User login
“Caregiver Culture” and End-of-Life Discussions
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
CHAMP: A Real Winner at Teaching Geriatrics
The elderly constitute the fastest-growing segment of the U.S. population. According to one estimate, nearly one in five Americans will be 65 years old or older by 2050.1 Geriatric medicine has produced a plethora of information regarding older patients’ special needs, but when it comes to teaching medical students and residents, most curricular materials focus on the care and management of older outpatients, rather than inpatients. In an effort to fill this gap, faculty at the University of Chicago School of Medicine developed the Curriculum for the Hospitalized Aging Medical Patient (CHAMP). It is designed to help instructors teach the management of elderly inpatients. In this month’s issue of the Journal of Hospital Medicine, lead author Paula Podrazik, MD, associate professor in the section of geriatrics, department of medicine, University of Chicago, and her co-authors explain CHAMP as it was perceived by a targeted group of faculty learners.
—Paula Podrazik, MD, associate professor in the section of geriatrics, department of medicine, University of Chicago
CHAMP incorporates knowledge gleaned from first-hand experience and a review of the literature and existing models of care. “Our goal was to improve patient care and systems of hospital care through education by faculty development,” Dr. Podrazik tells The Hospitalist. The CHAMP program emphasizes issues of particular importance in geriatric hospital medicine, including frailty, avoiding hazards of hospitalization, palliation, and care transitions.
For example, “hospitalists need to know certain aspects of dementia care, such as how to recognize it and screen for it,” she explains. “They have to determine whether a particular patient is able to make decisions, and they have to understand what it is about this condition that puts these patients at higher risk in the hospital.” Another example includes medication review and “communicating medication changes when transitioning the patient to a skilled nursing facility, home, or a rehabilitation center.”
Dr. Podrazik and her colleagues hope CHAMP might entice more medical students and residents to consider entering geriatric medicine. “Half of the [hospital] beds in the U.S. are filled with patients who are at least 65 years old. Many students and residents base their career decisions on what they see during their hospital rotation, so this was a great opportunity for us, as geriatricians, to influence that decision.”
The program consists of learning modules presented in 12, four-hour sessions. The modules address four basic themes:
- Identification of the frail or vulnerable elderly patient;
- Recognition and avoidance of hospitalization hazards, such as falls and dementia;
- Palliative care and end-of-life issues; and
- Improving transitions of care.
Each module has specific learning objectives and an evaluation process based on the standard precepts of curriculum design. The first part of each session covers topics on geriatric inpatient medicine, such as high-risk medications, medication reconciliation, restraint use, care transitions, and other aspects of mandates from The Joint Commission, which have particular relevance to the care of elderly people. Faculty participants listen to 30- to 90-minute lectures on each topic, with an emphasis on applying the content during bedside teaching rounds.
Modules presented in the second half of the session cover teaching techniques, such as the Stanford Faculty Development Program for Medical Teachers, which uses case scenarios and practice sessions to polish participants’ teaching skills. Another component specifically developed for CHAMP is a mini-course called “Teaching on Today’s Wards.” It is designed to help non-geriatric faculty put more geriatrics content in their bedside rounds, and to improve bedside teaching techniques in the inpatient wards.
The CHAMP curriculum also addresses the core competencies designated by the Accreditation Council for Graduate Medical Education (ACGME), namely professionalism, communication, systems-based practice, and practice-based learning and improvement.
The basic principles of geriatric care already exist, Dr. Podrazik says. “It was our job to pull it all together,” she explains. “A program of this size and magnitude couldn’t have been done without the participation of people in a multitude of areas, including hospitalists, geriatricians, internists, and PhD educators. We had multiple champions who took different areas and just ran with them.”
With eight faculty scholars volunteering to serve as guinea pigs, Dr. Podrazik and her colleagues pilot-tested the program in the spring of 2004. By 2006, another 21 faculty members had participated in CHAMP, including nearly half of the university’s general medicine faculty and most of its hospitalists. The response was enthusiastic, she says, with learners praising the presentation of geriatric issues and concrete suggestions for incorporating the information in their own teaching sessions. Upon completion of the CHAMP series, participants reported feeling significantly more knowledgeable about geriatric content, had more positive attitudes toward older patients, and felt more confident in their ability to care for older patients and teach geriatric medicine.
A major challenge was “providing enough ongoing support to reinforce learning with an eye on the greater goal of changing teaching behaviors and clinical outcomes,” the authors wrote. To solve this problem, they added objective structural teaching evaluations (OSTEs), so participants could test their teaching skills and mastery of geriatric content. Practice-oriented games, exercises, and tutorials, and ongoing contact with CHAMP alumnae and faculty are provided, as well as access to support materials online. Efforts are under way to incorporate core CHAMP faculty members into hospitalist and general medicine lecture series. Also being considered is having a CHAMP core faculty member attend during inpatient ward rounds.
It appears as though CHAMP is starting to pay off, in terms of patient care, Dr. Podrazik says. Although she cautioned the findings are “really preliminary,” and data analysis is ongoing, clinical data “do show a beneficial effect on a number of patient care outcomes.” TH
Norra MacReady is a medical writer based in California.
Reference
1. Passel JS, Cohn D. U.S. population projections: 2005-2050. Pew Research Center. http://pewhispanic.org/reports/report.php?ReportID=85. Published February 11, 2008. Accessed Thursday, October 23, 2008.
The elderly constitute the fastest-growing segment of the U.S. population. According to one estimate, nearly one in five Americans will be 65 years old or older by 2050.1 Geriatric medicine has produced a plethora of information regarding older patients’ special needs, but when it comes to teaching medical students and residents, most curricular materials focus on the care and management of older outpatients, rather than inpatients. In an effort to fill this gap, faculty at the University of Chicago School of Medicine developed the Curriculum for the Hospitalized Aging Medical Patient (CHAMP). It is designed to help instructors teach the management of elderly inpatients. In this month’s issue of the Journal of Hospital Medicine, lead author Paula Podrazik, MD, associate professor in the section of geriatrics, department of medicine, University of Chicago, and her co-authors explain CHAMP as it was perceived by a targeted group of faculty learners.
—Paula Podrazik, MD, associate professor in the section of geriatrics, department of medicine, University of Chicago
CHAMP incorporates knowledge gleaned from first-hand experience and a review of the literature and existing models of care. “Our goal was to improve patient care and systems of hospital care through education by faculty development,” Dr. Podrazik tells The Hospitalist. The CHAMP program emphasizes issues of particular importance in geriatric hospital medicine, including frailty, avoiding hazards of hospitalization, palliation, and care transitions.
For example, “hospitalists need to know certain aspects of dementia care, such as how to recognize it and screen for it,” she explains. “They have to determine whether a particular patient is able to make decisions, and they have to understand what it is about this condition that puts these patients at higher risk in the hospital.” Another example includes medication review and “communicating medication changes when transitioning the patient to a skilled nursing facility, home, or a rehabilitation center.”
Dr. Podrazik and her colleagues hope CHAMP might entice more medical students and residents to consider entering geriatric medicine. “Half of the [hospital] beds in the U.S. are filled with patients who are at least 65 years old. Many students and residents base their career decisions on what they see during their hospital rotation, so this was a great opportunity for us, as geriatricians, to influence that decision.”
The program consists of learning modules presented in 12, four-hour sessions. The modules address four basic themes:
- Identification of the frail or vulnerable elderly patient;
- Recognition and avoidance of hospitalization hazards, such as falls and dementia;
- Palliative care and end-of-life issues; and
- Improving transitions of care.
Each module has specific learning objectives and an evaluation process based on the standard precepts of curriculum design. The first part of each session covers topics on geriatric inpatient medicine, such as high-risk medications, medication reconciliation, restraint use, care transitions, and other aspects of mandates from The Joint Commission, which have particular relevance to the care of elderly people. Faculty participants listen to 30- to 90-minute lectures on each topic, with an emphasis on applying the content during bedside teaching rounds.
Modules presented in the second half of the session cover teaching techniques, such as the Stanford Faculty Development Program for Medical Teachers, which uses case scenarios and practice sessions to polish participants’ teaching skills. Another component specifically developed for CHAMP is a mini-course called “Teaching on Today’s Wards.” It is designed to help non-geriatric faculty put more geriatrics content in their bedside rounds, and to improve bedside teaching techniques in the inpatient wards.
The CHAMP curriculum also addresses the core competencies designated by the Accreditation Council for Graduate Medical Education (ACGME), namely professionalism, communication, systems-based practice, and practice-based learning and improvement.
The basic principles of geriatric care already exist, Dr. Podrazik says. “It was our job to pull it all together,” she explains. “A program of this size and magnitude couldn’t have been done without the participation of people in a multitude of areas, including hospitalists, geriatricians, internists, and PhD educators. We had multiple champions who took different areas and just ran with them.”
With eight faculty scholars volunteering to serve as guinea pigs, Dr. Podrazik and her colleagues pilot-tested the program in the spring of 2004. By 2006, another 21 faculty members had participated in CHAMP, including nearly half of the university’s general medicine faculty and most of its hospitalists. The response was enthusiastic, she says, with learners praising the presentation of geriatric issues and concrete suggestions for incorporating the information in their own teaching sessions. Upon completion of the CHAMP series, participants reported feeling significantly more knowledgeable about geriatric content, had more positive attitudes toward older patients, and felt more confident in their ability to care for older patients and teach geriatric medicine.
A major challenge was “providing enough ongoing support to reinforce learning with an eye on the greater goal of changing teaching behaviors and clinical outcomes,” the authors wrote. To solve this problem, they added objective structural teaching evaluations (OSTEs), so participants could test their teaching skills and mastery of geriatric content. Practice-oriented games, exercises, and tutorials, and ongoing contact with CHAMP alumnae and faculty are provided, as well as access to support materials online. Efforts are under way to incorporate core CHAMP faculty members into hospitalist and general medicine lecture series. Also being considered is having a CHAMP core faculty member attend during inpatient ward rounds.
It appears as though CHAMP is starting to pay off, in terms of patient care, Dr. Podrazik says. Although she cautioned the findings are “really preliminary,” and data analysis is ongoing, clinical data “do show a beneficial effect on a number of patient care outcomes.” TH
Norra MacReady is a medical writer based in California.
Reference
1. Passel JS, Cohn D. U.S. population projections: 2005-2050. Pew Research Center. http://pewhispanic.org/reports/report.php?ReportID=85. Published February 11, 2008. Accessed Thursday, October 23, 2008.
The elderly constitute the fastest-growing segment of the U.S. population. According to one estimate, nearly one in five Americans will be 65 years old or older by 2050.1 Geriatric medicine has produced a plethora of information regarding older patients’ special needs, but when it comes to teaching medical students and residents, most curricular materials focus on the care and management of older outpatients, rather than inpatients. In an effort to fill this gap, faculty at the University of Chicago School of Medicine developed the Curriculum for the Hospitalized Aging Medical Patient (CHAMP). It is designed to help instructors teach the management of elderly inpatients. In this month’s issue of the Journal of Hospital Medicine, lead author Paula Podrazik, MD, associate professor in the section of geriatrics, department of medicine, University of Chicago, and her co-authors explain CHAMP as it was perceived by a targeted group of faculty learners.
—Paula Podrazik, MD, associate professor in the section of geriatrics, department of medicine, University of Chicago
CHAMP incorporates knowledge gleaned from first-hand experience and a review of the literature and existing models of care. “Our goal was to improve patient care and systems of hospital care through education by faculty development,” Dr. Podrazik tells The Hospitalist. The CHAMP program emphasizes issues of particular importance in geriatric hospital medicine, including frailty, avoiding hazards of hospitalization, palliation, and care transitions.
For example, “hospitalists need to know certain aspects of dementia care, such as how to recognize it and screen for it,” she explains. “They have to determine whether a particular patient is able to make decisions, and they have to understand what it is about this condition that puts these patients at higher risk in the hospital.” Another example includes medication review and “communicating medication changes when transitioning the patient to a skilled nursing facility, home, or a rehabilitation center.”
Dr. Podrazik and her colleagues hope CHAMP might entice more medical students and residents to consider entering geriatric medicine. “Half of the [hospital] beds in the U.S. are filled with patients who are at least 65 years old. Many students and residents base their career decisions on what they see during their hospital rotation, so this was a great opportunity for us, as geriatricians, to influence that decision.”
The program consists of learning modules presented in 12, four-hour sessions. The modules address four basic themes:
- Identification of the frail or vulnerable elderly patient;
- Recognition and avoidance of hospitalization hazards, such as falls and dementia;
- Palliative care and end-of-life issues; and
- Improving transitions of care.
Each module has specific learning objectives and an evaluation process based on the standard precepts of curriculum design. The first part of each session covers topics on geriatric inpatient medicine, such as high-risk medications, medication reconciliation, restraint use, care transitions, and other aspects of mandates from The Joint Commission, which have particular relevance to the care of elderly people. Faculty participants listen to 30- to 90-minute lectures on each topic, with an emphasis on applying the content during bedside teaching rounds.
Modules presented in the second half of the session cover teaching techniques, such as the Stanford Faculty Development Program for Medical Teachers, which uses case scenarios and practice sessions to polish participants’ teaching skills. Another component specifically developed for CHAMP is a mini-course called “Teaching on Today’s Wards.” It is designed to help non-geriatric faculty put more geriatrics content in their bedside rounds, and to improve bedside teaching techniques in the inpatient wards.
The CHAMP curriculum also addresses the core competencies designated by the Accreditation Council for Graduate Medical Education (ACGME), namely professionalism, communication, systems-based practice, and practice-based learning and improvement.
The basic principles of geriatric care already exist, Dr. Podrazik says. “It was our job to pull it all together,” she explains. “A program of this size and magnitude couldn’t have been done without the participation of people in a multitude of areas, including hospitalists, geriatricians, internists, and PhD educators. We had multiple champions who took different areas and just ran with them.”
With eight faculty scholars volunteering to serve as guinea pigs, Dr. Podrazik and her colleagues pilot-tested the program in the spring of 2004. By 2006, another 21 faculty members had participated in CHAMP, including nearly half of the university’s general medicine faculty and most of its hospitalists. The response was enthusiastic, she says, with learners praising the presentation of geriatric issues and concrete suggestions for incorporating the information in their own teaching sessions. Upon completion of the CHAMP series, participants reported feeling significantly more knowledgeable about geriatric content, had more positive attitudes toward older patients, and felt more confident in their ability to care for older patients and teach geriatric medicine.
A major challenge was “providing enough ongoing support to reinforce learning with an eye on the greater goal of changing teaching behaviors and clinical outcomes,” the authors wrote. To solve this problem, they added objective structural teaching evaluations (OSTEs), so participants could test their teaching skills and mastery of geriatric content. Practice-oriented games, exercises, and tutorials, and ongoing contact with CHAMP alumnae and faculty are provided, as well as access to support materials online. Efforts are under way to incorporate core CHAMP faculty members into hospitalist and general medicine lecture series. Also being considered is having a CHAMP core faculty member attend during inpatient ward rounds.
It appears as though CHAMP is starting to pay off, in terms of patient care, Dr. Podrazik says. Although she cautioned the findings are “really preliminary,” and data analysis is ongoing, clinical data “do show a beneficial effect on a number of patient care outcomes.” TH
Norra MacReady is a medical writer based in California.
Reference
1. Passel JS, Cohn D. U.S. population projections: 2005-2050. Pew Research Center. http://pewhispanic.org/reports/report.php?ReportID=85. Published February 11, 2008. Accessed Thursday, October 23, 2008.
The Burdens of Comanagement
It may be time for hospitalists to rethink their co-management relationships, says Eric Siegal, MD, chair of the Society of Hospital Medicine’s Public Policy Committee. Co-management is a mainstay of hospital medicine, but “recent, albeit limited evidence suggests hospitalist consultation and co-management may not be as effective as originally anticipated,” Dr. Siegal writes in this month’s Journal of Hospital Medicine.
He demonstrates his point with several studies, including the Hospitalist Orthopedic Team trial, which involved 526 patients who underwent elective hip or knee surgery at the Mayo Clinic. Hospitalist intervention reduced incidence of minor complications, such as urinary tract infections, but had no effect on more serious complications; it reduced adjusted length of stay (LOS) by a modest 0.5 days but did not affect actual LOS or cost per case. On the other hand, patients admitted to the Mayo Clinic for hip fractures derived a clear benefit from hospitalist co-management: Compared to the standard orthopedic service, the hospitalist team decreased time-to-surgery and lowered LOS by 2.2 days without compromising outcomes.
These and similar findings “support the common sense notion that hospitalists most benefit patients who are sick, frail, and medically or socially complex,” Dr. Siegal writes. “As a corollary, hospitalists probably offer relatively little benefit to surgical and specialty patients who are young or have compensated medical co-morbidities and/or straightforward disposition plans.”
Dr. Siegal says he wrote the article because he realized even though hospitalists share accountability and authority for patient care with other specialists, there’s rarely a clear line defining where one physician’s responsibilities end and the other’s begin. “My intention was to make people stop and think about what they were doing, rather than just doing it,” he tells The Hospitalist.
Co-management is a good example of the phenomenon known in the military as mission creep, Dr. Siegal explains. Mission creep occurs when a project originates with well-defined and perhaps limited goals, but then expands into areas for which it was never intended.
Co-management arose during California’s managed care heyday: Hospital administrators realized surgeons were having difficulty controlling patient length of stay and managing medical co-morbidities during surgery. Enter the hospitalist, charged with coordinating the care of the acutely ill in the most effective and efficient way possible. Surgeons and other specialists liked the idea of sharing responsibility with another physician, and administrators liked the effect on the bottom line.
So, little by little, co-management evolved from a strategy for managing only the most complicated cases to a routine practice at many institutions—even when hospitalists actually added little to a patient’s care. For example, a “patient with a stable GI bleed who needs little more than an endoscopy I would argue does not need co-management,” Dr. Siegal says. In fact, he points out in his paper, inserting the hospitalist into the situation above might work against the patient if it delays the gastroenterologist’s involvement and the endoscopy. A gastroenterologist who assumes a hospitalist is running the show may pay insufficient attention to the patient, Dr. Siegal writes.
Worse than that, having more than one physician involved may actually increase the risk of medical errors if the doctors give conflicting or inconsistent orders that confuse hospital staff, patients, or their families. In many cases, the specialist is simply better qualified to do the admitting, Dr. Siegal says. When a patient comes in with a cranial bleed, “if it was my mother, I wouldn’t want me admitting her,” he says.
Unnecessary co-management also can negatively affect hospitalists themselves to the extent that the process engenders burnout or unhappiness on the job, Dr. Siegal adds. Without set parameters, specialists may assume that hospitalists will conduct all patient admits. This “devalues the hospitalist,” he writes. “People start seeing us as glorified residents,” leading to “huge job dissatisfaction.”
Co-management does offer some benefits, though they vary based on situation, he says. At institutions with a limited pool of surgeons, neurologists, or other specialists, sharing duties with hospitalists can free up specialists for cases that need their specific expertise. When specialist availability isn’t a problem, however, the real—if unspoken—purpose of co-management may be to lighten the burden for superstar specialists who attract patients, prestige, and money. The result can be overworked, stressed out hospitalists who may inadvertently neglect patients requiring care.
The solution is to give hospitalists more of a say in the types of cases they co-manage, and a clearer delineation of the responsibilities of each party involved, according to Dr. Siegal. “Sit down with the specialists and revisit where you are,” he says. He also suggests calling on hospital administrators, if necessary, to mollify specialists who might dislike the idea of a change.
After all, Dr. Siegal warns, “just showing up to co-manage doesn’t mean you’re doing anything to help the patient. You should have definable outcomes that can help you say, “‘This is better.’” TH
Norra MacReady is a medical writer based in California.
It may be time for hospitalists to rethink their co-management relationships, says Eric Siegal, MD, chair of the Society of Hospital Medicine’s Public Policy Committee. Co-management is a mainstay of hospital medicine, but “recent, albeit limited evidence suggests hospitalist consultation and co-management may not be as effective as originally anticipated,” Dr. Siegal writes in this month’s Journal of Hospital Medicine.
He demonstrates his point with several studies, including the Hospitalist Orthopedic Team trial, which involved 526 patients who underwent elective hip or knee surgery at the Mayo Clinic. Hospitalist intervention reduced incidence of minor complications, such as urinary tract infections, but had no effect on more serious complications; it reduced adjusted length of stay (LOS) by a modest 0.5 days but did not affect actual LOS or cost per case. On the other hand, patients admitted to the Mayo Clinic for hip fractures derived a clear benefit from hospitalist co-management: Compared to the standard orthopedic service, the hospitalist team decreased time-to-surgery and lowered LOS by 2.2 days without compromising outcomes.
These and similar findings “support the common sense notion that hospitalists most benefit patients who are sick, frail, and medically or socially complex,” Dr. Siegal writes. “As a corollary, hospitalists probably offer relatively little benefit to surgical and specialty patients who are young or have compensated medical co-morbidities and/or straightforward disposition plans.”
Dr. Siegal says he wrote the article because he realized even though hospitalists share accountability and authority for patient care with other specialists, there’s rarely a clear line defining where one physician’s responsibilities end and the other’s begin. “My intention was to make people stop and think about what they were doing, rather than just doing it,” he tells The Hospitalist.
Co-management is a good example of the phenomenon known in the military as mission creep, Dr. Siegal explains. Mission creep occurs when a project originates with well-defined and perhaps limited goals, but then expands into areas for which it was never intended.
Co-management arose during California’s managed care heyday: Hospital administrators realized surgeons were having difficulty controlling patient length of stay and managing medical co-morbidities during surgery. Enter the hospitalist, charged with coordinating the care of the acutely ill in the most effective and efficient way possible. Surgeons and other specialists liked the idea of sharing responsibility with another physician, and administrators liked the effect on the bottom line.
So, little by little, co-management evolved from a strategy for managing only the most complicated cases to a routine practice at many institutions—even when hospitalists actually added little to a patient’s care. For example, a “patient with a stable GI bleed who needs little more than an endoscopy I would argue does not need co-management,” Dr. Siegal says. In fact, he points out in his paper, inserting the hospitalist into the situation above might work against the patient if it delays the gastroenterologist’s involvement and the endoscopy. A gastroenterologist who assumes a hospitalist is running the show may pay insufficient attention to the patient, Dr. Siegal writes.
Worse than that, having more than one physician involved may actually increase the risk of medical errors if the doctors give conflicting or inconsistent orders that confuse hospital staff, patients, or their families. In many cases, the specialist is simply better qualified to do the admitting, Dr. Siegal says. When a patient comes in with a cranial bleed, “if it was my mother, I wouldn’t want me admitting her,” he says.
Unnecessary co-management also can negatively affect hospitalists themselves to the extent that the process engenders burnout or unhappiness on the job, Dr. Siegal adds. Without set parameters, specialists may assume that hospitalists will conduct all patient admits. This “devalues the hospitalist,” he writes. “People start seeing us as glorified residents,” leading to “huge job dissatisfaction.”
Co-management does offer some benefits, though they vary based on situation, he says. At institutions with a limited pool of surgeons, neurologists, or other specialists, sharing duties with hospitalists can free up specialists for cases that need their specific expertise. When specialist availability isn’t a problem, however, the real—if unspoken—purpose of co-management may be to lighten the burden for superstar specialists who attract patients, prestige, and money. The result can be overworked, stressed out hospitalists who may inadvertently neglect patients requiring care.
The solution is to give hospitalists more of a say in the types of cases they co-manage, and a clearer delineation of the responsibilities of each party involved, according to Dr. Siegal. “Sit down with the specialists and revisit where you are,” he says. He also suggests calling on hospital administrators, if necessary, to mollify specialists who might dislike the idea of a change.
After all, Dr. Siegal warns, “just showing up to co-manage doesn’t mean you’re doing anything to help the patient. You should have definable outcomes that can help you say, “‘This is better.’” TH
Norra MacReady is a medical writer based in California.
It may be time for hospitalists to rethink their co-management relationships, says Eric Siegal, MD, chair of the Society of Hospital Medicine’s Public Policy Committee. Co-management is a mainstay of hospital medicine, but “recent, albeit limited evidence suggests hospitalist consultation and co-management may not be as effective as originally anticipated,” Dr. Siegal writes in this month’s Journal of Hospital Medicine.
He demonstrates his point with several studies, including the Hospitalist Orthopedic Team trial, which involved 526 patients who underwent elective hip or knee surgery at the Mayo Clinic. Hospitalist intervention reduced incidence of minor complications, such as urinary tract infections, but had no effect on more serious complications; it reduced adjusted length of stay (LOS) by a modest 0.5 days but did not affect actual LOS or cost per case. On the other hand, patients admitted to the Mayo Clinic for hip fractures derived a clear benefit from hospitalist co-management: Compared to the standard orthopedic service, the hospitalist team decreased time-to-surgery and lowered LOS by 2.2 days without compromising outcomes.
These and similar findings “support the common sense notion that hospitalists most benefit patients who are sick, frail, and medically or socially complex,” Dr. Siegal writes. “As a corollary, hospitalists probably offer relatively little benefit to surgical and specialty patients who are young or have compensated medical co-morbidities and/or straightforward disposition plans.”
Dr. Siegal says he wrote the article because he realized even though hospitalists share accountability and authority for patient care with other specialists, there’s rarely a clear line defining where one physician’s responsibilities end and the other’s begin. “My intention was to make people stop and think about what they were doing, rather than just doing it,” he tells The Hospitalist.
Co-management is a good example of the phenomenon known in the military as mission creep, Dr. Siegal explains. Mission creep occurs when a project originates with well-defined and perhaps limited goals, but then expands into areas for which it was never intended.
Co-management arose during California’s managed care heyday: Hospital administrators realized surgeons were having difficulty controlling patient length of stay and managing medical co-morbidities during surgery. Enter the hospitalist, charged with coordinating the care of the acutely ill in the most effective and efficient way possible. Surgeons and other specialists liked the idea of sharing responsibility with another physician, and administrators liked the effect on the bottom line.
So, little by little, co-management evolved from a strategy for managing only the most complicated cases to a routine practice at many institutions—even when hospitalists actually added little to a patient’s care. For example, a “patient with a stable GI bleed who needs little more than an endoscopy I would argue does not need co-management,” Dr. Siegal says. In fact, he points out in his paper, inserting the hospitalist into the situation above might work against the patient if it delays the gastroenterologist’s involvement and the endoscopy. A gastroenterologist who assumes a hospitalist is running the show may pay insufficient attention to the patient, Dr. Siegal writes.
Worse than that, having more than one physician involved may actually increase the risk of medical errors if the doctors give conflicting or inconsistent orders that confuse hospital staff, patients, or their families. In many cases, the specialist is simply better qualified to do the admitting, Dr. Siegal says. When a patient comes in with a cranial bleed, “if it was my mother, I wouldn’t want me admitting her,” he says.
Unnecessary co-management also can negatively affect hospitalists themselves to the extent that the process engenders burnout or unhappiness on the job, Dr. Siegal adds. Without set parameters, specialists may assume that hospitalists will conduct all patient admits. This “devalues the hospitalist,” he writes. “People start seeing us as glorified residents,” leading to “huge job dissatisfaction.”
Co-management does offer some benefits, though they vary based on situation, he says. At institutions with a limited pool of surgeons, neurologists, or other specialists, sharing duties with hospitalists can free up specialists for cases that need their specific expertise. When specialist availability isn’t a problem, however, the real—if unspoken—purpose of co-management may be to lighten the burden for superstar specialists who attract patients, prestige, and money. The result can be overworked, stressed out hospitalists who may inadvertently neglect patients requiring care.
The solution is to give hospitalists more of a say in the types of cases they co-manage, and a clearer delineation of the responsibilities of each party involved, according to Dr. Siegal. “Sit down with the specialists and revisit where you are,” he says. He also suggests calling on hospital administrators, if necessary, to mollify specialists who might dislike the idea of a change.
After all, Dr. Siegal warns, “just showing up to co-manage doesn’t mean you’re doing anything to help the patient. You should have definable outcomes that can help you say, “‘This is better.’” TH
Norra MacReady is a medical writer based in California.
Use Outside Help
Addressing the clinical and political issues raised by the use of non-housestaff services is one of the biggest challenges facing hospitalists at academic medical centers, according to a paper in this month’s issue of the Journal of Hospital Medicine.
Lead author Niraj Sehgal, MD, assistant clinical professor of medicine at the University of California, San Francisco (UCSF), and colleagues studied the non-housestaff services at five academic medical centers around the United States to identify what it takes to make the best use of non-housestaff services.
Reliance on these services will grow largely because of restrictions established in 2003 by the Accreditation Council of Graduate Medical Education (ACGME), which limit residents to an 80-hour workweek.
What’s more, it is possible that the ACGME may cut hours even more, given that many other countries have lower restrictions.
In other words, “most academic medical centers now realize residents no longer will be providing as much patient care as they used to,” Dr. Sehgal says.
For example, at UCSF, residents’ hours have been reduced by one-third since the restrictions were established. One way to handle the situation was to reduce the number of patient-hours per resident.
However, at the same time that ruling went into effect, UCSF also increased the number of beds in its hospital. In an effort to determine who is best suited to care for these patients, UCSF and other academic centers turned to non-housestaff services to pick up the slack. “Every residency program has struggled with different models,” he explains.
In their paper, Dr. Sehgal and his colleagues identify nine questions to consider in developing non-housestaff medicine services. The questions reflect key challenges facing medical centers that are building these services, such as:
- System equities: Avoid creating a two-tiered system in which non-housestaff hospitalists who mostly provide clinical care are viewed as second-class citizens compared with academic hospitalists, who also teach and conduct research. This also raises the question of how to define an academic hospitalist;
- Define the patient mix: Should non-housestaff physicians handle less acute patients, specific patient populations, or all patients above the limit for residents?;
- Recruitment and retention: Academic centers may have to offer non-housestaff hospitalists incentives, such as teaching or research opportunities, or financial rewards such as student loan forgiveness, to attract talented clinicians; and
- Compensation and incentives: This should reflect all aspects of the physician’s job, including quality improvement efforts, research activities, and excellence in teaching, as well as clinical productivity.
“How these questions are answered is often driven by local factors, such as the vision of local leadership and the availability of important resources,” Dr. Sehgal and his coauthors write. “Nevertheless, it is important for hospitals to share their experiences since best practices remain unclear.”
To explore how different centers and services address these issues, they compared the non-housestaff medicine services at Brigham and Women’s Hospital in Boston, Emory University in Atlanta, the University of Michigan in Ann Arbor, Northwestern University Medical Center in Chicago, and UCSF. The information was obtained from representatives at each center and was current as of July 2007.
The services ranged in age from two to five years old and covered 168 to 212 clinical days per year, or 15 to 20 shifts per month. Depending on the number of hospitalists in the service, they saw anywhere from 12 to 95 patients per day.
Further, they all provided coverage for 50% of weekends. For night coverage, one service used dedicated nocturnists, two relied exclusively on moonlighters, and the remainder split coverage between the two.
All the services were located within the university hospital, except for the one at UCSF, which was at an outlying affiliated hospital.
Compensation for non-housestaff hospitalists matched that of staff physicians at two hospitals; the other three hospitals offered non-housestaff physicians some type of financial incentive, either in the form of higher salary, student loan forgiveness, or a combination of the two.
This is an interesting era for hospitalists, who are striving to carve an academic niche for themselves while still performing their clinical duties, Dr. Sehgal notes.
Among the ways they can achieve that is by becoming more involved in other areas of medical center operations, such as information technology, quality and system improvements, and committee work.
Handled properly, these opportunities to collaborate can increase hospitalist prestige and visibility, as they become more involved in hospital leadership and research and share management responsibilities with their medical and surgical colleagues.
Smoothly integrating non-housestaff services into day-to-day function is another opportunity for hospitalists to demonstrate their leadership skills, because the use of these services will increase, Dr. Sehgal adds. This makes it necessary to keep studying the outside services and identifying the ways in which they differ from their housestaff counterparts in order to maximize their contributions.
This study shows that creating non-housestaff services involves the consideration of several important elements, including the patients to be seen by those services, and staffing issues, such as whether the service should be composed exclusively of hospitalists, or if other specialties also should be included.
Hospitalists will have to monitor quality control issues and staff retention, and make sure a two-tiered system does not develop between housestaff and non-housestaff physicians. “So far, there has been very little written about this,” Dr. Sehgal concludes. TH
Norra MacReady is a medical writer based in California.
Addressing the clinical and political issues raised by the use of non-housestaff services is one of the biggest challenges facing hospitalists at academic medical centers, according to a paper in this month’s issue of the Journal of Hospital Medicine.
Lead author Niraj Sehgal, MD, assistant clinical professor of medicine at the University of California, San Francisco (UCSF), and colleagues studied the non-housestaff services at five academic medical centers around the United States to identify what it takes to make the best use of non-housestaff services.
Reliance on these services will grow largely because of restrictions established in 2003 by the Accreditation Council of Graduate Medical Education (ACGME), which limit residents to an 80-hour workweek.
What’s more, it is possible that the ACGME may cut hours even more, given that many other countries have lower restrictions.
In other words, “most academic medical centers now realize residents no longer will be providing as much patient care as they used to,” Dr. Sehgal says.
For example, at UCSF, residents’ hours have been reduced by one-third since the restrictions were established. One way to handle the situation was to reduce the number of patient-hours per resident.
However, at the same time that ruling went into effect, UCSF also increased the number of beds in its hospital. In an effort to determine who is best suited to care for these patients, UCSF and other academic centers turned to non-housestaff services to pick up the slack. “Every residency program has struggled with different models,” he explains.
In their paper, Dr. Sehgal and his colleagues identify nine questions to consider in developing non-housestaff medicine services. The questions reflect key challenges facing medical centers that are building these services, such as:
- System equities: Avoid creating a two-tiered system in which non-housestaff hospitalists who mostly provide clinical care are viewed as second-class citizens compared with academic hospitalists, who also teach and conduct research. This also raises the question of how to define an academic hospitalist;
- Define the patient mix: Should non-housestaff physicians handle less acute patients, specific patient populations, or all patients above the limit for residents?;
- Recruitment and retention: Academic centers may have to offer non-housestaff hospitalists incentives, such as teaching or research opportunities, or financial rewards such as student loan forgiveness, to attract talented clinicians; and
- Compensation and incentives: This should reflect all aspects of the physician’s job, including quality improvement efforts, research activities, and excellence in teaching, as well as clinical productivity.
“How these questions are answered is often driven by local factors, such as the vision of local leadership and the availability of important resources,” Dr. Sehgal and his coauthors write. “Nevertheless, it is important for hospitals to share their experiences since best practices remain unclear.”
To explore how different centers and services address these issues, they compared the non-housestaff medicine services at Brigham and Women’s Hospital in Boston, Emory University in Atlanta, the University of Michigan in Ann Arbor, Northwestern University Medical Center in Chicago, and UCSF. The information was obtained from representatives at each center and was current as of July 2007.
The services ranged in age from two to five years old and covered 168 to 212 clinical days per year, or 15 to 20 shifts per month. Depending on the number of hospitalists in the service, they saw anywhere from 12 to 95 patients per day.
Further, they all provided coverage for 50% of weekends. For night coverage, one service used dedicated nocturnists, two relied exclusively on moonlighters, and the remainder split coverage between the two.
All the services were located within the university hospital, except for the one at UCSF, which was at an outlying affiliated hospital.
Compensation for non-housestaff hospitalists matched that of staff physicians at two hospitals; the other three hospitals offered non-housestaff physicians some type of financial incentive, either in the form of higher salary, student loan forgiveness, or a combination of the two.
This is an interesting era for hospitalists, who are striving to carve an academic niche for themselves while still performing their clinical duties, Dr. Sehgal notes.
Among the ways they can achieve that is by becoming more involved in other areas of medical center operations, such as information technology, quality and system improvements, and committee work.
Handled properly, these opportunities to collaborate can increase hospitalist prestige and visibility, as they become more involved in hospital leadership and research and share management responsibilities with their medical and surgical colleagues.
Smoothly integrating non-housestaff services into day-to-day function is another opportunity for hospitalists to demonstrate their leadership skills, because the use of these services will increase, Dr. Sehgal adds. This makes it necessary to keep studying the outside services and identifying the ways in which they differ from their housestaff counterparts in order to maximize their contributions.
This study shows that creating non-housestaff services involves the consideration of several important elements, including the patients to be seen by those services, and staffing issues, such as whether the service should be composed exclusively of hospitalists, or if other specialties also should be included.
Hospitalists will have to monitor quality control issues and staff retention, and make sure a two-tiered system does not develop between housestaff and non-housestaff physicians. “So far, there has been very little written about this,” Dr. Sehgal concludes. TH
Norra MacReady is a medical writer based in California.
Addressing the clinical and political issues raised by the use of non-housestaff services is one of the biggest challenges facing hospitalists at academic medical centers, according to a paper in this month’s issue of the Journal of Hospital Medicine.
Lead author Niraj Sehgal, MD, assistant clinical professor of medicine at the University of California, San Francisco (UCSF), and colleagues studied the non-housestaff services at five academic medical centers around the United States to identify what it takes to make the best use of non-housestaff services.
Reliance on these services will grow largely because of restrictions established in 2003 by the Accreditation Council of Graduate Medical Education (ACGME), which limit residents to an 80-hour workweek.
What’s more, it is possible that the ACGME may cut hours even more, given that many other countries have lower restrictions.
In other words, “most academic medical centers now realize residents no longer will be providing as much patient care as they used to,” Dr. Sehgal says.
For example, at UCSF, residents’ hours have been reduced by one-third since the restrictions were established. One way to handle the situation was to reduce the number of patient-hours per resident.
However, at the same time that ruling went into effect, UCSF also increased the number of beds in its hospital. In an effort to determine who is best suited to care for these patients, UCSF and other academic centers turned to non-housestaff services to pick up the slack. “Every residency program has struggled with different models,” he explains.
In their paper, Dr. Sehgal and his colleagues identify nine questions to consider in developing non-housestaff medicine services. The questions reflect key challenges facing medical centers that are building these services, such as:
- System equities: Avoid creating a two-tiered system in which non-housestaff hospitalists who mostly provide clinical care are viewed as second-class citizens compared with academic hospitalists, who also teach and conduct research. This also raises the question of how to define an academic hospitalist;
- Define the patient mix: Should non-housestaff physicians handle less acute patients, specific patient populations, or all patients above the limit for residents?;
- Recruitment and retention: Academic centers may have to offer non-housestaff hospitalists incentives, such as teaching or research opportunities, or financial rewards such as student loan forgiveness, to attract talented clinicians; and
- Compensation and incentives: This should reflect all aspects of the physician’s job, including quality improvement efforts, research activities, and excellence in teaching, as well as clinical productivity.
“How these questions are answered is often driven by local factors, such as the vision of local leadership and the availability of important resources,” Dr. Sehgal and his coauthors write. “Nevertheless, it is important for hospitals to share their experiences since best practices remain unclear.”
To explore how different centers and services address these issues, they compared the non-housestaff medicine services at Brigham and Women’s Hospital in Boston, Emory University in Atlanta, the University of Michigan in Ann Arbor, Northwestern University Medical Center in Chicago, and UCSF. The information was obtained from representatives at each center and was current as of July 2007.
The services ranged in age from two to five years old and covered 168 to 212 clinical days per year, or 15 to 20 shifts per month. Depending on the number of hospitalists in the service, they saw anywhere from 12 to 95 patients per day.
Further, they all provided coverage for 50% of weekends. For night coverage, one service used dedicated nocturnists, two relied exclusively on moonlighters, and the remainder split coverage between the two.
All the services were located within the university hospital, except for the one at UCSF, which was at an outlying affiliated hospital.
Compensation for non-housestaff hospitalists matched that of staff physicians at two hospitals; the other three hospitals offered non-housestaff physicians some type of financial incentive, either in the form of higher salary, student loan forgiveness, or a combination of the two.
This is an interesting era for hospitalists, who are striving to carve an academic niche for themselves while still performing their clinical duties, Dr. Sehgal notes.
Among the ways they can achieve that is by becoming more involved in other areas of medical center operations, such as information technology, quality and system improvements, and committee work.
Handled properly, these opportunities to collaborate can increase hospitalist prestige and visibility, as they become more involved in hospital leadership and research and share management responsibilities with their medical and surgical colleagues.
Smoothly integrating non-housestaff services into day-to-day function is another opportunity for hospitalists to demonstrate their leadership skills, because the use of these services will increase, Dr. Sehgal adds. This makes it necessary to keep studying the outside services and identifying the ways in which they differ from their housestaff counterparts in order to maximize their contributions.
This study shows that creating non-housestaff services involves the consideration of several important elements, including the patients to be seen by those services, and staffing issues, such as whether the service should be composed exclusively of hospitalists, or if other specialties also should be included.
Hospitalists will have to monitor quality control issues and staff retention, and make sure a two-tiered system does not develop between housestaff and non-housestaff physicians. “So far, there has been very little written about this,” Dr. Sehgal concludes. TH
Norra MacReady is a medical writer based in California.
The Specialist Advantage
The speed at which hospital medicine is growing is leaving many hospitalists in uncharted waters as they try to balance clinical practice and academic activities such as teaching, quality improvement, and research.
“Hospitalists often have great ideas but lack the resources to carry them out,” said Scott Flanders, MD, SHM president-elect, clinical associate professor of internal medicine, and director of the hospitalist program at the University of Michigan Health System, Ann Arbor.
Also, hospitalists do not always recognize the role of the subspecialist in diagnosing and treating complex patients—nor the advantages those specialists bring to designing and supporting clinical research. Given the nature of their education, specialists have a deeper understanding than hospitalists of the pathophysiologic concepts and scientific principles underlying important clinical questions, and are more likely to have had fellowship training that includes clinical research experience. They’re likely to be more adept at navigating outside bureaucracies to obtain grants for disease-based investigation.
All in all, specialist participation in hospital-based clinical research projects may improve project feasibility, increase the chances of obtaining money, and allow for wider dissemination of the results than if these projects had been undertaken by hospitalists alone.
“At large institutions, having hospitalists partner with clinical subspecialists could enhance patient enrollment and enhance funding opportunities, because subspecialists have a lot of credibility with funding agencies,” Dr. Flanders says.
Yet, clinical research programs performed by hospitalists and hospital medicine programs still are in an embryonic stage. In this month’s issue of the Journal of Hospital Medicine, he and his colleagues describe a new program for accelerating clinical and translational research by having hospitalists team with subspecialist physicians and other healthcare professionals to ask and answer novel research questions.
SHARP Solution
In the Specialist-Hospitalist Allied Research Program (SHARP), an academic hospitalist and an academic cardiologist serve as principle and co-principle investigators, respectively. Together, they direct a team of supporting personnel, including a hospitalist investigator, clinical research nurse, research associate, and clinical epidemiologist.
The program began in 2006, with the goal of facilitating multicenter, intervention-based clinical trials. Other aims include enhancing patient participation and supporting pilot projects that would generate enough data to attract money for more in-depth studies. The program is paid for three years by the department of internal medicine with revenues generated for the hospital medicine division.
Through SHARP, there will be “a pool of dollars to support a program and provide an infrastructure for a project,” Dr. Flanders says. “Otherwise, each new project would require a new team to find funding [and] perform data analysis.”
SHARP is, in part, an acknowledgment of the increasingly complex nature of clinical research, Dr. Flanders says. “Many big research projects involve more than one specialty, so there will always be a need to collaborate.”
In a sense, the program is an extension of what hospitalists do already. “Hospitalist work in general is often collaborative and team-based,” Dr. Flanders notes. “We frequently work with nurses and other hospital-based staff members.”
How it Works
A steering committee chaired by the two principle investigators and consisting of academic administrators from the University of Michigan will identify appropriate research projects, determine the best allocation of resources, and help the team overcome the bureaucratic hurdles that inevitably arise in any project that includes multiple departments and institutions.
The program has two opening projects. One is aimed at reducing the incidence of false-positive blood cultures. Right now, as many as half of all the blood cultures that test positive at the University of Michigan turn out to be contaminated. The SHARP team has started a randomized, controlled trial to compare the effects of several different skin antiseptics on the false-positive rate, and ultimately will test more than 12,000 blood culture sets. Other key outcomes will be the quantity of additional diagnostic testing generated by positive cultures, use of resources, and associated costs. Mortality and length of stay also will be examined as secondary outcomes.
The second study has been completed, and data analysis has begun. It examined the role of an inpatient clinical pharmacist in preventing medication errors related to hospital discharge among elderly patients.
“In our experience at the University of Michigan, patients frequently have medication-related adverse events after discharge because they do not understand what medications they should be taking, what they are used for, how to manage side effects, or whom to call with problems,” Dr. Flanders and his colleagues wrote. “In addition, predictable medication-related issues (such as ability to pay for a medicine or expected serum electrolyte changes with newly added medications) are not universally anticipated.”
The pharmacist divided his time between a non-resident hospitalist service and a resident general medicine service, focusing on high-risk patients older than 65. Those patients received pre-discharge counseling and post-discharge follow-up calls from the pharmacist within 72 hours and 30 days of leaving the hospital. The key outcomes include medication issues and actions taken by the pharmacist at or after discharge, as well as clinical outcomes such as emergency department visits, readmission rates, and healthcare-related costs.
So far, the biggest challenge faced by the hospitalists interested in SHARP simply has been finding enough hours in the day for it. One of the program’s goals is to generate grant money to hire supporting staff, but right now the doctors must participate on their own time. Nevertheless, says Dr. Flanders, the response to the program has been positive. “It facilitates the small, difficult steps [in funding and implementing research] along the way,” he says. “People have been pleasantly surprised that it works as well as it does.”TH
Norra MacReady is a medical writer based in California.
The speed at which hospital medicine is growing is leaving many hospitalists in uncharted waters as they try to balance clinical practice and academic activities such as teaching, quality improvement, and research.
“Hospitalists often have great ideas but lack the resources to carry them out,” said Scott Flanders, MD, SHM president-elect, clinical associate professor of internal medicine, and director of the hospitalist program at the University of Michigan Health System, Ann Arbor.
Also, hospitalists do not always recognize the role of the subspecialist in diagnosing and treating complex patients—nor the advantages those specialists bring to designing and supporting clinical research. Given the nature of their education, specialists have a deeper understanding than hospitalists of the pathophysiologic concepts and scientific principles underlying important clinical questions, and are more likely to have had fellowship training that includes clinical research experience. They’re likely to be more adept at navigating outside bureaucracies to obtain grants for disease-based investigation.
All in all, specialist participation in hospital-based clinical research projects may improve project feasibility, increase the chances of obtaining money, and allow for wider dissemination of the results than if these projects had been undertaken by hospitalists alone.
“At large institutions, having hospitalists partner with clinical subspecialists could enhance patient enrollment and enhance funding opportunities, because subspecialists have a lot of credibility with funding agencies,” Dr. Flanders says.
Yet, clinical research programs performed by hospitalists and hospital medicine programs still are in an embryonic stage. In this month’s issue of the Journal of Hospital Medicine, he and his colleagues describe a new program for accelerating clinical and translational research by having hospitalists team with subspecialist physicians and other healthcare professionals to ask and answer novel research questions.
SHARP Solution
In the Specialist-Hospitalist Allied Research Program (SHARP), an academic hospitalist and an academic cardiologist serve as principle and co-principle investigators, respectively. Together, they direct a team of supporting personnel, including a hospitalist investigator, clinical research nurse, research associate, and clinical epidemiologist.
The program began in 2006, with the goal of facilitating multicenter, intervention-based clinical trials. Other aims include enhancing patient participation and supporting pilot projects that would generate enough data to attract money for more in-depth studies. The program is paid for three years by the department of internal medicine with revenues generated for the hospital medicine division.
Through SHARP, there will be “a pool of dollars to support a program and provide an infrastructure for a project,” Dr. Flanders says. “Otherwise, each new project would require a new team to find funding [and] perform data analysis.”
SHARP is, in part, an acknowledgment of the increasingly complex nature of clinical research, Dr. Flanders says. “Many big research projects involve more than one specialty, so there will always be a need to collaborate.”
In a sense, the program is an extension of what hospitalists do already. “Hospitalist work in general is often collaborative and team-based,” Dr. Flanders notes. “We frequently work with nurses and other hospital-based staff members.”
How it Works
A steering committee chaired by the two principle investigators and consisting of academic administrators from the University of Michigan will identify appropriate research projects, determine the best allocation of resources, and help the team overcome the bureaucratic hurdles that inevitably arise in any project that includes multiple departments and institutions.
The program has two opening projects. One is aimed at reducing the incidence of false-positive blood cultures. Right now, as many as half of all the blood cultures that test positive at the University of Michigan turn out to be contaminated. The SHARP team has started a randomized, controlled trial to compare the effects of several different skin antiseptics on the false-positive rate, and ultimately will test more than 12,000 blood culture sets. Other key outcomes will be the quantity of additional diagnostic testing generated by positive cultures, use of resources, and associated costs. Mortality and length of stay also will be examined as secondary outcomes.
The second study has been completed, and data analysis has begun. It examined the role of an inpatient clinical pharmacist in preventing medication errors related to hospital discharge among elderly patients.
“In our experience at the University of Michigan, patients frequently have medication-related adverse events after discharge because they do not understand what medications they should be taking, what they are used for, how to manage side effects, or whom to call with problems,” Dr. Flanders and his colleagues wrote. “In addition, predictable medication-related issues (such as ability to pay for a medicine or expected serum electrolyte changes with newly added medications) are not universally anticipated.”
The pharmacist divided his time between a non-resident hospitalist service and a resident general medicine service, focusing on high-risk patients older than 65. Those patients received pre-discharge counseling and post-discharge follow-up calls from the pharmacist within 72 hours and 30 days of leaving the hospital. The key outcomes include medication issues and actions taken by the pharmacist at or after discharge, as well as clinical outcomes such as emergency department visits, readmission rates, and healthcare-related costs.
So far, the biggest challenge faced by the hospitalists interested in SHARP simply has been finding enough hours in the day for it. One of the program’s goals is to generate grant money to hire supporting staff, but right now the doctors must participate on their own time. Nevertheless, says Dr. Flanders, the response to the program has been positive. “It facilitates the small, difficult steps [in funding and implementing research] along the way,” he says. “People have been pleasantly surprised that it works as well as it does.”TH
Norra MacReady is a medical writer based in California.
The speed at which hospital medicine is growing is leaving many hospitalists in uncharted waters as they try to balance clinical practice and academic activities such as teaching, quality improvement, and research.
“Hospitalists often have great ideas but lack the resources to carry them out,” said Scott Flanders, MD, SHM president-elect, clinical associate professor of internal medicine, and director of the hospitalist program at the University of Michigan Health System, Ann Arbor.
Also, hospitalists do not always recognize the role of the subspecialist in diagnosing and treating complex patients—nor the advantages those specialists bring to designing and supporting clinical research. Given the nature of their education, specialists have a deeper understanding than hospitalists of the pathophysiologic concepts and scientific principles underlying important clinical questions, and are more likely to have had fellowship training that includes clinical research experience. They’re likely to be more adept at navigating outside bureaucracies to obtain grants for disease-based investigation.
All in all, specialist participation in hospital-based clinical research projects may improve project feasibility, increase the chances of obtaining money, and allow for wider dissemination of the results than if these projects had been undertaken by hospitalists alone.
“At large institutions, having hospitalists partner with clinical subspecialists could enhance patient enrollment and enhance funding opportunities, because subspecialists have a lot of credibility with funding agencies,” Dr. Flanders says.
Yet, clinical research programs performed by hospitalists and hospital medicine programs still are in an embryonic stage. In this month’s issue of the Journal of Hospital Medicine, he and his colleagues describe a new program for accelerating clinical and translational research by having hospitalists team with subspecialist physicians and other healthcare professionals to ask and answer novel research questions.
SHARP Solution
In the Specialist-Hospitalist Allied Research Program (SHARP), an academic hospitalist and an academic cardiologist serve as principle and co-principle investigators, respectively. Together, they direct a team of supporting personnel, including a hospitalist investigator, clinical research nurse, research associate, and clinical epidemiologist.
The program began in 2006, with the goal of facilitating multicenter, intervention-based clinical trials. Other aims include enhancing patient participation and supporting pilot projects that would generate enough data to attract money for more in-depth studies. The program is paid for three years by the department of internal medicine with revenues generated for the hospital medicine division.
Through SHARP, there will be “a pool of dollars to support a program and provide an infrastructure for a project,” Dr. Flanders says. “Otherwise, each new project would require a new team to find funding [and] perform data analysis.”
SHARP is, in part, an acknowledgment of the increasingly complex nature of clinical research, Dr. Flanders says. “Many big research projects involve more than one specialty, so there will always be a need to collaborate.”
In a sense, the program is an extension of what hospitalists do already. “Hospitalist work in general is often collaborative and team-based,” Dr. Flanders notes. “We frequently work with nurses and other hospital-based staff members.”
How it Works
A steering committee chaired by the two principle investigators and consisting of academic administrators from the University of Michigan will identify appropriate research projects, determine the best allocation of resources, and help the team overcome the bureaucratic hurdles that inevitably arise in any project that includes multiple departments and institutions.
The program has two opening projects. One is aimed at reducing the incidence of false-positive blood cultures. Right now, as many as half of all the blood cultures that test positive at the University of Michigan turn out to be contaminated. The SHARP team has started a randomized, controlled trial to compare the effects of several different skin antiseptics on the false-positive rate, and ultimately will test more than 12,000 blood culture sets. Other key outcomes will be the quantity of additional diagnostic testing generated by positive cultures, use of resources, and associated costs. Mortality and length of stay also will be examined as secondary outcomes.
The second study has been completed, and data analysis has begun. It examined the role of an inpatient clinical pharmacist in preventing medication errors related to hospital discharge among elderly patients.
“In our experience at the University of Michigan, patients frequently have medication-related adverse events after discharge because they do not understand what medications they should be taking, what they are used for, how to manage side effects, or whom to call with problems,” Dr. Flanders and his colleagues wrote. “In addition, predictable medication-related issues (such as ability to pay for a medicine or expected serum electrolyte changes with newly added medications) are not universally anticipated.”
The pharmacist divided his time between a non-resident hospitalist service and a resident general medicine service, focusing on high-risk patients older than 65. Those patients received pre-discharge counseling and post-discharge follow-up calls from the pharmacist within 72 hours and 30 days of leaving the hospital. The key outcomes include medication issues and actions taken by the pharmacist at or after discharge, as well as clinical outcomes such as emergency department visits, readmission rates, and healthcare-related costs.
So far, the biggest challenge faced by the hospitalists interested in SHARP simply has been finding enough hours in the day for it. One of the program’s goals is to generate grant money to hire supporting staff, but right now the doctors must participate on their own time. Nevertheless, says Dr. Flanders, the response to the program has been positive. “It facilitates the small, difficult steps [in funding and implementing research] along the way,” he says. “People have been pleasantly surprised that it works as well as it does.”TH
Norra MacReady is a medical writer based in California.
Wake-up Call for Nurses
Work schedules and levels of sleepiness among medical residents long have been a source of concern. A pilot study in the May-June issue of the Journal of Hospital Medicine shows nurses—especially those in high-stress specialties like intensive care—also could benefit from an extra 40 winks.
Lead author Salim Surani, MD, of the Baylor College of Medicine, and colleagues compared sleepiness in 10 intensive care unit (ICU) nurses to those of 10 floor nurses, all of whom worked night shifts beginning at 7 p.m. and ending at 7 a.m.
Sleepiness was assessed in three ways. On the morning after the third or fourth shift, each nurse underwent a modified version of the Multiple Sleep Latency Test (MSLT), which measured the time it took for them to fall asleep during two nap periods, one at 7:15 a.m., another at 8:30 a.m. Sleep latency less than five minutes is considered severely pathological. Before the MSLT, they filled out the Epworth Sleepiness Scale (ESS), a questionnaire designed to explore the subject’s chances of falling asleep under six different scenarios. The ESS is considered a well-standardized and validated measure of subjective sleepiness, with a score more than eight considered abnormal.

Finally, for the week leading up to the day of the test, the nurses maintained a sleep diary, recording their bedtimes, wake times, daytime naps, nocturnal awakenings, and comments about their feelings of sleepiness. Each participant received a $25 gift certificate at the completion of the study.
ICU nurses were chosen because they typically “must make extremely critical judgments; they must be alert enough to recognize abnormalities in their patients and react quickly enough when something goes wrong,” coauthor Shyamsunder Subramanian, MD, says. These demands take their toll, as some studies show ICU nurse burnout rates as high as 33%, leading the investigators to hypothesize that ICU nurses also would report feeling sleepier and having poorer sleep quality than floor nurses.
The results bore out the hypothesis. Among ICU nurses, the mean ESS score was 8.7, compared with a mean of 5.6 for the floor nurses (p=0.042). All in all, seven of the 10 ICU nurses had a score more than eight, compared with only two of the 10 floor nurses (p<0.005).
Similarly, the mean MSLT for the first nap period was 4.7 minutes for the ICU nurses and 10.9 minutes for the floor nurses (p=0.025), with nine of the 10 ICU nurses falling asleep in less than five minutes, compared with two of the floor nurses (p<0.005). ICU nurses also had a shorter MSLT overall, of 6.1 minutes, versus 10.6 minutes for the floor nurses, but this difference was not statistically significant. There also was no significant difference between the groups in mean nightly sleep time: ICU nurses reported a total 405 minutes, while the floor nurses clocked in at 416 minutes.
There are two probable interpretations of the data, said Dr. Subramanian, director of sleep services at Baylor. Perhaps it is simply too exhausting for people to function at a peak level of alertness, particularly in a demanding specialty like intensive care, for 12 hours. Or it could be burnout was as common among the ICU nurses in this study as it was for their colleagues in other studies, as reflected in their ESS scores, which rival the scores observed in people with depression or chronic illness and suggest a lower quality of everyday sleep. The findings most likely result from a combination of these factors, he notes.
This study is the first to evaluate sleepiness in night-shift nurses using the ESS and the MSLT, but not the first to document at least subjective reports of nurse sleepiness, the investigators wrote. The authors of a Japanese survey of 4,407 nurses estimated at least 26% of those respondents suffered from excess sleepiness, and in a survey of 502 American nurses, two-thirds said they struggled to stay awake during their shifts. Dr. Subramanian pointed out that in studies of emergency room doctors and nurses, as well as workers in other intense, high-stress occupations, vigilance dwindles and sleepiness mounts after eight and especially 10 hours.

This can have serious consequences for patients and healthcare workers alike, he warns.
Excessive sleepiness “correlates very robustly with medical errors, incorrect operation of medical equipment, and falling asleep while driving.” In fact, some hospitals provide shuttle buses to transport night-shift workers to and from work, fearing they may be too exhausted to drive.
The Accreditation Council for Graduate Medical Education (ACGME) has limited work weeks for medical residents to 80 hours and no more than 24 hours’ continuous time on duty, but “that has clearly not worked: ICU residents still are extremely sleepy even when they adhere to the ACGME regulations,” Dr. Subramanian said. He recommended no one shift last longer than eight hours, and that healthcare workers be required to demonstrate they are not sleepy when they report to work.
Dr. Subramanian and his coauthors also found the ICU nurses had a higher mean body mass index than the floor nurses, which might suggest they eat more as a way of coping with higher stress levels. “Most nurses are women, and in addition to working 12-hour shifts, they’re probably taking care of their families,” he explains. “They’re not going home and catching up on their sleep.” TH
Norra MacReady is a medical writer based in California.
Work schedules and levels of sleepiness among medical residents long have been a source of concern. A pilot study in the May-June issue of the Journal of Hospital Medicine shows nurses—especially those in high-stress specialties like intensive care—also could benefit from an extra 40 winks.
Lead author Salim Surani, MD, of the Baylor College of Medicine, and colleagues compared sleepiness in 10 intensive care unit (ICU) nurses to those of 10 floor nurses, all of whom worked night shifts beginning at 7 p.m. and ending at 7 a.m.
Sleepiness was assessed in three ways. On the morning after the third or fourth shift, each nurse underwent a modified version of the Multiple Sleep Latency Test (MSLT), which measured the time it took for them to fall asleep during two nap periods, one at 7:15 a.m., another at 8:30 a.m. Sleep latency less than five minutes is considered severely pathological. Before the MSLT, they filled out the Epworth Sleepiness Scale (ESS), a questionnaire designed to explore the subject’s chances of falling asleep under six different scenarios. The ESS is considered a well-standardized and validated measure of subjective sleepiness, with a score more than eight considered abnormal.
Finally, for the week leading up to the day of the test, the nurses maintained a sleep diary, recording their bedtimes, wake times, daytime naps, nocturnal awakenings, and comments about their feelings of sleepiness. Each participant received a $25 gift certificate at the completion of the study.
ICU nurses were chosen because they typically “must make extremely critical judgments; they must be alert enough to recognize abnormalities in their patients and react quickly enough when something goes wrong,” coauthor Shyamsunder Subramanian, MD, says. These demands take their toll, as some studies show ICU nurse burnout rates as high as 33%, leading the investigators to hypothesize that ICU nurses also would report feeling sleepier and having poorer sleep quality than floor nurses.
The results bore out the hypothesis. Among ICU nurses, the mean ESS score was 8.7, compared with a mean of 5.6 for the floor nurses (p=0.042). All in all, seven of the 10 ICU nurses had a score more than eight, compared with only two of the 10 floor nurses (p<0.005).
Similarly, the mean MSLT for the first nap period was 4.7 minutes for the ICU nurses and 10.9 minutes for the floor nurses (p=0.025), with nine of the 10 ICU nurses falling asleep in less than five minutes, compared with two of the floor nurses (p<0.005). ICU nurses also had a shorter MSLT overall, of 6.1 minutes, versus 10.6 minutes for the floor nurses, but this difference was not statistically significant. There also was no significant difference between the groups in mean nightly sleep time: ICU nurses reported a total 405 minutes, while the floor nurses clocked in at 416 minutes.
There are two probable interpretations of the data, said Dr. Subramanian, director of sleep services at Baylor. Perhaps it is simply too exhausting for people to function at a peak level of alertness, particularly in a demanding specialty like intensive care, for 12 hours. Or it could be burnout was as common among the ICU nurses in this study as it was for their colleagues in other studies, as reflected in their ESS scores, which rival the scores observed in people with depression or chronic illness and suggest a lower quality of everyday sleep. The findings most likely result from a combination of these factors, he notes.
This study is the first to evaluate sleepiness in night-shift nurses using the ESS and the MSLT, but not the first to document at least subjective reports of nurse sleepiness, the investigators wrote. The authors of a Japanese survey of 4,407 nurses estimated at least 26% of those respondents suffered from excess sleepiness, and in a survey of 502 American nurses, two-thirds said they struggled to stay awake during their shifts. Dr. Subramanian pointed out that in studies of emergency room doctors and nurses, as well as workers in other intense, high-stress occupations, vigilance dwindles and sleepiness mounts after eight and especially 10 hours.
This can have serious consequences for patients and healthcare workers alike, he warns.
Excessive sleepiness “correlates very robustly with medical errors, incorrect operation of medical equipment, and falling asleep while driving.” In fact, some hospitals provide shuttle buses to transport night-shift workers to and from work, fearing they may be too exhausted to drive.
The Accreditation Council for Graduate Medical Education (ACGME) has limited work weeks for medical residents to 80 hours and no more than 24 hours’ continuous time on duty, but “that has clearly not worked: ICU residents still are extremely sleepy even when they adhere to the ACGME regulations,” Dr. Subramanian said. He recommended no one shift last longer than eight hours, and that healthcare workers be required to demonstrate they are not sleepy when they report to work.
Dr. Subramanian and his coauthors also found the ICU nurses had a higher mean body mass index than the floor nurses, which might suggest they eat more as a way of coping with higher stress levels. “Most nurses are women, and in addition to working 12-hour shifts, they’re probably taking care of their families,” he explains. “They’re not going home and catching up on their sleep.” TH
Norra MacReady is a medical writer based in California.
Work schedules and levels of sleepiness among medical residents long have been a source of concern. A pilot study in the May-June issue of the Journal of Hospital Medicine shows nurses—especially those in high-stress specialties like intensive care—also could benefit from an extra 40 winks.
Lead author Salim Surani, MD, of the Baylor College of Medicine, and colleagues compared sleepiness in 10 intensive care unit (ICU) nurses to those of 10 floor nurses, all of whom worked night shifts beginning at 7 p.m. and ending at 7 a.m.
Sleepiness was assessed in three ways. On the morning after the third or fourth shift, each nurse underwent a modified version of the Multiple Sleep Latency Test (MSLT), which measured the time it took for them to fall asleep during two nap periods, one at 7:15 a.m., another at 8:30 a.m. Sleep latency less than five minutes is considered severely pathological. Before the MSLT, they filled out the Epworth Sleepiness Scale (ESS), a questionnaire designed to explore the subject’s chances of falling asleep under six different scenarios. The ESS is considered a well-standardized and validated measure of subjective sleepiness, with a score more than eight considered abnormal.
Finally, for the week leading up to the day of the test, the nurses maintained a sleep diary, recording their bedtimes, wake times, daytime naps, nocturnal awakenings, and comments about their feelings of sleepiness. Each participant received a $25 gift certificate at the completion of the study.
ICU nurses were chosen because they typically “must make extremely critical judgments; they must be alert enough to recognize abnormalities in their patients and react quickly enough when something goes wrong,” coauthor Shyamsunder Subramanian, MD, says. These demands take their toll, as some studies show ICU nurse burnout rates as high as 33%, leading the investigators to hypothesize that ICU nurses also would report feeling sleepier and having poorer sleep quality than floor nurses.
The results bore out the hypothesis. Among ICU nurses, the mean ESS score was 8.7, compared with a mean of 5.6 for the floor nurses (p=0.042). All in all, seven of the 10 ICU nurses had a score more than eight, compared with only two of the 10 floor nurses (p<0.005).
Similarly, the mean MSLT for the first nap period was 4.7 minutes for the ICU nurses and 10.9 minutes for the floor nurses (p=0.025), with nine of the 10 ICU nurses falling asleep in less than five minutes, compared with two of the floor nurses (p<0.005). ICU nurses also had a shorter MSLT overall, of 6.1 minutes, versus 10.6 minutes for the floor nurses, but this difference was not statistically significant. There also was no significant difference between the groups in mean nightly sleep time: ICU nurses reported a total 405 minutes, while the floor nurses clocked in at 416 minutes.
There are two probable interpretations of the data, said Dr. Subramanian, director of sleep services at Baylor. Perhaps it is simply too exhausting for people to function at a peak level of alertness, particularly in a demanding specialty like intensive care, for 12 hours. Or it could be burnout was as common among the ICU nurses in this study as it was for their colleagues in other studies, as reflected in their ESS scores, which rival the scores observed in people with depression or chronic illness and suggest a lower quality of everyday sleep. The findings most likely result from a combination of these factors, he notes.
This study is the first to evaluate sleepiness in night-shift nurses using the ESS and the MSLT, but not the first to document at least subjective reports of nurse sleepiness, the investigators wrote. The authors of a Japanese survey of 4,407 nurses estimated at least 26% of those respondents suffered from excess sleepiness, and in a survey of 502 American nurses, two-thirds said they struggled to stay awake during their shifts. Dr. Subramanian pointed out that in studies of emergency room doctors and nurses, as well as workers in other intense, high-stress occupations, vigilance dwindles and sleepiness mounts after eight and especially 10 hours.
This can have serious consequences for patients and healthcare workers alike, he warns.
Excessive sleepiness “correlates very robustly with medical errors, incorrect operation of medical equipment, and falling asleep while driving.” In fact, some hospitals provide shuttle buses to transport night-shift workers to and from work, fearing they may be too exhausted to drive.
The Accreditation Council for Graduate Medical Education (ACGME) has limited work weeks for medical residents to 80 hours and no more than 24 hours’ continuous time on duty, but “that has clearly not worked: ICU residents still are extremely sleepy even when they adhere to the ACGME regulations,” Dr. Subramanian said. He recommended no one shift last longer than eight hours, and that healthcare workers be required to demonstrate they are not sleepy when they report to work.
Dr. Subramanian and his coauthors also found the ICU nurses had a higher mean body mass index than the floor nurses, which might suggest they eat more as a way of coping with higher stress levels. “Most nurses are women, and in addition to working 12-hour shifts, they’re probably taking care of their families,” he explains. “They’re not going home and catching up on their sleep.” TH
Norra MacReady is a medical writer based in California.
Nurse Ratios Suffer
Several studies have linked lower nurse-to-patient ratios with fewer medical errors and deaths, better overall treatment, and reduced rates of nurse burnout. These findings led California, in 1999, to pass the country’s first law mandating a minimum nurse-to-patient staffing ratio.
By 2004, the mandated ratio was one licensed nurse for every six patients; that was decreased in 2005 to one nurse for every five patients. Since then, similar bills have been passed or proposed in at least 25 more states. The benefits to patients and nurses of these improved ratios are clear. However, their effect on hospitalists, other staff members, and hospitals have not been widely studied. Further, the mandates often do not come with additional money to implement them.
In this month’s issue of the Journal of Hospital Medicine, Patrick Conway, MD, and colleagues examine nurse staffing trends in California hospitals since the mandate went into effect. They were particularly interested in what they called “safety net” hospitals: urban, government-owned, resource-poor institutions with at least 36% of patients uninsured or on Medicaid.
Dr. Conway, a pediatric hospitalist and assistant professor of pediatrics at the Cincinnati Children’s Hospital Medical Center, and his coauthors hypothesized that cash-strapped hospitals would find it hard to meet the mandate and might shortchange other programs in an effort to comply. Laudable as such legislation might be, “we wanted to make it clear to hospitalists and hospitals that the ratios could have an impact on other goals they wanted to achieve, such as meeting pay-for-performance targets,” he says.
Using financial data from the California Office of Statewide Health Planning and Development, they examined staffing trends on adult general medical surgical units in short-term, acute-care general hospitals from 1993 to 2004, the most recent years for which complete data was available. For 2003 and 2004, they also analyzed staff ratios according to five characteristics: hospital ownership (profit, nonprofit, government-owned), market competitiveness, teaching status, location (urban vs. rural), and whether or not the hospital met the definition of a safety net facility.
From 1993-99, nurse staffing ratios remained flat; they rose steadily thereafter. Not surprisingly, the largest increase occurred between 2003 and 2004, the year implementation was slated to go into effect. During that period, the median ratio for all hospitals studied went from less than one nurse per four patients to more than 1:4, exceeding the mandated figure. Fewer than 25% of hospitals fell short of the minimum mandate of 1:5.

However, further analysis reveals more nuances. The mandate requires a minimum ratio of licensed nurses to patients; those nurses can be registered nurses (RNs), licensed vocational nurses (LVNs), or a combination. In 2004, only 2.4% of hospitals fell below the mandated minimum for that year of 1:6, compared with 5% from the year before—but 11.4% were below 1:5 (RNs plus LVNs). When RNs only were considered, 29.5% of hospitals fell short of one for every five patients.
Further, some states are considering a minimum mandate of one licensed nurse per every four patients—yet 40.4% of the hospitals in this study did not meet that standard. “This demonstrates the substantial increase in the proportion of hospitals that are below minimum ratios as the number of nurses or required training level of nurses is increased,” the authors point out.
The finding that nearly 30% of hospitals had less than one registered nurse for every five patients was surprising, says Dr. Conway, whose wife is a registered nurse. In other words, “if you or I or our parents were admitted to a hospital, your chances are about one in three that they will have less than one nurse for every five patients. That means each nurse has less time to spend per patient.”
For-profit hospitals, non-teaching hospitals, and hospitals in urban or more competitive locations fared best at achieving the mandated ratios. However, hospitals with high Medicaid or uninsured populations were significantly more likely to fall below the minimum ratios than their more affluent counterparts and did not achieve the marked gains in staffing ratios achieved in other facilities.
All in all, more than 20% of safety net hospitals failed to achieve the 2004 mandate of 1:5, compared with about 12% of the other types of hospitals.
Of the safety net hospitals that did achieve the mandate, one wonders what types of tradeoffs they had to make, Dr. Conway adds: “Are they closing emergency rooms? Investing less in new equipment and facilities? Hiring less-trained staff? This study raises those questions, although it doesn’t answer them.”
More and more, hospitalists are being held responsible for quality improvement programs and outcomes measures within hospitals. The targets monitored often are those most strongly influenced by nurse presence, such as the number of central line infections, pressure ulcers, urinary tract infections, ventilator-acquired pneumonia, and similar conditions.
On the other hand, “no one has yet studied what happens when a hospital goes from a ratio of 1:5 to 1:4,” Dr. Conway says. It is possible that the [patient] gains realized may not be large enough to justify the compromises a hospital might have to make in other areas to meet that goal. “We must determine what the tradeoffs are and identify optimal nurse staffing ratios. Adequate nurse staffing is a significant key to achieving a successful team management approach in a hospital.” TH
Norra MacReady is a medical writer based in California.
Editor’s note: Dr. Conway was featured in the February 2008 issue (p. 28) as a member of the White House Fellows Program.
Several studies have linked lower nurse-to-patient ratios with fewer medical errors and deaths, better overall treatment, and reduced rates of nurse burnout. These findings led California, in 1999, to pass the country’s first law mandating a minimum nurse-to-patient staffing ratio.
By 2004, the mandated ratio was one licensed nurse for every six patients; that was decreased in 2005 to one nurse for every five patients. Since then, similar bills have been passed or proposed in at least 25 more states. The benefits to patients and nurses of these improved ratios are clear. However, their effect on hospitalists, other staff members, and hospitals have not been widely studied. Further, the mandates often do not come with additional money to implement them.
In this month’s issue of the Journal of Hospital Medicine, Patrick Conway, MD, and colleagues examine nurse staffing trends in California hospitals since the mandate went into effect. They were particularly interested in what they called “safety net” hospitals: urban, government-owned, resource-poor institutions with at least 36% of patients uninsured or on Medicaid.
Dr. Conway, a pediatric hospitalist and assistant professor of pediatrics at the Cincinnati Children’s Hospital Medical Center, and his coauthors hypothesized that cash-strapped hospitals would find it hard to meet the mandate and might shortchange other programs in an effort to comply. Laudable as such legislation might be, “we wanted to make it clear to hospitalists and hospitals that the ratios could have an impact on other goals they wanted to achieve, such as meeting pay-for-performance targets,” he says.
Using financial data from the California Office of Statewide Health Planning and Development, they examined staffing trends on adult general medical surgical units in short-term, acute-care general hospitals from 1993 to 2004, the most recent years for which complete data was available. For 2003 and 2004, they also analyzed staff ratios according to five characteristics: hospital ownership (profit, nonprofit, government-owned), market competitiveness, teaching status, location (urban vs. rural), and whether or not the hospital met the definition of a safety net facility.
From 1993-99, nurse staffing ratios remained flat; they rose steadily thereafter. Not surprisingly, the largest increase occurred between 2003 and 2004, the year implementation was slated to go into effect. During that period, the median ratio for all hospitals studied went from less than one nurse per four patients to more than 1:4, exceeding the mandated figure. Fewer than 25% of hospitals fell short of the minimum mandate of 1:5.
However, further analysis reveals more nuances. The mandate requires a minimum ratio of licensed nurses to patients; those nurses can be registered nurses (RNs), licensed vocational nurses (LVNs), or a combination. In 2004, only 2.4% of hospitals fell below the mandated minimum for that year of 1:6, compared with 5% from the year before—but 11.4% were below 1:5 (RNs plus LVNs). When RNs only were considered, 29.5% of hospitals fell short of one for every five patients.
Further, some states are considering a minimum mandate of one licensed nurse per every four patients—yet 40.4% of the hospitals in this study did not meet that standard. “This demonstrates the substantial increase in the proportion of hospitals that are below minimum ratios as the number of nurses or required training level of nurses is increased,” the authors point out.
The finding that nearly 30% of hospitals had less than one registered nurse for every five patients was surprising, says Dr. Conway, whose wife is a registered nurse. In other words, “if you or I or our parents were admitted to a hospital, your chances are about one in three that they will have less than one nurse for every five patients. That means each nurse has less time to spend per patient.”
For-profit hospitals, non-teaching hospitals, and hospitals in urban or more competitive locations fared best at achieving the mandated ratios. However, hospitals with high Medicaid or uninsured populations were significantly more likely to fall below the minimum ratios than their more affluent counterparts and did not achieve the marked gains in staffing ratios achieved in other facilities.
All in all, more than 20% of safety net hospitals failed to achieve the 2004 mandate of 1:5, compared with about 12% of the other types of hospitals.
Of the safety net hospitals that did achieve the mandate, one wonders what types of tradeoffs they had to make, Dr. Conway adds: “Are they closing emergency rooms? Investing less in new equipment and facilities? Hiring less-trained staff? This study raises those questions, although it doesn’t answer them.”
More and more, hospitalists are being held responsible for quality improvement programs and outcomes measures within hospitals. The targets monitored often are those most strongly influenced by nurse presence, such as the number of central line infections, pressure ulcers, urinary tract infections, ventilator-acquired pneumonia, and similar conditions.
On the other hand, “no one has yet studied what happens when a hospital goes from a ratio of 1:5 to 1:4,” Dr. Conway says. It is possible that the [patient] gains realized may not be large enough to justify the compromises a hospital might have to make in other areas to meet that goal. “We must determine what the tradeoffs are and identify optimal nurse staffing ratios. Adequate nurse staffing is a significant key to achieving a successful team management approach in a hospital.” TH
Norra MacReady is a medical writer based in California.
Editor’s note: Dr. Conway was featured in the February 2008 issue (p. 28) as a member of the White House Fellows Program.
Several studies have linked lower nurse-to-patient ratios with fewer medical errors and deaths, better overall treatment, and reduced rates of nurse burnout. These findings led California, in 1999, to pass the country’s first law mandating a minimum nurse-to-patient staffing ratio.
By 2004, the mandated ratio was one licensed nurse for every six patients; that was decreased in 2005 to one nurse for every five patients. Since then, similar bills have been passed or proposed in at least 25 more states. The benefits to patients and nurses of these improved ratios are clear. However, their effect on hospitalists, other staff members, and hospitals have not been widely studied. Further, the mandates often do not come with additional money to implement them.
In this month’s issue of the Journal of Hospital Medicine, Patrick Conway, MD, and colleagues examine nurse staffing trends in California hospitals since the mandate went into effect. They were particularly interested in what they called “safety net” hospitals: urban, government-owned, resource-poor institutions with at least 36% of patients uninsured or on Medicaid.
Dr. Conway, a pediatric hospitalist and assistant professor of pediatrics at the Cincinnati Children’s Hospital Medical Center, and his coauthors hypothesized that cash-strapped hospitals would find it hard to meet the mandate and might shortchange other programs in an effort to comply. Laudable as such legislation might be, “we wanted to make it clear to hospitalists and hospitals that the ratios could have an impact on other goals they wanted to achieve, such as meeting pay-for-performance targets,” he says.
Using financial data from the California Office of Statewide Health Planning and Development, they examined staffing trends on adult general medical surgical units in short-term, acute-care general hospitals from 1993 to 2004, the most recent years for which complete data was available. For 2003 and 2004, they also analyzed staff ratios according to five characteristics: hospital ownership (profit, nonprofit, government-owned), market competitiveness, teaching status, location (urban vs. rural), and whether or not the hospital met the definition of a safety net facility.
From 1993-99, nurse staffing ratios remained flat; they rose steadily thereafter. Not surprisingly, the largest increase occurred between 2003 and 2004, the year implementation was slated to go into effect. During that period, the median ratio for all hospitals studied went from less than one nurse per four patients to more than 1:4, exceeding the mandated figure. Fewer than 25% of hospitals fell short of the minimum mandate of 1:5.
However, further analysis reveals more nuances. The mandate requires a minimum ratio of licensed nurses to patients; those nurses can be registered nurses (RNs), licensed vocational nurses (LVNs), or a combination. In 2004, only 2.4% of hospitals fell below the mandated minimum for that year of 1:6, compared with 5% from the year before—but 11.4% were below 1:5 (RNs plus LVNs). When RNs only were considered, 29.5% of hospitals fell short of one for every five patients.
Further, some states are considering a minimum mandate of one licensed nurse per every four patients—yet 40.4% of the hospitals in this study did not meet that standard. “This demonstrates the substantial increase in the proportion of hospitals that are below minimum ratios as the number of nurses or required training level of nurses is increased,” the authors point out.
The finding that nearly 30% of hospitals had less than one registered nurse for every five patients was surprising, says Dr. Conway, whose wife is a registered nurse. In other words, “if you or I or our parents were admitted to a hospital, your chances are about one in three that they will have less than one nurse for every five patients. That means each nurse has less time to spend per patient.”
For-profit hospitals, non-teaching hospitals, and hospitals in urban or more competitive locations fared best at achieving the mandated ratios. However, hospitals with high Medicaid or uninsured populations were significantly more likely to fall below the minimum ratios than their more affluent counterparts and did not achieve the marked gains in staffing ratios achieved in other facilities.
All in all, more than 20% of safety net hospitals failed to achieve the 2004 mandate of 1:5, compared with about 12% of the other types of hospitals.
Of the safety net hospitals that did achieve the mandate, one wonders what types of tradeoffs they had to make, Dr. Conway adds: “Are they closing emergency rooms? Investing less in new equipment and facilities? Hiring less-trained staff? This study raises those questions, although it doesn’t answer them.”
More and more, hospitalists are being held responsible for quality improvement programs and outcomes measures within hospitals. The targets monitored often are those most strongly influenced by nurse presence, such as the number of central line infections, pressure ulcers, urinary tract infections, ventilator-acquired pneumonia, and similar conditions.
On the other hand, “no one has yet studied what happens when a hospital goes from a ratio of 1:5 to 1:4,” Dr. Conway says. It is possible that the [patient] gains realized may not be large enough to justify the compromises a hospital might have to make in other areas to meet that goal. “We must determine what the tradeoffs are and identify optimal nurse staffing ratios. Adequate nurse staffing is a significant key to achieving a successful team management approach in a hospital.” TH
Norra MacReady is a medical writer based in California.
Editor’s note: Dr. Conway was featured in the February 2008 issue (p. 28) as a member of the White House Fellows Program.
Drug Misuse Varies
Elderly inpatients’ risk of receiving potentially inappropriate medication (PIM) varies widely depending on where in the country they’re hospitalized and the specialty of their attending physicians, according to a study in the March-April edition of the Journal of Hospital Medicine.
Hospitalists may be encouraged by the fact that they, along with geriatricians, internists, and family physicians, were less likely than cardiologists to prescribe PIMs. Still, the major take-home message of the study is to “examine your individual practice and think about whether it’s appropriate to prescribe these medications,” says lead author Michael Rothberg, MD, assistant professor of medicine at Tufts University School of Medicine in Boston.
PIM use was highest in hospitals in the South. There, 55% of elderly patients received at least one PIM, compared with 34% of patients in Northeastern hospitals, where PIM use was lowest. The exact reason for this discrepancy is not known, but Dr. Rothberg hypothesizes that “we tend to prescribe like people in our hospital and like people in our region.” In other words, “it has to do with learning from the people around us.”
Most interesting to him is the wide variation in prescribing practices among individual doctors—even within the same specialty. “The decision to prescribe a drug is based on the individual provider and has to do with how you as a doctor feel about these drugs,” he explains. Although nearly half of all of the patients had received at least one PIM, there were seven hospitals in which those drugs never were prescribed. Somehow, “they found a way to care for people without [those medications],” he points out.
PIM use has been examined among elderly outpatients and nursing home residents, but only a handful of small studies have looked at the problem in hospital inpatients, says Dr. Rothberg. He and his coauthors used data from hospitals across the United States participating in Perspective, a database developed by Charlotte, N.C.-based Premier to measure quality and healthcare utilization.
The survey included patients 65 years or older admitted between Sept. 1, 2002, and June 30, 2005. Their principal diagnoses were acute myocardial infarction, chronic obstructive pulmonary disease, chest pain, community acquired pneumonia, congestive heart failure, ischemic stroke, or urinary tract infection. Surgical patients were excluded. Using the 2002 update of the Beers criteria for PIM use in older adults, the authors identified the total number of PIMs administered to each patient during his or her hospital stay. They further classified each PIM as high- or low-severity, based on the expert consensus expressed in the 1997 update of the Beers criteria.
Data were available on 493,971 patients from 384 hospitals. Of those individuals, 49% received at least one PIM, and 6% received three or more. Thirty-eight percent of patients received at least one PIM with a high severity rating.
The three agents most likely to be prescribed were promethazine, diphenhydramine, and propoxyphene—probably because these drugs treat the problems most commonly encountered in hospitals, such as allergies, sleep problems, nausea, and pain, Dr. Rothberg says.
Hospital region emerged as the most important predictor of PIM use. Compared with patients in the Midwest, patients in the South had an odds ratio of 1.63 of receiving a high-severity PIM. The odds ratio for patients in the West was 1.43. Patients in the Northeast had an odds ratio of 0.85.
The median rate of prescribing high-severity PIMs was lowest among geriatricians, at 24%. Rates among hospitalists, internists, and family physicians were 33% to 36%. Cardiologists had the highest rate: 48% prescribed at least one high-severity PIM.
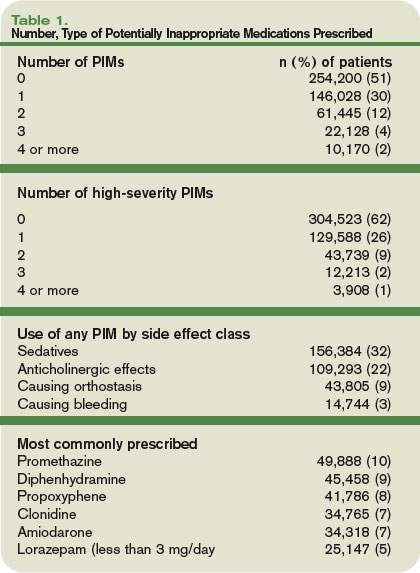
Interestingly, older patient age also was associated with a lower risk of PIM use. Of patients 85 or older, 42% received at least one PIM, compared with 53% of patients age 65 to 74 (p<0.0001). This suggests that “doctors are aware that the older patients are more frail and vulnerable” and take extra care to avoid prescribing PIMs to people in that age range, Dr. Rothberg says. A diagnosis of stroke or chronic obstructive pulmonary disease also was associated with a lower risk of receiving a PIM—further evidence that “doctors were, to some extent, taking patient factors into account” when prescribing medication.
PIM use among inpatients, as reported in this study, far exceeds the rates published for elders dwelling in the community or in nursing homes, writes Daniel S. Budnitz, MD, MPH, in an editorial accompanying the study.
The wide variation in prescribing practices means each facility must monitor its use of PIMs, just as individual hospitals monitor antibiotic use and resistance, advises Dr. Budnitz, a medical officer in the Division of Healthcare Quality Promotion at the Centers for Disease Control and Prevention. He also points out that the evidence that PIMs cause clinically significant adverse events is “weak and based largely on observational studies with inconsistent results.” The drugs in the Beers criteria are “potentially” inappropriate, he says, but some centers have recategorized them as “ ‘always avoid’ medications, ‘rarely acceptable’ medications, and medications which, indeed, have ‘some indications’ for use in older adults.” Thus, some variation among hospitals may be acceptable.
Rather than concentrate on the Beers criteria, hospitalists should focus “on identifying and mitigating the most common and most severe adverse drug events occurring in their hospitals,” such as bleeding from anticoagulants, hypoglycemic events from insulin, and oversedation from opioid analgesics, Dr. Budnitz points out. TH
Norra MacReady is a medical writer based in California.
Elderly inpatients’ risk of receiving potentially inappropriate medication (PIM) varies widely depending on where in the country they’re hospitalized and the specialty of their attending physicians, according to a study in the March-April edition of the Journal of Hospital Medicine.
Hospitalists may be encouraged by the fact that they, along with geriatricians, internists, and family physicians, were less likely than cardiologists to prescribe PIMs. Still, the major take-home message of the study is to “examine your individual practice and think about whether it’s appropriate to prescribe these medications,” says lead author Michael Rothberg, MD, assistant professor of medicine at Tufts University School of Medicine in Boston.
PIM use was highest in hospitals in the South. There, 55% of elderly patients received at least one PIM, compared with 34% of patients in Northeastern hospitals, where PIM use was lowest. The exact reason for this discrepancy is not known, but Dr. Rothberg hypothesizes that “we tend to prescribe like people in our hospital and like people in our region.” In other words, “it has to do with learning from the people around us.”
Most interesting to him is the wide variation in prescribing practices among individual doctors—even within the same specialty. “The decision to prescribe a drug is based on the individual provider and has to do with how you as a doctor feel about these drugs,” he explains. Although nearly half of all of the patients had received at least one PIM, there were seven hospitals in which those drugs never were prescribed. Somehow, “they found a way to care for people without [those medications],” he points out.
PIM use has been examined among elderly outpatients and nursing home residents, but only a handful of small studies have looked at the problem in hospital inpatients, says Dr. Rothberg. He and his coauthors used data from hospitals across the United States participating in Perspective, a database developed by Charlotte, N.C.-based Premier to measure quality and healthcare utilization.
The survey included patients 65 years or older admitted between Sept. 1, 2002, and June 30, 2005. Their principal diagnoses were acute myocardial infarction, chronic obstructive pulmonary disease, chest pain, community acquired pneumonia, congestive heart failure, ischemic stroke, or urinary tract infection. Surgical patients were excluded. Using the 2002 update of the Beers criteria for PIM use in older adults, the authors identified the total number of PIMs administered to each patient during his or her hospital stay. They further classified each PIM as high- or low-severity, based on the expert consensus expressed in the 1997 update of the Beers criteria.
Data were available on 493,971 patients from 384 hospitals. Of those individuals, 49% received at least one PIM, and 6% received three or more. Thirty-eight percent of patients received at least one PIM with a high severity rating.
The three agents most likely to be prescribed were promethazine, diphenhydramine, and propoxyphene—probably because these drugs treat the problems most commonly encountered in hospitals, such as allergies, sleep problems, nausea, and pain, Dr. Rothberg says.
Hospital region emerged as the most important predictor of PIM use. Compared with patients in the Midwest, patients in the South had an odds ratio of 1.63 of receiving a high-severity PIM. The odds ratio for patients in the West was 1.43. Patients in the Northeast had an odds ratio of 0.85.
The median rate of prescribing high-severity PIMs was lowest among geriatricians, at 24%. Rates among hospitalists, internists, and family physicians were 33% to 36%. Cardiologists had the highest rate: 48% prescribed at least one high-severity PIM.
Interestingly, older patient age also was associated with a lower risk of PIM use. Of patients 85 or older, 42% received at least one PIM, compared with 53% of patients age 65 to 74 (p<0.0001). This suggests that “doctors are aware that the older patients are more frail and vulnerable” and take extra care to avoid prescribing PIMs to people in that age range, Dr. Rothberg says. A diagnosis of stroke or chronic obstructive pulmonary disease also was associated with a lower risk of receiving a PIM—further evidence that “doctors were, to some extent, taking patient factors into account” when prescribing medication.
PIM use among inpatients, as reported in this study, far exceeds the rates published for elders dwelling in the community or in nursing homes, writes Daniel S. Budnitz, MD, MPH, in an editorial accompanying the study.
The wide variation in prescribing practices means each facility must monitor its use of PIMs, just as individual hospitals monitor antibiotic use and resistance, advises Dr. Budnitz, a medical officer in the Division of Healthcare Quality Promotion at the Centers for Disease Control and Prevention. He also points out that the evidence that PIMs cause clinically significant adverse events is “weak and based largely on observational studies with inconsistent results.” The drugs in the Beers criteria are “potentially” inappropriate, he says, but some centers have recategorized them as “ ‘always avoid’ medications, ‘rarely acceptable’ medications, and medications which, indeed, have ‘some indications’ for use in older adults.” Thus, some variation among hospitals may be acceptable.
Rather than concentrate on the Beers criteria, hospitalists should focus “on identifying and mitigating the most common and most severe adverse drug events occurring in their hospitals,” such as bleeding from anticoagulants, hypoglycemic events from insulin, and oversedation from opioid analgesics, Dr. Budnitz points out. TH
Norra MacReady is a medical writer based in California.
Elderly inpatients’ risk of receiving potentially inappropriate medication (PIM) varies widely depending on where in the country they’re hospitalized and the specialty of their attending physicians, according to a study in the March-April edition of the Journal of Hospital Medicine.
Hospitalists may be encouraged by the fact that they, along with geriatricians, internists, and family physicians, were less likely than cardiologists to prescribe PIMs. Still, the major take-home message of the study is to “examine your individual practice and think about whether it’s appropriate to prescribe these medications,” says lead author Michael Rothberg, MD, assistant professor of medicine at Tufts University School of Medicine in Boston.
PIM use was highest in hospitals in the South. There, 55% of elderly patients received at least one PIM, compared with 34% of patients in Northeastern hospitals, where PIM use was lowest. The exact reason for this discrepancy is not known, but Dr. Rothberg hypothesizes that “we tend to prescribe like people in our hospital and like people in our region.” In other words, “it has to do with learning from the people around us.”
Most interesting to him is the wide variation in prescribing practices among individual doctors—even within the same specialty. “The decision to prescribe a drug is based on the individual provider and has to do with how you as a doctor feel about these drugs,” he explains. Although nearly half of all of the patients had received at least one PIM, there were seven hospitals in which those drugs never were prescribed. Somehow, “they found a way to care for people without [those medications],” he points out.
PIM use has been examined among elderly outpatients and nursing home residents, but only a handful of small studies have looked at the problem in hospital inpatients, says Dr. Rothberg. He and his coauthors used data from hospitals across the United States participating in Perspective, a database developed by Charlotte, N.C.-based Premier to measure quality and healthcare utilization.
The survey included patients 65 years or older admitted between Sept. 1, 2002, and June 30, 2005. Their principal diagnoses were acute myocardial infarction, chronic obstructive pulmonary disease, chest pain, community acquired pneumonia, congestive heart failure, ischemic stroke, or urinary tract infection. Surgical patients were excluded. Using the 2002 update of the Beers criteria for PIM use in older adults, the authors identified the total number of PIMs administered to each patient during his or her hospital stay. They further classified each PIM as high- or low-severity, based on the expert consensus expressed in the 1997 update of the Beers criteria.
Data were available on 493,971 patients from 384 hospitals. Of those individuals, 49% received at least one PIM, and 6% received three or more. Thirty-eight percent of patients received at least one PIM with a high severity rating.
The three agents most likely to be prescribed were promethazine, diphenhydramine, and propoxyphene—probably because these drugs treat the problems most commonly encountered in hospitals, such as allergies, sleep problems, nausea, and pain, Dr. Rothberg says.
Hospital region emerged as the most important predictor of PIM use. Compared with patients in the Midwest, patients in the South had an odds ratio of 1.63 of receiving a high-severity PIM. The odds ratio for patients in the West was 1.43. Patients in the Northeast had an odds ratio of 0.85.
The median rate of prescribing high-severity PIMs was lowest among geriatricians, at 24%. Rates among hospitalists, internists, and family physicians were 33% to 36%. Cardiologists had the highest rate: 48% prescribed at least one high-severity PIM.
Interestingly, older patient age also was associated with a lower risk of PIM use. Of patients 85 or older, 42% received at least one PIM, compared with 53% of patients age 65 to 74 (p<0.0001). This suggests that “doctors are aware that the older patients are more frail and vulnerable” and take extra care to avoid prescribing PIMs to people in that age range, Dr. Rothberg says. A diagnosis of stroke or chronic obstructive pulmonary disease also was associated with a lower risk of receiving a PIM—further evidence that “doctors were, to some extent, taking patient factors into account” when prescribing medication.
PIM use among inpatients, as reported in this study, far exceeds the rates published for elders dwelling in the community or in nursing homes, writes Daniel S. Budnitz, MD, MPH, in an editorial accompanying the study.
The wide variation in prescribing practices means each facility must monitor its use of PIMs, just as individual hospitals monitor antibiotic use and resistance, advises Dr. Budnitz, a medical officer in the Division of Healthcare Quality Promotion at the Centers for Disease Control and Prevention. He also points out that the evidence that PIMs cause clinically significant adverse events is “weak and based largely on observational studies with inconsistent results.” The drugs in the Beers criteria are “potentially” inappropriate, he says, but some centers have recategorized them as “ ‘always avoid’ medications, ‘rarely acceptable’ medications, and medications which, indeed, have ‘some indications’ for use in older adults.” Thus, some variation among hospitals may be acceptable.
Rather than concentrate on the Beers criteria, hospitalists should focus “on identifying and mitigating the most common and most severe adverse drug events occurring in their hospitals,” such as bleeding from anticoagulants, hypoglycemic events from insulin, and oversedation from opioid analgesics, Dr. Budnitz points out. TH
Norra MacReady is a medical writer based in California.
Teamwork Triumphs
Hospitalists regularly list daily workload and long working hours among their top concerns—but some of their tasks can be delegated to another member of the healthcare team.
“There is a perception that a lot of the activities hospitalists spend their time on don’t need to be done by a hospitalist,” said Kevin O’Leary, MD, assistant professor of medicine and associate division chief, Division of Hospital Medicine, Northwestern University Feinberg School of Medicine in Chicago.
For example, at Northwestern, hospitalists engage in discharge activities, case management, and communication with families. All this can be performed by someone else with clinical training, Dr. O’Leary says. The hospital has unit-based care coordinators (UCCs), but they follow all patients on a 30-bed unit and do not go on rounds with the hospitalists. “Their duties were more aligned with the hospital’s interests than the hospitalists’,” Dr. O’Leary explains. He and his colleagues decided to study the effect of assigning hospitalist care coordinators (HCCs) to work with hospitalists exclusively. Their findings are featured in this month’s Journal of Hospital Medicine.
The study covered the 12 weeks from September 2006, through November 2006. During that time, half the hospitalists on duty each week were randomly assigned to work with an HCC, while the other hospitalists continued working in their usual fashion. The HCCs performed the same duties as the UCCs, plus additional ones such as obtaining outside medical records and attending to more discharge details (see Table 1, below). All the HCCs were registered nurses who performed only team-related duties for the duration of the study.
The hospitalists and HCCs rounded together each morning as a team. They collaborated on the daily plan of care and decided on specific duties for each team member to accomplish. Essentially, the HCCs “allowed the physicians to focus more on clinical rather than ancillary issues,” Dr. O’Leary notes.

Activities related to the discharge process were a key feature of the HCC role. Among other things, they started discharge, arranged for home care, and wrote instructions. “We think that if this program is adopted long-term, HCCs could be key in planning the discharge process to improve patient safety,” Dr. O’Leary says. “For example, they could call patients at home to make sure they’re taking their medication.”
At the end of each week, the hospitalists completed an on-line survey measuring their satisfaction with the program and its effects on their efficiency. Patients also were contacted seven to 14 days after discharge and asked about their satisfaction with the discharge process.
Five hospitalists were on duty on any given week, for a total 60 hospitalist weeks. Of those, hospitalist-HCC teams accounted for 31 weeks (52%), and control hospitalists the remaining 29 (48%). Of the 31 hospitalists who completed a team week, 28 (90%) reported that the team approach improved their efficiency and job satisfaction. They singled out activities relating to communication with nurses and those associated with discharge planning and execution as particularly benefiting from the presence of an HCC.
“One of the advantages that hospitalists told us about working with the HCC was that it allowed them to be in two places at once,” Dr. O’Leary says. “[For example,] if a new admission came in before they were done with morning rounds, the hospitalist could begin the admission while the HCC looked in on their old patients. Or, if two admissions came at once, the hospitalist could begin to admit one of the patients while the HCC gathered background information on the second.
“Also, having an extra pair of hands was incredibly helpful on rounds for patients who had wounds that needed to be undressed and examined, or for helping to turn or move patients who were otherwise difficult to examine.”
The HCCs were not formally surveyed, but all said they would rather continue as team members than return to their old duties.
Of 71 patients who completed the discharge satisfaction interview, 44 (62%) were cared for by a hospitalist-HCC team, but their satisfaction levels were no different from those reported by patients cared for by control hospitalists.
There was also a suggestion that the addition of the HCC lowered costs and shortened length of stay. Patients cared for by a team incurred an unadjusted mean cost of $10,052.96 +/-$11,708.73, compared with an unadjusted mean cost of $11,703.19 +/-$20,455.78 incurred by the control patients (p=0.008). Unadjusted mean length of stay was 4.70 +/-4.15 days for patients cared for by a team, compared with 5.07 +/- 3.99 for patients seen by control hospitalists (p=0.005). Both findings lost significance on multivariate regression analysis, but the hospital is planning a longer study with a larger sample size to see if truly significant differences emerge.
The HCCs helped in two basic ways, Dr. O’Leary concludes. They lightened the physicians’ workload, and they were able to add a nurse’s perspective to patient care. For example, if the hospitalist wrote an order for a diuretic, the HCC could alert the unit nurse to check the computer for the order. “They had a unique ability to see what the nurses needed to know, because they were nurses themselves,” he says.
Hospitalists aren’t the only physicians who could benefit from this arrangement, he adds. “For physicians in a lot of specialties, there are lots of activities that don’t necessarily need to be done by the doctor. The right support would make them happier and more efficient.”TH
Norra MacReady is a medical writer based in California.
Hospitalists regularly list daily workload and long working hours among their top concerns—but some of their tasks can be delegated to another member of the healthcare team.
“There is a perception that a lot of the activities hospitalists spend their time on don’t need to be done by a hospitalist,” said Kevin O’Leary, MD, assistant professor of medicine and associate division chief, Division of Hospital Medicine, Northwestern University Feinberg School of Medicine in Chicago.
For example, at Northwestern, hospitalists engage in discharge activities, case management, and communication with families. All this can be performed by someone else with clinical training, Dr. O’Leary says. The hospital has unit-based care coordinators (UCCs), but they follow all patients on a 30-bed unit and do not go on rounds with the hospitalists. “Their duties were more aligned with the hospital’s interests than the hospitalists’,” Dr. O’Leary explains. He and his colleagues decided to study the effect of assigning hospitalist care coordinators (HCCs) to work with hospitalists exclusively. Their findings are featured in this month’s Journal of Hospital Medicine.
The study covered the 12 weeks from September 2006, through November 2006. During that time, half the hospitalists on duty each week were randomly assigned to work with an HCC, while the other hospitalists continued working in their usual fashion. The HCCs performed the same duties as the UCCs, plus additional ones such as obtaining outside medical records and attending to more discharge details (see Table 1, below). All the HCCs were registered nurses who performed only team-related duties for the duration of the study.
The hospitalists and HCCs rounded together each morning as a team. They collaborated on the daily plan of care and decided on specific duties for each team member to accomplish. Essentially, the HCCs “allowed the physicians to focus more on clinical rather than ancillary issues,” Dr. O’Leary notes.
Activities related to the discharge process were a key feature of the HCC role. Among other things, they started discharge, arranged for home care, and wrote instructions. “We think that if this program is adopted long-term, HCCs could be key in planning the discharge process to improve patient safety,” Dr. O’Leary says. “For example, they could call patients at home to make sure they’re taking their medication.”
At the end of each week, the hospitalists completed an on-line survey measuring their satisfaction with the program and its effects on their efficiency. Patients also were contacted seven to 14 days after discharge and asked about their satisfaction with the discharge process.
Five hospitalists were on duty on any given week, for a total 60 hospitalist weeks. Of those, hospitalist-HCC teams accounted for 31 weeks (52%), and control hospitalists the remaining 29 (48%). Of the 31 hospitalists who completed a team week, 28 (90%) reported that the team approach improved their efficiency and job satisfaction. They singled out activities relating to communication with nurses and those associated with discharge planning and execution as particularly benefiting from the presence of an HCC.
“One of the advantages that hospitalists told us about working with the HCC was that it allowed them to be in two places at once,” Dr. O’Leary says. “[For example,] if a new admission came in before they were done with morning rounds, the hospitalist could begin the admission while the HCC looked in on their old patients. Or, if two admissions came at once, the hospitalist could begin to admit one of the patients while the HCC gathered background information on the second.
“Also, having an extra pair of hands was incredibly helpful on rounds for patients who had wounds that needed to be undressed and examined, or for helping to turn or move patients who were otherwise difficult to examine.”
The HCCs were not formally surveyed, but all said they would rather continue as team members than return to their old duties.
Of 71 patients who completed the discharge satisfaction interview, 44 (62%) were cared for by a hospitalist-HCC team, but their satisfaction levels were no different from those reported by patients cared for by control hospitalists.
There was also a suggestion that the addition of the HCC lowered costs and shortened length of stay. Patients cared for by a team incurred an unadjusted mean cost of $10,052.96 +/-$11,708.73, compared with an unadjusted mean cost of $11,703.19 +/-$20,455.78 incurred by the control patients (p=0.008). Unadjusted mean length of stay was 4.70 +/-4.15 days for patients cared for by a team, compared with 5.07 +/- 3.99 for patients seen by control hospitalists (p=0.005). Both findings lost significance on multivariate regression analysis, but the hospital is planning a longer study with a larger sample size to see if truly significant differences emerge.
The HCCs helped in two basic ways, Dr. O’Leary concludes. They lightened the physicians’ workload, and they were able to add a nurse’s perspective to patient care. For example, if the hospitalist wrote an order for a diuretic, the HCC could alert the unit nurse to check the computer for the order. “They had a unique ability to see what the nurses needed to know, because they were nurses themselves,” he says.
Hospitalists aren’t the only physicians who could benefit from this arrangement, he adds. “For physicians in a lot of specialties, there are lots of activities that don’t necessarily need to be done by the doctor. The right support would make them happier and more efficient.”TH
Norra MacReady is a medical writer based in California.
Hospitalists regularly list daily workload and long working hours among their top concerns—but some of their tasks can be delegated to another member of the healthcare team.
“There is a perception that a lot of the activities hospitalists spend their time on don’t need to be done by a hospitalist,” said Kevin O’Leary, MD, assistant professor of medicine and associate division chief, Division of Hospital Medicine, Northwestern University Feinberg School of Medicine in Chicago.
For example, at Northwestern, hospitalists engage in discharge activities, case management, and communication with families. All this can be performed by someone else with clinical training, Dr. O’Leary says. The hospital has unit-based care coordinators (UCCs), but they follow all patients on a 30-bed unit and do not go on rounds with the hospitalists. “Their duties were more aligned with the hospital’s interests than the hospitalists’,” Dr. O’Leary explains. He and his colleagues decided to study the effect of assigning hospitalist care coordinators (HCCs) to work with hospitalists exclusively. Their findings are featured in this month’s Journal of Hospital Medicine.
The study covered the 12 weeks from September 2006, through November 2006. During that time, half the hospitalists on duty each week were randomly assigned to work with an HCC, while the other hospitalists continued working in their usual fashion. The HCCs performed the same duties as the UCCs, plus additional ones such as obtaining outside medical records and attending to more discharge details (see Table 1, below). All the HCCs were registered nurses who performed only team-related duties for the duration of the study.
The hospitalists and HCCs rounded together each morning as a team. They collaborated on the daily plan of care and decided on specific duties for each team member to accomplish. Essentially, the HCCs “allowed the physicians to focus more on clinical rather than ancillary issues,” Dr. O’Leary notes.
Activities related to the discharge process were a key feature of the HCC role. Among other things, they started discharge, arranged for home care, and wrote instructions. “We think that if this program is adopted long-term, HCCs could be key in planning the discharge process to improve patient safety,” Dr. O’Leary says. “For example, they could call patients at home to make sure they’re taking their medication.”
At the end of each week, the hospitalists completed an on-line survey measuring their satisfaction with the program and its effects on their efficiency. Patients also were contacted seven to 14 days after discharge and asked about their satisfaction with the discharge process.
Five hospitalists were on duty on any given week, for a total 60 hospitalist weeks. Of those, hospitalist-HCC teams accounted for 31 weeks (52%), and control hospitalists the remaining 29 (48%). Of the 31 hospitalists who completed a team week, 28 (90%) reported that the team approach improved their efficiency and job satisfaction. They singled out activities relating to communication with nurses and those associated with discharge planning and execution as particularly benefiting from the presence of an HCC.
“One of the advantages that hospitalists told us about working with the HCC was that it allowed them to be in two places at once,” Dr. O’Leary says. “[For example,] if a new admission came in before they were done with morning rounds, the hospitalist could begin the admission while the HCC looked in on their old patients. Or, if two admissions came at once, the hospitalist could begin to admit one of the patients while the HCC gathered background information on the second.
“Also, having an extra pair of hands was incredibly helpful on rounds for patients who had wounds that needed to be undressed and examined, or for helping to turn or move patients who were otherwise difficult to examine.”
The HCCs were not formally surveyed, but all said they would rather continue as team members than return to their old duties.
Of 71 patients who completed the discharge satisfaction interview, 44 (62%) were cared for by a hospitalist-HCC team, but their satisfaction levels were no different from those reported by patients cared for by control hospitalists.
There was also a suggestion that the addition of the HCC lowered costs and shortened length of stay. Patients cared for by a team incurred an unadjusted mean cost of $10,052.96 +/-$11,708.73, compared with an unadjusted mean cost of $11,703.19 +/-$20,455.78 incurred by the control patients (p=0.008). Unadjusted mean length of stay was 4.70 +/-4.15 days for patients cared for by a team, compared with 5.07 +/- 3.99 for patients seen by control hospitalists (p=0.005). Both findings lost significance on multivariate regression analysis, but the hospital is planning a longer study with a larger sample size to see if truly significant differences emerge.
The HCCs helped in two basic ways, Dr. O’Leary concludes. They lightened the physicians’ workload, and they were able to add a nurse’s perspective to patient care. For example, if the hospitalist wrote an order for a diuretic, the HCC could alert the unit nurse to check the computer for the order. “They had a unique ability to see what the nurses needed to know, because they were nurses themselves,” he says.
Hospitalists aren’t the only physicians who could benefit from this arrangement, he adds. “For physicians in a lot of specialties, there are lots of activities that don’t necessarily need to be done by the doctor. The right support would make them happier and more efficient.”TH
Norra MacReady is a medical writer based in California.
Hail Fellows
Because hospital medicine is still a new specialty, the finer points of hospitalist education and training are being developed. According to two papers in this month’s Journal of Hospital Medicine, students, hospitalists, employers—even patients—are eager for programs that allow hospitalists to hone their skills.
In one study, investigators at the University of California, San Francisco (UCSF), designed a program for third-year medical students and pharmacy graduate students emphasizing the issues involved in making the transition from inpatient to outpatient care.
Patients often are overwhelmed by the change, and the situation is ripe for miscommunication and error. Students accustomed to seeing these individuals only in the hospital often underestimate the challenges patients confront when they leave the hospital with a bewildering array of instructions and medications.
Medical students also receive little exposure to the roles of caregivers from other fields, yet good transitional care involves professionals from several disciplines. The authors, led by Cindy Lai, MD, assistant clinical professor of medicine at UCSF, reason that “training students in interdisciplinary collaboration may improve their ability to provide quality care.”
They designed an inpatient medicine clerkship curriculum in which teams of medical and pharmacy students paid a home visit to a patient they had cared for in the hospital. After the visits, the students wrote summary letters to each patient’s primary care physician.
The home visits lasted one to two hours and in general consisted of an introduction to the patient’s living quarters, a review of symptoms and medication, a brief physical examination, and a home tour to check for relevant issues such as safety hazards or the patient’s ability to function independently. Students quickly discovered the visits consisted of much more than that.
“Across the board, the response that came back was the ability to view the patient as a person,” says Heather Nye, MD, PhD, assistant clinical professor of internal medicine and one of the authors of the study. Students found it inspiring to see patients as people in control of their surroundings and also were surprised how well or poorly some people did away from the hospital.

They learned how to maximize their interaction with the pharmacy students and how to anticipate problems patients might encounter at home, such as taking medicines appropriately or scheduling and keeping follow-up appointments.
Apparently, the lessons went both ways, with some patients inviting students to stay for dinner or dessert. “That human aspect was one of the most profound features of the visits,” Dr. Nye says.
She acknowledges that scheduling home visits regularly would require a commitment of time and money that is simply not feasible in today’s environment, especially after medical school. But she urged that instruction in transitional and interdisciplinary care be incorporated into the curriculum whenever possible. “We all understand that safe discharges require multiple disciplines,” she said. “It’s never too early to start teaching about transitional care.”
Medical school training is especially important because students and residents who specialize in hospital medicine will find fellowships in short supply. The few that exist function more to train educators rather than practicing physicians.
—Philip Goodman, MD, professor of internal medicine and biomedical engineering, University of Nevada, Reno, School of Medicine
This despite the fact hospital medicine has grown at a near-exponential pace, from 2000 practitioners in 1998 to 15,000 in 2005, with 30,000 projected by 2010.

Practicing hospitalists and residents Philip Goodman, MD, MS, and Andrius Januska, BS, of the University of Nevada, Reno, School of Medicine set about to gauge the value of and interest in a practical fellowship in hospital medicine to employers. They sent questionnaires to employers and practicing hospitalists. Of 103 employers, two-thirds indicated they would offer fellowship graduates a signing bonus or salary premium ranging from $10,000 to more than $20,000.
Of 101 practicing hospitalists, 58% felt a clinical fellowship probably or strongly would be a good career move. Further, 91% said it would at least possibly be a good move. And 57% of the residents thinking of a career in hospital medicine said they would consider a one-year clinical fellowship if one were available.
“I was surprised at how strongly practicing hospitalists, most of whom are not academics, supported the value of an intense year of clinical hospital medicine fellowship training,” says Dr. Goodman, professor of internal medicine and biomedical engineering. “Most felt that graduating internal medicine residents ‘probably’ or ‘strongly’ should consider such fellowship training. I had expected a more neutral response, reflecting a balanced response bias of those with strong feelings at either extreme.”
Such training can offer new physicians a chance to develop expertise and leadership capabilities that might otherwise require years of on-the-job experience, he explains. Fellowship training also might elevate hospitalists to a level of prestige equaling that of other subspecialties, he says.
Ironically, the specialty’s rapid growth is probably slowing the establishment of fellowship programs, because residents can command annual salaries of $160,000 to $200,000 upon graduation with no special fellowship training. But a few months into it, they often realize a fellowship would have helped them master some of the unique aspects of hospital medicine, such as process of care, communication, productivity and medicolegal insight, and quality improvement, Dr. Goodman notes.
The University of Nevada will start training its first six hospitalist fellows next year. “I wouldn’t be surprised if most applicants were those who had recently taken hospitalist positions but realized the professional impact a year of polishing school can provide,” he says. TH
Norra MacReady is a medical writer based in California.
Because hospital medicine is still a new specialty, the finer points of hospitalist education and training are being developed. According to two papers in this month’s Journal of Hospital Medicine, students, hospitalists, employers—even patients—are eager for programs that allow hospitalists to hone their skills.
In one study, investigators at the University of California, San Francisco (UCSF), designed a program for third-year medical students and pharmacy graduate students emphasizing the issues involved in making the transition from inpatient to outpatient care.
Patients often are overwhelmed by the change, and the situation is ripe for miscommunication and error. Students accustomed to seeing these individuals only in the hospital often underestimate the challenges patients confront when they leave the hospital with a bewildering array of instructions and medications.
Medical students also receive little exposure to the roles of caregivers from other fields, yet good transitional care involves professionals from several disciplines. The authors, led by Cindy Lai, MD, assistant clinical professor of medicine at UCSF, reason that “training students in interdisciplinary collaboration may improve their ability to provide quality care.”
They designed an inpatient medicine clerkship curriculum in which teams of medical and pharmacy students paid a home visit to a patient they had cared for in the hospital. After the visits, the students wrote summary letters to each patient’s primary care physician.
The home visits lasted one to two hours and in general consisted of an introduction to the patient’s living quarters, a review of symptoms and medication, a brief physical examination, and a home tour to check for relevant issues such as safety hazards or the patient’s ability to function independently. Students quickly discovered the visits consisted of much more than that.
“Across the board, the response that came back was the ability to view the patient as a person,” says Heather Nye, MD, PhD, assistant clinical professor of internal medicine and one of the authors of the study. Students found it inspiring to see patients as people in control of their surroundings and also were surprised how well or poorly some people did away from the hospital.
They learned how to maximize their interaction with the pharmacy students and how to anticipate problems patients might encounter at home, such as taking medicines appropriately or scheduling and keeping follow-up appointments.
Apparently, the lessons went both ways, with some patients inviting students to stay for dinner or dessert. “That human aspect was one of the most profound features of the visits,” Dr. Nye says.
She acknowledges that scheduling home visits regularly would require a commitment of time and money that is simply not feasible in today’s environment, especially after medical school. But she urged that instruction in transitional and interdisciplinary care be incorporated into the curriculum whenever possible. “We all understand that safe discharges require multiple disciplines,” she said. “It’s never too early to start teaching about transitional care.”
Medical school training is especially important because students and residents who specialize in hospital medicine will find fellowships in short supply. The few that exist function more to train educators rather than practicing physicians.
—Philip Goodman, MD, professor of internal medicine and biomedical engineering, University of Nevada, Reno, School of Medicine
This despite the fact hospital medicine has grown at a near-exponential pace, from 2000 practitioners in 1998 to 15,000 in 2005, with 30,000 projected by 2010.
Practicing hospitalists and residents Philip Goodman, MD, MS, and Andrius Januska, BS, of the University of Nevada, Reno, School of Medicine set about to gauge the value of and interest in a practical fellowship in hospital medicine to employers. They sent questionnaires to employers and practicing hospitalists. Of 103 employers, two-thirds indicated they would offer fellowship graduates a signing bonus or salary premium ranging from $10,000 to more than $20,000.
Of 101 practicing hospitalists, 58% felt a clinical fellowship probably or strongly would be a good career move. Further, 91% said it would at least possibly be a good move. And 57% of the residents thinking of a career in hospital medicine said they would consider a one-year clinical fellowship if one were available.
“I was surprised at how strongly practicing hospitalists, most of whom are not academics, supported the value of an intense year of clinical hospital medicine fellowship training,” says Dr. Goodman, professor of internal medicine and biomedical engineering. “Most felt that graduating internal medicine residents ‘probably’ or ‘strongly’ should consider such fellowship training. I had expected a more neutral response, reflecting a balanced response bias of those with strong feelings at either extreme.”
Such training can offer new physicians a chance to develop expertise and leadership capabilities that might otherwise require years of on-the-job experience, he explains. Fellowship training also might elevate hospitalists to a level of prestige equaling that of other subspecialties, he says.
Ironically, the specialty’s rapid growth is probably slowing the establishment of fellowship programs, because residents can command annual salaries of $160,000 to $200,000 upon graduation with no special fellowship training. But a few months into it, they often realize a fellowship would have helped them master some of the unique aspects of hospital medicine, such as process of care, communication, productivity and medicolegal insight, and quality improvement, Dr. Goodman notes.
The University of Nevada will start training its first six hospitalist fellows next year. “I wouldn’t be surprised if most applicants were those who had recently taken hospitalist positions but realized the professional impact a year of polishing school can provide,” he says. TH
Norra MacReady is a medical writer based in California.
Because hospital medicine is still a new specialty, the finer points of hospitalist education and training are being developed. According to two papers in this month’s Journal of Hospital Medicine, students, hospitalists, employers—even patients—are eager for programs that allow hospitalists to hone their skills.
In one study, investigators at the University of California, San Francisco (UCSF), designed a program for third-year medical students and pharmacy graduate students emphasizing the issues involved in making the transition from inpatient to outpatient care.
Patients often are overwhelmed by the change, and the situation is ripe for miscommunication and error. Students accustomed to seeing these individuals only in the hospital often underestimate the challenges patients confront when they leave the hospital with a bewildering array of instructions and medications.
Medical students also receive little exposure to the roles of caregivers from other fields, yet good transitional care involves professionals from several disciplines. The authors, led by Cindy Lai, MD, assistant clinical professor of medicine at UCSF, reason that “training students in interdisciplinary collaboration may improve their ability to provide quality care.”
They designed an inpatient medicine clerkship curriculum in which teams of medical and pharmacy students paid a home visit to a patient they had cared for in the hospital. After the visits, the students wrote summary letters to each patient’s primary care physician.
The home visits lasted one to two hours and in general consisted of an introduction to the patient’s living quarters, a review of symptoms and medication, a brief physical examination, and a home tour to check for relevant issues such as safety hazards or the patient’s ability to function independently. Students quickly discovered the visits consisted of much more than that.
“Across the board, the response that came back was the ability to view the patient as a person,” says Heather Nye, MD, PhD, assistant clinical professor of internal medicine and one of the authors of the study. Students found it inspiring to see patients as people in control of their surroundings and also were surprised how well or poorly some people did away from the hospital.
They learned how to maximize their interaction with the pharmacy students and how to anticipate problems patients might encounter at home, such as taking medicines appropriately or scheduling and keeping follow-up appointments.
Apparently, the lessons went both ways, with some patients inviting students to stay for dinner or dessert. “That human aspect was one of the most profound features of the visits,” Dr. Nye says.
She acknowledges that scheduling home visits regularly would require a commitment of time and money that is simply not feasible in today’s environment, especially after medical school. But she urged that instruction in transitional and interdisciplinary care be incorporated into the curriculum whenever possible. “We all understand that safe discharges require multiple disciplines,” she said. “It’s never too early to start teaching about transitional care.”
Medical school training is especially important because students and residents who specialize in hospital medicine will find fellowships in short supply. The few that exist function more to train educators rather than practicing physicians.
—Philip Goodman, MD, professor of internal medicine and biomedical engineering, University of Nevada, Reno, School of Medicine
This despite the fact hospital medicine has grown at a near-exponential pace, from 2000 practitioners in 1998 to 15,000 in 2005, with 30,000 projected by 2010.
Practicing hospitalists and residents Philip Goodman, MD, MS, and Andrius Januska, BS, of the University of Nevada, Reno, School of Medicine set about to gauge the value of and interest in a practical fellowship in hospital medicine to employers. They sent questionnaires to employers and practicing hospitalists. Of 103 employers, two-thirds indicated they would offer fellowship graduates a signing bonus or salary premium ranging from $10,000 to more than $20,000.
Of 101 practicing hospitalists, 58% felt a clinical fellowship probably or strongly would be a good career move. Further, 91% said it would at least possibly be a good move. And 57% of the residents thinking of a career in hospital medicine said they would consider a one-year clinical fellowship if one were available.
“I was surprised at how strongly practicing hospitalists, most of whom are not academics, supported the value of an intense year of clinical hospital medicine fellowship training,” says Dr. Goodman, professor of internal medicine and biomedical engineering. “Most felt that graduating internal medicine residents ‘probably’ or ‘strongly’ should consider such fellowship training. I had expected a more neutral response, reflecting a balanced response bias of those with strong feelings at either extreme.”
Such training can offer new physicians a chance to develop expertise and leadership capabilities that might otherwise require years of on-the-job experience, he explains. Fellowship training also might elevate hospitalists to a level of prestige equaling that of other subspecialties, he says.
Ironically, the specialty’s rapid growth is probably slowing the establishment of fellowship programs, because residents can command annual salaries of $160,000 to $200,000 upon graduation with no special fellowship training. But a few months into it, they often realize a fellowship would have helped them master some of the unique aspects of hospital medicine, such as process of care, communication, productivity and medicolegal insight, and quality improvement, Dr. Goodman notes.
The University of Nevada will start training its first six hospitalist fellows next year. “I wouldn’t be surprised if most applicants were those who had recently taken hospitalist positions but realized the professional impact a year of polishing school can provide,” he says. TH
Norra MacReady is a medical writer based in California.