User login
BP meds: This simple change improves outcomes
Advise patients with uncontrolled hypertension to take at least one of their blood pressure (BP) medications at bedtime instead of in the morning. Nighttime dosing leads to better control and lowers the risk of major cardiovascular events.1,2
STRENGTH OF RECOMMENDATION
B: Based on a well-done randomized clinical trial (RCT) and a subgroup analysis.
Hermida RC, Ayala DE, Mojón A, et al. Influence of circadian time of hypertension treatment on cardiovascular risk: results of the MAPEC study. Chronobiol Int. 2010;27:1629-1651.
Hermida RC, Ayala DE, Mojón A, et al. Influence of time of day of blood pressure-lowering treatment on cardiovascular risk in hypertensive patients with type 2 diabetes. Diabetes Care. 2011;34:1270-1276.
ILLUSTRATIVE CASES
- A 60-year-old man has struggled to get his BP under control despite the use of 3 anti-hypertensives. Is there anything you can recommend to improve his BP control and lower his cardiovascular risk?
- You prescribe hydrochlorothiazide for a 55-year-old woman with newly diagnosed hypertension. What can you tell her about how to take the medication to maximize its beneficial effects?
Management of hypertension often centers around BP measurements taken in a doctor’s office during the day, although both BP and metabolism fluctuate with circadian rhythms. Most people experience an increase in pressure during the day, with peaks in the morning and evening, followed by a decline in BP while they sleep at night.3
The focus belongs on nighttime BP
Sleeping BP is getting considerable attention, particularly the phenomenon of nondipping. Commonly defined as a <10% decline in systolic pressure during sleep, nondipping is associated with an increased risk of cardiovascular events, such as heart attack and stroke.4 What’s more, mean BP during the night is a better predictor of cardiovascular disease (CVD) risk than BP while the patient is awake.5,6
Evidence suggests that taking an anti-hypertensive medication at night increases its therapeutic effect,7 yet most patients take it in the morning.8 The study detailed in this PURL was designed to investigate whether bedtime dosing significantly affects BP control and CVD risk.
STUDY SUMMARY: Bedtime dosing benefits patients, and there’s no downside
The MAPEC study was an open-label RCT conducted at a single center in Spain.1 Patients were enrolled if they had a diagnosis of either untreated hypertension (based on ambulatory BP monitoring [ABPM] criteria) or resistant hypertension (uncontrolled on ≥3 optimally dosed antihypertensive medications). Exclusion criteria included pregnancy, a history of drug/alcohol abuse, night shift work, acquired immune deficiency syndrome, type 1 diabetes, secondary hypertension, and a previous CVD diagnosis.
Patients were randomly assigned to one of 2 time-of-day dosing groups: morning dosing of all their BP medications (n=1109) or dosing of ≥1 BP medications at bedtime (n=1092). ABPM—in which patients wore a monitor that recorded their BP every 20 minutes during the day and every 30 minutes at night for 48 hours—was conducted once a year, or more frequently when medication adjustments occurred. The use of a specific drug was not required, but physicians were instructed to adjust medications according to a study-specific ABPM protocol.
Patients were followed for a mean of 5.6 years for the endpoints of CVD events and mortality. These endpoints were assessed by researchers blinded to patients’ treatment assignment.
At baseline, the 2 groups were similar in age (mean of 55 years), percentage of men (48%), presence of comorbidities, and baseline clinic and ambulatory BP. Throughout the study, patients in the bedtime dosing group had lower mean asleep systolic and diastolic BP, a lower prevalence of a non-dipping pattern, and a higher prevalence of controlled ambulatory BP. The bedtime group also had a lower risk of total CVD events (relative risk [RR]=0.39; 95% confidence interval [CI], 0.29-0.51; P<.001) and major CVD events (RR=0.33; 95% CI, 0.19-0.55; P<.001), and fewer overall deaths (4.16/1000 vs 2.11/1000 patient-years; P=.008) (TABLE). To prevent one CVD event, 63 patients would need to take their BP medication at bedtime instead of in the morning for one year. To prevent one death, 488 patient would need to adhere to the nighttime schedule for one year.
A subgroup analysis of patients with type 2 diabetes (n=448)2 had similar results: For this population, too, bedtime dosing led to lower asleep BP, a lower prevalence of a non-dipping pattern, and a higher prevalence of controlled ambulatory BP, as well as a lower risk of total CVD events, major CVD events, and CVD-related death. The differences persisted after correction for the use of statins and aspirin. Among those in this subgroup analysis, 29 patients would need to take their BP medications at bedtime for one year to prevent one CVD event, and 263 patients would need to be treated for one year to prevent one death.
TABLE
Dosing of BP meds: A look at outcomes
| Events/1000 patient-years | Morning dosing | Bedtime dosing | P between groups |
|---|---|---|---|
| overall (n=2201)1 | |||
| Total events* | 27.80 | 11.95 | <.001 |
| CVd death | 2.08 | 0.53 | .006 |
| Cardiovascular events | 11.00 | 5.27 | <.001 |
| Cerebrovascular events | 3.57 | 1.23 | .001 |
| Diabetes subgroup (n=448)2 | |||
| Total events* | 54.24 | 19.80 | <.001 |
| CVd death | 4.79 | 0.86 | .038 |
| Cardiovascular events | 15.95 | 6.89 | .008 |
| Cerebrovascular events | 6.38 | 0.86 | .010 |
| *Includes death from all causes and cardiovascular and cerebrovascular events. BP, blood pressure; CVD, cardiovascular disease. | |||
WHAT’S NEW: Advantages of preventing nondipping are clearly established
We’ve known that a nondipping pattern is associated with higher cardiovascular risks and that taking antihypertensives at bedtime decreases the prevalence of nondipping patterns. The MAPEC study, however, is the first prospective trial to show that bedtime dosing of BP medications lowers the risk of CVD events and death.
CAVEATS: Methodology, non-US guidelines raise questions about applicability here
MAPEC was an open-label study, meaning that the physicians adjusting BP medications were aware of the treatment groups to which their patients were allocated. Physicians were given guidelines for the titration of medications, but it is unclear whether they treated patients in both treatment groups identically. Patients were also aware of their treatment group, which creates the potential for bias if one group adhered to their medications more closely than the other.
The study was a single-center trial conducted in Spain, which may limit its generalizability to the United States. Notably, Spain’s medication guidelines differ from ours, with angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, beta-blockers, and calcium channel blockers as first-line medications and hydrochlorothiazide as a second-line option.
While ABPM appears to be a better indicator of CVD risk compared with clinic BP monitoring, most US physicians still rely on readings taken in their office for diagnosing and managing hypertension. How ambulatory BP translates to clinic BP is somewhat unclear.
CHALLENGES TO IMPLEMENTATION: Some patients and providers may resist the switch
We see few challenges to implementing bedtime dosing of BP medications for patients with uncontrolled hypertension. It is possible, however, that patients who have a long-standing routine of taking their medications in the morning may be resistant to change. Also, pharmacists and nurses, as well as some physicians, may continue recommending morning dosing, which could be confusing for patients.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Hermida RC, Ayala DE, Mojón A, et al. Influence of circadian time of hypertension treatment on cardiovascular risk: results of the MAPEC study. Chronobiol Int. 2010;27:1629-1651.
2. Hermida RC, Ayala DE, Mojón A, et al. Influence of time of day of blood pressure-lowering treatment on cardiovascular risk in hypertensive patients with type 2 diabetes. Diabetes Care. 2011;34:1270-1276.
3. Hermida RC, Ayala DE, Portaluppi F. Circadian variation of blood pressure: the basis for the chronotherapy of hypertension. Adv Drug Deliv Rev. 2007;59:904-922.
4. Verdecchia P, Porcellati C, Schillaci G, et al. Ambulatory blood pressure: an independent predictor of prognosis in essential hypertension. Hypertension. 1994;24:793-801.
5. Dolan E, Stanton A, Thijs L, et al. Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin study outcome. Hypertension. 2005;46:156-161.
6. Hermida RC, Ayala DE, Mojón A, et al. Decreasing sleep-time blood pressure determined by ambulatory monitoring reduces cardiovascular risk. J Am Coll Cardiol. 2011;58:1165-1173.
7. De la Sierra A, Redon J, Banegas JR, et al. Prevalence and factors associated with circadian blood pressure patterns in hypertensive patients. Hypertension. 2009;53:466-472.
8. Hermida RC, Ayala DE, Calvo C, et al. Chronotherapy of hypertension: administration-time-dependent effects of treatment on the circadian pattern of blood pressure. Adv Drug Deliv Rev. 2007;59:923-939.
Advise patients with uncontrolled hypertension to take at least one of their blood pressure (BP) medications at bedtime instead of in the morning. Nighttime dosing leads to better control and lowers the risk of major cardiovascular events.1,2
STRENGTH OF RECOMMENDATION
B: Based on a well-done randomized clinical trial (RCT) and a subgroup analysis.
Hermida RC, Ayala DE, Mojón A, et al. Influence of circadian time of hypertension treatment on cardiovascular risk: results of the MAPEC study. Chronobiol Int. 2010;27:1629-1651.
Hermida RC, Ayala DE, Mojón A, et al. Influence of time of day of blood pressure-lowering treatment on cardiovascular risk in hypertensive patients with type 2 diabetes. Diabetes Care. 2011;34:1270-1276.
ILLUSTRATIVE CASES
- A 60-year-old man has struggled to get his BP under control despite the use of 3 anti-hypertensives. Is there anything you can recommend to improve his BP control and lower his cardiovascular risk?
- You prescribe hydrochlorothiazide for a 55-year-old woman with newly diagnosed hypertension. What can you tell her about how to take the medication to maximize its beneficial effects?
Management of hypertension often centers around BP measurements taken in a doctor’s office during the day, although both BP and metabolism fluctuate with circadian rhythms. Most people experience an increase in pressure during the day, with peaks in the morning and evening, followed by a decline in BP while they sleep at night.3
The focus belongs on nighttime BP
Sleeping BP is getting considerable attention, particularly the phenomenon of nondipping. Commonly defined as a <10% decline in systolic pressure during sleep, nondipping is associated with an increased risk of cardiovascular events, such as heart attack and stroke.4 What’s more, mean BP during the night is a better predictor of cardiovascular disease (CVD) risk than BP while the patient is awake.5,6
Evidence suggests that taking an anti-hypertensive medication at night increases its therapeutic effect,7 yet most patients take it in the morning.8 The study detailed in this PURL was designed to investigate whether bedtime dosing significantly affects BP control and CVD risk.
STUDY SUMMARY: Bedtime dosing benefits patients, and there’s no downside
The MAPEC study was an open-label RCT conducted at a single center in Spain.1 Patients were enrolled if they had a diagnosis of either untreated hypertension (based on ambulatory BP monitoring [ABPM] criteria) or resistant hypertension (uncontrolled on ≥3 optimally dosed antihypertensive medications). Exclusion criteria included pregnancy, a history of drug/alcohol abuse, night shift work, acquired immune deficiency syndrome, type 1 diabetes, secondary hypertension, and a previous CVD diagnosis.
Patients were randomly assigned to one of 2 time-of-day dosing groups: morning dosing of all their BP medications (n=1109) or dosing of ≥1 BP medications at bedtime (n=1092). ABPM—in which patients wore a monitor that recorded their BP every 20 minutes during the day and every 30 minutes at night for 48 hours—was conducted once a year, or more frequently when medication adjustments occurred. The use of a specific drug was not required, but physicians were instructed to adjust medications according to a study-specific ABPM protocol.
Patients were followed for a mean of 5.6 years for the endpoints of CVD events and mortality. These endpoints were assessed by researchers blinded to patients’ treatment assignment.
At baseline, the 2 groups were similar in age (mean of 55 years), percentage of men (48%), presence of comorbidities, and baseline clinic and ambulatory BP. Throughout the study, patients in the bedtime dosing group had lower mean asleep systolic and diastolic BP, a lower prevalence of a non-dipping pattern, and a higher prevalence of controlled ambulatory BP. The bedtime group also had a lower risk of total CVD events (relative risk [RR]=0.39; 95% confidence interval [CI], 0.29-0.51; P<.001) and major CVD events (RR=0.33; 95% CI, 0.19-0.55; P<.001), and fewer overall deaths (4.16/1000 vs 2.11/1000 patient-years; P=.008) (TABLE). To prevent one CVD event, 63 patients would need to take their BP medication at bedtime instead of in the morning for one year. To prevent one death, 488 patient would need to adhere to the nighttime schedule for one year.
A subgroup analysis of patients with type 2 diabetes (n=448)2 had similar results: For this population, too, bedtime dosing led to lower asleep BP, a lower prevalence of a non-dipping pattern, and a higher prevalence of controlled ambulatory BP, as well as a lower risk of total CVD events, major CVD events, and CVD-related death. The differences persisted after correction for the use of statins and aspirin. Among those in this subgroup analysis, 29 patients would need to take their BP medications at bedtime for one year to prevent one CVD event, and 263 patients would need to be treated for one year to prevent one death.
TABLE
Dosing of BP meds: A look at outcomes
| Events/1000 patient-years | Morning dosing | Bedtime dosing | P between groups |
|---|---|---|---|
| overall (n=2201)1 | |||
| Total events* | 27.80 | 11.95 | <.001 |
| CVd death | 2.08 | 0.53 | .006 |
| Cardiovascular events | 11.00 | 5.27 | <.001 |
| Cerebrovascular events | 3.57 | 1.23 | .001 |
| Diabetes subgroup (n=448)2 | |||
| Total events* | 54.24 | 19.80 | <.001 |
| CVd death | 4.79 | 0.86 | .038 |
| Cardiovascular events | 15.95 | 6.89 | .008 |
| Cerebrovascular events | 6.38 | 0.86 | .010 |
| *Includes death from all causes and cardiovascular and cerebrovascular events. BP, blood pressure; CVD, cardiovascular disease. | |||
WHAT’S NEW: Advantages of preventing nondipping are clearly established
We’ve known that a nondipping pattern is associated with higher cardiovascular risks and that taking antihypertensives at bedtime decreases the prevalence of nondipping patterns. The MAPEC study, however, is the first prospective trial to show that bedtime dosing of BP medications lowers the risk of CVD events and death.
CAVEATS: Methodology, non-US guidelines raise questions about applicability here
MAPEC was an open-label study, meaning that the physicians adjusting BP medications were aware of the treatment groups to which their patients were allocated. Physicians were given guidelines for the titration of medications, but it is unclear whether they treated patients in both treatment groups identically. Patients were also aware of their treatment group, which creates the potential for bias if one group adhered to their medications more closely than the other.
The study was a single-center trial conducted in Spain, which may limit its generalizability to the United States. Notably, Spain’s medication guidelines differ from ours, with angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, beta-blockers, and calcium channel blockers as first-line medications and hydrochlorothiazide as a second-line option.
While ABPM appears to be a better indicator of CVD risk compared with clinic BP monitoring, most US physicians still rely on readings taken in their office for diagnosing and managing hypertension. How ambulatory BP translates to clinic BP is somewhat unclear.
CHALLENGES TO IMPLEMENTATION: Some patients and providers may resist the switch
We see few challenges to implementing bedtime dosing of BP medications for patients with uncontrolled hypertension. It is possible, however, that patients who have a long-standing routine of taking their medications in the morning may be resistant to change. Also, pharmacists and nurses, as well as some physicians, may continue recommending morning dosing, which could be confusing for patients.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Advise patients with uncontrolled hypertension to take at least one of their blood pressure (BP) medications at bedtime instead of in the morning. Nighttime dosing leads to better control and lowers the risk of major cardiovascular events.1,2
STRENGTH OF RECOMMENDATION
B: Based on a well-done randomized clinical trial (RCT) and a subgroup analysis.
Hermida RC, Ayala DE, Mojón A, et al. Influence of circadian time of hypertension treatment on cardiovascular risk: results of the MAPEC study. Chronobiol Int. 2010;27:1629-1651.
Hermida RC, Ayala DE, Mojón A, et al. Influence of time of day of blood pressure-lowering treatment on cardiovascular risk in hypertensive patients with type 2 diabetes. Diabetes Care. 2011;34:1270-1276.
ILLUSTRATIVE CASES
- A 60-year-old man has struggled to get his BP under control despite the use of 3 anti-hypertensives. Is there anything you can recommend to improve his BP control and lower his cardiovascular risk?
- You prescribe hydrochlorothiazide for a 55-year-old woman with newly diagnosed hypertension. What can you tell her about how to take the medication to maximize its beneficial effects?
Management of hypertension often centers around BP measurements taken in a doctor’s office during the day, although both BP and metabolism fluctuate with circadian rhythms. Most people experience an increase in pressure during the day, with peaks in the morning and evening, followed by a decline in BP while they sleep at night.3
The focus belongs on nighttime BP
Sleeping BP is getting considerable attention, particularly the phenomenon of nondipping. Commonly defined as a <10% decline in systolic pressure during sleep, nondipping is associated with an increased risk of cardiovascular events, such as heart attack and stroke.4 What’s more, mean BP during the night is a better predictor of cardiovascular disease (CVD) risk than BP while the patient is awake.5,6
Evidence suggests that taking an anti-hypertensive medication at night increases its therapeutic effect,7 yet most patients take it in the morning.8 The study detailed in this PURL was designed to investigate whether bedtime dosing significantly affects BP control and CVD risk.
STUDY SUMMARY: Bedtime dosing benefits patients, and there’s no downside
The MAPEC study was an open-label RCT conducted at a single center in Spain.1 Patients were enrolled if they had a diagnosis of either untreated hypertension (based on ambulatory BP monitoring [ABPM] criteria) or resistant hypertension (uncontrolled on ≥3 optimally dosed antihypertensive medications). Exclusion criteria included pregnancy, a history of drug/alcohol abuse, night shift work, acquired immune deficiency syndrome, type 1 diabetes, secondary hypertension, and a previous CVD diagnosis.
Patients were randomly assigned to one of 2 time-of-day dosing groups: morning dosing of all their BP medications (n=1109) or dosing of ≥1 BP medications at bedtime (n=1092). ABPM—in which patients wore a monitor that recorded their BP every 20 minutes during the day and every 30 minutes at night for 48 hours—was conducted once a year, or more frequently when medication adjustments occurred. The use of a specific drug was not required, but physicians were instructed to adjust medications according to a study-specific ABPM protocol.
Patients were followed for a mean of 5.6 years for the endpoints of CVD events and mortality. These endpoints were assessed by researchers blinded to patients’ treatment assignment.
At baseline, the 2 groups were similar in age (mean of 55 years), percentage of men (48%), presence of comorbidities, and baseline clinic and ambulatory BP. Throughout the study, patients in the bedtime dosing group had lower mean asleep systolic and diastolic BP, a lower prevalence of a non-dipping pattern, and a higher prevalence of controlled ambulatory BP. The bedtime group also had a lower risk of total CVD events (relative risk [RR]=0.39; 95% confidence interval [CI], 0.29-0.51; P<.001) and major CVD events (RR=0.33; 95% CI, 0.19-0.55; P<.001), and fewer overall deaths (4.16/1000 vs 2.11/1000 patient-years; P=.008) (TABLE). To prevent one CVD event, 63 patients would need to take their BP medication at bedtime instead of in the morning for one year. To prevent one death, 488 patient would need to adhere to the nighttime schedule for one year.
A subgroup analysis of patients with type 2 diabetes (n=448)2 had similar results: For this population, too, bedtime dosing led to lower asleep BP, a lower prevalence of a non-dipping pattern, and a higher prevalence of controlled ambulatory BP, as well as a lower risk of total CVD events, major CVD events, and CVD-related death. The differences persisted after correction for the use of statins and aspirin. Among those in this subgroup analysis, 29 patients would need to take their BP medications at bedtime for one year to prevent one CVD event, and 263 patients would need to be treated for one year to prevent one death.
TABLE
Dosing of BP meds: A look at outcomes
| Events/1000 patient-years | Morning dosing | Bedtime dosing | P between groups |
|---|---|---|---|
| overall (n=2201)1 | |||
| Total events* | 27.80 | 11.95 | <.001 |
| CVd death | 2.08 | 0.53 | .006 |
| Cardiovascular events | 11.00 | 5.27 | <.001 |
| Cerebrovascular events | 3.57 | 1.23 | .001 |
| Diabetes subgroup (n=448)2 | |||
| Total events* | 54.24 | 19.80 | <.001 |
| CVd death | 4.79 | 0.86 | .038 |
| Cardiovascular events | 15.95 | 6.89 | .008 |
| Cerebrovascular events | 6.38 | 0.86 | .010 |
| *Includes death from all causes and cardiovascular and cerebrovascular events. BP, blood pressure; CVD, cardiovascular disease. | |||
WHAT’S NEW: Advantages of preventing nondipping are clearly established
We’ve known that a nondipping pattern is associated with higher cardiovascular risks and that taking antihypertensives at bedtime decreases the prevalence of nondipping patterns. The MAPEC study, however, is the first prospective trial to show that bedtime dosing of BP medications lowers the risk of CVD events and death.
CAVEATS: Methodology, non-US guidelines raise questions about applicability here
MAPEC was an open-label study, meaning that the physicians adjusting BP medications were aware of the treatment groups to which their patients were allocated. Physicians were given guidelines for the titration of medications, but it is unclear whether they treated patients in both treatment groups identically. Patients were also aware of their treatment group, which creates the potential for bias if one group adhered to their medications more closely than the other.
The study was a single-center trial conducted in Spain, which may limit its generalizability to the United States. Notably, Spain’s medication guidelines differ from ours, with angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, beta-blockers, and calcium channel blockers as first-line medications and hydrochlorothiazide as a second-line option.
While ABPM appears to be a better indicator of CVD risk compared with clinic BP monitoring, most US physicians still rely on readings taken in their office for diagnosing and managing hypertension. How ambulatory BP translates to clinic BP is somewhat unclear.
CHALLENGES TO IMPLEMENTATION: Some patients and providers may resist the switch
We see few challenges to implementing bedtime dosing of BP medications for patients with uncontrolled hypertension. It is possible, however, that patients who have a long-standing routine of taking their medications in the morning may be resistant to change. Also, pharmacists and nurses, as well as some physicians, may continue recommending morning dosing, which could be confusing for patients.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Hermida RC, Ayala DE, Mojón A, et al. Influence of circadian time of hypertension treatment on cardiovascular risk: results of the MAPEC study. Chronobiol Int. 2010;27:1629-1651.
2. Hermida RC, Ayala DE, Mojón A, et al. Influence of time of day of blood pressure-lowering treatment on cardiovascular risk in hypertensive patients with type 2 diabetes. Diabetes Care. 2011;34:1270-1276.
3. Hermida RC, Ayala DE, Portaluppi F. Circadian variation of blood pressure: the basis for the chronotherapy of hypertension. Adv Drug Deliv Rev. 2007;59:904-922.
4. Verdecchia P, Porcellati C, Schillaci G, et al. Ambulatory blood pressure: an independent predictor of prognosis in essential hypertension. Hypertension. 1994;24:793-801.
5. Dolan E, Stanton A, Thijs L, et al. Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin study outcome. Hypertension. 2005;46:156-161.
6. Hermida RC, Ayala DE, Mojón A, et al. Decreasing sleep-time blood pressure determined by ambulatory monitoring reduces cardiovascular risk. J Am Coll Cardiol. 2011;58:1165-1173.
7. De la Sierra A, Redon J, Banegas JR, et al. Prevalence and factors associated with circadian blood pressure patterns in hypertensive patients. Hypertension. 2009;53:466-472.
8. Hermida RC, Ayala DE, Calvo C, et al. Chronotherapy of hypertension: administration-time-dependent effects of treatment on the circadian pattern of blood pressure. Adv Drug Deliv Rev. 2007;59:923-939.
1. Hermida RC, Ayala DE, Mojón A, et al. Influence of circadian time of hypertension treatment on cardiovascular risk: results of the MAPEC study. Chronobiol Int. 2010;27:1629-1651.
2. Hermida RC, Ayala DE, Mojón A, et al. Influence of time of day of blood pressure-lowering treatment on cardiovascular risk in hypertensive patients with type 2 diabetes. Diabetes Care. 2011;34:1270-1276.
3. Hermida RC, Ayala DE, Portaluppi F. Circadian variation of blood pressure: the basis for the chronotherapy of hypertension. Adv Drug Deliv Rev. 2007;59:904-922.
4. Verdecchia P, Porcellati C, Schillaci G, et al. Ambulatory blood pressure: an independent predictor of prognosis in essential hypertension. Hypertension. 1994;24:793-801.
5. Dolan E, Stanton A, Thijs L, et al. Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin study outcome. Hypertension. 2005;46:156-161.
6. Hermida RC, Ayala DE, Mojón A, et al. Decreasing sleep-time blood pressure determined by ambulatory monitoring reduces cardiovascular risk. J Am Coll Cardiol. 2011;58:1165-1173.
7. De la Sierra A, Redon J, Banegas JR, et al. Prevalence and factors associated with circadian blood pressure patterns in hypertensive patients. Hypertension. 2009;53:466-472.
8. Hermida RC, Ayala DE, Calvo C, et al. Chronotherapy of hypertension: administration-time-dependent effects of treatment on the circadian pattern of blood pressure. Adv Drug Deliv Rev. 2007;59:923-939.
Copyright © 2012 The Family Physicians Inquiries Network.
All rights reserved.
Postprostatectomy incontinence? Here’s help
Recommend behavioral therapy—incorporating pelvic floor muscle training and bladder control strategies—to men experiencing incontinence after prostatectomy.1
STRENGTH OF RECOMMENDATION
B: Based on a single unblinded randomized controlled trial (RCT).
Goode PS, Burgio KL, Johnson TM, et al. Behavioral therapy with or without biofeedback and pelvic floor electrical stimulation for persistent postprostatectomy incontinence: a randomized controlled trial. JAMA. 2011;305:151-159.1
ILLUSTRATIVE CASE
Mr. H, age 75, underwent radical prostatectomy for prostate cancer a year ago. Since then, he leaks urine when he coughs and occasionally has complete loss of bladder control. His lack of control has forced him to curtail many of his normal activities and he wants to know what help you can provide.
Routine prostate-specific antigen (PSA) screening has led to an increase in the diagnosis of localized prostate cancer, and prostatectomy is a common treatment. Approximately 90,000 US men undergo radical prostatectomy each year,2 and most are left with some degree of incontinence.
Years later, bladder control problems remain
Surgical advances have attempted to minimize nerve and bladder neck damage, but some degree of incontinence is still common after radical prostatectomy. According to the 2000 Prostate Cancer Outcomes Study, 80% of men experienced some incontinence 6 months after radical prostatectomy. After 2 years, 68% of men still had some degree of incontinence,3 and 8% reported frequent or total incontinence. Five years after prostatectomy, only 35% of patients reported complete bladder control vs 87% presurgery.4
A 2004 systematic review showed that behavioral therapy (mostly biofeedback) reduced symptoms in patients with all types of urinary incontinence.5 Many studies, including a 2010 Cochrane review,6 have shown that women with incontinence benefit from pelvic floor muscle training. No randomized trials have assessed the benefit of behavioral therapy for men with incontinence related to postprostatectomy—until now.
STUDY SUMMARY: Behavioral therapy has long-term payoff
The study by Goode et al was an RCT of behavioral therapy for men who had urinary incontinence after radical prostatectomy and whose symptoms persisted more than a year later. It included patients with ≥3 episodes of incontinence per week. Men were excluded if they were undergoing other treatment for prostate cancer, had a high postvoid residual volume or a history of certain bladder surgeries, or were unable to reliably report symptoms. Participants were permitted to continue taking medication for incontinence, with the exception of anticholinergics.
Participants (n=208 from 3 sites) were randomized to one of 3 arms in a blinded fashion with concealed allocation: behavioral therapy alone, behavioral therapy and biofeedback with electrical stimulation, or a control group of men who could elect to try these therapies at a later date.
Behavioral therapy consisted of 4 visits with a physician or nurse practitioner over an 8-week period. At the first visit, patients received instruction in pelvic floor muscle training. Patients then practiced contraction and relaxation exercises and urinary flow control at home. At the second visit, patients learned techniques to avoid episodes of incontinence, such as performing pelvic muscle contractions with stress symptom triggers. During the final 2 visits, patients received advice about control of persistent problems identified in symptom diaries they were required to keep. In addition, continued daily pelvic floor exercises were recommended at the last session.
Men in the group that received biofeedback with electrical stimulation had the same visit schedule, but received additional pelvic floor training—with electrode-mediated feedback and electrical stimulation of pelvic floor muscles during each visit and daily at home. Patients in the control group had the same visit frequency but received no treatment. After 8 weeks, however, the controls were given the opportunity to try behavioral therapy.
Baseline characteristics and attrition rates were similar in all 3 groups. Outcomes were based on an intention-to-treat analysis. At 8 weeks, men receiving behavioral therapy, with or without electrical stimulation and biofeedback, experienced a 55% decrease in incontinence (from 28 episodes per week at baseline to 13 per week); patients in the control group had a 24% decrease (from 25 episodes to 20 per week) (P=.001). More patients in the behavioral groups were completely continent at 8 weeks (16% vs 6% for the controls); the number needed to treat to achieve complete continence was 10. Electrical stimulation and biofeedback provided no added benefit compared with behavioral therapy alone.
Patients in the 2 treatment groups also had clinically significant benefits in some quality-of-life measures (impact of urinary symptoms on travel, emotion, and voiding) and in symptom-specific quality-of-life scores. Patient satisfaction at 8 weeks was higher in the treatment groups: 26 of the 58 men who received behavioral therapy were “delighted, pleased, or mostly satisfied,” vs 9 of 60 in the control group (P=.006 for overall group difference).
Adherence to the behavioral therapy protocol was 100% at 8 weeks and remained high (91%) one year later. Improvement in symptoms continued at one year, with patients in both treatment groups reporting a clinically significant (50%) reduction in incontinence episodes compared with baseline.
WHAT’S NEW: We have evidence-based help for postprostatectomy incontinence
We now have evidence that an 8-week program of pelvic floor training and bladder control strategies reduces the frequency of incontinence in men who have undergone radical prostatectomy.
CAVEATS: The effects of time weren’t factored in
Patients were obviously aware of group assignment, so there is the possibility of treatment bias contributing to the positive self-reported outcomes. While the treatment groups showed both a greater initial improvement and persistent improvement in their symptoms at one year, symptoms of patients in the control group were not measured after a year, so the sustained improvement could reflect resolution of incontinence with time.
CHALLENGES TO IMPLEMENTATION: Locating clinicians who can train patients
The type of behavioral therapy featured in this study may not be easily accessible to all patients. The researchers suggest consulting the National Association for Continence (http://www.nafc.org), a private nonprofit organization whose members include physical therapists, nurses, and physicians. They also cite the Wound Ostomy and Continence Nurses Society (http://www.wocn.org) as a resource in locating nurses who provide these services.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Goode PS, Burgio KL, Johnson TM, et al. Behavioral therapy with or without biofeedback and pelvic floor electrical stimulation for persistent postprostatectomy incontinence: a randomized controlled trial. JAMA. 2011;305:151-159.
2. Barbash GI, Glied SA. New technology and health care costs—the case of robot-assisted surgery. N Engl J Med. 2010;363:701-704.
3. Stanford JL, Feng Z, Hamilton AS, et al. Urinary and sexual function after radical prostatectomy for clinically localized prostate cancer: the Prostate Cancer Outcomes Study. JAMA. 2000;283:354-360.
4. Penson DF, McLerran D, Feng Z, et al. 5-year urinary and sexual outcomes after radical prostatectomy: results from the prostate cancer outcomes study. J Urol. 2005;173:1701-1705.
5. Teunisse TA, de Jonge A, van Weel C, et al. Treating urinary incontinence in the elderly—conservative therapies that work: a systematic review. J Fam Pract. 2004;53:25-30, 32.
6. Dumoulin C, Hay-Smith J. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev. 2010;(1):CD005654.-
Recommend behavioral therapy—incorporating pelvic floor muscle training and bladder control strategies—to men experiencing incontinence after prostatectomy.1
STRENGTH OF RECOMMENDATION
B: Based on a single unblinded randomized controlled trial (RCT).
Goode PS, Burgio KL, Johnson TM, et al. Behavioral therapy with or without biofeedback and pelvic floor electrical stimulation for persistent postprostatectomy incontinence: a randomized controlled trial. JAMA. 2011;305:151-159.1
ILLUSTRATIVE CASE
Mr. H, age 75, underwent radical prostatectomy for prostate cancer a year ago. Since then, he leaks urine when he coughs and occasionally has complete loss of bladder control. His lack of control has forced him to curtail many of his normal activities and he wants to know what help you can provide.
Routine prostate-specific antigen (PSA) screening has led to an increase in the diagnosis of localized prostate cancer, and prostatectomy is a common treatment. Approximately 90,000 US men undergo radical prostatectomy each year,2 and most are left with some degree of incontinence.
Years later, bladder control problems remain
Surgical advances have attempted to minimize nerve and bladder neck damage, but some degree of incontinence is still common after radical prostatectomy. According to the 2000 Prostate Cancer Outcomes Study, 80% of men experienced some incontinence 6 months after radical prostatectomy. After 2 years, 68% of men still had some degree of incontinence,3 and 8% reported frequent or total incontinence. Five years after prostatectomy, only 35% of patients reported complete bladder control vs 87% presurgery.4
A 2004 systematic review showed that behavioral therapy (mostly biofeedback) reduced symptoms in patients with all types of urinary incontinence.5 Many studies, including a 2010 Cochrane review,6 have shown that women with incontinence benefit from pelvic floor muscle training. No randomized trials have assessed the benefit of behavioral therapy for men with incontinence related to postprostatectomy—until now.
STUDY SUMMARY: Behavioral therapy has long-term payoff
The study by Goode et al was an RCT of behavioral therapy for men who had urinary incontinence after radical prostatectomy and whose symptoms persisted more than a year later. It included patients with ≥3 episodes of incontinence per week. Men were excluded if they were undergoing other treatment for prostate cancer, had a high postvoid residual volume or a history of certain bladder surgeries, or were unable to reliably report symptoms. Participants were permitted to continue taking medication for incontinence, with the exception of anticholinergics.
Participants (n=208 from 3 sites) were randomized to one of 3 arms in a blinded fashion with concealed allocation: behavioral therapy alone, behavioral therapy and biofeedback with electrical stimulation, or a control group of men who could elect to try these therapies at a later date.
Behavioral therapy consisted of 4 visits with a physician or nurse practitioner over an 8-week period. At the first visit, patients received instruction in pelvic floor muscle training. Patients then practiced contraction and relaxation exercises and urinary flow control at home. At the second visit, patients learned techniques to avoid episodes of incontinence, such as performing pelvic muscle contractions with stress symptom triggers. During the final 2 visits, patients received advice about control of persistent problems identified in symptom diaries they were required to keep. In addition, continued daily pelvic floor exercises were recommended at the last session.
Men in the group that received biofeedback with electrical stimulation had the same visit schedule, but received additional pelvic floor training—with electrode-mediated feedback and electrical stimulation of pelvic floor muscles during each visit and daily at home. Patients in the control group had the same visit frequency but received no treatment. After 8 weeks, however, the controls were given the opportunity to try behavioral therapy.
Baseline characteristics and attrition rates were similar in all 3 groups. Outcomes were based on an intention-to-treat analysis. At 8 weeks, men receiving behavioral therapy, with or without electrical stimulation and biofeedback, experienced a 55% decrease in incontinence (from 28 episodes per week at baseline to 13 per week); patients in the control group had a 24% decrease (from 25 episodes to 20 per week) (P=.001). More patients in the behavioral groups were completely continent at 8 weeks (16% vs 6% for the controls); the number needed to treat to achieve complete continence was 10. Electrical stimulation and biofeedback provided no added benefit compared with behavioral therapy alone.
Patients in the 2 treatment groups also had clinically significant benefits in some quality-of-life measures (impact of urinary symptoms on travel, emotion, and voiding) and in symptom-specific quality-of-life scores. Patient satisfaction at 8 weeks was higher in the treatment groups: 26 of the 58 men who received behavioral therapy were “delighted, pleased, or mostly satisfied,” vs 9 of 60 in the control group (P=.006 for overall group difference).
Adherence to the behavioral therapy protocol was 100% at 8 weeks and remained high (91%) one year later. Improvement in symptoms continued at one year, with patients in both treatment groups reporting a clinically significant (50%) reduction in incontinence episodes compared with baseline.
WHAT’S NEW: We have evidence-based help for postprostatectomy incontinence
We now have evidence that an 8-week program of pelvic floor training and bladder control strategies reduces the frequency of incontinence in men who have undergone radical prostatectomy.
CAVEATS: The effects of time weren’t factored in
Patients were obviously aware of group assignment, so there is the possibility of treatment bias contributing to the positive self-reported outcomes. While the treatment groups showed both a greater initial improvement and persistent improvement in their symptoms at one year, symptoms of patients in the control group were not measured after a year, so the sustained improvement could reflect resolution of incontinence with time.
CHALLENGES TO IMPLEMENTATION: Locating clinicians who can train patients
The type of behavioral therapy featured in this study may not be easily accessible to all patients. The researchers suggest consulting the National Association for Continence (http://www.nafc.org), a private nonprofit organization whose members include physical therapists, nurses, and physicians. They also cite the Wound Ostomy and Continence Nurses Society (http://www.wocn.org) as a resource in locating nurses who provide these services.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Recommend behavioral therapy—incorporating pelvic floor muscle training and bladder control strategies—to men experiencing incontinence after prostatectomy.1
STRENGTH OF RECOMMENDATION
B: Based on a single unblinded randomized controlled trial (RCT).
Goode PS, Burgio KL, Johnson TM, et al. Behavioral therapy with or without biofeedback and pelvic floor electrical stimulation for persistent postprostatectomy incontinence: a randomized controlled trial. JAMA. 2011;305:151-159.1
ILLUSTRATIVE CASE
Mr. H, age 75, underwent radical prostatectomy for prostate cancer a year ago. Since then, he leaks urine when he coughs and occasionally has complete loss of bladder control. His lack of control has forced him to curtail many of his normal activities and he wants to know what help you can provide.
Routine prostate-specific antigen (PSA) screening has led to an increase in the diagnosis of localized prostate cancer, and prostatectomy is a common treatment. Approximately 90,000 US men undergo radical prostatectomy each year,2 and most are left with some degree of incontinence.
Years later, bladder control problems remain
Surgical advances have attempted to minimize nerve and bladder neck damage, but some degree of incontinence is still common after radical prostatectomy. According to the 2000 Prostate Cancer Outcomes Study, 80% of men experienced some incontinence 6 months after radical prostatectomy. After 2 years, 68% of men still had some degree of incontinence,3 and 8% reported frequent or total incontinence. Five years after prostatectomy, only 35% of patients reported complete bladder control vs 87% presurgery.4
A 2004 systematic review showed that behavioral therapy (mostly biofeedback) reduced symptoms in patients with all types of urinary incontinence.5 Many studies, including a 2010 Cochrane review,6 have shown that women with incontinence benefit from pelvic floor muscle training. No randomized trials have assessed the benefit of behavioral therapy for men with incontinence related to postprostatectomy—until now.
STUDY SUMMARY: Behavioral therapy has long-term payoff
The study by Goode et al was an RCT of behavioral therapy for men who had urinary incontinence after radical prostatectomy and whose symptoms persisted more than a year later. It included patients with ≥3 episodes of incontinence per week. Men were excluded if they were undergoing other treatment for prostate cancer, had a high postvoid residual volume or a history of certain bladder surgeries, or were unable to reliably report symptoms. Participants were permitted to continue taking medication for incontinence, with the exception of anticholinergics.
Participants (n=208 from 3 sites) were randomized to one of 3 arms in a blinded fashion with concealed allocation: behavioral therapy alone, behavioral therapy and biofeedback with electrical stimulation, or a control group of men who could elect to try these therapies at a later date.
Behavioral therapy consisted of 4 visits with a physician or nurse practitioner over an 8-week period. At the first visit, patients received instruction in pelvic floor muscle training. Patients then practiced contraction and relaxation exercises and urinary flow control at home. At the second visit, patients learned techniques to avoid episodes of incontinence, such as performing pelvic muscle contractions with stress symptom triggers. During the final 2 visits, patients received advice about control of persistent problems identified in symptom diaries they were required to keep. In addition, continued daily pelvic floor exercises were recommended at the last session.
Men in the group that received biofeedback with electrical stimulation had the same visit schedule, but received additional pelvic floor training—with electrode-mediated feedback and electrical stimulation of pelvic floor muscles during each visit and daily at home. Patients in the control group had the same visit frequency but received no treatment. After 8 weeks, however, the controls were given the opportunity to try behavioral therapy.
Baseline characteristics and attrition rates were similar in all 3 groups. Outcomes were based on an intention-to-treat analysis. At 8 weeks, men receiving behavioral therapy, with or without electrical stimulation and biofeedback, experienced a 55% decrease in incontinence (from 28 episodes per week at baseline to 13 per week); patients in the control group had a 24% decrease (from 25 episodes to 20 per week) (P=.001). More patients in the behavioral groups were completely continent at 8 weeks (16% vs 6% for the controls); the number needed to treat to achieve complete continence was 10. Electrical stimulation and biofeedback provided no added benefit compared with behavioral therapy alone.
Patients in the 2 treatment groups also had clinically significant benefits in some quality-of-life measures (impact of urinary symptoms on travel, emotion, and voiding) and in symptom-specific quality-of-life scores. Patient satisfaction at 8 weeks was higher in the treatment groups: 26 of the 58 men who received behavioral therapy were “delighted, pleased, or mostly satisfied,” vs 9 of 60 in the control group (P=.006 for overall group difference).
Adherence to the behavioral therapy protocol was 100% at 8 weeks and remained high (91%) one year later. Improvement in symptoms continued at one year, with patients in both treatment groups reporting a clinically significant (50%) reduction in incontinence episodes compared with baseline.
WHAT’S NEW: We have evidence-based help for postprostatectomy incontinence
We now have evidence that an 8-week program of pelvic floor training and bladder control strategies reduces the frequency of incontinence in men who have undergone radical prostatectomy.
CAVEATS: The effects of time weren’t factored in
Patients were obviously aware of group assignment, so there is the possibility of treatment bias contributing to the positive self-reported outcomes. While the treatment groups showed both a greater initial improvement and persistent improvement in their symptoms at one year, symptoms of patients in the control group were not measured after a year, so the sustained improvement could reflect resolution of incontinence with time.
CHALLENGES TO IMPLEMENTATION: Locating clinicians who can train patients
The type of behavioral therapy featured in this study may not be easily accessible to all patients. The researchers suggest consulting the National Association for Continence (http://www.nafc.org), a private nonprofit organization whose members include physical therapists, nurses, and physicians. They also cite the Wound Ostomy and Continence Nurses Society (http://www.wocn.org) as a resource in locating nurses who provide these services.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Goode PS, Burgio KL, Johnson TM, et al. Behavioral therapy with or without biofeedback and pelvic floor electrical stimulation for persistent postprostatectomy incontinence: a randomized controlled trial. JAMA. 2011;305:151-159.
2. Barbash GI, Glied SA. New technology and health care costs—the case of robot-assisted surgery. N Engl J Med. 2010;363:701-704.
3. Stanford JL, Feng Z, Hamilton AS, et al. Urinary and sexual function after radical prostatectomy for clinically localized prostate cancer: the Prostate Cancer Outcomes Study. JAMA. 2000;283:354-360.
4. Penson DF, McLerran D, Feng Z, et al. 5-year urinary and sexual outcomes after radical prostatectomy: results from the prostate cancer outcomes study. J Urol. 2005;173:1701-1705.
5. Teunisse TA, de Jonge A, van Weel C, et al. Treating urinary incontinence in the elderly—conservative therapies that work: a systematic review. J Fam Pract. 2004;53:25-30, 32.
6. Dumoulin C, Hay-Smith J. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev. 2010;(1):CD005654.-
1. Goode PS, Burgio KL, Johnson TM, et al. Behavioral therapy with or without biofeedback and pelvic floor electrical stimulation for persistent postprostatectomy incontinence: a randomized controlled trial. JAMA. 2011;305:151-159.
2. Barbash GI, Glied SA. New technology and health care costs—the case of robot-assisted surgery. N Engl J Med. 2010;363:701-704.
3. Stanford JL, Feng Z, Hamilton AS, et al. Urinary and sexual function after radical prostatectomy for clinically localized prostate cancer: the Prostate Cancer Outcomes Study. JAMA. 2000;283:354-360.
4. Penson DF, McLerran D, Feng Z, et al. 5-year urinary and sexual outcomes after radical prostatectomy: results from the prostate cancer outcomes study. J Urol. 2005;173:1701-1705.
5. Teunisse TA, de Jonge A, van Weel C, et al. Treating urinary incontinence in the elderly—conservative therapies that work: a systematic review. J Fam Pract. 2004;53:25-30, 32.
6. Dumoulin C, Hay-Smith J. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev. 2010;(1):CD005654.-
Copyright © 2011 The Family Physicians Inquiries Network.
All rights reserved.
Another option for patients with liver disease
Consider prescribing rifaximin for patients with hepatic encephalopathy, not only as a treatment for acute episodes but also to prevent a recurrence.1
STRENGTH OF RECOMMENDATION:
A: Based on a high-quality randomized controlled trial (RCT)
Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362:1071-1081.
ILLUSTRATIVE CASE
A 64-year-old patient with chronic liver disease has been hospitalized on 3 occasions for hepatic encephalopathy, all while he was taking lactulose. He is still taking it, but wonders if there are other ways to prevent future episodes of hepatic encephalopathy. What can you tell him?
Characterized by periods of impaired cognition of varying severity, hepatic encephalopathy is a common complication of chronic liver disease—and a frequent cause of hospitalization, morbidity, and mortality in this patient population. Up to 70% of patients with cirrhosis may have some degree of hepatic encephalopathy,2 which can occur without provocation or be triggered by gastrointestinal (GI) bleeding, infection, kidney disease, electrolyte abnormalities, shunt placement, respiratory disease, or anemia. Hepatic encephalopathy is thought to be caused by elevated ammonia levels.
Current first-line treatment is not problem-free
Patients with chronic liver disease and hepatic encephalopathy are often placed on nonabsorbable disaccharides, such as lactulose, to prevent recurrent hepatic encephalopathy. However, disaccharides’ effectiveness as prophylaxis is unproven.3 In addition, many patients have difficulty tolerating lactulose because of its taste and GI side effects.
A 2004 Cochrane review examined the effectiveness of lactulose in preventing hepatic encephalopathy.3 The reviewers also compared the effectiveness of an oral antibiotic, rifaximin, with lactulose for this purpose. Rifaximin, like lactu-lose, is believed to work by reducing ammonia in the gut. The antibiotic is a well-established treatment for acute hepatic encephalopathy, but not widely used for preventive purposes.
The reviewers found rifaximin to be more effective compared with lactulose at preventing recurrent episodes of hepatic encephalopathy (number needed to treat [NNT]=11).3 Other studies have also suggested that the antibiotic, which has minimal systemic absorption, may be as effective as, or more effective than, lactu-lose in preventing recurrences.4,5 The new RCT detailed in this PURL took another look at rifaximin’s usefulness as prophylaxis.
STUDY SUMMARY: Patients on rifaximin had better outcomes
The study by Bass et al was a double-blinded RCT enrolling 299 patients with chronic liver disease.1 Criteria for inclusion were age ≥18 years, a minimum of 2 prior episodes of hepatic encephalopathy, remission from hepatic encephalopathy at the time of enrollment, and mild to moderate liver disease severity, defined as a score ≤25 on the Model for End-Stage Liver Disease (MELD) scale.6 (The scale ranges from 6 to 40, with higher numbers indicating more severe disease.) The researchers excluded patients for whom liver transplant was imminent and those with conditions that precipitate hepatic encephalopathy, as described earlier.
Patients were assigned to either rifaximin 550 mg twice a day (140 patients) or placebo (159 patients) for 6 months. Both groups had similar baseline characteristics, including a high percentage of subjects (>90%) with concomitant lactulose use. The researchers assessed the patients at clinic visits every 2 weeks, both by their Conn score (the scale commonly used to grade hepatic encephalopathy) and grade of asterixis, and during telephone calls on alternate weeks. Analysis was by intention-to-treat.
The primary endpoint was the mean time to the first episode of hepatic encephalopathy, which was 130.0 (±56.5) days in the rifaximin group and 105.7 (±62.7) days in the control group. During the 6-month study period, 22% of patients in the rifaximin group experienced a breakthrough hepatic encephalopathy event, vs 45.9% of the placebo group (95% confidence interval, 0.28-0.64; P<0.001; hazard ratio=0.42; NNT=9). Both groups had high rates of compliance (~84%) and high rates of adverse events (80%). Two patients receiving rifaximin experienced Clostridium difficile infections, from which they recovered. Death rates were similar in both groups, and were attributed to liver disease progression.
WHAT’S NEW?: FDA approves rifaximin to prevent recurrence
This trial adds further support for the use of rifaximin in the prevention of recurrent episodes of hepatic encephalopathy. In addition, the US Food and Drug Administration approved the antibiotic for that purpose in March of this year.7 Given the lack of proven, well-tolerated treatments to prevent hepatic encephalopathy in patients with liver disease and the significant morbidity and mortality associated with this complication, family physicians should consider prescribing rifaximin for patients with prior episodes of hepatic encephalopathy. Rifaximin resistance is not common and, because its activity is concentrated in the gut, resistance is unlikely to become a significant issue.
CAVEATS: Long-term safety has not been established
Because of this study’s short duration (6 months) and relatively small sample size, we cannot be certain of its long-term effects or safety. However, patients with advanced liver disease and recurrent hepatic encephalopathy have a poor prognosis, and a treatment that is effective, even if just for 6 months, is meaningful.
Also, because this study excluded patients with more severe liver disease (MELD score >25), we have no data to guide the use of rifaximin in this patient population. However, the mechanism of action and risk of adverse effects are likely to be similar.
Finally, the manufacturer of the drug was involved in the study design, data collection, data analysis, and manuscript preparation.
CHALLENGES TO IMPLEMENTATION: Drug cost and coverage are potential barriers
Rifaximin is available in the United States in 200- and 550-mg tablets, so it can be dosed at 1100 or 1200 mg per day in divided doses. The drug is not generic, however, and is costly: A month’s supply of the 550-mg tablets is about $1300 (a supply of the 200-mg tablets is even more expensive),8 and the drug may not be covered by insurance.
Acknowledgement
The PURls Surveillance System is supported in part by Grant number UL1RR024999 from the National Center for Research Resources; the grant was a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362:1071-1081.
2. Riordan SM, Williams R. Treatment of hepatic encephalopathy. N Engl J Med. 1997;337:473-479.
3. Als-Nielsen B, Gluud LL, Gluud C. Nonabsorbable disaccharides for hepatic encephalopathy. Cochrane Database Syst Rev. 2004;(2):CD003044.-
4. Paik YH, Lee KS, Han KH, et al. Comparison of rifaximin and lactulose for the treatment of hepatic encephalopathy: a prospective randomized study. Yonsei Med J. 2005;46:399-407.
5. Lawrence KR, Klee JA. Rifaximin for the treatment of hepatic encephalopathy. Pharmacotherapy. 2008;28:1019-1032.
6. Mayo Clinic. The MELD model, UNOS modification. Available at: http://www.mayoclinic.org/meld/mayomodel6.html. Accessed August 16, 2010.
7. US Food and Drug Administration. FDA approves new use of Xifaxan for patients with liver disease. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm206104.htm. Updated March 26, 2010. Accessed July 7, 2010.
8. Drugstore.com. Available at: http://www.drugstore.com/. Accessed August 20, 2010.
Consider prescribing rifaximin for patients with hepatic encephalopathy, not only as a treatment for acute episodes but also to prevent a recurrence.1
STRENGTH OF RECOMMENDATION:
A: Based on a high-quality randomized controlled trial (RCT)
Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362:1071-1081.
ILLUSTRATIVE CASE
A 64-year-old patient with chronic liver disease has been hospitalized on 3 occasions for hepatic encephalopathy, all while he was taking lactulose. He is still taking it, but wonders if there are other ways to prevent future episodes of hepatic encephalopathy. What can you tell him?
Characterized by periods of impaired cognition of varying severity, hepatic encephalopathy is a common complication of chronic liver disease—and a frequent cause of hospitalization, morbidity, and mortality in this patient population. Up to 70% of patients with cirrhosis may have some degree of hepatic encephalopathy,2 which can occur without provocation or be triggered by gastrointestinal (GI) bleeding, infection, kidney disease, electrolyte abnormalities, shunt placement, respiratory disease, or anemia. Hepatic encephalopathy is thought to be caused by elevated ammonia levels.
Current first-line treatment is not problem-free
Patients with chronic liver disease and hepatic encephalopathy are often placed on nonabsorbable disaccharides, such as lactulose, to prevent recurrent hepatic encephalopathy. However, disaccharides’ effectiveness as prophylaxis is unproven.3 In addition, many patients have difficulty tolerating lactulose because of its taste and GI side effects.
A 2004 Cochrane review examined the effectiveness of lactulose in preventing hepatic encephalopathy.3 The reviewers also compared the effectiveness of an oral antibiotic, rifaximin, with lactulose for this purpose. Rifaximin, like lactu-lose, is believed to work by reducing ammonia in the gut. The antibiotic is a well-established treatment for acute hepatic encephalopathy, but not widely used for preventive purposes.
The reviewers found rifaximin to be more effective compared with lactulose at preventing recurrent episodes of hepatic encephalopathy (number needed to treat [NNT]=11).3 Other studies have also suggested that the antibiotic, which has minimal systemic absorption, may be as effective as, or more effective than, lactu-lose in preventing recurrences.4,5 The new RCT detailed in this PURL took another look at rifaximin’s usefulness as prophylaxis.
STUDY SUMMARY: Patients on rifaximin had better outcomes
The study by Bass et al was a double-blinded RCT enrolling 299 patients with chronic liver disease.1 Criteria for inclusion were age ≥18 years, a minimum of 2 prior episodes of hepatic encephalopathy, remission from hepatic encephalopathy at the time of enrollment, and mild to moderate liver disease severity, defined as a score ≤25 on the Model for End-Stage Liver Disease (MELD) scale.6 (The scale ranges from 6 to 40, with higher numbers indicating more severe disease.) The researchers excluded patients for whom liver transplant was imminent and those with conditions that precipitate hepatic encephalopathy, as described earlier.
Patients were assigned to either rifaximin 550 mg twice a day (140 patients) or placebo (159 patients) for 6 months. Both groups had similar baseline characteristics, including a high percentage of subjects (>90%) with concomitant lactulose use. The researchers assessed the patients at clinic visits every 2 weeks, both by their Conn score (the scale commonly used to grade hepatic encephalopathy) and grade of asterixis, and during telephone calls on alternate weeks. Analysis was by intention-to-treat.
The primary endpoint was the mean time to the first episode of hepatic encephalopathy, which was 130.0 (±56.5) days in the rifaximin group and 105.7 (±62.7) days in the control group. During the 6-month study period, 22% of patients in the rifaximin group experienced a breakthrough hepatic encephalopathy event, vs 45.9% of the placebo group (95% confidence interval, 0.28-0.64; P<0.001; hazard ratio=0.42; NNT=9). Both groups had high rates of compliance (~84%) and high rates of adverse events (80%). Two patients receiving rifaximin experienced Clostridium difficile infections, from which they recovered. Death rates were similar in both groups, and were attributed to liver disease progression.
WHAT’S NEW?: FDA approves rifaximin to prevent recurrence
This trial adds further support for the use of rifaximin in the prevention of recurrent episodes of hepatic encephalopathy. In addition, the US Food and Drug Administration approved the antibiotic for that purpose in March of this year.7 Given the lack of proven, well-tolerated treatments to prevent hepatic encephalopathy in patients with liver disease and the significant morbidity and mortality associated with this complication, family physicians should consider prescribing rifaximin for patients with prior episodes of hepatic encephalopathy. Rifaximin resistance is not common and, because its activity is concentrated in the gut, resistance is unlikely to become a significant issue.
CAVEATS: Long-term safety has not been established
Because of this study’s short duration (6 months) and relatively small sample size, we cannot be certain of its long-term effects or safety. However, patients with advanced liver disease and recurrent hepatic encephalopathy have a poor prognosis, and a treatment that is effective, even if just for 6 months, is meaningful.
Also, because this study excluded patients with more severe liver disease (MELD score >25), we have no data to guide the use of rifaximin in this patient population. However, the mechanism of action and risk of adverse effects are likely to be similar.
Finally, the manufacturer of the drug was involved in the study design, data collection, data analysis, and manuscript preparation.
CHALLENGES TO IMPLEMENTATION: Drug cost and coverage are potential barriers
Rifaximin is available in the United States in 200- and 550-mg tablets, so it can be dosed at 1100 or 1200 mg per day in divided doses. The drug is not generic, however, and is costly: A month’s supply of the 550-mg tablets is about $1300 (a supply of the 200-mg tablets is even more expensive),8 and the drug may not be covered by insurance.
Acknowledgement
The PURls Surveillance System is supported in part by Grant number UL1RR024999 from the National Center for Research Resources; the grant was a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Consider prescribing rifaximin for patients with hepatic encephalopathy, not only as a treatment for acute episodes but also to prevent a recurrence.1
STRENGTH OF RECOMMENDATION:
A: Based on a high-quality randomized controlled trial (RCT)
Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362:1071-1081.
ILLUSTRATIVE CASE
A 64-year-old patient with chronic liver disease has been hospitalized on 3 occasions for hepatic encephalopathy, all while he was taking lactulose. He is still taking it, but wonders if there are other ways to prevent future episodes of hepatic encephalopathy. What can you tell him?
Characterized by periods of impaired cognition of varying severity, hepatic encephalopathy is a common complication of chronic liver disease—and a frequent cause of hospitalization, morbidity, and mortality in this patient population. Up to 70% of patients with cirrhosis may have some degree of hepatic encephalopathy,2 which can occur without provocation or be triggered by gastrointestinal (GI) bleeding, infection, kidney disease, electrolyte abnormalities, shunt placement, respiratory disease, or anemia. Hepatic encephalopathy is thought to be caused by elevated ammonia levels.
Current first-line treatment is not problem-free
Patients with chronic liver disease and hepatic encephalopathy are often placed on nonabsorbable disaccharides, such as lactulose, to prevent recurrent hepatic encephalopathy. However, disaccharides’ effectiveness as prophylaxis is unproven.3 In addition, many patients have difficulty tolerating lactulose because of its taste and GI side effects.
A 2004 Cochrane review examined the effectiveness of lactulose in preventing hepatic encephalopathy.3 The reviewers also compared the effectiveness of an oral antibiotic, rifaximin, with lactulose for this purpose. Rifaximin, like lactu-lose, is believed to work by reducing ammonia in the gut. The antibiotic is a well-established treatment for acute hepatic encephalopathy, but not widely used for preventive purposes.
The reviewers found rifaximin to be more effective compared with lactulose at preventing recurrent episodes of hepatic encephalopathy (number needed to treat [NNT]=11).3 Other studies have also suggested that the antibiotic, which has minimal systemic absorption, may be as effective as, or more effective than, lactu-lose in preventing recurrences.4,5 The new RCT detailed in this PURL took another look at rifaximin’s usefulness as prophylaxis.
STUDY SUMMARY: Patients on rifaximin had better outcomes
The study by Bass et al was a double-blinded RCT enrolling 299 patients with chronic liver disease.1 Criteria for inclusion were age ≥18 years, a minimum of 2 prior episodes of hepatic encephalopathy, remission from hepatic encephalopathy at the time of enrollment, and mild to moderate liver disease severity, defined as a score ≤25 on the Model for End-Stage Liver Disease (MELD) scale.6 (The scale ranges from 6 to 40, with higher numbers indicating more severe disease.) The researchers excluded patients for whom liver transplant was imminent and those with conditions that precipitate hepatic encephalopathy, as described earlier.
Patients were assigned to either rifaximin 550 mg twice a day (140 patients) or placebo (159 patients) for 6 months. Both groups had similar baseline characteristics, including a high percentage of subjects (>90%) with concomitant lactulose use. The researchers assessed the patients at clinic visits every 2 weeks, both by their Conn score (the scale commonly used to grade hepatic encephalopathy) and grade of asterixis, and during telephone calls on alternate weeks. Analysis was by intention-to-treat.
The primary endpoint was the mean time to the first episode of hepatic encephalopathy, which was 130.0 (±56.5) days in the rifaximin group and 105.7 (±62.7) days in the control group. During the 6-month study period, 22% of patients in the rifaximin group experienced a breakthrough hepatic encephalopathy event, vs 45.9% of the placebo group (95% confidence interval, 0.28-0.64; P<0.001; hazard ratio=0.42; NNT=9). Both groups had high rates of compliance (~84%) and high rates of adverse events (80%). Two patients receiving rifaximin experienced Clostridium difficile infections, from which they recovered. Death rates were similar in both groups, and were attributed to liver disease progression.
WHAT’S NEW?: FDA approves rifaximin to prevent recurrence
This trial adds further support for the use of rifaximin in the prevention of recurrent episodes of hepatic encephalopathy. In addition, the US Food and Drug Administration approved the antibiotic for that purpose in March of this year.7 Given the lack of proven, well-tolerated treatments to prevent hepatic encephalopathy in patients with liver disease and the significant morbidity and mortality associated with this complication, family physicians should consider prescribing rifaximin for patients with prior episodes of hepatic encephalopathy. Rifaximin resistance is not common and, because its activity is concentrated in the gut, resistance is unlikely to become a significant issue.
CAVEATS: Long-term safety has not been established
Because of this study’s short duration (6 months) and relatively small sample size, we cannot be certain of its long-term effects or safety. However, patients with advanced liver disease and recurrent hepatic encephalopathy have a poor prognosis, and a treatment that is effective, even if just for 6 months, is meaningful.
Also, because this study excluded patients with more severe liver disease (MELD score >25), we have no data to guide the use of rifaximin in this patient population. However, the mechanism of action and risk of adverse effects are likely to be similar.
Finally, the manufacturer of the drug was involved in the study design, data collection, data analysis, and manuscript preparation.
CHALLENGES TO IMPLEMENTATION: Drug cost and coverage are potential barriers
Rifaximin is available in the United States in 200- and 550-mg tablets, so it can be dosed at 1100 or 1200 mg per day in divided doses. The drug is not generic, however, and is costly: A month’s supply of the 550-mg tablets is about $1300 (a supply of the 200-mg tablets is even more expensive),8 and the drug may not be covered by insurance.
Acknowledgement
The PURls Surveillance System is supported in part by Grant number UL1RR024999 from the National Center for Research Resources; the grant was a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362:1071-1081.
2. Riordan SM, Williams R. Treatment of hepatic encephalopathy. N Engl J Med. 1997;337:473-479.
3. Als-Nielsen B, Gluud LL, Gluud C. Nonabsorbable disaccharides for hepatic encephalopathy. Cochrane Database Syst Rev. 2004;(2):CD003044.-
4. Paik YH, Lee KS, Han KH, et al. Comparison of rifaximin and lactulose for the treatment of hepatic encephalopathy: a prospective randomized study. Yonsei Med J. 2005;46:399-407.
5. Lawrence KR, Klee JA. Rifaximin for the treatment of hepatic encephalopathy. Pharmacotherapy. 2008;28:1019-1032.
6. Mayo Clinic. The MELD model, UNOS modification. Available at: http://www.mayoclinic.org/meld/mayomodel6.html. Accessed August 16, 2010.
7. US Food and Drug Administration. FDA approves new use of Xifaxan for patients with liver disease. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm206104.htm. Updated March 26, 2010. Accessed July 7, 2010.
8. Drugstore.com. Available at: http://www.drugstore.com/. Accessed August 20, 2010.
1. Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362:1071-1081.
2. Riordan SM, Williams R. Treatment of hepatic encephalopathy. N Engl J Med. 1997;337:473-479.
3. Als-Nielsen B, Gluud LL, Gluud C. Nonabsorbable disaccharides for hepatic encephalopathy. Cochrane Database Syst Rev. 2004;(2):CD003044.-
4. Paik YH, Lee KS, Han KH, et al. Comparison of rifaximin and lactulose for the treatment of hepatic encephalopathy: a prospective randomized study. Yonsei Med J. 2005;46:399-407.
5. Lawrence KR, Klee JA. Rifaximin for the treatment of hepatic encephalopathy. Pharmacotherapy. 2008;28:1019-1032.
6. Mayo Clinic. The MELD model, UNOS modification. Available at: http://www.mayoclinic.org/meld/mayomodel6.html. Accessed August 16, 2010.
7. US Food and Drug Administration. FDA approves new use of Xifaxan for patients with liver disease. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm206104.htm. Updated March 26, 2010. Accessed July 7, 2010.
8. Drugstore.com. Available at: http://www.drugstore.com/. Accessed August 20, 2010.
Copyright © 2010 The Family Physicians Inquiries Network.
All rights reserved.
Bisphosphonate therapy: When not to monitor BMD
After starting patients on bisphosphonates for osteoporosis, wait at least 3 years before ordering a repeat dual-energy x-ray absorptiometry (DXA) scan.1
STRENGTH OF RECOMMENDATION
C: Based on a secondary analysis of a large randomized controlled trial.
Bell KL, Hayen A, Macaskill P, et al. Value of routine monitoring of bone mineral density after starting bisphosphonate treatment: secondary analysis of treatment data. BMJ. 2009;338:b2266.
ILLUSTRATIVE CASE
CASE: Ms. K, a 68-year-old woman diagnosed with osteoporosis on a screening DXA scan a year ago, has been taking a bisphosphonate ever since. She’s anxious to know whether the medication is working and asks if it’s time for a repeat DXA scan. What should you tell her?
Fragility fractures from osteoporosis are common in postmenopausal women. In the year 2000 alone, an estimated 9 million such fractures occurred worldwide.2 Treatment with bisphosphonates has been found to reduce the risk of fragility fractures,3 and the United States Preventive Services Task Force (USPSTF) recommends a DXA scan to screen for osteoporosis in women older than 65 years and some younger women at increased risk.4
Monitoring treatment: How often?
Although recommendations for how often to monitor bone mineral density (BMD) after initiating treatment vary, the consensus has been that periodic monitoring is useful. But there have been no randomized trials evaluating BMD testing in patients taking bisphosphonates.
The use of DXA scans to identify osteoporosis has been shown to be a cost-effective strategy in women older than 65 years,5 but there has not been a cost/benefit analysis of follow-up DXA scanning after initiating treatment. The cost of a scan ranges from about $150 to $300, and it is not known how many patients undergo repeat DXA scanning after starting treatment.
STUDY SUMMARY: Yearly scans are not helpful
The study we report on here is a secondary analysis of data from the Fracture Intervention Trial (FIT).6 In 1993, FIT randomized 6457 US women ages 55 to 80 years with low hip bone density to either alendronate or placebo. The initial dose of alendronate was 5 mg/d, but was later increased to 10 mg/d when other studies found that the higher dose was more effective. FIT showed that alendronate increased BMD and decreased the risk of vertebral fracture.7
Bell et al1 used a mixed-model statistical analysis to compare “within-person variation” in BMD (variation in DXA results over time in individuals) and “between-person variation” in BMD (variation in DXA results over time in the population of patients). The BMD of all FIT participants in both the control and treatment groups was measured at baseline and at the 1-, 2-, and 3-year marks. Each individual was always tested on the same scanner to minimize differences in machinery.
Individual results vary from year to year. The researchers found that the within-person variation was about 10 times greater than the between-person variation. This finding suggests that the precision of DXA scan measurements is not that reliable from 1 test to another.
The average annual increase in BMD in patients in the alendronate group was 0.0085 g/cm2—which is smaller than the typical year-to-year (within-person) variation of 0.013 g/cm2. It would therefore be difficult to differentiate the medication’s effect from the random variation inherent in DXA scans.
Response is favorable after 3 years of treatment. While there is variation in test results from year to year, longer-term findings are more reliable. After 3 years of treatment, 97.5% of patients taking alendronate had an increase in hip BMD of at least 0.019 g/cm2, with a strong correlation between hip and spine measurements. Although this represents a relatively small change in Z and T scores, this increase in hip BMD is considered a favorable response that warrants continued treatment. These findings are consistent with a previous analysis of BMD monitoring in women taking bisphosphonates, in which those who had the largest drop in BMD after the first year of treatment typically had a large gain over the second year.8
WHAT’S NEW: Now we know early testing is unnecessary
Not many studies are available to provide guidance about the interval between BMD measurements after starting a bisphosphonate. This study advises us that it is not necessary to recheck BMD for at least 3 years after starting treatment. Elimination of early repeat DXA testing could result in significant cost savings.
CAVEATS: Findings contradict usual recommendations
Physicians should be aware that the conclusion of this study is not in line with recommendations from a number of prominent organizations. The American Association of Clinical Endocrinology,9 the National Osteoporosis Foundation,10 and the North American Menopause Society11 all recommend follow-up DXA testing in 1 or 2 years.
High-risk patient exception. The delay in repeat DXA testing may not be appropriate for patients at higher risk of bone density loss. However, a separate analysis of higher-risk groups was not done.
Finally, while the findings of Bell et al suggest that we should wait at least 3 years before retesting, it is still not clear whether there is any benefit to repeat DXA testing at any interval, given the nearly universal response rate. It is also possible that advances in DXA technology will reduce some of the variation in BMD results.
CHALLENGES TO IMPLEMENTATION: Anxious patients
Patients like Ms. K may ask their physicians to retest well before 3 years. Yet those who undergo scanning after a shorter interval may be discouraged by early results. Advising patients that the treatment is almost uniformly effective in increasing BMD should reassure them that sticking with treatment is worthwhile.
Acknowledgment
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Bell KL, Hayen A, Macaskill P, et al. Value of routine monitoring of bone mineral density after starting bisphosphonate treatment: secondary analysis of treatment data. BMJ. 2009;338:b2266.-
2. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17:1726.-
3. MacLean C, Newberry S, et al. Systematic review: comparative effectiveness of treatments to prevent fractures in men and women with low bone density or osteoporosis. Ann Intern Med. 2008;148:197-213.
4. Agency for Healthcare Research and Quality United States Preventive Services Task Force. Screening for osteoporosis in postmenopausal women. Available at: http://www.ahrq.gov/clinic/3rduspstf/osteoporosis/osteorr.htm . Accessed October 13, 2009.
5. Schousboe JT. Cost effectiveness of screen-and-treat strategies for low bone mineral density: how do we screen, who do we screen, and who do we treat? Appl Health Econ Health Policy. 2008;6:1-18.
6. Black DM, Nevitt MC, Cauley J, et al. Design of the fracture intervention trial. Osteopor Int. 2003;3(suppl 3):S29-S39.
7. Cummings S, Black D, Thompson D, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures. JAMA. 1998;280:2077-2082.
8. Cummings S, Palermo B, Browner W, et al. Monitoring osteoporosis therapy with bone densitometry: misleading changes and regression to the mean. Fracture Intervention Trial Research Group. JAMA. 2000;283:1318-1321.
9. AACE Osteoporosis Task Force American Association of Clinical Endocrinologists medical guidelines for clinical practice for the prevention and treatment of postmenopausal osteoporosis: 2001 edition with selected updates for 2003. Endocr Pract. 2003;9:544-564.
10. National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of Osteoporosis. Washington DC: NOF; 2008.
11. Management of postmenopausal osteoporosis: position statement of the North American Menopause Society Menopause. 2002;9:84-101.
After starting patients on bisphosphonates for osteoporosis, wait at least 3 years before ordering a repeat dual-energy x-ray absorptiometry (DXA) scan.1
STRENGTH OF RECOMMENDATION
C: Based on a secondary analysis of a large randomized controlled trial.
Bell KL, Hayen A, Macaskill P, et al. Value of routine monitoring of bone mineral density after starting bisphosphonate treatment: secondary analysis of treatment data. BMJ. 2009;338:b2266.
ILLUSTRATIVE CASE
CASE: Ms. K, a 68-year-old woman diagnosed with osteoporosis on a screening DXA scan a year ago, has been taking a bisphosphonate ever since. She’s anxious to know whether the medication is working and asks if it’s time for a repeat DXA scan. What should you tell her?
Fragility fractures from osteoporosis are common in postmenopausal women. In the year 2000 alone, an estimated 9 million such fractures occurred worldwide.2 Treatment with bisphosphonates has been found to reduce the risk of fragility fractures,3 and the United States Preventive Services Task Force (USPSTF) recommends a DXA scan to screen for osteoporosis in women older than 65 years and some younger women at increased risk.4
Monitoring treatment: How often?
Although recommendations for how often to monitor bone mineral density (BMD) after initiating treatment vary, the consensus has been that periodic monitoring is useful. But there have been no randomized trials evaluating BMD testing in patients taking bisphosphonates.
The use of DXA scans to identify osteoporosis has been shown to be a cost-effective strategy in women older than 65 years,5 but there has not been a cost/benefit analysis of follow-up DXA scanning after initiating treatment. The cost of a scan ranges from about $150 to $300, and it is not known how many patients undergo repeat DXA scanning after starting treatment.
STUDY SUMMARY: Yearly scans are not helpful
The study we report on here is a secondary analysis of data from the Fracture Intervention Trial (FIT).6 In 1993, FIT randomized 6457 US women ages 55 to 80 years with low hip bone density to either alendronate or placebo. The initial dose of alendronate was 5 mg/d, but was later increased to 10 mg/d when other studies found that the higher dose was more effective. FIT showed that alendronate increased BMD and decreased the risk of vertebral fracture.7
Bell et al1 used a mixed-model statistical analysis to compare “within-person variation” in BMD (variation in DXA results over time in individuals) and “between-person variation” in BMD (variation in DXA results over time in the population of patients). The BMD of all FIT participants in both the control and treatment groups was measured at baseline and at the 1-, 2-, and 3-year marks. Each individual was always tested on the same scanner to minimize differences in machinery.
Individual results vary from year to year. The researchers found that the within-person variation was about 10 times greater than the between-person variation. This finding suggests that the precision of DXA scan measurements is not that reliable from 1 test to another.
The average annual increase in BMD in patients in the alendronate group was 0.0085 g/cm2—which is smaller than the typical year-to-year (within-person) variation of 0.013 g/cm2. It would therefore be difficult to differentiate the medication’s effect from the random variation inherent in DXA scans.
Response is favorable after 3 years of treatment. While there is variation in test results from year to year, longer-term findings are more reliable. After 3 years of treatment, 97.5% of patients taking alendronate had an increase in hip BMD of at least 0.019 g/cm2, with a strong correlation between hip and spine measurements. Although this represents a relatively small change in Z and T scores, this increase in hip BMD is considered a favorable response that warrants continued treatment. These findings are consistent with a previous analysis of BMD monitoring in women taking bisphosphonates, in which those who had the largest drop in BMD after the first year of treatment typically had a large gain over the second year.8
WHAT’S NEW: Now we know early testing is unnecessary
Not many studies are available to provide guidance about the interval between BMD measurements after starting a bisphosphonate. This study advises us that it is not necessary to recheck BMD for at least 3 years after starting treatment. Elimination of early repeat DXA testing could result in significant cost savings.
CAVEATS: Findings contradict usual recommendations
Physicians should be aware that the conclusion of this study is not in line with recommendations from a number of prominent organizations. The American Association of Clinical Endocrinology,9 the National Osteoporosis Foundation,10 and the North American Menopause Society11 all recommend follow-up DXA testing in 1 or 2 years.
High-risk patient exception. The delay in repeat DXA testing may not be appropriate for patients at higher risk of bone density loss. However, a separate analysis of higher-risk groups was not done.
Finally, while the findings of Bell et al suggest that we should wait at least 3 years before retesting, it is still not clear whether there is any benefit to repeat DXA testing at any interval, given the nearly universal response rate. It is also possible that advances in DXA technology will reduce some of the variation in BMD results.
CHALLENGES TO IMPLEMENTATION: Anxious patients
Patients like Ms. K may ask their physicians to retest well before 3 years. Yet those who undergo scanning after a shorter interval may be discouraged by early results. Advising patients that the treatment is almost uniformly effective in increasing BMD should reassure them that sticking with treatment is worthwhile.
Acknowledgment
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
After starting patients on bisphosphonates for osteoporosis, wait at least 3 years before ordering a repeat dual-energy x-ray absorptiometry (DXA) scan.1
STRENGTH OF RECOMMENDATION
C: Based on a secondary analysis of a large randomized controlled trial.
Bell KL, Hayen A, Macaskill P, et al. Value of routine monitoring of bone mineral density after starting bisphosphonate treatment: secondary analysis of treatment data. BMJ. 2009;338:b2266.
ILLUSTRATIVE CASE
CASE: Ms. K, a 68-year-old woman diagnosed with osteoporosis on a screening DXA scan a year ago, has been taking a bisphosphonate ever since. She’s anxious to know whether the medication is working and asks if it’s time for a repeat DXA scan. What should you tell her?
Fragility fractures from osteoporosis are common in postmenopausal women. In the year 2000 alone, an estimated 9 million such fractures occurred worldwide.2 Treatment with bisphosphonates has been found to reduce the risk of fragility fractures,3 and the United States Preventive Services Task Force (USPSTF) recommends a DXA scan to screen for osteoporosis in women older than 65 years and some younger women at increased risk.4
Monitoring treatment: How often?
Although recommendations for how often to monitor bone mineral density (BMD) after initiating treatment vary, the consensus has been that periodic monitoring is useful. But there have been no randomized trials evaluating BMD testing in patients taking bisphosphonates.
The use of DXA scans to identify osteoporosis has been shown to be a cost-effective strategy in women older than 65 years,5 but there has not been a cost/benefit analysis of follow-up DXA scanning after initiating treatment. The cost of a scan ranges from about $150 to $300, and it is not known how many patients undergo repeat DXA scanning after starting treatment.
STUDY SUMMARY: Yearly scans are not helpful
The study we report on here is a secondary analysis of data from the Fracture Intervention Trial (FIT).6 In 1993, FIT randomized 6457 US women ages 55 to 80 years with low hip bone density to either alendronate or placebo. The initial dose of alendronate was 5 mg/d, but was later increased to 10 mg/d when other studies found that the higher dose was more effective. FIT showed that alendronate increased BMD and decreased the risk of vertebral fracture.7
Bell et al1 used a mixed-model statistical analysis to compare “within-person variation” in BMD (variation in DXA results over time in individuals) and “between-person variation” in BMD (variation in DXA results over time in the population of patients). The BMD of all FIT participants in both the control and treatment groups was measured at baseline and at the 1-, 2-, and 3-year marks. Each individual was always tested on the same scanner to minimize differences in machinery.
Individual results vary from year to year. The researchers found that the within-person variation was about 10 times greater than the between-person variation. This finding suggests that the precision of DXA scan measurements is not that reliable from 1 test to another.
The average annual increase in BMD in patients in the alendronate group was 0.0085 g/cm2—which is smaller than the typical year-to-year (within-person) variation of 0.013 g/cm2. It would therefore be difficult to differentiate the medication’s effect from the random variation inherent in DXA scans.
Response is favorable after 3 years of treatment. While there is variation in test results from year to year, longer-term findings are more reliable. After 3 years of treatment, 97.5% of patients taking alendronate had an increase in hip BMD of at least 0.019 g/cm2, with a strong correlation between hip and spine measurements. Although this represents a relatively small change in Z and T scores, this increase in hip BMD is considered a favorable response that warrants continued treatment. These findings are consistent with a previous analysis of BMD monitoring in women taking bisphosphonates, in which those who had the largest drop in BMD after the first year of treatment typically had a large gain over the second year.8
WHAT’S NEW: Now we know early testing is unnecessary
Not many studies are available to provide guidance about the interval between BMD measurements after starting a bisphosphonate. This study advises us that it is not necessary to recheck BMD for at least 3 years after starting treatment. Elimination of early repeat DXA testing could result in significant cost savings.
CAVEATS: Findings contradict usual recommendations
Physicians should be aware that the conclusion of this study is not in line with recommendations from a number of prominent organizations. The American Association of Clinical Endocrinology,9 the National Osteoporosis Foundation,10 and the North American Menopause Society11 all recommend follow-up DXA testing in 1 or 2 years.
High-risk patient exception. The delay in repeat DXA testing may not be appropriate for patients at higher risk of bone density loss. However, a separate analysis of higher-risk groups was not done.
Finally, while the findings of Bell et al suggest that we should wait at least 3 years before retesting, it is still not clear whether there is any benefit to repeat DXA testing at any interval, given the nearly universal response rate. It is also possible that advances in DXA technology will reduce some of the variation in BMD results.
CHALLENGES TO IMPLEMENTATION: Anxious patients
Patients like Ms. K may ask their physicians to retest well before 3 years. Yet those who undergo scanning after a shorter interval may be discouraged by early results. Advising patients that the treatment is almost uniformly effective in increasing BMD should reassure them that sticking with treatment is worthwhile.
Acknowledgment
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Bell KL, Hayen A, Macaskill P, et al. Value of routine monitoring of bone mineral density after starting bisphosphonate treatment: secondary analysis of treatment data. BMJ. 2009;338:b2266.-
2. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17:1726.-
3. MacLean C, Newberry S, et al. Systematic review: comparative effectiveness of treatments to prevent fractures in men and women with low bone density or osteoporosis. Ann Intern Med. 2008;148:197-213.
4. Agency for Healthcare Research and Quality United States Preventive Services Task Force. Screening for osteoporosis in postmenopausal women. Available at: http://www.ahrq.gov/clinic/3rduspstf/osteoporosis/osteorr.htm . Accessed October 13, 2009.
5. Schousboe JT. Cost effectiveness of screen-and-treat strategies for low bone mineral density: how do we screen, who do we screen, and who do we treat? Appl Health Econ Health Policy. 2008;6:1-18.
6. Black DM, Nevitt MC, Cauley J, et al. Design of the fracture intervention trial. Osteopor Int. 2003;3(suppl 3):S29-S39.
7. Cummings S, Black D, Thompson D, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures. JAMA. 1998;280:2077-2082.
8. Cummings S, Palermo B, Browner W, et al. Monitoring osteoporosis therapy with bone densitometry: misleading changes and regression to the mean. Fracture Intervention Trial Research Group. JAMA. 2000;283:1318-1321.
9. AACE Osteoporosis Task Force American Association of Clinical Endocrinologists medical guidelines for clinical practice for the prevention and treatment of postmenopausal osteoporosis: 2001 edition with selected updates for 2003. Endocr Pract. 2003;9:544-564.
10. National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of Osteoporosis. Washington DC: NOF; 2008.
11. Management of postmenopausal osteoporosis: position statement of the North American Menopause Society Menopause. 2002;9:84-101.
1. Bell KL, Hayen A, Macaskill P, et al. Value of routine monitoring of bone mineral density after starting bisphosphonate treatment: secondary analysis of treatment data. BMJ. 2009;338:b2266.-
2. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17:1726.-
3. MacLean C, Newberry S, et al. Systematic review: comparative effectiveness of treatments to prevent fractures in men and women with low bone density or osteoporosis. Ann Intern Med. 2008;148:197-213.
4. Agency for Healthcare Research and Quality United States Preventive Services Task Force. Screening for osteoporosis in postmenopausal women. Available at: http://www.ahrq.gov/clinic/3rduspstf/osteoporosis/osteorr.htm . Accessed October 13, 2009.
5. Schousboe JT. Cost effectiveness of screen-and-treat strategies for low bone mineral density: how do we screen, who do we screen, and who do we treat? Appl Health Econ Health Policy. 2008;6:1-18.
6. Black DM, Nevitt MC, Cauley J, et al. Design of the fracture intervention trial. Osteopor Int. 2003;3(suppl 3):S29-S39.
7. Cummings S, Black D, Thompson D, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures. JAMA. 1998;280:2077-2082.
8. Cummings S, Palermo B, Browner W, et al. Monitoring osteoporosis therapy with bone densitometry: misleading changes and regression to the mean. Fracture Intervention Trial Research Group. JAMA. 2000;283:1318-1321.
9. AACE Osteoporosis Task Force American Association of Clinical Endocrinologists medical guidelines for clinical practice for the prevention and treatment of postmenopausal osteoporosis: 2001 edition with selected updates for 2003. Endocr Pract. 2003;9:544-564.
10. National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of Osteoporosis. Washington DC: NOF; 2008.
11. Management of postmenopausal osteoporosis: position statement of the North American Menopause Society Menopause. 2002;9:84-101.
Copyright © 2009 The Family Physicians Inquiries Network.
All rights reserved.
Ovary-sparing hysterectomy: Is it right for your patient?
Advise patients undergoing hysterectomy for benign conditions that there are benefits to conserving their ovaries. The risk of coronary heart disease (CHD) and death is lower in women whose ovaries are conserved, compared with those who have had them removed.1
Strength of recommendation:
B: A large, high-quality observational study.
Parker WH, Broder MS, Chang E, et al. Ovarian conservation at the time of hysterectomy and long-term health outcomes in the Nurses’ Health Study. Obstet Gynecol. 2009;113:1027-1037.
ILLUSTRATIVE CASE
A 44-year-old woman with a family history of early CHD is considering hysterectomy for painful uterine fibroids. She’s thinking about undergoing concurrent bilateral oophorectomy to prevent ovarian cancer and asks for your input. How would you advise her?
Hysterectomy is the most common gynecologic surgery in the United States. In 2003, more than 600,000 hysterectomies were performed; 89% were not associated with malignancies.2
Ovarian conservation is not the norm
Data from the University Health-System Consortium Clinical Database indicate that between 2002 and 2008, about 55% of women who had a hysterectomy that was not cancer-related underwent oophorectomy. Rates of concurrent oophorectomy included:
- 68% of women ages 65 and older
- 77% of women ages 51 to 64
- 48% of women ages 31 to 50
- 3% of women ages 18 to 30.
A recent analysis from the Centers for Disease Control and Prevention found that among women who underwent hysterectomy for any reason between 1994 and 1998, 55% also had their ovaries removed.3
Hormones and CHD: An unanswered question
Over the last several decades, there has been a great deal of interest in the relationship between hormones and CHD, much of it stemming from the controversy about hormone replacement therapy (HRT). The findings of the Women’s Health Initiative implicated combined exogenous hormones (estrogen and progestin) as a risk factor for CHD.4 Endogenous hormone production, however, may protect against CHD; some studies have demonstrated a decreased risk of cardiovascular death with later age of menopause.5,6
Current oophorectomy recommendations are age-specific. The American College of Obstetricians and Gynecologists (ACOG) recommends that strong consideration be given to ovarian conservation in premenopausal women who are not at risk for ovarian cancer. For postmenopausal women, however, ACOG recommends consideration of oophorectomy as prophylaxis.7 These recommendations are based on expert opinion. Previous studies suggest that ovarian conservation may improve survival in specific age groups.8,9 The large, high-quality observational study reviewed here provides further guidance about the role of ovarian conservation across all age groups.
STUDY SUMMARY: Oophorectomy increases risk of CHD and death
This observational study1 was part of the Nurses’ Health Study. It included 29,380 women, of which 16,345 (55.6%) underwent hysterectomy with bilateral oophorectomy and 13,035 (44.4%) had hysterectomy with ovarian conservation. Women with unilateral oophorectomy were excluded, as were those who had a history of CHD or stroke, and women for whom pertinent data, such as age, were missing. A follow-up survey was sent to participants every 2 years for 24 years, with an average return rate of 90%.
Women who had undergone bilateral oophorectomy had an increased risk of CHD and all-cause mortality ( TABLE ). The authors estimated that with a postsurgical life span of approximately 35 years, every 9 oophorectomies would result in 1 additional death. The authors also pointed out there were no age exceptions: Ovarian-sparing surgery was linked to improved survival in every age group.
Oophorectomy did have a protective effect against breast cancer, ovarian cancer (number needed to treat=220), and total cancer incidence, but it was associated with an increased incidence of lung cancer (number needed to harm=190) and total cancer mortality. There was no significant difference in rates of stroke, pulmonary embolus, colorectal cancer, or hip fracture.
TABLE
Oophorectomy (vs ovarian conservation) increases key risks1
| RISK FACTOR | MULTIVARIATE–ADJUSTED HR (95% CI) |
|---|---|
| CHD (fatal and nonfatal) | 1.17 (1.02-1.35) |
| Breast cancer | 0.75 (0.68-0.84) |
| Lung cancer | 1.26 (1.02-1.56) |
| Ovarian cancer | 0.04 (0.01-0.09) |
| Total cancer | 0.90 (0.84-0.96) |
| Total cancer mortality | 1.17 (1.04-1.32) |
| All-cause mortality | 1.12 (1.03-1.21) |
| CHD, coronary heart disease; CI, confidence interval; HR, hazard ratio. | |
WHAT’S NEW: Ovarian conservation: Better for all ages
The evidence is clear: Conserving the ovaries, rather than removing them, during hysterectomy is associated with a lower risk of CHD and both all-cause and cancer-related mortality.
What about the patient’s age? A 2005 analysis suggested that ovarian conservation conferred a survival benefit compared to oophorectomy in women <65 years.8 Similarly, a 2006 cohort study found increased mortality in women <45 years who underwent concurrent oophorectomy.9 But this is the first study to demonstrate that ovarian-sparing surgery is associated with improved survival in women of every age group.
CAVEATS: Study sample and HRT use could affect outcome
The average age of patients in the treatment (oophorectomy) arm was higher than that of patients in the control group; the women in the treatment group were older at the time of hysterectomy (46.8 vs 43.3 years), as well. This should not bias the results, which were adjusted by age and many other variables.
Nonrepresentative sample. This group of nurses is not representative of the general population in several important aspects, including socioeconomic status, educational level, and race (94% Caucasian). This may limit the generalizability of the findings.
Study design. The observational design and the fact that the patients themselves decided whether or not to undergo oophorectomy also raise the possibility of unmeasured confounding factors.
Cancer risk. Women with known BRCA mutations were not studied separately, but the results were adjusted for family history of breast or ovarian cancer. The authors stated that a subgroup analysis of women with a family history of ovarian cancer had similar outcomes, although the data were not included
HRT use. As might be expected, patients in the oophorectomy arm of the study were more likely to use HRT. Since the completion of the study in 2000, practice recommendations have shifted against combined HRT use. Unopposed estrogen, which is not thought to increase the incidence of cardiovascular disease, remains a treatment option for women who have undergone hysterectomy and oophorectomy. But the overall effect of unopposed estrogen on survival is still uncertain.4 It is unclear how the recent decline in the use of exogenous hormones would affect these results.
BARRIERS TO IMPLEMENTATION: FP-GYN communication can be difficult
This study provides important information for primary care physicians to discuss with female patients and their gynecologists. However, some doctors may not have relationships with the gynecologists in their community, or have limited (or no) influence or input into which specialists their patients see. In addition, some gynecologists may hesitate to perform hysterectomy without oophorectomy in some cases for technical reasons.10
Concern about prevention of ovarian cancer must be balanced with increased risk of mortality and CHD events. It may be helpful to tell patients who are about to undergo hysterectomy for a benign condition that women are nearly 30 times more likely to die of cardiovascular disease (CHD or stroke) than ovarian cancer (413,800/year vs 14,700/year).11
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
The authors wish to acknowledge Sofia Medvedev, PhD, of the University HealthSystem Consortium in Oak Brook, Ill, for analysis of the National Ambulatory Medical Care Survey data and the UHC Clinical Database.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Parker WH, Broder MS, Chang E, et al. Ovarian conservation at the time of hysterectomy and long-term health outcomes in the Nurses’ Health Study. Obstet Gynecol. 2009;113:1027-1037.
2. Wu JM, Wechter ME, Geller EJ, et al. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110:1091.-
3. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project (HCUP), 1988-2001: a federal-state industry partnership in health data. July 2003. Available at http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5105al.htm. Accessed June 8, 2009.
4. Anderson GL, Limacher M, Assaf AF, et al. Effect of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701.-
5. Ossewaarde ME, Bots ML, Verbeek AL, et al. Age at menopause, cause-specific mortality and total life expectancy. Epidemiology. 2005;16:556-562.
6. Atsma F, Bartelink M, Grobbee D, et al. Postmenopausal status and early menopause as independent risk factors for cardiovascular disease: a meta-analysis. Menopause. 2006;13:265-279.
7. American College of Obstetricians and Gynecologists. Elective and risk-reducing salpingo-oophorectomy. ACOG Practice Bulletin No 89. Washington, DC: ACOG; 2008.
8. Parker WH, Broder MS, Liu Z, et al. Ovarian conservation at the time of hysterectomy for benign disease. Obstet Gynecol. 2005;106:219-226.
9. Rocca W, Grossardt B, de Andrade M, et al. Survival patterns after oophorectomy in premenopausal women: a population-based cohort study. Lancet Oncol. 2006;7:821-828.
10. Priver D. Oophorectomy in young women may not be so harmful. OBG Management. 2009;21(8):11.-
11. Kung H, Hoyert D, Xu J, et al. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56:1-120.
Advise patients undergoing hysterectomy for benign conditions that there are benefits to conserving their ovaries. The risk of coronary heart disease (CHD) and death is lower in women whose ovaries are conserved, compared with those who have had them removed.1
Strength of recommendation:
B: A large, high-quality observational study.
Parker WH, Broder MS, Chang E, et al. Ovarian conservation at the time of hysterectomy and long-term health outcomes in the Nurses’ Health Study. Obstet Gynecol. 2009;113:1027-1037.
ILLUSTRATIVE CASE
A 44-year-old woman with a family history of early CHD is considering hysterectomy for painful uterine fibroids. She’s thinking about undergoing concurrent bilateral oophorectomy to prevent ovarian cancer and asks for your input. How would you advise her?
Hysterectomy is the most common gynecologic surgery in the United States. In 2003, more than 600,000 hysterectomies were performed; 89% were not associated with malignancies.2
Ovarian conservation is not the norm
Data from the University Health-System Consortium Clinical Database indicate that between 2002 and 2008, about 55% of women who had a hysterectomy that was not cancer-related underwent oophorectomy. Rates of concurrent oophorectomy included:
- 68% of women ages 65 and older
- 77% of women ages 51 to 64
- 48% of women ages 31 to 50
- 3% of women ages 18 to 30.
A recent analysis from the Centers for Disease Control and Prevention found that among women who underwent hysterectomy for any reason between 1994 and 1998, 55% also had their ovaries removed.3
Hormones and CHD: An unanswered question
Over the last several decades, there has been a great deal of interest in the relationship between hormones and CHD, much of it stemming from the controversy about hormone replacement therapy (HRT). The findings of the Women’s Health Initiative implicated combined exogenous hormones (estrogen and progestin) as a risk factor for CHD.4 Endogenous hormone production, however, may protect against CHD; some studies have demonstrated a decreased risk of cardiovascular death with later age of menopause.5,6
Current oophorectomy recommendations are age-specific. The American College of Obstetricians and Gynecologists (ACOG) recommends that strong consideration be given to ovarian conservation in premenopausal women who are not at risk for ovarian cancer. For postmenopausal women, however, ACOG recommends consideration of oophorectomy as prophylaxis.7 These recommendations are based on expert opinion. Previous studies suggest that ovarian conservation may improve survival in specific age groups.8,9 The large, high-quality observational study reviewed here provides further guidance about the role of ovarian conservation across all age groups.
STUDY SUMMARY: Oophorectomy increases risk of CHD and death
This observational study1 was part of the Nurses’ Health Study. It included 29,380 women, of which 16,345 (55.6%) underwent hysterectomy with bilateral oophorectomy and 13,035 (44.4%) had hysterectomy with ovarian conservation. Women with unilateral oophorectomy were excluded, as were those who had a history of CHD or stroke, and women for whom pertinent data, such as age, were missing. A follow-up survey was sent to participants every 2 years for 24 years, with an average return rate of 90%.
Women who had undergone bilateral oophorectomy had an increased risk of CHD and all-cause mortality ( TABLE ). The authors estimated that with a postsurgical life span of approximately 35 years, every 9 oophorectomies would result in 1 additional death. The authors also pointed out there were no age exceptions: Ovarian-sparing surgery was linked to improved survival in every age group.
Oophorectomy did have a protective effect against breast cancer, ovarian cancer (number needed to treat=220), and total cancer incidence, but it was associated with an increased incidence of lung cancer (number needed to harm=190) and total cancer mortality. There was no significant difference in rates of stroke, pulmonary embolus, colorectal cancer, or hip fracture.
TABLE
Oophorectomy (vs ovarian conservation) increases key risks1
| RISK FACTOR | MULTIVARIATE–ADJUSTED HR (95% CI) |
|---|---|
| CHD (fatal and nonfatal) | 1.17 (1.02-1.35) |
| Breast cancer | 0.75 (0.68-0.84) |
| Lung cancer | 1.26 (1.02-1.56) |
| Ovarian cancer | 0.04 (0.01-0.09) |
| Total cancer | 0.90 (0.84-0.96) |
| Total cancer mortality | 1.17 (1.04-1.32) |
| All-cause mortality | 1.12 (1.03-1.21) |
| CHD, coronary heart disease; CI, confidence interval; HR, hazard ratio. | |
WHAT’S NEW: Ovarian conservation: Better for all ages
The evidence is clear: Conserving the ovaries, rather than removing them, during hysterectomy is associated with a lower risk of CHD and both all-cause and cancer-related mortality.
What about the patient’s age? A 2005 analysis suggested that ovarian conservation conferred a survival benefit compared to oophorectomy in women <65 years.8 Similarly, a 2006 cohort study found increased mortality in women <45 years who underwent concurrent oophorectomy.9 But this is the first study to demonstrate that ovarian-sparing surgery is associated with improved survival in women of every age group.
CAVEATS: Study sample and HRT use could affect outcome
The average age of patients in the treatment (oophorectomy) arm was higher than that of patients in the control group; the women in the treatment group were older at the time of hysterectomy (46.8 vs 43.3 years), as well. This should not bias the results, which were adjusted by age and many other variables.
Nonrepresentative sample. This group of nurses is not representative of the general population in several important aspects, including socioeconomic status, educational level, and race (94% Caucasian). This may limit the generalizability of the findings.
Study design. The observational design and the fact that the patients themselves decided whether or not to undergo oophorectomy also raise the possibility of unmeasured confounding factors.
Cancer risk. Women with known BRCA mutations were not studied separately, but the results were adjusted for family history of breast or ovarian cancer. The authors stated that a subgroup analysis of women with a family history of ovarian cancer had similar outcomes, although the data were not included
HRT use. As might be expected, patients in the oophorectomy arm of the study were more likely to use HRT. Since the completion of the study in 2000, practice recommendations have shifted against combined HRT use. Unopposed estrogen, which is not thought to increase the incidence of cardiovascular disease, remains a treatment option for women who have undergone hysterectomy and oophorectomy. But the overall effect of unopposed estrogen on survival is still uncertain.4 It is unclear how the recent decline in the use of exogenous hormones would affect these results.
BARRIERS TO IMPLEMENTATION: FP-GYN communication can be difficult
This study provides important information for primary care physicians to discuss with female patients and their gynecologists. However, some doctors may not have relationships with the gynecologists in their community, or have limited (or no) influence or input into which specialists their patients see. In addition, some gynecologists may hesitate to perform hysterectomy without oophorectomy in some cases for technical reasons.10
Concern about prevention of ovarian cancer must be balanced with increased risk of mortality and CHD events. It may be helpful to tell patients who are about to undergo hysterectomy for a benign condition that women are nearly 30 times more likely to die of cardiovascular disease (CHD or stroke) than ovarian cancer (413,800/year vs 14,700/year).11
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
The authors wish to acknowledge Sofia Medvedev, PhD, of the University HealthSystem Consortium in Oak Brook, Ill, for analysis of the National Ambulatory Medical Care Survey data and the UHC Clinical Database.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
Advise patients undergoing hysterectomy for benign conditions that there are benefits to conserving their ovaries. The risk of coronary heart disease (CHD) and death is lower in women whose ovaries are conserved, compared with those who have had them removed.1
Strength of recommendation:
B: A large, high-quality observational study.
Parker WH, Broder MS, Chang E, et al. Ovarian conservation at the time of hysterectomy and long-term health outcomes in the Nurses’ Health Study. Obstet Gynecol. 2009;113:1027-1037.
ILLUSTRATIVE CASE
A 44-year-old woman with a family history of early CHD is considering hysterectomy for painful uterine fibroids. She’s thinking about undergoing concurrent bilateral oophorectomy to prevent ovarian cancer and asks for your input. How would you advise her?
Hysterectomy is the most common gynecologic surgery in the United States. In 2003, more than 600,000 hysterectomies were performed; 89% were not associated with malignancies.2
Ovarian conservation is not the norm
Data from the University Health-System Consortium Clinical Database indicate that between 2002 and 2008, about 55% of women who had a hysterectomy that was not cancer-related underwent oophorectomy. Rates of concurrent oophorectomy included:
- 68% of women ages 65 and older
- 77% of women ages 51 to 64
- 48% of women ages 31 to 50
- 3% of women ages 18 to 30.
A recent analysis from the Centers for Disease Control and Prevention found that among women who underwent hysterectomy for any reason between 1994 and 1998, 55% also had their ovaries removed.3
Hormones and CHD: An unanswered question
Over the last several decades, there has been a great deal of interest in the relationship between hormones and CHD, much of it stemming from the controversy about hormone replacement therapy (HRT). The findings of the Women’s Health Initiative implicated combined exogenous hormones (estrogen and progestin) as a risk factor for CHD.4 Endogenous hormone production, however, may protect against CHD; some studies have demonstrated a decreased risk of cardiovascular death with later age of menopause.5,6
Current oophorectomy recommendations are age-specific. The American College of Obstetricians and Gynecologists (ACOG) recommends that strong consideration be given to ovarian conservation in premenopausal women who are not at risk for ovarian cancer. For postmenopausal women, however, ACOG recommends consideration of oophorectomy as prophylaxis.7 These recommendations are based on expert opinion. Previous studies suggest that ovarian conservation may improve survival in specific age groups.8,9 The large, high-quality observational study reviewed here provides further guidance about the role of ovarian conservation across all age groups.
STUDY SUMMARY: Oophorectomy increases risk of CHD and death
This observational study1 was part of the Nurses’ Health Study. It included 29,380 women, of which 16,345 (55.6%) underwent hysterectomy with bilateral oophorectomy and 13,035 (44.4%) had hysterectomy with ovarian conservation. Women with unilateral oophorectomy were excluded, as were those who had a history of CHD or stroke, and women for whom pertinent data, such as age, were missing. A follow-up survey was sent to participants every 2 years for 24 years, with an average return rate of 90%.
Women who had undergone bilateral oophorectomy had an increased risk of CHD and all-cause mortality ( TABLE ). The authors estimated that with a postsurgical life span of approximately 35 years, every 9 oophorectomies would result in 1 additional death. The authors also pointed out there were no age exceptions: Ovarian-sparing surgery was linked to improved survival in every age group.
Oophorectomy did have a protective effect against breast cancer, ovarian cancer (number needed to treat=220), and total cancer incidence, but it was associated with an increased incidence of lung cancer (number needed to harm=190) and total cancer mortality. There was no significant difference in rates of stroke, pulmonary embolus, colorectal cancer, or hip fracture.
TABLE
Oophorectomy (vs ovarian conservation) increases key risks1
| RISK FACTOR | MULTIVARIATE–ADJUSTED HR (95% CI) |
|---|---|
| CHD (fatal and nonfatal) | 1.17 (1.02-1.35) |
| Breast cancer | 0.75 (0.68-0.84) |
| Lung cancer | 1.26 (1.02-1.56) |
| Ovarian cancer | 0.04 (0.01-0.09) |
| Total cancer | 0.90 (0.84-0.96) |
| Total cancer mortality | 1.17 (1.04-1.32) |
| All-cause mortality | 1.12 (1.03-1.21) |
| CHD, coronary heart disease; CI, confidence interval; HR, hazard ratio. | |
WHAT’S NEW: Ovarian conservation: Better for all ages
The evidence is clear: Conserving the ovaries, rather than removing them, during hysterectomy is associated with a lower risk of CHD and both all-cause and cancer-related mortality.
What about the patient’s age? A 2005 analysis suggested that ovarian conservation conferred a survival benefit compared to oophorectomy in women <65 years.8 Similarly, a 2006 cohort study found increased mortality in women <45 years who underwent concurrent oophorectomy.9 But this is the first study to demonstrate that ovarian-sparing surgery is associated with improved survival in women of every age group.
CAVEATS: Study sample and HRT use could affect outcome
The average age of patients in the treatment (oophorectomy) arm was higher than that of patients in the control group; the women in the treatment group were older at the time of hysterectomy (46.8 vs 43.3 years), as well. This should not bias the results, which were adjusted by age and many other variables.
Nonrepresentative sample. This group of nurses is not representative of the general population in several important aspects, including socioeconomic status, educational level, and race (94% Caucasian). This may limit the generalizability of the findings.
Study design. The observational design and the fact that the patients themselves decided whether or not to undergo oophorectomy also raise the possibility of unmeasured confounding factors.
Cancer risk. Women with known BRCA mutations were not studied separately, but the results were adjusted for family history of breast or ovarian cancer. The authors stated that a subgroup analysis of women with a family history of ovarian cancer had similar outcomes, although the data were not included
HRT use. As might be expected, patients in the oophorectomy arm of the study were more likely to use HRT. Since the completion of the study in 2000, practice recommendations have shifted against combined HRT use. Unopposed estrogen, which is not thought to increase the incidence of cardiovascular disease, remains a treatment option for women who have undergone hysterectomy and oophorectomy. But the overall effect of unopposed estrogen on survival is still uncertain.4 It is unclear how the recent decline in the use of exogenous hormones would affect these results.
BARRIERS TO IMPLEMENTATION: FP-GYN communication can be difficult
This study provides important information for primary care physicians to discuss with female patients and their gynecologists. However, some doctors may not have relationships with the gynecologists in their community, or have limited (or no) influence or input into which specialists their patients see. In addition, some gynecologists may hesitate to perform hysterectomy without oophorectomy in some cases for technical reasons.10
Concern about prevention of ovarian cancer must be balanced with increased risk of mortality and CHD events. It may be helpful to tell patients who are about to undergo hysterectomy for a benign condition that women are nearly 30 times more likely to die of cardiovascular disease (CHD or stroke) than ovarian cancer (413,800/year vs 14,700/year).11
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
The authors wish to acknowledge Sofia Medvedev, PhD, of the University HealthSystem Consortium in Oak Brook, Ill, for analysis of the National Ambulatory Medical Care Survey data and the UHC Clinical Database.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Parker WH, Broder MS, Chang E, et al. Ovarian conservation at the time of hysterectomy and long-term health outcomes in the Nurses’ Health Study. Obstet Gynecol. 2009;113:1027-1037.
2. Wu JM, Wechter ME, Geller EJ, et al. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110:1091.-
3. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project (HCUP), 1988-2001: a federal-state industry partnership in health data. July 2003. Available at http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5105al.htm. Accessed June 8, 2009.
4. Anderson GL, Limacher M, Assaf AF, et al. Effect of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701.-
5. Ossewaarde ME, Bots ML, Verbeek AL, et al. Age at menopause, cause-specific mortality and total life expectancy. Epidemiology. 2005;16:556-562.
6. Atsma F, Bartelink M, Grobbee D, et al. Postmenopausal status and early menopause as independent risk factors for cardiovascular disease: a meta-analysis. Menopause. 2006;13:265-279.
7. American College of Obstetricians and Gynecologists. Elective and risk-reducing salpingo-oophorectomy. ACOG Practice Bulletin No 89. Washington, DC: ACOG; 2008.
8. Parker WH, Broder MS, Liu Z, et al. Ovarian conservation at the time of hysterectomy for benign disease. Obstet Gynecol. 2005;106:219-226.
9. Rocca W, Grossardt B, de Andrade M, et al. Survival patterns after oophorectomy in premenopausal women: a population-based cohort study. Lancet Oncol. 2006;7:821-828.
10. Priver D. Oophorectomy in young women may not be so harmful. OBG Management. 2009;21(8):11.-
11. Kung H, Hoyert D, Xu J, et al. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56:1-120.
1. Parker WH, Broder MS, Chang E, et al. Ovarian conservation at the time of hysterectomy and long-term health outcomes in the Nurses’ Health Study. Obstet Gynecol. 2009;113:1027-1037.
2. Wu JM, Wechter ME, Geller EJ, et al. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110:1091.-
3. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project (HCUP), 1988-2001: a federal-state industry partnership in health data. July 2003. Available at http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5105al.htm. Accessed June 8, 2009.
4. Anderson GL, Limacher M, Assaf AF, et al. Effect of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701.-
5. Ossewaarde ME, Bots ML, Verbeek AL, et al. Age at menopause, cause-specific mortality and total life expectancy. Epidemiology. 2005;16:556-562.
6. Atsma F, Bartelink M, Grobbee D, et al. Postmenopausal status and early menopause as independent risk factors for cardiovascular disease: a meta-analysis. Menopause. 2006;13:265-279.
7. American College of Obstetricians and Gynecologists. Elective and risk-reducing salpingo-oophorectomy. ACOG Practice Bulletin No 89. Washington, DC: ACOG; 2008.
8. Parker WH, Broder MS, Liu Z, et al. Ovarian conservation at the time of hysterectomy for benign disease. Obstet Gynecol. 2005;106:219-226.
9. Rocca W, Grossardt B, de Andrade M, et al. Survival patterns after oophorectomy in premenopausal women: a population-based cohort study. Lancet Oncol. 2006;7:821-828.
10. Priver D. Oophorectomy in young women may not be so harmful. OBG Management. 2009;21(8):11.-
11. Kung H, Hoyert D, Xu J, et al. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56:1-120.
Copyright © 2009 The Family Physicians Inquiries Network.
All rights reserved.
What is the recommended approach to asymptomatic patients who develop a reactive PPD?
Clinical evaluation and chest x-ray are recommended for asymptomatic patients with a positive purified protein derivative (PPD) test result, to exclude the slight possibility of active tuberculosis (TB). Patients with radiographic evidence of old (healed) TB infection should also undergo sputum testing (strength of recommendation [SOR]: C, expert opinion).
Treatment with isoniazid (INH) monotherapy (300 mg/d) reduces progression of latent tuberculosis to active disease (SOR: A, large randomized controlled trials [RCT]), with 9 months as the optimal treatment length (SOR: B, derivation from RCTs). A 3-month course of combined rifampin (600 mg/d) and INH (300 mg/d) is equivalent in efficacy to INH monotherapy and is associated with similar rates of toxicity (SOR: A, meta-analysis of RCTs), but this regimen is not included in Centers for Disease Control and Prevention recommendations.
Address patient concerns about TB and treatment side effects
Richard Guthmann, MD
University of Illinois at Chicago/Advocate Illinois Masonic Family Medicine Residency, Chicago
Patients’ understanding of tuberculosis—the disease, the treatment, and the outcome—poses an important challenge in the care of an asymptomatic PPD-positive patient. These patients may ask, “Will I get sick? Do I have to take the medicine? Are there side effects? And would you take the medicine?” We need to be prepared to answer these questions.
Most patients with a positive PPD will not get active tuberculosis, but when they do it can be serious and it can spread easily. The medication significantly decreases the risk of developing active tuberculosis. The medication side effects are uncommon but can be severe. These side effects are reversible if the medication is stopped promptly. Under the supervision of my physician, I would take the medicine.
Evidence summary
Clinical evaluation with medical history and physical exam, chest radiography, and selected sputum sampling to exclude active tuberculosis are part of the recommended algorithm for all patients who develop a positive PPD (FIGURE).1-3 These recommendations are derived from expert opinion, and their usefulness has not been evaluated in any population-based study of asymptomatic PPD-positive patients.
A comprehensive review of RCTs from the 1950s and 1960s demonstrated that INH treatment of patients with latent tuberculosis infection is effective in decreasing the progression to active tuberculosis.4 A series of double-blinded RCTs performed by the US Public Health Service included 25,923 patients with latent tuberculosis who were randomized to receive either daily INH or placebo for 1 year with 6- to 10-year follow-up. Groups studied included household contacts of patients with active tuberculosis (rate of progression to active disease in placebo group [baseline rate]=27/1000, relative risk with INH [RR]=0.4, number needed to treat [NNT]=63), patients in mental institutions (baseline rate=12/1000, RR=0.3, NNT=121), and patients with x-ray findings of healed tuberculosis (baseline rate=69/1000, RR=0.4, NNT=23).
The optimal length of treatment for PPD-positive patients without active disease was evaluated through 1 double-blinded RCT enrolling 28,000 patients with 5-year follow-up after 12, 24, or 52 weeks of INH or placebo. Active TB developed in 0.35% (24/6919) after 52 weeks of INH compared with 0.49% (34/6965) after 24 weeks (RR=1.4, NNT=708).5 Incidence in the placebo group was 1.4%. Subgroup analysis determined that maximum efficacy with fewest side effects was achieved at 9 months.6 Nine months of INH is also recommended for HIV-positive patients, based on extrapolations from these and other studies.3
INH monotherapy was compared with combination INH and rifampin in a 2005 meta-analysis of 5 RCTs of variable quality involving 1926 patients.7 This meta-analysis found equivalency in risk of active TB and mortality between INH monotherapy for 6 to 12 months and the combination of rifampin and INH for 3 months (pooled risk difference=0%; 95% confidence interval [CI], –1% to 2%). This study also showed similar rates of adverse events in both groups (pooled risk difference=–1%; 95% CI, –7% to 5%). Short-course combination rifampin and pyrazinamide is no longer recommended after an open-label RCT with 589 patients demonstrated severe hepatoxicity in 7.7% (16/207) on a 2-month course of pyrazinamide and rifampin, compared with 1% (2/204) on 6 months of INH (RR=7.9, number needed to harm=15).8 Rifampin monotherapy has only been studied in patients with silicosis in a RCT enrolling 652 participants with latent tuberculosis. A 12-week course of rifampin (600 mg daily) was as effective as 6 months of INH in preventing development of active TB over the next 5 years.9
FIGURE
Suggested workup of asymptomatic, HIV-negative patients with a positive PPD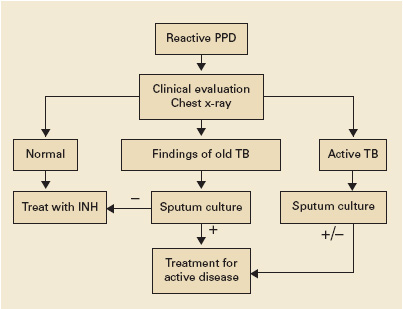
Source: Am J Respir Crit Care Med 2000;2 Jasmer et al, N Engl J Med 2002.3
Recommendations from others
Centers for Disease Control and Prevention, American Thoracic Society, and Infectious Disease Society of America guidelines recommend targeted screening of high-risk persons followed by further clinical evaluation of all those with a reactive PPD (FIGURE).2,10 The recommended treatment regimen for latent TB is daily INH for 9 months. Less preferable regimens are daily INH for 6 months, or daily rifampin for 4 months in patients who cannot tolerate INH. A 2-month course of rifampin and pyrazinamide is no longer recommended. The recent meta-analysis supporting a 3-month regimen of combination INH and rifampin has not been incorporated into expert guidelines.7
1. Diagnostic standards and classification of tuberculosis in adults and children. Am J Respir Crit Care Med 2000;161:1376-1395.
2. Targeted tuberculin testing and treatment of latent tuberculosis infection. Am J Respir Crit Care Med 2000;161:S221-S247.
3. Jasmer RM, Nahid P, Hopewell PC. Clinical practice. Latent tuberculosis infection. N Engl J Med 2002;347:1860-1866.
4. Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis. A general review. Bibl Tuberc 1970;26:28-106.
5. Efficacy of various durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the IUAT trial. Bull World Health Organ 1982;60:555-564.
6. Comstock GW. How much isoniazid is needed for prevention of tuberculosis among immunocompetent adults? Int J Tuberc Lung Dis 1999;3:847-850.
7. Ena J, Valls V. Short-course therapy with rifampin plus isoniazid, compared with standard therapy with isoniazid, for latent tuberculosis infection: a meta-analysis. Clin Infect Dis 2005;40:670-676.
8. Jasmer RM, Saukkonen JJ, Blumberg HM, et al. Short-course rifampin and pyrazinamide compared with isoniazid for latent tuberculosis infection: a multicenter clinical trial. Ann Intern Med 2002;137:640-647.
9. Hong Kong Chest Service/Tuberculosis Research Centre, Madras/British Medical Research Council. A double-blind placebo-controlled clinical trial of three antituberculosis chemoprophylaxis regimens in patients with silicosis in Hong Kong. Am Rev Respir Dis 1992;145:36-41.
10. Taylor Z, Nolan CM, Blumberg HM. Controlling tuberculosis in the United States. MMWR Recomm Rep 2005;54(RR-12):1-81.
Clinical evaluation and chest x-ray are recommended for asymptomatic patients with a positive purified protein derivative (PPD) test result, to exclude the slight possibility of active tuberculosis (TB). Patients with radiographic evidence of old (healed) TB infection should also undergo sputum testing (strength of recommendation [SOR]: C, expert opinion).
Treatment with isoniazid (INH) monotherapy (300 mg/d) reduces progression of latent tuberculosis to active disease (SOR: A, large randomized controlled trials [RCT]), with 9 months as the optimal treatment length (SOR: B, derivation from RCTs). A 3-month course of combined rifampin (600 mg/d) and INH (300 mg/d) is equivalent in efficacy to INH monotherapy and is associated with similar rates of toxicity (SOR: A, meta-analysis of RCTs), but this regimen is not included in Centers for Disease Control and Prevention recommendations.
Address patient concerns about TB and treatment side effects
Richard Guthmann, MD
University of Illinois at Chicago/Advocate Illinois Masonic Family Medicine Residency, Chicago
Patients’ understanding of tuberculosis—the disease, the treatment, and the outcome—poses an important challenge in the care of an asymptomatic PPD-positive patient. These patients may ask, “Will I get sick? Do I have to take the medicine? Are there side effects? And would you take the medicine?” We need to be prepared to answer these questions.
Most patients with a positive PPD will not get active tuberculosis, but when they do it can be serious and it can spread easily. The medication significantly decreases the risk of developing active tuberculosis. The medication side effects are uncommon but can be severe. These side effects are reversible if the medication is stopped promptly. Under the supervision of my physician, I would take the medicine.
Evidence summary
Clinical evaluation with medical history and physical exam, chest radiography, and selected sputum sampling to exclude active tuberculosis are part of the recommended algorithm for all patients who develop a positive PPD (FIGURE).1-3 These recommendations are derived from expert opinion, and their usefulness has not been evaluated in any population-based study of asymptomatic PPD-positive patients.
A comprehensive review of RCTs from the 1950s and 1960s demonstrated that INH treatment of patients with latent tuberculosis infection is effective in decreasing the progression to active tuberculosis.4 A series of double-blinded RCTs performed by the US Public Health Service included 25,923 patients with latent tuberculosis who were randomized to receive either daily INH or placebo for 1 year with 6- to 10-year follow-up. Groups studied included household contacts of patients with active tuberculosis (rate of progression to active disease in placebo group [baseline rate]=27/1000, relative risk with INH [RR]=0.4, number needed to treat [NNT]=63), patients in mental institutions (baseline rate=12/1000, RR=0.3, NNT=121), and patients with x-ray findings of healed tuberculosis (baseline rate=69/1000, RR=0.4, NNT=23).
The optimal length of treatment for PPD-positive patients without active disease was evaluated through 1 double-blinded RCT enrolling 28,000 patients with 5-year follow-up after 12, 24, or 52 weeks of INH or placebo. Active TB developed in 0.35% (24/6919) after 52 weeks of INH compared with 0.49% (34/6965) after 24 weeks (RR=1.4, NNT=708).5 Incidence in the placebo group was 1.4%. Subgroup analysis determined that maximum efficacy with fewest side effects was achieved at 9 months.6 Nine months of INH is also recommended for HIV-positive patients, based on extrapolations from these and other studies.3
INH monotherapy was compared with combination INH and rifampin in a 2005 meta-analysis of 5 RCTs of variable quality involving 1926 patients.7 This meta-analysis found equivalency in risk of active TB and mortality between INH monotherapy for 6 to 12 months and the combination of rifampin and INH for 3 months (pooled risk difference=0%; 95% confidence interval [CI], –1% to 2%). This study also showed similar rates of adverse events in both groups (pooled risk difference=–1%; 95% CI, –7% to 5%). Short-course combination rifampin and pyrazinamide is no longer recommended after an open-label RCT with 589 patients demonstrated severe hepatoxicity in 7.7% (16/207) on a 2-month course of pyrazinamide and rifampin, compared with 1% (2/204) on 6 months of INH (RR=7.9, number needed to harm=15).8 Rifampin monotherapy has only been studied in patients with silicosis in a RCT enrolling 652 participants with latent tuberculosis. A 12-week course of rifampin (600 mg daily) was as effective as 6 months of INH in preventing development of active TB over the next 5 years.9
FIGURE
Suggested workup of asymptomatic, HIV-negative patients with a positive PPD
Source: Am J Respir Crit Care Med 2000;2 Jasmer et al, N Engl J Med 2002.3
Recommendations from others
Centers for Disease Control and Prevention, American Thoracic Society, and Infectious Disease Society of America guidelines recommend targeted screening of high-risk persons followed by further clinical evaluation of all those with a reactive PPD (FIGURE).2,10 The recommended treatment regimen for latent TB is daily INH for 9 months. Less preferable regimens are daily INH for 6 months, or daily rifampin for 4 months in patients who cannot tolerate INH. A 2-month course of rifampin and pyrazinamide is no longer recommended. The recent meta-analysis supporting a 3-month regimen of combination INH and rifampin has not been incorporated into expert guidelines.7
Clinical evaluation and chest x-ray are recommended for asymptomatic patients with a positive purified protein derivative (PPD) test result, to exclude the slight possibility of active tuberculosis (TB). Patients with radiographic evidence of old (healed) TB infection should also undergo sputum testing (strength of recommendation [SOR]: C, expert opinion).
Treatment with isoniazid (INH) monotherapy (300 mg/d) reduces progression of latent tuberculosis to active disease (SOR: A, large randomized controlled trials [RCT]), with 9 months as the optimal treatment length (SOR: B, derivation from RCTs). A 3-month course of combined rifampin (600 mg/d) and INH (300 mg/d) is equivalent in efficacy to INH monotherapy and is associated with similar rates of toxicity (SOR: A, meta-analysis of RCTs), but this regimen is not included in Centers for Disease Control and Prevention recommendations.
Address patient concerns about TB and treatment side effects
Richard Guthmann, MD
University of Illinois at Chicago/Advocate Illinois Masonic Family Medicine Residency, Chicago
Patients’ understanding of tuberculosis—the disease, the treatment, and the outcome—poses an important challenge in the care of an asymptomatic PPD-positive patient. These patients may ask, “Will I get sick? Do I have to take the medicine? Are there side effects? And would you take the medicine?” We need to be prepared to answer these questions.
Most patients with a positive PPD will not get active tuberculosis, but when they do it can be serious and it can spread easily. The medication significantly decreases the risk of developing active tuberculosis. The medication side effects are uncommon but can be severe. These side effects are reversible if the medication is stopped promptly. Under the supervision of my physician, I would take the medicine.
Evidence summary
Clinical evaluation with medical history and physical exam, chest radiography, and selected sputum sampling to exclude active tuberculosis are part of the recommended algorithm for all patients who develop a positive PPD (FIGURE).1-3 These recommendations are derived from expert opinion, and their usefulness has not been evaluated in any population-based study of asymptomatic PPD-positive patients.
A comprehensive review of RCTs from the 1950s and 1960s demonstrated that INH treatment of patients with latent tuberculosis infection is effective in decreasing the progression to active tuberculosis.4 A series of double-blinded RCTs performed by the US Public Health Service included 25,923 patients with latent tuberculosis who were randomized to receive either daily INH or placebo for 1 year with 6- to 10-year follow-up. Groups studied included household contacts of patients with active tuberculosis (rate of progression to active disease in placebo group [baseline rate]=27/1000, relative risk with INH [RR]=0.4, number needed to treat [NNT]=63), patients in mental institutions (baseline rate=12/1000, RR=0.3, NNT=121), and patients with x-ray findings of healed tuberculosis (baseline rate=69/1000, RR=0.4, NNT=23).
The optimal length of treatment for PPD-positive patients without active disease was evaluated through 1 double-blinded RCT enrolling 28,000 patients with 5-year follow-up after 12, 24, or 52 weeks of INH or placebo. Active TB developed in 0.35% (24/6919) after 52 weeks of INH compared with 0.49% (34/6965) after 24 weeks (RR=1.4, NNT=708).5 Incidence in the placebo group was 1.4%. Subgroup analysis determined that maximum efficacy with fewest side effects was achieved at 9 months.6 Nine months of INH is also recommended for HIV-positive patients, based on extrapolations from these and other studies.3
INH monotherapy was compared with combination INH and rifampin in a 2005 meta-analysis of 5 RCTs of variable quality involving 1926 patients.7 This meta-analysis found equivalency in risk of active TB and mortality between INH monotherapy for 6 to 12 months and the combination of rifampin and INH for 3 months (pooled risk difference=0%; 95% confidence interval [CI], –1% to 2%). This study also showed similar rates of adverse events in both groups (pooled risk difference=–1%; 95% CI, –7% to 5%). Short-course combination rifampin and pyrazinamide is no longer recommended after an open-label RCT with 589 patients demonstrated severe hepatoxicity in 7.7% (16/207) on a 2-month course of pyrazinamide and rifampin, compared with 1% (2/204) on 6 months of INH (RR=7.9, number needed to harm=15).8 Rifampin monotherapy has only been studied in patients with silicosis in a RCT enrolling 652 participants with latent tuberculosis. A 12-week course of rifampin (600 mg daily) was as effective as 6 months of INH in preventing development of active TB over the next 5 years.9
FIGURE
Suggested workup of asymptomatic, HIV-negative patients with a positive PPD
Source: Am J Respir Crit Care Med 2000;2 Jasmer et al, N Engl J Med 2002.3
Recommendations from others
Centers for Disease Control and Prevention, American Thoracic Society, and Infectious Disease Society of America guidelines recommend targeted screening of high-risk persons followed by further clinical evaluation of all those with a reactive PPD (FIGURE).2,10 The recommended treatment regimen for latent TB is daily INH for 9 months. Less preferable regimens are daily INH for 6 months, or daily rifampin for 4 months in patients who cannot tolerate INH. A 2-month course of rifampin and pyrazinamide is no longer recommended. The recent meta-analysis supporting a 3-month regimen of combination INH and rifampin has not been incorporated into expert guidelines.7
1. Diagnostic standards and classification of tuberculosis in adults and children. Am J Respir Crit Care Med 2000;161:1376-1395.
2. Targeted tuberculin testing and treatment of latent tuberculosis infection. Am J Respir Crit Care Med 2000;161:S221-S247.
3. Jasmer RM, Nahid P, Hopewell PC. Clinical practice. Latent tuberculosis infection. N Engl J Med 2002;347:1860-1866.
4. Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis. A general review. Bibl Tuberc 1970;26:28-106.
5. Efficacy of various durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the IUAT trial. Bull World Health Organ 1982;60:555-564.
6. Comstock GW. How much isoniazid is needed for prevention of tuberculosis among immunocompetent adults? Int J Tuberc Lung Dis 1999;3:847-850.
7. Ena J, Valls V. Short-course therapy with rifampin plus isoniazid, compared with standard therapy with isoniazid, for latent tuberculosis infection: a meta-analysis. Clin Infect Dis 2005;40:670-676.
8. Jasmer RM, Saukkonen JJ, Blumberg HM, et al. Short-course rifampin and pyrazinamide compared with isoniazid for latent tuberculosis infection: a multicenter clinical trial. Ann Intern Med 2002;137:640-647.
9. Hong Kong Chest Service/Tuberculosis Research Centre, Madras/British Medical Research Council. A double-blind placebo-controlled clinical trial of three antituberculosis chemoprophylaxis regimens in patients with silicosis in Hong Kong. Am Rev Respir Dis 1992;145:36-41.
10. Taylor Z, Nolan CM, Blumberg HM. Controlling tuberculosis in the United States. MMWR Recomm Rep 2005;54(RR-12):1-81.
1. Diagnostic standards and classification of tuberculosis in adults and children. Am J Respir Crit Care Med 2000;161:1376-1395.
2. Targeted tuberculin testing and treatment of latent tuberculosis infection. Am J Respir Crit Care Med 2000;161:S221-S247.
3. Jasmer RM, Nahid P, Hopewell PC. Clinical practice. Latent tuberculosis infection. N Engl J Med 2002;347:1860-1866.
4. Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis. A general review. Bibl Tuberc 1970;26:28-106.
5. Efficacy of various durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the IUAT trial. Bull World Health Organ 1982;60:555-564.
6. Comstock GW. How much isoniazid is needed for prevention of tuberculosis among immunocompetent adults? Int J Tuberc Lung Dis 1999;3:847-850.
7. Ena J, Valls V. Short-course therapy with rifampin plus isoniazid, compared with standard therapy with isoniazid, for latent tuberculosis infection: a meta-analysis. Clin Infect Dis 2005;40:670-676.
8. Jasmer RM, Saukkonen JJ, Blumberg HM, et al. Short-course rifampin and pyrazinamide compared with isoniazid for latent tuberculosis infection: a multicenter clinical trial. Ann Intern Med 2002;137:640-647.
9. Hong Kong Chest Service/Tuberculosis Research Centre, Madras/British Medical Research Council. A double-blind placebo-controlled clinical trial of three antituberculosis chemoprophylaxis regimens in patients with silicosis in Hong Kong. Am Rev Respir Dis 1992;145:36-41.
10. Taylor Z, Nolan CM, Blumberg HM. Controlling tuberculosis in the United States. MMWR Recomm Rep 2005;54(RR-12):1-81.
Evidence-based answers from the Family Physicians Inquiries Network