User login
Scapular Pain
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).

Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.


Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.

Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)




Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).
Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.
Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.
Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).
Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.
Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.
Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Lateral Thigh Pain
A 67-year-old, slightly obese female was referred for poorly controlled hypertension and complaints of bilateral hip pain. Her pain worsens at night: It wakes her up when she rolls over on her hips. She also feels more pain when she is going up stairs.
Recently, she had difficulty bearing weight on her left hip. She has used a cane purchased at a yard sale for the past two and a half years. Daily ibuprofen provides her with little relief.
Physical Exam
On exam, we found that the patient had lateral thigh tenderness over the greater trochanter bilaterally and slight groin pain on internal/external rotation bilaterally. (See photos 1 and 2.)
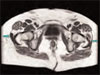
We ordered an MRI because of concern that there might be a hip fracture. The results of the MRI indicate that both trochanteric bursae were inflamed and filled with fluid. The left bursa had much more fluid than the right. (See photo 3.)


Trochanteric Bursitis
We see trochanteric bursitis in runners and also after local trauma. This condition is most commonly found, however, in individuals with gait disturbances, such as those caused by a post-stroke condition, a discrepancy in leg length, pregnancy, medically complicated obesity, or improperly adjusted canes and walkers.
The pain caused by trochanteric bursitis may be severe and may radiate into the buttock or anterior thigh, mimicking fracture or radiculopathy.
The Trochanteric Bursae
There are three trochanteric bursae around the greater trochanter: two major and one minor. The minor bursa is the subgluteus minimus bursa, which is located above and slightly anterior to the proximal superior surface of the greater trochanter.
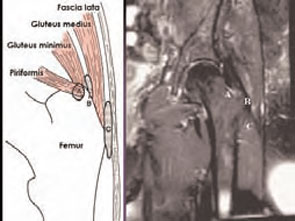
There are two major bursae. The subgluteus medius bursa can be found beneath the gluteus medius muscle, posterior and superior to the proximal edge of the greater trochanter. The subgluteus maximus bursa is lateral to the greater trochanter but separated from the trochanter by the gluteus medius muscle beneath the converging fibers of the tensor fascia lata and the gluteus maximus muscle and fascia as they join to form the iliotibial tract. Almond-shaped, 4 to 6 cm in length, and 2 to 4 cm in width, this bursa functions as a gliding mechanism for the anterior portion of the gluteus maximus tendon as it passes over the greater trochanter to insert into the iliotibial band. (See photo 4.)
Treatment
Although non-steroidal anti-inflammatory drugs (NSAIDs) provide relief to some patients, the elderly, who are most affected by trochanteric bursitis, frequently have contraindications to NSAID use. Local steroid injections provide durable relief for most patients. To limit recurrences, correct gait abnormalities and strengthen postural and hip muscles.

Trochanteric Bursitis Injection
To administer a trochanteric bursitis injection, first locate the subgluteus maximus bursa by palpating the greater trochanter. The bursa is located directly above the periosteum.
Next, identify an area of point tenderness. Instill a mixture of steroid and local anesthetic. The correct location will be confirmed by immediate pain relief; the steroid effect, however, may take up to week to provide pain relief. (See photo 5.)

Three-Month Follow-Up
The patient returned three months after her trochanateric bursae were injected with a depo-steroid preparation Today she no longer requires a cane. She is sleeping well and climbing stairs easily. Her blood pressure is well controlled, and she is on minimal medications after withdrawal of NSAIDs. She enjoys a renewed interest in German folk dancing.
Prevention
Prevention hinges on normalizing the gait abnormality that caused the bursal inflammation. That usually means strengthening the quadriceps—with or without a properly adjusted gait assist device such as a cane or an orthotic. (See photo 6.) TH
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
A 67-year-old, slightly obese female was referred for poorly controlled hypertension and complaints of bilateral hip pain. Her pain worsens at night: It wakes her up when she rolls over on her hips. She also feels more pain when she is going up stairs.
Recently, she had difficulty bearing weight on her left hip. She has used a cane purchased at a yard sale for the past two and a half years. Daily ibuprofen provides her with little relief.
Physical Exam
On exam, we found that the patient had lateral thigh tenderness over the greater trochanter bilaterally and slight groin pain on internal/external rotation bilaterally. (See photos 1 and 2.)
We ordered an MRI because of concern that there might be a hip fracture. The results of the MRI indicate that both trochanteric bursae were inflamed and filled with fluid. The left bursa had much more fluid than the right. (See photo 3.)
Trochanteric Bursitis
We see trochanteric bursitis in runners and also after local trauma. This condition is most commonly found, however, in individuals with gait disturbances, such as those caused by a post-stroke condition, a discrepancy in leg length, pregnancy, medically complicated obesity, or improperly adjusted canes and walkers.
The pain caused by trochanteric bursitis may be severe and may radiate into the buttock or anterior thigh, mimicking fracture or radiculopathy.
The Trochanteric Bursae
There are three trochanteric bursae around the greater trochanter: two major and one minor. The minor bursa is the subgluteus minimus bursa, which is located above and slightly anterior to the proximal superior surface of the greater trochanter.
There are two major bursae. The subgluteus medius bursa can be found beneath the gluteus medius muscle, posterior and superior to the proximal edge of the greater trochanter. The subgluteus maximus bursa is lateral to the greater trochanter but separated from the trochanter by the gluteus medius muscle beneath the converging fibers of the tensor fascia lata and the gluteus maximus muscle and fascia as they join to form the iliotibial tract. Almond-shaped, 4 to 6 cm in length, and 2 to 4 cm in width, this bursa functions as a gliding mechanism for the anterior portion of the gluteus maximus tendon as it passes over the greater trochanter to insert into the iliotibial band. (See photo 4.)
Treatment
Although non-steroidal anti-inflammatory drugs (NSAIDs) provide relief to some patients, the elderly, who are most affected by trochanteric bursitis, frequently have contraindications to NSAID use. Local steroid injections provide durable relief for most patients. To limit recurrences, correct gait abnormalities and strengthen postural and hip muscles.
Trochanteric Bursitis Injection
To administer a trochanteric bursitis injection, first locate the subgluteus maximus bursa by palpating the greater trochanter. The bursa is located directly above the periosteum.
Next, identify an area of point tenderness. Instill a mixture of steroid and local anesthetic. The correct location will be confirmed by immediate pain relief; the steroid effect, however, may take up to week to provide pain relief. (See photo 5.)
Three-Month Follow-Up
The patient returned three months after her trochanateric bursae were injected with a depo-steroid preparation Today she no longer requires a cane. She is sleeping well and climbing stairs easily. Her blood pressure is well controlled, and she is on minimal medications after withdrawal of NSAIDs. She enjoys a renewed interest in German folk dancing.
Prevention
Prevention hinges on normalizing the gait abnormality that caused the bursal inflammation. That usually means strengthening the quadriceps—with or without a properly adjusted gait assist device such as a cane or an orthotic. (See photo 6.) TH
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
A 67-year-old, slightly obese female was referred for poorly controlled hypertension and complaints of bilateral hip pain. Her pain worsens at night: It wakes her up when she rolls over on her hips. She also feels more pain when she is going up stairs.
Recently, she had difficulty bearing weight on her left hip. She has used a cane purchased at a yard sale for the past two and a half years. Daily ibuprofen provides her with little relief.
Physical Exam
On exam, we found that the patient had lateral thigh tenderness over the greater trochanter bilaterally and slight groin pain on internal/external rotation bilaterally. (See photos 1 and 2.)
We ordered an MRI because of concern that there might be a hip fracture. The results of the MRI indicate that both trochanteric bursae were inflamed and filled with fluid. The left bursa had much more fluid than the right. (See photo 3.)
Trochanteric Bursitis
We see trochanteric bursitis in runners and also after local trauma. This condition is most commonly found, however, in individuals with gait disturbances, such as those caused by a post-stroke condition, a discrepancy in leg length, pregnancy, medically complicated obesity, or improperly adjusted canes and walkers.
The pain caused by trochanteric bursitis may be severe and may radiate into the buttock or anterior thigh, mimicking fracture or radiculopathy.
The Trochanteric Bursae
There are three trochanteric bursae around the greater trochanter: two major and one minor. The minor bursa is the subgluteus minimus bursa, which is located above and slightly anterior to the proximal superior surface of the greater trochanter.
There are two major bursae. The subgluteus medius bursa can be found beneath the gluteus medius muscle, posterior and superior to the proximal edge of the greater trochanter. The subgluteus maximus bursa is lateral to the greater trochanter but separated from the trochanter by the gluteus medius muscle beneath the converging fibers of the tensor fascia lata and the gluteus maximus muscle and fascia as they join to form the iliotibial tract. Almond-shaped, 4 to 6 cm in length, and 2 to 4 cm in width, this bursa functions as a gliding mechanism for the anterior portion of the gluteus maximus tendon as it passes over the greater trochanter to insert into the iliotibial band. (See photo 4.)
Treatment
Although non-steroidal anti-inflammatory drugs (NSAIDs) provide relief to some patients, the elderly, who are most affected by trochanteric bursitis, frequently have contraindications to NSAID use. Local steroid injections provide durable relief for most patients. To limit recurrences, correct gait abnormalities and strengthen postural and hip muscles.
Trochanteric Bursitis Injection
To administer a trochanteric bursitis injection, first locate the subgluteus maximus bursa by palpating the greater trochanter. The bursa is located directly above the periosteum.
Next, identify an area of point tenderness. Instill a mixture of steroid and local anesthetic. The correct location will be confirmed by immediate pain relief; the steroid effect, however, may take up to week to provide pain relief. (See photo 5.)
Three-Month Follow-Up
The patient returned three months after her trochanateric bursae were injected with a depo-steroid preparation Today she no longer requires a cane. She is sleeping well and climbing stairs easily. Her blood pressure is well controlled, and she is on minimal medications after withdrawal of NSAIDs. She enjoys a renewed interest in German folk dancing.
Prevention
Prevention hinges on normalizing the gait abnormality that caused the bursal inflammation. That usually means strengthening the quadriceps—with or without a properly adjusted gait assist device such as a cane or an orthotic. (See photo 6.) TH
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.