User login
Treating psychiatric reactions to medical illness
Mrs. M, 35, is undergoing breast cancer treatment. She is referred to the consultation-liaison service by an emergency room physician for evaluation of suicidal thoughts.
Mrs. M has been crying for 2 hours. She awoke this morning feeling that she could no longer deal with “the unknown.” She has lost her hair and 30 pounds during chemotherapy and hardly recognized herself in the bathroom mirror. She thought about killing herself until one of her children walked by. After they went to school, she drove to the emergency room.
When you ask if she has had other thoughts of hurting herself, she says, “I would never do anything like that to my family, but the fact that I was thinking about it really scared me.”
Each patient responds uniquely to the emotional trauma of having a chronic or life-threatening medical illness. Coping styles depend on medical, psychological, and social factors as well as the person’s personality and experiences. Reactions range from mature to psychotic.
To help you guide patients such as Mrs. M through difficult medical treatments and decisions, we describe:
- a psychiatric workup to identify maladaptive response to illness
- typical emotional and behavioral responses to chronic illness
- how to provide psychotherapy tailored to the needs of 7 personality styles of medically ill patients.
Psychiatric Workup
Mrs. M is married with 3 sons. She found a lump on her breast 4 months ago but decided to wait “because, I thought, ‘it can’t be anything bad; it will go away.’” When the lump remained 3 months later, she consulted a specialist who diagnosed breast cancer.
Mrs. M underwent a lumpectomy and has been receiving weekly chemotherapy. Besides losing her hair, she says she has no appetite. Looking at food or driving close to the hospital makes her nauseous. She starts vomiting before she arrives for chemotherapy.
Though her family supports and encourages her, she can’t stop thinking about death. She feels isolated, lonely, and cries often. “No one understands what I am going through,” she says. “How can I share these feelings with them?”
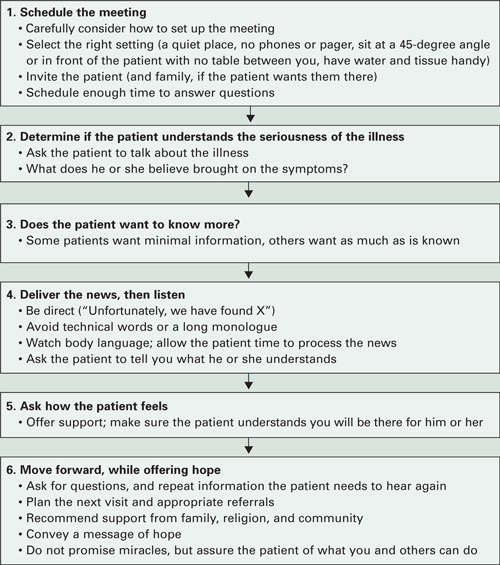
Physicians such as the specialist who diagnosed Mrs. M’s cancer often must communicate difficult information. Careful planning when delivering bad news (Box 1)1,2 can set the stage for a healthier emotional and behavioral response.
Chronic illness causes depression in up to 25% of patients.3 At particular risk of developing depressive symptoms are patients with:
- poor physical condition
- poorly controlled pain
- advanced illness
- history of major depressive disorder
- family history of depression and suicide
- certain cancers, such as of the pancreas, lung, head or neck.4
Mechanisms of depression in illness. Depression can be the first symptom of some medical illnesses, such as pancreatic or liver cancer. Diseases that directly affect the brain—such as Parkinson’s disease, multiple sclerosis, and systemic lupus erythematosus—can cause depression. Patients disabled by spinal cord injury, stroke, or cancer also are at risk for depression.
Treatment is the same, whether illness-related chemical changes or the patient’s emotional response to disability is causing the depression. When diagnosing depression in medically ill patients, DSM-IV-TR recommends using criteria for major depression and providing treatment, whatever the cause.
Mrs. M has trouble sharing feelings of hopelessness with her family. Her changes in demeanor and isolation from everyday activities are clues to clinical depression and anxiety.
Depression can be difficult to diagnose when medical illness causes depression-like symptoms.5 To make the diagnosis, ask patients with chronic illness about depression’s emotional symptoms (hopelessness, withdrawal from others, sadness, ruminating thoughts, frequent crying spells), rather than its physical symptoms of poor eating, disturbed sleep, or low energy that may stem from the medical illness. Patients might not be as hard on themselves if they feel the medical illness—not poor coping on their part—caused their depression.
Box 1 6 steps for delivering bad medical news
Source: Adapted from references 1, 2Workup. Our workup of Mrs. M includes thyroid function tests, CBC, comprehensive metabolic panel, and brain MRI to rule out metastasis. All are negative. In her history, Mrs. M reports a previous episode of major depression 5 years ago that was successfully treated with sertraline for 1 year.
Consistent with her workup and symptoms, we diagnose major depression without psychosis. Cancer patients who report hopelessness are at increased risk of suicide. Because of her family support and religious beliefs, however, we feel she can safely go home and return for follow-up the next week.
Emotional response to illness
Mrs. M starts weekly outpatient appointments at our clinic. Because sertraline has worked for her in the past, it is our first choice to increase her energy, improve her mood, and decrease her hopelessness. Initial dosage is 25 mg/d for the first 3 days, with an increase to 50 mg/d for 1 month, and 100 mg/d thereafter. She reports no side effects.
In some patients, sertraline can cause adverse gastrointestinal effects such as upset stomach or nausea. Other antidepressants such as mirtazapine could improve patients’ sleep and decrease nausea.
Mrs. M also begins cognitive-behavioral therapy (CBT) to help her deal with negative thoughts, and relaxation training to combat her anxiety before chemotherapy. We recommend a local breast cancer support group, and Mrs. M starts going twice a month. She feels relieved that other patients are experiencing feelings similar to hers.
Medication plus CBT has been shown to be the most effective treatment for patients who meet criteria for depression and anxiety disorders. CBT has been shown to help patients manage physical symptoms and reframe negative thoughts associated with many chronic illnesses, including breast cancer, Parkinson’s disease, epilepsy, rheumatoid arthritis, and multiple sclerosis.6-10
Core emotions. Medically ill patients experience a range of core emotions, which Lazarus11 identified as anger, anxiety, guilt, fright, shame, sadness, happiness, envy, relief, and hope. Identifying the source of these emotions is important to counseling patients effectively.
For example, a patient experiencing fright might fear death, pain, disability, stigma, disfigurement, or other eventualities. Mrs. M has said she can’t stop thinking about dying. By knowing what the patient fears (Table 1),12 we can more effectively reassure and offer support, even when little else can be done.
Table 1
Common fears of patients reacting to diagnosis of chronic illness
|
| Source: Reference 12 |
Defensive behaviors. Patient’s behavioral responses may be adaptive or maladaptive; treatment nonadherence is one maladaptive response (Box 2).13,14 The patient history can suggest how well a person has adapted to past losses and disappointments. Patients may try to protect themselves against emotional and physical pain with psychotic, immature, neurotic, or mature defense mechanisms.15
Psychotic defenses are characterized by regression until patients lose touch with reality. Delusions and fantasy isolate them from the harshness of a serious medical condition. Antipsychotic medication and patience are often indicated.16
Immature defenses—as seen in patients with borderline personality disorder—can irritate and alienate the medical team. Physicians may not understand why their best efforts are thwarted or negated. Well-intentioned, caring doctors often try harder when the verbal attacks begin, but soon even the hardiest can wither under the patient’s criticism and threats.
Depressed medically ill patients adhere poorly to treatment schedules and other recommendations, which may cut their chances of survival.13 Up to 2% of hospital discharges are initiated by patients against medical advice.
Causes of refusing or discontinuing treatment may include anger towards the medical team or caregiver,14 anxiety, or withdrawal from addictive substances. Some patients who sign themselves out may be psychotic or confused by delirium or dementia. Others may be in denial of their illness.
Untreated psychiatric disorders can cause illness-specific nonadherence. Patients with:
- depression might not have the energy or motivation to follow the treatment.
- bipolar disorder might feel they don’t need the treatment.
- psychotic disorders may feel threatened by the treatment or the doctor.
Psychiatric patients may avoid taking medications prescribed for medical illness if they fear side effects or interactions with their psychotropics. Some don’t tell their medical practitioners about their psychiatric diagnoses because of the stigma associated with mental illness.
Psychiatrists can counsel the medical team to:
- pull back and focus on setting treatment objectives
- encourage the patient to work as a team member to ensure the best possible care
- communicate with the patient and care team to prevent divisions among the staff.
Neurotic defenses are in play when patients blame themselves and suffer internally. Give them ample opportunities to explore their feelings.
Mature defenses are seen in those who show concern for others, may express humor, and can adaptively plan, thus gaining the respect of others. Spirituality and optimism allow them to feel more at peace and less controlled by the illness.
Support these patients by encouraging their coping skills. For example, if spirituality has helped before, it may again strengthen them and their families.
Improving coping skills. By recognizing which patients are struggling, you can provide support to strengthen their coping abilities. Initially, Mrs. M was using neurotic defense mechanisms and internalizing her emotions. With the help of CBT, she begins to rely on more mature defenses. Her improved coping skills allow her to share her feelings during group therapy and with her family.
Encouraging adaptive behavior
Mrs. M is in remission when chemotherapy ends, but she worries that the cancer will come back. “The fear is still there,” she says. “You can’t be called a survivor for 5 years.”
She continues biweekly psychotherapy for the next year, and sertraline, 100 mg/d. She is doing well and has volunteered to help other newly-diagnosed patients at the cancer center.
Personality styles. Kahana and Bibring17 described 7 personality types that affect how patients cope with illnesses. Based on our experience, we suggest how to observe these styles, identify the emotional pain behind them, and respond in ways that will help each type of patient (Table 2).17
These personality types are not necessarily personality disorders; rather, they describe pervasive characteristics of coping styles. Some individuals will not match the descriptions of any of these types, and others may fall into more than one. Mrs. M, for example, shows traits of more than one personality style, including avoidant and mild schizoid features.
We helped her by engaging her in psychiatric treatment, helping her better understand her medical situation, and restoring her sense of control in making medical decisions. We discussed psycho-therapy as a two-way street, outlining her responsibilities to practice new CBT skills to use during treatment and in remission.
Table 2
Recommended treatment approaches for 7 patient personalities
| Personality | Patients who… | Often feel… | Are helped by… |
|---|---|---|---|
| Dependent | ask many questions, making it hard for you to end conversations or leave the room | afraid you won’t find them worthy, won’t want to care for them | regular, brief sessions (set tactful limits that will reassure patient and not annoy staff) |
| Obsessive | are insistent, detail-oriented | angry when they can’t control their illness, the staff, and the schedule | detailed explanations (provide choices whenever possible, try to use patient input collaboratively) |
| Narcissistic | are self-centered, criticize others, believe no one is qualified to care for them | fearful, threatened, and vulnerable | avoiding confrontation but emphasizing that they deserve the best care staff can provide (keep patient informed; be sure all staff provides the same message) |
| Suffering victim | always have symptoms and request much attention; might not follow recommendations | suffering is their role; views illness and its treatments as punishment, but hopes doctor will keep trying | regular visits, no matter how variable the complaints |
| Paranoid | do not trust doctors, refuse to participate in treatment plans or sign out | taken advantage of by others or purposefully neglected or harmed | staying calm (don’t argue; offer understanding of patient’s position, provide clear recommendations |
| Histrionic | are flirtatious, want to call doctors by first names | need to be ‘special’ to the physician; fear illness will invalidate them or make them unattractive | encouraging patient to verbalize concerns (set boundaries for relationship; remain courteous and objective) |
| Schizoid | are very lonely, tend to avoid medical care | doctors are invading their privacy | engaging patient in making medical decisions |
| Source: Adapted from reference 17 | |||
Supportive therapy. Encourage patients to seek support from family and friends.18 Some benefit from meeting other patients with the same needs, fears, and questions.19 The Internet is a good resource to find local support groups.
Becoming sick or disabled and having to change one’s lifestyle can damage a person’s self esteem. Encourage patients to help others by volunteering, participating in research, or engaging in other activities that provide hope, gratification, and a sense of service.20
Some patients regain control and battle their fears by becoming experts on their diseases. This approach will not help those who become anxious learning about prognosis and side effects, however, and prefer to have limited information about their illnesses. Your knowledge of a patient’s personality type can help you determine whether added information might alleviate or worsen that patient’s stress.
Personal transformation can occur when patients face mortality. Their perceptions about what is important and how to achieve their goals can change dramatically.
Related resources
- National Cancer Institute. Coping with cancer. www.cancer.gov/cancertopics/coping.
- American Psychiatric Association. Patient education site with links to topics such as coping with AIDS/HIV, postpartum depression, alcohol abuse, mental health of the elderly, and common childhood disorders. www.healthyminds.org.
- Groves M, Muskin P. Psychological responses to illness. In: Bourgeois JA, Hales RE, Shahrokh N (eds). Textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:68-88.
Drug brand names
- Mirtazapine • Remeron
- Sertraline • Zoloft
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Bailey W, Buckman R, Lenzi R, et al. SPIKES - a six-step protocol for delivering bad news; application to the patient with cancer. Oncologist 2000;5:4,302-11.
2. Koenig HG, Larson DB, Larson SS. Religion and coping with serious medical illness. Ann Pharmacother 2001;35(3):352-9.
3. Faller H, Schmidt M. Prognostic value of depressive coping and depression in survival of lung cancer patients. Psychooncology 2004;13(5):359-63.
4. Holland JC. Psychological care of patients: psycho-oncology’s contribution. J Clin Oncol 2003;21(23 suppl):253s-265s.
5. Lovejoy NC, Tabor D, Matteis M, Lillis P. Cancer-related depression: Part I. Neurologic alterations and cognitive-behavioral therapy. Oncol Nurs Forum 2000;27(4):667-78.
6. Cole K, Vaughan FL. The feasibility of using cognitive behaviour therapy for depression associated with Parkinson’s disease: a literature review. Parkinsonism Relat Disord 2005;11(5):269-76
7. Goldstein LH, McAlpine M, Deale A, et al. Cognitive behaviour therapy with adults with intractable epilepsy and psychiatric co-morbidity: preliminary observations on changes in psychological state and seizure frequency. Behav Res Ther 2003;41(4):447-60.
8. Evers AW, Kraaimaat FW, van Riel PL, de Jong AJ. Tailored cognitive-behavioral therapy in early rheumatoid arthritis for patients at risk: a randomized controlled trial. Pain 2002;100(1-2):141-53.
9. Mohr DC, Likosky W, Bertagnolli A, et al. Telephone-administered cognitive-behavioral therapy for the treatment of depressive symptoms in multiple sclerosis. J Consult Clin Psychol 2000;68(2):356-61.
10. Tatrow K. Montgomery GH. Cognitive behavioral therapy techniques for distress and pain in breast cancer patients: a meta-analysis. J Behav Med 2006;29(1):17-27.
11. Lazarus RS, Folkman S. Stress, appraisal and coping. New York: Springer, 1984.
12. Gazzola L, Muskin PR. The impact of stress and the objective of psychosocial interventions. In: Schein LA, Bernard HS, Spitz HI, Muskin PR (eds). Psychosocial treatment for medical conditions: principles and techniques. New York: Brunner-Routledge; 2003: 373-406.
13. Uitterhoeve RJ, Vernooy M, Litjens M, et al. Psychosocial interventions for patients with advanced cancer - a systematic review of the literature. Br J Cancer 2004;91(6):1050-62.
14. Perry S, Viederman M. Management of emotional reactions to acute medical illness. Med Clin North Am 1981;65:3-14.
15. Gabbard G. Major modalities: psychoanalytic/psychodynamic. In: Gabbard G, Beck J, Holmes J, eds. Oxford textbook of psychotherapy. New York: Oxford University Press; 2005:3-13.
16. Groves M, Muskin P. Psychological responses to illness In: Bourgeois JA, Hales RE, Shahrokh N (eds). Textbook of psychosomatic medicine Washington, DC: American Psychiatric Publishing; 2005:68-88.
17. Kahana RJ, Bibring G. Personality types in medical management. In: Zinberg NE (ed). Psychiatry and medical practice in a general hospital. New York: International Universities Press, 1964:108-23.
18. Johnson KS, Elbert-Avila KI, Tulsky JA. The influence of spiritual beliefs and practices on the treatment p of African Americans: a review of the literature. J Am Geriatr Soc 2005;53(4):711-19.
19. Vos PJ, Visser AP, Garssen B, et al. Effects of delayed psychosocial interventions versus early psychosocial interventions for women with early stage breast cancer. Patient Educ Couns 2006;60(2):212-9
20. Breitbart W, Gibson C, Poppito SR, Berg A. Psychotherapeutic interventions at the end of life: a focus on meaning and spirituality. Can J Psychiatry 2004;49(6):366-72.
Mrs. M, 35, is undergoing breast cancer treatment. She is referred to the consultation-liaison service by an emergency room physician for evaluation of suicidal thoughts.
Mrs. M has been crying for 2 hours. She awoke this morning feeling that she could no longer deal with “the unknown.” She has lost her hair and 30 pounds during chemotherapy and hardly recognized herself in the bathroom mirror. She thought about killing herself until one of her children walked by. After they went to school, she drove to the emergency room.
When you ask if she has had other thoughts of hurting herself, she says, “I would never do anything like that to my family, but the fact that I was thinking about it really scared me.”
Each patient responds uniquely to the emotional trauma of having a chronic or life-threatening medical illness. Coping styles depend on medical, psychological, and social factors as well as the person’s personality and experiences. Reactions range from mature to psychotic.
To help you guide patients such as Mrs. M through difficult medical treatments and decisions, we describe:
- a psychiatric workup to identify maladaptive response to illness
- typical emotional and behavioral responses to chronic illness
- how to provide psychotherapy tailored to the needs of 7 personality styles of medically ill patients.
Psychiatric Workup
Mrs. M is married with 3 sons. She found a lump on her breast 4 months ago but decided to wait “because, I thought, ‘it can’t be anything bad; it will go away.’” When the lump remained 3 months later, she consulted a specialist who diagnosed breast cancer.
Mrs. M underwent a lumpectomy and has been receiving weekly chemotherapy. Besides losing her hair, she says she has no appetite. Looking at food or driving close to the hospital makes her nauseous. She starts vomiting before she arrives for chemotherapy.
Though her family supports and encourages her, she can’t stop thinking about death. She feels isolated, lonely, and cries often. “No one understands what I am going through,” she says. “How can I share these feelings with them?”
Physicians such as the specialist who diagnosed Mrs. M’s cancer often must communicate difficult information. Careful planning when delivering bad news (Box 1)1,2 can set the stage for a healthier emotional and behavioral response.
Chronic illness causes depression in up to 25% of patients.3 At particular risk of developing depressive symptoms are patients with:
- poor physical condition
- poorly controlled pain
- advanced illness
- history of major depressive disorder
- family history of depression and suicide
- certain cancers, such as of the pancreas, lung, head or neck.4
Mechanisms of depression in illness. Depression can be the first symptom of some medical illnesses, such as pancreatic or liver cancer. Diseases that directly affect the brain—such as Parkinson’s disease, multiple sclerosis, and systemic lupus erythematosus—can cause depression. Patients disabled by spinal cord injury, stroke, or cancer also are at risk for depression.
Treatment is the same, whether illness-related chemical changes or the patient’s emotional response to disability is causing the depression. When diagnosing depression in medically ill patients, DSM-IV-TR recommends using criteria for major depression and providing treatment, whatever the cause.
Mrs. M has trouble sharing feelings of hopelessness with her family. Her changes in demeanor and isolation from everyday activities are clues to clinical depression and anxiety.
Depression can be difficult to diagnose when medical illness causes depression-like symptoms.5 To make the diagnosis, ask patients with chronic illness about depression’s emotional symptoms (hopelessness, withdrawal from others, sadness, ruminating thoughts, frequent crying spells), rather than its physical symptoms of poor eating, disturbed sleep, or low energy that may stem from the medical illness. Patients might not be as hard on themselves if they feel the medical illness—not poor coping on their part—caused their depression.
Box 1 6 steps for delivering bad medical news
Source: Adapted from references 1, 2Workup. Our workup of Mrs. M includes thyroid function tests, CBC, comprehensive metabolic panel, and brain MRI to rule out metastasis. All are negative. In her history, Mrs. M reports a previous episode of major depression 5 years ago that was successfully treated with sertraline for 1 year.
Consistent with her workup and symptoms, we diagnose major depression without psychosis. Cancer patients who report hopelessness are at increased risk of suicide. Because of her family support and religious beliefs, however, we feel she can safely go home and return for follow-up the next week.
Emotional response to illness
Mrs. M starts weekly outpatient appointments at our clinic. Because sertraline has worked for her in the past, it is our first choice to increase her energy, improve her mood, and decrease her hopelessness. Initial dosage is 25 mg/d for the first 3 days, with an increase to 50 mg/d for 1 month, and 100 mg/d thereafter. She reports no side effects.
In some patients, sertraline can cause adverse gastrointestinal effects such as upset stomach or nausea. Other antidepressants such as mirtazapine could improve patients’ sleep and decrease nausea.
Mrs. M also begins cognitive-behavioral therapy (CBT) to help her deal with negative thoughts, and relaxation training to combat her anxiety before chemotherapy. We recommend a local breast cancer support group, and Mrs. M starts going twice a month. She feels relieved that other patients are experiencing feelings similar to hers.
Medication plus CBT has been shown to be the most effective treatment for patients who meet criteria for depression and anxiety disorders. CBT has been shown to help patients manage physical symptoms and reframe negative thoughts associated with many chronic illnesses, including breast cancer, Parkinson’s disease, epilepsy, rheumatoid arthritis, and multiple sclerosis.6-10
Core emotions. Medically ill patients experience a range of core emotions, which Lazarus11 identified as anger, anxiety, guilt, fright, shame, sadness, happiness, envy, relief, and hope. Identifying the source of these emotions is important to counseling patients effectively.
For example, a patient experiencing fright might fear death, pain, disability, stigma, disfigurement, or other eventualities. Mrs. M has said she can’t stop thinking about dying. By knowing what the patient fears (Table 1),12 we can more effectively reassure and offer support, even when little else can be done.
Table 1
Common fears of patients reacting to diagnosis of chronic illness
|
| Source: Reference 12 |
Defensive behaviors. Patient’s behavioral responses may be adaptive or maladaptive; treatment nonadherence is one maladaptive response (Box 2).13,14 The patient history can suggest how well a person has adapted to past losses and disappointments. Patients may try to protect themselves against emotional and physical pain with psychotic, immature, neurotic, or mature defense mechanisms.15
Psychotic defenses are characterized by regression until patients lose touch with reality. Delusions and fantasy isolate them from the harshness of a serious medical condition. Antipsychotic medication and patience are often indicated.16
Immature defenses—as seen in patients with borderline personality disorder—can irritate and alienate the medical team. Physicians may not understand why their best efforts are thwarted or negated. Well-intentioned, caring doctors often try harder when the verbal attacks begin, but soon even the hardiest can wither under the patient’s criticism and threats.
Depressed medically ill patients adhere poorly to treatment schedules and other recommendations, which may cut their chances of survival.13 Up to 2% of hospital discharges are initiated by patients against medical advice.
Causes of refusing or discontinuing treatment may include anger towards the medical team or caregiver,14 anxiety, or withdrawal from addictive substances. Some patients who sign themselves out may be psychotic or confused by delirium or dementia. Others may be in denial of their illness.
Untreated psychiatric disorders can cause illness-specific nonadherence. Patients with:
- depression might not have the energy or motivation to follow the treatment.
- bipolar disorder might feel they don’t need the treatment.
- psychotic disorders may feel threatened by the treatment or the doctor.
Psychiatric patients may avoid taking medications prescribed for medical illness if they fear side effects or interactions with their psychotropics. Some don’t tell their medical practitioners about their psychiatric diagnoses because of the stigma associated with mental illness.
Psychiatrists can counsel the medical team to:
- pull back and focus on setting treatment objectives
- encourage the patient to work as a team member to ensure the best possible care
- communicate with the patient and care team to prevent divisions among the staff.
Neurotic defenses are in play when patients blame themselves and suffer internally. Give them ample opportunities to explore their feelings.
Mature defenses are seen in those who show concern for others, may express humor, and can adaptively plan, thus gaining the respect of others. Spirituality and optimism allow them to feel more at peace and less controlled by the illness.
Support these patients by encouraging their coping skills. For example, if spirituality has helped before, it may again strengthen them and their families.
Improving coping skills. By recognizing which patients are struggling, you can provide support to strengthen their coping abilities. Initially, Mrs. M was using neurotic defense mechanisms and internalizing her emotions. With the help of CBT, she begins to rely on more mature defenses. Her improved coping skills allow her to share her feelings during group therapy and with her family.
Encouraging adaptive behavior
Mrs. M is in remission when chemotherapy ends, but she worries that the cancer will come back. “The fear is still there,” she says. “You can’t be called a survivor for 5 years.”
She continues biweekly psychotherapy for the next year, and sertraline, 100 mg/d. She is doing well and has volunteered to help other newly-diagnosed patients at the cancer center.
Personality styles. Kahana and Bibring17 described 7 personality types that affect how patients cope with illnesses. Based on our experience, we suggest how to observe these styles, identify the emotional pain behind them, and respond in ways that will help each type of patient (Table 2).17
These personality types are not necessarily personality disorders; rather, they describe pervasive characteristics of coping styles. Some individuals will not match the descriptions of any of these types, and others may fall into more than one. Mrs. M, for example, shows traits of more than one personality style, including avoidant and mild schizoid features.
We helped her by engaging her in psychiatric treatment, helping her better understand her medical situation, and restoring her sense of control in making medical decisions. We discussed psycho-therapy as a two-way street, outlining her responsibilities to practice new CBT skills to use during treatment and in remission.
Table 2
Recommended treatment approaches for 7 patient personalities
| Personality | Patients who… | Often feel… | Are helped by… |
|---|---|---|---|
| Dependent | ask many questions, making it hard for you to end conversations or leave the room | afraid you won’t find them worthy, won’t want to care for them | regular, brief sessions (set tactful limits that will reassure patient and not annoy staff) |
| Obsessive | are insistent, detail-oriented | angry when they can’t control their illness, the staff, and the schedule | detailed explanations (provide choices whenever possible, try to use patient input collaboratively) |
| Narcissistic | are self-centered, criticize others, believe no one is qualified to care for them | fearful, threatened, and vulnerable | avoiding confrontation but emphasizing that they deserve the best care staff can provide (keep patient informed; be sure all staff provides the same message) |
| Suffering victim | always have symptoms and request much attention; might not follow recommendations | suffering is their role; views illness and its treatments as punishment, but hopes doctor will keep trying | regular visits, no matter how variable the complaints |
| Paranoid | do not trust doctors, refuse to participate in treatment plans or sign out | taken advantage of by others or purposefully neglected or harmed | staying calm (don’t argue; offer understanding of patient’s position, provide clear recommendations |
| Histrionic | are flirtatious, want to call doctors by first names | need to be ‘special’ to the physician; fear illness will invalidate them or make them unattractive | encouraging patient to verbalize concerns (set boundaries for relationship; remain courteous and objective) |
| Schizoid | are very lonely, tend to avoid medical care | doctors are invading their privacy | engaging patient in making medical decisions |
| Source: Adapted from reference 17 | |||
Supportive therapy. Encourage patients to seek support from family and friends.18 Some benefit from meeting other patients with the same needs, fears, and questions.19 The Internet is a good resource to find local support groups.
Becoming sick or disabled and having to change one’s lifestyle can damage a person’s self esteem. Encourage patients to help others by volunteering, participating in research, or engaging in other activities that provide hope, gratification, and a sense of service.20
Some patients regain control and battle their fears by becoming experts on their diseases. This approach will not help those who become anxious learning about prognosis and side effects, however, and prefer to have limited information about their illnesses. Your knowledge of a patient’s personality type can help you determine whether added information might alleviate or worsen that patient’s stress.
Personal transformation can occur when patients face mortality. Their perceptions about what is important and how to achieve their goals can change dramatically.
Related resources
- National Cancer Institute. Coping with cancer. www.cancer.gov/cancertopics/coping.
- American Psychiatric Association. Patient education site with links to topics such as coping with AIDS/HIV, postpartum depression, alcohol abuse, mental health of the elderly, and common childhood disorders. www.healthyminds.org.
- Groves M, Muskin P. Psychological responses to illness. In: Bourgeois JA, Hales RE, Shahrokh N (eds). Textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:68-88.
Drug brand names
- Mirtazapine • Remeron
- Sertraline • Zoloft
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mrs. M, 35, is undergoing breast cancer treatment. She is referred to the consultation-liaison service by an emergency room physician for evaluation of suicidal thoughts.
Mrs. M has been crying for 2 hours. She awoke this morning feeling that she could no longer deal with “the unknown.” She has lost her hair and 30 pounds during chemotherapy and hardly recognized herself in the bathroom mirror. She thought about killing herself until one of her children walked by. After they went to school, she drove to the emergency room.
When you ask if she has had other thoughts of hurting herself, she says, “I would never do anything like that to my family, but the fact that I was thinking about it really scared me.”
Each patient responds uniquely to the emotional trauma of having a chronic or life-threatening medical illness. Coping styles depend on medical, psychological, and social factors as well as the person’s personality and experiences. Reactions range from mature to psychotic.
To help you guide patients such as Mrs. M through difficult medical treatments and decisions, we describe:
- a psychiatric workup to identify maladaptive response to illness
- typical emotional and behavioral responses to chronic illness
- how to provide psychotherapy tailored to the needs of 7 personality styles of medically ill patients.
Psychiatric Workup
Mrs. M is married with 3 sons. She found a lump on her breast 4 months ago but decided to wait “because, I thought, ‘it can’t be anything bad; it will go away.’” When the lump remained 3 months later, she consulted a specialist who diagnosed breast cancer.
Mrs. M underwent a lumpectomy and has been receiving weekly chemotherapy. Besides losing her hair, she says she has no appetite. Looking at food or driving close to the hospital makes her nauseous. She starts vomiting before she arrives for chemotherapy.
Though her family supports and encourages her, she can’t stop thinking about death. She feels isolated, lonely, and cries often. “No one understands what I am going through,” she says. “How can I share these feelings with them?”
Physicians such as the specialist who diagnosed Mrs. M’s cancer often must communicate difficult information. Careful planning when delivering bad news (Box 1)1,2 can set the stage for a healthier emotional and behavioral response.
Chronic illness causes depression in up to 25% of patients.3 At particular risk of developing depressive symptoms are patients with:
- poor physical condition
- poorly controlled pain
- advanced illness
- history of major depressive disorder
- family history of depression and suicide
- certain cancers, such as of the pancreas, lung, head or neck.4
Mechanisms of depression in illness. Depression can be the first symptom of some medical illnesses, such as pancreatic or liver cancer. Diseases that directly affect the brain—such as Parkinson’s disease, multiple sclerosis, and systemic lupus erythematosus—can cause depression. Patients disabled by spinal cord injury, stroke, or cancer also are at risk for depression.
Treatment is the same, whether illness-related chemical changes or the patient’s emotional response to disability is causing the depression. When diagnosing depression in medically ill patients, DSM-IV-TR recommends using criteria for major depression and providing treatment, whatever the cause.
Mrs. M has trouble sharing feelings of hopelessness with her family. Her changes in demeanor and isolation from everyday activities are clues to clinical depression and anxiety.
Depression can be difficult to diagnose when medical illness causes depression-like symptoms.5 To make the diagnosis, ask patients with chronic illness about depression’s emotional symptoms (hopelessness, withdrawal from others, sadness, ruminating thoughts, frequent crying spells), rather than its physical symptoms of poor eating, disturbed sleep, or low energy that may stem from the medical illness. Patients might not be as hard on themselves if they feel the medical illness—not poor coping on their part—caused their depression.
Box 1 6 steps for delivering bad medical news
Source: Adapted from references 1, 2Workup. Our workup of Mrs. M includes thyroid function tests, CBC, comprehensive metabolic panel, and brain MRI to rule out metastasis. All are negative. In her history, Mrs. M reports a previous episode of major depression 5 years ago that was successfully treated with sertraline for 1 year.
Consistent with her workup and symptoms, we diagnose major depression without psychosis. Cancer patients who report hopelessness are at increased risk of suicide. Because of her family support and religious beliefs, however, we feel she can safely go home and return for follow-up the next week.
Emotional response to illness
Mrs. M starts weekly outpatient appointments at our clinic. Because sertraline has worked for her in the past, it is our first choice to increase her energy, improve her mood, and decrease her hopelessness. Initial dosage is 25 mg/d for the first 3 days, with an increase to 50 mg/d for 1 month, and 100 mg/d thereafter. She reports no side effects.
In some patients, sertraline can cause adverse gastrointestinal effects such as upset stomach or nausea. Other antidepressants such as mirtazapine could improve patients’ sleep and decrease nausea.
Mrs. M also begins cognitive-behavioral therapy (CBT) to help her deal with negative thoughts, and relaxation training to combat her anxiety before chemotherapy. We recommend a local breast cancer support group, and Mrs. M starts going twice a month. She feels relieved that other patients are experiencing feelings similar to hers.
Medication plus CBT has been shown to be the most effective treatment for patients who meet criteria for depression and anxiety disorders. CBT has been shown to help patients manage physical symptoms and reframe negative thoughts associated with many chronic illnesses, including breast cancer, Parkinson’s disease, epilepsy, rheumatoid arthritis, and multiple sclerosis.6-10
Core emotions. Medically ill patients experience a range of core emotions, which Lazarus11 identified as anger, anxiety, guilt, fright, shame, sadness, happiness, envy, relief, and hope. Identifying the source of these emotions is important to counseling patients effectively.
For example, a patient experiencing fright might fear death, pain, disability, stigma, disfigurement, or other eventualities. Mrs. M has said she can’t stop thinking about dying. By knowing what the patient fears (Table 1),12 we can more effectively reassure and offer support, even when little else can be done.
Table 1
Common fears of patients reacting to diagnosis of chronic illness
|
| Source: Reference 12 |
Defensive behaviors. Patient’s behavioral responses may be adaptive or maladaptive; treatment nonadherence is one maladaptive response (Box 2).13,14 The patient history can suggest how well a person has adapted to past losses and disappointments. Patients may try to protect themselves against emotional and physical pain with psychotic, immature, neurotic, or mature defense mechanisms.15
Psychotic defenses are characterized by regression until patients lose touch with reality. Delusions and fantasy isolate them from the harshness of a serious medical condition. Antipsychotic medication and patience are often indicated.16
Immature defenses—as seen in patients with borderline personality disorder—can irritate and alienate the medical team. Physicians may not understand why their best efforts are thwarted or negated. Well-intentioned, caring doctors often try harder when the verbal attacks begin, but soon even the hardiest can wither under the patient’s criticism and threats.
Depressed medically ill patients adhere poorly to treatment schedules and other recommendations, which may cut their chances of survival.13 Up to 2% of hospital discharges are initiated by patients against medical advice.
Causes of refusing or discontinuing treatment may include anger towards the medical team or caregiver,14 anxiety, or withdrawal from addictive substances. Some patients who sign themselves out may be psychotic or confused by delirium or dementia. Others may be in denial of their illness.
Untreated psychiatric disorders can cause illness-specific nonadherence. Patients with:
- depression might not have the energy or motivation to follow the treatment.
- bipolar disorder might feel they don’t need the treatment.
- psychotic disorders may feel threatened by the treatment or the doctor.
Psychiatric patients may avoid taking medications prescribed for medical illness if they fear side effects or interactions with their psychotropics. Some don’t tell their medical practitioners about their psychiatric diagnoses because of the stigma associated with mental illness.
Psychiatrists can counsel the medical team to:
- pull back and focus on setting treatment objectives
- encourage the patient to work as a team member to ensure the best possible care
- communicate with the patient and care team to prevent divisions among the staff.
Neurotic defenses are in play when patients blame themselves and suffer internally. Give them ample opportunities to explore their feelings.
Mature defenses are seen in those who show concern for others, may express humor, and can adaptively plan, thus gaining the respect of others. Spirituality and optimism allow them to feel more at peace and less controlled by the illness.
Support these patients by encouraging their coping skills. For example, if spirituality has helped before, it may again strengthen them and their families.
Improving coping skills. By recognizing which patients are struggling, you can provide support to strengthen their coping abilities. Initially, Mrs. M was using neurotic defense mechanisms and internalizing her emotions. With the help of CBT, she begins to rely on more mature defenses. Her improved coping skills allow her to share her feelings during group therapy and with her family.
Encouraging adaptive behavior
Mrs. M is in remission when chemotherapy ends, but she worries that the cancer will come back. “The fear is still there,” she says. “You can’t be called a survivor for 5 years.”
She continues biweekly psychotherapy for the next year, and sertraline, 100 mg/d. She is doing well and has volunteered to help other newly-diagnosed patients at the cancer center.
Personality styles. Kahana and Bibring17 described 7 personality types that affect how patients cope with illnesses. Based on our experience, we suggest how to observe these styles, identify the emotional pain behind them, and respond in ways that will help each type of patient (Table 2).17
These personality types are not necessarily personality disorders; rather, they describe pervasive characteristics of coping styles. Some individuals will not match the descriptions of any of these types, and others may fall into more than one. Mrs. M, for example, shows traits of more than one personality style, including avoidant and mild schizoid features.
We helped her by engaging her in psychiatric treatment, helping her better understand her medical situation, and restoring her sense of control in making medical decisions. We discussed psycho-therapy as a two-way street, outlining her responsibilities to practice new CBT skills to use during treatment and in remission.
Table 2
Recommended treatment approaches for 7 patient personalities
| Personality | Patients who… | Often feel… | Are helped by… |
|---|---|---|---|
| Dependent | ask many questions, making it hard for you to end conversations or leave the room | afraid you won’t find them worthy, won’t want to care for them | regular, brief sessions (set tactful limits that will reassure patient and not annoy staff) |
| Obsessive | are insistent, detail-oriented | angry when they can’t control their illness, the staff, and the schedule | detailed explanations (provide choices whenever possible, try to use patient input collaboratively) |
| Narcissistic | are self-centered, criticize others, believe no one is qualified to care for them | fearful, threatened, and vulnerable | avoiding confrontation but emphasizing that they deserve the best care staff can provide (keep patient informed; be sure all staff provides the same message) |
| Suffering victim | always have symptoms and request much attention; might not follow recommendations | suffering is their role; views illness and its treatments as punishment, but hopes doctor will keep trying | regular visits, no matter how variable the complaints |
| Paranoid | do not trust doctors, refuse to participate in treatment plans or sign out | taken advantage of by others or purposefully neglected or harmed | staying calm (don’t argue; offer understanding of patient’s position, provide clear recommendations |
| Histrionic | are flirtatious, want to call doctors by first names | need to be ‘special’ to the physician; fear illness will invalidate them or make them unattractive | encouraging patient to verbalize concerns (set boundaries for relationship; remain courteous and objective) |
| Schizoid | are very lonely, tend to avoid medical care | doctors are invading their privacy | engaging patient in making medical decisions |
| Source: Adapted from reference 17 | |||
Supportive therapy. Encourage patients to seek support from family and friends.18 Some benefit from meeting other patients with the same needs, fears, and questions.19 The Internet is a good resource to find local support groups.
Becoming sick or disabled and having to change one’s lifestyle can damage a person’s self esteem. Encourage patients to help others by volunteering, participating in research, or engaging in other activities that provide hope, gratification, and a sense of service.20
Some patients regain control and battle their fears by becoming experts on their diseases. This approach will not help those who become anxious learning about prognosis and side effects, however, and prefer to have limited information about their illnesses. Your knowledge of a patient’s personality type can help you determine whether added information might alleviate or worsen that patient’s stress.
Personal transformation can occur when patients face mortality. Their perceptions about what is important and how to achieve their goals can change dramatically.
Related resources
- National Cancer Institute. Coping with cancer. www.cancer.gov/cancertopics/coping.
- American Psychiatric Association. Patient education site with links to topics such as coping with AIDS/HIV, postpartum depression, alcohol abuse, mental health of the elderly, and common childhood disorders. www.healthyminds.org.
- Groves M, Muskin P. Psychological responses to illness. In: Bourgeois JA, Hales RE, Shahrokh N (eds). Textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:68-88.
Drug brand names
- Mirtazapine • Remeron
- Sertraline • Zoloft
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Bailey W, Buckman R, Lenzi R, et al. SPIKES - a six-step protocol for delivering bad news; application to the patient with cancer. Oncologist 2000;5:4,302-11.
2. Koenig HG, Larson DB, Larson SS. Religion and coping with serious medical illness. Ann Pharmacother 2001;35(3):352-9.
3. Faller H, Schmidt M. Prognostic value of depressive coping and depression in survival of lung cancer patients. Psychooncology 2004;13(5):359-63.
4. Holland JC. Psychological care of patients: psycho-oncology’s contribution. J Clin Oncol 2003;21(23 suppl):253s-265s.
5. Lovejoy NC, Tabor D, Matteis M, Lillis P. Cancer-related depression: Part I. Neurologic alterations and cognitive-behavioral therapy. Oncol Nurs Forum 2000;27(4):667-78.
6. Cole K, Vaughan FL. The feasibility of using cognitive behaviour therapy for depression associated with Parkinson’s disease: a literature review. Parkinsonism Relat Disord 2005;11(5):269-76
7. Goldstein LH, McAlpine M, Deale A, et al. Cognitive behaviour therapy with adults with intractable epilepsy and psychiatric co-morbidity: preliminary observations on changes in psychological state and seizure frequency. Behav Res Ther 2003;41(4):447-60.
8. Evers AW, Kraaimaat FW, van Riel PL, de Jong AJ. Tailored cognitive-behavioral therapy in early rheumatoid arthritis for patients at risk: a randomized controlled trial. Pain 2002;100(1-2):141-53.
9. Mohr DC, Likosky W, Bertagnolli A, et al. Telephone-administered cognitive-behavioral therapy for the treatment of depressive symptoms in multiple sclerosis. J Consult Clin Psychol 2000;68(2):356-61.
10. Tatrow K. Montgomery GH. Cognitive behavioral therapy techniques for distress and pain in breast cancer patients: a meta-analysis. J Behav Med 2006;29(1):17-27.
11. Lazarus RS, Folkman S. Stress, appraisal and coping. New York: Springer, 1984.
12. Gazzola L, Muskin PR. The impact of stress and the objective of psychosocial interventions. In: Schein LA, Bernard HS, Spitz HI, Muskin PR (eds). Psychosocial treatment for medical conditions: principles and techniques. New York: Brunner-Routledge; 2003: 373-406.
13. Uitterhoeve RJ, Vernooy M, Litjens M, et al. Psychosocial interventions for patients with advanced cancer - a systematic review of the literature. Br J Cancer 2004;91(6):1050-62.
14. Perry S, Viederman M. Management of emotional reactions to acute medical illness. Med Clin North Am 1981;65:3-14.
15. Gabbard G. Major modalities: psychoanalytic/psychodynamic. In: Gabbard G, Beck J, Holmes J, eds. Oxford textbook of psychotherapy. New York: Oxford University Press; 2005:3-13.
16. Groves M, Muskin P. Psychological responses to illness In: Bourgeois JA, Hales RE, Shahrokh N (eds). Textbook of psychosomatic medicine Washington, DC: American Psychiatric Publishing; 2005:68-88.
17. Kahana RJ, Bibring G. Personality types in medical management. In: Zinberg NE (ed). Psychiatry and medical practice in a general hospital. New York: International Universities Press, 1964:108-23.
18. Johnson KS, Elbert-Avila KI, Tulsky JA. The influence of spiritual beliefs and practices on the treatment p of African Americans: a review of the literature. J Am Geriatr Soc 2005;53(4):711-19.
19. Vos PJ, Visser AP, Garssen B, et al. Effects of delayed psychosocial interventions versus early psychosocial interventions for women with early stage breast cancer. Patient Educ Couns 2006;60(2):212-9
20. Breitbart W, Gibson C, Poppito SR, Berg A. Psychotherapeutic interventions at the end of life: a focus on meaning and spirituality. Can J Psychiatry 2004;49(6):366-72.
1. Bailey W, Buckman R, Lenzi R, et al. SPIKES - a six-step protocol for delivering bad news; application to the patient with cancer. Oncologist 2000;5:4,302-11.
2. Koenig HG, Larson DB, Larson SS. Religion and coping with serious medical illness. Ann Pharmacother 2001;35(3):352-9.
3. Faller H, Schmidt M. Prognostic value of depressive coping and depression in survival of lung cancer patients. Psychooncology 2004;13(5):359-63.
4. Holland JC. Psychological care of patients: psycho-oncology’s contribution. J Clin Oncol 2003;21(23 suppl):253s-265s.
5. Lovejoy NC, Tabor D, Matteis M, Lillis P. Cancer-related depression: Part I. Neurologic alterations and cognitive-behavioral therapy. Oncol Nurs Forum 2000;27(4):667-78.
6. Cole K, Vaughan FL. The feasibility of using cognitive behaviour therapy for depression associated with Parkinson’s disease: a literature review. Parkinsonism Relat Disord 2005;11(5):269-76
7. Goldstein LH, McAlpine M, Deale A, et al. Cognitive behaviour therapy with adults with intractable epilepsy and psychiatric co-morbidity: preliminary observations on changes in psychological state and seizure frequency. Behav Res Ther 2003;41(4):447-60.
8. Evers AW, Kraaimaat FW, van Riel PL, de Jong AJ. Tailored cognitive-behavioral therapy in early rheumatoid arthritis for patients at risk: a randomized controlled trial. Pain 2002;100(1-2):141-53.
9. Mohr DC, Likosky W, Bertagnolli A, et al. Telephone-administered cognitive-behavioral therapy for the treatment of depressive symptoms in multiple sclerosis. J Consult Clin Psychol 2000;68(2):356-61.
10. Tatrow K. Montgomery GH. Cognitive behavioral therapy techniques for distress and pain in breast cancer patients: a meta-analysis. J Behav Med 2006;29(1):17-27.
11. Lazarus RS, Folkman S. Stress, appraisal and coping. New York: Springer, 1984.
12. Gazzola L, Muskin PR. The impact of stress and the objective of psychosocial interventions. In: Schein LA, Bernard HS, Spitz HI, Muskin PR (eds). Psychosocial treatment for medical conditions: principles and techniques. New York: Brunner-Routledge; 2003: 373-406.
13. Uitterhoeve RJ, Vernooy M, Litjens M, et al. Psychosocial interventions for patients with advanced cancer - a systematic review of the literature. Br J Cancer 2004;91(6):1050-62.
14. Perry S, Viederman M. Management of emotional reactions to acute medical illness. Med Clin North Am 1981;65:3-14.
15. Gabbard G. Major modalities: psychoanalytic/psychodynamic. In: Gabbard G, Beck J, Holmes J, eds. Oxford textbook of psychotherapy. New York: Oxford University Press; 2005:3-13.
16. Groves M, Muskin P. Psychological responses to illness In: Bourgeois JA, Hales RE, Shahrokh N (eds). Textbook of psychosomatic medicine Washington, DC: American Psychiatric Publishing; 2005:68-88.
17. Kahana RJ, Bibring G. Personality types in medical management. In: Zinberg NE (ed). Psychiatry and medical practice in a general hospital. New York: International Universities Press, 1964:108-23.
18. Johnson KS, Elbert-Avila KI, Tulsky JA. The influence of spiritual beliefs and practices on the treatment p of African Americans: a review of the literature. J Am Geriatr Soc 2005;53(4):711-19.
19. Vos PJ, Visser AP, Garssen B, et al. Effects of delayed psychosocial interventions versus early psychosocial interventions for women with early stage breast cancer. Patient Educ Couns 2006;60(2):212-9
20. Breitbart W, Gibson C, Poppito SR, Berg A. Psychotherapeutic interventions at the end of life: a focus on meaning and spirituality. Can J Psychiatry 2004;49(6):366-72.