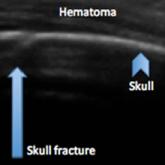
Article Identifying Pediatric Skull Fracture Using Point-of-Care Ultrasound Author: Rebecca Caton, MD Pavitra Kotini-Shah, MD Abdulaziz Ahmed Joseph S. Colla, MD, RDMS Evaluating pediatric patients presenting to the ED with head trauma can be a... Read More
Article Emergency Ultrasound: Identification of Aortic Dissection Using Limited Bedside Ultrasound Author: Joseph S. Colla, MD Pavitra Kotini-Shah, MD Ryan B. Scholz, DO Wesley Eilbert, MD Read More