User login
Injection Pearls
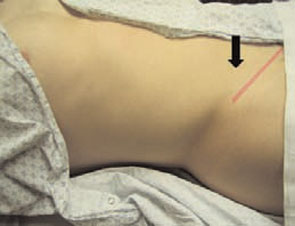
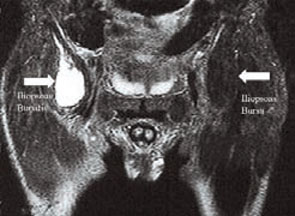
A 29-year-old male warehouse worker noticed pain in his right lower quadrant. The pain was intense and poorly localized (arrow) and increased with lifting or resisted hip flexion. Appendicitis was diagnosed, but pain persisted post-operatively. Necrotizing fasciitis was suspected, but repeated debridements failed to relieve the pain.


Physical Exam
The inguinal ligament runs parallel to the inguinal crease (pink pencil line—see right). About midway in its length, the ligament became difficult to identify due to an exquisitely tender doughy area (arrow). Palpation of this area reproduced the patent’s symptoms, along with poorly localized lower abdominal pain. An attempted sit-up caused similar symptoms.
Anatomy
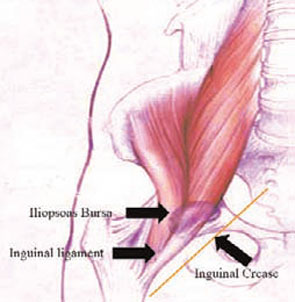
The iliopsoas bursa is located where the inguinal ligament, the iliopsoas tendon, and the transversus tendon intersect. An inflamed iliopsoas bursa is palpable as a doughy mass below the midpoint of the length of the inguinal ligament, lateral to the femoral artery. Most often the opposite, unaffected side demonstrates a normal, pencil-thin, easily defined, non-tender inguinal ligament.
Iliopsoas Bursitis/Tendonitis
The iliopsoas bursa is the largest bursa in the body and communicates with the hip joint in 15% of patients. Bursitis/tendonitis is caused by overuse and friction as the tendon rides over the iliopectineal eminence of the pubis. The condition is associated with lifting, unloading trucks, and participating in sports requiring extensive use of the hip flexors (e.g., soccer, ballet, uphill running, hurdling, jumping). Iliopsoas bursitis/tendonitis is characterized by deep groin pain, sometimes radiating to the anterior hip or thigh, and is often accompanied by a snapping sensation. The patient may limp.
The pain is difficult for patients to localize and challenging for clinicians to reproduce. In fact, the average time from the onset of symptoms to diagnosis is 31 to 42 months. It is common for many other diagnoses to be entertained and treated with no improvement. Physical examination will reveal pain on deep palpation over the femoral triangle, where the musculotendinous junction of the iliopsoas can be palpated as a doughy diffuse area of tenderness at the midpoint of the inguinal ligament.
Pain may also be produced when the affected hip is extended or when the supine patient raises his or her heels off the table at about 15 degrees. In the latter position, the only active hip flexor is the iliopsoas.
Imaging
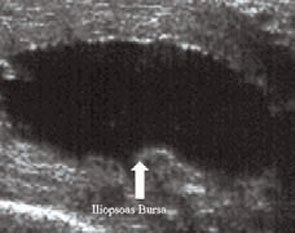
Although these procedures are not necessary for diagnosis, iliopsoas bursitis is best visualized using ultrasound or MRI—either of which will reveal a collection of fluid adjacent to the muscle. Treatment is conservative and consists of rest followed by stretching of the hip flexors and rotators, then strengthening and gradual return to work or sport. As in any overuse injury, biomechanical abnormalities must be sought and corrected. While most patients resolve spontaneously, corticosteroid injections are helpful in about one-third of patients. Rarely, surgical management of recalcitrant cases is warranted.
Iliopsoas Bursitis/Tendonitis Injection
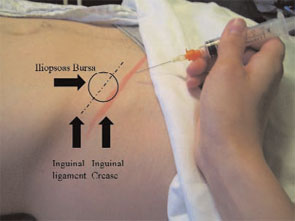
The following procedure should be followed when administering a corticosteroid injection. With the fingers of one hand, identify and isolate the inguinal ligament in the area of doughy discomfort. With the other hand, insert a 1.5-inch needle to its hub, parallel to the ligament, and inject a steroid and lidocaine mixture slowly while withdrawing the needle to avoid inadvertently injecting the ligament or any tendons.
A medium-acting depot steroid gives good, long-lasting relief. A mixture of lidocaine or bupivacaine and the steroid allows for immediate relief, as well as confirmation that the steroid reached its target. TH
Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, and Dr. Ficalora is an associate professor in internal medicine at the Mayo Clinic College of Medicine.
A 29-year-old male warehouse worker noticed pain in his right lower quadrant. The pain was intense and poorly localized (arrow) and increased with lifting or resisted hip flexion. Appendicitis was diagnosed, but pain persisted post-operatively. Necrotizing fasciitis was suspected, but repeated debridements failed to relieve the pain.
Physical Exam
The inguinal ligament runs parallel to the inguinal crease (pink pencil line—see right). About midway in its length, the ligament became difficult to identify due to an exquisitely tender doughy area (arrow). Palpation of this area reproduced the patent’s symptoms, along with poorly localized lower abdominal pain. An attempted sit-up caused similar symptoms.
Anatomy
The iliopsoas bursa is located where the inguinal ligament, the iliopsoas tendon, and the transversus tendon intersect. An inflamed iliopsoas bursa is palpable as a doughy mass below the midpoint of the length of the inguinal ligament, lateral to the femoral artery. Most often the opposite, unaffected side demonstrates a normal, pencil-thin, easily defined, non-tender inguinal ligament.
Iliopsoas Bursitis/Tendonitis
The iliopsoas bursa is the largest bursa in the body and communicates with the hip joint in 15% of patients. Bursitis/tendonitis is caused by overuse and friction as the tendon rides over the iliopectineal eminence of the pubis. The condition is associated with lifting, unloading trucks, and participating in sports requiring extensive use of the hip flexors (e.g., soccer, ballet, uphill running, hurdling, jumping). Iliopsoas bursitis/tendonitis is characterized by deep groin pain, sometimes radiating to the anterior hip or thigh, and is often accompanied by a snapping sensation. The patient may limp.
The pain is difficult for patients to localize and challenging for clinicians to reproduce. In fact, the average time from the onset of symptoms to diagnosis is 31 to 42 months. It is common for many other diagnoses to be entertained and treated with no improvement. Physical examination will reveal pain on deep palpation over the femoral triangle, where the musculotendinous junction of the iliopsoas can be palpated as a doughy diffuse area of tenderness at the midpoint of the inguinal ligament.
Pain may also be produced when the affected hip is extended or when the supine patient raises his or her heels off the table at about 15 degrees. In the latter position, the only active hip flexor is the iliopsoas.
Imaging
Although these procedures are not necessary for diagnosis, iliopsoas bursitis is best visualized using ultrasound or MRI—either of which will reveal a collection of fluid adjacent to the muscle. Treatment is conservative and consists of rest followed by stretching of the hip flexors and rotators, then strengthening and gradual return to work or sport. As in any overuse injury, biomechanical abnormalities must be sought and corrected. While most patients resolve spontaneously, corticosteroid injections are helpful in about one-third of patients. Rarely, surgical management of recalcitrant cases is warranted.
Iliopsoas Bursitis/Tendonitis Injection
The following procedure should be followed when administering a corticosteroid injection. With the fingers of one hand, identify and isolate the inguinal ligament in the area of doughy discomfort. With the other hand, insert a 1.5-inch needle to its hub, parallel to the ligament, and inject a steroid and lidocaine mixture slowly while withdrawing the needle to avoid inadvertently injecting the ligament or any tendons.
A medium-acting depot steroid gives good, long-lasting relief. A mixture of lidocaine or bupivacaine and the steroid allows for immediate relief, as well as confirmation that the steroid reached its target. TH
Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, and Dr. Ficalora is an associate professor in internal medicine at the Mayo Clinic College of Medicine.
A 29-year-old male warehouse worker noticed pain in his right lower quadrant. The pain was intense and poorly localized (arrow) and increased with lifting or resisted hip flexion. Appendicitis was diagnosed, but pain persisted post-operatively. Necrotizing fasciitis was suspected, but repeated debridements failed to relieve the pain.
Physical Exam
The inguinal ligament runs parallel to the inguinal crease (pink pencil line—see right). About midway in its length, the ligament became difficult to identify due to an exquisitely tender doughy area (arrow). Palpation of this area reproduced the patent’s symptoms, along with poorly localized lower abdominal pain. An attempted sit-up caused similar symptoms.
Anatomy
The iliopsoas bursa is located where the inguinal ligament, the iliopsoas tendon, and the transversus tendon intersect. An inflamed iliopsoas bursa is palpable as a doughy mass below the midpoint of the length of the inguinal ligament, lateral to the femoral artery. Most often the opposite, unaffected side demonstrates a normal, pencil-thin, easily defined, non-tender inguinal ligament.
Iliopsoas Bursitis/Tendonitis
The iliopsoas bursa is the largest bursa in the body and communicates with the hip joint in 15% of patients. Bursitis/tendonitis is caused by overuse and friction as the tendon rides over the iliopectineal eminence of the pubis. The condition is associated with lifting, unloading trucks, and participating in sports requiring extensive use of the hip flexors (e.g., soccer, ballet, uphill running, hurdling, jumping). Iliopsoas bursitis/tendonitis is characterized by deep groin pain, sometimes radiating to the anterior hip or thigh, and is often accompanied by a snapping sensation. The patient may limp.
The pain is difficult for patients to localize and challenging for clinicians to reproduce. In fact, the average time from the onset of symptoms to diagnosis is 31 to 42 months. It is common for many other diagnoses to be entertained and treated with no improvement. Physical examination will reveal pain on deep palpation over the femoral triangle, where the musculotendinous junction of the iliopsoas can be palpated as a doughy diffuse area of tenderness at the midpoint of the inguinal ligament.
Pain may also be produced when the affected hip is extended or when the supine patient raises his or her heels off the table at about 15 degrees. In the latter position, the only active hip flexor is the iliopsoas.
Imaging
Although these procedures are not necessary for diagnosis, iliopsoas bursitis is best visualized using ultrasound or MRI—either of which will reveal a collection of fluid adjacent to the muscle. Treatment is conservative and consists of rest followed by stretching of the hip flexors and rotators, then strengthening and gradual return to work or sport. As in any overuse injury, biomechanical abnormalities must be sought and corrected. While most patients resolve spontaneously, corticosteroid injections are helpful in about one-third of patients. Rarely, surgical management of recalcitrant cases is warranted.
Iliopsoas Bursitis/Tendonitis Injection
The following procedure should be followed when administering a corticosteroid injection. With the fingers of one hand, identify and isolate the inguinal ligament in the area of doughy discomfort. With the other hand, insert a 1.5-inch needle to its hub, parallel to the ligament, and inject a steroid and lidocaine mixture slowly while withdrawing the needle to avoid inadvertently injecting the ligament or any tendons.
A medium-acting depot steroid gives good, long-lasting relief. A mixture of lidocaine or bupivacaine and the steroid allows for immediate relief, as well as confirmation that the steroid reached its target. TH
Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, and Dr. Ficalora is an associate professor in internal medicine at the Mayo Clinic College of Medicine.