Interventional cardiology has made great strides in the last few decades. Percutaneous coronary intervention (PCI) is among the most commonly performed medical procedures globally.1 At the time of inception, PCI was plagued by high complication rates—balloon catheters had a 50% target-lesion restenosis rate at 6 months and required emergency bypass surgery in up to 6% patients.2 With passage of time, the complication rate of PCI has markedly decreased.
Figure 1. Reduction of restenosis rates by stent type.
The introduction of stents had a dramatic impact on lowering the complication rates. Initially, the bare-metal stents (BMS) reduced the stent restenosis rate to 10% to 15%. Drug-eluting stents (DES) have further revolutionized the field (Figure 1), significantly lowering rates of stent thrombosis (less than 0.5% in 1 year) and risk of restenosis (less than 5% in 1 year).3–6 The second-generation DES widely used in contemporary practice have made even more reductions owing to their improved designs and metallic and polymer composition; and concurrent advancements in the medical management, including use of antithrombotic and antiproliferative drugs, have further contributed to improved rates.
Figure 2. Second- vs first-generation drug-eluting stents.
What, then, is to be hoped for? Unfortunately, with the advent of stents, complications such as stent thrombosis and stent restenosis also emerged. These complications can be life-threatening in the form of post-procedural or late myocardial infarction and cardiac death. Thus, although the US Food and Drug Administration (FDA) assesses target-lesion failure (defined as a composite of cardiac death, target vessel myocardial infarction, or ischemia-driven target vessel revascularization) at 1 year, patients can have complications for the remainder of their lives. Despite the advancements attained by the second-generation DES over their predecessors, the issue of stent thrombosis and restenosis continues to plague second-generation DES with a 2% to 2.5% increased rate of target-lesion failure each year, seemingly forever (Figure 2).7,8
This article will briefly discuss the stent design and pathophysiology driving stent thrombosis and restenosis along with potential strategies to mitigate the problem. It pays special emphasis to bioresorbable stents, given their increasing interest among interventional cardiologists and patients, and given their potential to transform the practice of PCI.
STENT DESIGN
Contemporary DES essentially consist of three components:
A metallic alloy with a mesh-like design serves as the platform for the stent.
This framework is coated with a multi-layered polymer that holds and releases the active drug in a controlled manner so that its effects can be extended.
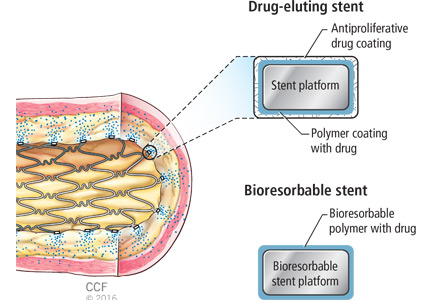
Figure 3. Components of drug-eluting and bioresorbable stents.An antiproliferative drug (absent in the bioresorbable stents) that inhibits the smooth muscle proliferation and neointimal hyperplastic response: sirolimus or paclitaxel in first-generation DES; everolimus or zotarolimus in second-generation DES (Figure 3).
WHAT CAUSES STENT THROMBOSIS AND RESTENOSIS?
Several theories and pathophysiological mechanisms have been proposed to explain these late adverse events (Table 1). However, our overall understanding of the cause remains modest at best. The major factor seems to be persistent presence of polymer on the stent and the ensuing inflammation. The second issue appears to be related to neoatherosclerosis that is generally defined as lipid or calcified neointima. Neoatherosclerosis is especially problematic for the second-generation DES. Neoatherosclerosis eventually predisposes to the development of thin cap fibroadenoma, and the rupture of thin cap leads to stent thrombosis and restenosis.
Autopsy studies suggest that approximately 50% of first- and second-generation DES start developing neoatherosclerosis within 1 to 3 years of implantation.9 Turbulence created by thick strutted stents or incomplete impaction of stents to the vessel wall predisposes the stents to platelet aggregation and fibrinogen deposition, thereby increasing the risk of neoatherosclerosis. Despite these pathologic insights, no treatment strategy has been shown to attenuate the problem, with the exception of high-dose statins.
CAN WE SOLVE THE PROBLEM?
Three technological approaches have been proposed to overcome stent thrombosis and restenosis:
Stents coated with bioresorbable polymers that quickly degrade
Stents without polymers
Stents that are completely resorbed.
STENTS WITH BIORESORBABLE POLYMERS
As described above, the presence of a polymer on the stent predisposes it to inflammation. Therefore, it would be logical to hypothesize that a bioresorbable polymer would reduce the inflammation. This approach is typified by the second-generation paclitaxel-eluting stent (Synergy, Boston Scientific). It has a biodegradable coating that resorbs within 4 months and releases everolimus in a dose intensity similar to that seen with the contemporary second-generation DES.
The largest trial of this device to date, the Evolve II study, randomly assigned 1,684 patients to the biostable-polymer, everolimus-eluting chromium stent (Promus, Boston Scientific) or the paclitaxel-eluting stent (Synergy, Boston Scientific).10 Two-year follow-up data suggest that the rate of target-lesion failure was 9.4% in the paclitaxel-eluting stent patients vs 8.5% in the everolimus-eluting stent patients. Notably, no definite stent thrombosis was seen in the Synergy-treated patients 24 hours after the initial device implantation.
STENTS WITHOUT POLYMERS
If polymers predispose to inflammation, stents without polymers should mitigate the risk. Such stent types are exemplified by the BioFreedom (Biosensors International) stainless steel stent, a polymer-free umirolimus (also known as biolimus A9)-eluting stent. These stents have a microstructured surface that holds the drug without a polymer and releases the active drug over a few months.
The LEADERS FREE clinical trial studied this stent in 2,466 patients at high risk of bleeding.11 The patients were randomized to receive either a BMS or the polymer-free stent. All patients were required to receive dual antiplatelet therapy for only 1 month. At 1 year, the composite risk of cardiac death, myocardial infarction, and stent thrombois was 9.4% in patients with BioFreedom stents vs 12.9% in BMS patients. Of note, the primary end point did not include stent restenosis, thereby not disadvantaging the BMS.
Medtronic’s polymer-free, sirolimus-eluting stent is currently under investigation in the RevElution clinical trial.12 It has a cylindrical structure with the core replaced by the active drug sirolimus. Abluminal holes in the stent allow controlled release of the drug. A pharmacokinetic analysis show that 90% of the medication is released within the first 90 days and that tissue concentrations are maintained in the therapeutic range until at least that time.13 This actually exceeds that of the second-generation everolimus-eluting DES.
BIORESORBABLE STENTS
Bioresorbable scaffolds or stents disappear entirely over time and have drawn considerable attention in the interventional cardiology community. The FDA recently approved Abbott’s Poly-L-Lactic Acid (PLLA) everolimus-eluting stent (Absorb). The rate of bioresorption of this device can be controlled by modulating the respective contribution of amorphous and crystalline PLLA backbone. The advantage of bioresorbable stents appears to stem from the fact that with bioresorbable devices, the vessel may actually expand and the purported nidus for inflammation goes away. This has been demonstrated by serial intravascular ultrasound-based studies.14
The return of pulsatility also appears to modulate the transition of smooth muscles from proliferative back to their contractile phenotype. This has been hypothesized to reduce the risk of neoatherosclerosis and, consequently, stent restenosis. The limitation of this device is the large strut size (157 micron for Absorb vs 81 microns for Xience). Dissolving metallic scaffolds also tend to have thicker struts than the current DES (120 vs approximately 80 microns).
The Absorb III trial was a pivotal noninferiority US trial that led to the device approval.15 In this trial, 2,008 patients were randomized to receive the Absorb bioresorbable, everolimus-eluting stent or the DES Xience. The primary study end point was target-lesion failure at 1 year. As is often the case with US landmark studies, patient and lesion complexities were limited. Patients with acute coronary syndrome, elevated cardiac enzymes, high-risk anatomic lesions such as bifurcation lesions, and chronic total occlusion were excluded. Patients with diabetes comprised less than one-third of the patients, and lesions were relatively short at 13 ± 6 mm.
Figure 4. ABSORB learnings: MICAT. Pre-dilation with noncompliant balloon sized 1:1 to normal vessel with complete balloon expansion; post-dilation at 14–16 atmospheres.
Device success per lesion was lower with Absorb than with Xience (94.3% vs 99.3%; P < .0001). This is likely due to the larger strut size. Absorb III did meet the prespecified primary end point for noninferiority (P = .007), although the rate of adverse events was somewhat higher (7.8% vs 6.1%). A subgroup analysis reveals that 19% of all lesions were smaller than what was originally intended, and in these patients, the Absorb device performed poorly with a 4.6% risk of device thrombosis. When limited to patients with the intended reference vessel sizes, the results of target-lesion failure and stent thrombosis were similar (6.6% vs 5.5% and 0.8% vs 0.5%, respectively).15
The implantation technique also seems to have influenced the results, with increased use of post-dilation as the study evolved. Recent observations from the MICAT group have shown that the use of high pressure post-dilation and other procedural advancements may considerably reduce adverse outcomes associated with Absorb (Figure 4).16 Thus, while the pooled analysis in the form of a meta-analysis has suggested an increased risk of device thrombosis,17 the difference is attenuated by selecting lesions of appropriate size, high-pressure post-dilation, and procedural advancements (Table 2).
CONCLUSION AND THE WAY FORWARD
Current first-generation bioresorbable stents can achieve results similar to those of second-generation DES, provided that they are used in patients with noncomplicated coronary lesions and the implant techniques are optimized. We do not know the outcomes of bioresorbable stents in patients with complex lesions. Current experience suggests that other changes in technique would be needed. For example, minimizing scaffold overlap in long and bifurcating lesions. Whether that would translate into diminishing the rate of late adverse events remains to be determined. As of now, we only have data on approximately 100 highly selected patients beyond 3 years (no adverse events 2.5 to 5 years after implantation).
Several investigational second-generation bioresorbable stents, including Elixir’s Dissolve PLLA, Boston Scientific’s FAST, and a newer version of Absorb, are in early clinical trials. Smaller strut thickness holds the promise of attenuating the risk of stent thrombosis. Since the polymer persists, no reduction in dual antiplatelet therapy duration is likely to be achieved.
Results from long-term follow-up of Absorb III and on-going trials are eagerly awaited to ascertain whether the rate of late complications of DES can be mitigated. It would not be surprising if the second-generation bioresorbable stents make DES a thing of the past within the next decade.
References
Palmerini T, Benedetto U, Biondi-Zoccai G, et al. Long-term safety of drug-eluting and bare-metal stents: evidence from a comprehensive network meta-analysis. J Am Coll Cardiol 2015; 65:2496–2507.
Bates ER. Balancing the evidence base on coronary stents. N Engl J Med 2016; 375:1286–1288.
Macaya C, Serruys PW, Ruygrok P, et al. Continued benefit of coronary stenting versus balloon angioplasty: one-year clinical follow-up of BENESTENT trial. BENESTENT Study Group. J Am Coll Cardiol 1996; 27:255–261.
Fajadet J, Wijns W, Laarman GJ; for the ENDEAVOR II Investigators. Randomized, double-blind, multicenter study of the Endeavor zotarolimus-eluting phosphorylcholine-encapsulated stent for treatment of native coronary artery lesions: clinical and angiographic results of the ENDEAVOR II trial. Circulation 2006; 114:798–806.
Kirtane AJ, Leon MB, Ball MW, et al; ENDEAVOR IV Investigators. The “final” 5-year follow-up from the ENDEAVOR IV trial comparing a zotarolimus-eluting stent with a paclitaxel-eluting stent. JACC Cardiovasc Interv 2013; 6:325–333.
Stone GW, Midei M, Newman W, et al; SPIRIT III Investigators. Comparison of an everolimus-eluting stent and a paclitaxel-eluting stent in patients with coronary artery disease: a randomized trial. JAMA 2008; 299:1903–1913.
Gada H, Kirtane AJ, Newman W, et al. 5-year results of a randomized comparison of XIENCE V everolimus-eluting and TAXUS paclitaxel-eluting stents: final results from the SPIRIT III trial (clinical evaluation of the XIENCE V everolimus eluting coronary stent system in the treatment of patients with de novo native coronary artery lesions). JACC Cardiovasc Interv 2013; 6:1263–1266.
Benedetto U, Raja SG, Soliman RFB, et al; on behalf of the Harefield Cardiac Outcomes Research Group. Minimally invasive direct coronary artery bypass improves late survival compared with drug-eluting stents in isolated proximal left anterior descending artery disease: a 10-year follow-up, single-center, propensity score analysis. J Thorac Cardiovasc Surg 2014; 148:1316–1322.
Virmani R, CV Path Institute. Problems encountered with drug-eluting stent. Presented at Transcatheter Cardiovascular Therapeutics (TCT); October 11–15, 2015; San Francisco, CA.
Kereiakes DJ, Meredith IT, Windecker S, et al. Efficacy and safety of a novel bioabsorbable polymer-coated, everolimus-eluting coronary stent: the EVOLVE II Randomized Trial. Circ Cardiovasc Interv 2015; 8:e002372.
Urban P, Meredith IT, Abizaid A, et al; for the LEADERS FREE Investigators. Polymer-free drug-coated coronary stents in patients at high bleeding risk. N Engl J Med 2015; 373:2038–2047.
Worthley SG, Abizaid A, Kirtane AJ, Simon D, Windecker S, Stone GW. Stent strut coverage and stent apposition after implantation of a novel drug-filled coronary stent: optical coherence tomography results from RevElution trial. J Am Coll Cardiol 2015; 66(suppl B):B235 [Abstract TCT-579].
Abizaid A, Costa RA, Schofer J, et al. Serial multimodality imaging and 2-year clinical outcomes of the novel DESolve novolimus-eluting bioresorbable coronary scaffold system for the treatment of single de novo coronary lesions. JACC Cardiovasc Interv 2016; 9:565–574.
Ellis SG, Kereiakes DJ, Metzger DC, et al; for the ABOSRB III Investigators. Everolimus-eluting bioresorbable scaffolds for coronary artery disease. N Engl J Med 2015; 373:1905–1915.
Puricel S, Cuculi F, Weissner M, et al. Bioresorbable coronary scaffold thrombosis: multicenter comprehensive analysis of clinical presentation, mechanisms, and predictors. J Am Coll Cardiol 2016; 67:921−931.
Stone GW, Gao R, Kimura T, et al. 1-year outcomes with the Absorb bioresorbable scaffold in patients with coronary artery disease: a patient-level, pooled meta-analysis. Lancet 2016; 387:1277–1289.
Stephen G. Ellis, MD Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic
Haris Riaz, MD Resident, Department of Internal Medicine, Cleveland Clinic
Correspondence: Stephen G. Ellis, MD, Department of Cardiovascular Medicine, J2-3, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; elliss@ccf.org
Dr. Ellis reported consulting for Abbott Vascular. Dr. Riaz reported no financial interests or relationships that pose a potential conflict of interest with this article.
Stephen G. Ellis, MD Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic
Haris Riaz, MD Resident, Department of Internal Medicine, Cleveland Clinic
Correspondence: Stephen G. Ellis, MD, Department of Cardiovascular Medicine, J2-3, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; elliss@ccf.org
Dr. Ellis reported consulting for Abbott Vascular. Dr. Riaz reported no financial interests or relationships that pose a potential conflict of interest with this article.
Author and Disclosure Information
Stephen G. Ellis, MD Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic
Haris Riaz, MD Resident, Department of Internal Medicine, Cleveland Clinic
Correspondence: Stephen G. Ellis, MD, Department of Cardiovascular Medicine, J2-3, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; elliss@ccf.org
Dr. Ellis reported consulting for Abbott Vascular. Dr. Riaz reported no financial interests or relationships that pose a potential conflict of interest with this article.
Interventional cardiology has made great strides in the last few decades. Percutaneous coronary intervention (PCI) is among the most commonly performed medical procedures globally.1 At the time of inception, PCI was plagued by high complication rates—balloon catheters had a 50% target-lesion restenosis rate at 6 months and required emergency bypass surgery in up to 6% patients.2 With passage of time, the complication rate of PCI has markedly decreased.
Figure 1. Reduction of restenosis rates by stent type.
The introduction of stents had a dramatic impact on lowering the complication rates. Initially, the bare-metal stents (BMS) reduced the stent restenosis rate to 10% to 15%. Drug-eluting stents (DES) have further revolutionized the field (Figure 1), significantly lowering rates of stent thrombosis (less than 0.5% in 1 year) and risk of restenosis (less than 5% in 1 year).3–6 The second-generation DES widely used in contemporary practice have made even more reductions owing to their improved designs and metallic and polymer composition; and concurrent advancements in the medical management, including use of antithrombotic and antiproliferative drugs, have further contributed to improved rates.
Figure 2. Second- vs first-generation drug-eluting stents.
What, then, is to be hoped for? Unfortunately, with the advent of stents, complications such as stent thrombosis and stent restenosis also emerged. These complications can be life-threatening in the form of post-procedural or late myocardial infarction and cardiac death. Thus, although the US Food and Drug Administration (FDA) assesses target-lesion failure (defined as a composite of cardiac death, target vessel myocardial infarction, or ischemia-driven target vessel revascularization) at 1 year, patients can have complications for the remainder of their lives. Despite the advancements attained by the second-generation DES over their predecessors, the issue of stent thrombosis and restenosis continues to plague second-generation DES with a 2% to 2.5% increased rate of target-lesion failure each year, seemingly forever (Figure 2).7,8
This article will briefly discuss the stent design and pathophysiology driving stent thrombosis and restenosis along with potential strategies to mitigate the problem. It pays special emphasis to bioresorbable stents, given their increasing interest among interventional cardiologists and patients, and given their potential to transform the practice of PCI.
STENT DESIGN
Contemporary DES essentially consist of three components:
A metallic alloy with a mesh-like design serves as the platform for the stent.
This framework is coated with a multi-layered polymer that holds and releases the active drug in a controlled manner so that its effects can be extended.
Figure 3. Components of drug-eluting and bioresorbable stents.An antiproliferative drug (absent in the bioresorbable stents) that inhibits the smooth muscle proliferation and neointimal hyperplastic response: sirolimus or paclitaxel in first-generation DES; everolimus or zotarolimus in second-generation DES (Figure 3).
WHAT CAUSES STENT THROMBOSIS AND RESTENOSIS?
Several theories and pathophysiological mechanisms have been proposed to explain these late adverse events (Table 1). However, our overall understanding of the cause remains modest at best. The major factor seems to be persistent presence of polymer on the stent and the ensuing inflammation. The second issue appears to be related to neoatherosclerosis that is generally defined as lipid or calcified neointima. Neoatherosclerosis is especially problematic for the second-generation DES. Neoatherosclerosis eventually predisposes to the development of thin cap fibroadenoma, and the rupture of thin cap leads to stent thrombosis and restenosis.
Autopsy studies suggest that approximately 50% of first- and second-generation DES start developing neoatherosclerosis within 1 to 3 years of implantation.9 Turbulence created by thick strutted stents or incomplete impaction of stents to the vessel wall predisposes the stents to platelet aggregation and fibrinogen deposition, thereby increasing the risk of neoatherosclerosis. Despite these pathologic insights, no treatment strategy has been shown to attenuate the problem, with the exception of high-dose statins.
CAN WE SOLVE THE PROBLEM?
Three technological approaches have been proposed to overcome stent thrombosis and restenosis:
Stents coated with bioresorbable polymers that quickly degrade
Stents without polymers
Stents that are completely resorbed.
STENTS WITH BIORESORBABLE POLYMERS
As described above, the presence of a polymer on the stent predisposes it to inflammation. Therefore, it would be logical to hypothesize that a bioresorbable polymer would reduce the inflammation. This approach is typified by the second-generation paclitaxel-eluting stent (Synergy, Boston Scientific). It has a biodegradable coating that resorbs within 4 months and releases everolimus in a dose intensity similar to that seen with the contemporary second-generation DES.
The largest trial of this device to date, the Evolve II study, randomly assigned 1,684 patients to the biostable-polymer, everolimus-eluting chromium stent (Promus, Boston Scientific) or the paclitaxel-eluting stent (Synergy, Boston Scientific).10 Two-year follow-up data suggest that the rate of target-lesion failure was 9.4% in the paclitaxel-eluting stent patients vs 8.5% in the everolimus-eluting stent patients. Notably, no definite stent thrombosis was seen in the Synergy-treated patients 24 hours after the initial device implantation.
STENTS WITHOUT POLYMERS
If polymers predispose to inflammation, stents without polymers should mitigate the risk. Such stent types are exemplified by the BioFreedom (Biosensors International) stainless steel stent, a polymer-free umirolimus (also known as biolimus A9)-eluting stent. These stents have a microstructured surface that holds the drug without a polymer and releases the active drug over a few months.
The LEADERS FREE clinical trial studied this stent in 2,466 patients at high risk of bleeding.11 The patients were randomized to receive either a BMS or the polymer-free stent. All patients were required to receive dual antiplatelet therapy for only 1 month. At 1 year, the composite risk of cardiac death, myocardial infarction, and stent thrombois was 9.4% in patients with BioFreedom stents vs 12.9% in BMS patients. Of note, the primary end point did not include stent restenosis, thereby not disadvantaging the BMS.
Medtronic’s polymer-free, sirolimus-eluting stent is currently under investigation in the RevElution clinical trial.12 It has a cylindrical structure with the core replaced by the active drug sirolimus. Abluminal holes in the stent allow controlled release of the drug. A pharmacokinetic analysis show that 90% of the medication is released within the first 90 days and that tissue concentrations are maintained in the therapeutic range until at least that time.13 This actually exceeds that of the second-generation everolimus-eluting DES.
BIORESORBABLE STENTS
Bioresorbable scaffolds or stents disappear entirely over time and have drawn considerable attention in the interventional cardiology community. The FDA recently approved Abbott’s Poly-L-Lactic Acid (PLLA) everolimus-eluting stent (Absorb). The rate of bioresorption of this device can be controlled by modulating the respective contribution of amorphous and crystalline PLLA backbone. The advantage of bioresorbable stents appears to stem from the fact that with bioresorbable devices, the vessel may actually expand and the purported nidus for inflammation goes away. This has been demonstrated by serial intravascular ultrasound-based studies.14
The return of pulsatility also appears to modulate the transition of smooth muscles from proliferative back to their contractile phenotype. This has been hypothesized to reduce the risk of neoatherosclerosis and, consequently, stent restenosis. The limitation of this device is the large strut size (157 micron for Absorb vs 81 microns for Xience). Dissolving metallic scaffolds also tend to have thicker struts than the current DES (120 vs approximately 80 microns).
The Absorb III trial was a pivotal noninferiority US trial that led to the device approval.15 In this trial, 2,008 patients were randomized to receive the Absorb bioresorbable, everolimus-eluting stent or the DES Xience. The primary study end point was target-lesion failure at 1 year. As is often the case with US landmark studies, patient and lesion complexities were limited. Patients with acute coronary syndrome, elevated cardiac enzymes, high-risk anatomic lesions such as bifurcation lesions, and chronic total occlusion were excluded. Patients with diabetes comprised less than one-third of the patients, and lesions were relatively short at 13 ± 6 mm.
Figure 4. ABSORB learnings: MICAT. Pre-dilation with noncompliant balloon sized 1:1 to normal vessel with complete balloon expansion; post-dilation at 14–16 atmospheres.
Device success per lesion was lower with Absorb than with Xience (94.3% vs 99.3%; P < .0001). This is likely due to the larger strut size. Absorb III did meet the prespecified primary end point for noninferiority (P = .007), although the rate of adverse events was somewhat higher (7.8% vs 6.1%). A subgroup analysis reveals that 19% of all lesions were smaller than what was originally intended, and in these patients, the Absorb device performed poorly with a 4.6% risk of device thrombosis. When limited to patients with the intended reference vessel sizes, the results of target-lesion failure and stent thrombosis were similar (6.6% vs 5.5% and 0.8% vs 0.5%, respectively).15
The implantation technique also seems to have influenced the results, with increased use of post-dilation as the study evolved. Recent observations from the MICAT group have shown that the use of high pressure post-dilation and other procedural advancements may considerably reduce adverse outcomes associated with Absorb (Figure 4).16 Thus, while the pooled analysis in the form of a meta-analysis has suggested an increased risk of device thrombosis,17 the difference is attenuated by selecting lesions of appropriate size, high-pressure post-dilation, and procedural advancements (Table 2).
CONCLUSION AND THE WAY FORWARD
Current first-generation bioresorbable stents can achieve results similar to those of second-generation DES, provided that they are used in patients with noncomplicated coronary lesions and the implant techniques are optimized. We do not know the outcomes of bioresorbable stents in patients with complex lesions. Current experience suggests that other changes in technique would be needed. For example, minimizing scaffold overlap in long and bifurcating lesions. Whether that would translate into diminishing the rate of late adverse events remains to be determined. As of now, we only have data on approximately 100 highly selected patients beyond 3 years (no adverse events 2.5 to 5 years after implantation).
Several investigational second-generation bioresorbable stents, including Elixir’s Dissolve PLLA, Boston Scientific’s FAST, and a newer version of Absorb, are in early clinical trials. Smaller strut thickness holds the promise of attenuating the risk of stent thrombosis. Since the polymer persists, no reduction in dual antiplatelet therapy duration is likely to be achieved.
Results from long-term follow-up of Absorb III and on-going trials are eagerly awaited to ascertain whether the rate of late complications of DES can be mitigated. It would not be surprising if the second-generation bioresorbable stents make DES a thing of the past within the next decade.
Interventional cardiology has made great strides in the last few decades. Percutaneous coronary intervention (PCI) is among the most commonly performed medical procedures globally.1 At the time of inception, PCI was plagued by high complication rates—balloon catheters had a 50% target-lesion restenosis rate at 6 months and required emergency bypass surgery in up to 6% patients.2 With passage of time, the complication rate of PCI has markedly decreased.
Figure 1. Reduction of restenosis rates by stent type.
The introduction of stents had a dramatic impact on lowering the complication rates. Initially, the bare-metal stents (BMS) reduced the stent restenosis rate to 10% to 15%. Drug-eluting stents (DES) have further revolutionized the field (Figure 1), significantly lowering rates of stent thrombosis (less than 0.5% in 1 year) and risk of restenosis (less than 5% in 1 year).3–6 The second-generation DES widely used in contemporary practice have made even more reductions owing to their improved designs and metallic and polymer composition; and concurrent advancements in the medical management, including use of antithrombotic and antiproliferative drugs, have further contributed to improved rates.
Figure 2. Second- vs first-generation drug-eluting stents.
What, then, is to be hoped for? Unfortunately, with the advent of stents, complications such as stent thrombosis and stent restenosis also emerged. These complications can be life-threatening in the form of post-procedural or late myocardial infarction and cardiac death. Thus, although the US Food and Drug Administration (FDA) assesses target-lesion failure (defined as a composite of cardiac death, target vessel myocardial infarction, or ischemia-driven target vessel revascularization) at 1 year, patients can have complications for the remainder of their lives. Despite the advancements attained by the second-generation DES over their predecessors, the issue of stent thrombosis and restenosis continues to plague second-generation DES with a 2% to 2.5% increased rate of target-lesion failure each year, seemingly forever (Figure 2).7,8
This article will briefly discuss the stent design and pathophysiology driving stent thrombosis and restenosis along with potential strategies to mitigate the problem. It pays special emphasis to bioresorbable stents, given their increasing interest among interventional cardiologists and patients, and given their potential to transform the practice of PCI.
STENT DESIGN
Contemporary DES essentially consist of three components:
A metallic alloy with a mesh-like design serves as the platform for the stent.
This framework is coated with a multi-layered polymer that holds and releases the active drug in a controlled manner so that its effects can be extended.
Figure 3. Components of drug-eluting and bioresorbable stents.An antiproliferative drug (absent in the bioresorbable stents) that inhibits the smooth muscle proliferation and neointimal hyperplastic response: sirolimus or paclitaxel in first-generation DES; everolimus or zotarolimus in second-generation DES (Figure 3).
WHAT CAUSES STENT THROMBOSIS AND RESTENOSIS?
Several theories and pathophysiological mechanisms have been proposed to explain these late adverse events (Table 1). However, our overall understanding of the cause remains modest at best. The major factor seems to be persistent presence of polymer on the stent and the ensuing inflammation. The second issue appears to be related to neoatherosclerosis that is generally defined as lipid or calcified neointima. Neoatherosclerosis is especially problematic for the second-generation DES. Neoatherosclerosis eventually predisposes to the development of thin cap fibroadenoma, and the rupture of thin cap leads to stent thrombosis and restenosis.
Autopsy studies suggest that approximately 50% of first- and second-generation DES start developing neoatherosclerosis within 1 to 3 years of implantation.9 Turbulence created by thick strutted stents or incomplete impaction of stents to the vessel wall predisposes the stents to platelet aggregation and fibrinogen deposition, thereby increasing the risk of neoatherosclerosis. Despite these pathologic insights, no treatment strategy has been shown to attenuate the problem, with the exception of high-dose statins.
CAN WE SOLVE THE PROBLEM?
Three technological approaches have been proposed to overcome stent thrombosis and restenosis:
Stents coated with bioresorbable polymers that quickly degrade
Stents without polymers
Stents that are completely resorbed.
STENTS WITH BIORESORBABLE POLYMERS
As described above, the presence of a polymer on the stent predisposes it to inflammation. Therefore, it would be logical to hypothesize that a bioresorbable polymer would reduce the inflammation. This approach is typified by the second-generation paclitaxel-eluting stent (Synergy, Boston Scientific). It has a biodegradable coating that resorbs within 4 months and releases everolimus in a dose intensity similar to that seen with the contemporary second-generation DES.
The largest trial of this device to date, the Evolve II study, randomly assigned 1,684 patients to the biostable-polymer, everolimus-eluting chromium stent (Promus, Boston Scientific) or the paclitaxel-eluting stent (Synergy, Boston Scientific).10 Two-year follow-up data suggest that the rate of target-lesion failure was 9.4% in the paclitaxel-eluting stent patients vs 8.5% in the everolimus-eluting stent patients. Notably, no definite stent thrombosis was seen in the Synergy-treated patients 24 hours after the initial device implantation.
STENTS WITHOUT POLYMERS
If polymers predispose to inflammation, stents without polymers should mitigate the risk. Such stent types are exemplified by the BioFreedom (Biosensors International) stainless steel stent, a polymer-free umirolimus (also known as biolimus A9)-eluting stent. These stents have a microstructured surface that holds the drug without a polymer and releases the active drug over a few months.
The LEADERS FREE clinical trial studied this stent in 2,466 patients at high risk of bleeding.11 The patients were randomized to receive either a BMS or the polymer-free stent. All patients were required to receive dual antiplatelet therapy for only 1 month. At 1 year, the composite risk of cardiac death, myocardial infarction, and stent thrombois was 9.4% in patients with BioFreedom stents vs 12.9% in BMS patients. Of note, the primary end point did not include stent restenosis, thereby not disadvantaging the BMS.
Medtronic’s polymer-free, sirolimus-eluting stent is currently under investigation in the RevElution clinical trial.12 It has a cylindrical structure with the core replaced by the active drug sirolimus. Abluminal holes in the stent allow controlled release of the drug. A pharmacokinetic analysis show that 90% of the medication is released within the first 90 days and that tissue concentrations are maintained in the therapeutic range until at least that time.13 This actually exceeds that of the second-generation everolimus-eluting DES.
BIORESORBABLE STENTS
Bioresorbable scaffolds or stents disappear entirely over time and have drawn considerable attention in the interventional cardiology community. The FDA recently approved Abbott’s Poly-L-Lactic Acid (PLLA) everolimus-eluting stent (Absorb). The rate of bioresorption of this device can be controlled by modulating the respective contribution of amorphous and crystalline PLLA backbone. The advantage of bioresorbable stents appears to stem from the fact that with bioresorbable devices, the vessel may actually expand and the purported nidus for inflammation goes away. This has been demonstrated by serial intravascular ultrasound-based studies.14
The return of pulsatility also appears to modulate the transition of smooth muscles from proliferative back to their contractile phenotype. This has been hypothesized to reduce the risk of neoatherosclerosis and, consequently, stent restenosis. The limitation of this device is the large strut size (157 micron for Absorb vs 81 microns for Xience). Dissolving metallic scaffolds also tend to have thicker struts than the current DES (120 vs approximately 80 microns).
The Absorb III trial was a pivotal noninferiority US trial that led to the device approval.15 In this trial, 2,008 patients were randomized to receive the Absorb bioresorbable, everolimus-eluting stent or the DES Xience. The primary study end point was target-lesion failure at 1 year. As is often the case with US landmark studies, patient and lesion complexities were limited. Patients with acute coronary syndrome, elevated cardiac enzymes, high-risk anatomic lesions such as bifurcation lesions, and chronic total occlusion were excluded. Patients with diabetes comprised less than one-third of the patients, and lesions were relatively short at 13 ± 6 mm.
Figure 4. ABSORB learnings: MICAT. Pre-dilation with noncompliant balloon sized 1:1 to normal vessel with complete balloon expansion; post-dilation at 14–16 atmospheres.
Device success per lesion was lower with Absorb than with Xience (94.3% vs 99.3%; P < .0001). This is likely due to the larger strut size. Absorb III did meet the prespecified primary end point for noninferiority (P = .007), although the rate of adverse events was somewhat higher (7.8% vs 6.1%). A subgroup analysis reveals that 19% of all lesions were smaller than what was originally intended, and in these patients, the Absorb device performed poorly with a 4.6% risk of device thrombosis. When limited to patients with the intended reference vessel sizes, the results of target-lesion failure and stent thrombosis were similar (6.6% vs 5.5% and 0.8% vs 0.5%, respectively).15
The implantation technique also seems to have influenced the results, with increased use of post-dilation as the study evolved. Recent observations from the MICAT group have shown that the use of high pressure post-dilation and other procedural advancements may considerably reduce adverse outcomes associated with Absorb (Figure 4).16 Thus, while the pooled analysis in the form of a meta-analysis has suggested an increased risk of device thrombosis,17 the difference is attenuated by selecting lesions of appropriate size, high-pressure post-dilation, and procedural advancements (Table 2).
CONCLUSION AND THE WAY FORWARD
Current first-generation bioresorbable stents can achieve results similar to those of second-generation DES, provided that they are used in patients with noncomplicated coronary lesions and the implant techniques are optimized. We do not know the outcomes of bioresorbable stents in patients with complex lesions. Current experience suggests that other changes in technique would be needed. For example, minimizing scaffold overlap in long and bifurcating lesions. Whether that would translate into diminishing the rate of late adverse events remains to be determined. As of now, we only have data on approximately 100 highly selected patients beyond 3 years (no adverse events 2.5 to 5 years after implantation).
Several investigational second-generation bioresorbable stents, including Elixir’s Dissolve PLLA, Boston Scientific’s FAST, and a newer version of Absorb, are in early clinical trials. Smaller strut thickness holds the promise of attenuating the risk of stent thrombosis. Since the polymer persists, no reduction in dual antiplatelet therapy duration is likely to be achieved.
Results from long-term follow-up of Absorb III and on-going trials are eagerly awaited to ascertain whether the rate of late complications of DES can be mitigated. It would not be surprising if the second-generation bioresorbable stents make DES a thing of the past within the next decade.
References
Palmerini T, Benedetto U, Biondi-Zoccai G, et al. Long-term safety of drug-eluting and bare-metal stents: evidence from a comprehensive network meta-analysis. J Am Coll Cardiol 2015; 65:2496–2507.
Bates ER. Balancing the evidence base on coronary stents. N Engl J Med 2016; 375:1286–1288.
Macaya C, Serruys PW, Ruygrok P, et al. Continued benefit of coronary stenting versus balloon angioplasty: one-year clinical follow-up of BENESTENT trial. BENESTENT Study Group. J Am Coll Cardiol 1996; 27:255–261.
Fajadet J, Wijns W, Laarman GJ; for the ENDEAVOR II Investigators. Randomized, double-blind, multicenter study of the Endeavor zotarolimus-eluting phosphorylcholine-encapsulated stent for treatment of native coronary artery lesions: clinical and angiographic results of the ENDEAVOR II trial. Circulation 2006; 114:798–806.
Kirtane AJ, Leon MB, Ball MW, et al; ENDEAVOR IV Investigators. The “final” 5-year follow-up from the ENDEAVOR IV trial comparing a zotarolimus-eluting stent with a paclitaxel-eluting stent. JACC Cardiovasc Interv 2013; 6:325–333.
Stone GW, Midei M, Newman W, et al; SPIRIT III Investigators. Comparison of an everolimus-eluting stent and a paclitaxel-eluting stent in patients with coronary artery disease: a randomized trial. JAMA 2008; 299:1903–1913.
Gada H, Kirtane AJ, Newman W, et al. 5-year results of a randomized comparison of XIENCE V everolimus-eluting and TAXUS paclitaxel-eluting stents: final results from the SPIRIT III trial (clinical evaluation of the XIENCE V everolimus eluting coronary stent system in the treatment of patients with de novo native coronary artery lesions). JACC Cardiovasc Interv 2013; 6:1263–1266.
Benedetto U, Raja SG, Soliman RFB, et al; on behalf of the Harefield Cardiac Outcomes Research Group. Minimally invasive direct coronary artery bypass improves late survival compared with drug-eluting stents in isolated proximal left anterior descending artery disease: a 10-year follow-up, single-center, propensity score analysis. J Thorac Cardiovasc Surg 2014; 148:1316–1322.
Virmani R, CV Path Institute. Problems encountered with drug-eluting stent. Presented at Transcatheter Cardiovascular Therapeutics (TCT); October 11–15, 2015; San Francisco, CA.
Kereiakes DJ, Meredith IT, Windecker S, et al. Efficacy and safety of a novel bioabsorbable polymer-coated, everolimus-eluting coronary stent: the EVOLVE II Randomized Trial. Circ Cardiovasc Interv 2015; 8:e002372.
Urban P, Meredith IT, Abizaid A, et al; for the LEADERS FREE Investigators. Polymer-free drug-coated coronary stents in patients at high bleeding risk. N Engl J Med 2015; 373:2038–2047.
Worthley SG, Abizaid A, Kirtane AJ, Simon D, Windecker S, Stone GW. Stent strut coverage and stent apposition after implantation of a novel drug-filled coronary stent: optical coherence tomography results from RevElution trial. J Am Coll Cardiol 2015; 66(suppl B):B235 [Abstract TCT-579].
Abizaid A, Costa RA, Schofer J, et al. Serial multimodality imaging and 2-year clinical outcomes of the novel DESolve novolimus-eluting bioresorbable coronary scaffold system for the treatment of single de novo coronary lesions. JACC Cardiovasc Interv 2016; 9:565–574.
Ellis SG, Kereiakes DJ, Metzger DC, et al; for the ABOSRB III Investigators. Everolimus-eluting bioresorbable scaffolds for coronary artery disease. N Engl J Med 2015; 373:1905–1915.
Puricel S, Cuculi F, Weissner M, et al. Bioresorbable coronary scaffold thrombosis: multicenter comprehensive analysis of clinical presentation, mechanisms, and predictors. J Am Coll Cardiol 2016; 67:921−931.
Stone GW, Gao R, Kimura T, et al. 1-year outcomes with the Absorb bioresorbable scaffold in patients with coronary artery disease: a patient-level, pooled meta-analysis. Lancet 2016; 387:1277–1289.
References
Palmerini T, Benedetto U, Biondi-Zoccai G, et al. Long-term safety of drug-eluting and bare-metal stents: evidence from a comprehensive network meta-analysis. J Am Coll Cardiol 2015; 65:2496–2507.
Bates ER. Balancing the evidence base on coronary stents. N Engl J Med 2016; 375:1286–1288.
Macaya C, Serruys PW, Ruygrok P, et al. Continued benefit of coronary stenting versus balloon angioplasty: one-year clinical follow-up of BENESTENT trial. BENESTENT Study Group. J Am Coll Cardiol 1996; 27:255–261.
Fajadet J, Wijns W, Laarman GJ; for the ENDEAVOR II Investigators. Randomized, double-blind, multicenter study of the Endeavor zotarolimus-eluting phosphorylcholine-encapsulated stent for treatment of native coronary artery lesions: clinical and angiographic results of the ENDEAVOR II trial. Circulation 2006; 114:798–806.
Kirtane AJ, Leon MB, Ball MW, et al; ENDEAVOR IV Investigators. The “final” 5-year follow-up from the ENDEAVOR IV trial comparing a zotarolimus-eluting stent with a paclitaxel-eluting stent. JACC Cardiovasc Interv 2013; 6:325–333.
Stone GW, Midei M, Newman W, et al; SPIRIT III Investigators. Comparison of an everolimus-eluting stent and a paclitaxel-eluting stent in patients with coronary artery disease: a randomized trial. JAMA 2008; 299:1903–1913.
Gada H, Kirtane AJ, Newman W, et al. 5-year results of a randomized comparison of XIENCE V everolimus-eluting and TAXUS paclitaxel-eluting stents: final results from the SPIRIT III trial (clinical evaluation of the XIENCE V everolimus eluting coronary stent system in the treatment of patients with de novo native coronary artery lesions). JACC Cardiovasc Interv 2013; 6:1263–1266.
Benedetto U, Raja SG, Soliman RFB, et al; on behalf of the Harefield Cardiac Outcomes Research Group. Minimally invasive direct coronary artery bypass improves late survival compared with drug-eluting stents in isolated proximal left anterior descending artery disease: a 10-year follow-up, single-center, propensity score analysis. J Thorac Cardiovasc Surg 2014; 148:1316–1322.
Virmani R, CV Path Institute. Problems encountered with drug-eluting stent. Presented at Transcatheter Cardiovascular Therapeutics (TCT); October 11–15, 2015; San Francisco, CA.
Kereiakes DJ, Meredith IT, Windecker S, et al. Efficacy and safety of a novel bioabsorbable polymer-coated, everolimus-eluting coronary stent: the EVOLVE II Randomized Trial. Circ Cardiovasc Interv 2015; 8:e002372.
Urban P, Meredith IT, Abizaid A, et al; for the LEADERS FREE Investigators. Polymer-free drug-coated coronary stents in patients at high bleeding risk. N Engl J Med 2015; 373:2038–2047.
Worthley SG, Abizaid A, Kirtane AJ, Simon D, Windecker S, Stone GW. Stent strut coverage and stent apposition after implantation of a novel drug-filled coronary stent: optical coherence tomography results from RevElution trial. J Am Coll Cardiol 2015; 66(suppl B):B235 [Abstract TCT-579].
Abizaid A, Costa RA, Schofer J, et al. Serial multimodality imaging and 2-year clinical outcomes of the novel DESolve novolimus-eluting bioresorbable coronary scaffold system for the treatment of single de novo coronary lesions. JACC Cardiovasc Interv 2016; 9:565–574.
Ellis SG, Kereiakes DJ, Metzger DC, et al; for the ABOSRB III Investigators. Everolimus-eluting bioresorbable scaffolds for coronary artery disease. N Engl J Med 2015; 373:1905–1915.
Puricel S, Cuculi F, Weissner M, et al. Bioresorbable coronary scaffold thrombosis: multicenter comprehensive analysis of clinical presentation, mechanisms, and predictors. J Am Coll Cardiol 2016; 67:921−931.
Stone GW, Gao R, Kimura T, et al. 1-year outcomes with the Absorb bioresorbable scaffold in patients with coronary artery disease: a patient-level, pooled meta-analysis. Lancet 2016; 387:1277–1289.
Bioresorbable stents: The future of interventional cardiology?
Display Headline
Bioresorbable stents: The future of interventional cardiology?
Legacy Keywords
stents, percutaneous coronary intervention, PCI, bare metal stent, BMS, drug-eluting stents, DES, thrombosis, everolimus, Promus, paclitaxel, Synergy, Boston Scientific, Medtronic, BioFreedom, Biosensors International, sirolimus, Stephen Ellis, Haris Riaz
Legacy Keywords
stents, percutaneous coronary intervention, PCI, bare metal stent, BMS, drug-eluting stents, DES, thrombosis, everolimus, Promus, paclitaxel, Synergy, Boston Scientific, Medtronic, BioFreedom, Biosensors International, sirolimus, Stephen Ellis, Haris Riaz
Citation Override
Cleveland Clinic Journal of Medicine 2016 November; 83(suppl 2):S18-S23
Inside the Article
KEY POINTS
Stents have dramatically improved outcomes associated with percutaneous coronary angioplasty.
Bare-metal stents were the first stents developed, followed by first- and second-generation drug-eluting stents, which have progressively reduced complication rates.
Despite the improvements with conventional stents, persistent rates of restenosis and stent thrombosis remain, which can lead to increased coronary morbidity and mortality.
New stent technologies include stents coated with bioresorbable polymers, stents without polymers, and completely bioresorbable stents.
Disallow All Ads
Alternative CME
Consolidated Pubs: Do Not Show Source Publication Logo
Mark G. Rabbat, MD Department of Internal Medicine, Cleveland Clinic
Anthony A. Bavry, MD, MPH Department of Cardiovascular Medicine, Cleveland Clinic
Deepak L. Bhatt, MD Associate Professor of Medicine, Cleveland Clinic Lerner College of Medicine; Associate Director, Cleveland Clinic Cardiovascular Coordinating Center; Staff, Cardiac, Peripheral, and Carotid Intervention, Department of Cardiovascular Medicine, Cleveland Clinic
Stephen G. Ellis, MD Professor of Medicine, Cleveland Clinic Lerner College of Medicine; Head, Section of Invasive Cardiology, Department of Cardiovascular Medicine, Cleveland Clinic
Address: Stephen G. Ellis, MD, Department of Cardiovascular Medicine, F25, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: elliss@ccf.org
Dr. Bavry has received honoraria from Genesis.
Dr. Bhatt has served as a consultant to AstraZeneca, Bristol-Myers Squibb, Centocor, Daiichi-Sankyo, Eisai, Eli Lilly, GlaxoSmithKline, Millennium, Paringenix, PDL, Sanofi-Aventis, Schering-Plough, and The Medicines Company.
Dr. Ellis has served as a consultant to Cordis, Boston Scientific, and Abbott, and receives research support from Cordis and Medtronic.
Mark G. Rabbat, MD Department of Internal Medicine, Cleveland Clinic
Anthony A. Bavry, MD, MPH Department of Cardiovascular Medicine, Cleveland Clinic
Deepak L. Bhatt, MD Associate Professor of Medicine, Cleveland Clinic Lerner College of Medicine; Associate Director, Cleveland Clinic Cardiovascular Coordinating Center; Staff, Cardiac, Peripheral, and Carotid Intervention, Department of Cardiovascular Medicine, Cleveland Clinic
Stephen G. Ellis, MD Professor of Medicine, Cleveland Clinic Lerner College of Medicine; Head, Section of Invasive Cardiology, Department of Cardiovascular Medicine, Cleveland Clinic
Address: Stephen G. Ellis, MD, Department of Cardiovascular Medicine, F25, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: elliss@ccf.org
Dr. Bavry has received honoraria from Genesis.
Dr. Bhatt has served as a consultant to AstraZeneca, Bristol-Myers Squibb, Centocor, Daiichi-Sankyo, Eisai, Eli Lilly, GlaxoSmithKline, Millennium, Paringenix, PDL, Sanofi-Aventis, Schering-Plough, and The Medicines Company.
Dr. Ellis has served as a consultant to Cordis, Boston Scientific, and Abbott, and receives research support from Cordis and Medtronic.
Author and Disclosure Information
Mark G. Rabbat, MD Department of Internal Medicine, Cleveland Clinic
Anthony A. Bavry, MD, MPH Department of Cardiovascular Medicine, Cleveland Clinic
Deepak L. Bhatt, MD Associate Professor of Medicine, Cleveland Clinic Lerner College of Medicine; Associate Director, Cleveland Clinic Cardiovascular Coordinating Center; Staff, Cardiac, Peripheral, and Carotid Intervention, Department of Cardiovascular Medicine, Cleveland Clinic
Stephen G. Ellis, MD Professor of Medicine, Cleveland Clinic Lerner College of Medicine; Head, Section of Invasive Cardiology, Department of Cardiovascular Medicine, Cleveland Clinic
Address: Stephen G. Ellis, MD, Department of Cardiovascular Medicine, F25, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: elliss@ccf.org
Dr. Bavry has received honoraria from Genesis.
Dr. Bhatt has served as a consultant to AstraZeneca, Bristol-Myers Squibb, Centocor, Daiichi-Sankyo, Eisai, Eli Lilly, GlaxoSmithKline, Millennium, Paringenix, PDL, Sanofi-Aventis, Schering-Plough, and The Medicines Company.
Dr. Ellis has served as a consultant to Cordis, Boston Scientific, and Abbott, and receives research support from Cordis and Medtronic.
Cameron Haery, MD Department of Cardiovascular Medicine, The Cleveland Clinic Foundation
Ravish Sachar, MD Department of Cardiovascular Medicine, The Cleveland Clinic Foundation
Stephen G. Ellis, MD Director, Sones Catheterization Laboratories, Department of Cardiovascular Medicine, The Cleveland Clinic Foundation
Address: Stephen G. Ellis, MD, Director, Sones Catheterization Laboratories, F25, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail elliss@ccf.org
Dr. Ellis has indicated that he has received grant or research support from the Cordis and Medtronic corporations and serves as a consultant for the Cordis, Boston Scientific, and Guidant corporations.
This paper discusses therapies that are experimental or that are not approved by the US Food and Drug Administration for the use under discussion.
Cameron Haery, MD Department of Cardiovascular Medicine, The Cleveland Clinic Foundation
Ravish Sachar, MD Department of Cardiovascular Medicine, The Cleveland Clinic Foundation
Stephen G. Ellis, MD Director, Sones Catheterization Laboratories, Department of Cardiovascular Medicine, The Cleveland Clinic Foundation
Address: Stephen G. Ellis, MD, Director, Sones Catheterization Laboratories, F25, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail elliss@ccf.org
Dr. Ellis has indicated that he has received grant or research support from the Cordis and Medtronic corporations and serves as a consultant for the Cordis, Boston Scientific, and Guidant corporations.
This paper discusses therapies that are experimental or that are not approved by the US Food and Drug Administration for the use under discussion.
Author and Disclosure Information
Cameron Haery, MD Department of Cardiovascular Medicine, The Cleveland Clinic Foundation
Ravish Sachar, MD Department of Cardiovascular Medicine, The Cleveland Clinic Foundation
Stephen G. Ellis, MD Director, Sones Catheterization Laboratories, Department of Cardiovascular Medicine, The Cleveland Clinic Foundation
Address: Stephen G. Ellis, MD, Director, Sones Catheterization Laboratories, F25, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail elliss@ccf.org
Dr. Ellis has indicated that he has received grant or research support from the Cordis and Medtronic corporations and serves as a consultant for the Cordis, Boston Scientific, and Guidant corporations.
This paper discusses therapies that are experimental or that are not approved by the US Food and Drug Administration for the use under discussion.