.
METHODOLOGY:
- How the immune systems of B cell–deficient patients respond to SARS-CoV-2 infection and vaccination is not fully understood.
- Researchers evaluated anti–SARS-CoV-2 T-cell responses in 33 patients treated with rituximab (RTX), 12 patients with common variable immune deficiency, and 44 controls.
- The study analyzed effector and memory CD4+ and CD8+ T-cell responses to SARS-CoV-2 after infection and vaccination.
TAKEAWAY:
- All B cell–deficient individuals (those treated with RTX or those with a diagnosis of common variable immune deficiency) had increased effector and memory T-cell responses after SARS-CoV-2 vaccination, compared with controls.
- Patients treated with RTX who were vaccinated against COVID-19 had 4.8-fold reduced odds of moderate or severe disease. (These data were not available for patients with common variable immune deficiency.)
- RTX treatment was associated with a decrease in preexisting T-cell immunity in unvaccinated patients, regardless of prior infection with SARS-CoV-2.
- This association was not found in vaccinated patients treated with RTX.
IN PRACTICE:
“[These findings] provide support for vaccination in this vulnerable population and demonstrate the potential benefit of vaccine-induced CD8+ T-cell responses on reducing disease severity from SARS-CoV-2 infection in the absence of spike protein–specific antibodies,” the authors wrote.
SOURCE:
The study was published online on November 29 in Science Translational Medicine. The first author is Reza Zonozi, MD, who conducted the research while at Massachusetts General Hospital, Boston, and is now in private practice in northern Virginia.
LIMITATIONS:
Researchers did not obtain specimens from patients with common variable immune deficiency after SARS-CoV-2 infection. Only a small subset of immunophenotyped participants had subsequent SARS-CoV-2 infection.
DISCLOSURES:
The research was supported by grants from the National Institutes of Health, the Centers for Disease Control and Prevention, the Howard Hughes Medical Institute, the Ragon Institute of Massachusetts General Hospital, Massachusetts Institute of Technology, and Harvard Medical School, the Mark and Lisa Schwartz Foundation and E. Schwartz; the Lambertus Family Foundation; and S. Edgerly and P. Edgerly. Four authors reported relationships with pharmaceutical companies including AbbVie, Bristol-Myers Squibb, Boehringer Ingelheim, Gilead Sciences, Merck, and Pfizer.
A version of this article first appeared on Medscape.com.
TOPLINE:
In individuals with low B-cell counts, T cells have enhanced responses to COVID-19 vaccination and may help prevent severe disease after infection.
METHODOLOGY:
- How the immune systems of B cell–deficient patients respond to SARS-CoV-2 infection and vaccination is not fully understood.
- Researchers evaluated anti–SARS-CoV-2 T-cell responses in 33 patients treated with rituximab (RTX), 12 patients with common variable immune deficiency, and 44 controls.
- The study analyzed effector and memory CD4+ and CD8+ T-cell responses to SARS-CoV-2 after infection and vaccination.
TAKEAWAY:
- All B cell–deficient individuals (those treated with RTX or those with a diagnosis of common variable immune deficiency) had increased effector and memory T-cell responses after SARS-CoV-2 vaccination, compared with controls.
- Patients treated with RTX who were vaccinated against COVID-19 had 4.8-fold reduced odds of moderate or severe disease. (These data were not available for patients with common variable immune deficiency.)
- RTX treatment was associated with a decrease in preexisting T-cell immunity in unvaccinated patients, regardless of prior infection with SARS-CoV-2.
- This association was not found in vaccinated patients treated with RTX.
IN PRACTICE:
“[These findings] provide support for vaccination in this vulnerable population and demonstrate the potential benefit of vaccine-induced CD8+ T-cell responses on reducing disease severity from SARS-CoV-2 infection in the absence of spike protein–specific antibodies,” the authors wrote.
SOURCE:
The study was published online on November 29 in Science Translational Medicine. The first author is Reza Zonozi, MD, who conducted the research while at Massachusetts General Hospital, Boston, and is now in private practice in northern Virginia.
LIMITATIONS:
Researchers did not obtain specimens from patients with common variable immune deficiency after SARS-CoV-2 infection. Only a small subset of immunophenotyped participants had subsequent SARS-CoV-2 infection.
DISCLOSURES:
The research was supported by grants from the National Institutes of Health, the Centers for Disease Control and Prevention, the Howard Hughes Medical Institute, the Ragon Institute of Massachusetts General Hospital, Massachusetts Institute of Technology, and Harvard Medical School, the Mark and Lisa Schwartz Foundation and E. Schwartz; the Lambertus Family Foundation; and S. Edgerly and P. Edgerly. Four authors reported relationships with pharmaceutical companies including AbbVie, Bristol-Myers Squibb, Boehringer Ingelheim, Gilead Sciences, Merck, and Pfizer.
A version of this article first appeared on Medscape.com.
Rheumatology Match Day results for 2024 follow trends of past years
While adult rheumatology programs continue to have high match rates, pediatric rheumatology programs remain less popular.
The National Residency Matching Program (NRMP) reported on Nov. 29 that rheumatology filled 124 of 127 programs (97.6%), with 273 (98.9%) of 276 positions filled. Comparatively, pediatric rheumatology filled 21 out of 38 programs (55%) and 32 (61.5%) of 52 positions.
This year, the number of programs and positions across all specialties rose by 3%, whereas the number of applications only rose by 0.4% (35 additional applicants).
“The growth of fellowship programs and positions in the Match reflect training opportunities and the future workforce trends of medical subspecialties,” said NRMP President Donna Lamb, DHSc, MBA, BSN, in a statement. “While the increase in applicant numbers did not keep pace with the increase in positions this year, the Match rate for applicants remains strong at 82%.”
In adult rheumatology, matched applicants included 117 MD graduates, 86 foreign applicants, 38 DO graduates, and 32 U.S. citizen international medical graduates. A total of 348 applicants preferred the specialty, and 78% matched to rheumatology, whereas 2% matched to a different specialty. Another 70 applicants (20%) did not match to any program.
In pediatric rheumatology, matched applicants included 23 MD graduates, 6 DO graduates, and 3 foreign applicants. All applicants who preferred pediatric rheumatology matched to a program.
Adult rheumatology was one of several specialties that filled over 95% of positions. The other specialties that matched at that rate were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, critical care medicine, gastroenterology, hematology and oncology, and pulmonary/critical care. Interventional Pulmonology and Oncology was the only specialty to achieve a 100% fill rate.
A version of this article first appeared on Medscape.com.
While adult rheumatology programs continue to have high match rates, pediatric rheumatology programs remain less popular.
The National Residency Matching Program (NRMP) reported on Nov. 29 that rheumatology filled 124 of 127 programs (97.6%), with 273 (98.9%) of 276 positions filled. Comparatively, pediatric rheumatology filled 21 out of 38 programs (55%) and 32 (61.5%) of 52 positions.
This year, the number of programs and positions across all specialties rose by 3%, whereas the number of applications only rose by 0.4% (35 additional applicants).
“The growth of fellowship programs and positions in the Match reflect training opportunities and the future workforce trends of medical subspecialties,” said NRMP President Donna Lamb, DHSc, MBA, BSN, in a statement. “While the increase in applicant numbers did not keep pace with the increase in positions this year, the Match rate for applicants remains strong at 82%.”
In adult rheumatology, matched applicants included 117 MD graduates, 86 foreign applicants, 38 DO graduates, and 32 U.S. citizen international medical graduates. A total of 348 applicants preferred the specialty, and 78% matched to rheumatology, whereas 2% matched to a different specialty. Another 70 applicants (20%) did not match to any program.
In pediatric rheumatology, matched applicants included 23 MD graduates, 6 DO graduates, and 3 foreign applicants. All applicants who preferred pediatric rheumatology matched to a program.
Adult rheumatology was one of several specialties that filled over 95% of positions. The other specialties that matched at that rate were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, critical care medicine, gastroenterology, hematology and oncology, and pulmonary/critical care. Interventional Pulmonology and Oncology was the only specialty to achieve a 100% fill rate.
A version of this article first appeared on Medscape.com.
While adult rheumatology programs continue to have high match rates, pediatric rheumatology programs remain less popular.
The National Residency Matching Program (NRMP) reported on Nov. 29 that rheumatology filled 124 of 127 programs (97.6%), with 273 (98.9%) of 276 positions filled. Comparatively, pediatric rheumatology filled 21 out of 38 programs (55%) and 32 (61.5%) of 52 positions.
This year, the number of programs and positions across all specialties rose by 3%, whereas the number of applications only rose by 0.4% (35 additional applicants).
“The growth of fellowship programs and positions in the Match reflect training opportunities and the future workforce trends of medical subspecialties,” said NRMP President Donna Lamb, DHSc, MBA, BSN, in a statement. “While the increase in applicant numbers did not keep pace with the increase in positions this year, the Match rate for applicants remains strong at 82%.”
In adult rheumatology, matched applicants included 117 MD graduates, 86 foreign applicants, 38 DO graduates, and 32 U.S. citizen international medical graduates. A total of 348 applicants preferred the specialty, and 78% matched to rheumatology, whereas 2% matched to a different specialty. Another 70 applicants (20%) did not match to any program.
In pediatric rheumatology, matched applicants included 23 MD graduates, 6 DO graduates, and 3 foreign applicants. All applicants who preferred pediatric rheumatology matched to a program.
Adult rheumatology was one of several specialties that filled over 95% of positions. The other specialties that matched at that rate were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, critical care medicine, gastroenterology, hematology and oncology, and pulmonary/critical care. Interventional Pulmonology and Oncology was the only specialty to achieve a 100% fill rate.
A version of this article first appeared on Medscape.com.
Telemedicine not yet on par with in-person visits for rheumatology patients
TOPLINE:
Patients report higher satisfaction with in-person rheumatology visits over telemedicine appointments, according to new research.
METHODOLOGY:
- Investigators recruited established patients at rheumatology clinics at two tertiary medical centers (the University of Alabama at Birmingham and the University of California, San Francisco) from August 2021 to November 2022.
- 501 patients were randomly assigned to have in-person or telehealth appointments.
- After their visits, patients rated satisfaction using a 10-point Likert scale.
- The investigators compared the two visit types with regard to high post-visit satisfaction (score of 9 or 10).
TAKEAWAY:
- 90.1% of the patients who received in-person appointments were highly satisfied with their visit, compared with 76.7% of the telemedicine group.
- Nearly half of the telemedicine group (47.7%) said they would prefer an in-person visit for their next appointment, and 55.6% of the in-person group wanted the same type of visit for their next encounter.
- Less than 1 in 5 people in either group said they preferred telemedicine for their next visit.
- There was no difference between the two groups in self-efficacy for managing medications or medication adherence.
IN PRACTICE:
There was high satisfaction in both groups, but patients tended to prefer in-person to telemedicine visits for their rheumatology care.
SOURCE:
The study was presented at the annual meeting of the American College of Rheumatology by lead author Lesley E. Jackson, MD, of the University of Alabama at Birmingham.
LIMITATIONS:
The study population was mostly female (84%) and from one geographic area.
DISCLOSURES:
Funding was provided by the Rheumatology Research Foundation Innovative Research Award. The authors disclosed relationships with AbbVie, AstraZeneca, Gilead, Pfizer, and several other biopharmaceutical companies.
A version of this article first appeared on Medscape.com.
TOPLINE:
Patients report higher satisfaction with in-person rheumatology visits over telemedicine appointments, according to new research.
METHODOLOGY:
- Investigators recruited established patients at rheumatology clinics at two tertiary medical centers (the University of Alabama at Birmingham and the University of California, San Francisco) from August 2021 to November 2022.
- 501 patients were randomly assigned to have in-person or telehealth appointments.
- After their visits, patients rated satisfaction using a 10-point Likert scale.
- The investigators compared the two visit types with regard to high post-visit satisfaction (score of 9 or 10).
TAKEAWAY:
- 90.1% of the patients who received in-person appointments were highly satisfied with their visit, compared with 76.7% of the telemedicine group.
- Nearly half of the telemedicine group (47.7%) said they would prefer an in-person visit for their next appointment, and 55.6% of the in-person group wanted the same type of visit for their next encounter.
- Less than 1 in 5 people in either group said they preferred telemedicine for their next visit.
- There was no difference between the two groups in self-efficacy for managing medications or medication adherence.
IN PRACTICE:
There was high satisfaction in both groups, but patients tended to prefer in-person to telemedicine visits for their rheumatology care.
SOURCE:
The study was presented at the annual meeting of the American College of Rheumatology by lead author Lesley E. Jackson, MD, of the University of Alabama at Birmingham.
LIMITATIONS:
The study population was mostly female (84%) and from one geographic area.
DISCLOSURES:
Funding was provided by the Rheumatology Research Foundation Innovative Research Award. The authors disclosed relationships with AbbVie, AstraZeneca, Gilead, Pfizer, and several other biopharmaceutical companies.
A version of this article first appeared on Medscape.com.
TOPLINE:
Patients report higher satisfaction with in-person rheumatology visits over telemedicine appointments, according to new research.
METHODOLOGY:
- Investigators recruited established patients at rheumatology clinics at two tertiary medical centers (the University of Alabama at Birmingham and the University of California, San Francisco) from August 2021 to November 2022.
- 501 patients were randomly assigned to have in-person or telehealth appointments.
- After their visits, patients rated satisfaction using a 10-point Likert scale.
- The investigators compared the two visit types with regard to high post-visit satisfaction (score of 9 or 10).
TAKEAWAY:
- 90.1% of the patients who received in-person appointments were highly satisfied with their visit, compared with 76.7% of the telemedicine group.
- Nearly half of the telemedicine group (47.7%) said they would prefer an in-person visit for their next appointment, and 55.6% of the in-person group wanted the same type of visit for their next encounter.
- Less than 1 in 5 people in either group said they preferred telemedicine for their next visit.
- There was no difference between the two groups in self-efficacy for managing medications or medication adherence.
IN PRACTICE:
There was high satisfaction in both groups, but patients tended to prefer in-person to telemedicine visits for their rheumatology care.
SOURCE:
The study was presented at the annual meeting of the American College of Rheumatology by lead author Lesley E. Jackson, MD, of the University of Alabama at Birmingham.
LIMITATIONS:
The study population was mostly female (84%) and from one geographic area.
DISCLOSURES:
Funding was provided by the Rheumatology Research Foundation Innovative Research Award. The authors disclosed relationships with AbbVie, AstraZeneca, Gilead, Pfizer, and several other biopharmaceutical companies.
A version of this article first appeared on Medscape.com.
Risks quantified in medically optimized pregnancy with lupus
SAN DIEGO – In pregnant women with systemic lupus erythematosus (SLE), those with ill-timed pregnancies had poorer pregnancy outcomes, including preeclampsia and preterm birth.
Women with autoimmune conditions are at an increased risk for pregnancy complications, including pregnancy loss, preterm delivery, and increased need for cesarean delivery, said Catherine Sims, MD, a rheumatologist at Duke Health in Durham, N.C., who is focused on reproductive rheumatology. “The natural question, both clinically and from a research perspective, is: ‘What can we do in order to mitigate or minimize these complications?’ ” she said during a presentation at the annual meeting of the American College of Rheumatology.
While research suggests that patients who plan their pregnancies during times of well-controlled disease have the “best chances of improved pregnancy outcomes,” Dr. Sims and colleagues wanted to quantify how planning for pregnancy affected reproductive outcomes.
Dr. Sims recruited pregnant women with SLE and assessed if the women were medically optimized for pregnancy, if the pregnancy was intended, or both. Intended pregnancy was assessed by using a validated self-reported survey called the London Measure of Unplanned Pregnancy. Pregnant women were considered “medically optimized” for pregnancy if they were not on teratogenic medication, had continued pregnancy-compatible SLE medications, and had a urine protein-creatinine ratio of less than 1 gram in the 6 months prior to or during the first trimester. Intended pregnancies that were medically optimized were classified as “well timed.”
Of the 115 women enrolled in the study, about half had well-timed pregnancies, 20% were neither intended nor medically optimized, 17% were not intended but medically optimized, and 13% were intended but not medically optimized.
Women with ill-timed pregnancy – either not medically optimized and/or unintended – were generally younger and more likely to be single, on Medicare or Medicaid, and on income of less than $50,000 per year.
Ill-timed pregnancies had higher rates of mycophenolate exposure and higher physician-reported SLE disease activity. While patient-reported SLE activity was higher in patients who were not personally ready for pregnancy, in patients who had an intended pregnancy, there was no difference in self-reported SLE activity between those that were medically optimized and those not medically optimized.
“About a third of our patients are actually underestimating their true disease activity level when they are preparing for pregnancy,” Dr. Sims said. For example, while persistent proteinuria in a patient would drive up physician assessment of disease activity, the patient may not be experiencing any symptoms and is unaware of her condition.
In terms of pregnancy outcomes, women with unintended pregnancies had a 2.5 times higher incidence of preeclampsia, compared with those with intended pregnancies. Patients with unplanned pregnancies were also significantly more likely to experience stillbirth.
Women who were not medically optimized for pregnancy were three times as likely to experience preterm birth and preeclampsia compared with those with optimized pregnancies.
These outcomes drive home the importance of optimizing patients for pregnancy, Dr. Sims said, and effectively communicating this importance to patients, especially when they might not be perceiving their disease activity.
The study’s findings show providers “what we thought we knew, which is that there are some patients that are not as aware of their risk,” commented Lisa R. Sammaritano, MD, Hospital for Special Surgery, New York, who moderated the session where the research was presented. “It brings home the importance of counselling our patients about contraception [as well as] the importance of planning.”
Dr. Sims added that it is “crucial” to make this information easily accessible and digestible to patients. One important resource she mentioned is the HOP-STEP program, which stands for Healthy Outcomes in Pregnancy with SLE Through Education of Providers. The program, directed by researchers at Duke University, is designed to improve pregnancy planning in people with lupus. Direct-to-patient resources are key, she said, as patients can often be nervous to ask about pregnancy planning during appointments.
“They won’t want to bring a pregnancy with me in clinic because they’re afraid I’m just going to say, ‘don’t do it,’ ” Dr. Sims said. “But we are making decisions with the patient. Our patients are not asking for permission, but telling us what they want, and we need to meet them where they are at.”
A version of this article appeared on Medscape.com.
SAN DIEGO – In pregnant women with systemic lupus erythematosus (SLE), those with ill-timed pregnancies had poorer pregnancy outcomes, including preeclampsia and preterm birth.
Women with autoimmune conditions are at an increased risk for pregnancy complications, including pregnancy loss, preterm delivery, and increased need for cesarean delivery, said Catherine Sims, MD, a rheumatologist at Duke Health in Durham, N.C., who is focused on reproductive rheumatology. “The natural question, both clinically and from a research perspective, is: ‘What can we do in order to mitigate or minimize these complications?’ ” she said during a presentation at the annual meeting of the American College of Rheumatology.
While research suggests that patients who plan their pregnancies during times of well-controlled disease have the “best chances of improved pregnancy outcomes,” Dr. Sims and colleagues wanted to quantify how planning for pregnancy affected reproductive outcomes.
Dr. Sims recruited pregnant women with SLE and assessed if the women were medically optimized for pregnancy, if the pregnancy was intended, or both. Intended pregnancy was assessed by using a validated self-reported survey called the London Measure of Unplanned Pregnancy. Pregnant women were considered “medically optimized” for pregnancy if they were not on teratogenic medication, had continued pregnancy-compatible SLE medications, and had a urine protein-creatinine ratio of less than 1 gram in the 6 months prior to or during the first trimester. Intended pregnancies that were medically optimized were classified as “well timed.”
Of the 115 women enrolled in the study, about half had well-timed pregnancies, 20% were neither intended nor medically optimized, 17% were not intended but medically optimized, and 13% were intended but not medically optimized.
Women with ill-timed pregnancy – either not medically optimized and/or unintended – were generally younger and more likely to be single, on Medicare or Medicaid, and on income of less than $50,000 per year.
Ill-timed pregnancies had higher rates of mycophenolate exposure and higher physician-reported SLE disease activity. While patient-reported SLE activity was higher in patients who were not personally ready for pregnancy, in patients who had an intended pregnancy, there was no difference in self-reported SLE activity between those that were medically optimized and those not medically optimized.
“About a third of our patients are actually underestimating their true disease activity level when they are preparing for pregnancy,” Dr. Sims said. For example, while persistent proteinuria in a patient would drive up physician assessment of disease activity, the patient may not be experiencing any symptoms and is unaware of her condition.
In terms of pregnancy outcomes, women with unintended pregnancies had a 2.5 times higher incidence of preeclampsia, compared with those with intended pregnancies. Patients with unplanned pregnancies were also significantly more likely to experience stillbirth.
Women who were not medically optimized for pregnancy were three times as likely to experience preterm birth and preeclampsia compared with those with optimized pregnancies.
These outcomes drive home the importance of optimizing patients for pregnancy, Dr. Sims said, and effectively communicating this importance to patients, especially when they might not be perceiving their disease activity.
The study’s findings show providers “what we thought we knew, which is that there are some patients that are not as aware of their risk,” commented Lisa R. Sammaritano, MD, Hospital for Special Surgery, New York, who moderated the session where the research was presented. “It brings home the importance of counselling our patients about contraception [as well as] the importance of planning.”
Dr. Sims added that it is “crucial” to make this information easily accessible and digestible to patients. One important resource she mentioned is the HOP-STEP program, which stands for Healthy Outcomes in Pregnancy with SLE Through Education of Providers. The program, directed by researchers at Duke University, is designed to improve pregnancy planning in people with lupus. Direct-to-patient resources are key, she said, as patients can often be nervous to ask about pregnancy planning during appointments.
“They won’t want to bring a pregnancy with me in clinic because they’re afraid I’m just going to say, ‘don’t do it,’ ” Dr. Sims said. “But we are making decisions with the patient. Our patients are not asking for permission, but telling us what they want, and we need to meet them where they are at.”
A version of this article appeared on Medscape.com.
SAN DIEGO – In pregnant women with systemic lupus erythematosus (SLE), those with ill-timed pregnancies had poorer pregnancy outcomes, including preeclampsia and preterm birth.
Women with autoimmune conditions are at an increased risk for pregnancy complications, including pregnancy loss, preterm delivery, and increased need for cesarean delivery, said Catherine Sims, MD, a rheumatologist at Duke Health in Durham, N.C., who is focused on reproductive rheumatology. “The natural question, both clinically and from a research perspective, is: ‘What can we do in order to mitigate or minimize these complications?’ ” she said during a presentation at the annual meeting of the American College of Rheumatology.
While research suggests that patients who plan their pregnancies during times of well-controlled disease have the “best chances of improved pregnancy outcomes,” Dr. Sims and colleagues wanted to quantify how planning for pregnancy affected reproductive outcomes.
Dr. Sims recruited pregnant women with SLE and assessed if the women were medically optimized for pregnancy, if the pregnancy was intended, or both. Intended pregnancy was assessed by using a validated self-reported survey called the London Measure of Unplanned Pregnancy. Pregnant women were considered “medically optimized” for pregnancy if they were not on teratogenic medication, had continued pregnancy-compatible SLE medications, and had a urine protein-creatinine ratio of less than 1 gram in the 6 months prior to or during the first trimester. Intended pregnancies that were medically optimized were classified as “well timed.”
Of the 115 women enrolled in the study, about half had well-timed pregnancies, 20% were neither intended nor medically optimized, 17% were not intended but medically optimized, and 13% were intended but not medically optimized.
Women with ill-timed pregnancy – either not medically optimized and/or unintended – were generally younger and more likely to be single, on Medicare or Medicaid, and on income of less than $50,000 per year.
Ill-timed pregnancies had higher rates of mycophenolate exposure and higher physician-reported SLE disease activity. While patient-reported SLE activity was higher in patients who were not personally ready for pregnancy, in patients who had an intended pregnancy, there was no difference in self-reported SLE activity between those that were medically optimized and those not medically optimized.
“About a third of our patients are actually underestimating their true disease activity level when they are preparing for pregnancy,” Dr. Sims said. For example, while persistent proteinuria in a patient would drive up physician assessment of disease activity, the patient may not be experiencing any symptoms and is unaware of her condition.
In terms of pregnancy outcomes, women with unintended pregnancies had a 2.5 times higher incidence of preeclampsia, compared with those with intended pregnancies. Patients with unplanned pregnancies were also significantly more likely to experience stillbirth.
Women who were not medically optimized for pregnancy were three times as likely to experience preterm birth and preeclampsia compared with those with optimized pregnancies.
These outcomes drive home the importance of optimizing patients for pregnancy, Dr. Sims said, and effectively communicating this importance to patients, especially when they might not be perceiving their disease activity.
The study’s findings show providers “what we thought we knew, which is that there are some patients that are not as aware of their risk,” commented Lisa R. Sammaritano, MD, Hospital for Special Surgery, New York, who moderated the session where the research was presented. “It brings home the importance of counselling our patients about contraception [as well as] the importance of planning.”
Dr. Sims added that it is “crucial” to make this information easily accessible and digestible to patients. One important resource she mentioned is the HOP-STEP program, which stands for Healthy Outcomes in Pregnancy with SLE Through Education of Providers. The program, directed by researchers at Duke University, is designed to improve pregnancy planning in people with lupus. Direct-to-patient resources are key, she said, as patients can often be nervous to ask about pregnancy planning during appointments.
“They won’t want to bring a pregnancy with me in clinic because they’re afraid I’m just going to say, ‘don’t do it,’ ” Dr. Sims said. “But we are making decisions with the patient. Our patients are not asking for permission, but telling us what they want, and we need to meet them where they are at.”
A version of this article appeared on Medscape.com.
AT ACR 2023
Telemedicine offers solution for late cancellations and no-show appointments
TOPLINE:
Converting late cancellations and no-show appointments to telemedicine visits increases access to care without the need for rescheduling, according to new research.
METHODOLOGY:
- Investigators identified adult rheumatology patients with late cancellations (within 24 hours of appointment) or impending no-show appointments from September 2020 to March 2023.
- These patients were contacted and were offered the option of converting their in-person appointment to a telemedicine visit, either by phone or video.
- The program was piloted at one clinic beginning Sept. 1, 2020, and was expanded to a second clinic on Sept. 1, 2021.
TAKEAWAY:
- Of 624 eligible visits, 516 (83%) were converted to telehealth visits. Phone visits were slightly more popular than video visits (54% vs. 46%, respectively).
- Patients who were older, who lived in a rural area, or who were on Medicare and Medicaid were more likely to opt for phone visits.
- The intervention resulted in an additional 258 hours of patient care.
- The reduction in lost revenue for phone versus video telemedicine visits was $7,298 ($39.19 per appointment).
IN PRACTICE:
“Our simple, targeted strategy of converting appointments to telehealth when an in-person appointment is identified as at-risk resulted in significant access gains and modest revenue loss reduction,” with net gains overall, the authors write.
SOURCE:
Sancia Ferguson MD, MPH, of the University of Wisconsin-Madison School of Medicine, presented the research at the annual meeting of the American College of Rheumatology, abstract 1007.
LIMITATIONS:
The study was conducted at two clinics in the UW Health system and may not be implementable in smaller practices.
DISCLOSURES:
Senior author Christie Bartels, MD, also of University of Washington-Madison School of Medicine, reports receiving a research grant from Pfizer unrelated to this study.
A version of this article appeared on Medscape.com.
TOPLINE:
Converting late cancellations and no-show appointments to telemedicine visits increases access to care without the need for rescheduling, according to new research.
METHODOLOGY:
- Investigators identified adult rheumatology patients with late cancellations (within 24 hours of appointment) or impending no-show appointments from September 2020 to March 2023.
- These patients were contacted and were offered the option of converting their in-person appointment to a telemedicine visit, either by phone or video.
- The program was piloted at one clinic beginning Sept. 1, 2020, and was expanded to a second clinic on Sept. 1, 2021.
TAKEAWAY:
- Of 624 eligible visits, 516 (83%) were converted to telehealth visits. Phone visits were slightly more popular than video visits (54% vs. 46%, respectively).
- Patients who were older, who lived in a rural area, or who were on Medicare and Medicaid were more likely to opt for phone visits.
- The intervention resulted in an additional 258 hours of patient care.
- The reduction in lost revenue for phone versus video telemedicine visits was $7,298 ($39.19 per appointment).
IN PRACTICE:
“Our simple, targeted strategy of converting appointments to telehealth when an in-person appointment is identified as at-risk resulted in significant access gains and modest revenue loss reduction,” with net gains overall, the authors write.
SOURCE:
Sancia Ferguson MD, MPH, of the University of Wisconsin-Madison School of Medicine, presented the research at the annual meeting of the American College of Rheumatology, abstract 1007.
LIMITATIONS:
The study was conducted at two clinics in the UW Health system and may not be implementable in smaller practices.
DISCLOSURES:
Senior author Christie Bartels, MD, also of University of Washington-Madison School of Medicine, reports receiving a research grant from Pfizer unrelated to this study.
A version of this article appeared on Medscape.com.
TOPLINE:
Converting late cancellations and no-show appointments to telemedicine visits increases access to care without the need for rescheduling, according to new research.
METHODOLOGY:
- Investigators identified adult rheumatology patients with late cancellations (within 24 hours of appointment) or impending no-show appointments from September 2020 to March 2023.
- These patients were contacted and were offered the option of converting their in-person appointment to a telemedicine visit, either by phone or video.
- The program was piloted at one clinic beginning Sept. 1, 2020, and was expanded to a second clinic on Sept. 1, 2021.
TAKEAWAY:
- Of 624 eligible visits, 516 (83%) were converted to telehealth visits. Phone visits were slightly more popular than video visits (54% vs. 46%, respectively).
- Patients who were older, who lived in a rural area, or who were on Medicare and Medicaid were more likely to opt for phone visits.
- The intervention resulted in an additional 258 hours of patient care.
- The reduction in lost revenue for phone versus video telemedicine visits was $7,298 ($39.19 per appointment).
IN PRACTICE:
“Our simple, targeted strategy of converting appointments to telehealth when an in-person appointment is identified as at-risk resulted in significant access gains and modest revenue loss reduction,” with net gains overall, the authors write.
SOURCE:
Sancia Ferguson MD, MPH, of the University of Wisconsin-Madison School of Medicine, presented the research at the annual meeting of the American College of Rheumatology, abstract 1007.
LIMITATIONS:
The study was conducted at two clinics in the UW Health system and may not be implementable in smaller practices.
DISCLOSURES:
Senior author Christie Bartels, MD, also of University of Washington-Madison School of Medicine, reports receiving a research grant from Pfizer unrelated to this study.
A version of this article appeared on Medscape.com.
Split-dose methotrexate speeds RA response over single dose
SAN DIEGO – A split dose of methotrexate (MTX) given orally once per week showed significantly higher efficacy in patients with rheumatoid arthritis at 16 weeks, compared with a single MTX dose weekly, according to new research. By 24 weeks, efficacy measures were similar for both groups.
However, fewer patients in the split-dose group needed additional disease-modifying antirheumatic drugs (DMARDs) to control disease activity.
MTX is a highly utilized, inexpensive drug for RA, but only about 30% of patients can achieve low disease activity or remission on MTX monotherapy, said Varun Dhir, MD, MBBS, of the Postgraduate Institute of Medical Education and Research, Chandigarh, India. He co-authored and presented the research at the annual meeting of the American College of Rheumatology.
Part of the problem is that “oral methotrexate absorption from the gut reduces as the doses go up,” Dr. Dhir noted, because the transport mechanism gets saturated. MTX delivered subcutaneously is one way to improve efficacy, but patients can be needle-averse, and in some countries, like India, pre-filled syringes are not available, he said.
There is pharmacokinetic data dating back 20 years that suggest split-dose MTX could be more efficacious. “However, there are no randomized controlled trials to date, and the guidelines therefore are silent on this approach,” Dr. Dhir said.
To address this question, Dr. Dhir and colleagues recruited patients with RA from six centers across India. Patients were aged 18-60 years, seropositive (rheumatoid factor or anti-citrullinated protein antibodies), and had a disease duration of 5 years or fewer. Patients had active disease, defined as at least four tender joints and at least two swollen joints, and were not taking any DMARDs except for hydroxychloroquine and/or low-dose prednisolone.
A total of 253 patients were randomly assigned to a single 25-mg dose or a split-dose of MTX once weekly (10 mg in the morning and 15 mg in the evening on the same day). The primary outcome was a European Alliance of Associations for Rheumatology (EULAR) good response at 24 weeks. At the 16-week mark, if patients had not achieved low disease activity based on a 28-joint Disease Activity Score (DAS28) greater than 3.2, a blinded assessor could add either leflunomide or sulfasalazine to the continued MTX therapy.
At baseline, there was no difference between the groups’ DAS28, but after 16 weeks, DAS28 was significantly lower in the split-dose group, compared with the single-dose group (4.4 vs. 5.1; P < .001), and a higher percentage of patients in the split-dose group had a EULAR good response.
About three-quarters (76.6%) of patients in the split-dose group experienced an improvement of at least 20% in ACR response criteria (ACR20), compared with 52% in the single-dose group. The split-dose group also had higher proportion of patients achieving ACR50 and ACR70.
About one-third of the split-dose group (35%) added an additional DMARD at 16 weeks, compared with 54.5% of the single-dose group (P = .005).
After 24 weeks, DAS28 scores remained lower in the split-dose group (4.1 vs. 4.5; P = .03), but there were no other differences in treatment responses. Health Assessment Questionnaire scores were the same between both groups at 16 and 24 weeks.
The primary outcome was not met, although Dr. Dhir noted a flaw in the study design that could have affected the results. By allowing patients to add additional DMARDs at 16 weeks, “there were two factors which were affecting the primary outcome” at 24 weeks, he told this news organization. “I feel there was a robust result at least at 16 weeks.”
While there were no major adverse events, the split-dose group had higher rates of transaminitis (elevated liver enzymes) during the study, and low white blood cell count was higher in the single-dose group at 24 weeks. There was no difference in MTX intolerance between the two groups.
“It looks like [the split-dose group] gets out of the block faster. It’s a faster effect,” although the other group did catch up, Janet Pope, MD, MPH, of Western University, London, Ont., said in an interview. She was not involved with the research. Two positive results were the earlier ACR responses in the split-dose group as well as fewer patients in that same group needing to add another DMARD to therapy.
“In my opinion, if it’s equal cost, why not try it and see?” she said.
In a separate presentation referring to the abstract, Joan Bathon, MD, director of rheumatology at Columbia University, New York City, noted that these results align with ACR 2021 recommendations. Dr. Bathon was not involved with this study but was on the writing committee establishing those 2021 guidelines.
“The recommendation – with low certainty of evidence – was that for patients who are intolerant to MTX, that split-dose of oral MTX is worth trying before you switch to a different DMARD,” she said. “I think these data support that concept.”
Dr. Dhir and Dr. Bathon had no relevant financial relationships. Dr. Pope disclosed financial relationships with AbbVie/Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Fresenius Kabi, GlaxoSmithKline, Janssen, Mallinckrodt, Novartis, Organon, Pfizer, Sandoz, and Viatris.
A version of this article first appeared on Medscape.com.
SAN DIEGO – A split dose of methotrexate (MTX) given orally once per week showed significantly higher efficacy in patients with rheumatoid arthritis at 16 weeks, compared with a single MTX dose weekly, according to new research. By 24 weeks, efficacy measures were similar for both groups.
However, fewer patients in the split-dose group needed additional disease-modifying antirheumatic drugs (DMARDs) to control disease activity.
MTX is a highly utilized, inexpensive drug for RA, but only about 30% of patients can achieve low disease activity or remission on MTX monotherapy, said Varun Dhir, MD, MBBS, of the Postgraduate Institute of Medical Education and Research, Chandigarh, India. He co-authored and presented the research at the annual meeting of the American College of Rheumatology.
Part of the problem is that “oral methotrexate absorption from the gut reduces as the doses go up,” Dr. Dhir noted, because the transport mechanism gets saturated. MTX delivered subcutaneously is one way to improve efficacy, but patients can be needle-averse, and in some countries, like India, pre-filled syringes are not available, he said.
There is pharmacokinetic data dating back 20 years that suggest split-dose MTX could be more efficacious. “However, there are no randomized controlled trials to date, and the guidelines therefore are silent on this approach,” Dr. Dhir said.
To address this question, Dr. Dhir and colleagues recruited patients with RA from six centers across India. Patients were aged 18-60 years, seropositive (rheumatoid factor or anti-citrullinated protein antibodies), and had a disease duration of 5 years or fewer. Patients had active disease, defined as at least four tender joints and at least two swollen joints, and were not taking any DMARDs except for hydroxychloroquine and/or low-dose prednisolone.
A total of 253 patients were randomly assigned to a single 25-mg dose or a split-dose of MTX once weekly (10 mg in the morning and 15 mg in the evening on the same day). The primary outcome was a European Alliance of Associations for Rheumatology (EULAR) good response at 24 weeks. At the 16-week mark, if patients had not achieved low disease activity based on a 28-joint Disease Activity Score (DAS28) greater than 3.2, a blinded assessor could add either leflunomide or sulfasalazine to the continued MTX therapy.
At baseline, there was no difference between the groups’ DAS28, but after 16 weeks, DAS28 was significantly lower in the split-dose group, compared with the single-dose group (4.4 vs. 5.1; P < .001), and a higher percentage of patients in the split-dose group had a EULAR good response.
About three-quarters (76.6%) of patients in the split-dose group experienced an improvement of at least 20% in ACR response criteria (ACR20), compared with 52% in the single-dose group. The split-dose group also had higher proportion of patients achieving ACR50 and ACR70.
About one-third of the split-dose group (35%) added an additional DMARD at 16 weeks, compared with 54.5% of the single-dose group (P = .005).
After 24 weeks, DAS28 scores remained lower in the split-dose group (4.1 vs. 4.5; P = .03), but there were no other differences in treatment responses. Health Assessment Questionnaire scores were the same between both groups at 16 and 24 weeks.
The primary outcome was not met, although Dr. Dhir noted a flaw in the study design that could have affected the results. By allowing patients to add additional DMARDs at 16 weeks, “there were two factors which were affecting the primary outcome” at 24 weeks, he told this news organization. “I feel there was a robust result at least at 16 weeks.”
While there were no major adverse events, the split-dose group had higher rates of transaminitis (elevated liver enzymes) during the study, and low white blood cell count was higher in the single-dose group at 24 weeks. There was no difference in MTX intolerance between the two groups.
“It looks like [the split-dose group] gets out of the block faster. It’s a faster effect,” although the other group did catch up, Janet Pope, MD, MPH, of Western University, London, Ont., said in an interview. She was not involved with the research. Two positive results were the earlier ACR responses in the split-dose group as well as fewer patients in that same group needing to add another DMARD to therapy.
“In my opinion, if it’s equal cost, why not try it and see?” she said.
In a separate presentation referring to the abstract, Joan Bathon, MD, director of rheumatology at Columbia University, New York City, noted that these results align with ACR 2021 recommendations. Dr. Bathon was not involved with this study but was on the writing committee establishing those 2021 guidelines.
“The recommendation – with low certainty of evidence – was that for patients who are intolerant to MTX, that split-dose of oral MTX is worth trying before you switch to a different DMARD,” she said. “I think these data support that concept.”
Dr. Dhir and Dr. Bathon had no relevant financial relationships. Dr. Pope disclosed financial relationships with AbbVie/Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Fresenius Kabi, GlaxoSmithKline, Janssen, Mallinckrodt, Novartis, Organon, Pfizer, Sandoz, and Viatris.
A version of this article first appeared on Medscape.com.
SAN DIEGO – A split dose of methotrexate (MTX) given orally once per week showed significantly higher efficacy in patients with rheumatoid arthritis at 16 weeks, compared with a single MTX dose weekly, according to new research. By 24 weeks, efficacy measures were similar for both groups.
However, fewer patients in the split-dose group needed additional disease-modifying antirheumatic drugs (DMARDs) to control disease activity.
MTX is a highly utilized, inexpensive drug for RA, but only about 30% of patients can achieve low disease activity or remission on MTX monotherapy, said Varun Dhir, MD, MBBS, of the Postgraduate Institute of Medical Education and Research, Chandigarh, India. He co-authored and presented the research at the annual meeting of the American College of Rheumatology.
Part of the problem is that “oral methotrexate absorption from the gut reduces as the doses go up,” Dr. Dhir noted, because the transport mechanism gets saturated. MTX delivered subcutaneously is one way to improve efficacy, but patients can be needle-averse, and in some countries, like India, pre-filled syringes are not available, he said.
There is pharmacokinetic data dating back 20 years that suggest split-dose MTX could be more efficacious. “However, there are no randomized controlled trials to date, and the guidelines therefore are silent on this approach,” Dr. Dhir said.
To address this question, Dr. Dhir and colleagues recruited patients with RA from six centers across India. Patients were aged 18-60 years, seropositive (rheumatoid factor or anti-citrullinated protein antibodies), and had a disease duration of 5 years or fewer. Patients had active disease, defined as at least four tender joints and at least two swollen joints, and were not taking any DMARDs except for hydroxychloroquine and/or low-dose prednisolone.
A total of 253 patients were randomly assigned to a single 25-mg dose or a split-dose of MTX once weekly (10 mg in the morning and 15 mg in the evening on the same day). The primary outcome was a European Alliance of Associations for Rheumatology (EULAR) good response at 24 weeks. At the 16-week mark, if patients had not achieved low disease activity based on a 28-joint Disease Activity Score (DAS28) greater than 3.2, a blinded assessor could add either leflunomide or sulfasalazine to the continued MTX therapy.
At baseline, there was no difference between the groups’ DAS28, but after 16 weeks, DAS28 was significantly lower in the split-dose group, compared with the single-dose group (4.4 vs. 5.1; P < .001), and a higher percentage of patients in the split-dose group had a EULAR good response.
About three-quarters (76.6%) of patients in the split-dose group experienced an improvement of at least 20% in ACR response criteria (ACR20), compared with 52% in the single-dose group. The split-dose group also had higher proportion of patients achieving ACR50 and ACR70.
About one-third of the split-dose group (35%) added an additional DMARD at 16 weeks, compared with 54.5% of the single-dose group (P = .005).
After 24 weeks, DAS28 scores remained lower in the split-dose group (4.1 vs. 4.5; P = .03), but there were no other differences in treatment responses. Health Assessment Questionnaire scores were the same between both groups at 16 and 24 weeks.
The primary outcome was not met, although Dr. Dhir noted a flaw in the study design that could have affected the results. By allowing patients to add additional DMARDs at 16 weeks, “there were two factors which were affecting the primary outcome” at 24 weeks, he told this news organization. “I feel there was a robust result at least at 16 weeks.”
While there were no major adverse events, the split-dose group had higher rates of transaminitis (elevated liver enzymes) during the study, and low white blood cell count was higher in the single-dose group at 24 weeks. There was no difference in MTX intolerance between the two groups.
“It looks like [the split-dose group] gets out of the block faster. It’s a faster effect,” although the other group did catch up, Janet Pope, MD, MPH, of Western University, London, Ont., said in an interview. She was not involved with the research. Two positive results were the earlier ACR responses in the split-dose group as well as fewer patients in that same group needing to add another DMARD to therapy.
“In my opinion, if it’s equal cost, why not try it and see?” she said.
In a separate presentation referring to the abstract, Joan Bathon, MD, director of rheumatology at Columbia University, New York City, noted that these results align with ACR 2021 recommendations. Dr. Bathon was not involved with this study but was on the writing committee establishing those 2021 guidelines.
“The recommendation – with low certainty of evidence – was that for patients who are intolerant to MTX, that split-dose of oral MTX is worth trying before you switch to a different DMARD,” she said. “I think these data support that concept.”
Dr. Dhir and Dr. Bathon had no relevant financial relationships. Dr. Pope disclosed financial relationships with AbbVie/Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Fresenius Kabi, GlaxoSmithKline, Janssen, Mallinckrodt, Novartis, Organon, Pfizer, Sandoz, and Viatris.
A version of this article first appeared on Medscape.com.
AT ACR 2023

First referral guide issued for axial spondyloarthritis
SAN DIEGO – The Spondyloarthritis Research and Treatment Network (SPARTAN) has created the first referral recommendations for axial spondyloarthritis (axSpA).
The draft recommendations use a points scoring system, with the goal that at least one in three patients referred would be diagnosed with axSpA, an inflammatory arthritis that affects the central skeleton and shares a genetic overlap with skin psoriasis, inflammatory bowel disease, and inflammatory eye disease.
Patients with axSpA can wait 10 years after symptom onset to be diagnosed with the condition. There are currently no guidelines to advise clinicians on when to refer to a rheumatologist, and with the rheumatology workforce shortage, “it is impossible for rheumatologists to evaluate the 20% of adults in the U.S. who have chronic back pain,” said Maureen Dubreuil, MD, a rheumatologist at Boston University. She presented the work at the annual meeting of the American College of Rheumatology.
To address this issue, Dr. Dubreuil and colleagues conducted a literature review to determine how predictive different spondyloarthritis features were of eventual axSpA diagnosis. The interdisciplinary team identified 38 studies published before March 2022, and uncovered 28 individual potential features associated with axSpA, including pain sites, family history of axSpA and related conditions, blood markers of inflammation, genetic testing, and imaging findings.
Inflammatory back pain elements had the lower predictive values, with positive likelihood ratios (LR+) ranging from 1.15 to 2.32, while imaging findings were the most predictive (LR+s from 6.40 to 10.02).
Using a Delphi exercise and discrete choice experiments, members narrowed the checklist down to 10 features. These 10 features were assigned points, with a score of 3 points qualifying for a referral of adults 45 years or younger with chronic pain (3 or more months) in the back, hip, or buttock.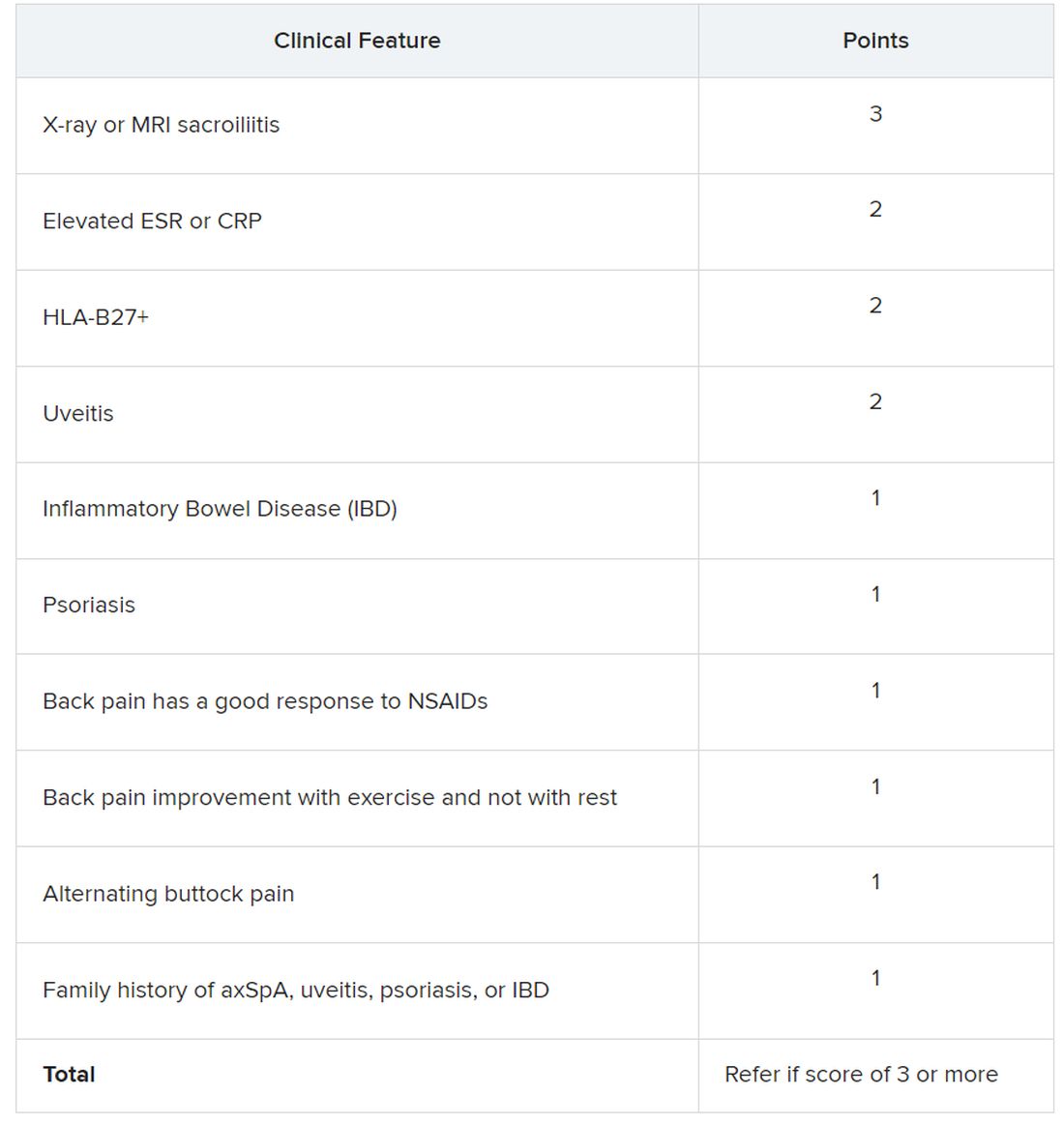
Sacroiliitis seen on imaging, either by x-ray or MRI, received the highest score of 3 points. Dr. Dubreuil emphasized that imaging was not required for a referral, but if a patient has received imaging “that shows sacroiliitis, that is sufficient for referral to a rheumatologist,” she said in her presentation.
Elevated erythrocyte sedimentation rate or C-reactive protein, HLA-B27 positivity, and uveitis score 2 points. Inflammatory bowel disease; psoriasis; back pain with good response to NSAIDs; back pain improvement with exercise and not with rest; alternating buttock pain; and family history of axial spondyloarthritis, uveitis, psoriasis, or IBD score 1 point.
Dr. Dubreuil and colleagues expect that these criteria for referral will result in about one in three referred adults aged 45 years or younger with chronic back pain being diagnosed with axSpA. They also say additional research is necessary to understand if these recommendations increase probability of axSpA diagnosis and reduce diagnostic delays.
“We’re now getting to the stage where we are creating this screening tool, but [testing the] performance of the screening tool is going to be the major next step,” said Mark Hwang, MD, of UTHealth Houston in an interview with this news organization. He is a member of SPARTAN but was not involved with authoring the recommendations. “Will the screening tool enhance the ability on the back end to identify axSpA? We don’t know yet.”
Jon Chan, MD, a rheumatologist at the University of British Columbia, Vancouver, agreed that these recommendations “are a good first step,” but that more awareness about axSpA from nonrheumatologists would also be helpful in identifying new axSpA patients. He is also a member of SPARTAN and comoderated with Dr. Hwang the session where the new recommendations were presented. “I think other diseases like rheumatoid arthritis or lupus have a lot more recognition in the nonrheumatology community,” he told this news organization.
Connecting with other health professionals who see a lot of patients with back pain – physiotherapists, chiropractors, and chronic pain physicians – could also be helpful, he added. “A lot of times, patients go straight to a physio and circumvent the doctor,” he said.
Dr. Chan reports success in educating other departments. “I put up a poster in the emergency department saying, ‘If you’re young with back pain and uveitis, you need to be seen by rheumatology,’ and we’ve identified a ton of axSpA patients that way,” he said. “Maybe their uveitis was very mild, but their back pain was quite severe, and no one really clued in.”
Dr. Dubreuil disclosed financial relationships with Amgen, Pfizer, and UCB Pharma. Her abstract coauthors disclosed financial relationships with multiple pharmaceutical companies. Dr. Hwang consults for UCB and has received research support from Janssen. Dr. Chan has relationships with AbbVie/Abbott, Eli Lilly, Janssen, Novartis, and UCB.
SAN DIEGO – The Spondyloarthritis Research and Treatment Network (SPARTAN) has created the first referral recommendations for axial spondyloarthritis (axSpA).
The draft recommendations use a points scoring system, with the goal that at least one in three patients referred would be diagnosed with axSpA, an inflammatory arthritis that affects the central skeleton and shares a genetic overlap with skin psoriasis, inflammatory bowel disease, and inflammatory eye disease.
Patients with axSpA can wait 10 years after symptom onset to be diagnosed with the condition. There are currently no guidelines to advise clinicians on when to refer to a rheumatologist, and with the rheumatology workforce shortage, “it is impossible for rheumatologists to evaluate the 20% of adults in the U.S. who have chronic back pain,” said Maureen Dubreuil, MD, a rheumatologist at Boston University. She presented the work at the annual meeting of the American College of Rheumatology.
To address this issue, Dr. Dubreuil and colleagues conducted a literature review to determine how predictive different spondyloarthritis features were of eventual axSpA diagnosis. The interdisciplinary team identified 38 studies published before March 2022, and uncovered 28 individual potential features associated with axSpA, including pain sites, family history of axSpA and related conditions, blood markers of inflammation, genetic testing, and imaging findings.
Inflammatory back pain elements had the lower predictive values, with positive likelihood ratios (LR+) ranging from 1.15 to 2.32, while imaging findings were the most predictive (LR+s from 6.40 to 10.02).
Using a Delphi exercise and discrete choice experiments, members narrowed the checklist down to 10 features. These 10 features were assigned points, with a score of 3 points qualifying for a referral of adults 45 years or younger with chronic pain (3 or more months) in the back, hip, or buttock.
Sacroiliitis seen on imaging, either by x-ray or MRI, received the highest score of 3 points. Dr. Dubreuil emphasized that imaging was not required for a referral, but if a patient has received imaging “that shows sacroiliitis, that is sufficient for referral to a rheumatologist,” she said in her presentation.
Elevated erythrocyte sedimentation rate or C-reactive protein, HLA-B27 positivity, and uveitis score 2 points. Inflammatory bowel disease; psoriasis; back pain with good response to NSAIDs; back pain improvement with exercise and not with rest; alternating buttock pain; and family history of axial spondyloarthritis, uveitis, psoriasis, or IBD score 1 point.
Dr. Dubreuil and colleagues expect that these criteria for referral will result in about one in three referred adults aged 45 years or younger with chronic back pain being diagnosed with axSpA. They also say additional research is necessary to understand if these recommendations increase probability of axSpA diagnosis and reduce diagnostic delays.
“We’re now getting to the stage where we are creating this screening tool, but [testing the] performance of the screening tool is going to be the major next step,” said Mark Hwang, MD, of UTHealth Houston in an interview with this news organization. He is a member of SPARTAN but was not involved with authoring the recommendations. “Will the screening tool enhance the ability on the back end to identify axSpA? We don’t know yet.”
Jon Chan, MD, a rheumatologist at the University of British Columbia, Vancouver, agreed that these recommendations “are a good first step,” but that more awareness about axSpA from nonrheumatologists would also be helpful in identifying new axSpA patients. He is also a member of SPARTAN and comoderated with Dr. Hwang the session where the new recommendations were presented. “I think other diseases like rheumatoid arthritis or lupus have a lot more recognition in the nonrheumatology community,” he told this news organization.
Connecting with other health professionals who see a lot of patients with back pain – physiotherapists, chiropractors, and chronic pain physicians – could also be helpful, he added. “A lot of times, patients go straight to a physio and circumvent the doctor,” he said.
Dr. Chan reports success in educating other departments. “I put up a poster in the emergency department saying, ‘If you’re young with back pain and uveitis, you need to be seen by rheumatology,’ and we’ve identified a ton of axSpA patients that way,” he said. “Maybe their uveitis was very mild, but their back pain was quite severe, and no one really clued in.”
Dr. Dubreuil disclosed financial relationships with Amgen, Pfizer, and UCB Pharma. Her abstract coauthors disclosed financial relationships with multiple pharmaceutical companies. Dr. Hwang consults for UCB and has received research support from Janssen. Dr. Chan has relationships with AbbVie/Abbott, Eli Lilly, Janssen, Novartis, and UCB.
SAN DIEGO – The Spondyloarthritis Research and Treatment Network (SPARTAN) has created the first referral recommendations for axial spondyloarthritis (axSpA).
The draft recommendations use a points scoring system, with the goal that at least one in three patients referred would be diagnosed with axSpA, an inflammatory arthritis that affects the central skeleton and shares a genetic overlap with skin psoriasis, inflammatory bowel disease, and inflammatory eye disease.
Patients with axSpA can wait 10 years after symptom onset to be diagnosed with the condition. There are currently no guidelines to advise clinicians on when to refer to a rheumatologist, and with the rheumatology workforce shortage, “it is impossible for rheumatologists to evaluate the 20% of adults in the U.S. who have chronic back pain,” said Maureen Dubreuil, MD, a rheumatologist at Boston University. She presented the work at the annual meeting of the American College of Rheumatology.
To address this issue, Dr. Dubreuil and colleagues conducted a literature review to determine how predictive different spondyloarthritis features were of eventual axSpA diagnosis. The interdisciplinary team identified 38 studies published before March 2022, and uncovered 28 individual potential features associated with axSpA, including pain sites, family history of axSpA and related conditions, blood markers of inflammation, genetic testing, and imaging findings.
Inflammatory back pain elements had the lower predictive values, with positive likelihood ratios (LR+) ranging from 1.15 to 2.32, while imaging findings were the most predictive (LR+s from 6.40 to 10.02).
Using a Delphi exercise and discrete choice experiments, members narrowed the checklist down to 10 features. These 10 features were assigned points, with a score of 3 points qualifying for a referral of adults 45 years or younger with chronic pain (3 or more months) in the back, hip, or buttock.
Sacroiliitis seen on imaging, either by x-ray or MRI, received the highest score of 3 points. Dr. Dubreuil emphasized that imaging was not required for a referral, but if a patient has received imaging “that shows sacroiliitis, that is sufficient for referral to a rheumatologist,” she said in her presentation.
Elevated erythrocyte sedimentation rate or C-reactive protein, HLA-B27 positivity, and uveitis score 2 points. Inflammatory bowel disease; psoriasis; back pain with good response to NSAIDs; back pain improvement with exercise and not with rest; alternating buttock pain; and family history of axial spondyloarthritis, uveitis, psoriasis, or IBD score 1 point.
Dr. Dubreuil and colleagues expect that these criteria for referral will result in about one in three referred adults aged 45 years or younger with chronic back pain being diagnosed with axSpA. They also say additional research is necessary to understand if these recommendations increase probability of axSpA diagnosis and reduce diagnostic delays.
“We’re now getting to the stage where we are creating this screening tool, but [testing the] performance of the screening tool is going to be the major next step,” said Mark Hwang, MD, of UTHealth Houston in an interview with this news organization. He is a member of SPARTAN but was not involved with authoring the recommendations. “Will the screening tool enhance the ability on the back end to identify axSpA? We don’t know yet.”
Jon Chan, MD, a rheumatologist at the University of British Columbia, Vancouver, agreed that these recommendations “are a good first step,” but that more awareness about axSpA from nonrheumatologists would also be helpful in identifying new axSpA patients. He is also a member of SPARTAN and comoderated with Dr. Hwang the session where the new recommendations were presented. “I think other diseases like rheumatoid arthritis or lupus have a lot more recognition in the nonrheumatology community,” he told this news organization.
Connecting with other health professionals who see a lot of patients with back pain – physiotherapists, chiropractors, and chronic pain physicians – could also be helpful, he added. “A lot of times, patients go straight to a physio and circumvent the doctor,” he said.
Dr. Chan reports success in educating other departments. “I put up a poster in the emergency department saying, ‘If you’re young with back pain and uveitis, you need to be seen by rheumatology,’ and we’ve identified a ton of axSpA patients that way,” he said. “Maybe their uveitis was very mild, but their back pain was quite severe, and no one really clued in.”
Dr. Dubreuil disclosed financial relationships with Amgen, Pfizer, and UCB Pharma. Her abstract coauthors disclosed financial relationships with multiple pharmaceutical companies. Dr. Hwang consults for UCB and has received research support from Janssen. Dr. Chan has relationships with AbbVie/Abbott, Eli Lilly, Janssen, Novartis, and UCB.
AT ACR 2023