User login
Improving Feedback to Ward Residents
Feedback has long been recognized as pivotal to the attainment of clinical acumen and skills in medical training.1 Formative feedback can give trainees insight into their strengths and weaknesses, and provide them with clear goals and methods to attain those goals.1, 2 In fact, feedback given regularly over time by a respected figure has shown to improve physician performance.3 However, most faculty are not trained to provide effective feedback. As a result, supervisors often believe they are giving more feedback than trainees believe they are receiving, and residents receive little feedback that they perceive as useful.4 Most residents receive little to no feedback on their communications skills4 or professionalism,5 and rarely receive corrective feedback.6, 7
Faculty may fail to give feedback to residents for a number of reasons. Those barriers most commonly cited in the literature are discomfort with criticizing residents,6, 7 lack of time,4 and lack of direct observation of residents in clinical settings.810 Several studies have looked at tools to guide feedback and address the barrier of discomfort with criticism.6, 7, 11 Some showed improvements in overall feedback, though often supervisors gave only positive feedback and avoided giving feedback about weaknesses.6, 7, 11 Despite the recognition of lack of time as a barrier to feedback,4 most studies on feedback interventions thus far have not included setting aside time for the feedback to occur.6, 7, 11, 12 Finally, a number of studies utilized objective structured clinical examinations (OSCEs) coupled with immediate feedback to improve direct observation of residents, with success in improving feedback related to the encounter.9, 10, 13 To address the gaps in the current literature, the goals of our study were to address 2 specific barriers to feedback for residents: lack of time and discomfort with giving feedback.
The aim of this study was to improve Internal Medicine (IM) residents' and attendings' experiences with feedback on the wards using a pocket card and a dedicated feedback session. We developed and evaluated the pocket feedback card and session for faculty to improve the quality and frequency of their feedback to residents in the inpatient setting. We performed a randomized trial to evaluate our intervention. We hypothesized that the intervention would: 1) improve the quality and quantity of attendings' feedback given to IM ward residents; and 2) improve attendings' comfort with feedback delivery on the wards.
PARTICIPANTS AND METHODS
Setting
The study was performed at Mount Sinai Medical Center in New York City, New York, between July 2008 and January 2009.
Participants
Participants in this study were IM residents and ward teaching attendings on inpatient ward teams at Mount Sinai Medical Center from July 2008 to January 2009. There are 12 ward teams on 3 inpatient services (each service has 4 teams) during each block at our hospital. Ward teams are made up of 1 teaching attending, 1 resident, 1 to 3 interns, and 1 to 2 medical students. The majority of attendings are on the ward service for 4‐week blocks, but some are only on for 1 or 2 weeks. Teams included in the randomization were the General Medicine and Gastroenterology/Cardiology service teams. Half of the General Medicine service attendings are hospitalists. Ward teams were excluded from the study randomization if the attending on the team was on the wards for less than 2 weeks, or if the attending had already been assigned to the experimental group in a previous block, given the influence of having used the card and feedback session previously. Since residents were unaware of the intervention and random assignments were based on attendings, residents could be assigned to the intervention group or the control group on any given inpatient rotation. Therefore, a resident could be in the control group in 1 block and the intervention group in his/her next block on the wards or vice versa, or could be assigned to either the intervention or the control group on more than 1 occasion. Because resident participants were blinded to their team's assignment (as intervention or control) and all surveys were anonymous (tracked as intervention or control by the team name only), it was not possible to exclude residents based on their prior participation or to match the surveys completed by the same residents.
Study Design
We performed a prospective randomized study to evaluate our educational innovation. The unit of randomization was the ward team. For each block, approximately half of the 6‐8 teams were randomized to the intervention group and half to the control group. Randomization assignments were completed the day prior to the start of the block using the random allocation software based on the ward team letters (blind to the attending and resident names). Of the 48 possible ward teams (8 teams per block over 6 blocks), 36 teams were randomized to the intervention or control groups, and 12 teams were not based on the above exclusion criteria. Of the 36 teams, 16 (composed of 16 attendings and 48 residents and interns) were randomized to the intervention group, and 20 (composed of 20 attendings and 63 residents and interns) were randomized to the control group.
The study was blinded such that residents and attendings in the control group were unaware of the study. The study was exempt from IRB review by the Mount Sinai Institutional Review Board, and Grants and Contracts Office, as an evaluation of the effectiveness of an instructional technique in medical education.
Intervention Design
We designed a pocket feedback card to guide a feedback session and assist attendings in giving useful feedback to IM residents on the wards (Figure 1).14 The individual items and categories were adapted from the Accreditation Council for Graduate Medical Education (ACGME) Common Program Requirements Core Competencies section and were revised via the expert consensus of the authors.14 We included 20 items related to resident skills, knowledge, attitudes, and behaviors important to the care of hospitalized patients, grouped under the 6 ACGME core competency domains.14 Many of these items correspond to competencies in the Society of Hospital Medicine (SHM) Core Competencies; in particular, the categories of Systems‐Based Practice and Practice‐Based Learning mirror competencies in the SHM Core Competencies Healthcare Systems chapter.15 Each item utilized a 5‐point Likert scale (1 = very poor, 3 = at expected level, 5 = superior) to evaluate resident performance (Figure 1). We created this card to serve as a directive and specific guide for attendings to provide feedback about specific domains and to give more constructive feedback. The card was to be used during a specific dedicated feedback session in order to overcome the commonly cited barrier of lack of time.
Program Implementation
On the first day of the block, both groups of attendings received the standard inpatient ward orientation given by the program director, including instructions about teaching and administrative responsibilities, and explicit instructions to provide mid‐rotation feedback to residents. Attendings randomized to the intervention group had an additional 5‐minute orientation given by 1 of the investigators. The orientation included a brief discussion on the importance of feedback and an introduction to the items on the card.2 In addition, faculty were instructed to dedicate 1 mid‐rotation attending rounds as a feedback session, to meet individually for 10‐15 minutes with each of the 3‐4 residents on their team, and to use the card to provide feedback on skills in each domain. As noted on the feedback card, if a resident scored less than 3 on a skill set, the attending was instructed to give examples of skills within that domain needing improvement and to offer suggestions for improvement. The intervention group was also asked not to discuss the card or session with others. No other instructions were provided.
Survey Design
At the end of each block, residents and attendings in both groups completed questionnaires to assess satisfaction with, and attitudes toward, feedback (Supporting Information Appendices 1 and 2 in the online version of this article). Survey questions were based on the competency areas included in the feedback card, previously published surveys evaluating feedback interventions,5, 9, 11 and expert opinion. The resident survey was designed to address the impact of feedback on the domains of resident knowledge, clinical and communication skills, and attitudes about feedback from supervisors and peers. We utilized a 5‐point Likert scale including: strongly disagree, disagree, neutral, agree, and strongly agree. The attending survey addressed attendings' satisfaction with feedback encounters and resident performance. At the completion of the study, investigators compared responses in intervention and control groups.
Statistical Analysis
For purposes of analysis, due to the relatively small number of responses for certain answer choices, the Likert scale was converted to a dichotomous variable. The responses of agree and strongly agree were coded as agree; and disagree, strongly disagree, and neutral were coded as disagree. Neutral was coded as disagree in order to avoid overestimating positive attitudes and, in effect, bias our results toward the null hypothesis. Differences between groups were analyzed using chi‐square Fisher's exact test (2‐sided).
Qualitative Interviews
In order to understand the relative contribution of the feedback card versus the feedback session, we performed a qualitative survey of attendings in the intervention group. Following the conclusion of the study period, we selected a convenience sample of 8 attendings from the intervention group for these brief qualitative interviews. We asked 3 basic questions. Was the intervention of the feedback card and dedicated time for feedback useful? Did you find one component, either the card or the dedicated time for feedback, more useful than the other? Were there any negative effects on patient care, education, or other areas, from using an attending rounds as a feedback session? This data was coded and analyzed for common themes.
RESULTS
During the 6‐month study period, 34 teaching attendings (over 36 attending inpatient blocks) and 93 IM residents (over 111 resident inpatient blocks) participated in the study. Thirty‐four of 36 attending surveys and 96 of 111 resident surveys were completed. The overall survey response rates for residents and attendings were 85% and 94%, respectively. Two attendings participated during 2 separate blocks, first in the control group and then in the intervention group, and 18 residents participated during 2 separate blocks. No attendings or residents participated more than twice.
Resident survey response rate was 81.2% in the intervention group and 87.3% in the control group (Table 1). Residents in the intervention group reported receiving more feedback regarding skills they did well (89.7% vs 63.6%, P = 0.004) and skills needing improvement (51.3% vs 25.5%, P = 0.02) than those in the control group. In addition, more intervention residents reported receiving useful information regarding how to improve their skills (53.8% vs 27.3%, P = 0.01), and reported actually improving both their clinical skills (61.5% vs 27.8%, P = 0.001) and their professionalism/communication skills (51.3% vs 29.1%, P = 0.03) based on feedback received from attendings.
| Survey Item | Resident Intervention Agree* % (No.) N = 39 | Resident Control Agree*% (No.) N = 55 | P Value |
|---|---|---|---|
| |||
| I did NOT receive a sufficient amount of feedback from my attending supervisor(s) this block. | 20.5 (8) | 38.2 (21) | 0.08 |
| I received feedback from my attending regarding skills I did well during this block. | 89.7 (35) | 63.6 (35) | 0.004 |
| I received feedback from my attending regarding specific skills that needed improvement during this block. | 51.3 (20) | 25.5 (14) | 0.02 |
| I received useful information from my attending about how to improve my skills during this block. | 53.8 (21) | 27.3 (15) | 0.01 |
| I improved my clinical skills based on feedback I received from my attending this block. | 61.5 (24) | 27.8 (15) | 0.001 |
| I improved my professionalism/communication skills based on feedback I received from my attending this block. | 51.3 (20) | 29.1 (16) | 0.03 |
| I improved my knowledge base because of feedback I received from my attending this block. | 64.1 (25) | 60.0 (33) | 0.83 |
| The feedback I received from my attending this block gave me an overall sense of my performance more than it helped me identify specific areas for improvement. | 64.1 (25) | 65.5 (36) | 1.0 |
| Feedback from colleagues (other interns and residents) is more helpful than feedback from attendings. | 41.0 (16) | 43.6 (24) | 0.84 |
| Independent of feedback received from others, I am able to identify areas in which I need improvement. | 84.6 (33) | 80.0 (44) | 0.60 |
The attending survey response rates for the intervention and control groups were 100% and 90%, respectively. In general, both groups of attendings reported that they were comfortable giving feedback and that they did, in fact, give feedback in each area during their ward block (Table 2). More intervention attendings felt that at least 1 of their residents improved their professionalism/communication skills based on the feedback given (76.9% vs 31.1%, P = 0.02). There were no other significant differences between the groups of attendings.
| Survey Item | Attending Intervention Agree* % (No.) N = 16 | Attending Control Agree* % (No.) N = 18 | P Value |
|---|---|---|---|
| |||
| Giving feedback to housestaff was DIFFICULT this block. | 6.3 (1) | 16.7 (3) | 0.60 |
| I was comfortable giving feedback to my housestaff this block. | 93.8 (15) | 94.4 (17) | 1.00 |
| I did NOT give a sufficient amount of feedback to my housestaff this block. | 18.8 (3) | 38.9 (7) | 0.27 |
| My skills in giving feedback improved during this block. | 50 (8) | 16.7 (3) | 0.07 |
| I gave feedback to housestaff regarding skills they did well during this block. | 100 (16) | 94.4 (17) | 1.00 |
| I gave feedback to housestaff which targeted specific areas for their improvement. | 81.3 (13) | 70.6 (12) | 0.69 |
| At least one of my housestaff improved his/her clinical skills based on feedback I gave this block. | 68.8 (11) | 47.1 (8) | 0.30 |
| At least one of my housestaff improved his/her professionalism/communication skills based on feedback I gave this block. | 76.9 (10) | 31.1 (5) | 0.02 |
| At least one of my housestaff improved his/her fund of knowledge based on feedback I gave this block. | 50.0 (8) | 52.9 (9) | 1.00 |
| Housestaff found the feedback I gave them useful. | 66.7 (10) | 62.5 (10) | 1.00 |
| I find it DIFFICULT to find time during inpatient rotations to give feedback to residents regarding their performance. | 50.0 (8) | 33.3 (6) | 0.49 |
Intervention attendings also shared their attitudes toward the feedback card and session. A majority felt that using 1 attending rounds as a feedback session helped create a dedicated time for giving feedback (68.8%), and that the feedback card helped them to give specific, constructive feedback (62.5%). Most attendings reported they would use the feedback card and session again during future inpatient blocks (81%), and would recommend them to other attendings (75%).
Qualitative data from intervention attending interviews revealed further thoughts about the feedback card and feedback session. Most attendings interviewed (7/8) felt that the card was useful for the structure and topic guidance it provided. Half felt that setting aside time for feedback was the more useful component. The other half reported that, because they usually set aside time for feedback regardless, the card was more useful. None of the attendings felt that the feedback card or session was detrimental for patient care or education, and many said that the intervention had positive effects on these areas. For example, 1 attending said that the session added to patient care because I used particular [patient] cases as examples for giving feedback.
DISCUSSION
In this randomized study, we found that a simple pocket feedback card and dedicated feedback session was acceptable to ward attendings and improved resident satisfaction with feedback. Unlike most prior studies of feedback, we demonstrated more feedback around skills needing improvement, and intervention residents felt the feedback they received helped them improve their skills. Our educational intervention was unique in that it combined a pocket card to structure feedback content and dedicated time to structure the feedback process, to address 2 of the major barriers to giving feedback: lack of time and lack of comfort.
The pocket card itself as a tool for improving feedback is innovative and valuable. As a short but directive guide, the card supports attendings' delivery of relevant and specific feedback about residents' performance, and because it is based on the ACGME competencies, it may help attendings focus feedback on areas in which they will later evaluate residents. The inclusion of a prespecified time for giving feedback was important as well, in that it allowed for face‐to‐face feedback to occur, as opposed to a passing comment after a presentation or brief notes in a written final evaluation. Both the card and the feedback session seemed equally important for the success of this intervention, with attitudes varying based on individual attending preferences. Those who usually set aside time for feedback on their own found the card more useful, whereas those who had more trouble finding time for feedback found the specific session more useful. Most attendings found the intervention as a whole helpful, and without any detrimental effects on patient care or education. The card and session may be particularly valuable for hospital attendings, given their growing presence as teachers and supervisors for residents, and their busy days on the wards.
Our study results have important implications for resident training in the hospital. Improving resident receipt of feedback about strengths and weaknesses is an ACGME training requirement, and specific guidance about how to improve skills is critical for focusing improvement efforts. Previous studies have demonstrated that directive feedback in medical training can lead to a variety of performance improvements, including better evaluations by other professionals,9, 16 and objective improvements in resident communication skills,17 chart documentation,18 and clinical management of patients.11, 15, 19 By improving the quality of feedback across several domains and facilitating the feedback process, our intervention may lead to similar improvements. Future studies should examine the global impact of guided feedback as in our study. Perhaps most importantly, attendings found the intervention acceptable and would recommend its use, implying longer term sustainability of its integration into the hospital routine.
One strength of our study was its prospective randomized design. Despite the importance of rigor in medical education research, there remains a paucity of randomized studies to evaluate educational interventions for residents in inpatient settings. Few studies of feedback interventions in particular have performed randomized trials,5, 6, 11 and only one has examined a feedback intervention in a randomized fashion in the inpatient setting.12 This evaluation of a 20‐minute intervention, and a reminder card for supervising attendings to improve written and verbal feedback to residents, modestly improved the amount of verbal feedback given to residents, but did not impact the number of residents receiving mid‐rotation feedback or feedback overall as our study did by report.12
There were several important limitations to our study. First, because this was a single institution study, we only achieved modest sample sizes, particularly in the attending groups, and were unable to assess all of the differences in attending attitudes related to feedback. Second, control and intervention participants were on service simultaneously, which may have led to contamination of the control group and an underestimation of the true impact of our intervention. Since residents were not exclusive to 1 study group on 1 occasion (18 of the 93 residents participated during 2 separate blocks), our results may be biased. In particular, those residents who had the intervention first, and were subsequently in the control group, may have rated the control experience worse than they would have otherwise, creating a bias in favor of a positive result for our intervention. Nonetheless, we believe this situation was uncommon and the potential associated bias minimal. Further, this study assessed attitudes related to feedback and self‐reported knowledge and skills, but did not directly assess resident knowledge, skills, or patient outcomes. We recognize the importance of these outcomes and hope that future interventions can determine these important downstream effects of feedback. We were also unable to assess the card and session's impact on attendings' comfort with feedback, because most attendings in both groups reported feeling comfortable giving feedback. This result may indicate that attendings actually are comfortable giving feedback, or may suggest some element of social desirability bias. Finally, in this study, we designed an intervention which combined the pocket card and dedicated feedback time. We did not quantitatively examine the effect of either component alone, and it is unclear if offering the feedback card without protected time or offering protected time without a guide would have impacted feedback on the wards. However, qualitative data from our study support the use of both components, and implementing the 2 components together is feasible in any inpatient teaching setting.
Despite these limitations, protected time for feedback guided by a pocket feedback card is a simple intervention that appears to improve feedback quantity and quality for ward residents, and guides them to improve their performance. Our low‐intensity intervention helped attendings give residents the tools to improve their clinical and communication skills. An opportunity to make a positive impact on resident education with such a small intervention is rare. The use of a feedback card with protected feedback time could be easily implemented in any training program, and is a valuable tool for busy hospitalists who are more commonly supervising residents on their inpatient rotations.
- .Feedback in clinical medical education.JAMA.1983;250(6):777–781.
- ,.Giving feedback in medical education: verification of recommended techniques.J Gen Intern Med.1998;13(2):111–116.
- ,,,,.Systematic review of the literature on assessment, feedback and physicians' clinical performance: BEME Guide No. 7.Med Teach.2006;28(2):117–128.
- ,,,.Missed opportunities: a descriptive assessment of teaching and attitudes regarding communication skills in a surgical residency.Curr Surg.2006;63(6):401–409.
- ,,.Impact of a 360‐degree professionalism assessment on faculty comfort and skills in feedback delivery.J Gen Intern Med.2008;23(7):969–972.
- ,.Daily encounter cards facilitate competency‐based feedback while leniency bias persists.CJEM.2008;10(1):44–50.
- ,,,,.Teaching compassion and respect. Attending physicians' responses to problematic behaviors.J Gen Intern Med.1999;14(1):49–55.
- .Faculty and the observation of trainees' clinical skills: problems and opportunities.Acad Med.2004;79(1):16–22.
- ,.Direct observation of residents in the emergency department: a structured educational program.Acad Emerg Med.2009;16(4):343–351.
- ,,, et al.Evaluation of a novel assessment form for observing medical residents: a randomised, controlled trial.Med Educ.2008;42(12):1234–1242.
- ,,, et al.Resident evaluations: the use of daily evaluation forms in rheumatology ambulatory care.J Rheumatol.2009;36(6):1298–1303.
- ,,,.Effectiveness of a focused educational intervention on resident evaluations from faculty a randomized controlled trial.J Gen Intern Med.2001;16(7):427–434.
- ,,.Effects of training in direct observation of medical residents' clinical competence: a randomized trial.Ann Intern Med.2004;140(11):874–881.
- Internal Medicine Program Requirements. ACGME. July 1, 2009. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/140_internal_medicine_07012009.pdf. Accessed November 8,2009.
- ,,,,.How to use the core competencies in hospital medicine: a framework for curriculum development.J Hosp Med. 2006;1(suppl 1):57–67.
- ,,,,.Debriefing in the intensive care unit: a feedback tool to facilitate bedside teaching.Crit Care Med.2007;35(3):738–754.
- ,,, et al.Use of an innovative video feedback technique to enhance communication skills training.Med Educ.2004;38(2):145–157.
- .The impact of feedback to medical housestaff on chart documentation and quality of care in the outpatient setting.J Gen Intern Med.1997;12(6):352–356.
- ,,,.Feedback and the mini clinical evaluation exercise.J Gen Intern Med.2004;19(5 pt 2):558–561.
Feedback has long been recognized as pivotal to the attainment of clinical acumen and skills in medical training.1 Formative feedback can give trainees insight into their strengths and weaknesses, and provide them with clear goals and methods to attain those goals.1, 2 In fact, feedback given regularly over time by a respected figure has shown to improve physician performance.3 However, most faculty are not trained to provide effective feedback. As a result, supervisors often believe they are giving more feedback than trainees believe they are receiving, and residents receive little feedback that they perceive as useful.4 Most residents receive little to no feedback on their communications skills4 or professionalism,5 and rarely receive corrective feedback.6, 7
Faculty may fail to give feedback to residents for a number of reasons. Those barriers most commonly cited in the literature are discomfort with criticizing residents,6, 7 lack of time,4 and lack of direct observation of residents in clinical settings.810 Several studies have looked at tools to guide feedback and address the barrier of discomfort with criticism.6, 7, 11 Some showed improvements in overall feedback, though often supervisors gave only positive feedback and avoided giving feedback about weaknesses.6, 7, 11 Despite the recognition of lack of time as a barrier to feedback,4 most studies on feedback interventions thus far have not included setting aside time for the feedback to occur.6, 7, 11, 12 Finally, a number of studies utilized objective structured clinical examinations (OSCEs) coupled with immediate feedback to improve direct observation of residents, with success in improving feedback related to the encounter.9, 10, 13 To address the gaps in the current literature, the goals of our study were to address 2 specific barriers to feedback for residents: lack of time and discomfort with giving feedback.
The aim of this study was to improve Internal Medicine (IM) residents' and attendings' experiences with feedback on the wards using a pocket card and a dedicated feedback session. We developed and evaluated the pocket feedback card and session for faculty to improve the quality and frequency of their feedback to residents in the inpatient setting. We performed a randomized trial to evaluate our intervention. We hypothesized that the intervention would: 1) improve the quality and quantity of attendings' feedback given to IM ward residents; and 2) improve attendings' comfort with feedback delivery on the wards.
PARTICIPANTS AND METHODS
Setting
The study was performed at Mount Sinai Medical Center in New York City, New York, between July 2008 and January 2009.
Participants
Participants in this study were IM residents and ward teaching attendings on inpatient ward teams at Mount Sinai Medical Center from July 2008 to January 2009. There are 12 ward teams on 3 inpatient services (each service has 4 teams) during each block at our hospital. Ward teams are made up of 1 teaching attending, 1 resident, 1 to 3 interns, and 1 to 2 medical students. The majority of attendings are on the ward service for 4‐week blocks, but some are only on for 1 or 2 weeks. Teams included in the randomization were the General Medicine and Gastroenterology/Cardiology service teams. Half of the General Medicine service attendings are hospitalists. Ward teams were excluded from the study randomization if the attending on the team was on the wards for less than 2 weeks, or if the attending had already been assigned to the experimental group in a previous block, given the influence of having used the card and feedback session previously. Since residents were unaware of the intervention and random assignments were based on attendings, residents could be assigned to the intervention group or the control group on any given inpatient rotation. Therefore, a resident could be in the control group in 1 block and the intervention group in his/her next block on the wards or vice versa, or could be assigned to either the intervention or the control group on more than 1 occasion. Because resident participants were blinded to their team's assignment (as intervention or control) and all surveys were anonymous (tracked as intervention or control by the team name only), it was not possible to exclude residents based on their prior participation or to match the surveys completed by the same residents.
Study Design
We performed a prospective randomized study to evaluate our educational innovation. The unit of randomization was the ward team. For each block, approximately half of the 6‐8 teams were randomized to the intervention group and half to the control group. Randomization assignments were completed the day prior to the start of the block using the random allocation software based on the ward team letters (blind to the attending and resident names). Of the 48 possible ward teams (8 teams per block over 6 blocks), 36 teams were randomized to the intervention or control groups, and 12 teams were not based on the above exclusion criteria. Of the 36 teams, 16 (composed of 16 attendings and 48 residents and interns) were randomized to the intervention group, and 20 (composed of 20 attendings and 63 residents and interns) were randomized to the control group.
The study was blinded such that residents and attendings in the control group were unaware of the study. The study was exempt from IRB review by the Mount Sinai Institutional Review Board, and Grants and Contracts Office, as an evaluation of the effectiveness of an instructional technique in medical education.
Intervention Design
We designed a pocket feedback card to guide a feedback session and assist attendings in giving useful feedback to IM residents on the wards (Figure 1).14 The individual items and categories were adapted from the Accreditation Council for Graduate Medical Education (ACGME) Common Program Requirements Core Competencies section and were revised via the expert consensus of the authors.14 We included 20 items related to resident skills, knowledge, attitudes, and behaviors important to the care of hospitalized patients, grouped under the 6 ACGME core competency domains.14 Many of these items correspond to competencies in the Society of Hospital Medicine (SHM) Core Competencies; in particular, the categories of Systems‐Based Practice and Practice‐Based Learning mirror competencies in the SHM Core Competencies Healthcare Systems chapter.15 Each item utilized a 5‐point Likert scale (1 = very poor, 3 = at expected level, 5 = superior) to evaluate resident performance (Figure 1). We created this card to serve as a directive and specific guide for attendings to provide feedback about specific domains and to give more constructive feedback. The card was to be used during a specific dedicated feedback session in order to overcome the commonly cited barrier of lack of time.
Program Implementation
On the first day of the block, both groups of attendings received the standard inpatient ward orientation given by the program director, including instructions about teaching and administrative responsibilities, and explicit instructions to provide mid‐rotation feedback to residents. Attendings randomized to the intervention group had an additional 5‐minute orientation given by 1 of the investigators. The orientation included a brief discussion on the importance of feedback and an introduction to the items on the card.2 In addition, faculty were instructed to dedicate 1 mid‐rotation attending rounds as a feedback session, to meet individually for 10‐15 minutes with each of the 3‐4 residents on their team, and to use the card to provide feedback on skills in each domain. As noted on the feedback card, if a resident scored less than 3 on a skill set, the attending was instructed to give examples of skills within that domain needing improvement and to offer suggestions for improvement. The intervention group was also asked not to discuss the card or session with others. No other instructions were provided.
Survey Design
At the end of each block, residents and attendings in both groups completed questionnaires to assess satisfaction with, and attitudes toward, feedback (Supporting Information Appendices 1 and 2 in the online version of this article). Survey questions were based on the competency areas included in the feedback card, previously published surveys evaluating feedback interventions,5, 9, 11 and expert opinion. The resident survey was designed to address the impact of feedback on the domains of resident knowledge, clinical and communication skills, and attitudes about feedback from supervisors and peers. We utilized a 5‐point Likert scale including: strongly disagree, disagree, neutral, agree, and strongly agree. The attending survey addressed attendings' satisfaction with feedback encounters and resident performance. At the completion of the study, investigators compared responses in intervention and control groups.
Statistical Analysis
For purposes of analysis, due to the relatively small number of responses for certain answer choices, the Likert scale was converted to a dichotomous variable. The responses of agree and strongly agree were coded as agree; and disagree, strongly disagree, and neutral were coded as disagree. Neutral was coded as disagree in order to avoid overestimating positive attitudes and, in effect, bias our results toward the null hypothesis. Differences between groups were analyzed using chi‐square Fisher's exact test (2‐sided).
Qualitative Interviews
In order to understand the relative contribution of the feedback card versus the feedback session, we performed a qualitative survey of attendings in the intervention group. Following the conclusion of the study period, we selected a convenience sample of 8 attendings from the intervention group for these brief qualitative interviews. We asked 3 basic questions. Was the intervention of the feedback card and dedicated time for feedback useful? Did you find one component, either the card or the dedicated time for feedback, more useful than the other? Were there any negative effects on patient care, education, or other areas, from using an attending rounds as a feedback session? This data was coded and analyzed for common themes.
RESULTS
During the 6‐month study period, 34 teaching attendings (over 36 attending inpatient blocks) and 93 IM residents (over 111 resident inpatient blocks) participated in the study. Thirty‐four of 36 attending surveys and 96 of 111 resident surveys were completed. The overall survey response rates for residents and attendings were 85% and 94%, respectively. Two attendings participated during 2 separate blocks, first in the control group and then in the intervention group, and 18 residents participated during 2 separate blocks. No attendings or residents participated more than twice.
Resident survey response rate was 81.2% in the intervention group and 87.3% in the control group (Table 1). Residents in the intervention group reported receiving more feedback regarding skills they did well (89.7% vs 63.6%, P = 0.004) and skills needing improvement (51.3% vs 25.5%, P = 0.02) than those in the control group. In addition, more intervention residents reported receiving useful information regarding how to improve their skills (53.8% vs 27.3%, P = 0.01), and reported actually improving both their clinical skills (61.5% vs 27.8%, P = 0.001) and their professionalism/communication skills (51.3% vs 29.1%, P = 0.03) based on feedback received from attendings.
| Survey Item | Resident Intervention Agree* % (No.) N = 39 | Resident Control Agree*% (No.) N = 55 | P Value |
|---|---|---|---|
| |||
| I did NOT receive a sufficient amount of feedback from my attending supervisor(s) this block. | 20.5 (8) | 38.2 (21) | 0.08 |
| I received feedback from my attending regarding skills I did well during this block. | 89.7 (35) | 63.6 (35) | 0.004 |
| I received feedback from my attending regarding specific skills that needed improvement during this block. | 51.3 (20) | 25.5 (14) | 0.02 |
| I received useful information from my attending about how to improve my skills during this block. | 53.8 (21) | 27.3 (15) | 0.01 |
| I improved my clinical skills based on feedback I received from my attending this block. | 61.5 (24) | 27.8 (15) | 0.001 |
| I improved my professionalism/communication skills based on feedback I received from my attending this block. | 51.3 (20) | 29.1 (16) | 0.03 |
| I improved my knowledge base because of feedback I received from my attending this block. | 64.1 (25) | 60.0 (33) | 0.83 |
| The feedback I received from my attending this block gave me an overall sense of my performance more than it helped me identify specific areas for improvement. | 64.1 (25) | 65.5 (36) | 1.0 |
| Feedback from colleagues (other interns and residents) is more helpful than feedback from attendings. | 41.0 (16) | 43.6 (24) | 0.84 |
| Independent of feedback received from others, I am able to identify areas in which I need improvement. | 84.6 (33) | 80.0 (44) | 0.60 |
The attending survey response rates for the intervention and control groups were 100% and 90%, respectively. In general, both groups of attendings reported that they were comfortable giving feedback and that they did, in fact, give feedback in each area during their ward block (Table 2). More intervention attendings felt that at least 1 of their residents improved their professionalism/communication skills based on the feedback given (76.9% vs 31.1%, P = 0.02). There were no other significant differences between the groups of attendings.
| Survey Item | Attending Intervention Agree* % (No.) N = 16 | Attending Control Agree* % (No.) N = 18 | P Value |
|---|---|---|---|
| |||
| Giving feedback to housestaff was DIFFICULT this block. | 6.3 (1) | 16.7 (3) | 0.60 |
| I was comfortable giving feedback to my housestaff this block. | 93.8 (15) | 94.4 (17) | 1.00 |
| I did NOT give a sufficient amount of feedback to my housestaff this block. | 18.8 (3) | 38.9 (7) | 0.27 |
| My skills in giving feedback improved during this block. | 50 (8) | 16.7 (3) | 0.07 |
| I gave feedback to housestaff regarding skills they did well during this block. | 100 (16) | 94.4 (17) | 1.00 |
| I gave feedback to housestaff which targeted specific areas for their improvement. | 81.3 (13) | 70.6 (12) | 0.69 |
| At least one of my housestaff improved his/her clinical skills based on feedback I gave this block. | 68.8 (11) | 47.1 (8) | 0.30 |
| At least one of my housestaff improved his/her professionalism/communication skills based on feedback I gave this block. | 76.9 (10) | 31.1 (5) | 0.02 |
| At least one of my housestaff improved his/her fund of knowledge based on feedback I gave this block. | 50.0 (8) | 52.9 (9) | 1.00 |
| Housestaff found the feedback I gave them useful. | 66.7 (10) | 62.5 (10) | 1.00 |
| I find it DIFFICULT to find time during inpatient rotations to give feedback to residents regarding their performance. | 50.0 (8) | 33.3 (6) | 0.49 |
Intervention attendings also shared their attitudes toward the feedback card and session. A majority felt that using 1 attending rounds as a feedback session helped create a dedicated time for giving feedback (68.8%), and that the feedback card helped them to give specific, constructive feedback (62.5%). Most attendings reported they would use the feedback card and session again during future inpatient blocks (81%), and would recommend them to other attendings (75%).
Qualitative data from intervention attending interviews revealed further thoughts about the feedback card and feedback session. Most attendings interviewed (7/8) felt that the card was useful for the structure and topic guidance it provided. Half felt that setting aside time for feedback was the more useful component. The other half reported that, because they usually set aside time for feedback regardless, the card was more useful. None of the attendings felt that the feedback card or session was detrimental for patient care or education, and many said that the intervention had positive effects on these areas. For example, 1 attending said that the session added to patient care because I used particular [patient] cases as examples for giving feedback.
DISCUSSION
In this randomized study, we found that a simple pocket feedback card and dedicated feedback session was acceptable to ward attendings and improved resident satisfaction with feedback. Unlike most prior studies of feedback, we demonstrated more feedback around skills needing improvement, and intervention residents felt the feedback they received helped them improve their skills. Our educational intervention was unique in that it combined a pocket card to structure feedback content and dedicated time to structure the feedback process, to address 2 of the major barriers to giving feedback: lack of time and lack of comfort.
The pocket card itself as a tool for improving feedback is innovative and valuable. As a short but directive guide, the card supports attendings' delivery of relevant and specific feedback about residents' performance, and because it is based on the ACGME competencies, it may help attendings focus feedback on areas in which they will later evaluate residents. The inclusion of a prespecified time for giving feedback was important as well, in that it allowed for face‐to‐face feedback to occur, as opposed to a passing comment after a presentation or brief notes in a written final evaluation. Both the card and the feedback session seemed equally important for the success of this intervention, with attitudes varying based on individual attending preferences. Those who usually set aside time for feedback on their own found the card more useful, whereas those who had more trouble finding time for feedback found the specific session more useful. Most attendings found the intervention as a whole helpful, and without any detrimental effects on patient care or education. The card and session may be particularly valuable for hospital attendings, given their growing presence as teachers and supervisors for residents, and their busy days on the wards.
Our study results have important implications for resident training in the hospital. Improving resident receipt of feedback about strengths and weaknesses is an ACGME training requirement, and specific guidance about how to improve skills is critical for focusing improvement efforts. Previous studies have demonstrated that directive feedback in medical training can lead to a variety of performance improvements, including better evaluations by other professionals,9, 16 and objective improvements in resident communication skills,17 chart documentation,18 and clinical management of patients.11, 15, 19 By improving the quality of feedback across several domains and facilitating the feedback process, our intervention may lead to similar improvements. Future studies should examine the global impact of guided feedback as in our study. Perhaps most importantly, attendings found the intervention acceptable and would recommend its use, implying longer term sustainability of its integration into the hospital routine.
One strength of our study was its prospective randomized design. Despite the importance of rigor in medical education research, there remains a paucity of randomized studies to evaluate educational interventions for residents in inpatient settings. Few studies of feedback interventions in particular have performed randomized trials,5, 6, 11 and only one has examined a feedback intervention in a randomized fashion in the inpatient setting.12 This evaluation of a 20‐minute intervention, and a reminder card for supervising attendings to improve written and verbal feedback to residents, modestly improved the amount of verbal feedback given to residents, but did not impact the number of residents receiving mid‐rotation feedback or feedback overall as our study did by report.12
There were several important limitations to our study. First, because this was a single institution study, we only achieved modest sample sizes, particularly in the attending groups, and were unable to assess all of the differences in attending attitudes related to feedback. Second, control and intervention participants were on service simultaneously, which may have led to contamination of the control group and an underestimation of the true impact of our intervention. Since residents were not exclusive to 1 study group on 1 occasion (18 of the 93 residents participated during 2 separate blocks), our results may be biased. In particular, those residents who had the intervention first, and were subsequently in the control group, may have rated the control experience worse than they would have otherwise, creating a bias in favor of a positive result for our intervention. Nonetheless, we believe this situation was uncommon and the potential associated bias minimal. Further, this study assessed attitudes related to feedback and self‐reported knowledge and skills, but did not directly assess resident knowledge, skills, or patient outcomes. We recognize the importance of these outcomes and hope that future interventions can determine these important downstream effects of feedback. We were also unable to assess the card and session's impact on attendings' comfort with feedback, because most attendings in both groups reported feeling comfortable giving feedback. This result may indicate that attendings actually are comfortable giving feedback, or may suggest some element of social desirability bias. Finally, in this study, we designed an intervention which combined the pocket card and dedicated feedback time. We did not quantitatively examine the effect of either component alone, and it is unclear if offering the feedback card without protected time or offering protected time without a guide would have impacted feedback on the wards. However, qualitative data from our study support the use of both components, and implementing the 2 components together is feasible in any inpatient teaching setting.
Despite these limitations, protected time for feedback guided by a pocket feedback card is a simple intervention that appears to improve feedback quantity and quality for ward residents, and guides them to improve their performance. Our low‐intensity intervention helped attendings give residents the tools to improve their clinical and communication skills. An opportunity to make a positive impact on resident education with such a small intervention is rare. The use of a feedback card with protected feedback time could be easily implemented in any training program, and is a valuable tool for busy hospitalists who are more commonly supervising residents on their inpatient rotations.
Feedback has long been recognized as pivotal to the attainment of clinical acumen and skills in medical training.1 Formative feedback can give trainees insight into their strengths and weaknesses, and provide them with clear goals and methods to attain those goals.1, 2 In fact, feedback given regularly over time by a respected figure has shown to improve physician performance.3 However, most faculty are not trained to provide effective feedback. As a result, supervisors often believe they are giving more feedback than trainees believe they are receiving, and residents receive little feedback that they perceive as useful.4 Most residents receive little to no feedback on their communications skills4 or professionalism,5 and rarely receive corrective feedback.6, 7
Faculty may fail to give feedback to residents for a number of reasons. Those barriers most commonly cited in the literature are discomfort with criticizing residents,6, 7 lack of time,4 and lack of direct observation of residents in clinical settings.810 Several studies have looked at tools to guide feedback and address the barrier of discomfort with criticism.6, 7, 11 Some showed improvements in overall feedback, though often supervisors gave only positive feedback and avoided giving feedback about weaknesses.6, 7, 11 Despite the recognition of lack of time as a barrier to feedback,4 most studies on feedback interventions thus far have not included setting aside time for the feedback to occur.6, 7, 11, 12 Finally, a number of studies utilized objective structured clinical examinations (OSCEs) coupled with immediate feedback to improve direct observation of residents, with success in improving feedback related to the encounter.9, 10, 13 To address the gaps in the current literature, the goals of our study were to address 2 specific barriers to feedback for residents: lack of time and discomfort with giving feedback.
The aim of this study was to improve Internal Medicine (IM) residents' and attendings' experiences with feedback on the wards using a pocket card and a dedicated feedback session. We developed and evaluated the pocket feedback card and session for faculty to improve the quality and frequency of their feedback to residents in the inpatient setting. We performed a randomized trial to evaluate our intervention. We hypothesized that the intervention would: 1) improve the quality and quantity of attendings' feedback given to IM ward residents; and 2) improve attendings' comfort with feedback delivery on the wards.
PARTICIPANTS AND METHODS
Setting
The study was performed at Mount Sinai Medical Center in New York City, New York, between July 2008 and January 2009.
Participants
Participants in this study were IM residents and ward teaching attendings on inpatient ward teams at Mount Sinai Medical Center from July 2008 to January 2009. There are 12 ward teams on 3 inpatient services (each service has 4 teams) during each block at our hospital. Ward teams are made up of 1 teaching attending, 1 resident, 1 to 3 interns, and 1 to 2 medical students. The majority of attendings are on the ward service for 4‐week blocks, but some are only on for 1 or 2 weeks. Teams included in the randomization were the General Medicine and Gastroenterology/Cardiology service teams. Half of the General Medicine service attendings are hospitalists. Ward teams were excluded from the study randomization if the attending on the team was on the wards for less than 2 weeks, or if the attending had already been assigned to the experimental group in a previous block, given the influence of having used the card and feedback session previously. Since residents were unaware of the intervention and random assignments were based on attendings, residents could be assigned to the intervention group or the control group on any given inpatient rotation. Therefore, a resident could be in the control group in 1 block and the intervention group in his/her next block on the wards or vice versa, or could be assigned to either the intervention or the control group on more than 1 occasion. Because resident participants were blinded to their team's assignment (as intervention or control) and all surveys were anonymous (tracked as intervention or control by the team name only), it was not possible to exclude residents based on their prior participation or to match the surveys completed by the same residents.
Study Design
We performed a prospective randomized study to evaluate our educational innovation. The unit of randomization was the ward team. For each block, approximately half of the 6‐8 teams were randomized to the intervention group and half to the control group. Randomization assignments were completed the day prior to the start of the block using the random allocation software based on the ward team letters (blind to the attending and resident names). Of the 48 possible ward teams (8 teams per block over 6 blocks), 36 teams were randomized to the intervention or control groups, and 12 teams were not based on the above exclusion criteria. Of the 36 teams, 16 (composed of 16 attendings and 48 residents and interns) were randomized to the intervention group, and 20 (composed of 20 attendings and 63 residents and interns) were randomized to the control group.
The study was blinded such that residents and attendings in the control group were unaware of the study. The study was exempt from IRB review by the Mount Sinai Institutional Review Board, and Grants and Contracts Office, as an evaluation of the effectiveness of an instructional technique in medical education.
Intervention Design
We designed a pocket feedback card to guide a feedback session and assist attendings in giving useful feedback to IM residents on the wards (Figure 1).14 The individual items and categories were adapted from the Accreditation Council for Graduate Medical Education (ACGME) Common Program Requirements Core Competencies section and were revised via the expert consensus of the authors.14 We included 20 items related to resident skills, knowledge, attitudes, and behaviors important to the care of hospitalized patients, grouped under the 6 ACGME core competency domains.14 Many of these items correspond to competencies in the Society of Hospital Medicine (SHM) Core Competencies; in particular, the categories of Systems‐Based Practice and Practice‐Based Learning mirror competencies in the SHM Core Competencies Healthcare Systems chapter.15 Each item utilized a 5‐point Likert scale (1 = very poor, 3 = at expected level, 5 = superior) to evaluate resident performance (Figure 1). We created this card to serve as a directive and specific guide for attendings to provide feedback about specific domains and to give more constructive feedback. The card was to be used during a specific dedicated feedback session in order to overcome the commonly cited barrier of lack of time.
Program Implementation
On the first day of the block, both groups of attendings received the standard inpatient ward orientation given by the program director, including instructions about teaching and administrative responsibilities, and explicit instructions to provide mid‐rotation feedback to residents. Attendings randomized to the intervention group had an additional 5‐minute orientation given by 1 of the investigators. The orientation included a brief discussion on the importance of feedback and an introduction to the items on the card.2 In addition, faculty were instructed to dedicate 1 mid‐rotation attending rounds as a feedback session, to meet individually for 10‐15 minutes with each of the 3‐4 residents on their team, and to use the card to provide feedback on skills in each domain. As noted on the feedback card, if a resident scored less than 3 on a skill set, the attending was instructed to give examples of skills within that domain needing improvement and to offer suggestions for improvement. The intervention group was also asked not to discuss the card or session with others. No other instructions were provided.
Survey Design
At the end of each block, residents and attendings in both groups completed questionnaires to assess satisfaction with, and attitudes toward, feedback (Supporting Information Appendices 1 and 2 in the online version of this article). Survey questions were based on the competency areas included in the feedback card, previously published surveys evaluating feedback interventions,5, 9, 11 and expert opinion. The resident survey was designed to address the impact of feedback on the domains of resident knowledge, clinical and communication skills, and attitudes about feedback from supervisors and peers. We utilized a 5‐point Likert scale including: strongly disagree, disagree, neutral, agree, and strongly agree. The attending survey addressed attendings' satisfaction with feedback encounters and resident performance. At the completion of the study, investigators compared responses in intervention and control groups.
Statistical Analysis
For purposes of analysis, due to the relatively small number of responses for certain answer choices, the Likert scale was converted to a dichotomous variable. The responses of agree and strongly agree were coded as agree; and disagree, strongly disagree, and neutral were coded as disagree. Neutral was coded as disagree in order to avoid overestimating positive attitudes and, in effect, bias our results toward the null hypothesis. Differences between groups were analyzed using chi‐square Fisher's exact test (2‐sided).
Qualitative Interviews
In order to understand the relative contribution of the feedback card versus the feedback session, we performed a qualitative survey of attendings in the intervention group. Following the conclusion of the study period, we selected a convenience sample of 8 attendings from the intervention group for these brief qualitative interviews. We asked 3 basic questions. Was the intervention of the feedback card and dedicated time for feedback useful? Did you find one component, either the card or the dedicated time for feedback, more useful than the other? Were there any negative effects on patient care, education, or other areas, from using an attending rounds as a feedback session? This data was coded and analyzed for common themes.
RESULTS
During the 6‐month study period, 34 teaching attendings (over 36 attending inpatient blocks) and 93 IM residents (over 111 resident inpatient blocks) participated in the study. Thirty‐four of 36 attending surveys and 96 of 111 resident surveys were completed. The overall survey response rates for residents and attendings were 85% and 94%, respectively. Two attendings participated during 2 separate blocks, first in the control group and then in the intervention group, and 18 residents participated during 2 separate blocks. No attendings or residents participated more than twice.
Resident survey response rate was 81.2% in the intervention group and 87.3% in the control group (Table 1). Residents in the intervention group reported receiving more feedback regarding skills they did well (89.7% vs 63.6%, P = 0.004) and skills needing improvement (51.3% vs 25.5%, P = 0.02) than those in the control group. In addition, more intervention residents reported receiving useful information regarding how to improve their skills (53.8% vs 27.3%, P = 0.01), and reported actually improving both their clinical skills (61.5% vs 27.8%, P = 0.001) and their professionalism/communication skills (51.3% vs 29.1%, P = 0.03) based on feedback received from attendings.
| Survey Item | Resident Intervention Agree* % (No.) N = 39 | Resident Control Agree*% (No.) N = 55 | P Value |
|---|---|---|---|
| |||
| I did NOT receive a sufficient amount of feedback from my attending supervisor(s) this block. | 20.5 (8) | 38.2 (21) | 0.08 |
| I received feedback from my attending regarding skills I did well during this block. | 89.7 (35) | 63.6 (35) | 0.004 |
| I received feedback from my attending regarding specific skills that needed improvement during this block. | 51.3 (20) | 25.5 (14) | 0.02 |
| I received useful information from my attending about how to improve my skills during this block. | 53.8 (21) | 27.3 (15) | 0.01 |
| I improved my clinical skills based on feedback I received from my attending this block. | 61.5 (24) | 27.8 (15) | 0.001 |
| I improved my professionalism/communication skills based on feedback I received from my attending this block. | 51.3 (20) | 29.1 (16) | 0.03 |
| I improved my knowledge base because of feedback I received from my attending this block. | 64.1 (25) | 60.0 (33) | 0.83 |
| The feedback I received from my attending this block gave me an overall sense of my performance more than it helped me identify specific areas for improvement. | 64.1 (25) | 65.5 (36) | 1.0 |
| Feedback from colleagues (other interns and residents) is more helpful than feedback from attendings. | 41.0 (16) | 43.6 (24) | 0.84 |
| Independent of feedback received from others, I am able to identify areas in which I need improvement. | 84.6 (33) | 80.0 (44) | 0.60 |
The attending survey response rates for the intervention and control groups were 100% and 90%, respectively. In general, both groups of attendings reported that they were comfortable giving feedback and that they did, in fact, give feedback in each area during their ward block (Table 2). More intervention attendings felt that at least 1 of their residents improved their professionalism/communication skills based on the feedback given (76.9% vs 31.1%, P = 0.02). There were no other significant differences between the groups of attendings.
| Survey Item | Attending Intervention Agree* % (No.) N = 16 | Attending Control Agree* % (No.) N = 18 | P Value |
|---|---|---|---|
| |||
| Giving feedback to housestaff was DIFFICULT this block. | 6.3 (1) | 16.7 (3) | 0.60 |
| I was comfortable giving feedback to my housestaff this block. | 93.8 (15) | 94.4 (17) | 1.00 |
| I did NOT give a sufficient amount of feedback to my housestaff this block. | 18.8 (3) | 38.9 (7) | 0.27 |
| My skills in giving feedback improved during this block. | 50 (8) | 16.7 (3) | 0.07 |
| I gave feedback to housestaff regarding skills they did well during this block. | 100 (16) | 94.4 (17) | 1.00 |
| I gave feedback to housestaff which targeted specific areas for their improvement. | 81.3 (13) | 70.6 (12) | 0.69 |
| At least one of my housestaff improved his/her clinical skills based on feedback I gave this block. | 68.8 (11) | 47.1 (8) | 0.30 |
| At least one of my housestaff improved his/her professionalism/communication skills based on feedback I gave this block. | 76.9 (10) | 31.1 (5) | 0.02 |
| At least one of my housestaff improved his/her fund of knowledge based on feedback I gave this block. | 50.0 (8) | 52.9 (9) | 1.00 |
| Housestaff found the feedback I gave them useful. | 66.7 (10) | 62.5 (10) | 1.00 |
| I find it DIFFICULT to find time during inpatient rotations to give feedback to residents regarding their performance. | 50.0 (8) | 33.3 (6) | 0.49 |
Intervention attendings also shared their attitudes toward the feedback card and session. A majority felt that using 1 attending rounds as a feedback session helped create a dedicated time for giving feedback (68.8%), and that the feedback card helped them to give specific, constructive feedback (62.5%). Most attendings reported they would use the feedback card and session again during future inpatient blocks (81%), and would recommend them to other attendings (75%).
Qualitative data from intervention attending interviews revealed further thoughts about the feedback card and feedback session. Most attendings interviewed (7/8) felt that the card was useful for the structure and topic guidance it provided. Half felt that setting aside time for feedback was the more useful component. The other half reported that, because they usually set aside time for feedback regardless, the card was more useful. None of the attendings felt that the feedback card or session was detrimental for patient care or education, and many said that the intervention had positive effects on these areas. For example, 1 attending said that the session added to patient care because I used particular [patient] cases as examples for giving feedback.
DISCUSSION
In this randomized study, we found that a simple pocket feedback card and dedicated feedback session was acceptable to ward attendings and improved resident satisfaction with feedback. Unlike most prior studies of feedback, we demonstrated more feedback around skills needing improvement, and intervention residents felt the feedback they received helped them improve their skills. Our educational intervention was unique in that it combined a pocket card to structure feedback content and dedicated time to structure the feedback process, to address 2 of the major barriers to giving feedback: lack of time and lack of comfort.
The pocket card itself as a tool for improving feedback is innovative and valuable. As a short but directive guide, the card supports attendings' delivery of relevant and specific feedback about residents' performance, and because it is based on the ACGME competencies, it may help attendings focus feedback on areas in which they will later evaluate residents. The inclusion of a prespecified time for giving feedback was important as well, in that it allowed for face‐to‐face feedback to occur, as opposed to a passing comment after a presentation or brief notes in a written final evaluation. Both the card and the feedback session seemed equally important for the success of this intervention, with attitudes varying based on individual attending preferences. Those who usually set aside time for feedback on their own found the card more useful, whereas those who had more trouble finding time for feedback found the specific session more useful. Most attendings found the intervention as a whole helpful, and without any detrimental effects on patient care or education. The card and session may be particularly valuable for hospital attendings, given their growing presence as teachers and supervisors for residents, and their busy days on the wards.
Our study results have important implications for resident training in the hospital. Improving resident receipt of feedback about strengths and weaknesses is an ACGME training requirement, and specific guidance about how to improve skills is critical for focusing improvement efforts. Previous studies have demonstrated that directive feedback in medical training can lead to a variety of performance improvements, including better evaluations by other professionals,9, 16 and objective improvements in resident communication skills,17 chart documentation,18 and clinical management of patients.11, 15, 19 By improving the quality of feedback across several domains and facilitating the feedback process, our intervention may lead to similar improvements. Future studies should examine the global impact of guided feedback as in our study. Perhaps most importantly, attendings found the intervention acceptable and would recommend its use, implying longer term sustainability of its integration into the hospital routine.
One strength of our study was its prospective randomized design. Despite the importance of rigor in medical education research, there remains a paucity of randomized studies to evaluate educational interventions for residents in inpatient settings. Few studies of feedback interventions in particular have performed randomized trials,5, 6, 11 and only one has examined a feedback intervention in a randomized fashion in the inpatient setting.12 This evaluation of a 20‐minute intervention, and a reminder card for supervising attendings to improve written and verbal feedback to residents, modestly improved the amount of verbal feedback given to residents, but did not impact the number of residents receiving mid‐rotation feedback or feedback overall as our study did by report.12
There were several important limitations to our study. First, because this was a single institution study, we only achieved modest sample sizes, particularly in the attending groups, and were unable to assess all of the differences in attending attitudes related to feedback. Second, control and intervention participants were on service simultaneously, which may have led to contamination of the control group and an underestimation of the true impact of our intervention. Since residents were not exclusive to 1 study group on 1 occasion (18 of the 93 residents participated during 2 separate blocks), our results may be biased. In particular, those residents who had the intervention first, and were subsequently in the control group, may have rated the control experience worse than they would have otherwise, creating a bias in favor of a positive result for our intervention. Nonetheless, we believe this situation was uncommon and the potential associated bias minimal. Further, this study assessed attitudes related to feedback and self‐reported knowledge and skills, but did not directly assess resident knowledge, skills, or patient outcomes. We recognize the importance of these outcomes and hope that future interventions can determine these important downstream effects of feedback. We were also unable to assess the card and session's impact on attendings' comfort with feedback, because most attendings in both groups reported feeling comfortable giving feedback. This result may indicate that attendings actually are comfortable giving feedback, or may suggest some element of social desirability bias. Finally, in this study, we designed an intervention which combined the pocket card and dedicated feedback time. We did not quantitatively examine the effect of either component alone, and it is unclear if offering the feedback card without protected time or offering protected time without a guide would have impacted feedback on the wards. However, qualitative data from our study support the use of both components, and implementing the 2 components together is feasible in any inpatient teaching setting.
Despite these limitations, protected time for feedback guided by a pocket feedback card is a simple intervention that appears to improve feedback quantity and quality for ward residents, and guides them to improve their performance. Our low‐intensity intervention helped attendings give residents the tools to improve their clinical and communication skills. An opportunity to make a positive impact on resident education with such a small intervention is rare. The use of a feedback card with protected feedback time could be easily implemented in any training program, and is a valuable tool for busy hospitalists who are more commonly supervising residents on their inpatient rotations.
- .Feedback in clinical medical education.JAMA.1983;250(6):777–781.
- ,.Giving feedback in medical education: verification of recommended techniques.J Gen Intern Med.1998;13(2):111–116.
- ,,,,.Systematic review of the literature on assessment, feedback and physicians' clinical performance: BEME Guide No. 7.Med Teach.2006;28(2):117–128.
- ,,,.Missed opportunities: a descriptive assessment of teaching and attitudes regarding communication skills in a surgical residency.Curr Surg.2006;63(6):401–409.
- ,,.Impact of a 360‐degree professionalism assessment on faculty comfort and skills in feedback delivery.J Gen Intern Med.2008;23(7):969–972.
- ,.Daily encounter cards facilitate competency‐based feedback while leniency bias persists.CJEM.2008;10(1):44–50.
- ,,,,.Teaching compassion and respect. Attending physicians' responses to problematic behaviors.J Gen Intern Med.1999;14(1):49–55.
- .Faculty and the observation of trainees' clinical skills: problems and opportunities.Acad Med.2004;79(1):16–22.
- ,.Direct observation of residents in the emergency department: a structured educational program.Acad Emerg Med.2009;16(4):343–351.
- ,,, et al.Evaluation of a novel assessment form for observing medical residents: a randomised, controlled trial.Med Educ.2008;42(12):1234–1242.
- ,,, et al.Resident evaluations: the use of daily evaluation forms in rheumatology ambulatory care.J Rheumatol.2009;36(6):1298–1303.
- ,,,.Effectiveness of a focused educational intervention on resident evaluations from faculty a randomized controlled trial.J Gen Intern Med.2001;16(7):427–434.
- ,,.Effects of training in direct observation of medical residents' clinical competence: a randomized trial.Ann Intern Med.2004;140(11):874–881.
- Internal Medicine Program Requirements. ACGME. July 1, 2009. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/140_internal_medicine_07012009.pdf. Accessed November 8,2009.
- ,,,,.How to use the core competencies in hospital medicine: a framework for curriculum development.J Hosp Med. 2006;1(suppl 1):57–67.
- ,,,,.Debriefing in the intensive care unit: a feedback tool to facilitate bedside teaching.Crit Care Med.2007;35(3):738–754.
- ,,, et al.Use of an innovative video feedback technique to enhance communication skills training.Med Educ.2004;38(2):145–157.
- .The impact of feedback to medical housestaff on chart documentation and quality of care in the outpatient setting.J Gen Intern Med.1997;12(6):352–356.
- ,,,.Feedback and the mini clinical evaluation exercise.J Gen Intern Med.2004;19(5 pt 2):558–561.
- .Feedback in clinical medical education.JAMA.1983;250(6):777–781.
- ,.Giving feedback in medical education: verification of recommended techniques.J Gen Intern Med.1998;13(2):111–116.
- ,,,,.Systematic review of the literature on assessment, feedback and physicians' clinical performance: BEME Guide No. 7.Med Teach.2006;28(2):117–128.
- ,,,.Missed opportunities: a descriptive assessment of teaching and attitudes regarding communication skills in a surgical residency.Curr Surg.2006;63(6):401–409.
- ,,.Impact of a 360‐degree professionalism assessment on faculty comfort and skills in feedback delivery.J Gen Intern Med.2008;23(7):969–972.
- ,.Daily encounter cards facilitate competency‐based feedback while leniency bias persists.CJEM.2008;10(1):44–50.
- ,,,,.Teaching compassion and respect. Attending physicians' responses to problematic behaviors.J Gen Intern Med.1999;14(1):49–55.
- .Faculty and the observation of trainees' clinical skills: problems and opportunities.Acad Med.2004;79(1):16–22.
- ,.Direct observation of residents in the emergency department: a structured educational program.Acad Emerg Med.2009;16(4):343–351.
- ,,, et al.Evaluation of a novel assessment form for observing medical residents: a randomised, controlled trial.Med Educ.2008;42(12):1234–1242.
- ,,, et al.Resident evaluations: the use of daily evaluation forms in rheumatology ambulatory care.J Rheumatol.2009;36(6):1298–1303.
- ,,,.Effectiveness of a focused educational intervention on resident evaluations from faculty a randomized controlled trial.J Gen Intern Med.2001;16(7):427–434.
- ,,.Effects of training in direct observation of medical residents' clinical competence: a randomized trial.Ann Intern Med.2004;140(11):874–881.
- Internal Medicine Program Requirements. ACGME. July 1, 2009. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/140_internal_medicine_07012009.pdf. Accessed November 8,2009.
- ,,,,.How to use the core competencies in hospital medicine: a framework for curriculum development.J Hosp Med. 2006;1(suppl 1):57–67.
- ,,,,.Debriefing in the intensive care unit: a feedback tool to facilitate bedside teaching.Crit Care Med.2007;35(3):738–754.
- ,,, et al.Use of an innovative video feedback technique to enhance communication skills training.Med Educ.2004;38(2):145–157.
- .The impact of feedback to medical housestaff on chart documentation and quality of care in the outpatient setting.J Gen Intern Med.1997;12(6):352–356.
- ,,,.Feedback and the mini clinical evaluation exercise.J Gen Intern Med.2004;19(5 pt 2):558–561.
Copyright © 2011 Society of Hospital Medicine
Discharge Summary Completion
Discharge summaries (DS) correlate with rates of rehospitalization1, 2 and adverse events after discharge.3 The Joint Commission on the Accreditation of Healthcare Organizations acknowledges their importance and mandates that certain elements be included.4 Thus far, however, DS are not standardized across institutions and there is no expectation that they be available at postdischarge visits. There have been numerous attempts to improve the quality of DS by using more structured formats or computer generated summaries with positive results in term of comprehensiveness, clarity, and practitioner satisfaction58 but with persistence of serious errors and omissions.9
Postgraduate training is often the first opportunity for physicians to learn information transfer management skills. Unfortunately, DS are created by house staff who have minimal training in this area11 and feel like they have to learn by osmosis,12 resulting in poor quality DS and lack of availability at the point of care.1315
Previous research suggested that individualized feedback sessions for Internal Medicine residents improved the quality of certain aspects of their completed DS.10 We postulated that an audit and feedback educational intervention on DS for first year geriatric medicine fellows would also improve their quality. This technique involves chart or case review of clinical practice behaviors for a specific task followed by recommendation of new behaviors when applicable.16 Audit and feedback incorporates adult learning theory,1719 an essential part of continuous quality improvement that fits within the Accreditation Council for Graduate Medical Education (ACGME) competency of practice based learning and improvement,20 as an educational activity.
Methods
Setting
We conducted a preintervention post intervention study at the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai Medical Center (MSMC) in New York City between July 1, 2006 and June 30, 2007. The study received an exemption from the MSMC Institutional Review Board. First year geriatric medicine fellows at MSMC were required to complete 2 months of inpatient service; the first during the first 6 months of the academic year and the second during the last 6 months of the year. Fellows dictated all DS, which were transcribed and routed for signature to the attending of record. Prior to our study, a discharge summary template consisting of 21 items was developed for clinical use. Template items, agreed upon by an expert internal panel of geriatricians and interprofessional faculty, were selected for their importance in assuring a safe transition of older adults from the inpatient to the outpatient setting.
Participants
All 5 first‐year fellows at the Brookdale Department of Geriatrics and Palliative Medicine at MSMC were invited to participate in the study.
Intervention
Audit #1
All available DS for each fellow's first month of inpatient service were audited for completeness of the 21 item discharge summary template by 1 author (AD). The 21 items were focused on 4 distinct periods of the hospitalization: admission, hospital course, discharge planning, and postdischarge care (Figure 1).
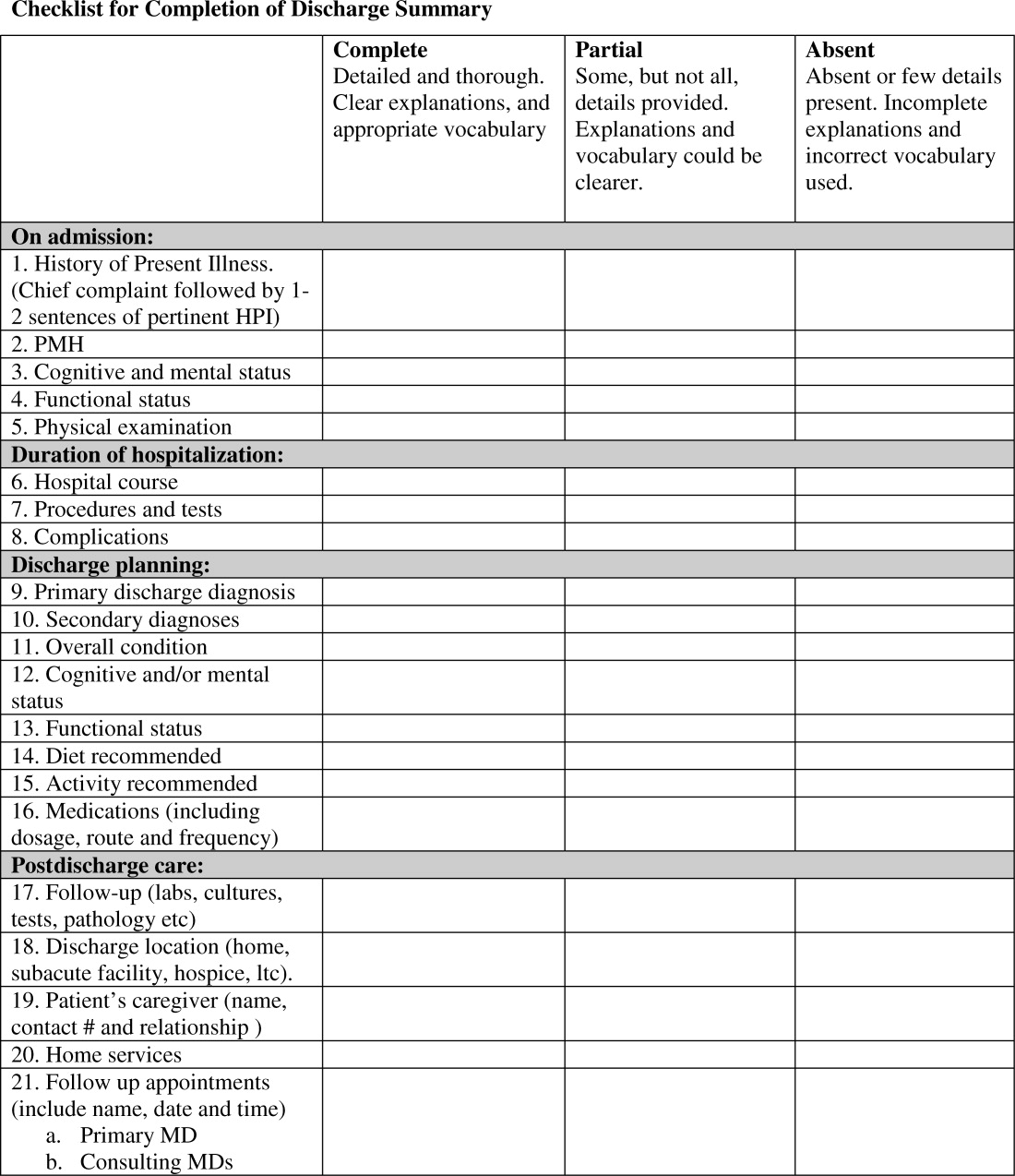
Content under each of the 21 items was classified as complete, partially complete, or absent. An item was considered complete if most information was present and appropriate medical terms were used, partially complete if information was unclear, and absent if no information was present for that area of the DS. To ensure investigator reliability, a random sample of 25% of each fellow's DS was scored by 2 additional investigators (RK and HF) and all disagreements were reviewed and resolved by consensus.
Feedback
Between December 2006 and January 2007, one‐on‐one formative feedback sessions were scheduled. The sessions were approximately 30 minutes long, confidential, performed by 1 of the authors (AD) and followed a written format. During these sessions, each fellow received the results of their discharge summary audit, each partially complete or absent item was discussed, and the importance of DS was emphasized.
Audit #2
All available DS for each fellow's second month of inpatient service were audited for completeness, using the same 21 item assessment tool and the same scoring system.
Statistical Analysis
To determine the impact of our audit and feedback intervention, we compared scores before and after formative feedback sessions, both overall and for the composite discharge summary scores for each of the 4 domains of care: admission, hospital course, discharge‐planning, and postdischarge care. Scores were dichotomized as being complete or partially complete or absent. We used generalized estimating equations to account for the clustering of DS within fellows. Analyses were performed using SAS 9.1 (SAS Institute, Inc., Cary, NC). All statistical tests were 2‐tailed and used a type I error rate of 0.01 to account for multiple comparisons.
Results
Five fellows participated, 4 of whom were women; 2 were in postgraduate year 4, 3 in year 5. A total of 158 DS were audited, 89 prefeedback and 79 postfeedback. Each fellow dictated an average of 17 DS during each inpatient month.
During Audit #1, the 21 item DS were complete among 71%, incomplete among 18%, absent among 11%. Admission items, hospital course items, and discharge planning items were complete among 70%, 78%, and 77% of DS respectively, but postdischarge items were complete among only 57%. Examining individual items, the lowest completion rates were found for test result follow‐up (42%), caregiver information (10%), and home services (64%), as well for assessment at admission and discharge of cognitive and mental status (56% and 53% respectively) and functional status (57% and 40%). Of note, all these items are of particular importance to geriatric care.
After receiving the audit and feedback intervention, fellows were more likely to complete all required discharge summary data when compared to prior‐to‐feedback (91% vs. 71%, P < 0.001). Discharge summary completeness improved for all composite outcomes examining the four domains of care: admission (93% vs. 70%, P < 0.001), hospital course (93% vs. 78%, P < 0.001), discharge planning (93% vs. 77%, P < 0.02), and postdischarge care (83% vs. 57%., P < 0.001) (Table 1).
| Criteria | Preintervention | Postintervention | P Value* | ||
|---|---|---|---|---|---|
| Complete | Absent | Complete | Absent | ||
| |||||
| Admission composite (5 items) | 70 (3585) | 30 (1565) | 93 (79100) | 7 (021) | <0.001 |
| HPI | 79 (38100) | 21 (1563) | 100 | 0 | <0.001 |
| PMH | 94 (75100) | 5 (025) | 99 (93100) | 1 (07) | <0.001 |
| Cognitive/mental status | 56 (1979) | 44 (2182) | 99 (93100) | 1 (07) | <0.001 |
| Functional status | 57 (2588) | 43 (1375) | 97 (89100) | 2 (010) | 0.001 |
| Physical exam | 63 (19100) | 37 (082) | 72 (0100) | 28 (5100) | 0.27 |
| Hospital course composite (3 items) | 78 (2593) | 22 (775) | 93 (76100) | 7 (023) | <0.001 |
| Hospital course | 84 (25100) | 15 (076) | 99 (93100) | 1 (07) | <0.001 |
| Procedures and tests | 70 (690) | 30 (1094) | 90 (57100) | 10 (043) | <0.001 |
| Complications | 80 (4490) | 20 (556) | 90 (77100) | 10 (023) | 0.07 |
| Discharge planning composite (8 items) | 77 (4989) | 22 (1151) | 93 (64100) | 7 (036) | 0.02 |
| Primary diagnosis | 93 (75100) | 6 (026) | 100 | 0 | 0.03 |
| Secondary diagnosis | 82 (56100) | 18 (044) | 100 | 0 | 0.002 |
| Overall condition | 81 (38100) | 19 (062) | 86 (21100) | 14 (079) | 0.47 |
| Cognitive/mental status | 53 (1380) | 57 (2088) | 97 (93100) | 3 (07) | <0.001 |
| Functional status | 40 (1381) | 50 (1988) | 99 (93100) | 1 (07) | <0.001 |
| Diet | 89 (63100) | 12 (538) | 81 (0100) | 19 (0100) | 0.25 |
| Activity | 89 (69100) | 11 (032) | 82 (0100) | 18 (0100) | 0.49 |
| Medications | 83 (50100) | 17 (050) | 100 | 0 | 0.002 |
| Postdischarge care composite (5 items) | 57 (4183) | 43 (1759) | 83 (6998) | 18 (231) | <0.001 |
| F/U results | 42 (1190) | 58 (1089) | 81 (50100) | 20 (050) | 0.02 |
| Discharge location | 92 (88100) | 8 (012) | 100 | 0 | 0.02 |
| Caregiver info | 10 (025) | 89 (75100) | 48 (795) | 52 (584) | <0.001 |
| Home services | 64 (32100) | 35 (068) | 87 (7195) | 12 (029) | <0.001 |
| F/U appointments | 78 (33100) | 23 (067) | 96 (86100) | 4 (014) | <0.001 |
| Overall composite (21 items) | 71 (4287) | 29 (1358) | 91 (7399) | 9 (227) | <0.001 |
Discussion
Our study found that audit and feedback sessions significantly improved the completeness of DS dictated by geriatric medicine fellows at 1 academic medical center. Before feedback, completeness was high in most traditional areas of the DS including admission data, hospital course, and discharge planning, but was low in other areas critical for safe transitions of older adults such as postdischarge care, test follow‐up, caregiver information, and cognitive and functional status changes. These findings were surprising, as using a template should render a completion rate close to 100%. Notably, during feedback sessions, fellows suggested low completion rates were due to lack of awareness regarding the importance of completing all 21 items of the template and missing documentation in patient medical records.
Feedback sessions dramatically improved overall completeness of subsequent DS and in most of areas of specific importance for geriatric care, although we remain uncertain why all areas did not show improvement (for example, caregiver information completion remained low). One possible explanation is the lack of accurate documentation for all necessary items in the hospital medical record. Moreover, we did not observe completion improvement for other items, ie, diet and activity. Overall, we believe that drawing attention to areas of particular importance to geriatric care transitions and providing learners with individual reports on their performance increased their awareness and motivated changes to their practice, improving discharge summary completion.
Our study has limitations. This study was a pilot intervention without a control group, because of time and budgetary constraints. Also, we were unable to assess for sustainability because the fellows studied for this project graduated after the second audit. Third, we studied discharge summary completion; further research should focus on accuracy of discharge summary content. Finally, while we did not use any advanced technologies or materials, faculty time required to conduct the audit and feedback in this study was estimated at 45 hours. In our opinion this estimate would classify our audit and feedback intervention as a low external cost and moderately‐high human cost intervention, which may represent a potential barrier to generalizability. On the other hand, we believe that even an audit of a small sample of DS done by a physician could provide valuable data for feedback and would involve less faculty time.
Our finding that audit and feedback sessions improved the completeness of DS among house‐staff is important for 2 reasons. First, we were able to demonstrate that focused feedback targeted to areas of particular importance to the transition of older adults changed subsequent behavior and resulted in improved documentation of these areas. Second, our study provides evidence of a programmatic approach to address the ACGME competency of practice‐based learning and improvement. We believe that our intervention can be reproduced by training programs across the country and are hopeful that such interventions will result in improved patient outcomes during critical care transitions such as hospital discharge.
- ,Quality assessment of a discharge summary system.CMAJ.1995;152:1437–1442.
- ,,Accuracy of information on medicines in hospital discharge summaries.Intern Med J.2006;36:221–225.
- ,,,,The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138:161–167.
- Available at: http://www.jointcommission.org./. The Joint Commission Requirements/Hospitals/Record of Care/Patient safety. Accessed July2010.
- ,,,,General practitioners' attitudes to computer‐generated surgical discharge letters.Med J Aust.1992;157(6):380–382.
- ,,,Do primary care physicians prefer dictated or computer‐generated discharge summaries?Am J Dis Child.1993;147(9):986–988.
- ,,,,,Evaluation of a computer‐generated discharge summary for patients with acute coronary syndromes.Br J Gen Pract.1998;48(429):1163–1164.
- ,,, et al.Creating a better discharge summary: improvement in quality and timeliness using an electronic dischanrge summary,J Hosp Med.2009;4(4):219–225.
- ,Communication with general practitioners after accident and emergency attendance: computer generated letters are often deficient.Emerg Med J.2003;20(3):256–257.
- ,,Evaluation of electronic discharge summaries: a comparison of documentation in electronic and handwritten discharge summaries.Int J Med Inform.2008;77:613–620.
- ,,,,,Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program.Acad Med.2006;81:S5–S8.
- ,,Experience of medical senior house officers in preparing discharge summaries.BMJ.1996;312:350.
- ,,,,,Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297:831–841.
- ,,,Primary care physician attitudes regarding communication with hospitalists.Dis Mon.2002;48:218–229.
- ,,Improving the continuity of care following discharge of patients hospitalized with heart failure: is the discharge summary adequate?Can J Cardiol.2003;19:365–370.
- Effects of continuing medical education on improving physician clinical care and patient health: a review of systematic reviews.Int J Technol Assess Health Care.2005;21:380–385.
- ,,, et al.Impact of feedback and didactic sessions on the reporting behavior of upper endoscopic findings by physicians and nurses.Clin Gastroenterol Hepatol.2007;5:326–330.
- ,,Prospective assessment of the impact of feedback on colonoscopy performance.Aliment Pharmacol Ther.2006;24:313–318.
- ,,, et al.Inpatient care to community care: improving clinical handover in the private mental health setting.Med J Aust.2009;190(11 Suppl):S144–S149.
- Available at: http://www.Acgme.org, Record of care, Treatment, and Serives, Standard RC.02.04.01. Accessed July2010.
Discharge summaries (DS) correlate with rates of rehospitalization1, 2 and adverse events after discharge.3 The Joint Commission on the Accreditation of Healthcare Organizations acknowledges their importance and mandates that certain elements be included.4 Thus far, however, DS are not standardized across institutions and there is no expectation that they be available at postdischarge visits. There have been numerous attempts to improve the quality of DS by using more structured formats or computer generated summaries with positive results in term of comprehensiveness, clarity, and practitioner satisfaction58 but with persistence of serious errors and omissions.9
Postgraduate training is often the first opportunity for physicians to learn information transfer management skills. Unfortunately, DS are created by house staff who have minimal training in this area11 and feel like they have to learn by osmosis,12 resulting in poor quality DS and lack of availability at the point of care.1315
Previous research suggested that individualized feedback sessions for Internal Medicine residents improved the quality of certain aspects of their completed DS.10 We postulated that an audit and feedback educational intervention on DS for first year geriatric medicine fellows would also improve their quality. This technique involves chart or case review of clinical practice behaviors for a specific task followed by recommendation of new behaviors when applicable.16 Audit and feedback incorporates adult learning theory,1719 an essential part of continuous quality improvement that fits within the Accreditation Council for Graduate Medical Education (ACGME) competency of practice based learning and improvement,20 as an educational activity.
Methods
Setting
We conducted a preintervention post intervention study at the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai Medical Center (MSMC) in New York City between July 1, 2006 and June 30, 2007. The study received an exemption from the MSMC Institutional Review Board. First year geriatric medicine fellows at MSMC were required to complete 2 months of inpatient service; the first during the first 6 months of the academic year and the second during the last 6 months of the year. Fellows dictated all DS, which were transcribed and routed for signature to the attending of record. Prior to our study, a discharge summary template consisting of 21 items was developed for clinical use. Template items, agreed upon by an expert internal panel of geriatricians and interprofessional faculty, were selected for their importance in assuring a safe transition of older adults from the inpatient to the outpatient setting.
Participants
All 5 first‐year fellows at the Brookdale Department of Geriatrics and Palliative Medicine at MSMC were invited to participate in the study.
Intervention
Audit #1
All available DS for each fellow's first month of inpatient service were audited for completeness of the 21 item discharge summary template by 1 author (AD). The 21 items were focused on 4 distinct periods of the hospitalization: admission, hospital course, discharge planning, and postdischarge care (Figure 1).
Content under each of the 21 items was classified as complete, partially complete, or absent. An item was considered complete if most information was present and appropriate medical terms were used, partially complete if information was unclear, and absent if no information was present for that area of the DS. To ensure investigator reliability, a random sample of 25% of each fellow's DS was scored by 2 additional investigators (RK and HF) and all disagreements were reviewed and resolved by consensus.
Feedback
Between December 2006 and January 2007, one‐on‐one formative feedback sessions were scheduled. The sessions were approximately 30 minutes long, confidential, performed by 1 of the authors (AD) and followed a written format. During these sessions, each fellow received the results of their discharge summary audit, each partially complete or absent item was discussed, and the importance of DS was emphasized.
Audit #2
All available DS for each fellow's second month of inpatient service were audited for completeness, using the same 21 item assessment tool and the same scoring system.
Statistical Analysis
To determine the impact of our audit and feedback intervention, we compared scores before and after formative feedback sessions, both overall and for the composite discharge summary scores for each of the 4 domains of care: admission, hospital course, discharge‐planning, and postdischarge care. Scores were dichotomized as being complete or partially complete or absent. We used generalized estimating equations to account for the clustering of DS within fellows. Analyses were performed using SAS 9.1 (SAS Institute, Inc., Cary, NC). All statistical tests were 2‐tailed and used a type I error rate of 0.01 to account for multiple comparisons.
Results
Five fellows participated, 4 of whom were women; 2 were in postgraduate year 4, 3 in year 5. A total of 158 DS were audited, 89 prefeedback and 79 postfeedback. Each fellow dictated an average of 17 DS during each inpatient month.
During Audit #1, the 21 item DS were complete among 71%, incomplete among 18%, absent among 11%. Admission items, hospital course items, and discharge planning items were complete among 70%, 78%, and 77% of DS respectively, but postdischarge items were complete among only 57%. Examining individual items, the lowest completion rates were found for test result follow‐up (42%), caregiver information (10%), and home services (64%), as well for assessment at admission and discharge of cognitive and mental status (56% and 53% respectively) and functional status (57% and 40%). Of note, all these items are of particular importance to geriatric care.
After receiving the audit and feedback intervention, fellows were more likely to complete all required discharge summary data when compared to prior‐to‐feedback (91% vs. 71%, P < 0.001). Discharge summary completeness improved for all composite outcomes examining the four domains of care: admission (93% vs. 70%, P < 0.001), hospital course (93% vs. 78%, P < 0.001), discharge planning (93% vs. 77%, P < 0.02), and postdischarge care (83% vs. 57%., P < 0.001) (Table 1).
| Criteria | Preintervention | Postintervention | P Value* | ||
|---|---|---|---|---|---|
| Complete | Absent | Complete | Absent | ||
| |||||
| Admission composite (5 items) | 70 (3585) | 30 (1565) | 93 (79100) | 7 (021) | <0.001 |
| HPI | 79 (38100) | 21 (1563) | 100 | 0 | <0.001 |
| PMH | 94 (75100) | 5 (025) | 99 (93100) | 1 (07) | <0.001 |
| Cognitive/mental status | 56 (1979) | 44 (2182) | 99 (93100) | 1 (07) | <0.001 |
| Functional status | 57 (2588) | 43 (1375) | 97 (89100) | 2 (010) | 0.001 |
| Physical exam | 63 (19100) | 37 (082) | 72 (0100) | 28 (5100) | 0.27 |
| Hospital course composite (3 items) | 78 (2593) | 22 (775) | 93 (76100) | 7 (023) | <0.001 |
| Hospital course | 84 (25100) | 15 (076) | 99 (93100) | 1 (07) | <0.001 |
| Procedures and tests | 70 (690) | 30 (1094) | 90 (57100) | 10 (043) | <0.001 |
| Complications | 80 (4490) | 20 (556) | 90 (77100) | 10 (023) | 0.07 |
| Discharge planning composite (8 items) | 77 (4989) | 22 (1151) | 93 (64100) | 7 (036) | 0.02 |
| Primary diagnosis | 93 (75100) | 6 (026) | 100 | 0 | 0.03 |
| Secondary diagnosis | 82 (56100) | 18 (044) | 100 | 0 | 0.002 |
| Overall condition | 81 (38100) | 19 (062) | 86 (21100) | 14 (079) | 0.47 |
| Cognitive/mental status | 53 (1380) | 57 (2088) | 97 (93100) | 3 (07) | <0.001 |
| Functional status | 40 (1381) | 50 (1988) | 99 (93100) | 1 (07) | <0.001 |
| Diet | 89 (63100) | 12 (538) | 81 (0100) | 19 (0100) | 0.25 |
| Activity | 89 (69100) | 11 (032) | 82 (0100) | 18 (0100) | 0.49 |
| Medications | 83 (50100) | 17 (050) | 100 | 0 | 0.002 |
| Postdischarge care composite (5 items) | 57 (4183) | 43 (1759) | 83 (6998) | 18 (231) | <0.001 |
| F/U results | 42 (1190) | 58 (1089) | 81 (50100) | 20 (050) | 0.02 |
| Discharge location | 92 (88100) | 8 (012) | 100 | 0 | 0.02 |
| Caregiver info | 10 (025) | 89 (75100) | 48 (795) | 52 (584) | <0.001 |
| Home services | 64 (32100) | 35 (068) | 87 (7195) | 12 (029) | <0.001 |
| F/U appointments | 78 (33100) | 23 (067) | 96 (86100) | 4 (014) | <0.001 |
| Overall composite (21 items) | 71 (4287) | 29 (1358) | 91 (7399) | 9 (227) | <0.001 |
Discussion
Our study found that audit and feedback sessions significantly improved the completeness of DS dictated by geriatric medicine fellows at 1 academic medical center. Before feedback, completeness was high in most traditional areas of the DS including admission data, hospital course, and discharge planning, but was low in other areas critical for safe transitions of older adults such as postdischarge care, test follow‐up, caregiver information, and cognitive and functional status changes. These findings were surprising, as using a template should render a completion rate close to 100%. Notably, during feedback sessions, fellows suggested low completion rates were due to lack of awareness regarding the importance of completing all 21 items of the template and missing documentation in patient medical records.
Feedback sessions dramatically improved overall completeness of subsequent DS and in most of areas of specific importance for geriatric care, although we remain uncertain why all areas did not show improvement (for example, caregiver information completion remained low). One possible explanation is the lack of accurate documentation for all necessary items in the hospital medical record. Moreover, we did not observe completion improvement for other items, ie, diet and activity. Overall, we believe that drawing attention to areas of particular importance to geriatric care transitions and providing learners with individual reports on their performance increased their awareness and motivated changes to their practice, improving discharge summary completion.
Our study has limitations. This study was a pilot intervention without a control group, because of time and budgetary constraints. Also, we were unable to assess for sustainability because the fellows studied for this project graduated after the second audit. Third, we studied discharge summary completion; further research should focus on accuracy of discharge summary content. Finally, while we did not use any advanced technologies or materials, faculty time required to conduct the audit and feedback in this study was estimated at 45 hours. In our opinion this estimate would classify our audit and feedback intervention as a low external cost and moderately‐high human cost intervention, which may represent a potential barrier to generalizability. On the other hand, we believe that even an audit of a small sample of DS done by a physician could provide valuable data for feedback and would involve less faculty time.
Our finding that audit and feedback sessions improved the completeness of DS among house‐staff is important for 2 reasons. First, we were able to demonstrate that focused feedback targeted to areas of particular importance to the transition of older adults changed subsequent behavior and resulted in improved documentation of these areas. Second, our study provides evidence of a programmatic approach to address the ACGME competency of practice‐based learning and improvement. We believe that our intervention can be reproduced by training programs across the country and are hopeful that such interventions will result in improved patient outcomes during critical care transitions such as hospital discharge.
Discharge summaries (DS) correlate with rates of rehospitalization1, 2 and adverse events after discharge.3 The Joint Commission on the Accreditation of Healthcare Organizations acknowledges their importance and mandates that certain elements be included.4 Thus far, however, DS are not standardized across institutions and there is no expectation that they be available at postdischarge visits. There have been numerous attempts to improve the quality of DS by using more structured formats or computer generated summaries with positive results in term of comprehensiveness, clarity, and practitioner satisfaction58 but with persistence of serious errors and omissions.9
Postgraduate training is often the first opportunity for physicians to learn information transfer management skills. Unfortunately, DS are created by house staff who have minimal training in this area11 and feel like they have to learn by osmosis,12 resulting in poor quality DS and lack of availability at the point of care.1315
Previous research suggested that individualized feedback sessions for Internal Medicine residents improved the quality of certain aspects of their completed DS.10 We postulated that an audit and feedback educational intervention on DS for first year geriatric medicine fellows would also improve their quality. This technique involves chart or case review of clinical practice behaviors for a specific task followed by recommendation of new behaviors when applicable.16 Audit and feedback incorporates adult learning theory,1719 an essential part of continuous quality improvement that fits within the Accreditation Council for Graduate Medical Education (ACGME) competency of practice based learning and improvement,20 as an educational activity.
Methods
Setting
We conducted a preintervention post intervention study at the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai Medical Center (MSMC) in New York City between July 1, 2006 and June 30, 2007. The study received an exemption from the MSMC Institutional Review Board. First year geriatric medicine fellows at MSMC were required to complete 2 months of inpatient service; the first during the first 6 months of the academic year and the second during the last 6 months of the year. Fellows dictated all DS, which were transcribed and routed for signature to the attending of record. Prior to our study, a discharge summary template consisting of 21 items was developed for clinical use. Template items, agreed upon by an expert internal panel of geriatricians and interprofessional faculty, were selected for their importance in assuring a safe transition of older adults from the inpatient to the outpatient setting.
Participants
All 5 first‐year fellows at the Brookdale Department of Geriatrics and Palliative Medicine at MSMC were invited to participate in the study.
Intervention
Audit #1
All available DS for each fellow's first month of inpatient service were audited for completeness of the 21 item discharge summary template by 1 author (AD). The 21 items were focused on 4 distinct periods of the hospitalization: admission, hospital course, discharge planning, and postdischarge care (Figure 1).
Content under each of the 21 items was classified as complete, partially complete, or absent. An item was considered complete if most information was present and appropriate medical terms were used, partially complete if information was unclear, and absent if no information was present for that area of the DS. To ensure investigator reliability, a random sample of 25% of each fellow's DS was scored by 2 additional investigators (RK and HF) and all disagreements were reviewed and resolved by consensus.
Feedback
Between December 2006 and January 2007, one‐on‐one formative feedback sessions were scheduled. The sessions were approximately 30 minutes long, confidential, performed by 1 of the authors (AD) and followed a written format. During these sessions, each fellow received the results of their discharge summary audit, each partially complete or absent item was discussed, and the importance of DS was emphasized.
Audit #2
All available DS for each fellow's second month of inpatient service were audited for completeness, using the same 21 item assessment tool and the same scoring system.
Statistical Analysis
To determine the impact of our audit and feedback intervention, we compared scores before and after formative feedback sessions, both overall and for the composite discharge summary scores for each of the 4 domains of care: admission, hospital course, discharge‐planning, and postdischarge care. Scores were dichotomized as being complete or partially complete or absent. We used generalized estimating equations to account for the clustering of DS within fellows. Analyses were performed using SAS 9.1 (SAS Institute, Inc., Cary, NC). All statistical tests were 2‐tailed and used a type I error rate of 0.01 to account for multiple comparisons.
Results
Five fellows participated, 4 of whom were women; 2 were in postgraduate year 4, 3 in year 5. A total of 158 DS were audited, 89 prefeedback and 79 postfeedback. Each fellow dictated an average of 17 DS during each inpatient month.
During Audit #1, the 21 item DS were complete among 71%, incomplete among 18%, absent among 11%. Admission items, hospital course items, and discharge planning items were complete among 70%, 78%, and 77% of DS respectively, but postdischarge items were complete among only 57%. Examining individual items, the lowest completion rates were found for test result follow‐up (42%), caregiver information (10%), and home services (64%), as well for assessment at admission and discharge of cognitive and mental status (56% and 53% respectively) and functional status (57% and 40%). Of note, all these items are of particular importance to geriatric care.
After receiving the audit and feedback intervention, fellows were more likely to complete all required discharge summary data when compared to prior‐to‐feedback (91% vs. 71%, P < 0.001). Discharge summary completeness improved for all composite outcomes examining the four domains of care: admission (93% vs. 70%, P < 0.001), hospital course (93% vs. 78%, P < 0.001), discharge planning (93% vs. 77%, P < 0.02), and postdischarge care (83% vs. 57%., P < 0.001) (Table 1).
| Criteria | Preintervention | Postintervention | P Value* | ||
|---|---|---|---|---|---|
| Complete | Absent | Complete | Absent | ||
| |||||
| Admission composite (5 items) | 70 (3585) | 30 (1565) | 93 (79100) | 7 (021) | <0.001 |
| HPI | 79 (38100) | 21 (1563) | 100 | 0 | <0.001 |
| PMH | 94 (75100) | 5 (025) | 99 (93100) | 1 (07) | <0.001 |
| Cognitive/mental status | 56 (1979) | 44 (2182) | 99 (93100) | 1 (07) | <0.001 |
| Functional status | 57 (2588) | 43 (1375) | 97 (89100) | 2 (010) | 0.001 |
| Physical exam | 63 (19100) | 37 (082) | 72 (0100) | 28 (5100) | 0.27 |
| Hospital course composite (3 items) | 78 (2593) | 22 (775) | 93 (76100) | 7 (023) | <0.001 |
| Hospital course | 84 (25100) | 15 (076) | 99 (93100) | 1 (07) | <0.001 |
| Procedures and tests | 70 (690) | 30 (1094) | 90 (57100) | 10 (043) | <0.001 |
| Complications | 80 (4490) | 20 (556) | 90 (77100) | 10 (023) | 0.07 |
| Discharge planning composite (8 items) | 77 (4989) | 22 (1151) | 93 (64100) | 7 (036) | 0.02 |
| Primary diagnosis | 93 (75100) | 6 (026) | 100 | 0 | 0.03 |
| Secondary diagnosis | 82 (56100) | 18 (044) | 100 | 0 | 0.002 |
| Overall condition | 81 (38100) | 19 (062) | 86 (21100) | 14 (079) | 0.47 |
| Cognitive/mental status | 53 (1380) | 57 (2088) | 97 (93100) | 3 (07) | <0.001 |
| Functional status | 40 (1381) | 50 (1988) | 99 (93100) | 1 (07) | <0.001 |
| Diet | 89 (63100) | 12 (538) | 81 (0100) | 19 (0100) | 0.25 |
| Activity | 89 (69100) | 11 (032) | 82 (0100) | 18 (0100) | 0.49 |
| Medications | 83 (50100) | 17 (050) | 100 | 0 | 0.002 |
| Postdischarge care composite (5 items) | 57 (4183) | 43 (1759) | 83 (6998) | 18 (231) | <0.001 |
| F/U results | 42 (1190) | 58 (1089) | 81 (50100) | 20 (050) | 0.02 |
| Discharge location | 92 (88100) | 8 (012) | 100 | 0 | 0.02 |
| Caregiver info | 10 (025) | 89 (75100) | 48 (795) | 52 (584) | <0.001 |
| Home services | 64 (32100) | 35 (068) | 87 (7195) | 12 (029) | <0.001 |
| F/U appointments | 78 (33100) | 23 (067) | 96 (86100) | 4 (014) | <0.001 |
| Overall composite (21 items) | 71 (4287) | 29 (1358) | 91 (7399) | 9 (227) | <0.001 |
Discussion
Our study found that audit and feedback sessions significantly improved the completeness of DS dictated by geriatric medicine fellows at 1 academic medical center. Before feedback, completeness was high in most traditional areas of the DS including admission data, hospital course, and discharge planning, but was low in other areas critical for safe transitions of older adults such as postdischarge care, test follow‐up, caregiver information, and cognitive and functional status changes. These findings were surprising, as using a template should render a completion rate close to 100%. Notably, during feedback sessions, fellows suggested low completion rates were due to lack of awareness regarding the importance of completing all 21 items of the template and missing documentation in patient medical records.
Feedback sessions dramatically improved overall completeness of subsequent DS and in most of areas of specific importance for geriatric care, although we remain uncertain why all areas did not show improvement (for example, caregiver information completion remained low). One possible explanation is the lack of accurate documentation for all necessary items in the hospital medical record. Moreover, we did not observe completion improvement for other items, ie, diet and activity. Overall, we believe that drawing attention to areas of particular importance to geriatric care transitions and providing learners with individual reports on their performance increased their awareness and motivated changes to their practice, improving discharge summary completion.
Our study has limitations. This study was a pilot intervention without a control group, because of time and budgetary constraints. Also, we were unable to assess for sustainability because the fellows studied for this project graduated after the second audit. Third, we studied discharge summary completion; further research should focus on accuracy of discharge summary content. Finally, while we did not use any advanced technologies or materials, faculty time required to conduct the audit and feedback in this study was estimated at 45 hours. In our opinion this estimate would classify our audit and feedback intervention as a low external cost and moderately‐high human cost intervention, which may represent a potential barrier to generalizability. On the other hand, we believe that even an audit of a small sample of DS done by a physician could provide valuable data for feedback and would involve less faculty time.
Our finding that audit and feedback sessions improved the completeness of DS among house‐staff is important for 2 reasons. First, we were able to demonstrate that focused feedback targeted to areas of particular importance to the transition of older adults changed subsequent behavior and resulted in improved documentation of these areas. Second, our study provides evidence of a programmatic approach to address the ACGME competency of practice‐based learning and improvement. We believe that our intervention can be reproduced by training programs across the country and are hopeful that such interventions will result in improved patient outcomes during critical care transitions such as hospital discharge.
- ,Quality assessment of a discharge summary system.CMAJ.1995;152:1437–1442.
- ,,Accuracy of information on medicines in hospital discharge summaries.Intern Med J.2006;36:221–225.
- ,,,,The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138:161–167.
- Available at: http://www.jointcommission.org./. The Joint Commission Requirements/Hospitals/Record of Care/Patient safety. Accessed July2010.
- ,,,,General practitioners' attitudes to computer‐generated surgical discharge letters.Med J Aust.1992;157(6):380–382.
- ,,,Do primary care physicians prefer dictated or computer‐generated discharge summaries?Am J Dis Child.1993;147(9):986–988.
- ,,,,,Evaluation of a computer‐generated discharge summary for patients with acute coronary syndromes.Br J Gen Pract.1998;48(429):1163–1164.
- ,,, et al.Creating a better discharge summary: improvement in quality and timeliness using an electronic dischanrge summary,J Hosp Med.2009;4(4):219–225.
- ,Communication with general practitioners after accident and emergency attendance: computer generated letters are often deficient.Emerg Med J.2003;20(3):256–257.
- ,,Evaluation of electronic discharge summaries: a comparison of documentation in electronic and handwritten discharge summaries.Int J Med Inform.2008;77:613–620.
- ,,,,,Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program.Acad Med.2006;81:S5–S8.
- ,,Experience of medical senior house officers in preparing discharge summaries.BMJ.1996;312:350.
- ,,,,,Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297:831–841.
- ,,,Primary care physician attitudes regarding communication with hospitalists.Dis Mon.2002;48:218–229.
- ,,Improving the continuity of care following discharge of patients hospitalized with heart failure: is the discharge summary adequate?Can J Cardiol.2003;19:365–370.
- Effects of continuing medical education on improving physician clinical care and patient health: a review of systematic reviews.Int J Technol Assess Health Care.2005;21:380–385.
- ,,, et al.Impact of feedback and didactic sessions on the reporting behavior of upper endoscopic findings by physicians and nurses.Clin Gastroenterol Hepatol.2007;5:326–330.
- ,,Prospective assessment of the impact of feedback on colonoscopy performance.Aliment Pharmacol Ther.2006;24:313–318.
- ,,, et al.Inpatient care to community care: improving clinical handover in the private mental health setting.Med J Aust.2009;190(11 Suppl):S144–S149.
- Available at: http://www.Acgme.org, Record of care, Treatment, and Serives, Standard RC.02.04.01. Accessed July2010.
- ,Quality assessment of a discharge summary system.CMAJ.1995;152:1437–1442.
- ,,Accuracy of information on medicines in hospital discharge summaries.Intern Med J.2006;36:221–225.
- ,,,,The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138:161–167.
- Available at: http://www.jointcommission.org./. The Joint Commission Requirements/Hospitals/Record of Care/Patient safety. Accessed July2010.
- ,,,,General practitioners' attitudes to computer‐generated surgical discharge letters.Med J Aust.1992;157(6):380–382.
- ,,,Do primary care physicians prefer dictated or computer‐generated discharge summaries?Am J Dis Child.1993;147(9):986–988.
- ,,,,,Evaluation of a computer‐generated discharge summary for patients with acute coronary syndromes.Br J Gen Pract.1998;48(429):1163–1164.
- ,,, et al.Creating a better discharge summary: improvement in quality and timeliness using an electronic dischanrge summary,J Hosp Med.2009;4(4):219–225.
- ,Communication with general practitioners after accident and emergency attendance: computer generated letters are often deficient.Emerg Med J.2003;20(3):256–257.
- ,,Evaluation of electronic discharge summaries: a comparison of documentation in electronic and handwritten discharge summaries.Int J Med Inform.2008;77:613–620.
- ,,,,,Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program.Acad Med.2006;81:S5–S8.
- ,,Experience of medical senior house officers in preparing discharge summaries.BMJ.1996;312:350.
- ,,,,,Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297:831–841.
- ,,,Primary care physician attitudes regarding communication with hospitalists.Dis Mon.2002;48:218–229.
- ,,Improving the continuity of care following discharge of patients hospitalized with heart failure: is the discharge summary adequate?Can J Cardiol.2003;19:365–370.
- Effects of continuing medical education on improving physician clinical care and patient health: a review of systematic reviews.Int J Technol Assess Health Care.2005;21:380–385.
- ,,, et al.Impact of feedback and didactic sessions on the reporting behavior of upper endoscopic findings by physicians and nurses.Clin Gastroenterol Hepatol.2007;5:326–330.
- ,,Prospective assessment of the impact of feedback on colonoscopy performance.Aliment Pharmacol Ther.2006;24:313–318.
- ,,, et al.Inpatient care to community care: improving clinical handover in the private mental health setting.Med J Aust.2009;190(11 Suppl):S144–S149.
- Available at: http://www.Acgme.org, Record of care, Treatment, and Serives, Standard RC.02.04.01. Accessed July2010.
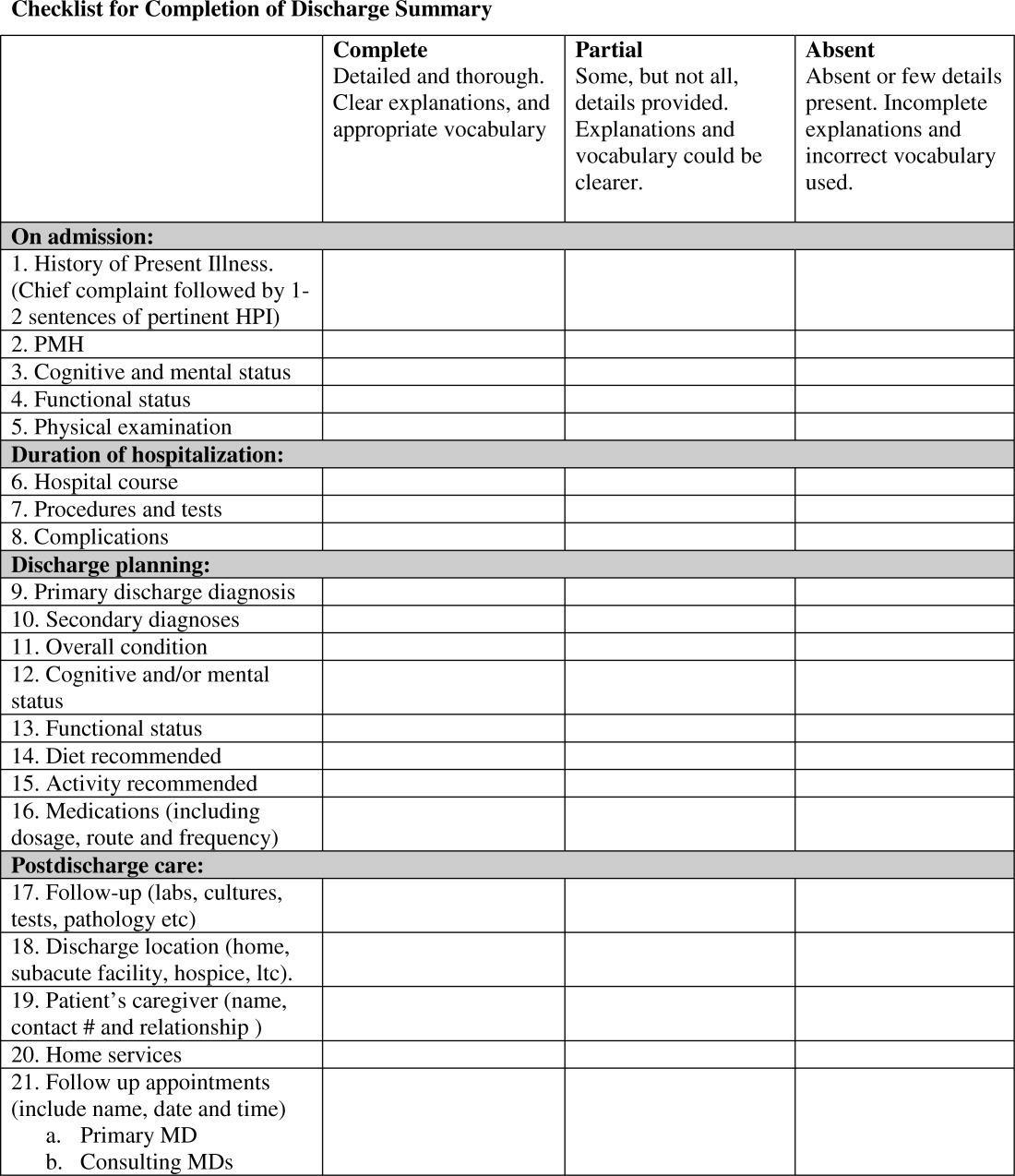
Injury Predictors After Inpatient Falls
An estimated 2% to 15% of all hospitalized patients experience at least one fall.1 Approximately 30% of such falls result in injury and up to 6% may be serious in nature.1, 2 These injuries can result in pain, functional impairment, disability, or even death, and can contribute to longer lengths of stay, increased health care costs, and nursing home placement.25 As a result, inpatient falls have become a major priority for hospital quality assurance programs, and hospital risk management departments have begun to target inpatient falls as a source of legal liability.13, 6, 7 Recently, the Centers for Medicare and Medicaid Services announced that it will no longer pay for preventable complications of hospitalizations, including falls and fall‐related injury.8
Much of the literature on falls comes from community and long‐term care settings, and only a few studies have investigated falls during acute care hospitalization.3, 9, 10 From these studies, risk factors for inpatient falls have been identified and various models have been developed to predict an individual patient's risk of falling. However, unlike in the community setting, interventions to prevent falls in the acute care setting have not proven to be beneficial.11, 12 Commonly used approaches including restraints, alarms, bracelets, or having a volunteer sit with high‐risk patients have not been found to be effective.13, 14 Only 1 study found a multicomponent care plan that targeted specific risk factors in older inpatients to be associated with a reduced relative risk of recorded falls.15 Given this dearth of consistent evidence for the prevention of falls in hospitalized inpatients, the American Geriatrics Society has identified this as a gap area for future research.16
There are also limited data regarding predictors of injury after inpatient falls. A few small studies have identified potential risk factors for sustaining an injury after a fall in acute care, such as age >75 years, altered mental status, increased comorbidities, visual impairment, falls in the bathroom, and admission to a geriatric psychiatry floor.2, 5, 17 However, to our knowledge, there are no studies that have identified potential characteristics of inpatients found immediately after a fall that predict an injury. Providers who assess inpatients who have fallen need guidance on how to identify those in need of further evaluation and testing. This study sought to quantify the types and severity of injuries resulting from inpatient falls and to identify predictors of injury after a fall among a cohort of patients who fell at an urban academic medical center.
Patients and Methods
Patient Population
The study population included all inpatients on 13 medical and surgical units who experienced a fall between January 1, 2006 and December 31, 2006, while hospitalized at an 1171‐bed urban academic medical center. Telemetry, intensive care, pediatric, psychiatric, rehabilitation, and obstetrics or gynecology units were excluded from this analysis; the patients on these units are special populations that are qualitatively different than other acute care patients and have a different set of risk factor for falls and predictors of fall‐related injury. The study was approved by the institutional review board of the Mount Sinai School of Medicine.
Data Collection
Inpatient falls were identified retrospectively by review of hospital incident reports, which are most often completed by the unit nurses. In our institution, all falls generate an incident report. Using a standardized abstraction form, patient characteristics, circumstances surrounding falls, and fall‐related injuries were collected from the reports.
Laboratory data for anemia (hemoglobin < 12.0 g/dL), low albumin (<3.5 g/dL), elevated creatinine (>1.5 mg/dL), prolonged partial thromboplastin time (>35 seconds), and elevated international normalized ratio (INR > 1.3), were extracted from the patient's computerized medical record, if available. Number of days from admission to the fall, length of stay to the nearest hundredth of a day, and discharge disposition were also recorded for each patient.
Results of all radiographic studies, including x‐ray, ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI), performed within 2 weeks after the fall were obtained. The indication for the imaging study was assessed from the order given to the radiology department and from the patient's medical record. A positive finding on an imaging study was defined as evidence of intracranial hemorrhage, fracture, joint effusion, soft‐tissue swelling, or any other injury potentially caused by trauma. Fall‐related injury was defined as positive findings on any of these imaging studies that were performed as a result of the fall. Evaluation of fall‐related injuries was conducted by a reviewer blinded to the baseline patient characteristics and laboratory data.
Statistical Analyses
Baseline characteristics and risk factors of patients with and without fall‐related injuries were compared using the chi square test or Student t test as appropriate. Univariate and multivariate logistic regression were used to calculate adjusted odds ratios (ORs) for injury after an inpatient fall. The multivariate model was developed using a manual forward method. Prior research shows that patients with recurrent falls do so in the same manner and for the same reasons.2, 3, 17 Thus, analyses were performed including only the first fall episode as the outcome of interest. Analyses were performed with SPSS statistical software (SPSS Inc., Chicago, IL) using 2‐sided P values.
Results
During the study period, 513 inpatients sustained 636 falls at the Mount Sinai Medical Center. There were 54,257 admissions to the hospital with 322,670 total patient days during this time. Therefore the fall incidence rate was 1.97 falls per 1,000 patient days. Characteristics of inpatients who fell are shown in Table 1. Most patients had 1 fall episode; however, 95 patients (19%) fell multiple times (range, 2‐6 events). There were no significant differences between recurrent fallers and those who fell once with respect to baseline characteristics, injuries sustained, or discharge disposition.
| Characteristic | Number of Patients (n = 513) [number (%)] |
|---|---|
| |
| Age (years) | 70 (21‐104) |
| Age >75 years | 202 (39) |
| Male gender | 255 (50) |
| Assessed at risk of falling | |
| Yes | 378 (74) |
| No | 2 (5) |
| Unknown | 110 (21) |
| Number of falls | |
| 1 | 418 (82) |
| 2 | 78 (15) |
| 3 | 10 (2) |
| 4 | 4 (1) |
| 5 | 2 (0.4) |
| 6 | 1 (0.2) |
| Multiple falls | 95 (19) |
Fall Circumstances
The majority of patients who fell (74%) had been assessed by the nursing staff as being at risk for falling prior to the event. Overall, most falls (73%) occurred on medical rather than surgical units. The units with the most falls were geriatrics, neurology, and general medicine. Details about circumstances surrounding the falls are shown in Table 2. In most instances (71%) patients were found on the floor after the fall while less than 8% of falls were witnessed. Approximately 12% of patients received sedatives within 4 hours of falling (40% opioids, 30% benzodiazepines, 16% zolpidem, and 14% other). Laboratory values at the time of fall revealed that 70% of patients who fell were anemic, 62% had low albumin, and 19% had an elevated creatinine. Almost 20% of the patients had a prolonged partial thromboplastin time (PTT) and 18% had an elevated INR.
| Characteristic | Number of Falls (n = 513) [number (%)]* |
|---|---|
| |
| Location | |
| Medical unit | 374 (73) |
| Surgical unit | 139 (27) |
| Time | |
| Day shift (7:00 AM to 6:59 PM) | 225 (44) |
| Night shift (7:00 PM to 6:59 AM) | 282 (56) |
| Character of fall | |
| Assisted to floor | 15 (3) |
| Fall alleged | 92 (18) |
| Fall witnessed | 39 (8) |
| Found on Floor | 363 (71) |
| Unknown | 4 (<1) |
| Fall‐related activity | |
| Ambulation | 164 (32) |
| Bathroom | 122 (24) |
| Bed | 21 (4) |
| Chair | 19 (4) |
| Other/unknown | 187 (36) |
| Mental status | |
| Oriented | 274 (53) |
| Confused | 151 (29) |
| Unknown | 88 (17) |
| Activity level ordered | |
| Ambulatory | 246 (48) |
| Nonambulatory | 135 (26) |
| Unknown | 132 (26) |
| Siderails | |
| Complete | 15 (3) |
| Partial | 352 (69) |
| None | 15 (3) |
| Unknown | 126 (25) |
| Environmental obstacle | |
| None | 355 (69) |
| Wet | 20 (4) |
| Debris | 2 (<1) |
| Unknown | 136 (27) |
| Restraints | |
| Yes | 3 (<1) |
| No | 374 (73) |
| Unknown | 136 (27) |
| Sedative use | |
| Total | 64 (12) |
| Opioids | 28 (6) |
| Benzos | 21 (4) |
| Antipsychotics | 7 (1) |
| Other | 8 (2) |
| Evidence of trauma | |
| Yes | 25 (5) |
| No | 285 (56) |
| Unknown | 203 (40) |
The median number of days from patient admission until they fell was 4 days (range, 0‐134), with 70% of patients falling within the first week of admission. In general, there was no difference in fall rate by time of day, though slightly more falls (56%) occurred during the night shift (7 PM to 7 AM).
Fall‐related Outcomes
Twenty‐five patients (5%) had evidence of trauma on physical exam after the fall, including lacerations, swelling, and ecchymoses, as documented by the evaluating nurse. A total of 120 imaging procedures were ordered following the first fall; when all inpatient falls were included, 145 imaging procedures were ordered. Most imaging studies (87%) did not show significant findings. Among studies with positive findings, the most common abnormality was fracture, including 3 hip, 1 humeral, 1 vertebral, 1 nasal, and 1 rib fracture. Other injuries found on imaging studies included 1 subdural hematoma, 1 acute cerebral infarct, 2 soft‐tissue hematomas, and 2 knee effusions. The acute cerebral infarct was not considered to be a result of the fall. Additionally, 3 patients had soft‐tissue swelling noted on head CT and 1 had Foley catheter‐related trauma.
The average length of stay for the 513 inpatients who fell was 20 days (range, 7‐444) compared to 6 days for all patients admitted to the hospital during the same period. Among inpatients who fell, there was no statistical difference in length of stay between those who did and those who did not have a fall‐related injury found on imaging. More than one‐half (53%) of the patients who fell were discharged to home, 21% to rehabilitation facilities, 12% to nursing homes, and 9% died during the hospitalization.
Results of Univariate Analysis
Univariate predictors of injury after a fall are shown in Table 3. Patients having evidence of trauma indicated by the evaluating nurse after a fall had an increased risk for having an abnormal imaging study (OR = 14.7, P < 0.001). Having an activity level of ambulatory ordered by the provider (OR = 2.5, P = 0.09), falling during the night shift (OR = 2.5, P = 0.11), having ambulation as the fall‐related activity (OR = 2.2, P = 0.12), and older age (P = 0.19) all showed a trend toward higher rates of injury being found after a fall. There was no significant association between fall‐related injury and being an elderly patient (age > 75 years), sedative use, falling in the bathroom, or having an elevated PTT or INR.
| Variable | Patients without injury (n = 497) [number (%)] | Patients with injury (n = 16) [number (%)] | OR | P Value |
|---|---|---|---|---|
| ||||
| Elderly | 195 (39) | 7 (44) | 1.2 | 0.72 |
| Gender male | 245 (49) | 10 (63) | 1.7 | 0.30 |
| Location surgical unit | 142 (29) | 6 (38) | 1.5 | 0.44 |
| At risk of falling prior to event | 365 (73) | 13 (8) | 1.6 | 0.49 |
| Protocol in place | 338 (68) | 11 (69) | 1.0 | 0.95 |
| Activity level ambulatory | 235 (47) | 11 (69) | 2.5 | 0.09 |
| Occurrence on night shift | 270 (54) | 12 (75) | 2.5 | 0.11 |
| Restraint use | 3 (1) | 0 (0) | ||
| Sedative within 4 hours | 61 (12) | 3 (19) | 1.6 | 0.44 |
| Fall related to ambulation | 156 (31) | 8 (50) | 2.2 | 0.12 |
| Evidence of trauma | 19 (4) | 6 (38) | 14.7 | <0.001 |
| Prolonged PTT | 93 (19) | 5 (31) | 1.9 | 0.29 |
| Elevated INR | 90 (18) | 3 (19) | 1.0 | 0.96 |
| Anemia | 351 (71) | 9 (56) | 0.6 | 0.32 |
| Elevated creatinine | 97 (20) | 2 (13) | 0.7 | 0.60 |
| Low albumin | 309 (62) | 8 (50) | 1.6 | 0.58 |
Multivariate Predictors of Injury
In multivariate analysis, after adjusting for age and sex, evidence of trauma after a fall (OR = 24.6, P < 0.001) and having an activity level of ambulatory ordered by the provider (OR = 7.3, P = 0.01) were independent predictors of injury being found on imaging studies (Table 4). Analyses limited to the 120 patients who had imaging found that the association between evidence of trauma (OR = 6.22, P = 0.02) and having an activity level of ambulatory ordered (OR = 5.53, P = 0.04) remained statistically significant.
| Variable | All Patients (n = 513) | Patients with Imaging (n = 120)* | ||
|---|---|---|---|---|
| OR | P Value | OR | P Value | |
| ||||
| Age | 1.03 | 0.17 | 1.016 | 0.52 |
| Gender | 3.19 | 0.11 | 2.843 | 0.17 |
| Evidence of trauma | 24.63 | <0.001 | 6.22 | 0.02 |
| Activity level ambulatory | 7.33 | 0.01 | 5.53 | 0.04 |
Discussion
Inpatient falls are common and result in significant patient morbidity and increased healthcare costs. Falls in the acute care setting have also proven to be difficult to prevent and as a result have become a priority for patient safety and hospital quality.
Our study confirms that a high percentage of patients with an initial fall will have recurrent falls.1 Additionally, the majority of patients in this cohort fell despite having been assessed as at risk for falling prior to the event. The types of injuries sustained after inpatient falls (eg, subdural hematoma, multiple fractures, joint effusions, other hematomas, and soft‐tissue swelling) are similar to those found by other authors.2, 3, 17, 18
In this study, inpatient falls were associated with an almost 2‐week increase in length of stay. Though we cannot say that this was directly due to falls, and an increased length of stay may just be a marker of severity of illness, this association warrants further study, perhaps with a matched control group of patients who did not fall, and has implications for healthcare cost containment.
We found that having evidence of trauma after a fall and having an activity level of ambulatory ordered by the provider were independent predictors of injury being found after an inpatient fall. It seems intuitive that patients who have physical evidence of trauma, such as lacerations or bruising, would be more likely to have an underlying injury. Clinically, this confirms that providers should have a high index of suspicion for injury being found on imaging studies in such patients. Similar findings have been noted in the emergency medicine literature that further support the validity of our findings.19
Less clear are the reasons for the observed association between having an activity level of ambulatory ordered and higher risk of injury after an inpatient fall. Prior studies have found that ambulatory inpatients are less likely to use assistive devices that they use at home while hospitalized and are less likely to call for help; these factors may contribute to falls.2, 3 However, the interpretation of this finding is limited by the fact that 26% of the patients who fell had an unknown activity level ordered.
Altered mental status, comorbidity, age > 75 years, visual impairment, falling in the bathroom, and being on a geriatric psychiatry floor have previously been found to be risk factors for sustaining an injury after an inpatient fall.2, 5, 17 Conversely, this study did not find altered mental status to be a significant predictor of injury. One reason may be that this was subjectively determined by the evaluating nurse and not by a standardized measure of cognitive impairment. Patients who are oriented may also be more likely to report unwitnessed falls and injuries than patients with altered mental status.3
There was also no association between age and fall‐related injury in our cohort. On univariate analysis, patients who were older in age were more likely to have an injury found after an inpatient fall but this was not statistically significant. Previous authors have suggested that today's inpatients are increasingly ill and may have risk factors for falls and injuries that are independent of age, such as multiple comorbid conditions or deconditioning.3
We hypothesized that patients who are anticoagulated and had an elevated INR or PTT would be more likely to sustain an injury. Anemic inpatients have also been found to be at increased risk of falls.20 We found no significant association between fall‐related injury being found on imaging studies and anemia, low albumin, elevated creatinine, prolonged PTT, or elevated INR. Not every patient who fell had these laboratory values available. However, even when only inpatients who fell and had laboratory tests were included in the analysis, there was still no association with fall‐related injury.
This study has several limitations. First, a low number of serious injuries was found on imaging studies after inpatient falls in this cohort; this limited the power of the study to identify predictors of fall‐related injury.
Second, fall‐related injury was defined as a positive finding on imaging studies within 2 weeks of an inpatient fall. Thus, some fall‐related injuries may have been missed in patients who did not have imaging. However, any patient who had a serious injury after a fall and remained hospitalized would likely have had symptoms such as pain or altered mental status that would have led to an imaging study. Moreover, the analysis was repeated including only inpatients who fell and had imaging, and the association between having evidence of trauma and having an activity level of ambulatory ordered and sustaining a fall‐related injury remained significant.
Third, we relied on hospital incident reports to identify inpatient falls. These reports yield a limited amount of information and may be inaccurate or incomplete. A recent study also raised concern that incident reports significantly underreport actual fall incidence.21 However, previous studies have found no indication that falls are underreported and suggest that incident reports are an established custom in hospital culture.1, 22 Medical staff are aware that administrators want to keep track of hospital fall rates for both quality improvement and documentation for risk management.1, 22 It is unlikely that severe falls or falls leading to serious injury are not reported. A different source of underreporting may actually be failure of patients to tell the medical team about an unwitnessed fall. Older patients may be concerned they will be placed in nursing homes and those with memory loss may forget to report a minor fall. Education of patients and family members could improve reporting of inpatient falls and further our understanding of contributing factors.
Finally, although the evaluation of fall‐related injuries was conducted by a blinded reviewer, the potential for bias does exist among even the best‐intentioned reviewers. Additionally, there may be some degree of variability within the reviewer's data abstraction.
This study adds valuable information about the epidemiology of inpatient falls at large, urban, tertiary‐care academic medical centers, including characteristics of patients who fell, circumstances surrounding falls, injuries sustained, and predictors of fall‐related injury found on imaging. Although additional research is essential to identify methods to effectively prevent inpatient falls, this study contributes to the limited data in this area, can guide providers who are evaluating inpatients who have fallen, and may be used to design future investigations. It is imperative that measures are identified to avoid the frequent adverse outcomes that result from inpatient falls. Insurance companies, hospital administrators, patients, and providers will be demanding that a safe environment be a key component of quality of care measures.
This study draws attention to the scope of the problem at our institution that is common to hospitals across the country. In our study, our academic medical center had a fall rate consistent with published reports, but new efforts have been focused on quality improvement in this area. An interdisciplinary fall prevention committee has been formed that includes physicians, nurses, patient care assistants, physical therapists, pharmacists, and representatives from information technology (IT). Currently, a program of a fall risk‐factor assessment with targeted interventions to reduce those risk factors is being developed for all high‐risk patients and will be piloted on inpatient units.
Acknowledgements
The authors thank Susan Emro, BS, Department of Health Policy, Susan Davis, MS, MPH, RN, CNAA, Department of Nursing, and Albert Siu, MD, MSPH, Brookdale Department of Geriatrics and Adult Development, for their review of this article. Author contributions were as followsconception and design: S.M.B, R.K., and T.M.; collection and assembly of data: S.M.B.; analysis and interpretation of the data: S.M.B, R.K., and J.W.; drafting of the article: S.M.B.; critical revision of the article for important intellectual content: R.K. and J.W.; final approval of the article: S.M.B, R.K., and J.W.; statistical expertise: J.W.; obtaining of funding: S.M.B.
- ,,,.Risk of falls for hospitalized patients: a predictive model based on routinely available data.J Clin Epidemiol.2001;54(12):1258–1266.
- ,,, et al.A case‐control study of patient, medication, and care‐related risk factors for inpatient falls.J Gen Intern Med.2005;20(2):116–122.
- ,,, et al.Characteristics and circumstances of falls in a hospital setting: a prospective analysis.J Gen Intern Med.2004;19(7):732–739.
- ,,,.Falls and consequent injuries in hospitalized patients: effects of an interdisciplinary falls prevention program.BMC Health Serv Res.2006;6:69.
- ,,,.Serious falls in hospitalized patients: correlates and resource utilization.Am J Med.1995;99(2):137–143.
- ,.Using tools to assess and prevent inpatient falls.Jt Comm J Qual Saf.2003;29(7):363–368.
- ,,.Incidence and risk factors for inpatient falls in an academic acute‐care hospital.J Nippon Med Sch.2006;73(5):265–270.
- .Nonpayment for performance? Medicare's new reimbursement rule.N Engl J Med.2007;357(16):1573–1575.
- .Clinical practice. preventing falls in elderly persons.N Engl J Med.2003;348(1):42–49.
- .Building the science of falls‐prevention research.J Am Geriatr Soc.2004;52(3):461–462.
- ,,,,,.Interventions for preventing falls in acute‐ and chronic‐care hospitals: a systematic review and meta‐analysis.J Am Geriatr Soc.2008;56(1):29–36.
- ,,, et al.Interventions for the prevention of falls in older adults: systematic review and meta‐analysis of randomised clinical trials.BMJ.2004;328(7441):680.
- ,,, et al.Acceptability of fall prevention measures for hospital inpatients.Age Ageing.2004;33(4):400–401.
- ,,, et al.Can volunteer companions prevent falls among inpatients? A feasibility study using a pre‐post comparative design.BMC Geriatr.2006;6:11.
- ,,,,.Using targeted risk factor reduction to prevent falls in older in‐patients: a randomised controlled trial.Age Ageing.2004;33(4):390–395.
- .Prevention of falls in hospital inpatients: agendas for research and practice.Age Ageing.2004;33(4):328–330.
- ,,, et al.Patterns and predictors of inpatient falls and fall‐related injuries in a large academic hospital.Infect Control Hosp Epidemiol.2005;26(10):822–827.
- ,,,,.The relationship of falls to injury among hospital in‐patients.Int J Clin Pract.2005;59(1):17–20.
- ,,,,,.Indications for computed tomography in patients with minor head injury.N Engl J Med.2000;343(2):100–105.
- ,,.Anemia increases risk for falls in hospitalized older adults: an evaluation of falls in 362 hospitalized, ambulatory, long‐term care, and community patients.J Am Med Dir Assoc.2006;7(5):287–293.
- ,,,,,.Improving the capture of fall events in hospitals: combining a service for evaluating inpatient falls with an incident report system.J Am Geriatr Soc.2008;56(4):701–704.
- ,,, et al.Attitudes and barriers to incident reporting: a collaborative hospital study.Qual Saf Health Care.2006;15(1):39–43.
An estimated 2% to 15% of all hospitalized patients experience at least one fall.1 Approximately 30% of such falls result in injury and up to 6% may be serious in nature.1, 2 These injuries can result in pain, functional impairment, disability, or even death, and can contribute to longer lengths of stay, increased health care costs, and nursing home placement.25 As a result, inpatient falls have become a major priority for hospital quality assurance programs, and hospital risk management departments have begun to target inpatient falls as a source of legal liability.13, 6, 7 Recently, the Centers for Medicare and Medicaid Services announced that it will no longer pay for preventable complications of hospitalizations, including falls and fall‐related injury.8
Much of the literature on falls comes from community and long‐term care settings, and only a few studies have investigated falls during acute care hospitalization.3, 9, 10 From these studies, risk factors for inpatient falls have been identified and various models have been developed to predict an individual patient's risk of falling. However, unlike in the community setting, interventions to prevent falls in the acute care setting have not proven to be beneficial.11, 12 Commonly used approaches including restraints, alarms, bracelets, or having a volunteer sit with high‐risk patients have not been found to be effective.13, 14 Only 1 study found a multicomponent care plan that targeted specific risk factors in older inpatients to be associated with a reduced relative risk of recorded falls.15 Given this dearth of consistent evidence for the prevention of falls in hospitalized inpatients, the American Geriatrics Society has identified this as a gap area for future research.16
There are also limited data regarding predictors of injury after inpatient falls. A few small studies have identified potential risk factors for sustaining an injury after a fall in acute care, such as age >75 years, altered mental status, increased comorbidities, visual impairment, falls in the bathroom, and admission to a geriatric psychiatry floor.2, 5, 17 However, to our knowledge, there are no studies that have identified potential characteristics of inpatients found immediately after a fall that predict an injury. Providers who assess inpatients who have fallen need guidance on how to identify those in need of further evaluation and testing. This study sought to quantify the types and severity of injuries resulting from inpatient falls and to identify predictors of injury after a fall among a cohort of patients who fell at an urban academic medical center.
Patients and Methods
Patient Population
The study population included all inpatients on 13 medical and surgical units who experienced a fall between January 1, 2006 and December 31, 2006, while hospitalized at an 1171‐bed urban academic medical center. Telemetry, intensive care, pediatric, psychiatric, rehabilitation, and obstetrics or gynecology units were excluded from this analysis; the patients on these units are special populations that are qualitatively different than other acute care patients and have a different set of risk factor for falls and predictors of fall‐related injury. The study was approved by the institutional review board of the Mount Sinai School of Medicine.
Data Collection
Inpatient falls were identified retrospectively by review of hospital incident reports, which are most often completed by the unit nurses. In our institution, all falls generate an incident report. Using a standardized abstraction form, patient characteristics, circumstances surrounding falls, and fall‐related injuries were collected from the reports.
Laboratory data for anemia (hemoglobin < 12.0 g/dL), low albumin (<3.5 g/dL), elevated creatinine (>1.5 mg/dL), prolonged partial thromboplastin time (>35 seconds), and elevated international normalized ratio (INR > 1.3), were extracted from the patient's computerized medical record, if available. Number of days from admission to the fall, length of stay to the nearest hundredth of a day, and discharge disposition were also recorded for each patient.
Results of all radiographic studies, including x‐ray, ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI), performed within 2 weeks after the fall were obtained. The indication for the imaging study was assessed from the order given to the radiology department and from the patient's medical record. A positive finding on an imaging study was defined as evidence of intracranial hemorrhage, fracture, joint effusion, soft‐tissue swelling, or any other injury potentially caused by trauma. Fall‐related injury was defined as positive findings on any of these imaging studies that were performed as a result of the fall. Evaluation of fall‐related injuries was conducted by a reviewer blinded to the baseline patient characteristics and laboratory data.
Statistical Analyses
Baseline characteristics and risk factors of patients with and without fall‐related injuries were compared using the chi square test or Student t test as appropriate. Univariate and multivariate logistic regression were used to calculate adjusted odds ratios (ORs) for injury after an inpatient fall. The multivariate model was developed using a manual forward method. Prior research shows that patients with recurrent falls do so in the same manner and for the same reasons.2, 3, 17 Thus, analyses were performed including only the first fall episode as the outcome of interest. Analyses were performed with SPSS statistical software (SPSS Inc., Chicago, IL) using 2‐sided P values.
Results
During the study period, 513 inpatients sustained 636 falls at the Mount Sinai Medical Center. There were 54,257 admissions to the hospital with 322,670 total patient days during this time. Therefore the fall incidence rate was 1.97 falls per 1,000 patient days. Characteristics of inpatients who fell are shown in Table 1. Most patients had 1 fall episode; however, 95 patients (19%) fell multiple times (range, 2‐6 events). There were no significant differences between recurrent fallers and those who fell once with respect to baseline characteristics, injuries sustained, or discharge disposition.
| Characteristic | Number of Patients (n = 513) [number (%)] |
|---|---|
| |
| Age (years) | 70 (21‐104) |
| Age >75 years | 202 (39) |
| Male gender | 255 (50) |
| Assessed at risk of falling | |
| Yes | 378 (74) |
| No | 2 (5) |
| Unknown | 110 (21) |
| Number of falls | |
| 1 | 418 (82) |
| 2 | 78 (15) |
| 3 | 10 (2) |
| 4 | 4 (1) |
| 5 | 2 (0.4) |
| 6 | 1 (0.2) |
| Multiple falls | 95 (19) |
Fall Circumstances
The majority of patients who fell (74%) had been assessed by the nursing staff as being at risk for falling prior to the event. Overall, most falls (73%) occurred on medical rather than surgical units. The units with the most falls were geriatrics, neurology, and general medicine. Details about circumstances surrounding the falls are shown in Table 2. In most instances (71%) patients were found on the floor after the fall while less than 8% of falls were witnessed. Approximately 12% of patients received sedatives within 4 hours of falling (40% opioids, 30% benzodiazepines, 16% zolpidem, and 14% other). Laboratory values at the time of fall revealed that 70% of patients who fell were anemic, 62% had low albumin, and 19% had an elevated creatinine. Almost 20% of the patients had a prolonged partial thromboplastin time (PTT) and 18% had an elevated INR.
| Characteristic | Number of Falls (n = 513) [number (%)]* |
|---|---|
| |
| Location | |
| Medical unit | 374 (73) |
| Surgical unit | 139 (27) |
| Time | |
| Day shift (7:00 AM to 6:59 PM) | 225 (44) |
| Night shift (7:00 PM to 6:59 AM) | 282 (56) |
| Character of fall | |
| Assisted to floor | 15 (3) |
| Fall alleged | 92 (18) |
| Fall witnessed | 39 (8) |
| Found on Floor | 363 (71) |
| Unknown | 4 (<1) |
| Fall‐related activity | |
| Ambulation | 164 (32) |
| Bathroom | 122 (24) |
| Bed | 21 (4) |
| Chair | 19 (4) |
| Other/unknown | 187 (36) |
| Mental status | |
| Oriented | 274 (53) |
| Confused | 151 (29) |
| Unknown | 88 (17) |
| Activity level ordered | |
| Ambulatory | 246 (48) |
| Nonambulatory | 135 (26) |
| Unknown | 132 (26) |
| Siderails | |
| Complete | 15 (3) |
| Partial | 352 (69) |
| None | 15 (3) |
| Unknown | 126 (25) |
| Environmental obstacle | |
| None | 355 (69) |
| Wet | 20 (4) |
| Debris | 2 (<1) |
| Unknown | 136 (27) |
| Restraints | |
| Yes | 3 (<1) |
| No | 374 (73) |
| Unknown | 136 (27) |
| Sedative use | |
| Total | 64 (12) |
| Opioids | 28 (6) |
| Benzos | 21 (4) |
| Antipsychotics | 7 (1) |
| Other | 8 (2) |
| Evidence of trauma | |
| Yes | 25 (5) |
| No | 285 (56) |
| Unknown | 203 (40) |
The median number of days from patient admission until they fell was 4 days (range, 0‐134), with 70% of patients falling within the first week of admission. In general, there was no difference in fall rate by time of day, though slightly more falls (56%) occurred during the night shift (7 PM to 7 AM).
Fall‐related Outcomes
Twenty‐five patients (5%) had evidence of trauma on physical exam after the fall, including lacerations, swelling, and ecchymoses, as documented by the evaluating nurse. A total of 120 imaging procedures were ordered following the first fall; when all inpatient falls were included, 145 imaging procedures were ordered. Most imaging studies (87%) did not show significant findings. Among studies with positive findings, the most common abnormality was fracture, including 3 hip, 1 humeral, 1 vertebral, 1 nasal, and 1 rib fracture. Other injuries found on imaging studies included 1 subdural hematoma, 1 acute cerebral infarct, 2 soft‐tissue hematomas, and 2 knee effusions. The acute cerebral infarct was not considered to be a result of the fall. Additionally, 3 patients had soft‐tissue swelling noted on head CT and 1 had Foley catheter‐related trauma.
The average length of stay for the 513 inpatients who fell was 20 days (range, 7‐444) compared to 6 days for all patients admitted to the hospital during the same period. Among inpatients who fell, there was no statistical difference in length of stay between those who did and those who did not have a fall‐related injury found on imaging. More than one‐half (53%) of the patients who fell were discharged to home, 21% to rehabilitation facilities, 12% to nursing homes, and 9% died during the hospitalization.
Results of Univariate Analysis
Univariate predictors of injury after a fall are shown in Table 3. Patients having evidence of trauma indicated by the evaluating nurse after a fall had an increased risk for having an abnormal imaging study (OR = 14.7, P < 0.001). Having an activity level of ambulatory ordered by the provider (OR = 2.5, P = 0.09), falling during the night shift (OR = 2.5, P = 0.11), having ambulation as the fall‐related activity (OR = 2.2, P = 0.12), and older age (P = 0.19) all showed a trend toward higher rates of injury being found after a fall. There was no significant association between fall‐related injury and being an elderly patient (age > 75 years), sedative use, falling in the bathroom, or having an elevated PTT or INR.
| Variable | Patients without injury (n = 497) [number (%)] | Patients with injury (n = 16) [number (%)] | OR | P Value |
|---|---|---|---|---|
| ||||
| Elderly | 195 (39) | 7 (44) | 1.2 | 0.72 |
| Gender male | 245 (49) | 10 (63) | 1.7 | 0.30 |
| Location surgical unit | 142 (29) | 6 (38) | 1.5 | 0.44 |
| At risk of falling prior to event | 365 (73) | 13 (8) | 1.6 | 0.49 |
| Protocol in place | 338 (68) | 11 (69) | 1.0 | 0.95 |
| Activity level ambulatory | 235 (47) | 11 (69) | 2.5 | 0.09 |
| Occurrence on night shift | 270 (54) | 12 (75) | 2.5 | 0.11 |
| Restraint use | 3 (1) | 0 (0) | ||
| Sedative within 4 hours | 61 (12) | 3 (19) | 1.6 | 0.44 |
| Fall related to ambulation | 156 (31) | 8 (50) | 2.2 | 0.12 |
| Evidence of trauma | 19 (4) | 6 (38) | 14.7 | <0.001 |
| Prolonged PTT | 93 (19) | 5 (31) | 1.9 | 0.29 |
| Elevated INR | 90 (18) | 3 (19) | 1.0 | 0.96 |
| Anemia | 351 (71) | 9 (56) | 0.6 | 0.32 |
| Elevated creatinine | 97 (20) | 2 (13) | 0.7 | 0.60 |
| Low albumin | 309 (62) | 8 (50) | 1.6 | 0.58 |
Multivariate Predictors of Injury
In multivariate analysis, after adjusting for age and sex, evidence of trauma after a fall (OR = 24.6, P < 0.001) and having an activity level of ambulatory ordered by the provider (OR = 7.3, P = 0.01) were independent predictors of injury being found on imaging studies (Table 4). Analyses limited to the 120 patients who had imaging found that the association between evidence of trauma (OR = 6.22, P = 0.02) and having an activity level of ambulatory ordered (OR = 5.53, P = 0.04) remained statistically significant.
| Variable | All Patients (n = 513) | Patients with Imaging (n = 120)* | ||
|---|---|---|---|---|
| OR | P Value | OR | P Value | |
| ||||
| Age | 1.03 | 0.17 | 1.016 | 0.52 |
| Gender | 3.19 | 0.11 | 2.843 | 0.17 |
| Evidence of trauma | 24.63 | <0.001 | 6.22 | 0.02 |
| Activity level ambulatory | 7.33 | 0.01 | 5.53 | 0.04 |
Discussion
Inpatient falls are common and result in significant patient morbidity and increased healthcare costs. Falls in the acute care setting have also proven to be difficult to prevent and as a result have become a priority for patient safety and hospital quality.
Our study confirms that a high percentage of patients with an initial fall will have recurrent falls.1 Additionally, the majority of patients in this cohort fell despite having been assessed as at risk for falling prior to the event. The types of injuries sustained after inpatient falls (eg, subdural hematoma, multiple fractures, joint effusions, other hematomas, and soft‐tissue swelling) are similar to those found by other authors.2, 3, 17, 18
In this study, inpatient falls were associated with an almost 2‐week increase in length of stay. Though we cannot say that this was directly due to falls, and an increased length of stay may just be a marker of severity of illness, this association warrants further study, perhaps with a matched control group of patients who did not fall, and has implications for healthcare cost containment.
We found that having evidence of trauma after a fall and having an activity level of ambulatory ordered by the provider were independent predictors of injury being found after an inpatient fall. It seems intuitive that patients who have physical evidence of trauma, such as lacerations or bruising, would be more likely to have an underlying injury. Clinically, this confirms that providers should have a high index of suspicion for injury being found on imaging studies in such patients. Similar findings have been noted in the emergency medicine literature that further support the validity of our findings.19
Less clear are the reasons for the observed association between having an activity level of ambulatory ordered and higher risk of injury after an inpatient fall. Prior studies have found that ambulatory inpatients are less likely to use assistive devices that they use at home while hospitalized and are less likely to call for help; these factors may contribute to falls.2, 3 However, the interpretation of this finding is limited by the fact that 26% of the patients who fell had an unknown activity level ordered.
Altered mental status, comorbidity, age > 75 years, visual impairment, falling in the bathroom, and being on a geriatric psychiatry floor have previously been found to be risk factors for sustaining an injury after an inpatient fall.2, 5, 17 Conversely, this study did not find altered mental status to be a significant predictor of injury. One reason may be that this was subjectively determined by the evaluating nurse and not by a standardized measure of cognitive impairment. Patients who are oriented may also be more likely to report unwitnessed falls and injuries than patients with altered mental status.3
There was also no association between age and fall‐related injury in our cohort. On univariate analysis, patients who were older in age were more likely to have an injury found after an inpatient fall but this was not statistically significant. Previous authors have suggested that today's inpatients are increasingly ill and may have risk factors for falls and injuries that are independent of age, such as multiple comorbid conditions or deconditioning.3
We hypothesized that patients who are anticoagulated and had an elevated INR or PTT would be more likely to sustain an injury. Anemic inpatients have also been found to be at increased risk of falls.20 We found no significant association between fall‐related injury being found on imaging studies and anemia, low albumin, elevated creatinine, prolonged PTT, or elevated INR. Not every patient who fell had these laboratory values available. However, even when only inpatients who fell and had laboratory tests were included in the analysis, there was still no association with fall‐related injury.
This study has several limitations. First, a low number of serious injuries was found on imaging studies after inpatient falls in this cohort; this limited the power of the study to identify predictors of fall‐related injury.
Second, fall‐related injury was defined as a positive finding on imaging studies within 2 weeks of an inpatient fall. Thus, some fall‐related injuries may have been missed in patients who did not have imaging. However, any patient who had a serious injury after a fall and remained hospitalized would likely have had symptoms such as pain or altered mental status that would have led to an imaging study. Moreover, the analysis was repeated including only inpatients who fell and had imaging, and the association between having evidence of trauma and having an activity level of ambulatory ordered and sustaining a fall‐related injury remained significant.
Third, we relied on hospital incident reports to identify inpatient falls. These reports yield a limited amount of information and may be inaccurate or incomplete. A recent study also raised concern that incident reports significantly underreport actual fall incidence.21 However, previous studies have found no indication that falls are underreported and suggest that incident reports are an established custom in hospital culture.1, 22 Medical staff are aware that administrators want to keep track of hospital fall rates for both quality improvement and documentation for risk management.1, 22 It is unlikely that severe falls or falls leading to serious injury are not reported. A different source of underreporting may actually be failure of patients to tell the medical team about an unwitnessed fall. Older patients may be concerned they will be placed in nursing homes and those with memory loss may forget to report a minor fall. Education of patients and family members could improve reporting of inpatient falls and further our understanding of contributing factors.
Finally, although the evaluation of fall‐related injuries was conducted by a blinded reviewer, the potential for bias does exist among even the best‐intentioned reviewers. Additionally, there may be some degree of variability within the reviewer's data abstraction.
This study adds valuable information about the epidemiology of inpatient falls at large, urban, tertiary‐care academic medical centers, including characteristics of patients who fell, circumstances surrounding falls, injuries sustained, and predictors of fall‐related injury found on imaging. Although additional research is essential to identify methods to effectively prevent inpatient falls, this study contributes to the limited data in this area, can guide providers who are evaluating inpatients who have fallen, and may be used to design future investigations. It is imperative that measures are identified to avoid the frequent adverse outcomes that result from inpatient falls. Insurance companies, hospital administrators, patients, and providers will be demanding that a safe environment be a key component of quality of care measures.
This study draws attention to the scope of the problem at our institution that is common to hospitals across the country. In our study, our academic medical center had a fall rate consistent with published reports, but new efforts have been focused on quality improvement in this area. An interdisciplinary fall prevention committee has been formed that includes physicians, nurses, patient care assistants, physical therapists, pharmacists, and representatives from information technology (IT). Currently, a program of a fall risk‐factor assessment with targeted interventions to reduce those risk factors is being developed for all high‐risk patients and will be piloted on inpatient units.
Acknowledgements
The authors thank Susan Emro, BS, Department of Health Policy, Susan Davis, MS, MPH, RN, CNAA, Department of Nursing, and Albert Siu, MD, MSPH, Brookdale Department of Geriatrics and Adult Development, for their review of this article. Author contributions were as followsconception and design: S.M.B, R.K., and T.M.; collection and assembly of data: S.M.B.; analysis and interpretation of the data: S.M.B, R.K., and J.W.; drafting of the article: S.M.B.; critical revision of the article for important intellectual content: R.K. and J.W.; final approval of the article: S.M.B, R.K., and J.W.; statistical expertise: J.W.; obtaining of funding: S.M.B.
An estimated 2% to 15% of all hospitalized patients experience at least one fall.1 Approximately 30% of such falls result in injury and up to 6% may be serious in nature.1, 2 These injuries can result in pain, functional impairment, disability, or even death, and can contribute to longer lengths of stay, increased health care costs, and nursing home placement.25 As a result, inpatient falls have become a major priority for hospital quality assurance programs, and hospital risk management departments have begun to target inpatient falls as a source of legal liability.13, 6, 7 Recently, the Centers for Medicare and Medicaid Services announced that it will no longer pay for preventable complications of hospitalizations, including falls and fall‐related injury.8
Much of the literature on falls comes from community and long‐term care settings, and only a few studies have investigated falls during acute care hospitalization.3, 9, 10 From these studies, risk factors for inpatient falls have been identified and various models have been developed to predict an individual patient's risk of falling. However, unlike in the community setting, interventions to prevent falls in the acute care setting have not proven to be beneficial.11, 12 Commonly used approaches including restraints, alarms, bracelets, or having a volunteer sit with high‐risk patients have not been found to be effective.13, 14 Only 1 study found a multicomponent care plan that targeted specific risk factors in older inpatients to be associated with a reduced relative risk of recorded falls.15 Given this dearth of consistent evidence for the prevention of falls in hospitalized inpatients, the American Geriatrics Society has identified this as a gap area for future research.16
There are also limited data regarding predictors of injury after inpatient falls. A few small studies have identified potential risk factors for sustaining an injury after a fall in acute care, such as age >75 years, altered mental status, increased comorbidities, visual impairment, falls in the bathroom, and admission to a geriatric psychiatry floor.2, 5, 17 However, to our knowledge, there are no studies that have identified potential characteristics of inpatients found immediately after a fall that predict an injury. Providers who assess inpatients who have fallen need guidance on how to identify those in need of further evaluation and testing. This study sought to quantify the types and severity of injuries resulting from inpatient falls and to identify predictors of injury after a fall among a cohort of patients who fell at an urban academic medical center.
Patients and Methods
Patient Population
The study population included all inpatients on 13 medical and surgical units who experienced a fall between January 1, 2006 and December 31, 2006, while hospitalized at an 1171‐bed urban academic medical center. Telemetry, intensive care, pediatric, psychiatric, rehabilitation, and obstetrics or gynecology units were excluded from this analysis; the patients on these units are special populations that are qualitatively different than other acute care patients and have a different set of risk factor for falls and predictors of fall‐related injury. The study was approved by the institutional review board of the Mount Sinai School of Medicine.
Data Collection
Inpatient falls were identified retrospectively by review of hospital incident reports, which are most often completed by the unit nurses. In our institution, all falls generate an incident report. Using a standardized abstraction form, patient characteristics, circumstances surrounding falls, and fall‐related injuries were collected from the reports.
Laboratory data for anemia (hemoglobin < 12.0 g/dL), low albumin (<3.5 g/dL), elevated creatinine (>1.5 mg/dL), prolonged partial thromboplastin time (>35 seconds), and elevated international normalized ratio (INR > 1.3), were extracted from the patient's computerized medical record, if available. Number of days from admission to the fall, length of stay to the nearest hundredth of a day, and discharge disposition were also recorded for each patient.
Results of all radiographic studies, including x‐ray, ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI), performed within 2 weeks after the fall were obtained. The indication for the imaging study was assessed from the order given to the radiology department and from the patient's medical record. A positive finding on an imaging study was defined as evidence of intracranial hemorrhage, fracture, joint effusion, soft‐tissue swelling, or any other injury potentially caused by trauma. Fall‐related injury was defined as positive findings on any of these imaging studies that were performed as a result of the fall. Evaluation of fall‐related injuries was conducted by a reviewer blinded to the baseline patient characteristics and laboratory data.
Statistical Analyses
Baseline characteristics and risk factors of patients with and without fall‐related injuries were compared using the chi square test or Student t test as appropriate. Univariate and multivariate logistic regression were used to calculate adjusted odds ratios (ORs) for injury after an inpatient fall. The multivariate model was developed using a manual forward method. Prior research shows that patients with recurrent falls do so in the same manner and for the same reasons.2, 3, 17 Thus, analyses were performed including only the first fall episode as the outcome of interest. Analyses were performed with SPSS statistical software (SPSS Inc., Chicago, IL) using 2‐sided P values.
Results
During the study period, 513 inpatients sustained 636 falls at the Mount Sinai Medical Center. There were 54,257 admissions to the hospital with 322,670 total patient days during this time. Therefore the fall incidence rate was 1.97 falls per 1,000 patient days. Characteristics of inpatients who fell are shown in Table 1. Most patients had 1 fall episode; however, 95 patients (19%) fell multiple times (range, 2‐6 events). There were no significant differences between recurrent fallers and those who fell once with respect to baseline characteristics, injuries sustained, or discharge disposition.
| Characteristic | Number of Patients (n = 513) [number (%)] |
|---|---|
| |
| Age (years) | 70 (21‐104) |
| Age >75 years | 202 (39) |
| Male gender | 255 (50) |
| Assessed at risk of falling | |
| Yes | 378 (74) |
| No | 2 (5) |
| Unknown | 110 (21) |
| Number of falls | |
| 1 | 418 (82) |
| 2 | 78 (15) |
| 3 | 10 (2) |
| 4 | 4 (1) |
| 5 | 2 (0.4) |
| 6 | 1 (0.2) |
| Multiple falls | 95 (19) |
Fall Circumstances
The majority of patients who fell (74%) had been assessed by the nursing staff as being at risk for falling prior to the event. Overall, most falls (73%) occurred on medical rather than surgical units. The units with the most falls were geriatrics, neurology, and general medicine. Details about circumstances surrounding the falls are shown in Table 2. In most instances (71%) patients were found on the floor after the fall while less than 8% of falls were witnessed. Approximately 12% of patients received sedatives within 4 hours of falling (40% opioids, 30% benzodiazepines, 16% zolpidem, and 14% other). Laboratory values at the time of fall revealed that 70% of patients who fell were anemic, 62% had low albumin, and 19% had an elevated creatinine. Almost 20% of the patients had a prolonged partial thromboplastin time (PTT) and 18% had an elevated INR.
| Characteristic | Number of Falls (n = 513) [number (%)]* |
|---|---|
| |
| Location | |
| Medical unit | 374 (73) |
| Surgical unit | 139 (27) |
| Time | |
| Day shift (7:00 AM to 6:59 PM) | 225 (44) |
| Night shift (7:00 PM to 6:59 AM) | 282 (56) |
| Character of fall | |
| Assisted to floor | 15 (3) |
| Fall alleged | 92 (18) |
| Fall witnessed | 39 (8) |
| Found on Floor | 363 (71) |
| Unknown | 4 (<1) |
| Fall‐related activity | |
| Ambulation | 164 (32) |
| Bathroom | 122 (24) |
| Bed | 21 (4) |
| Chair | 19 (4) |
| Other/unknown | 187 (36) |
| Mental status | |
| Oriented | 274 (53) |
| Confused | 151 (29) |
| Unknown | 88 (17) |
| Activity level ordered | |
| Ambulatory | 246 (48) |
| Nonambulatory | 135 (26) |
| Unknown | 132 (26) |
| Siderails | |
| Complete | 15 (3) |
| Partial | 352 (69) |
| None | 15 (3) |
| Unknown | 126 (25) |
| Environmental obstacle | |
| None | 355 (69) |
| Wet | 20 (4) |
| Debris | 2 (<1) |
| Unknown | 136 (27) |
| Restraints | |
| Yes | 3 (<1) |
| No | 374 (73) |
| Unknown | 136 (27) |
| Sedative use | |
| Total | 64 (12) |
| Opioids | 28 (6) |
| Benzos | 21 (4) |
| Antipsychotics | 7 (1) |
| Other | 8 (2) |
| Evidence of trauma | |
| Yes | 25 (5) |
| No | 285 (56) |
| Unknown | 203 (40) |
The median number of days from patient admission until they fell was 4 days (range, 0‐134), with 70% of patients falling within the first week of admission. In general, there was no difference in fall rate by time of day, though slightly more falls (56%) occurred during the night shift (7 PM to 7 AM).
Fall‐related Outcomes
Twenty‐five patients (5%) had evidence of trauma on physical exam after the fall, including lacerations, swelling, and ecchymoses, as documented by the evaluating nurse. A total of 120 imaging procedures were ordered following the first fall; when all inpatient falls were included, 145 imaging procedures were ordered. Most imaging studies (87%) did not show significant findings. Among studies with positive findings, the most common abnormality was fracture, including 3 hip, 1 humeral, 1 vertebral, 1 nasal, and 1 rib fracture. Other injuries found on imaging studies included 1 subdural hematoma, 1 acute cerebral infarct, 2 soft‐tissue hematomas, and 2 knee effusions. The acute cerebral infarct was not considered to be a result of the fall. Additionally, 3 patients had soft‐tissue swelling noted on head CT and 1 had Foley catheter‐related trauma.
The average length of stay for the 513 inpatients who fell was 20 days (range, 7‐444) compared to 6 days for all patients admitted to the hospital during the same period. Among inpatients who fell, there was no statistical difference in length of stay between those who did and those who did not have a fall‐related injury found on imaging. More than one‐half (53%) of the patients who fell were discharged to home, 21% to rehabilitation facilities, 12% to nursing homes, and 9% died during the hospitalization.
Results of Univariate Analysis
Univariate predictors of injury after a fall are shown in Table 3. Patients having evidence of trauma indicated by the evaluating nurse after a fall had an increased risk for having an abnormal imaging study (OR = 14.7, P < 0.001). Having an activity level of ambulatory ordered by the provider (OR = 2.5, P = 0.09), falling during the night shift (OR = 2.5, P = 0.11), having ambulation as the fall‐related activity (OR = 2.2, P = 0.12), and older age (P = 0.19) all showed a trend toward higher rates of injury being found after a fall. There was no significant association between fall‐related injury and being an elderly patient (age > 75 years), sedative use, falling in the bathroom, or having an elevated PTT or INR.
| Variable | Patients without injury (n = 497) [number (%)] | Patients with injury (n = 16) [number (%)] | OR | P Value |
|---|---|---|---|---|
| ||||
| Elderly | 195 (39) | 7 (44) | 1.2 | 0.72 |
| Gender male | 245 (49) | 10 (63) | 1.7 | 0.30 |
| Location surgical unit | 142 (29) | 6 (38) | 1.5 | 0.44 |
| At risk of falling prior to event | 365 (73) | 13 (8) | 1.6 | 0.49 |
| Protocol in place | 338 (68) | 11 (69) | 1.0 | 0.95 |
| Activity level ambulatory | 235 (47) | 11 (69) | 2.5 | 0.09 |
| Occurrence on night shift | 270 (54) | 12 (75) | 2.5 | 0.11 |
| Restraint use | 3 (1) | 0 (0) | ||
| Sedative within 4 hours | 61 (12) | 3 (19) | 1.6 | 0.44 |
| Fall related to ambulation | 156 (31) | 8 (50) | 2.2 | 0.12 |
| Evidence of trauma | 19 (4) | 6 (38) | 14.7 | <0.001 |
| Prolonged PTT | 93 (19) | 5 (31) | 1.9 | 0.29 |
| Elevated INR | 90 (18) | 3 (19) | 1.0 | 0.96 |
| Anemia | 351 (71) | 9 (56) | 0.6 | 0.32 |
| Elevated creatinine | 97 (20) | 2 (13) | 0.7 | 0.60 |
| Low albumin | 309 (62) | 8 (50) | 1.6 | 0.58 |
Multivariate Predictors of Injury
In multivariate analysis, after adjusting for age and sex, evidence of trauma after a fall (OR = 24.6, P < 0.001) and having an activity level of ambulatory ordered by the provider (OR = 7.3, P = 0.01) were independent predictors of injury being found on imaging studies (Table 4). Analyses limited to the 120 patients who had imaging found that the association between evidence of trauma (OR = 6.22, P = 0.02) and having an activity level of ambulatory ordered (OR = 5.53, P = 0.04) remained statistically significant.
| Variable | All Patients (n = 513) | Patients with Imaging (n = 120)* | ||
|---|---|---|---|---|
| OR | P Value | OR | P Value | |
| ||||
| Age | 1.03 | 0.17 | 1.016 | 0.52 |
| Gender | 3.19 | 0.11 | 2.843 | 0.17 |
| Evidence of trauma | 24.63 | <0.001 | 6.22 | 0.02 |
| Activity level ambulatory | 7.33 | 0.01 | 5.53 | 0.04 |
Discussion
Inpatient falls are common and result in significant patient morbidity and increased healthcare costs. Falls in the acute care setting have also proven to be difficult to prevent and as a result have become a priority for patient safety and hospital quality.
Our study confirms that a high percentage of patients with an initial fall will have recurrent falls.1 Additionally, the majority of patients in this cohort fell despite having been assessed as at risk for falling prior to the event. The types of injuries sustained after inpatient falls (eg, subdural hematoma, multiple fractures, joint effusions, other hematomas, and soft‐tissue swelling) are similar to those found by other authors.2, 3, 17, 18
In this study, inpatient falls were associated with an almost 2‐week increase in length of stay. Though we cannot say that this was directly due to falls, and an increased length of stay may just be a marker of severity of illness, this association warrants further study, perhaps with a matched control group of patients who did not fall, and has implications for healthcare cost containment.
We found that having evidence of trauma after a fall and having an activity level of ambulatory ordered by the provider were independent predictors of injury being found after an inpatient fall. It seems intuitive that patients who have physical evidence of trauma, such as lacerations or bruising, would be more likely to have an underlying injury. Clinically, this confirms that providers should have a high index of suspicion for injury being found on imaging studies in such patients. Similar findings have been noted in the emergency medicine literature that further support the validity of our findings.19
Less clear are the reasons for the observed association between having an activity level of ambulatory ordered and higher risk of injury after an inpatient fall. Prior studies have found that ambulatory inpatients are less likely to use assistive devices that they use at home while hospitalized and are less likely to call for help; these factors may contribute to falls.2, 3 However, the interpretation of this finding is limited by the fact that 26% of the patients who fell had an unknown activity level ordered.
Altered mental status, comorbidity, age > 75 years, visual impairment, falling in the bathroom, and being on a geriatric psychiatry floor have previously been found to be risk factors for sustaining an injury after an inpatient fall.2, 5, 17 Conversely, this study did not find altered mental status to be a significant predictor of injury. One reason may be that this was subjectively determined by the evaluating nurse and not by a standardized measure of cognitive impairment. Patients who are oriented may also be more likely to report unwitnessed falls and injuries than patients with altered mental status.3
There was also no association between age and fall‐related injury in our cohort. On univariate analysis, patients who were older in age were more likely to have an injury found after an inpatient fall but this was not statistically significant. Previous authors have suggested that today's inpatients are increasingly ill and may have risk factors for falls and injuries that are independent of age, such as multiple comorbid conditions or deconditioning.3
We hypothesized that patients who are anticoagulated and had an elevated INR or PTT would be more likely to sustain an injury. Anemic inpatients have also been found to be at increased risk of falls.20 We found no significant association between fall‐related injury being found on imaging studies and anemia, low albumin, elevated creatinine, prolonged PTT, or elevated INR. Not every patient who fell had these laboratory values available. However, even when only inpatients who fell and had laboratory tests were included in the analysis, there was still no association with fall‐related injury.
This study has several limitations. First, a low number of serious injuries was found on imaging studies after inpatient falls in this cohort; this limited the power of the study to identify predictors of fall‐related injury.
Second, fall‐related injury was defined as a positive finding on imaging studies within 2 weeks of an inpatient fall. Thus, some fall‐related injuries may have been missed in patients who did not have imaging. However, any patient who had a serious injury after a fall and remained hospitalized would likely have had symptoms such as pain or altered mental status that would have led to an imaging study. Moreover, the analysis was repeated including only inpatients who fell and had imaging, and the association between having evidence of trauma and having an activity level of ambulatory ordered and sustaining a fall‐related injury remained significant.
Third, we relied on hospital incident reports to identify inpatient falls. These reports yield a limited amount of information and may be inaccurate or incomplete. A recent study also raised concern that incident reports significantly underreport actual fall incidence.21 However, previous studies have found no indication that falls are underreported and suggest that incident reports are an established custom in hospital culture.1, 22 Medical staff are aware that administrators want to keep track of hospital fall rates for both quality improvement and documentation for risk management.1, 22 It is unlikely that severe falls or falls leading to serious injury are not reported. A different source of underreporting may actually be failure of patients to tell the medical team about an unwitnessed fall. Older patients may be concerned they will be placed in nursing homes and those with memory loss may forget to report a minor fall. Education of patients and family members could improve reporting of inpatient falls and further our understanding of contributing factors.
Finally, although the evaluation of fall‐related injuries was conducted by a blinded reviewer, the potential for bias does exist among even the best‐intentioned reviewers. Additionally, there may be some degree of variability within the reviewer's data abstraction.
This study adds valuable information about the epidemiology of inpatient falls at large, urban, tertiary‐care academic medical centers, including characteristics of patients who fell, circumstances surrounding falls, injuries sustained, and predictors of fall‐related injury found on imaging. Although additional research is essential to identify methods to effectively prevent inpatient falls, this study contributes to the limited data in this area, can guide providers who are evaluating inpatients who have fallen, and may be used to design future investigations. It is imperative that measures are identified to avoid the frequent adverse outcomes that result from inpatient falls. Insurance companies, hospital administrators, patients, and providers will be demanding that a safe environment be a key component of quality of care measures.
This study draws attention to the scope of the problem at our institution that is common to hospitals across the country. In our study, our academic medical center had a fall rate consistent with published reports, but new efforts have been focused on quality improvement in this area. An interdisciplinary fall prevention committee has been formed that includes physicians, nurses, patient care assistants, physical therapists, pharmacists, and representatives from information technology (IT). Currently, a program of a fall risk‐factor assessment with targeted interventions to reduce those risk factors is being developed for all high‐risk patients and will be piloted on inpatient units.
Acknowledgements
The authors thank Susan Emro, BS, Department of Health Policy, Susan Davis, MS, MPH, RN, CNAA, Department of Nursing, and Albert Siu, MD, MSPH, Brookdale Department of Geriatrics and Adult Development, for their review of this article. Author contributions were as followsconception and design: S.M.B, R.K., and T.M.; collection and assembly of data: S.M.B.; analysis and interpretation of the data: S.M.B, R.K., and J.W.; drafting of the article: S.M.B.; critical revision of the article for important intellectual content: R.K. and J.W.; final approval of the article: S.M.B, R.K., and J.W.; statistical expertise: J.W.; obtaining of funding: S.M.B.
- ,,,.Risk of falls for hospitalized patients: a predictive model based on routinely available data.J Clin Epidemiol.2001;54(12):1258–1266.
- ,,, et al.A case‐control study of patient, medication, and care‐related risk factors for inpatient falls.J Gen Intern Med.2005;20(2):116–122.
- ,,, et al.Characteristics and circumstances of falls in a hospital setting: a prospective analysis.J Gen Intern Med.2004;19(7):732–739.
- ,,,.Falls and consequent injuries in hospitalized patients: effects of an interdisciplinary falls prevention program.BMC Health Serv Res.2006;6:69.
- ,,,.Serious falls in hospitalized patients: correlates and resource utilization.Am J Med.1995;99(2):137–143.
- ,.Using tools to assess and prevent inpatient falls.Jt Comm J Qual Saf.2003;29(7):363–368.
- ,,.Incidence and risk factors for inpatient falls in an academic acute‐care hospital.J Nippon Med Sch.2006;73(5):265–270.
- .Nonpayment for performance? Medicare's new reimbursement rule.N Engl J Med.2007;357(16):1573–1575.
- .Clinical practice. preventing falls in elderly persons.N Engl J Med.2003;348(1):42–49.
- .Building the science of falls‐prevention research.J Am Geriatr Soc.2004;52(3):461–462.
- ,,,,,.Interventions for preventing falls in acute‐ and chronic‐care hospitals: a systematic review and meta‐analysis.J Am Geriatr Soc.2008;56(1):29–36.
- ,,, et al.Interventions for the prevention of falls in older adults: systematic review and meta‐analysis of randomised clinical trials.BMJ.2004;328(7441):680.
- ,,, et al.Acceptability of fall prevention measures for hospital inpatients.Age Ageing.2004;33(4):400–401.
- ,,, et al.Can volunteer companions prevent falls among inpatients? A feasibility study using a pre‐post comparative design.BMC Geriatr.2006;6:11.
- ,,,,.Using targeted risk factor reduction to prevent falls in older in‐patients: a randomised controlled trial.Age Ageing.2004;33(4):390–395.
- .Prevention of falls in hospital inpatients: agendas for research and practice.Age Ageing.2004;33(4):328–330.
- ,,, et al.Patterns and predictors of inpatient falls and fall‐related injuries in a large academic hospital.Infect Control Hosp Epidemiol.2005;26(10):822–827.
- ,,,,.The relationship of falls to injury among hospital in‐patients.Int J Clin Pract.2005;59(1):17–20.
- ,,,,,.Indications for computed tomography in patients with minor head injury.N Engl J Med.2000;343(2):100–105.
- ,,.Anemia increases risk for falls in hospitalized older adults: an evaluation of falls in 362 hospitalized, ambulatory, long‐term care, and community patients.J Am Med Dir Assoc.2006;7(5):287–293.
- ,,,,,.Improving the capture of fall events in hospitals: combining a service for evaluating inpatient falls with an incident report system.J Am Geriatr Soc.2008;56(4):701–704.
- ,,, et al.Attitudes and barriers to incident reporting: a collaborative hospital study.Qual Saf Health Care.2006;15(1):39–43.
- ,,,.Risk of falls for hospitalized patients: a predictive model based on routinely available data.J Clin Epidemiol.2001;54(12):1258–1266.
- ,,, et al.A case‐control study of patient, medication, and care‐related risk factors for inpatient falls.J Gen Intern Med.2005;20(2):116–122.
- ,,, et al.Characteristics and circumstances of falls in a hospital setting: a prospective analysis.J Gen Intern Med.2004;19(7):732–739.
- ,,,.Falls and consequent injuries in hospitalized patients: effects of an interdisciplinary falls prevention program.BMC Health Serv Res.2006;6:69.
- ,,,.Serious falls in hospitalized patients: correlates and resource utilization.Am J Med.1995;99(2):137–143.
- ,.Using tools to assess and prevent inpatient falls.Jt Comm J Qual Saf.2003;29(7):363–368.
- ,,.Incidence and risk factors for inpatient falls in an academic acute‐care hospital.J Nippon Med Sch.2006;73(5):265–270.
- .Nonpayment for performance? Medicare's new reimbursement rule.N Engl J Med.2007;357(16):1573–1575.
- .Clinical practice. preventing falls in elderly persons.N Engl J Med.2003;348(1):42–49.
- .Building the science of falls‐prevention research.J Am Geriatr Soc.2004;52(3):461–462.
- ,,,,,.Interventions for preventing falls in acute‐ and chronic‐care hospitals: a systematic review and meta‐analysis.J Am Geriatr Soc.2008;56(1):29–36.
- ,,, et al.Interventions for the prevention of falls in older adults: systematic review and meta‐analysis of randomised clinical trials.BMJ.2004;328(7441):680.
- ,,, et al.Acceptability of fall prevention measures for hospital inpatients.Age Ageing.2004;33(4):400–401.
- ,,, et al.Can volunteer companions prevent falls among inpatients? A feasibility study using a pre‐post comparative design.BMC Geriatr.2006;6:11.
- ,,,,.Using targeted risk factor reduction to prevent falls in older in‐patients: a randomised controlled trial.Age Ageing.2004;33(4):390–395.
- .Prevention of falls in hospital inpatients: agendas for research and practice.Age Ageing.2004;33(4):328–330.
- ,,, et al.Patterns and predictors of inpatient falls and fall‐related injuries in a large academic hospital.Infect Control Hosp Epidemiol.2005;26(10):822–827.
- ,,,,.The relationship of falls to injury among hospital in‐patients.Int J Clin Pract.2005;59(1):17–20.
- ,,,,,.Indications for computed tomography in patients with minor head injury.N Engl J Med.2000;343(2):100–105.
- ,,.Anemia increases risk for falls in hospitalized older adults: an evaluation of falls in 362 hospitalized, ambulatory, long‐term care, and community patients.J Am Med Dir Assoc.2006;7(5):287–293.
- ,,,,,.Improving the capture of fall events in hospitals: combining a service for evaluating inpatient falls with an incident report system.J Am Geriatr Soc.2008;56(4):701–704.
- ,,, et al.Attitudes and barriers to incident reporting: a collaborative hospital study.Qual Saf Health Care.2006;15(1):39–43.
Copyright © 2010 Society of Hospital Medicine